reasons for missing appointments in general
advertisement

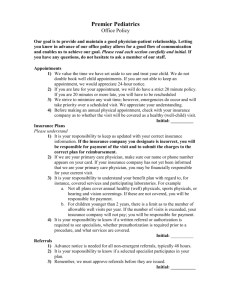
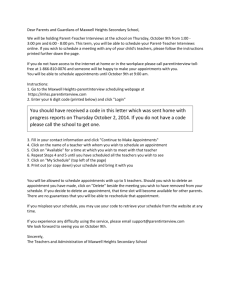
Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers RESEARCH ARTICLE REASONS FOR MISSING APPOINTMENTS IN GENERAL CLINICS OF PRIMARY HEALTH CARE CENTER IN RIYADH MILITARY HOSPITAL, SAUDI ARABIA Zahi Alhamad Department of Family and Community Medicine, Prince Sultan Military Medical City, Riyadh, Saudi Arabia Correspondence to: Zahi Alhamad (mezo106@gmail.com) DOI: 10.5455/ijmsph.2013.2.256-265 Received Date: 07.01.12013 Accepted Date: 07.01.2013 ABSTRACT Background: Non-attendance in general practice has received increasing attention over the past few years. Its relationship with access to health care has been recognized. Missed appointments have serious clinical and economic consequences. Aims & Objective: This study aims to identify the reasons for missing appointments in general clinics in Alwazarat health care center during the period from December 2010 to March 2011. Material and Methods: All eligible patients who missed appointments to general clinics, in Alwazarat center and controls that show up for their appointment, were enrolled in the study using quasi-randomization for sample selection. On the same day of missing the appointment three clerks were assigned by the doctor in-charge of the center to assist in data collection. A structured phone interview was conducted with patients enrolled in the study and the control group using a validated questionnaire. Results: The demographic factors associated with missing appointments were: female gender, younger age group and poor socioeconomic status. The important top five causes for missing appointments were: difficulty booking an appointment, work commitment, long distance travel, unavailability of transportation, visiting another health care facility. Among the group who missed appointment, the impact of missing appointment on health care service was unknown. Conclusion: Knowledge of the factors that are associated with missed appointments facilitates the prospective identification of patients at risk of missing appointment and helps the continuous quality improvement for future planning which may include program modifications, and formulation of strategies to reduce the risk and rate of nonattendance. KEY-WORDS: Missed Appointments; Primary Health Care; Saudi Arabia Introduction Failure to keep scheduled clinic appointments (missed appointments, no-shows, nonattendance) is a common problem in ambulatory settings. Thousands of patients miss their appointments every year in all kinds of practices including general practice clinics.[1] Little is known about which patients miss appointments or why they do so. At one end of the spectrum such people may be seen as a vulnerable group with multiple health problems and difficult lives, while at the other end they may be considered as nuisances who repeatedly fail to keep appointments which could have been used more gainfully for people in greater need.i Indeed, while missed appointments may be welcomed by many general practitioners (GPs), they are clearly seen as a source of frustration by others.[2] 258 International Rates of missed appointments vary among countries, and according to practices, patient mix and type of settings. Studies reported missed appointment rates in the range of 2% to 30% with higher rates pertaining to psychiatric settings.[3-7] Locally two studies from Saudi Arabia eastern and central region found very high rates of missed appointments 23.7% and 30% [1,8] respectively. The current prevalence is yet to be determined. Missed appointments have serious clinical and economic impacts. It disrupts continuity of patient care, delays treatment, and affects doctor–patient relationship and increases the cost of health care.[4] The non-attendance of clinic appointments impacts negatively on patient care, since patients may miss out on the opportunity to receive treatment or screening for their illness.[2] Non-attendance of International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers appointments is one of the major contributors to poor control in diabetic patients. ii A study conducted in USA (2005) revealed that missed appointment was the most significant factor related to treatment failure.[3] Missing the appointment and late cancellation preclude other eligible patients from receiving care they deserve, exerts a huge strain on the system and prolongs booking and waiting time in the clinic for other patients.[9] It also deprives other patients of earlier appointments which affect their quality of care.[1] Furthermore, the non-attendance of prescheduled appointments adds to the frustrations of health care providers who already have difficulty in managing the patient load on the clinics. Economically, missed appointment has significant impact on the ability to provide efficient and effective outpatient services. It results in wasting financial and social costs.[6,7] A study evaluating the financial significance of failed appointments revealed that non-attendance results in allocated resources not being utilized.[3] The social cost of missed appointment is the costs of unused or misused resources such as ward capacity and possible misuse of patients’ time.[5-8,10,11] This puts an extra load on the health care system and costs the ministry of defence a large amount of money and contributes to depletion of limited resources. Apart from few studies done in Saudi Arabia[1.8] the subject of missed appointments was not widely studied. Fewer studies were carried out in primary care setting.[3,4] The reasons for missing scheduled or "booked" appointments in general practice in Saudi Arabia were not particularly addressed yet. Previous research has been conducted in a variety of practice settings in USA[5,12] and Europe[8,9,13] to elicit determinants of non-attendance. The factors identified include: younger age, single marital status, health belief factors, patients who have larger families and less education, low socioeconomic class and previous history of missed appointments; but no factor has been persistently evident in all studies. The causes in our population might differ and they are expected to be different from those in other countries and societies according to the special cultural, religious and local characters of the Saudi society. 259 Over the last several years there has been a lot of apparent development in the health care system in Saudi Arabia. Hence reasons and prevalence of non-attendance are expected to have changed somehow. Factors that were not associated with the problem at that time could be significant nowadays, e.g. travel time and travel distance.[8] In a military population health seeking pattern and behavior might differ due to the nature of work and could have an impact on keeping the appointments of the person and his family as well. Factors among RMH patients are expected to be different, especially because no study has been carried out in Riyadh Military Hospital (RMH) to identify such reasons. This study is meant to fill an important gap of knowledge about the Saudi population (especially military) with regard to keeping health care appointments. It aimed at identifying the reasons for missing appointments in general clinics in one of primary health care centers in Riyadh during the period from December 2010 to March 2011. Materials and Methods This is a cross sectional study investigating the rate and causes of missing appointments in Alwazarat primary health care center in Riyadh at the end of year 2010 and start of 2011. In Riyadh military hospital the main family and community medicine center is located in Alwazarat neighborhood. Alwazarat family and community health center is located in the central area of Riyadh where most of the ministries and two other hospitals are located in close proximity. It serves a population of approximately 250,000 most of them being military personnel, ministry of defense staff and their dependent families. About forty clinics are being operated daily in sessions starting from eight o'clock a.m. till four o'clock p.m. The clinics are run by staff of general practitioners ranging from senior house officers to senior family medicine consultants of both genders. In addition to general clinics and chronic disease clinics designed for the follow up of patients of chronic diseases e.g. diabetes, hypertension, bronchial asthma, the center includes some outreach clinics of the main hospital for pediatrics, International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers dermatology, ophthalmology antenatal, well baby and well woman which are being run by specialized doctors in those fields. Scheduling appointments in Alwazarat PHC center is being done by several means; patients can book an appointment through telephone, RMH website, or could be referred by the physician or given follow up appointments in chronic disease clinic. For general clinics the appointments are booked within one day only. All patients who booked appointments to general clinics, in Alwazarat center, whether the appointment was made through telephone call, RMH internet web site or made in person, were considered eligible. A study group of patients who missed their booked appointments and a control group of patients who showed up for their appointment in the same day were selected until the total sample size was reached. Sample Size The sample size was estimated to determine the prevalence of any cause of missed appointment of 20% or more, with a 3% absolute precision and a 95% level of confidence. Using the single proportion equation for dichotomous variables (Epi-Info 6.04), the calculated sample size was 682 subjects. After adjustment for a dropout rate of 10%, it was estimated to be 760 subjects, 380 subjects in each group. A list of non-attendees and controls, which show up for their appointment, were retrospectively identified and considered to be enrolled in the study. A systematic random sample of every third patient was obtained. Patients were contacted on the same day of missing the appointment to avoid recall bias and confounding factors like preweekend days, bad weather and heavy traffic. Working Definition of Missing Appointment 1. Non-attending patients were defined as patients who missed at least one prescheduled appointment with the general clinic in Alwazarat center during the period from December 1st 2010 to March 31st 2011. 2. Patients who showed up later than the appointment time and were not seen were also classified as non-attending. 260 Inclusion criteria were patients who had scheduled appointments in general clinics in the study period were included in the sampling frame. All patients included in the study were required to be able to speak and understand Arabic or English. In addition to guardians on behalf of their children who were 18 years of age or younger. Exclusion criteria were patients who do not have contact telephone numbers registered in the system. If a family of two or more missed an appointment they were counted as one regardless of their number. In addition to patients who are unable to respond due to physical or mental disability. Three clerks were assigned by the doctor in-charge of the center to assist in data collection. A structured phone interview was conducted with patients of the study and the control group. Each clerk attended a two-hour training orientation session, and additional training was gained during the pilot study. Clinic appointment records and attendance registers were used to identify those patients who had prescheduled appointments and those who failed to attend. At the end of Session two for each working day (4 p.m.), a list was made by a senior clerk who was assigned to this job by the doctor in-charge of the center. The list included names of the patients, medical record numbers and the available contact numbers of all non-attending patients, and controls for whom contact details were available, from this list the first and every third patient were selected to be phoned within one day of missing the appointment. Consent for the study was obtained from patients verbally. If the mobile number was invalid or the call was not answered the land line was tried if available. If the person was not available at that time another call was made within one day before considering the patient as a non-responder. The phone interview was conducted by the researcher himself with the help of two male and one female clerk. The female clerk conducted the interview with female patients when appropriate. The assisting clerks received training on how to conduct the telephone interview in a standard 2-hour session to minimize interviewer bias. The calls were made from Alwazarat center between 3 p.m. and 8 p.m. International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers Saturday through Wednesday from December 1st 2010 to 31st March 2011. The data collection tool in this study is a questionnaire designed for both defaulters and controls. It was developed by the researcher to collect data via telephone interview. Time allocated for each interview was about an average of seven minutes (estimated from the pilot study). The questionnaire was adopted from several relevant studies. It was modified, appraised and distributed to three consultants to evaluate it regarding clarity and suitability to study objective. A list of 14 items found to be the reasons for missed appointments in previous studies 14-17 were identified and administered to respondents. The initial version of the questionnaire was field tested as a pilot of about 5% of the total sample size, to test for applicability. It was revised into its final format and the time allocated for the phone interview was adjusted. Issues addressed in the questionnaire included demographic and socioeconomic data, satisfaction with overall past clinic experience, and reasons for missing appointments. The study protocol was submitted for approval to the Research Committee of the Family and Community Medicine department in Riyadh Military Hospital. Verbal consent was obtained from all the participants in the study by phone and all participants were reassured regarding the anonymity and confidentiality of the study results and that this study was not going to affect their future access to health care services. Data Entry and Analysis Data was entered on daily basis directly into SPSS program, version 17 which was used for analysis. Demographic and socioeconomic factors of both groups were analyzed and compared. The two groups were compared, using Chi squared as the main statistical significance test to assess the difference between the study and control groups. Results The study included 750 subjects of which 653 subjects agreed to participate in the study and completed the telephone based questionnaire giving a response rate of 85.9 %. Around 14 % of patients 261 in both groups declined to participate in the study or could not be reached after several attempts. The response rate in the study group was (84%) and in the control group was (86%). Table 1 shows the basic demographic characteristics of the participants in study and control groups. Male participants in the missed group were significantly lower than females, 23.1 % vs. 76.9 % respectively. More than 60% of participants in both groups were below the age of 40. Around 52.3% of the participants had a crowding index of less than one. Around 78.4 % of patients in the missed group had a crowding index of One or more as compared to 69.3% in the control group (P = 0.008). There was no relationship between the marital status and adherence to appointment. Results showed that number of children in the family was not a significant factor for missing appointment (P= 0.8). The level of education was found to be of a significant factor between the two groups only at the level of patients who were illiterate or without formal education, where these were more in the group who missed an appointment. The distribution of other classes of education was similar in the two groups. Employed participants were significantly higher in control group compared to the group who missed the appointment. Regarding the means of transportation it was patients who used their own cars who were more likely to keep their appointments. More people in the missed group were dependent on others to drive them to the clinic than in control group, 78.7% vs. 51.9% respectively. Table 2 shows the causes that were associated with missing appointment. Most frequently reported causes by study group were: difficulty booking an appointment, long distance travel, work commitment, unavailability of transportation and visiting another health care facility. The overall reasons for missing appointments ranked in descending order. Most frequent causes for missing appointment reported by both groups in descending order were: difficulty booking an appointment, work commitment, long distance travel, unavailability of transportation and visiting another health care facility are the top factors mentioned. Table 3 demonstrates the factors associated with missing appointments. the trip duration between the two groups was not a significant factor. Patients International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers who missed an appointment were more likely to be dependent on others for transportation (P=0.001). People in the missed appointment group were significantly more likely to have missed an appointment in the past than their controls 63.4% Vs 43.5% (P=0.001). The mean frequency of missing appointment in the Missed appointment group is significantly higher than that in the Control group. It indicated that defaulters showed a significantly greater tendency to miss more appointments compared to controls. (P=0.02). Patients who kept their appointments expressed more dissatisfaction with the service than patients who missed the appointment and vice versa. Table-1: Demographic Data of the Missed Appointment Group and Controls Group P Missed Control Variable χ2 value (N=347) (N=306) N (%) N (%) Gender Male 80 (23.1) 146 (47.7) 43.7 0.001 Female 267 (76.9) 160 (52.3) Age 0-20 73 (21) 36 (11.7) 10.05 0.001 21-40 162 (46.7) 168 (55) 4.39 0.03 41-60 83 (23.9) 79 (25.8) 0.31 0.57 60+ 29 (8.4) 23 (7.5) 0.16 0.69 Crowding index <1 75 (21.6) 94 (30.7) 7.03 0.008 1+ 272 (78.4) 212 (69.3) Marital status Single 36 (10.4) 29 (9.5) Married 294 (84.7) 267 (87.3) 1.3 0.52 Divorced/ widow 17 (4.9) 10 (3.3) No. of children Zero 87 (25.1) 81 (26.5) 1-2 95 (27.4) 79 (25.8) 3—4 96 (27.7) 87 (28.4) 1.3 0.856 5—6 49 (14.1) 37 (12.1) 7 or more 20 (5.8) 22 (7.2) Educational level No Formal Education 73 (21) 32 (10.4) 6.38 0.01 (Illiterate/read & write) Basic Education (Elementary/ 60 (17.3) 87 (28.4) 3.28 0.07 Intermediate) high school/ Diploma 161 (46.4) 139 (45.4) 0.04 0.84 university level 53 (15.3) 48 (15.7) 0.02 0.88 Employment status Employed 105 (30.3) 139 (45.4) 15.9 0.001 Unemployed 242 (69.7) 167 (54.6) Town of residence Riyadh 338 (97.4) 294 (96.1) 0.92 0.337 Out of Riyadh 9 (2.6) 12 (3.9) Table 4 shows the awareness of the impact of missing appointments. Patients in the control group were more aware of the impact of missing 262 appointments on the service than those in the study group 74.2% Vs. 64.3% respectively, the difference been statistically significant. Both groups are similarly aware of the impact of missing appointments on their health. Table-2: Causes of Missing Appointments Reported by Patients who missed an appointment and their controls, arranged in descending order of frequency according to the Missed group Group P Missed Control Reasons χ2 value N=347* N=306* N (%) N (%) Difficulty in booking 159 (45.8) 138 (45.1) 0.03 0.85 appointment Long distance travel 119 (34.3) 108 (35.3) 0.07 0.78 Work commitment * 113 (32.6) 132 (43.1) 7.75 0.005 Unavailability of 112 (32.3) 104 (34) 0.30 0.58 transportation Visiting another health care facility or alternative 65 (18.7) 55 (18) 0.06 0.80 medicine. child care 49 (14.1) 30 (9.8) 2.85 0.09 Not having a companion. 40 (11.5) 34 (11.1) 0.03 0.86 Inconvenient appointment 38 (11) 47 (15.3) 2.8 0.09 time Feeling better 23 (6.6) 30 (9.8) 2.2 0.13 Forgetting the appointment 20 (5.8) 38 (12.4) 8.9 0.002 * Mix up over the date/time of the appointment by pt or 13 (3.7) 9 (3) 0.32 0.56 practical error Not being well enough to 10 (2.8) 13 (4.2) 0.89 0.34 attend Long waiting time at the clinic from previous experience/ Perception of 6 (1.7) 42 (13.7) 34.3 0.001 Disrespect by the Health Care System * financial difficulties 5 (1.4) 8 (2.6) 1.15 0.28 Others 16 (4.6) 20 (6.5) 1.16 0.28 * Responses are not mutually exclusive. Table-3: Factors Associated with Missing Appointments Group P Factors χ2 Missed Control value N (%) N (%) < 30 67 (19.3) 70 (22.9) Trip Duration 31 – 60 233 (67.1) 196 (64.1) 1.25 0.53 (minutes) > 60 47 (13.5) 40 (13.1) Means of Dependent 273 (78.7) 159 (51.9) 51.8 0.001 Transport Independent 74 (20.3) 147 (48.0) Previously Yes 220 (63.4) 133 (43.5) Missed 26.02 0.001 No 127 (36.6) 173 (56.5) Appointment Dissatisfied 15 (4.5) 37 (12.8) 13.4 <0.001 Patient’s Neutral 21 (6.3) 29 (10.0) 2.7 0.10 Satisfaction Satisfied 300 (89.3) 224 (77.3) 18.0 <0.001 Mean frequency of missing 1.56 1.36 0.026# appointments * Driven by a relative/taxi; ** own car/own driver; # P-value of Mann-Whitney test International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers Table-4: Awareness Appointments Reasons On Health Care Services On Health Yes No Yes No of the Impact Group Missed Control N (%) N (%) 223 (64.3) 227 (74.2) 124 (35.7) 79 (25.8) 321 (92.5) 289 (94.4) 26 (7.5) 17 (5.6) of Missing χ2 P value 7.47 0.006 0.99 0.32 Figure-1: Percentage of Patients Favouring Confirmation of Appointments in the Missed Appointment Group and Control Figure-2: Percentage of Patients Favouring Certain Appointment Confirmation Method Figures 1 and 2 show that the vast majority of patients, in both groups, prefer to be reminded of their appointments, and most of them, prefer the confirmation with an SMS on their cell phones. Discussion The response rate reported in the present study is magnificent. It was possible with the continuous support of the department administration and fully dedicated data collectors who worked around the day including afternoon sessions and after hours to maximize the chances of patient availability and response. Most of the other studies done on this topic had variable and unpredictable response rates which ranged from 25% to 93% for studies conducted through telephone interviews.[11, 25] 263 The reasons for missing appointments in this study were approached on three main dimensions that is; the socio-demographic characteristics, what the patient perceives as cause of the problem and what could be verified as one through comparison with the control group. Regarding demographic variables female gender, young age group and poor socioeconomic status; in terms of high crowding index, lack of formal education and unemployment, were the factors associated with missing appointments. Neal RD et al. studied missing appointments in U.K. at primary care level and found female gender to be associated with missing appointments.[3] This study shows the same finding again despite that other local studies did not detect such a difference.[19] This disagreement could be due to different study methodology and population. This study shows that young patients below twenty years are more likely to miss an appointment than older patients. Patients between 21 and 39 years of age are more likely to keep theirs. The possible explanation for this observation could be the larger young population proportion in the community which is represented in the study sample. According to World Health Organization statistics in 2009, youth constitute the majority population in the Kingdom of Saudi Arabia.[3] R D Neal et al, and Nour El-Din et al. found that younger patients were more likely to miss appointments and missing appointments decreases with increase of age.[1,2] By doing sub-group analysis of those patients below twenty years of age the most commonly cited cause for non-attendance in both groups was difficulty booking an appointment followed by visiting another health care facility. It is known that acute illnesses are more common in younger age group. Parental anxiety at the time of acute illness and fearing the consequences of delayed medical consultation might lead to seeking urgent care e.g. Emergency department care, and hence not showing for the clinic appointment. Other top causes were related to parents' or guardians' limitations i.e. work commitment, long distance travel, child care and unavailability of transportation. Grruzd et, al. and Vikander et, al. reported better adherence to appointments in patients with chronic illness.[3,4] International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers Income, education, occupation and wealth are the important determinants of socioeconomic status. Crowding index is a tool used to assess socioeconomic status and income. It was found that socioeconomic status is a key factor for utilization of health care. Low socioeconomic level and living in deprived areas are indeed related to the deterioration of health care and its related measures including missing appointments.[2] In consistence with that, this study shows that, compared to controls, defaulters were more likely to: have a higher crowding index, lack formal education and be unemployed. As a result it is reasonable to conclude that missing appointments is associated with low socioeconomic status. Waller J et al, found that patients who miss appointments tend to come from a lower socio-economic class.[4] Neal RD, and others found that living in deprived area is associated with missing appointments in general clinics.[2,10] Several studies done in USA found that socioeconomic class is of [13,14,31] importance. Some of deprived groups also consult more, and it may be that they miss more appointments as a result of their making more appointments. Neal RD et al found that over 90% of the patients who missed an appointment subsequently consulted within three months and of these nearly 60% consulted for the stated problem that was going to be presented in the missed consultation.[28] It can be referred to as “Default as a function of attendance”.[3] Having a lower socioeconomic class is associated with having less education, being unemployed and having fewer resources. Non-attenders are less likely to own a car or a telephone and are more likely to be unemployed.[35,34] The effect of educational level was not detected in other studies, which may be due to smaller sample size.[3] The effect of socioeconomic factors cannot be ignored when looking at the reasons for missing appointments. Most of the reasons mentioned for missing appointment did not differ significantly between study group and controls. The following reasons were most frequently mentioned to justify missing an appointment by both groups : difficulty booking an appointment, work commitment, long distance travel, unavailability of transportation, visiting another health care facility, inconvenient 264 appointment time, child care, not having a companion, forgetting the appointment, feeling better, long waiting time / perception of disrespect by the health care system. This order is very similar to reasons found in other studies in U.S.A, U.K. and K.S.A.[1,9,18,19,21] Among the above mentioned reasons, work commitments, long waiting time and forgetfulness were cited more by controls (P<0.05). The first category of reasons is related to transportation. Missing appointments due to long distance, the most frequently cited reason, could be affected by other factors such as unavailability of transportation and financial difficulties. Easily accessible location of a health care center is very important part of access to care. Despite that the majority of participants (~97%) were residents in Riyadh, and the study center being located in the central area, long distance travel was a leading cause of missing appointments in the study group. Factors to blame could be centralization of health care to one center and traffic jams. Riyadh is a big, quickly growing and very crowded city. It has more than four major sections. Traffic jam problems have received a lot of formal and public attention in the last few years. Our results show that one-way trip to Alwazarat center takes about 31- 60 minutes for more than 60% of patients in either group. Finding transportation was a major problem for unemployed, females, with no-formal education. Transportation system in Saudi Arabia is based solely on private vehicle transportation. Driving and driver’s license is limited to males who are eighteen years of age or older. Other options for transportation are personal drivers and taxis, which are relatively expensive. Sometimes it is socially not acceptable for females to use the latter two without the company of a chaperon. Public transportation is not developed yet and not used by people for everyday within-city transportation. This could explain why the majority of patients with transportation difficulties are unemployed female patients. Around 78% of patients who reported unavailability of transportation were unemployed, majority of whom were females. Not working appears to create a hardship for getting transportation to an appointment. Detman et al. found that lack of formal education and International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers unemployment is linked to transportation problems leading to missing appointments. Patients who did not have formal education and those who were not working, were three and four times, respectively, more likely to report being unable to get a ride to the clinic as a barrier to keeping an appointment.[10] G Van der Meer and J.W. Loock found that Transportation constraints and long distance are the main reasons for missing appointments among cancer patients in South Africa.[38] It is not immediately clear why not working should prevent finding transportation to the clinic. Besides having better financial resources and being able to afford it, one possible explanation is that working men and women usually arrange for their work transportation which makes it easier to arrange for a ride for other purposes. The lack of a ride to the clinic is also a structural problem. Individuals lacking adequate means to get to the clinic experience hardship that is further exacerbated structurally by less than accessible public transportation and limited governmentfunded transportation. Financial constraints could restrict some people from getting a ride to the clinic. Alshammary et al., thought that the economic factors were irrelevant in terms of cost of health care as the service in governmental hospitals in Saudi Arabia is free.[19,20] That being true, the most pronounce effect of poor financial resources could be projected again on transportation, especially because income and crowding index figures point towards limited affordability of paid transportation. The second category of reasons is related to commitments and logistic difficulties. Sometimes patients miss doctor appointments because they have to manage other responsibilities, e.g. child care, work commitments, or because they do not have the necessary support e.g. not having a companion, or a baby sitter. According to other responsibilities the appointment time could be viewed as inappropriate. Those who reported child care as a reason for missing appointment were more in the study group. However, number of children was not significant factor. Campbell et al. identified child care as a cause for missing appointments. [3] Waller J. et al, and Beauchant S. et al. suggested that patients with low paid jobs may have difficulty in getting time off work or arranging 265 childcare.[4,35] Some patients, especially elderly and the less educated, face greater difficulty finding their way around new places. Not having a companion would lead to missing appointments for such groups. The time restriction resulting from appointment system is almost inevitable. Patients might not always have a choice to decide the appropriate time for their appointment. Enabling patients to do so might help reducing rate of nonattendance. While short booking has its advantages it comes to a down side when patient has other commitments and need to re-arrange their schedule in one day notice. Work commitment could be looked at from two angles. It could be of the patient himself or a person on whom the patient is dependent for transportation or escort, especially females, children and elderly who are more dependent on others for these matters. This could explain the higher prevalence of missing appointments in the younger age group. Forgetfulness as a cause of default was reported in the literature[9,10,19] Neal R. reported a prevalence of 40% in a study that included patients from seven practices in Yorkshire.[28] Contrarily in this study it was reported more in the control group in comparison to defaulters. As a matter of fact significantly fewer defaulters reported forgetting the appointment as a reason compared to controls (5.8% Vs 12.4%) (P=0.002). This might indicate that forgetting the appointment is rather used as an excuse than a real cause. Sometimes patients will realize late that they will not be able to attend, or that they don’t need to because they feel better. The lack of a clear and easy policy for cancelling appointments is a major concern. Large brochures and printed instruction leaflets on how to make and cancel appointments would be appropriate. Local studies found a relationship between the duration of intervals between appointments and keeping them and related that to forgetfulness of the appointment.[1,19,20] These studies were conducted in outpatient settings in secondary and tertiary hospitals, where appointments could be scheduled after weeks or months. This issue is eliminated in our setting of general primary care clinics where booking is initiated by patients one day prior to appointment time. In a study done in U.S. forgetting an appointment was cited as a top reason for missing both prenatal and paediatric International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers appointments despite current health department policy to phone clients with scheduled appointments the day before to remind them of the appointment. Costa et al, found that adoption of a reminder /recall system is successful in reducing rate of missing appointments.[3] Wilkinson M. suggested that the default rate of frequent nonattenders can be reduced by sending a simple letter, the effect lasting at least nine months. The subsequent number of booked appointments may also be reduced.[3] Dissatisfaction was expressed more in control group compared to defaulters. Dissatisfaction was shown also in the reasons mentioned for missing an appointment in this group such as long waiting time and perception of disrespect (P<0.05). This finding could not be directly explained. The data collection method could have led to interviewer bias which might play a role in this result. Realizing that long waiting time might affect rate of keeping appointments most of patients did not realize that prolonged waiting time is further enhanced by missing appointments and disrupting the clinic schedule. Other studies reported significant effect of patient satisfaction with services as a factor for adherence to appointments, patients who were satisfied with the service kept their appointments better.[3,7,21] Lack of awareness of impact of missing appointments on the service is thought to play an important role. Most patients in the missed appointment group were unaware of the implications of missing appointments. Lacy et al. found that patients were unaware of the financial impact of failed appointments and believed missing appointments may actually be a positive event for the clinician and staff.[7] there was no significant difference in patients beliefs regarding the impact of missing appointments on their health, between the two groups. Apathy i.e. being careless is thought to stand out when looking at patterns of habitual defaulting. It can be a factor that is somehow related to human nature, dissatisfaction and lack of rules. Humans tend to ignore regulations if there were no potential consequences. The habitual pattern is significantly more obvious among the missed appointment group. Murdock et al suggest that patient apathy plays a large role in the current burden of missed 266 appointments.[23] Cosgrove reported defaulting as a significant factor.[34] habitual This study shows better adherence to appointments in patients who are coming for follow up of a chronic problem, general check-up or obtaining a referral to a specialist. Nour El-Din et al. found that visiting the clinic to obtain results of investigation was associated with higher rates of adherence to appointments.[1] Gruzd et al. and Vikander et al. reported better adherence in patients with chronic illness.[30,31] An explanation is that people who has chronic illnesses and have regular follow up tend to be more aware of the importance of appointments. The effect of that could be confounded by age and other factors. People who come for general check-up usually have higher level of self-care. It was reported in the literature that reason of visit is not a significant factor. A study conducted in Switzerland did not find any significant effect of the reason of visits on the rate of missed appointments.[22] Other sporadic causes included among others: having to leave on a mission for work, oversleeping, having car trouble or an accident, unexpected visitors and having another appointment in the main hospital. Conclusion Conclusively, females and younger age patients tend to miss their appointments more than others. The important top five causes of missing appointments were: difficulty booking an appointment, work commitment, long distance travel, and unavailability of transportation and visiting another health care facility. Developing a flexible, easily accessible, interactive appointment system with Reminder / Recall system is highly recommended. References 1. 2. 3. Nour Eldin M, Al-Shakhs FN, Al-Oudah S. Missed Appointments at a University Hospital in Eastern Saudi Arabia: Magnitude and Association Factors. J Egypt Public Health Assoc 2008; 83(5- 6): 415-433 Neal RD, Lawlor DA, Allgar VL, Colledge M, Ali S, Hassey A, et al. Wilson. Missed appointments in general practice: retrospective data analysis from four practices. Br J Gen Pract 2001; 51: 830-832. Beecham L. Missed GP appointments cost NHS money. [News extra.] BMJ 1999; 319: 536. International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2 Zahi Alhamad. Reasons for Missing Appointments in Primary Health Care Centers 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. 23. Waller J, Hodgkin P. Defaulters in general practice: who are they and what can be done about them? Fam Pract 2000; 17: 252-253. Johnson BJ, Mold JW, Pontious JM. Reduction and management of no shows by family medicine residency practice exemplars. Ann Fam Med. 2007; 5(6): 534-9. Penneys NS, Glaser DA. The incidence of cancellation and nonattendance at a dermatology clinic. Am Acad Dermatol. 1999; 40 (5): 714-8. Lacy NL, Paulman A, Reuter MD, Lovejoy B. Why we don't come: patient perceptions on no-Shows. Ann Fam Med. 2004; 2 (6): 541-5. Griffiths J. Missed appointments rise by 60%. GP 2001; August 24: 7. Mohamed BA, Al-Doghaither AH. Missed appointments at public hospitals in Riyadh, Saudi Arabia. Saudi Med J. 2002; 23(4):388-92 Detman, LA, Gorzka, P. A Study of Un-kept Appointments in a Florida County Health Department. Paper presentation at the One Goal Summer Conference, Tampa, Florida, July 2000. Available from URL (accessed on 15/7/2011): http://health.usf.edu/publichealth/chilescenter/pdf/mi ssed%20appointments.pdf Mollentze WF, Koning JMM. Where have all the diabetics gone? S Afr Med J. 2007; 97: 6. Berg MB, Safren SA, Mimiaga MJ, Grasso C, Boswell S, Mayer KH. Non-adherence to medical appointments is associated with increased plasma HIV RNA and decreased CD4 cell counts in a community-based HIV primary care clinic. AIDS Care. 2005; 17(7): 902-7. Denberg TD, Coombes JM, Byers TE, Marcus AC, Feinberg LE, Steiner JF, et al. Effect of a mailed brochure on appointment-keeping for screening colonoscopy. Ann Intern Med. 2006;145(12):895-900. Zailinawati AH, Ng CJ, Nik-Sherina H. Why do patients with chronic illness fail to keep their appointment? A telephone interview. Asia Pac J Public Health. 2006;18(1):1-2. Moore CG, Wilson-Witherspoon P, Probst JC. Time and money: effects of no-shows at a family practice residency clinic. Fam Med 2001;33: 522–7. Ngwenya BT, Van Zyl DG, Webb EM. Factors influencing non-attendance of clinic appointments in diabetic patients at a Gauteng hospital in 2007/2008. JEMDSA 2009;14(2):106-109. Martin C, Perfect T, Mantle G. Nonattendance in primary care: the views of patients and practices on its causes, impact and solutions. Fam Pract. 2005; 22(6): 638-43. Bech M. The economics of non-attendance and the expected effect of charging a fine on non-attendees. Health Policy. 2005; 74(2): 181-91. Al-Shammari SA. Failures to keep primary care appointments in Saudi Arabia. Fam Pract Res J 1992; 12: 171–176. Al-Shammari SA, Ali M, Alshammari AR, Armstrong K. Prevalence of No-shows at a family practice clinic, King Fahad National Guard Hospital, Riyadh. Saudi Med J 1993; 14 (6):527-531 George A, Rubin B. Non-attendance in general practice: a systematic review and its implications for access to primary health care. Fam Pract. 2003; 20(2):178-84. Lehmann TN, Aebi A, lehmann D, Balandraux Olivet M, Stalder H. Missed appointment at Swiss university outpatient clinic. Public Health. 2007; 121(10):790-9. Murdock A et al. Why do patients not keep their appointments? J R Soc Med, 2002;95:284-6. 267 24. Barron WM. Failed appointments: Who misses them, why they are missed, and what can be done. Prim Care. 1980; 7(4): 563-574. 25. Kiefe CI, Harrison PL. Post-hospitalization follow-up appointment-keeping among the medically indigent. Journal of Community Health 1993; 18(5): 271-282. 26. Mirotznik J, Ginzler E, Zagon G, Baptiste A. Using the health belief model to explain clinic appointmentkeeping for the management of a chronic disease condition. J Community Health1998, 23(3): 195-210. 27. Pesata V, Pallija G, Webb AA. A descriptive study of missed appointments: families’ perceptions of barriers to care. J Pediatr Health Care. 1999, 13: 178-182. 28. Neal RD, Gambles MH, Allgar VL, et al. Reasons for and consequences of missed appointments in general practice in the UK: questionnaire survey and prospective review of medical records. BMC Family Practice 2005, 6:47. 29. World Health Organization Statistics. Available from URL (last accessed on 14/7/2011): http://www.emro.who.int/emrinfo/index.aspx?Ctry=sa a 30. Gruzd DC, Shear CL, Rodney WM. Determinants of noshow appointment behavior: the utility of multivariate analysis. Fam Med 1986; 18: 217–220. 31. Vikander T, Parnicky K, Demers R, Frisof K, Demers P, Chase N. New patient no shows in an urban family practice center: analysis and intervention. J Fam Practice 1986; 22: 263-268. 32. Oppenheim GL, Bergmann JJ, English EC. Failed appointments a review. J Fam Pract 1979;8:789-796. 33. Goldman L, Freidin R, Cook EF, Eigner J, Grich P. A multivariate approach to the prediction of no-show behavior in a primary care centre. Arch Intern Med 1982;142: 563-567. 34. Cosgrove MP. Defaulters in general practice: reasons for default and patterns of attendance. Br J Gen Pract 1990;40,50-52. 35. Beauchant S, Jones R. Socio-economic and demographic factors in patient non-attendance. Br J Healthcare Manage 1997;3:523-8. 36. Sharp DJ. Non-attendance at general practices and outpatient clinics. BMJ 2001; 323:1081–2 37. Killaspy H, Banerjee S, King M, Lloyd M. Prospective controlled study of psychiatric out-patient non-attendance. Characteristics and outcome. Br J Psychiatry 2000;176:160-5. 38. Van der Meer G, Loock JW. Loock. Why patients miss follow up appointments: a prospective control-matched study. East Afr J Public Health. 2008 Dec;5(3):154-6. 39. Campbell JD, Chez RA, Queen T, Barcelo A, Patron E. The no-show rate in a high-risk obstetric clinic. J Womens Health Gend Based Med. 2000 Oct;9(8):891-5. 40. da Costa TM, Salomão PL, Martha AS, Pisa IT, Sigulem D. The impact of short message service text messages sent as appointment reminders to patients’ cell phones at outpatient clinics in São Paulo, Brazil. Int J Med Inform. 2010 Jan;79(1):65-70. 41. Wilkinson M J B. Effecting change in frequent nonattenders. Br J Gen Pract, May 1994;233. Cite this article as: Alhamad Z. Reasons for Missing Appointments in General Clinics of Primary Health Care Center in Riyadh Military Hospital, Saudi Arabia. Int J Med Sci Public Health 2013; 2:258-267. Source of Support: Nil Conflict of interest: None declared International Journal of Medical Science and Public Health | 2013 | Vol 2 | Issue 2