Fiber Tract–based Atlas of Human White Matter Anatomy
advertisement

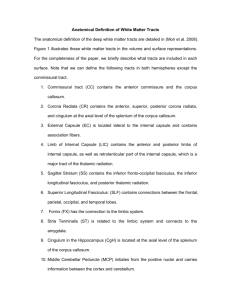
Radiology Special Report Setsu Wakana, MD Hangyi Jiang, PhD Lidia M. Nagae-Poetscher, MD Peter C. M. van Zijl, PhD Susumu Mori, PhD Index terms: Brain, anatomy, 10.92 Brain, MR, 10.121412, 10.121416, 10.121417 Brain, white matter, 10.92 Diffusion tensor, 10.121416 Special Reports Published online before print 10.1148/radiol.2301021640 Radiology 2004; 230:77– 87 Fiber Tract– based Atlas of Human White Matter Anatomy1 Two- and three-dimensional (3D) white matter atlases were created on the basis of high-spatial-resolution diffusion tensor magnetic resonance (MR) imaging and 3D tract reconstruction. The 3D trajectories of 17 prominent white matter tracts could be reconstructed and depicted. Tracts were superimposed on coregistered anatomic MR images to parcel the white matter. These parcellation maps were then compared with coregistered diffusion tensor imaging color maps to assign visible structures. The results showed (a) which anatomic structures can be identified on diffusion tensor images and (b) where these anatomic units are located at each section level and orientation. The atlas may prove useful for educational and clinical purposes. © Abbreviations: DT ⫽ diffusion tensor MPRAGE ⫽ magnetization-prepared rapid gradient echo ROI ⫽ region of interest 3D ⫽ three-dimensional 2D ⫽ two-dimensional 1 From the Department of Radiology and Radiological Science, Johns Hopkins University School of Medicine, 217 Traylor Bldg, 720 Rutland Ave, Baltimore, MD 21205; and F. M. Kirby Research Center for Functional Brain Imaging, Kennedy Krieger Institute, Baltimore, Md. From the 2002 RSNA scientific assembly. Supported by National Institutes of Health grants RO1 AG20012– 01 and P41 RR15241– 01. Received December 12, 2002; revision requested February 25, 2003; revision received May 8; accepted August 21. Address correspondence to S.M. (e-mail: susumu@mri.jhu.edu). Author contributions: Guarantor of integrity of entire study, S.M.; study concepts and design, S.M.; literature research, S.M., S.W.; clinical studies, S.W., S.M.; experimental studies, S.W., L.M.N.P.; data acquisition, S.W., H.J.; data analysis/ interpretation, S.W., H.J., L.M.N.P.; manuscript preparation, S.M., S.W.; manuscript definition of intellectual content, S.M., P.C.M.v.Z.; manuscript editing, S.M., S.W.; manuscript revision/review, S.M., S.W., P.C.M.v.Z.; manuscript final version approval, all authors © RSNA, 2003 RSNA, 2003 Diffusion tensor (DT) imaging is a magnetic resonance (MR) imaging technique that can be used to characterize the orientational properties of the diffusion process of water molecules (1,2). Usually, the information is contracted to two types of parameters: diffusion anisotropy, which represents the amount of directionality, and orientation of the axis along which water molecules move preferentially. Application of this technique to the brain has been demonstrated to provide exceptional information on white matter architecture (3–7). Because at present there are no other imaging modalities that can provide equivalent information, DT imaging is expected to become an important tool for the study of brain anatomy and the diagnosis of various white matter abnormalities. Recent developments in postprocessing algorithms for DT imaging also allow study of the threedimensional (3D) configuration of major white matter tracts, for which good agreement with postmortem anatomic studies has been reported (8 –12). Various types of DT imaging visualization schemes have been postulated. Orientationbased color coding (or, simply, color mapping) is a visualization approach in which the image brightness represents diffusion anisotropy, while a red-green-blue color scheme indicates tract orientation, assuming that the preferential diffusion axis coincides with the fiber orientation (5,13). This color map presentation has already proved to be useful for several brain diseases (5,14 –19), and, owing to the increased availability of MR units equipped with DT imaging capabilities, it is expected to become an important routine diagnostic method in the near future. This color map may pose some challenges to neuroradiologists, however, because the contrast and anatomic information it provides is complex and requires detailed knowledge of the 3D architecture of white matter. In addition, various intra–white matter structures that can be visualized on DT imaging color maps have not yet been clearly assigned. The purpose of our study was to create twodimensional (2D) and 3D white matter anatomic atlases based on high-spatial-resolution DT imaging data. IMAGING Subjects Data were acquired in four healthy volunteers (three men, one woman; age range, 21–29 years). The subjects did not have any history of neurologic abnormality. Institutional review board approval was obtained for the study, and informed consent was obtained from all subjects. 77 Radiology Data Acquisition A 1.5-T MR unit (Gyroscan NT; Philips Medical Systems, Best, the Netherlands) was used. DT imaging data were acquired by using a single-shot echo-planar imaging sequence with the sensitivity-encoding, or SENSE, parallel-imaging scheme (reduction factor, 2.5) (20,21). The imaging matrix was 112 ⫻ 112, with a field of view of 246 ⫻ 246 mm (nominal resolution, 2.2 mm) zero filled to 256 ⫻ 256 pixels. Transverse sections of 2.2-mm thickness were acquired parallel to the anterior commissure–posterior commissure line. A total of 55 sections covered the entire hemisphere and brainstem without gaps. Diffusion weighting was encoded along 30 independent orientations (22), and the b value was 700 mm2/ sec. Five additional images with minimal diffusion weighting (b ⫽ 33 mm2/sec) were also acquired. The acquisition time per dataset was approximately 6 minutes. To enhance the signal-to-noise ratio, imaging was repeated six times. Coregistered magnetization-prepared rapid gradient-echo (MPRAGE) images of the same resolution were recorded for anatomic guidance. Data Processing The DT imaging datasets were transferred to a workstation and processed by using DtiMap (H. Jiang, S. Mori; Johns Hopkins University, mri.kennedykrieger .org). All diffusion-weighted images were visually inspected by two authors (S.W., S.M.) for apparent artifacts due to subject motion and instrument malfunction. Subsequently, the six independent elements of the 3 ⫻ 3 diffusion tensor were calculated by two authors (S.W., L.M.N.P.) for each pixel by using multivariate linear fitting method. After diagonalization, three eigenvalues and three eigenvectors were obtained (1). For the anisotropy map, fractional anisotropy was used. The eigenvector associated with the largest eigenvalue was used as an indicator of fiber orientation. On the DT imaging color maps, red, green, and blue colors were assigned to right-left, anterior-posterior, and superior-inferior orientations, respectively (13). Three-dimensional Tract Reconstruction For the 3D tract reconstruction, the fiber assignment by means of continuous tracking, or FACT, method (8,23,24) was used, with a fractional anisotropy threshold of 0.15 and an inner product thresh78 䡠 Radiology 䡠 January 2004 Figure 1. Diagram shows the three operations used in this study. A, AND and NOT operations. Two ROIs (green) are placed on anatomic landmarks. When the AND operation is used, tracts that penetrate both ROIs are selected. In this example, black and red tracts are selected, while blue tracts are removed. NOT operation is used to remove specific tracts that penetrate one or multiple ROIs (orange). In this example, red tracts are removed. B, OR operation. Multiple tracking results when multiple ROIs are combined. AND operation poses a strong constraint in tracking results by selecting only tracts with known trajectories. This is a conservative approach for which results are potentially more accurate, with the disadvantage that it does not allow visualization of branching patterns between ROIs. The OR approach may be more susceptible to noise and partial volume effects. old of 0.75, which prohibited angles larger than 41° during tracking. To reconstruct tracts of interest, we used a multiple–region-of-interest (ROI) approach (9,25–27), which exploits existing anatomic knowledge of tract trajectories. Tracking was performed from all pixels inside the brain (“brute force” approach), and results that penetrated the manually defined ROIs were assigned to the specific tracts associated with the ROIs. When multiple ROIs were used for a tract of interest, we used three types of operations, AND, OR, and NOT (Fig 1), the choice of which depended on the characteristic trajectory of each tract. ROIs were placed by two authors (S.M., S.W.), who followed previously described protocols for brainstem fibers and association fibers (25,26). Fibers connecting the cortex and the brainstem (corticobulbar tract and corticospinal tract) were reconstructed by placing a first ROI at the cerebral peduncle and another at the internal capsule. Among these tracts, the corticospinal tract was identified by placing two ROIs at the pre- and postcentral gyri and the pyramidal tract in caudal portion of the pons. To reconstruct thalamocortical connections, the entire 3D volume of the thalamus was defined as the first ROI. The second ROIs for the anterior and posterior thalamic radiations were defined by using coronal sections, as described previously (26). For the superior thalamic radiation, the second ROI occupied the entire hemisphere within a transverse section above the corpus callosum. Fibers in the limbic system tend to be narrow and tubular, and a single tracking result sometimes failed to delineate the entire length. These tracts could be delineated by combining multiple two-ROI results. Specifically, the trajectories were divided into anterior, middle, and temporal regions and were reconstructed separately by using the two-ROI and AND operations. These results were subsequently combined with the OR operation to depict the entire length. Corticocortical connections through the corpus callosum were reconstructed by placing the first ROI in the corpus callosum at a midsagittal level. The second ROI was placed in the corona radiata, which was defined on two coronal sections (one anterior to the genu of and the other posterior to the splenium of the corpus callosum) and on one transverse section superior to the body of the corpus callosum. These three reconstruction results (obtained by using the two ROIs with the AND operation) were then combined by using the OR operation to depict the entire corpus callosum. Additional reconstruction for temporotemporal lobe connections (tapetum) was achieved by placing the second ROI in the temporal lobe. The NOT operation was also used to remove a subset of projections from a reconstruction result. An example is separation of the inferior longitudinal and fronto-occipital fasciculi (26). The NOT Wakana et al Radiology Figure 2. Four viewing angles of 3D depictions of brainstem fibers. A, Anterior view; B, left lateral view; C, superior view, D, oblique view from right posterior angle. Reconstructed fibers are corticospinal tract (cst, white), superior cerebellar peduncle (scp, purple), middle cerebellar peduncle (mcp, red), inferior cerebellar peduncle (icp, orange), and medial lemniscus (ml, light green). For anatomic guidance, ventricles (gray), substantia nigra (sn, blue), deep cerebellar nuclei (dcn, dark green), and thalamus (yellow) are also shown. operation was also used to remove “relayed” projections often observed in the thalamus. For example, if the anterior thalamic radiation is reconstructed by using one ROI at the thalamus and the another at the frontal lobe, a small number of projections that connect the frontal lobe and thalamus penetrate the thalamus and proceed to various brain regions such as the cortex, brainstem, and cerebellum. Some of these trajectories have been reproducibly observed and may be real connections, but they were removed because they apparently do not comply with the classical definition of the anterior thalamic radiation. One of the most important limitations of the tracking technique is that specificity may be lost for tracts that run parallel to (or are merged with) one another. In this situation, the tracking tends to retain the topology: Tracts coming from the right side to a merging point stay at the right side, and tracts from the left side stay at the left side (10). Because of this limitation and the somewhat ad hoc nature of ROI placement and the three operations for individual tracts, the 3D reconstruction results shown in this report should be treated as an approximation of tract configurations and locations that belong to the same tract Volume 230 䡠 Number 1 Figure 3. Four viewing angles of 3D depictions of projection and thalamic fibers. A, Anterior view; B, left lateral views; C, superior view; D, oblique view from right anterior angle. Reconstructed fibers are corticobulbar tracts (cbt, light blue), corticospinal tract (cst, white), anterior thalamic radiation (atr, bright purple), superior thalamic radiation (str, purple), and posterior thalamic radiation (ptr, dark blue). For anatomic guidance, fibers are depicted with putamen and globus pallidus (light green); caudate nucleus (dark green); thalamus (yellow); and the hippocampus, amygdala, and ventricles (gray). E, F, For better visualization of thalamic fibers, two additional lateral views, one without putamen and globus pallidus (E) and one without corticospinal and corticobulbar tracts (F) are also given. systems rather than precise connectivity maps. The reconstruction protocol described here was applied to the DT imaging data from the four subjects, and tracts shown in this report could be identified in all subjects. Three-dimensional Volume Definition of Various Anatomic Units By using the coregistered MPRAGE images, the ventricles, caudate nucleus, putamen (including globus pallidus), thalamus, hippocampus (including amygdala), substantia nigra, and deep cerebellar nuclei were manually defined to demonstrate the spatial relationship with various white matter tracts in three dimensions. Three-dimensional Demonstration The 3D depictions of trajectories of white matter tracts and volumes of gray matter nuclei were generated by using software (Amira; TGS, San Diego, Calif), with tube-type tract representation adopted from Zhang and Laidlaw (28) and Catani et al (27). DEMONSTRATION OF WHITE MATTER TRACTS: 3D PRESENTATION White matter tracts were classified into five functional categories: (a) tracts in the brainstem, (b) projection fibers (cortex–spinal cord, cortex-brainstem, and cortexthalamus connections), (c) association fibers (cortex-cortex connections), (d) limbic Atlas of Human White Matter Anatomy 䡠 79 Radiology Figure 5. Four viewing angles of 3D depictions of limbic system fibers. A, Anterior view; B, left lateral view; C, superior view; D, oblique view from right anterior angle. Reconstructed fibers are cingulum (cg, dark green), fornix (fx, light green), and stria terminalis (st, yellow). For anatomic guidance, hippocampus and amygdala (purple) and ventricles (gray) are also shown. Figure 4. Four viewing angles of 3D depictions of association fibers. A, Anterior view; B, left lateral view; C, superior view; D, oblique view from right anterior angle. Reconstructed fibers are superior longitudinal fasciculus (slf, yellow), inferior longitudinal fasciculus (ilf, brown), superior fronto-occipital fasciculus (sfo, beige), inferior frontooccipital fasciculus (ifo, orange), and uncinate fasciculus (unc, red). E, F, Left lateral views without superior longitudinal fasciculus (E) and inferior longitudinal fasciculus (F). system tracts, and (e) commissural fibers (right-left hemispheric connections). Tracts in the Brainstem The superior, middle, and inferior cerebellar peduncles; corticospinal tract; and medial lemniscus were reconstructed as shown in Figure 2 (25). For anatomic guidance, the ventricles, deep cerebellar nuclei, substantia nigra, and thalamus are also shown. (Note that colors assigned here are not related to tract orientation, unlike in color maps.) One end of the superior cerebellar peduncle terminates at the deep cerebellar nuclei; the other, at the thalamus. Although majority of the superior cerebellar peduncle was supposed to cross the midline at the decussation of the superior cerebellar peduncle, the reconstructed trajectory remained in the same hemisphere. This is due to the limitation of the fiber-tracking 80 䡠 Radiology 䡠 January 2004 technique, which tends to provide a “kissing” (⬎⬍) solution when two fibers have a crossing (⫻) trajectory (10). The trajectory of the inferior cerebellar peduncle approached the superior cerebellar peduncle from the inferolateral side and passed through the superior side toward the medial direction. The medial lemniscus traveled along the dorsal side of the midbrain and pons and turned sharply toward the ventral side of the brainstem at the level of the medulla. These trajectories agree well with postmortem anatomic descriptions of these tracts (29,30). Projection Fibers Trajectories of the main projection fibers are shown in Figure 3. It can be seen that the corticobulbar tract collects projections from many areas of the cortex to the brainstem. The projection from pre- and postcentral gyri (corticospinal tract) reaches the pyramidal tract at the pons. The thalamic projections and relationships with the thalamus can be seen clearly in Figure 3, E and F, where the putamen (Fig 3, E) and corticobulbar and corticospinal tracts (Fig 3, F) were removed. All thalamic radiations converged into the internal capsule, located between the putamen and the thalamus– caudate nucleus regions. Among other types of sensory connections between the thalamus and cortex, the posterior thalamic radiation includes the optic radiation. The corticobulbar and corticospinal tracts and the thalamic fibers all penetrate the internal capsule, where the cortex-brainstem connection occupies the more lateral regions. This type of preservation of topology seen in the internal capsule (ie, anterior part projecting to frontal lobe; posterior part, to occipital lobe; lateral part, to cortex; and medial part, to thalamus) may be due in part to the limitation of the tract-tracking technique, which generally does not allow tracing of crossing (⫻) configurations. Therefore, although the 3D reconstruction results can provide macroscopic views of the tracts, they cannot be directly interpreted in terms of detailed connectivity information. It is noteworWakana et al Radiology Figure 6. Four viewing angles show 3D depictions of callosal fibers. A, Anterior view; B, left lateral view; C, superior view; D, oblique view from right anterior angle. Corticocortical connections through corpus callosum (cc) are magenta. Subset of the tracts that project to temporal lobe (tapetum) are pink. thy, however, that the topologic preservation seen in the internal capsule actually agrees well with what has been postulated by neuroanatomists on the basis of postmortem results (30). Association Fibers There are numerous types of association fibers, according to reports of postmortem anatomic studies (29 –31). These include long-range, as well as shortrange, cortical U fibers. In this study, we focused on four well-documented association tracts, including the superior longitudinal fasciculus, inferior longitudinal fasciculus, inferior fronto-occipital fasciculus, and uncinate fasciculus (Fig 4). In a previous study (26), we reported that a white matter tract called the superior fronto-occipital fasciculus could not be identified with certainty by using the tract-reconstruction approach, although a tract of substantial size can be recognized at the location where this fascicle should be found. Catani et al (27) showed that this tract actually projects to the frontal and parietal lobes, and our present results confirm that finding. Figure 4 clearly shows the 3D relationship of these association fibers. The superior longitudinal fasciculus projects to most lateral regions of the temporal lobe with a characteristic C-shaped trajectory. Volume 230 䡠 Number 1 Figure 7. Three-dimensional presentation of projection (green), association (red), and callosal (blue) fibers. A, Anterior view; B, left lateral view; C, superior view; D, left anterosuperior view. To demonstrate relative locations of these three families of tracts, projection (Fig 3), association (Fig 4), and callosal (Fig 6) fibers are depicted simultaneously. E–G, Representative transverse sections. Pixels that share more than one family of tracts can be identified in terms of color: Magenta is formed by red (association) plus blue (callosal); yellow, by green (projection) plus red; and cyan, by green plus blue. Note dominant presence of projection fibers in cortical areas around the central sulcus (cs). acr ⫽ anterior region of corona radiata, ec ⫽ external capsule, ic ⫽ internal capsule, pcr ⫽ posterior region of corona radiata, scr ⫽ superior region of corona radiata. Trajectories of the inferior longitudinal and inferior fronto-occipital fasciculi can be more easily appreciated in Figure 4, E and F, in which the superior and inferior longitudinal fasciculi were removed. It can be seen the inferior longitudinal and inferior fronto-occipital fasciculi share most of the projections at the posterior temporal and occipital lobes, while the uncinate and inferior fronto-occipital fasciculi share the projections at the frontal lobe. The superior fronto-occipital fasciculus is unique in that it is the only association fiber tract that projects medially to the thalamus and along the ventricle. Limbic System Fibers It was possible to reconstruct the cingulum, fornix, and stria terminalis trajectories, which, together with the hippocampus and amygdala and the ventricles, are shown in Figure 5. The cingulum extensively collected projections from the nearby cingulate gyrus and extended into the temporal lobe. The fornix could be easily reconstructed at its body, which projected into the hypothalamus, while the differentiation of fornix from stria terminalis in the temporal lobe was not clear with the current imaging resolution (2.2 mm). The cingulum travels along the venAtlas of Human White Matter Anatomy 䡠 81 Radiology Figure 8. Transverse DT imaging color maps (first and third columns) and white matter parcellation maps (second and fourth columns). On parcellation maps, locations of intercepts of various tract trajectories are shown in the same colors used in Figures 2– 6. On color maps, red, green, and blue represent fibers running along right-left, anterior-posterior, and superior-inferior axes, respectively. Locations of white matter tracts are assigned on color maps. Several anatomic landmarks visible on color maps are also annotated on the basis of existing anatomic knowledge. Note that corona radiata consists of a mixture of various tracts (Fig 8 continues). tral surface of the hippocampus, while the fornix and stria terminalis project along the dorsal surface. Callosal Fibers Results of callosal fiber reconstruction are shown in Figure 6. The massive array of projections forms the so-called callosal radiation, which connects the corresponding areas of opposite hemisphere. The projections from the genu of the corpus callosum form the forceps minor; those from the splenium form the forceps major. There are also strong projections from the splenium that sweep inferiorly along the lateral margin of the posterior horn of the lateral ventricle and project into the temporal lobes; these projections are known collectively as the tapetum. 82 䡠 Radiology 䡠 January 2004 Topologic Relationships among Projection, Association, and Callosal Fibers Unlike the fibers in the limbic system, which all travel along the ventricles and hippocampus, the spatial relationships between projection, association, and callosal fibers may be difficult to appreciate. In Figure 7, tracts that belong to projection, association, and callosal fibers are assigned the colors green, red, and blue, respectively, and are depicted simultaneously. It can be seen that the association fibers tend to occupy most lateral regions; and the callosal fibers, the medial regions. On 2D images, brain areas where these fibers overlap can be identified by means of mixed colors such as yellow (green plus red), magenta (red plus blue), and cyan (green plus blue). Note that the same pixel can be shared by different tracts if vectors in two different pixels point to the same pixel. Figure 7, E–G, indicates that the temporal lobe and external capsule are occupied by association fibers; the internal capsule, by projection fibers; and the corona radiata, by all three families of fibers. DEMONSTRATION OF WHITE MATTER TRACTS: 2D PRESENTATION Figures 8 –10 show a series of DT imaging color maps in transverse, coronal, and sagittal planes, respectively. Coregistered MPRAGE images with color-coded white matter tracts (hereafter, white matter parWakana et al Radiology Figure 8 (continued). ac ⫽ anterior commissure, acr ⫽ anterior region of corona radiata, alic ⫽ anterior limb of internal capsule, cbt ⫽ corticobulbar tract, cg ⫽ cingulum, cp ⫽ cerebral peduncle, cst ⫽ corticospinal tract, dscp ⫽ decussation of superior cerebellar peduncle (scp), fx ⫽ fornix, icp ⫽ inferior cerebellar peduncle, ifo ⫽ inferior fronto-occipital fasciculus, ilf ⫽ inferior longitudinal fasciculus, mcp ⫽ middle cerebellar peduncle, ml ⫽ medial lemniscus, ot ⫽ optic tract, pcr ⫽ posterior region of corona radiata, plic ⫽ posterior limb of internal capsule, py ⫽ pyramidal tract, scr ⫽ superior region of internal capsule, sfo ⫽ superior fronto-occipital fasciculus, slf ⫽ superior longitudinal fasciculus, sn ⫽ substantia nigra, st ⫽ stria terminalis, unc ⫽ uncinate fasciculus, ⴱ ⫽ short-range association fibers, ⴱⴱ ⫽ vertical occipital fasciculus. cellation maps) are also shown for anatomic guidance. On the parcellation map, the tract trajectories (identified by using the 3D reconstruction) are superimposed on the MPRAGE images, with the same colors used in Figures 2– 6. By comparing the two types of images, various structures visible on the DT imaging color maps can be assigned. Brainstem Identification of the corticospinal tract and medial lemniscus on the color maps was straightforward at the pons levels (Fig 8, C–F). At the caudal pons-medulla level, the medial lemniscus became narrower and almost invisible at the decussation (lower level than that in Fig 8, Volume 230 䡠 Number 1 A and B). The relative locations of the superior and inferior cerebellar peduncles were difficult to distinguish at certain levels of the pons (eg, Fig 8, E and F), but side-by-side comparison with the 3Dbased parcellation information helped identification at those section levels. At the midbrain level, a structure with rightleft orientation could be always found at the midline (red tracts on Fig 8, I and J). On the basis of information regarding the trajectory of the superior cerebellar peduncle, which leads to this midline structure, we determined that the structure is the decussation of the superior cerebellar peduncle. In addition to the white matter tracts, the substantia nigra (Fig 8, I and J) and deep cerebellar nuclei (Fig 8, C and D) could be identified. The superior cerebellar peduncle terminated at the deep cerebellar nuclei, which agrees with the fact that neurons in the latter are the major sources of axons of the former. Projection and Callosal Fibers These fibers project along the superiorinferior axis for most of their courses, and transverse sections are the best 2D depictions for investigation of their assignment (Fig 8). At the midbrain level (Fig 8, I–L), the corticobulbar and corticospinal tracts could be identified in the cerebral peduncle; the corticospinal tract occupied the center portion of the cerebral peduncle, as has been previously reported (25). At the transverse level of the Atlas of Human White Matter Anatomy 䡠 83 Radiology Figure 9. Coronal DT imaging color maps (first and third columns) and parcellation maps (second and fourth columns). See caption for Figure 8 for color coding and abbreviations. internal capsule (Fig 8, M–P), the thalamic fibers (anterior, superior, and posterior thalamic radiations) joined the corticobulbar and corticospinal tracts. The anterior and posterior limbs of the internal capsule contained the anterior and superior thalamic radiations, respectively, and the retrolenticular part contained a mixture of the posterior thalamic radiation and association tracts 84 䡠 Radiology 䡠 January 2004 (see Fig 11 for nomenclature of internal capsule). The projection fibers extended to the corona radiata (anterior and posterior regions of corona radiata could be identified in Fig 8, M–R; superior region, in Fig 8, S–X), which consisted of a mixture of various association, projection, and callosal fibers, as also shown in Figure 7. Three colors were assigned to different regions of the thalamocortical connections (see also Fig 3). Distributions of these colors in the thalamus showed that the anterior thalamic radiation is associated with dorsomedial nuclei; the superior thalamic radiation, with ventrolateral nuclei; and the posterior thalamic radiation, with posterior nuclei (pulvinar) (Fig 11, A), which agrees well with postmortem histologic findings (see Fig 11, B) (30). Wakana et al Radiology Figure 10. Sagittal DT imaging color maps (first and third columns) and parcellation maps (second and fourth columns). See caption for Figure 8 for color coding and abbreviations. Figure 11. Comparison between 2D tracking-based parcellation of thalamus (A) and histologic study results (B). Anterior thalamic radiation (atr) projects from anterior and medial regions of the thalamus; superior thalamic radiation (str), from the lateral region; and posterior thalamic radiation (ptr), from the posterior region (pulvinar). (B adapted and reprinted, with permission, from reference 32.) Association Fibers These fibers travel along the anteriorposterior axis, and coronal sections (Fig 9) are most suitable for the study of their 2D locations. In the frontal lobe (Fig 9, G and H), it can be clearly seen that many association fibers (inferior fronto-occipital, uncinate, and superior longitudinal fasciculi) project through the external capsule, while the projection fibers (corticobulbar and thalamic fibers) penetrate the anterior limb of the internal capsule. In more anterior regions (eg, Fig 9, E and F, and more anterior sections), the assoVolume 230 䡠 Number 1 ciation fibers merge with the projection and thalamic fibers and further with callosal fibers in Figure 9, A and B, and more anterior sections. The inferior fronto-occipital and uncinate fasciculi have prominent projections to fronto-orbital cortical areas, which agrees with histologic findings (29). Throughout the levels in Figure 9, G–L, the inferior fronto-occipital fasciculus occupies the ventral area of the external capsule. The superior longitudinal fasciculus has a prominent projection into the frontal cortex around the sylvian fissure (Fig 9, K–P), while the tem- poral lobe is dominated by the inferior longitudinal fasciculus projection. It can be seen in Figure 9, O and P, and more posterior sections that the inferior fronto-occipital and inferior longitudinal fasciculi start to merge and that projection and thalamic fibers also join to form the retrolenticular part of the internal capsule and the posterior region of the corona radiata, which can be identified on the color maps (green in Fig 9, Q–T) at the area lateral to the ventricle. In Figure 9, S and T, the superior longitudinal fasciculus makes a sharp turn toward the temporal lobe. On the color map, this can be recognized as a change in color (from green to blue), which is located lateral to the posterior region of the corona radiata. In Figure 9, S and T, and Figure 8, O–R, it can be seen that the white matter lateral to the posterior horn of the lateral ventricle consists of three layers of tracts: The superior longitudinal fasciculus is the most lateral, with a superior-inferior orientation; the posterior region of the corona radiata (posterior thalamic radiation, corticobulbar tract, and inferior fronto-occipital and inferior longitudinal fasciculi), with an anteriorposterior orientation is in the middle; and the callosal projection to the temporal lobe (tapetum) is the most medial. Limbic Fibers Because of the complex trajectories of the cingulum, fornix, and stria terminalis, the 3D-tracking– based parcellation results substantially aided in the identification of these tracts on the color map. The core of the cingulum below Atlas of Human White Matter Anatomy 䡠 85 Radiology the cingulate gyrus could be easily identified on the color map due to the characteristic intense green color adjacent to the corpus callosum. Along its course, the cingulum collects prominent projections from the cingulate gyrus, although it is possible that the cingulum may contain some fibers from the corpus callosum. Posterior to the splenium of the corpus callosum (Figs 8, O–R; Fig 9, S and T), the cingulum turns sharply (the color becomes blue on the color map) toward the temporal lobe and travels along the ventral surface of the hippocampus (Fig 8, G–L; Fig 9, K–T) until it reaches the amygdala. The projection in the temporal lobe can also be appreciated in Figures 9, G–J, and 10, E–H. The fornix originates in the hypothalamic area, and its anterior and posterior projections in the hypothalamus can be identified on the color map (Fig 8, M and N). The body of the fornix can be easily identified in Figure 9, G–P. However, as the projection turned laterally (Fig 9, Q and R) and approached the hippocampus, the fornix–stria terminalis distinction became obscure at the current image resolution. Figure 10, G–J, shows the projection of the fornix and stria terminalis along the dorsal surface, while the cingulum travels along the ventral surface. Short-Range Association Fibers On the 2D parcellation maps shown in Figures 8–10, there were several white matter areas that were not classified in any of the tract families examined in this study. Most notable is a frontal white matter area indicated by a single asterisk (Fig 8, S and U; Fig 9, I and K; Fig 10, G) and an area in the lateral occipital lobe indicated by double asterisks (Fig 8, S; Fig 9, W; Fig 10, I). Figure 12 shows results of 3D tracking performed by placing ROIs in these areas (ROIs are shown in Fig 12). The results indicated the presence of short-range association fibers (U fibers) in these areas. The proximity of these tracts to the superior longitudinal fasciculus (see Fig 8, S and T) suggests that they could be a part of that fascicle, which is known to consist of both short- and long-range axonal fibers (31); the tract in the occipital lobe corresponded to what is called the vertical occipital fasciculus (33). DISCUSSION Other authors have reported 3D reconstructions of white matter tracts and 2D 86 䡠 Radiology 䡠 January 2004 color map assignments (5,13,25–27,34). In the present study, we extended their findings with a systematic comparison of the 3D tract reconstruction and 2D presentation by using high-spatial-resolution DT imaging datasets. Compared with conventional T1- and T2-weighted MR images, the DT-based color map provides far more information about white matter architecture. Owing to the increasing availability of DT imaging capabilities on clinical MR units, 2D DT color mapping is expected to be an important diagnostic tool in the near future. In this article, we have provided a 2D color map atlas with structural assignments, which should aid the interpretation of color maps in clinical studies. The 3D tract reconstructions served two purposes. First, they allowed us to visualize the trajectories of a tract of interest and the relationship of that tract with other tracts and gray matter nuclei. Second, once the trajectories of various tracts were reconstructed, the assignment of the color map structures became more straightforward by observing the coincidence of the trajectories in the 2D plane of interest. The 3D tract reconstruction protocols used in this study were based on those in previous publications by different groups (25–27), and the results were qualitatively identical, which confirmed the high reproducibility of the reconstruction method. The color map was created directly from the diffusion tensor vector field, and various tracts could be identified on the basis of the orientation information. Two tract systems may have the same color if their in-plane fiber orientations are the same, while the same tract system often changes color if it changes orientation. On the white matter parcellation map, the white matter was color coded differently for each tract. As a result, the same tract always has the same color and different tracts have different colors, simplifying the interpretation. However, clinical application of this approach is less straightforward, because the parcellation map requires 3D tract reconstruction, the result of which depends on ROI placement. The tracking result is also affected by image resolution and signal-tonoise ratio. For reproducible generation of the parcellation map, rather strict protocols for imaging and tract reconstruction must be defined and followed. In this study, 3D coordinate information for each tract was superimposed on MPRAGE images to create the parcellation map. Although the sensitivity-encoding acquisition drastically reduced image dis- Figure 12. Left lateral view of 3D reconstruction shows short-range association fibers. White boxes indicate approximate locations of ROIs used for reconstruction. Tracts shown in blue and magenta are white matter regions indicated by a single asterisk in Figures 8 –10; those shown in orange are regions indicated by double asterisks in Figures 8 –10. tortion related to inhomogeneity of the B0 constant magnetic induction field, a small amount of mismatch between DT and MPRAGE images remained around the sinus areas; thus, care must be taken when interpreting data in these regions. Various visible white matter structures on the DT imaging color map were assigned. Most of these white matter tract systems cannot be delineated on conventional MR images. The 2D and 3D white matter atlas presented in this article should be useful for teaching and clinical uses. The color map used in this study delineated not only detailed white matter anatomy but also gray matter structures such as the deep cerebellar nuclei and intrathalamic structures, which are difficult to identify on T1and T2-weighted MR images. The thalamus could be roughly divided into three regions. Dorsomedial regions appeared green (anterior-posterior orientation) and received projections from the frontal lobe, ventrolateral regions appeared blue (superior-inferior orientation) and received projections from superior areas of frontal and parietal lobes, and posterior regions (pulvinar) appeared red (right-left orientation) and received projections from the occipital lobes. As also pointed out by Wiegell et al (35), it may be possible to study thalamic structures by using DT imaging in the future, when even higher resolution DT imaging maps may become available with improved technical capabilities, such as higher magnetic field strength. In addition to the neuroanatomy revealed by the DT images, the atlas can provide important information for conventional MR imaging studies. For example, it has been a common practice to place an ROI in a white matter area to quantify such MR parameters as T1, T2, magnetization transfer rate, and diffuWakana et al Radiology sion anisotropy. In this process, care must be taken because some white matter areas consist of a mixture of various types of tracts or because, in some areas, a small amount of shift in ROI placement results in measurement of very different white matter tracts. The atlas can be used as a guide for the ROI placement strategy. Although the DT and 3D reconstruction techniques provide exciting new information about neuroanatomy, the limitations should also be emphasized. One of the most important limitations stems from that fact that DT imaging reflects the averaged water diffusion property within a pixel, which is an indirect indicator of the axonal structures. In fact, Wedeen et al (36) have convincingly shown that use of the diffusion tensor calculation to delineate the underlying axonal structures is often an oversimplification. In many cases, DT imaging results are biased by the dominant axonal component. For example, it has been reported (29,30) that callosal connections should extend not only to cortical areas close to the midline but also to more lateral areas. Our results failed to show these lateral projections, probably because of the massive projection fibers (corona radiata) located laterally to the callosal fibers. Similarly, branches of the projection fibers toward lateral cortical areas could not be observed, probably because of the large tract of association fibers running in the anterior-posterior orientation. Therefore, as mentioned earlier in this report, our atlases should be considered as maps of the core of the major white matter bundles, rather than as connectivity maps. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. CONCLUSION Various white matter tract systems were reconstructed by using high-spatial-resolution DT MR data sets with the goal of understanding 3D relationships between different tracts and between tracts and gray matter structures. In order to appreciate the detailed coordinates of the tracts of interest, the 3D trajectories were superimposed on MPRAGE MR images and were compared with 2D DT imaging color maps at various section levels and orientations. On the basis of the comparison, the color map structures were assigned, and a 2D color map atlas was created. The atlas may prove useful for teaching purposes and for future application of DT color mapping in clinical studies. References 1. Basser PJ, Mattiello J, Le Bihan D. MR diffusion tensor spectroscopy and imaging. Biophys J 1994; 66:259 –267. Volume 230 䡠 Number 1 15. 16. 17. 18. 19. 20. Beaulieu C. The basis of anisotropic water diffusion in the nervous system: a technical review. NMR Biomed 2002; 15:435–455. Moseley ME, Cohen Y, Kucharczyk J, et al. Diffusion-weighted MR imaging of anisotropic water diffusion in cat central nervous system. Radiology 1990; 176:439 – 445. Pierpaoli C, Jezzard P, Basser PJ, et al. Diffusion tensor MR imaging of human brain. Radiology 1996; 201:637– 648. Makris N, Worth AJ, Sorensen AG, et al. Morphometry of in vivo human white matter association pathways with diffusion weighted magnetic resonance imaging. Ann Neurol 1997; 42:951–962. Beaulieu C, Allen PS. Determinants of anisotropic water diffusion in nerves. Magn Reson Med 1994; 31:394 – 400. Henkelman R, Stanisz G, Kim J, Bronskill M. Anisotropy of NMR properties of tissues. Magn Reson Med 1994; 32:592– 601. Mori S, Crain BJ, Chacko VP, van Zijl PCM. Three dimensional tracking of axonal projections in the brain by magnetic resonance imaging. Ann Neurol 1999; 45:265–269. Conturo TE, Lori NF, Cull TS, et al. Tracking neuronal fiber pathways in the living human brain. Proc Natl Acad Sci U S A 1999; 96:10422–10427. Basser PJ, Pajevic S, Pierpaoli C, et al. In vitro fiber tractography using DT-MRI data. Magn Reson Med 2000; 44:625–632. Poupon C, Clark CA, Frouin V, et al. Regularization of diffusion-based direction maps for the tracking of brain white matter fascicules. Neuroimage 2000; 12:184 –195. Jones DK, Simmons A, Williams SC, Horsfield MA. Non-invasive assessment of axonal fiber connectivity in the human brain via diffusion tensor MRI. Magn Reson Med 1999; 42:37– 41. Pajevic S, Pierpaoli C. Color schemes to represent the orientation of anisotropic tissues from diffusion tensor data: application to white matter fiber tract mapping in the human brain. Magn Reson Med 1999; 42:526 –540. Inglis BA, Neubauer D, Yang L, et al. Diffusion tensor MR imaging and comparative histology of glioma engrafted in the rat spinal cord. AJNR Am J Neuroradiol 1999; 20:713–716. Huppi P, Maier S, Peled S, et al. Microstructural development of human newborn cerebral white matter assessed in vivo by diffusion tensor magnetic resonance imaging. Pediatr Res 1998; 44:584 –590. Pierpaoli C, Barnett A, Pajevic S, et al. Water diffusion changes in wallerian degeneration and their dependence on white matter architecture. Neuroimage 2001; 13:1174 –1185. Albayram S, Melhem ER, Mori S, et al. Holoprosencephaly in children: diffusion tensor MR imaging of white matter tracts of the brainstem—initial experience. Radiology 2002; 223:645– 651. Mori S, Fredericksen K, van Zijl PC, et al. Brain white matter anatomy of tumor patients using diffusion tensor imaging. Ann Neurol 2002; 51:377–380. Hoon AH Jr, Lawrie WT Jr, Melhem ER, et al. Diffusion tensor imaging of periventricular leukomalacia shows affected sensory cortex white matter pathways. Neurology 2002; 59:752–756. Pruessmann KP, Weiger M, Scheidegger MB, Boesiger P. SENSE: sensitivity encod- 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. ing for fast MRI. Magn Reson Med 1999; 42:952–962. Bammer R, Auer M, Keeling SL, et al. Diffusion tensor imaging using single-shot SENSEEPI. Magn Reson Med 2002; 48:128–136. Jones DK, Horsfield MA, Simmons A. Optimal strategies for measuring diffusion in anisotropic systems by magnetic resonance imaging. Magn Reson Med 1999; 42:515–525. Xue R, van Zijl PCM, Crain BJ, et al. In vivo three-dimensional reconstruction of rat brain axonal projections by diffusion tensor imaging. Magn Reson Med 1999; 42:1123–1127. Mori S, Van Zijl PC. Fiber tracking: principles and strategies—a technical review. NMR Biomed 2002; 15:468 – 480. Stieltjes B, Kaufmann WE, van Zijl PCM, et al. Diffusion tensor imaging and axonal tracking in the human brainstem. Neuroimage 2001; 14:723–735. Mori S, Kaufmann WE, Davatzikos C, et al. Imaging cortical association tracts in human brain. Magn Reson Med 2002; 47:215–223. Catani M, Howard RJ, Pajevic S, Jones DK. Virtual in vivo interactive dissection of white matter fasciculi in the human brain. Neuroimage 2002; 17:77–94. Zhang S, Laidlaw D. Elucidating neural structure in diffusion tensor MRI volumes using streamtubes and streamsurfaces (abstr). In: Proceedings of the Ninth Meeting of the International Society for Magnetic Resonance in Medicine. Berkeley, Calif: International Society for Magnetic Resonance in Medicine, 2001; 505. Carpenter M. Human neuroanatomy. Baltimore, Md: Williams & Wilkins, 1976. Nieuwenhuys R, Voogd J, van Huijzen C. The human central nervous system. Berlin, Germany: Springer-Verlag, 1983. Williams TH, Gluhbegovic N, Jew JY. The human brain: dissections of the real brain. Virtual Hospital, University of Iowa. Available at: www.vh.org/adult/provider/anatomy/ BrainAnatomy/BrainAnatomy.html. Accessed October 15, 2003. Nolte J, Angevine JB Jr. The human brain in photographs and diagrams. St Louis, Mo: Mosby, 2000. Kahle W, Leonhardt H, Platzer, W. Taschenatlas der anatomie fur studium and praxis in 3 banden. Stuttgart, Germany: Thieme, 1986. Mori S, Kaufmann WK, Pearlson GD, et al. In vivo visualization of human neural pathways by MRI. Ann Neurol 2000; 47:412–414. Wiegell MR, Larsson H, Wedeen V. Diffusion tensor MRI of the thalamus: differentiation of nuclei by their projections (abstr). In: Proceedings of the Seventh Meeting of the International Society for Magnetic Resonance in Medicine. Berkeley, Calif: International Society for Magnetic Resonance in Medicine, 1999; 934. Wedeen V, Reese TG, Tuch DS, et al. Mapping fiber orientation spectra in cerebral white matter with Fourier-transform diffusion MRI (abstr). In: Proceedings of the Eighth Meeting of the International Society for Magnetic Resonance in Medicine. Berkeley, Calif: International Society for Magnetic Resonance in Medicine, 2000; 82. Atlas of Human White Matter Anatomy 䡠 87