Clinical Anatomy and Physiology of the Chest and Lungs
advertisement

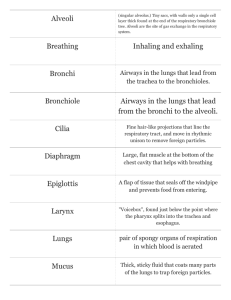
1 C H A P T E R 1 Clinical Anatomy and Physiology of the Chest and Lungs Many health workers have difficulty understanding and interpreting the clinical signs and symptoms of respiratory diseases. With a clear understanding of the basic anatomy and physiology of the chest and lungs it is much easier to understand these signs and symptoms This chapter will discuss: c The anatomy of the lower airways and the lungs c The function of the lungs exchange of oxygen and carbon dioxide c Different diseases effect different parts of the lungs c The defence and protection of the lungs The anatomy of the lower airways and the lungs The airways are divided into: c the upper respiratory tract, from the nostrils to the larynx or throat c the lower respiratory tract, from the throat to the diaphragm. The upper respiratory tract is covered in the manual on CONDITIONS OF THE EAR, NOSE AND THROAT. Below and on the next page are diagrams of the upper respiratory tract and the lower respiratory tract.. The important structures of the lower respiratory tract include: The trachea and bronchi The lower respiratory airway is wide at the trachea. The trachea divides into two main bronchi which enter the lungs. Each bronchus in turn divides several times into narrower and narrower bronchi. The trachea and bronchi have Pharynx cartilage support. Smaller bronchi and bronchioles The larger bronchi divide into smaller bronchi, which divide further into the bronchioles. The bronchioles are very narrow and have a diameter of 1mm or less. The bronchioles eventually lead into small sac-like structures called the alveoli. Larynx Oesophagus Trachea Upper respirator y tract Right Lung Left Lung Trachea Upper lobe Lymph nodes Bronchus Middle lobe Bronchioles Lower lobe Pleura Fissure Alveolus Mucous glands Trachea Mucous layer Bronchus Cross-section of airway Bronchiole Trachea and bronchus Diagram of the lower respirator y tract and lungs The airways consist of three layers including a mucous membrane and a muscle layer. Mucous glands are present in the lining of the airways. These glands are present until the very small bronchi. There are no mucous glands in the bronchioles. The alveoli Each bronchiole ends in a group of tiny sac-like structures, each one called an alveolus. Each lung has about 300 million alveoli. They are very small and cannot be seen easily with the naked eye. Each alveolus is surrounded by a capillary blood vessel. Gases, e.g. oxygen and carbon dioxide, move across the alveolar membrane into the blood vessels and vice versa. A continuous exchange of gases takes place between the alveoli and the capillary blood vessels that surround them. Bronchiole Alveolus Blood capillary Left lung Gas exchange The covering of the lungs - the pleura There is a double-layered covering of the lungs called the pleura. There is a small amount of lubricating fluid in between the two layers of the pleura. Other structures in the lungs The lungs also contain blood vessels and lymph channels. There are also many lymph nodes which are found mainly at the site where the main bronchi and large blood vessels enter the lung. This area is known as the hilum. Visceral pleura Pleural cavity Diaphragm DEFLATED INFLATED An enlarged pleural space in lung collapse (pneumothorax) Divisions of the lungs The lungs are divided into lobes. The right lung has three lobes (upper, middle, lower) and the left lung has two lobes (upper and lower). Membranes called fissures divide the lungs into lobes. It is important to know these structures because different respiratory diseases affect different parts of the airways and lungs The function of the lungs exchange of oxygen and carbon dioxide The main function of the lungs is to keep the correct amount of oxygen and carbon dioxide in the blood. In order to do this we breathe air into the airways of the lungs. The air then moves all the way down to the sac-like endings of the airways called the alveoli. In the alveoli, the oxygen from the air moves into the blood stream which surrounds each tiny alveolus. This vital oxygen is now available for the body's needs. Carbon dioxide, which is a waste product from body tissues, is carried in the blood stream to the lungs. In the lungs, the carbon dioxide is moved across the alveoli into the airways and then breathed out. Alveolus O2 Oxygen moves from alveolus into blood CO 2 Carbon dioxide moves from blood cell into alveolus Blood capillary Gas exchange The exchange of gases can be increased or decreased by breathing at a faster or slower rate, or by breathing more deeply. The body can increase the amount of oxygen and decrease the amount of carbon dioxide in the blood stream by breathing at a faster rate or more deeply. The body may have to breathe faster because: c The body needs more oxygen e.g. during exercise, running or straining. c The normal supply of oxygen is obstructed. There may be some obstruction to the flow of air in the airways or there may be an obstruction to the flow of gases across the alveoli into the blood stream. This may be due to diseases like asthma, bronchitis or pneumonia. Whatever the cause, the body will try to increase the amount of oxygen in the blood stream by breathing at a faster rate or more deeply. Most of the time the lungs are able to provide enough oxygen for the body's needs. If, for any reason, there is a severe shortage of oxygen in the blood, this will result in cyanosis. Cyanosis causes a blue colour of the lips, mouth and tongue. See Chapter 5 of the BASIC MEDICAL SCIENCES manual for more on cyanosis. There is carbon dioxide in the blood stream. Carbon dioxide is an acidic waste product of body metabolism. The level of carbon dioxide in the blood may rise because there may be an over production of carbon dioxide, e.g. from running or exercising. In some medical conditions, e.g. diabetes, there may be an over production of acid (ketones) which will also result in deeper breathing. By breathing faster or deeper the body will usually be able to correct the level of carbon dioxide. The faster we breathe, the more carbon dioxide is moved from the blood into the airways and then breathed out of the body. The normal respiratory rate is 12 - 20 breaths per minute in adults. A faster breathing rate is called tachypnoea (tachy = fast, pnoea = breathing) A fast breathing rate (tachypnoea) is an important sign of respiratory disease. A fast breathing rate can cause dehydration There is always some moisture (water) in the air that is breathed out. Therefore a fast breathing rate will result in water being lost from the body. If the breathing rate is increased for long periods of time it can result in dehydration. For this reason, it is very important to give plenty of fluids, orally or intravenously, to patients with respiratory disease or who have fast breathing rates for other reasons. This is especially important in young infants and children. Give plenty of fluids to patients with respiratory disease. In some diseases where the acid level in the blood rises, e.g. diabetes or aspirin poisoning, the body will increase its breathing rate to help get rid of the excess acid. The heart rate increases when the breathing rate increases. A faster breathing rate increases the amount of gases exchanged. The heart rate will increase the flow of blood through the lungs. When there is a normal breathing rate (12 - 20 breaths per minute), the amount of oxygen and carbon dioxide in the blood stream is at the correct level for the body's needs. Most respiratory diseases cause the breathing rate to increase. Since an increased breathing rate (tachypnoea) can cause dehydration, it is important to give fluids to patients with respiratory disease. Different diseases effect different parts of the lungs Different respiratory diseases effect different parts of the lungs and produce specific signs and symptoms. Diseases involving the lower respiratory tract include: c Infection of the bronchi is called bronchitis. In bronchitis the lining of the bronchi becomes inflamed, the mucous layer becomes thick and much excess mucus is produced. c Infection of the bronchioles is called bronchiolitis. c Infection of the alveoli is called pneumonia. Pneumonia usually affects one or more lobes (lobar pneumonia). c Tuberculosis is a chronic infection which usually affects the hilar lymph nodes and the alveoli. c Asthma is not a lung infection but an allergic condition. In asthma, the muscle layer of the smaller bronchi and bronchioles goes into spasm and causes the airways to narrow. c Lung cancers usually develop in the bronchi. c Pleurisy and asbestos dust affect the pleura. The defence and protection of the lungs The lung is exposed to many harmful agents which are present in the air that is breathed. For this reason, it has a very well developed defence system. The lungs are mainly protected by: c Mucous secretion Mucus is secreted by the bronchial mucous glands. The mucus forms a moist protective layer which lines the bronchi and bronchioles and also contains antibodies against infection. The mucus traps foreign bodies such as dust, dirt, bacteria and air pollution and so prevents them entering and establishing themselves in the airways. c Dehydration will dry out the mucus. When the mucus is dry and hard, it is more difficult for the lungs to protect themselves against infection and foreign bodies. Patients with respiratory disease must keep well-hydrated to prevent their mucus drying out and becoming hard and thick. c Fine hairs or cilia The cilia are fine hair-like structures which line the airways. This carpet-like layer moves systematically and pushes the mucus out of the airway. The mucus which is moved out the airway contains foreign bodies. In this way the cilia cleanse the lungs. Tobacco smoke and dehydration prevent the cilia from functioning properly. c The cough reflex Any irritant e.g. excessive mucus, dust, dirt or other foreign body, may stimulate the nerve endings in the airway and cause the person to cough out the irritant. c White blood cells in the alveoli - macrophages These cells lie in the alveoli and destroy dust particles and bacteria. Some important aspects of the anatomy and physiology of the lungs and lower respiratory tract have been discussed. The next chapter will focus on how to examine and interview a person with respiratory disease. Summar y: Clinical anatomy and physiology of the chest and lungs c The airways are divided into the upper and lower respiratory tract. The lower airways begin at the trachea and divide into two main bronchi which enter the lungs. In the lungs, the bronchi divide into smaller bronchi called bronchioles and finally reach the tiny air sacs called alveoli. c The airways generally have three layers, including a mucous membrane (with mucous glands) and a muscle layer. c The main function of the lungs is to maintain the correct amount of oxygen and carbon dioxide in the blood stream. c Oxygen in the alveoli of the lungs moves into the blood stream and carbon dioxide in the blood stream enters the lungs and is then breathed out. Most of the exchange of gases takes place across the alveoli. c By increasing or decreasing the breathing rate or by breathing more deeply, the body is able to increase or decrease the exchange of gases. c The normal respiratory rate is 12 - 20 breaths per minute. A faster breathing rate is called tachypnoea. Tachypnoea is an important sign of respiratory disease. c Breathing at a faster rate increases the amount of oxygen and decreases the amount of carbon dioxide in the blood stream. The breathing rate increases during exercise or as a result of respiratory diseases like asthma, bronchitis, pneumonia or severe diabetes. c If the breathing rate is increased for a long period of time, dehydration can occur. So it is important to give fluids to patients with respiratory disease or tachypnoea from other causes. c Different respiratory diseases affect different parts of the airways and lungs. c Mucous secretion, the cilia, the cough reflex and white blood cells (macrophages) all help to protect and defend the lungs against harmful agents in the air, e.g., dust, dirt, bacteria, smoke etc.