Document Development & Review Framework
advertisement

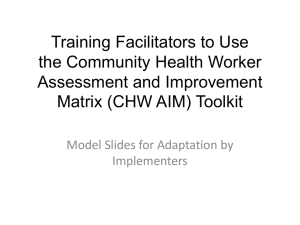
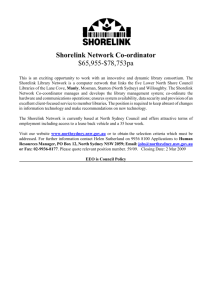
Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework DOCUMENT DEVELOPMENT AND REVIEW FRAMEWORK POLICY AND PROCEDURE © DOCUMENT SUMMARY/KEY POINTS Refer to the SCHN Document Development & Review Process flowchart. • The Director of Clinical Governance and Medical Administration has governance over SCHN policy processes. • SCHN document shall come under one Directorate. Directors are responsible for document development from within their area. • SCHN document development/review shall be underpinned by National and State policy (where available) and the respective Health Practitioner Code of Conduct and where applicable, Code of Ethics. • Line manager/s must approve/signoff new policy document development. • Document development and review teams should be multidisciplinary and consist of representatives of key stakeholders from the different SCHN facilities. • All key stakeholders must be given the opportunity to comment and approve the final draft of a document. • All SCHN documents must: o Be processed via ePolicy o Follow the endorsed approval process described in this policy. o Reflect considerations for family, cultural and ATSI health issues. o Be formatted using SCHN document templates. o Be reviewed within the defined review period. o Support best clinical or corporate practice (providing evidence where appropriate). o Be written in plain English • Documents are to be used ‘on-line’, wherever possible (hardcopies are discouraged). • Only one authorised version shall be available electronically at any one time. Approved by: Date Effective: Team Leader: SCHN Policy, Procedure & Guideline Committee 1st July 2014 Network Manager Policy & Procedures Review Period: 3 years Area/Dept: SCHN Clinical Governance Unit Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 1 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework CHANGE SUMMARY • Minor review to amend: o Review periods for documents with IV medications from annual to 3 yearly. o The approval process where SCHN PP&G are the peak approval body for SCHN documents and HCQC are notified of new documents. o Role titles of Clinical Governance Unit staff o At SCH, change in the location of where the hard copies are located. In the event where the intranet is down, SCH staff should go to the After Hours Nurse Manager office (i.e. no longer located in the Systems Integration Managers office). READ ACKNOWLEDGEMENT • All managers and any staff who are developing or reviewing a SCHN policy document should read this document. Approved by: Date Effective: Team Leader: SCHN Policy, Procedure & Guideline Committee 1st July 2014 Network Manager Policy & Procedures Review Period: 3 years Area/Dept: SCHN Clinical Governance Unit Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 2 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework SCHN Document Development and Review Process Flowchart Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 3 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework TABLE OF CONTENTS SCHN Document Development and Review Process Flowchart ....................................... 3 1 Introduction.................................................................................................................. 6 1.1 Purpose .........................................................................................................................6 1.2 Scope ............................................................................................................................6 1.3 Outcomes ......................................................................................................................6 1.4 Legislative Context ........................................................................................................ 6 1.5 Definitions ......................................................................................................................7 1.6 Abbreviations ................................................................................................................. 8 2 Policy and Principles .................................................................................................. 9 2.1 Principles .......................................................................................................................9 2.2 Policy .............................................................................................................................9 Governance .........................................................................................................................9 Document Review................................................................................................................ 9 Major amendments ............................................................................................................ 10 Minor amendments and no amendments .......................................................................... 10 Records Management ....................................................................................................... 10 3 Procedures ................................................................................................................. 11 3.1 Developing a Document .............................................................................................. 11 1. Needs Analysis ........................................................................................................ 11 2. Obtain approval to proceed...................................................................................... 11 3. Submit a request in ePolicy to DEVELOP a document ............................................ 11 4. Form a Document Development Team (DDT) ......................................................... 11 5. Perform a Literature Search ..................................................................................... 12 6. Drafting the Document ............................................................................................. 13 7. Establish a Risk Rating for the document ................................................................ 14 8. Consultation ............................................................................................................. 14 9. Submit draft document into ePolicy ......................................................................... 14 3.2 Reviewing a document ................................................................................................ 15 1. Mandatory Review Period ........................................................................................ 15 2. Submit a request in ePolicy to REVIEW a document .............................................. 15 3. Form a Document Review Team (DRT) .................................................................. 15 4. Review the document .............................................................................................. 15 5. Consultation ............................................................................................................. 16 6. Submit REVIEWED document into ePolicy ............................................................. 16 7. Overdue Documents for review ............................................................................... 16 3.3 Approval Process ........................................................................................................ 17 1. Stakeholder approval ............................................................................................... 17 2. Governing Committee approval (if necessary) ......................................................... 17 3. SCHN Policy, Procedure and Guideline Committee approval ................................. 17 4. Minor Amendment approval ..................................................................................... 17 5. Urgent Approval (performed in exceptional circumstances only) ............................. 18 4 Ad-hoc Feedback from staff ..................................................................................... 18 5 Document Implementation ....................................................................................... 19 6 Notification and Communication ............................................................................. 20 Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 4 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 7 Applying Risk ratings to SCHN documents ............................................................ 20 7.1 How assign a risk rating to a document ....................................................................... 21 8 Document Evaluation and Monitoring Compliance ............................................... 22 8.1 Additional compliance monitoring processes .............................................................. 23 Regular Auditing Program – SCHN documents................................................................. 23 Departmental Notification records – Auditing Program...................................................... 23 9 Availability of documents in the event of a Disaster ............................................. 23 9.1 Hard copies ................................................................................................................. 23 9.2 Electronic (soft) copies) ............................................................................................... 23 10 Processing NSW Ministry of Health Policy Documents ........................................ 24 11 Accountability Framework ........................................................................................ 24 11.1 Retention and Disposal of SCHN documents .............................................................. 24 11.2 Document Numbering System ..................................................................................... 24 11.3 When a document becomes active? ........................................................................... 25 12 Processing of Other Documents .............................................................................. 25 12.1 Standing Orders, Nurse Initiated Medication & Drug Protocols ................................... 25 12.2 Local Disaster Response Plans (at CHW) ................................................................... 25 12.3 Local Emergency Plans (at SCH) ................................................................................ 26 13 Bibliography............................................................................................................... 26 Appendix 1: Escalation process for policies overdue for review .................................... 27 Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 5 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 1 Introduction The Sydney Children’s Hospitals Network (SCHN) has a document development and management framework that will permit documents to be identified, developed, evaluated and reviewed in accordance with NSW Health and the Australian Council on Healthcare Standards (ACHS) Accreditation requirements and the National Safety and Quality Health Service Standards (published by the Australian Commission on Safety and Quality in Health Care). The CHW framework is based on NSW Health Policy Directive PD2009_029 and the AGREE Collaboration (Appraisal of Guidelines, Research and Evaluation), an internationally recognised document evaluation system. 1.1 Purpose This document describes the policy and related processes for document development, dissemination, implementation, evaluation and review, and outlines associated responsibilities of those processes. 1.2 Scope This policy and procedure applies to all staff working at SCHN who are or intend upon developing or reviewing a policy document that pertains to SCHN. 1.3 Outcomes Compliance with this policy and procedure ensures sound governance and document control of all SCHN policy documents. This will provide confidence to staff that their work practices are underpinned by evidence based and/or current best practices. 1.4 Legislative Context • Australian Standards (AS3806 Compliance Monitoring, 8000 – 8004 Corporate Governance) • Australian Standard/New Zealand Standard (AS/NZS4360 Risk Management) • Australian Standard/New Zealand Standard ISO 9001Quality Management Systems – requirements. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 6 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 1.5 Definitions Term Definition Departmental document Document containing information pertaining to the operations in a single department at Randwick or Westmead facility. Document 'Document’ is synonymous with policy, procedure, practice guideline or homecare guideline. Facility specific document Document containing information pertaining to the values, core principles and operations of a SCHN facility (e.g. Randwick or Westmead). Titles are to be suffixed by “SCH” or “CHW” or “NETS” or “CCC” or “PSN” Homecare Guideline Homecare Guidelines provide information based on one or more SCHN Practice Guidelines, but is expressed in a ‘parent/carer friendly’ lay version. When Homecare Guidelines are reviewed, they are to be submitted to the PP&G Committee simultaneously with the relevant SCHN Practice Guideline or Procedure. Key Search Words Nominated intuitive words which are representative of the content found within the document that staff may use to generate a search for the document on the Intranet. Major Amendment A change to a current document that is of a substantial nature, affecting or altering the effect, responsibility, stakeholders, meaning or intent of any part of the document. Minor Amendment A change to a current document that is of an insubstantial nature, not affecting or altering the effect, responsibility, meaning or intent of any part of the document. Network document Document containing information pertaining to the values, core principles and operations of SCHN (Randwick, Westmead, NETS, PSN or CCC facilities). Policy A directive or decision that requires mandatory compliance and is expected to be understood by relevant staff. Practice Guideline A set of directions or principles to assist the health care practitioner with patient care decisions about appropriate diagnostic, therapeutic or clinical procedures for specific clinical circumstances and are based on a thorough review of the literature. Procedure A set of documented instructions detailing the approved and recommended steps for a particular process, and be evidence based and be consistently applied (no deviations). Stakeholder Any person or group of people who affects or is affected by the document. Transdepartmental document Documents containing information pertaining to the operations of 2 departments within a single facility (i.e. SCH or CHW) or between 2 facilities. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 7 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 1.6 Abbreviations Abbreviation Term ACHS Australian Council on Healthcare Standards AGREE Appraisal of Guidelines, Research and Evaluation [in Europe] ATSI Aboriginal or Torres Strait Islander CALD Culturally And Linguistically Diverse CCC Children’s Court Clinic CHW The Children’s Hospital at Westmead DDT Document Development Team DRT Document Review Team HCQC Health Care Quality Committee IIMS Incident Information Monitoring System MoH NSW Ministry of Health NETS Neonatal & paediatric Emergency Transport Service RCA Root Cause Analysis PD Policy Directive (from NSW Ministry of Health) PP&G Committee Policy, Procedure and Guideline Committee PSN NSW Pregnancy and newborn Services Network SCH Sydney Children’s Hospital SCHN Sydney Children’s Hospitals Network Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 8 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 2 Policy and Principles 2.1 • Principles SCHN document development/review shall be underpinned by: o National and State policy (where available) and o The respective Health Practitioner Code of Conduct and where applicable, Code of Ethics. Refer to the Australian Health Practitioner Regulation Agency (AHPRA) for more information. 2.2 Policy Governance • All SCHN documents shall fall under one of the SCHN Directorates with each Director being responsible for document development/review, implementation and compliance within their area. Note: Where possible, all facility specific policy documents are to be transitioned to become SCHN policy documents. • All documents shall be tabled at the SCHN Policy, Procedure and Guideline (PP&G) Committee for approval. • All new Network and Facility specific documents shall be tabled at the SCHN Health Care Quality Committee (HCQC) for noting by the Executive. • Documents produced (or reviewed) at SCHN must: o Support best clinical or corporate practice (providing evidence where appropriate). o Reflect (and reference) legislated practice or NSW Ministry of Health policy. o Adhere to the SCHN approval process. o Be developed by a multidisciplinary team. o Be written in plain English • All SCHN documents must be submitted to ePolicy for document control purposes. • Document templates (available in Word) shall be used to ensure consistency in branding and ‘look and feel’ of the document. • Documents are to be used ‘on-line’, wherever possible (hardcopies are discouraged). • Only one authorised version shall be available electronically at any one time on the SCHN intranet or the SCHN internet. • Policy documents must not be uploaded onto the intranet or internet outside of the document control processes of ePolicy. Document Review • All SCHN documents will be reviewed every 3 years by the document owners unless otherwise stated in the Processing other Documents section of this policy. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 9 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework • SCHN documents may be reviewed prior to the above mentioned review period if legislation, clinical evidence and/or best practice (or any other reason to prompt a review) is changed. • The review procedures should be followed as outlined in Section 3.2 below. Major amendments • Major amendments will follow the procedures set out in Section 3.2 and will be tabled and reviewed for approval at the SCHN PP&G Committee. Minor amendments and no amendments • • Minor amendments made to a document may occur outside the document approval process however the amended document must be: o Approved by the document owner and o submitted to ePolicy for document control purposes Documents with minor amendments or no amendments are tabled at the SCHN PP&G Committee for noting. Records Management • The latest approved Word version will be stored in ePolicy; a centrally controlled database, electronically accessible to staff developing/reviewing a document. • All documents stored in ePolicy shall have SCHN approved identifiers attached. All identifiers are built into the SCHN templates. • The approved Word version is converted to PDF version and it is this version that is published onto a central ‘SCHN Policy’ intranet site accessible to all SCHN staff (CHW, SCH, NETS, PSN and CCC). • Policy documents published on the SCHN Policy intranet site shall be considered the authoritative source. Individual facility specific intranet sites shall link to this source. • Only the current PDF version is accessible to staff. o Previous Word version in ePolicy is not accessible to staff other than the owner and identified staff in the Clinical Governance Unit. ePolicy manages version control. o Previous PDF versions are archived to the ‘Expired Policies’ intranet site and is not accessible to staff other than identified staff in the Clinical Governance Unit. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 10 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 3 Procedures 3.1 Developing a Document Education is available – Contact the Clinical Governance Unit for details. 1. Needs Analysis • • A need may be identified by way of: Responsibility: Team Leader or other identified person o New evidence o Legislative changes or requirements. o Recommendations from Root Cause Analysis (RCA). o Incident Information Monitoring System (IIMS) data. o Actions from complaints management, accreditation or audit. o Risk Management outcomes. o Documenting commonly used ‘best practice’ processes used at SCHN If a need is identified: o Check if there is an existing SCHN document (Network, Facility specific or departmental or trans-departmental) already covering the issue. 2. Obtain approval to proceed Approval is required before development begins. Approval should be confirmed from the following: i. Responsibility: Team Leader Line Manager, Clinical Director and/or Director as appropriate. ii. ePolicy: Approval to proceed may be attained from ePolicy when the proposed document is registered in ePolicy (see point 3 directly below). 3. Submit a request in ePolicy to DEVELOP a document o Responsibility: Team Leader Register the document development in ePolicy. NOTE: SCH managers will have access to ePolicy in the first instance. (Refer to ePolicy Quick start for instructions on how to use ePolicy) o The Policy team in the Clinical Governance Unit ensure another team are not developing a similar document before approving the request. 4. Form a Document Development Team (DDT) o Responsibility: Team Leader A Document Development Team is a group of representative stakeholders. Team Leader should be identified if not already done so. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 11 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework o Network (SCHN) documents: multidisciplinary team from 2 or more SCHN facilities as appropriate. Facility specific documents: interdepartmental multidisciplinary team. Departmental or Trans-departmental documents: key departmental staff should be on the team. The DDT are responsible to: Determine if a policy, procedure or practice guideline is required. Determine if the document should be Network, facility, departmental or transdepartmental. Define the scope of the document and prioritise what needs to be in the document. Where appropriate, appraise/grade the evidence and make recommendations for practice. This is particularly important for clinical documents. Draft the document ensuring the purpose and any measures are clearly identifiable. The document should be concise and easy to read so the target group may understand it. Identify key performance indicators relating to the document. Consult with all stakeholders – multidisciplinary input is required. Implement and disseminate the document. Evaluate and review the document. 5. Perform a Literature Search Responsibility: Team Leader – delegation to other team members o Where appropriate, a literature search must be performed to ensure the information in the document is supported by latest evidence or best practice. o NHMRC Levels of Evidence Resource: http://www.nhmrc.gov.au/_files_nhmrc/file/guidelines/evidence_statement_form.pdf o Record key search words in ePolicy to assist literature searches at the next review. Referencing – Vancouver Style o The Vancouver referencing system should be used. o EndNote may be used to manage references. (Note: to import references into the document, ensure the template is NOT protected.) Contact Librarians for assistance with EndNote. EndNote and literature search education sessions are available. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 12 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 6. Drafting the Document Resource: How to write a policy document: Responsibility: Document Development Team http://chw.schn.health.nsw.gov.au/o/groups/ppc/resources/guidelines_-_how_to_write_a_policy_.pdf o Use the approved templates found in Word>File>New>My Templates>select required template. There are instructions provided within the template. Save the working document. o Structure it so that is easy to read and follows a logical sequence of events. o Provide headings and subheadings that assist the reader in finding information quickly and easily. Examples are provided in the above linked document. o Consider the audience who will be using the document. Set the language so they can understand it (i.e. use Plain English) and avoid using jargon. Use ‘active’ not ‘passive’ language (i.e. use phrases like “give panadol” rather than “panadol should be given”). o All SCHN documents, particularly Practice Guidelines, should be outcome focused. Wherever possible, KPIs should be identified to help measure the impact/success of the document. KPI statements are recorded in ePolicy. At the next review, KPI data is collected, analysed and documented in ePolicy. Refer to “Document Evaluation and Monitoring Compliance” Section for processes. o All SCHN documents must have a risk rating applied (MoH coversheets, departmental & trans-departmental documents are exempt). o Complete the following sections: Document Summary/Key Points: to provide the essential information at a glance. Change Summary: to highlight any changes from the previous version so staff don’t have to waste time looking for the changes. If the document is new, add ‘N/A – new document’ Read Acknowledgement: to assist managers identify relevant staff who may require training, who need to be very familiar with the document (these staff should read and acknowledge they understand the contents [e.g. sign off]), or staff who may only need to know about the document (i.e. read only). This provides evidence of understanding and is associated with the risk rating of the document. Generally for extreme and high risk documents, staff should read and sign a Policy Notification Record whilst for medium and low risk documents records of notification need only be minutes of meetings, emails, and memos. o Additional considerations: Family Considerations Any document developed needs to ensure that consumers are appropriately consulted and involved in the document development as appropriate. If families will be using the document it must be written in simple Plain English. Where appropriate, consumers/families should be given an opportunity to review the document as they are stakeholders too. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 13 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework Aboriginal Health All SCHN policies should consider the impact on the health of Aboriginal and Torres Strait Islander (ATSI) peoples. If a document is going to impact on the health (which includes the social, emotional and cultural well-being) of ATSI peoples, a statement identifying the issue/s should be included. NSW HealthPD2007_082 Culturally and Linguistically Diverse (CALD) Considerations Sensitivity to the cultural needs of families should be considered. Interpreters may be required or particular information may need to be translated for families. Sometimes presenting the information in picture form is appropriate. The Government Information (Public Access) [GIPA] Act NSW, 2009 states that Government agencies (such as SCHN) must have their policy documents freely available to the public (via the internet). There are only a few exceptions permitted under the constraints of the GIPA Act. All SCHN policy documents must reflect best practice and must be evidence based. Education is available: Contact the Clinical Governance Unit for ad-hoc education and advice. 7. Establish a Risk Rating for the document o Responsibility: Document Development Team Risk ratings may assist the team to develop outcomes and is also used in the document evaluation process. Refer to “Applying levels of risk to SCHN documents” Section. 8. Consultation Responsibility: Team Leader / Document Development Team o When a document is published it should never be a surprise to a stakeholder. o Consultation with stakeholders is essential. o Governing Committee/s should be included into this process. o Record responses from each representative and outcomes and/or actions for each response. 9. Submit draft document into ePolicy Responsibility: Team Leader o After stakeholder approval, the document is submitted into ePolicy. o Complete all of the ePolicy questions before submitting. o The document will be tabled at the SCHN PP&G Committee for approval. o All new SCHN & Facility specific documents approved at the SCHN PP&G Committee are then tabled at SCHN HCQC for noting. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 14 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 3.2 Reviewing a document 1. Mandatory Review Period Responsibility: CGU Policy team o All SCHN documents have a mandatory review period of three years. o Exception: Other documents outlined under ‘Processing of Other Documents’. o Document owners will be notified via email when a document is due for review (6 months before expiry). o Documents may be reviewed any time prior to mandatory review period expiry if required. 2. Submit a request in ePolicy to REVIEW a document Responsibility: Team Leader o Document custodian may download the draft document from under the “My Policies” tab in ePolicy. Use this version throughout the review. o Then register the document review in ePolicy. (Refer to ePolicy Quick start for instructions on how to use ePolicy) o The Policy Team in the Clinical Governance Unit ensure another team are not reviewing the document before approving the request. 3. Form a Document Review Team (DRT) o Team Leader should be identified if not already done so. o Representative stakeholder group: Responsibility: Team Leader Network Documents: inter-facility and interdepartmental multidisciplinary team. Facility Specific documents: interdepartmental multidisciplinary team, Departmental or Trans-departmental Documents: key departmental staff. 4. Review the document Responsibility: Team Leader / Document Review Team o Critically review the document to ensure it is still relevant. If deemed no longer relevant initiate withdrawal of the document, by contacting (in writing) the Network Manager Policy and Procedures. o Perform a literature search to ensure latest evidence/best practice is captured. o Make amendments to the ‘authorised’ Word version (including updating references) with ‘track changes’ turned on. If no amendments are required, the document must still travel through ePolicy in order to reset the review period. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 15 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework o Collect KPI data and other qualitative and quantitative data to evaluate the document. Refer to Document Evaluation and Monitoring Compliance section. o Refer to Approval Process if: Only minor amendments are required or Urgent review is required and the document needs to be ‘fast-tracked’. 5. Consultation Responsibility: Team Leader / Document Review Team o When reviewing a document consultation with stakeholders is essential. o Governing Committee/s should be included into this process. o Record responses from each representative and outcomes and/or actions for each response. 6. Submit REVIEWED document into ePolicy Responsibility: Team Leader o After stakeholder approval, the document is submitted into ePolicy. o Complete all ePolicy questions before submitting. 7. Overdue Documents for review Responsibility: CGU Policy Team o Document owner/team leader will be contacted prior to the expiry date (approx. 6 months prior) and guided through the required process. o An escalation process will be activated if documents remain overdue for review 6 months post expiry date. (refer to Appendix 1) The SCHN PP&G Committee shall action the process and will consult the appropriate senior managers. o Directors shall be notified of documents that are >12 months overdue for review and a report is entered into ERMS (risk register) for action. o Documents that remain overdue for review for an extended period of time (>12 months) without a clear rationale may risk ownership or being withdrawn from the intranet/internet. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 16 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 3.3 Approval Process 1. Stakeholder approval Responsibility: Team Leader o All representatives in the DDT or DRT should approve the final draft. o If for some reason a stakeholder is not represented, the document must be forwarded to the identified stakeholder for approval. o If a stakeholder does not approve, a consultation process should occur to facilitate approval. Record the discussion outcomes. o Outstanding issues may need to be escalated through line managers to resolve. 2. Governing Committee approval (if necessary) Responsibility: Team Leader o A governing committee may be a ‘reporting to’ Committee or a Committee such as the Drug Committee. o Governing committee should approve the document before for being tabled at the SCHN Policy and Procedure Committee. o The Policy Team in the Clinical Governance Unit can help facilitate this process. Contact the Clinical Governance Unit. 3. SCHN Policy, Procedure and Guideline Committee approval o All documents must be submitted into ePolicy for approval by the SCHN PP&G Committee. o Complete all information in ePolicy before submitting. 4. Minor Amendment approval Responsibility: Team Leader Responsibility: Team Leader o Document custodian/Team Leader must approve minor amendments. o Minor amendments must meet the criteria as defined in the “Definitions” section of this policy otherwise a full review will be required. o Submit a request into ePolicy and state in the ‘Additional Comments’ section of ePolicy ‘minor amendments required’. o In the ‘Change Summary’ section of the document, state the minor amendments. o Submit the amended document into ePolicy and complete all questions in ePolicy. o The document will be tabled at the SCHN PP&G Committee for noting. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 17 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 5. Urgent Approval (performed in exceptional circumstances only) o A document may need to be ‘fast-tracked’ through the approval process for patient safety, legal or other purposes. o The approval process may be fast-tracked at the discretion of the Director of Clinical Governance and Medical Administration (DCGMA) or delegate. o In these exceptional circumstances. o 4 Responsibility: Team Leader in consultation with NMPP/DCGMA Contact (in writing) the Network Manager Policy & Procedures (NMPP) identifying reasons for urgent approval. The NMPP will coordinate the approval process. The DCGMA (or delegate) may provide ‘approval’ for the document to be published on behalf of the SCHN PP&G Committee out of session. The document must be submitted into ePolicy with all questions being completed. Ad-hoc Feedback from staff Every document has an ‘ad-hoc’ feedback form electronically attached to it. Staff may access the form at any time via the ‘arrowed’ symbol on the SCHN Policy intranet page. Information may be forwarded anonymously or staff may choose to participate in discussions with the document authors. Submitted comments are forwarded to the document authors for follow-up/comment and depending upon the urgency of the submitted feedback, a review may be activated immediately or the feedback will be considered at the next mandatory review. All feedback is also discussed at the SCHN Policy, Procedure & Guideline Committee. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 18 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 5 Document Implementation Responsibility: Team Leader / DDT / DRT 1. A successful document will always have an implementation plan which incorporates an appropriate evaluation of the document at review. 2. Implementation is not simply limited to notifying staff of the new document. The document risk rating and scope shall determine the level of implementation required (e.g. careful and detailed implementation is required for high risk documents that effect many areas of SCHN or a facility). 3. The implementation and evaluation of the document should be discussed at the initial stages of the document development. Discussion should include: o Equipment needs analysis (for staff and parents) and associated communication strategies. Rationale: By providing the right equipment there are greater compliance outcomes. o Identifying the risk rating of the document and the expected frequency of staff accessing the document (e.g. extreme risk, high number of hits), Rationale: The higher the risk, more extensive education and implementation may be required. o Compliance points Rationale: What points of compliance are not negotiable and therefore further resources and education may need to focus on these points. This will guide the risk rating of the document. o Incident management and use of IIMS Rationale: IIMS is a resource to capture incidents. Educating staff to use IIMs to capture information relating to a document process can provide collated information on how to manage or prevent the incident re-occurring (i.e. the document can be amended to help staff avoid the incident re-occurring or processes /equipment can be improved or further education can be identified). o Identify a key performance indicator/s (Note: only use existing collection data-sets – do not create a new data-set unless essential) Rationale: A measure (KPI) can assist to identify if the associated processes or the document needs to change to match the expected KPI outcome. o Staff appraisals Rationale: If the document is extremely important for staff to perform their core business then compliance is necessary. Use the document in staff appraisals. o Staff and/or consumer feedback Rationale: End-user feedback should be captured as these persons often identify small but important issues that require action. 4. Implementation Action Plan tool: http://chw.schn.health.nsw.gov.au/o/groups/ppc/resources/action_plan_template_for_document_implementation.pdf Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 19 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 6 Notification and Communication The following 3 processes should occur: 1. Team leaders are notified of the approved document via ePolicy. o A list of approved documents is subsequently advertised in the following locations for notification to all staff: Electronic staff newsletter: “Chief Executive Update” ‘New Policies’ intranet page Monthly email to managers listing the recent NSW MoH policy documents. This email also provides a link to the ‘New Policies’ page. 2. Managers should notify their staff by reviewing the list of new and reviewed documents that are important to their area of work. o Responsibility: CGU Policy team Responsibility: Manager Notification records should be maintained. Refer to: Information about notification records: http://chw.schn.health.nsw.gov.au/o/groups/ppc/resources/staff_notification_records__information_sheet.pdf A staff notification ‘sign-off’ sheet: http://chw.schn.health.nsw.gov.au/o/groups/ppc/resources/policy_notification__staff_record_.pdf 3. The DDT/DRT should activate their implementation strategies which includes communication processes. 7 Responsibility: DDT / DRT Applying Risk ratings to SCHN documents • All SCHN and Facility specific documents should be risk rated. (Exempt: MoH coversheets & Department documents) • The level of risk is determined by the relationship between the consequences or outcome through non-compliance and the likelihood or probability of the outcome occurring (NSW MoH PD2009_039 Risk Management Policy Directive). • When evaluating a document for risk, consideration should be given to the impact a ‘non-compliance’ outcome or consequence has on patients, visitors, staff or the organisation. • Once a level of risk has been assigned, the document can be evaluated and monitored for compliance via ePolicy. Responsibility: Document Development Team Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 20 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 7.1 How assign a risk rating to a document STEP 1 – Determine the most severe consequence or outcome that may occur if there is non-compliance to the document. Refer to the MoH Risk Matrix and consequence examples table at: http://internal.health.nsw.gov.au/cgrm/rmra/risk_management/1_risk_matrix.pdf STEP 2 – Determine the likelihood of the consequence or outcome occurring. Likelihood is the chance of something happening and is measured in terms of probability or frequency. Probability (%) Frequency Likelihood > 95 – 100 Several times a week Almost certain > 70 – 95 Monthly or several times a year Likely Once every 1 – 2 years Possible > 5 – 30 Once every 2 – 5 years Unlikely <5 Greater than once every 5 years Rare > 30 – 70 OR or STEP 3 – Determine the risk rating Combine the selection of consequences and likelihood to determine the risk rating. The position on the MoH risk matrix is represented alphabetically from A – Y. Use the MoH Risk Matrix or the below table to determine the risk rating. STEP 4 – Interpret the results to determine the level of risk for the document and record it in ePolicy. • Extreme risk = red = [A – E] • High risk = orange = [F – K] • Medium risk = yellow = [L – T] • Low risk = green = [U – Y] Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 21 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 8 Document Evaluation and Monitoring Compliance Monitoring compliance is performed according to the level of risk Responsibility: Document applied to a SCHN or Facility specific document and is performed Review Team at each review. Therefore the following should be performed in order to evaluate if the document is performing the function or purpose it is supposed to be doing. All of the data collected is recorded in ePolicy. 1. Collect qualitative and quantitative data about the document. Collect the following: o How frequently the document is used (i.e. number of hits)? o Are there any reported non-compliance issues? o Are there any IIMS incidents related to the document? o Has there been any audits performed relating to the document? o Has there been any staff or consumer feedback relating to the document? o After collecting the KPI data, do the results match the expected outcome? o Is the document discussed at staff appraisals? o Does the DRT consider the document to be best practice and/or evidence based? 2. The DRT should reflect upon the data gathered and draw one or more of the following conclusions: i. Apart from updating information, there are no process changes required within the document or related work practice processes. That is, the document is performing its purpose and staff are complying. ii. Processes within the document needed to be changed to match the expected outcomes (e.g. KPI). That is, the expected outcomes are not occurring. The processes captured in the document need to change to try and align with the expected outcome. iii. Related work practices needed to change to match the document. That is, the document is performing its purpose but staff are not complying with the documented practices. iv. The document implementation strategy needs to be revised. That is, the document is performing its purpose, but staff cannot fully comply because they don’t know about the document and/or they need additional education or training. 3. The DRT should comment in ePolicy about the conclusions drawn. 4. The SCHN PP&G Committee will review and confirm the data collected along with the conclusions and may advise the DRT if further action is required. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 22 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 8.1 Additional compliance monitoring processes Regular Auditing Program – SCHN documents Responsibility: Clinical Governance Unit • Regular auditing of documents shall follow the requirements of the National Safety and Quality Health Service Standards. • The audits will be incorporated into projects/improvement activities wherever possible and use standardised audit tools. Departmental Notification records – Auditing Program • Auditing of departmental notification records shall occur periodically (e.g. six monthly). • Departments shall be selected at random and contacted prior to performing the audit. 9 Availability of documents in the event of a Disaster 9.1 Hard copies • A single set of hardcopy Network and facility specific documents are located in the After Hours Nurse Managers (AHNM) office. • These are to be used in emergency situations only. If accessed, it is the responsibility of the person accessing it to ensure the copy is returned as soon as practicable. • Managers are to maintain within their area a current hardcopy of: o Emergency Response Plan [CHW or SCH] HealthPlan and o Local Disaster Response Plan for their area. Hard copies of all other documents are discouraged. 9.2 Electronic (soft) copies) • A program has been developed to regularly update identified soft copies on the C:drives of SCHN computers. It is awaiting roll-out. • The most frequently accessed SCHN and facility specific documents will be available on the C:drive (i.e. not all policies will be found here). These documents should only be accessed if the SCHN/CHW and/or SCH intranet is non-operational. • Departmental documents from acute care areas may also be available via the C:drive in the same folder. • Managers outside acute areas are responsible to have a system in place for staff to access their local departmental documents. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 23 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 10 Processing NSW Ministry of Health Policy Documents • SCHN receives notification of state and national legislation via NSW Health Policy Directives. • SCHN person/s responsible to implement a MoH policy documents at SCHN is notified. Notifications are sent out weekly and notification records are maintained. • In addition, all SCHN managers are notified of all recent NSW MoH policy documents via a monthly “Recent NSW MoH policy document” email. • All NSW Health Policy Directives should be reflected in SCHN documents. The following should occur: Responsibility: NMPP o If SCHN does not have a corresponding document, a policy statement (coversheet) should be developed. o If SCHN does (or plans to) have a corresponding document, that document must be reviewed against the Policy Directive as soon as possible. o Both types of documents are to be submitted to ePolicy and undergo the appropriate approval processes. • Review period for MoH Policy Directive coversheets: 5 years. • MoH Policy Directive coversheets are exempt from the SCHN risk rating and document evaluation processes. • NSW MoH Guidelines and Information Bulletins may have associated SCHN documents. The development or review of such documents is at the discretion of the respective SCHN contact person. 11 Accountability Framework • Clinical Governance Unit is responsible to ensure there is a SCHN policy document framework and that it undergoes periodic review as required for all SCHN policies. • The SCHN DCGMA maintains governance over the SCHN Document Development and Review Framework policy and is responsible for the processes implemented at SCHN relating to policy document development and review. 11.1 Retention and Disposal of SCHN documents • All documents are currently kept indefinitely via ePolicy. • ePolicy is ‘backed-up daily. 11.2 Document Numbering System • Each SCHN document is issued a unique document number. • Refer to: http://chw.schn.health.nsw.gov.au/o/apps/ppc/epolicy/help/numbering_system.pdf Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 24 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 11.3 When a document becomes active? • All documents have 3 dates on the front page: o Date of Publishing o Date of Printing o Date Effective • A document becomes active or comes into effect at the ‘Date Effective’. • The review period starts from the date effective. 12 Processing of Other Documents 12.1 Standing Orders, Nurse Initiated Medication & Drug Protocols Approved by the Drug Committee 1. Obtain approval from appropriate senior nursing staff and/or senior medical staff to develop the document. 2. Complete the appropriate template. (Word>File>New>My Templates) 3. Register the document in ePolicy. 4. Obtain final draft sign-off by appropriate senior medical and/or nursing staff from relevant teams. 5. Submit the final version in ePolicy. 6. The NMPP submits the document to the Drug Committee for approval. 7. The document is published when Drug Committee approval is received. Review Period of Standing Orders, Nurse Initiated Medication and Drug Protocols o Standing Orders MUST be reviewed annually (NSW MoH PD2013_077). o Drug protocols and Nurse Initiated Medications are reviewed every 3 years. 12.2 Local Disaster Response Plans (at CHW) Approved by the CHW Emergency Plan Committee 1. Department Manager submits the Local Disaster Response Plan to the Emergency Response Committee for approval. 2. The approved CHW Local Disaster Plan is submitted to ePolicy and the document is published. Review Period for Local Disaster Plans o Local Disaster Plans are reviewed every 2 years. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 25 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework 12.3 Local Emergency Plans (at SCH) Approved by the Randwick Campus Emergency Plan Committee (Shared Service) 1. SCH Emergency Planning Committee submits the local (SCH) emergency management plan to the Randwick Campus Emergency Plan Committee for approval. 2. The approved Randwick Campus Emergency Management plan is submitted to SESLHD processes in addition to being submitted to ePolicy as a SCH facility specific document. The document is then published. 13 Bibliography 1. Australian Commission on Safety and Quality in Health Care “National Safety and Quality Health Service Standards”, September 2011 publication: http://www.safetyandquality.gov.au/wpcontent/uploads/2011/01/NSQHS-Standards-Sept2011.pdf (accessed Mar 2014) 2. Australian Health Practitioner Regulation Agency (AHPRA) website: http://www.ahpra.gov.au/ (accessed Mar 2014) 3. National Health & Medical Research Council (NHMRC) “A guide to the development, implementation and evaluation of clinical practice guidelines”. http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/cp30.pdf (Accessed Mar 2014) 4. “Government Information (Public Access) Act, 2009 (NSW): http://www.austlii.edu.au/au/legis/nsw/consol_act/giaa2009368/ (Accessed Mar 2014) 5. NSW MoH Policy Directive (PD2009_029) “Policy Distribution System (PDS) for NSW Health”: http://www0.health.nsw.gov.au/policies/pd/2009/pdf/PD2009_029.pdf (accessed Mar 2014) 6. NSW MoH Policy Directive (PD2013_042) “Medication Handling in NSW Public Health Facilities”: http://www0.health.nsw.gov.au/policies/pd/2013/pdf/PD2013_043.pdf (accessed Mar 2014) 7. NSW MoH Policy Directive (PD2007_082) “Aboriginal Health Impact Statement and Guidelines”: http://www0.health.nsw.gov.au/policies/pd/2007/pdf/PD2007_082.pdf (accessed Mar 2014) 8. NSW MoH Policy Directive (PD2009_039) “Risk Management – Enterprise-wide Policy and Framework”. http://www0.health.nsw.gov.au/policies/pd/2009/pdf/PD2009_039.pdf (accessed Mar 2014) 9. Appraisal of Guidelines, Research and Evaluation (AGREE) Collaboration: http://www.agreetrust.org/ (accessed Mar 2014) 10. Grimshaw J.M, Thomas R.E, MacLennan G et al. Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technology Assessment 2004. http://www.hta.ac.uk/execsumm/summ806.htm (accessed Mar 2014) 11. Fretheim A, Schunemann H. J, Oxman A. D. Improving the use of research evidence in guideline development: 15. Disseminating and implementing guidelines. Health Research Policy and Systems 2006, 4:27 12. Moulding N. T, Silagy C. A, and Weller D. P. A framework for effective management of change in clinical practice: dissemination and implementation of clinical practice guidelines. Qual. Health Care 1999; 8; 177 – 183. Copyright notice and disclaimer: The use of this document outside Sydney Children's Hospitals Network (SCHN), or its reproduction in whole or in part, is subject to acknowledgement that it is the property of SCHN. SCHN has done everything practicable to make this document accurate, up-to-date and in accordance with accepted legislation and standards at the date of publication. SCHN is not responsible for consequences arising from the use of this document outside SCHN. A current version of this document is only available electronically from the Hospitals. If printed, this document is only valid on the date of printing. Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 26 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory. Policy No: 1/A/12:9037-01:02 Policy: Document Development and Review Framework Appendix 1: Escalation process for policies overdue for review Date of Publishing: 11 July 2014 4:51 PM Date of Printing: 11 July 2014 K:\CHW P&P\ePolicy\Jun 14\Document Development & Review Framework.docx Page 27 of 27 This Policy/Procedure may be varied, withdrawn or replaced at any time. Compliance with this Policy/Procedure is mandatory.