Late Breaking Abstracts
advertisement

Late Breaking Abstracts
June 2015 | Volume 64 | Suppl. 1A | www.diabetes.org/diabetes
Late Breaking Abstracts
LB1
Subject Index
LB85
Abstract Author Index
LB88
Abstract Author Disclosure Information
LB98
scientificsessions.diabetes.org
Complications—Hypoglycemia
Late Breaking Abstracts
1‑LB
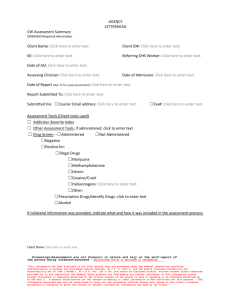
The Effect of Hypoglycemia on Progression of Atherosclerosis in
VA Diabetes Trial (VADT)
MICHAEL G. JAKOBY, SWATHI BEERAVOLU, SU AH BAE, SUMMI PARGAL, AMINA
JAFFAR, VEENA KESIREDDY, SHWETHA MALLIKARJUNA, LINDA READ, CHERYL
BURNS, Springfield, IL, Cincinnati, OH, Milwaukee, WI, San Leandro, CA
ARAMESH SAREMI, GIDEON BAHN, PETER D. REAVEN, Phoenix, AZ, Hines, IL
We examined whether hypoglycemia predicted the progression of
atherosclerosis in a substudy of the VADT. The effect of hypoglycemia (severe
episodes with loss of consciousness/requiring assistance, or documented
glucose <50 mg/dl) on progression of coronary artery calcium (CAC) was
determined in 197 participants with baseline and follow-up CT scans. During an
average follow-up time of 4.5 years between scans, a total of 97 participants
reported severe hypoglycemia (n=23) or glucose <50 (n=74). Frequency of
hypoglycemia was higher in the intensive compared to the standard treatment
group (77% vs. 24%, P <0.01). Hypoglycemia did not predict progression of
CAC in the entire group. However, there was a significant hypoglycemia by
treatment interaction (P=0.08 for hypoglycemia x treatment and P=0.01 for
severe hypoglycemia x treatment, respectively). People with hypoglycemia
in the standard group had significantly higher progression of CAC (Figure).
Age adjusted hypoglycemia predicted progression of CAC only in the
standard group (β =3.51 ± 1.71, P=0.04 and β = 6.46 ±2.71, P=0.01 for severe
hypoglycemia, respectively). Adjustment for all baseline differences including
baseline CAC, or on trial risk factors did not change the results. In conclusion,
although hypoglycemic episodes were more frequent in the intensive group,
they were associated with progression of CAC in the standard group only.
Basal/bolus insulin is the best approach for hospitalized patients with
diabetes mellitus, but little is published on strategies to synchronize delivery
of food and mealtime insulin. The SIU Hospital Diabetes Team implemented
and evaluated a program to link food delivery and prandial insulin at St.
John’s Hospital (Springfield, IL). Food Service personnel were equipped with
wireless phones and trained to contact nurses of tray drops during a three
month run in period. Primary study endpoint was proportion of insulin lispro
doses administered within 20 minutes of food delivery. Secondary endpoints
were frequency of insulin dosing errors, defined as a meal without insulin or
insulin without food, glycemic control measured by median capillary blood
glucose (CBG), and frequency of CBG below the diabetes team target of 80140 mg/dL. A prospective study with historical controls was performed, with
intervention data collected June 2014-January 2015 and June 2013-January
2014 serving as a historical control. All patients were managed by the
diabetes team. Nurses were notified at 96.1% of tray deliveries. Time
between meal and insulin was evaluated for 2,199 meals, 1,318 in the control
period and 881 after intervention. Mealtime insulin administered on time
increased from 49.7% to 57.7% for all meals (P = 0.0002), with significant
improvements at breakfast (58.8% vs. 44.0%, P < 0.0001) and lunch (60.9%
vs. 51.5%, P = 0.012). Insulin errors were reduced two-fold (2.4% to 1.2%),
a clinically meaningful result that was not quite statistically significant (P =
0.06). Median CBG was equivalent before and after the notification system
(159 mg/dL vs. 163 mg/dL, P = 0.46), but frequency of CBG < 80 mg/dL was
reduced two-fold (9.8% vs. 4.9%, P < 0.0001). A program to coordinate food
and prandial insulin improved diabetes management and patient safety in
hospital by increasing on time insulin administration, decreasing insulin
errors, and decreasing hypoglycemia rate.
Supported By: Friends of St. John’s Hospital
2‑LB
Pharmacokinetic (PK) and Pharmacodynamic (PD) Profiles of
BIOD-961 Compared with Marketed Glucagons
4‑LB
Unreported Therapeutic Effect of Liraglutide in Dumping Syndrome
LILIANA URIBE-BRUCE, LINDA MORROW, LORI CANNEY, PHILIP PICHOTTA,
MARCUS HOMPESCH, ALAN KRASNER, ERROL DE SOUZA, Chula Vista, CA,
Danbury, CT
CHRISTINE K. STIER, Frankfurt, Germany
7 patients with a new onset of a hyperinsulinemic hypoglycemia after
Roux-en-y gastric bypass were treated with Liraglutide to improve their
severe dumping symptoms. Liraglutide is an anti-diabetic GLP-1 (Glucagon
like peptide 1) mimetic, which modulates pancreatic insulin production. Its
spectrum of activity embraces neuro- and cardio protection, a decrease of
stomach emptying, glucagon secretion, hepatic glucose production, and
b-cell apoptosis and an increase of b-cell proliferation, insulin secretion and
biosynthesis, as well as glucose uptake and storage. Against doctrine, the
use of Liraglutide in these patients showed a remarkable decrease in insulin
secretion together with a better synchronization of corresponding plasma
glucose levels as measured by repeated oral glucose tolerance tests (OGTT).
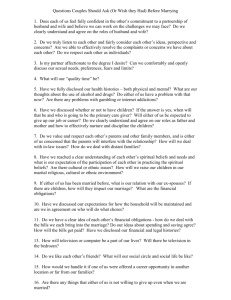
Multiple glucagon formulations for use in user-friendly devices are
currently in development for the treatment of severe hypoglycemia;
however, formulations that are not reconstituted immediately prior to use
have been associated with impaired absorption from the subcutaneous
(SC) space. BIOD-961 is a lyophilized glucagon formulation developed
for use in an auto-reconstitution device. The PK and PD profiles of BIOD961 were compared to those of two marketed glucagon formulations in
a Phase 1 randomized, six-period crossover study. On separate dosing
days, each subject received 1 mg of BIOD-961, Lilly glucagon, and Novo
glucagon delivered either SC or intramuscularly (IM). Fifteen normal,
healthy subjects were randomized into the study and 10 completed all
dosings. There were no statistically significant differences in maximal
glucose concentration (BGmax), area under the glucose concentration vs.
time curve (BGAUC0-240min), maximal glucagon concentration (Cmax) or area
under the curve for glucagon concentration vs. time curve (AUC0-240min)
(Table). Furthermore, standard criteria for PK and PD bioequivalence were
met when comparing BIOD-961 to Lilly glucagon (IM) and to Novo glucagon
(SC). The incidence of adverse events was similar among treatments. In
summary, BIOD-961 PK and PD profiles are substantially similar to both
comparator glucagons and likely to also show BE in a pivotal trial.
Table. Pharmacokinetic and Pharmacodynamic Parameters.
Parameter
SC BIOD-961 SC Lilly
SC Novo IM BIOD-961 IM Lilly
(n=12)
(n=11)
(n=12)
(n=11)
(n=11)
Cmax (µg/L)
9.01 ± 0.75 7.87 ± 0.79 9.16 ± 0.59 6.80 ± 0.52 6.75 ± 0.31
AUC0-240 min
559.5 ± 28.7 520.8 ± 29.8 570.5 ± 26.8 409.5 ± 39.2 402.6 ± 27.8
(µg*min/L)
Tmax (min)
26.7 ± 3.76 23.2 ± 1.82 20.8 ± 1.83 15.5 ± 2.07 17.7 ± 4.39
BGmax (mg/dL)
178.2 ± 7.3 170.9 ± 5.3 175.3 ± 5.9 182.9 ± 6.5 171.1 ± 6.7
BGAUC0-240 min 26118 ± 630 25915 ± 685 25240 ± 424 26184 ± 607 24960 ± 568
(mg*min/dL)
Time to BGmax
41.7 ± 4.1
43.6 ± 4.2 34.6 ± 3.2 40.5 ± 2.5
40.5 ± 3.4
(min)
IM Novo
(n=12)
7.22 ± 0.44
441.4 ± 42.7
14.6 ± 2.64
174.8 ± 5.5
25274 ± 485
44.6 ± 3.8
ADA-Funded Research
For author disclosure information, see page LB98.
LB1
POSTERS
Coordination of Inpatient Food Delivery and Mealtime Insulin
Administration Improves On-Time Insulin Dosing and Reduces Hypo­
glycemia
Acute and Chronic
Complications
3‑LB
Complications—Hypoglycemia
The SHARE system was able to identify and quantify the frequency of RH
in a real-life use environment. Cloud based health information provides the
opportunity for learning about actual diabetes management practices and
facilitate prompt actions on appropriate hypoglycemia treatment.
POSTERS
Acute and Chronic
Complications
Complications—Macrovascular—Atherosclerotic Cardiovascular Disease and Human Diabetes
Complications—Macrovascular—
Atherosclerotic Cardiovascular Disease and
Human Diabetes
6‑LB
The Cardiac Deficiency of Pyruvate Dehydrogenase Complex
Alters Cardiac Glucose Oxidation and Sensitizes Heart to Ischemic
Insults
WANQING SUN, QUAN LIU, JIYAN LENG, YANG ZHENG, JI LI, Changchun, China,
Buffalo, NY
Pyruvate Dehydrogenase Complex (PDH), plays a key role in aerobic
energy metabolism. We found that cardiac PDH deficiency mice easily
die and the PDH deficiency heart demonstrate significant hypertrophy
phenotype. We hypothesized that glucose oxidation regulated by PDH is
critical for the heart’s energy metabolism. The objectives of this study is to
characterize the signaling mechanisms by which PDH deficiency sensitizes
heart to myocardial infarction. The myocardial infarction was conducted by
ligation of left anterior descending coronary artery (LAD) in mice. The results
showed that PDH deficiency significantly increased myocardial infarct area
(p<0.01 versus WT groups), and the immunohistochemistry data showed that
cardiac PDH deficiency increased macrophage infiltration (p<0.01 vs. WT
groups). The staining of wheat germ agglutinin (WGA) and Masson trichrome
revealed greater hypertrophy and fibrosis in the PDH deficiency than WT
hearts (p<0.05). It indicated the importance of PDH’s modulation of glucose
metabolism in response to ischemic insults. Furthermore, we measured the
substrate metabolism of hearts in a working heart perfusion system. The
glucose oxidation rate was impaired in the cardiac PDH deficiency hearts
as compared to WT hearts during ischemia and reperfusion (I/R), while the
PDH activator, dichloroacetate (DCA), can augment glucose oxidation in
WT hearts during I/R. The AMP-activated protein kinase (AMPK) signaling
can lead to an increased glucose metabolism under ischemic stress in the
heart. Intriguingly. The immunoblotting data demonstrated that cardiac
PDH deficiency attenuates ischemic AMPK activation while DCA treatment
enhances the ischemic AMPK activation. Therefore, the present results
strongly suggest that PDH deficiency cause impaired ischemic AMPK
signaling response that could sensitize heart to ischemic injury induced by
ischemia and reperfusion.
5‑LB
Incidence of Hypoglycemia Overtreatment in the SHARE Real Life
Use Population
KATHERINE NAKAMURA, TOMAS WALKER, JAKE LEACH, LUCAS BOHNETT,
JORGE VALDES, ANDREW BALO, San Diego, CA
Hypoglycemia (≤ 70 mg/dL) can occur with insulin use and should
be treated with rapid acting carbohydrates. Over-treatment results in
“Rebound Hyperglycemia” (RH) (≥180 mg/dL). The frequency of RH is not
well understood. Identification of hypoglycemia and RH now can be made
in real-life using the commercial Dexcom SHARE system. CGM glucose data
stored on SHARE was used to identify hypoglycemic events along with the
subsequent glycemic rise. Hypoglycemic events occurring within a half hour
of each other were considered the same event. Over 50,000 hypoglycemic
events were identified from 1,177 users. Per person, on average, there were
0.96 events/day overall with 0.4 of the events/day occurring overnight (8p to
8a). Events were more common during the day (59%) vs. the night (41%). The
proportion of overall hypoglycemic events that were followed by RHs within
60 min was 18%, and within 90 min was 26%. RHs occurred more often during
the day (21%) vs. the night (13%). This analysis suggests that hypoglycemia is
frequent and that RH is not uncommon. The higher frequency of RH during the
day may be related to meals; RH at night is more likely due to overtreatment.
Supported By: American Diabetes Association (1-14-BS-131 to J.L.)
7‑LB
Phosphodiesterase Type-5 Inhibitor Use in Type 2 Diabetes Is
Associated with a Reduction in All-Cause Mortality
GEOFFREY I. HACKETT, Lichfield, United Kingdom
We retrospectively analysed the pseudoanonymised records of 42 GP
practices in Cheshire, UK and identified all 7860 men diagnosed with T2DM
before 1 January 2007. Data search was performed through the centralised
data facility afforded by Egton Medical Information Systems (EMIS®), a
commercial organization that provides health information systems for the
majority of family practices in the Cheshire county of the UK. Baseline
clinical characteristics and PDE5i treatment data for erectile dysfunction
(ED) were obtained. All analyses were conducted using the Stata statistical
software based on available patient data through January 31 2014. Amongst
those PDE5i treated individuals with a history of AMI there were fewer
ADA-Funded Research
For author disclosure information, see page LB98.
LB2
A vs. B 0.62 ( CI 0.41 – 0.95- P=0.027). For PDE5Is the HR was 0.17 (CI 0.05 0.56-) p=0.004 and for statin use HR was 0.59 (CI 0.36 0.97-) p=0.038.
In this cohort of type 2 diabetes men at high cardiovascular risk, low
baseline T was associated with increased mortality. After Cox analysis, T
therapy showed 62% reduction in mortality. Regular use of “on demand”
PDE5I use was associated with an independent reduction in all-cause
mortality.
Supported By: Bayer
The MicroRNAs in the Pathogenesis of Metabolic Memory
8‑LB
10‑LB
The Tumour Suppressor CDKN2A/p16INK4a Control Perivascular
Adipose Tissue Development
YUNFEI LIAO, LULU CHEN, XUEYU ZHONG, Wuhan, China
“Metabolic memory” is identified as a phenomenon that prior exposure to
hyperglycemia results in the long-lasting deleterious effects on cardiovascular
events. More and more researches show that epigenetics play an important
role in the pathogenesis of metabolic memory. It remains unclear whether
microRNA (miRNA) dysfunctions participate in the event. In this study, the
miRNA arrays were adopted to seek the miRNAs which may be involved
in the metabolic memory and verified in vivo and in vitro. Sixteen miRNAs
were found differentially expressed. Among these miRNAs, the expressions
of miR-125b, miR-146a-5p and miR-29a-3p were associated with persistent
impaired endothelial function and altered inflammatory gene expressions
including nuclear factor-κB (NF-κB) subunit p65. Direct inhibition of miR125b expression or increased miR-146a-5p expression blunted NF-κB signals
and improved the endothelial function. Luciferase reporter assays confirmed
the biochemical relationship for miR-125b targeting on tumor necrosis
factor alpha-induced protein 3 (TNFAIP3), and miR-146a targeting on TNF
receptor-associated factor 6 (TRAF6) and interleukin-1 receptor-associated
kinase 1 (IRAK1) during the activation of NF-κB pathway. Thus our findings
demonstrate that glucose induced changes in miR-125b and miR-146a-5p are
related to the long-lasting activation of NF-κB pathway and contribute to
follow-up metabolic memory.
SARAH HANNPU, KRISTIAAN WOUTERS, CÉLINE CUDEJKO, JONATHAN VANHOUTTE, ANTHONY LUCAS, EMANUEL BOUCHAERT, CASPER G. SCHALKWIJK,
ANNE TAILLEUX, BART STAELS, RÉJANE PAUMELLE, Boston, MA, Maastricht,
Netherlands, Lille, France
Genome wide association studies (GWAS) have linked variants on chromosome 9p21.3 situated near the CDKN2A/B locus with the risk for coronary artery disease (CAD) and type 2 diabetes (T2D). Both diseases are
characterized by accumulation of inflamed perivascular adipose tissue (pAT),
which contributes to the onset of endothelial dysfunction, atherosclerosis
and thrombosis. The CDKN2A/B locus encodes, amongst other genes, for
p16INK4A a well known tumor suppressor protein. As a cell cycle regulator,
p16INK4a is involved in senescence and aging. p16INK4a regulates fasting
induced hepatic gluconeogenesis. Moreover, p16INK4a is a modulator of
macrophage activation and polarization. Altogether these data suggest that
CDKN2A/B gene products may modulate the inflammatory response and glucose homeostasis leading to T2D development. However, whether it plays a
role in adipogenesis and pAT formation and/or phenotype is still unknown.
Using 3T3L1 preadipocytes cells and primary mouse embryonic fibroblasts
(MEF), we demonstrate that p16INK4a deficiency increased expression of
key adipocytes marker (CEBPa, PPARg, Adiponectin) and fat storage without
affecting clonal expansion. To study in vivo adipogenesis, we treated p16+/+
and p16-/- mice with rosiglitazone. Aortas of treated p16-/- mice displayed
increased expression of markers of adipogenesis and adipocyte precursor,
interestingly this effect was not observed in the other AT depots. As bone
marrow is a niche of preadipocyte precursor cells and since rosiglitazone has
been shown to mobilize these cells for peripheral adipogenesis, we tested
whether bone marrow p16-deficiency affects pAT depots by using chimeric
p16+/+Ldlr-/- and p16-/-Ldlr-/- mice fed a western diet. Bone marrow p16deficiency increased pAT around the aortic root. To conclude, we identify
a new role of p16INK4a in adipogenesis and pAT development which could
explain the link between genetic variants on 9p21 and CVD development.
Supported By: European Genomic Institute for Diabetes
11‑LB
Type 2 Diabetes Mellitus in Insulinization: Biochemical, Haemo‑
static, and Inflammatory Markers
NADMY A.Z. GONÇALVES, RENATA T. PETRI, RITA DE CÁSSIA R. GONÇALVES,
DANIELA A.M.G. DO BEM, BIOQUIMICA CLÍNICA UFES, Vitória, Brazil
The aim of this study was to investigate biochemical, haemostatic and
inflammatory markers in patients with diabetes mellitus type 2 (DM2)
who evolved into insulinization. This study was composed by 80 patients
attended in Primary Care Unit at Vitória (Brazil). The evaluated group was
composed by 40 patients with DM2 in insulinization, and 40 controls were
selected without DM2. There was no difference between groups regarding
age (57.05 ± 2.386 x 57.33 ± 1.819 years), sex and insulin resistance. In DM2
group 85% had diabetes for more than five years and the time of insulinization was around 5.54 (± 5.85) years. Markers of inflammation, hypercoagulability and fibrinolysis were studied: high-sensitive C reactive protein (hsCRP),
fibrinogen, D-dimer (D-Di) and plasminogen activator type 1 inhibitor (PAI1). The polymorphism (-675 4G / 5G) of the PAI-1 gene has been correlated
with plasma levels. Biochemical parameters included: glucose (G), glycated
hemoglobin (A1C), total cholesterol (TC), HDL cholesterol (HDL-C), LDL cholesterol (LDLc), triglycerides (TGC), urea and serum creatinine. There was
significant difference between groups for HDL-C, VLDL-C, TGC, urea, hsCRP
and fibrinogen. DM2 group in insulinization presented correlations between:
fibrinogen and D-Di, hsCRP and fibrinogen, PAI-1 and triglycerides, D-Di and
G (negative). In controls these correlations were observed: fibrinogen and
G, fibrinogen and hsCRP and PAI-1 and G. PAI-1 levels were higher in controls with genotype 4G4G. Binary logistic regression showed hypertensive
patients have a risk 4.18 (1.426 to 12.28, p=0.009) times more likely to have
DM2 with insulinization and that individuals with hyperfibrinogenemia have
a 3.29 (1.006 to 10.775, p=0.049) times greater risk. According to our results,
it is possible to suggest that patients with DM2 in insulinization have an
Supported By: National Natural Science Foundation of China
9‑LB
Testosterone Replacement Therapy and PDE5 Inhibitor Use in Type
2 Diabetes Are Independently Associated with a Reduction in AllCause Mortality
GEOFFREY I. HACKETT, Lichfield, United Kingdom
The diabetes registers of 5 UK general practices (n=857, mean age 63)
were screened for baseline total (TT), 12 nmol/l or less and free testosterone
(FT) 0.25nmol/l or less levels according to current EAU guidelines, between
April 2007 and April 2009 and allocated to 1 of 3 groups: A Normal T. B Low
T untreated, and C low T (treated with long acting testosterone undecanoate
in a RCCT ). We report follow up data after mean 5.8 years.
Unadjusted death rates were A 11.2% (36/320), B 16.85% (61/362) and C
3.43% (6/175) analyzed on an ITT basis. Men treated with T were a mean
5.4 years younger, had higher BMI, BP, HbA1c, baseline cholesterol and
were twice as likely (36.6 vs. 15.5%) to be taking a PDE5 inhibitor. After Cox
regression, the HR (CI) for C vs. B was 0.33 (CI 0.12 – 0.92- P=0.033) and for
ADA-Funded Research
For author disclosure information, see page LB98.
LB3
POSTERS
deaths compared to those never treated with a PDE5i (24.1% (51/161) versus
31.1% (332/1066) respectively). In the cohort of 432 men that had an incident
MI, those who used a PDE5i had a 50% reduction in the risk of mortality
(HR 0.50 (0.29-0.85); P=0.01). In this cohort of type 2 diabetes men at high
cardiovascular risk, PDE5i use was seemingly associated with a significant
reduction in both overall mortality and mortality in those with a history of
AMI.
Acute and Chronic
Complications
Complications—Macrovascular—Atherosclerotic
Late Breaking Abstracts
Cardiovascular Disease and Human Diabetes
Complications—Macrovascular—Atherosclerotic Cardiovascular Disease and Human Diabetes
14‑LB
Within-Visit Blood Pressure Variability Predicts Increase in Glyce‑
mia
Supported By: FAPESP
POSTERS
Acute and Chronic
Complications
exacerbated inflammatory state in addition to an increased thrombotic risk
being more favorable for the development of cardiovascular disease.
KAUMUDI J. JOSHIPURA, MARIBEL CAMPOS, FRANCISCO MUNOZ-TORRES,
ALBA D. RIVERA, JUAN C. ZEVALLOS, San Juan, PR
12‑LB
There is a bi-directional relationship between high blood pressure and
diabetes. Within-visit blood pressure variability (BPV) may impact autonomic
and humoral response, and is associated with pre-diabetes/diabetes in a
few cross-sectional studies, and the direction of the association is unclear.
This study evaluates within-visit systolic (SBPV) and diastolic (DBPV) variability as risk factors for increased glycemia over a 3 year follow-up, within
the ongoing San Juan Overweight Longitudinal Study (SOALS). The analysis
includes 634 overweight/obese, 40-65 year old Hispanics who completed
follow-up to date. Within-visit SBPV and DBPV are defined as the maximum
difference between the three baseline measures taken few minutes apart
using standard blood pressure techniques. Increased glycemia was defined
as > 20% increase from baseline in fasting glucose, 2 hour post load glucose
or HbA1c. The SBPV ranged from 0-36 mmHg (mean=4.1, SD=3.6), and DBPV
from 0-28 (mean=3.4, SD=3.0). Participants with SBPV >10 had significantly
increased risk of progression in glycemia compared to those with SBPV <
10 (RR=1.34, 95% CI: 1.02-1.76), and with increased risk of progression to
pre-diabetes/diabetes (RR=1.82, 95% CI: 1.10-3.00) within the 3 year followup. Both models adjusted for age, gender, smoking, physical activity, waist
circumference, reported hypertension diagnosis, and hypertension medication that may impact BPV. Additional control of SBP and DBP influenced the
estimates by <10%. The DBPV >10 did not show any association. The systolic
blood pressure variability, which can be easily assessed in routine office visits, may be an independent predictor of increased glycemia and progression
to pre-diabetes/diabetes.
The Involvement of PKC-theta-NF-kB in Regulating PAI-1 Expres‑
sion in Vascular Smooth Muscle Cells
HONG-CHI CHEN, YI-CHUN LIAO, YUNG-CHIEH LIN, JONG-KAI HSIAO, Hualien,
Taiwan, Taipei, Taiwan
Increased expression/activity of protein kinase C (PKC) isoforms in vascular smooth muscle cells (VSMC) have been shown to cause vasoconstriction,
leading to hypertension. The activation of PKC resulted from high concentrations of glucose and nonesterified fatty acids has been shown in vascular
cells of diabetic and insulin resistant patients, and of animal models, suggesting that it has significant roles in microvascular complication, cardiac
hypertrophy, and in promoting atherosclerosis. Since its discovery, PKC-theta has been recognized as a master regulator for the activation and survival
of T cells. However, current understanding of PKC-theta’s role in VSMC is
still very limited. In this study, we showed that Angiotensin II (Ang II) treatment stimulated a rapid and transient 5-fold increase of PKC-theta phosphorylation in rat VSMC in two minutes and this increase was reduced to two
fold in five minutes, suggesting that PKC-theta might be an effector in Ang II
signaling in VSMC. Further investigation showed that both Ang II-stimulated
mRNA and protein expressions of plasminogen activator inhibitor-1 (PAI-1),
the major regulator of both tissue and urokinase plasminogen activators,
were inhibited by a myristoylated PKC-theta pseudosubstrate. Accordingly,
the reporter gene assay revealed that the expression of a constitutively active PCK-theta mutant enhanced PAI-1 promoter activity, suggesting that
PKC-theta is mediating the Ang II-stimulated PAI-1 transcription in VSMC. In
addition, while pretreatment of BAY 11-7082, an inhibitor of nuclear factorκB (NF-κB), completely blocked Ang II-stimulated PAI-1 protein expression,
the PKC-theta inhibition reduced the Ang II-induced phosphorylation of IκB,
suggesting that NF-κB is downstream of PKC-theta signaling in VSMC. In
summary, our data suggest that PKC-theta-NF-κB signaling plays an important role in regulating PAI-1 transcriptional activation.
Supported By: R01DE020111, U54MD007587
15‑LB
Cardiovascular Outcomes of Saxagliptin Treatment in African
Americans with Type 2 Diabetes: Results from the SAVOR-TIMI 53
Trial
SAMUEL DAGOGO-JACK, KWAME OSEI, BENJAMIN M. SCIRICA, LAWRENCE
A. LEITER, KYUNGAH IM, BOAZ HIRSHBERG, ITAMAR RAZ, DEEPAK L. BHATT,
SAVOR-TIMI 53 STEERING COMMITTEE AND INVESTIGATORS, Memphis, TN, Columbus, OH, Boston, MA, Toronto, ON, Canada, Wilmington, DE, Jerusalem, Israel
13‑LB
Effects of Sitagliptin plus Granulocyte-Colony Stimulating Factor
in Patients after Acute Myocardial Infarction (Sitagrami Trial)—
Cardiac and Vascular Outcomes
African Americans (AA) have higher prevalence of type 2 diabetes (T2DM)
and higher mortality from cardiovascular disease (CVD) than Whites, but
race-specific data on CVD outcomes from prospective studies are scant.
The SAVOR-TIMI 53 trial randomly assigned T2DM patients with high CVD
risk to receive saxagliptin (SAXA) or placebo (PLO) and followed them for a
median of 2.1 yr. North America enrollees (N=5136) self-identified as nonHispanic Black/AA (N=459); non-Hispanic White (WA) (N=3750), Hispanic
(HA) (N=785) or non-Hispanic Asian (N=142). The primary endpoint was the
composite of CV death, myocardial infarction (MI), or ischemic stroke. The
secondary composite endpoint was CV death, MI, stroke, hospitalization for
unstable angina, heart failure (HF), or coronary revascularization. A primary
endpoint occurred in 38 (8.3%) AA, 46 (6.4%) HA, 289 (7.7%) WA, and 12
(9.2%) Asians (P=0.37). Secondary composite endpoint occurred in 16.2%,
11.5%, 15%, and 15%, respectively (P=0.06). Hospitalization for heart failure occurred in 6.3% of AA, 2.7% of HA, 4.1% of WA, and 3.1% of Asians
(P=0.01); other secondary endpoints did not differ significantly by race/ethnicity. SAXA treatment (vs. PLO) did not increase or decrease the risk of the
primary (8.4% vs. 8.2%, P=0.72) or secondary composite endpoints (17.6%
vs. 14.9%, P=0.61) in AA or other racial/ethnic groups studied. SAXA treatment (vs. PLO) was associated with increased risk of hospitalization for HF
in WA (4.9% vs. 3.3%, P=0.008) but not in AA (5.4% vs. 7.0%, P=0.47), HA
(2.5% vs. 2.8%, P=0.90), or others. In conclusion, Blacks in the SAVOR-TIMI
53 study had a higher risk of hospitalization for heart failure compared to
other racial groups, but that risk was not exacerbated by SAXA treatment.
Although actual events were few, SAXA neither increased nor decreased
the risk of the primary and secondary composite endpoints in AA or other
subgroups. (ClinicalTrials.gov: NCT01107886).
CHRISTOPH BRENNER, HANS D. THEISS, CHRISTINE ADRION, ULRICH GRABMAIER, DANIEL THEISEN, FRANZ VON ZIEGLER, ALEXANDER LEBER, ALEXANDER BECKER, HAE-YOUNG SOHN, ELLEN HOFFMANN, ULRICH MANSMANN,
GERHARD STEINBECK, WOLFGANG-MICHAEL FRANZ, Innsbruck, Austria, Munich,
Germany
In previous pre-clinical studies we have shown that G-CSF based mobilization of bone marrow stem cells in combination with genetic or pharmacological DPP4 inhibition mediates an enhanced recruitment of these stem
cells into the ischemic myocardium via the SDF1/CXCR4 axis after acute
myocardial infarction. This led to an improved cardiac remodeling, enhanced
heart function and increased survival. We have translated these promising
results into a phase III, multi-center, randomized, double-blind and placebocontrolled efficacy and safety trial. As treatment effect we hypothesized
an absolute increase in left/right ventricular ejection fraction of 3.5% six
months after acute myocardial infarction mediated by cardiac regeneration
after application of G-CSF and the DPP4 inhibitor Sitagliptin (SITAGRAMI trial; EudraCT: 2007-003941-34; clinicaltrials.gov: NCT00650143). We enrolled
a total of 174 patients that suffered from large myocardial infarction (either
ST-segment elevation infarction or total occluded coronary vessel, maximum creatine kinase elevation (mean 3081, SD 2106 U/l)) and underwent
successful percutaneous coronary intervention within 24 hours. Patients
were stratified (diabetes, sex) and randomized in a 1:1 ratio. Individuals were
treated with either placebo or G-CSF (10μg/kg/d) over a period of 5 days
together with Sitagliptin (100mg/d) for 28 days. Cardiac MRI was performed
at screening visit and after 6 months, additional clinical follow-up visits were
scheduled after 6 weeks and 12 months. Regarding the primary endpoint
in the final analysis, we could not find a beneficial effect of our therapy on
the mean change in left ventricular EF after 6 months (4.5% treatment vs.
4.7% placebo). Besides primary endpoint data we will present planned and
unplanned secondary endpoints with focus on gender differences and the
effect of GCSF plus Sitagliptin treatment on vascular outcomes.
Supported By: Heinz Nixdorf Foundation
ADA-Funded Research
For author disclosure information, see page LB98.
LB4
Complications—Macrovascular—Cellular
Mechanisms of Atherogenesis in Diabetes
Complications—Nephropathy—Basic and
Experimental Science
16‑LB
18‑LB
Circulating Microvesicles from Diabetic Patients Carry Less miR126 and Have Detrimental Effects on Endothelial Progenitor Cells
Activating of GLP-1 Ameliorates Obesity-related Kidney Disease via
Improving the Metabolism of Triglyceride in Renal Mesangial Cells
HALA AMMAR, XIAOTANG MA, ABOAJELA AJENA, THOMAS M. KOROSCIL,
YANFANG CHEN, JI C. BIHL, Dayton, OH, Zhanjiang, China
YAOMING XUE, MEIPING GUAN, YANMEI ZENG, FUPING LYV, Guangzhou, China
DPP-4 inhibitors have been shown to ameliorate diabetic nephropathy, in
which lipid metabolic disorder may involve. However, it is unknown whether
GLP-1 can improve obesity-related kidney disease through the regulation
of local lipid metabolism of kidney. First, the mice model of obesity-related
kidney disease were established in apoE gene knockout C57BL/6J mice
(6-week-old, apoE-/-) fed with a high fat diet (HFD). Sitagliptin, a DPP-4 inhibitor was mixed in the diet at 0.3% of concentration. At 16th week the
kidney tissues of mice were harvested. In sitagliptin-treated group, the renal
oil-red O staining (+) area was significantly decreased compared with control group. Then we investigate the effects of Exendin-4, a GLP-1 analog, in
triglyceride metabolism of renal mesangial cells. Rat mesangial cells (MCs)
were treated by oleate (200uM) combinated with exendin-4 of different
concentrations. The triglyceride contents in MCs were determined by oilred O staining and glyceridase assay. The gene expressions of SREBP, FAS,
PPARα, CPT-1 and ATGL were analyzed by qRT-PCR. Exendin-4 inhibited
the triglycerides accumulation induced by oleate. The mRNA expressions
of SREBP and FAS were significantly downregulated, while PPARα, CPT-1
and ATGL gene expressions were upregulated by Exendin-4. We conclude
that Exendin-4 improves the lipid metabolism of MCs, which is a potential
mechanism through which Exendin-4 ameliorates the obesity-related kidney
disease. These results help to explain some of the beneficial effects of exendin-4 on obesity-related kidney disease.
Endothelial progenitor cells (EPCs) are reduced in number and dysfunctional in diabetic patients. Determining the factors that impair EPC function
could provide therapy targets for diabetes. Our previous study has demonstrated that circulating microvesicles (cMVs) from diabetic mouse have detrimental effects on EPCs. In this study, we compared the effects of cMVs
from diabetic patients and healthy subjects on EPCs from healthy subjects or
diabetic patients. After co-incubation with cMVs for 24 hours, the EPCs were
collected to determine the migration ability by an assay kit, the apoptotic
rate and reactive oxidative species (ROS) production by flow cytometry. The
levels of miR-126 in cMVs were measured by qPCR. The levels of miR-126
target protein (VEGFR2) in EPCs were also analyzed after co-incubation. To
determine whether miR-126 was involved in MVs-mediated effects, miR-126
inhibitor or mimic was added during the co-incubation. Our results showed:
(1) Compared to EPCs from healthy subjects, EPCs from diabetic patients
displayed a decrease in migration ability and an increase in apoptotic rate
and ROS production; (2) Co-incubation with cMVs from healthy subjects was
able to improve the migration ability and decreased apoptosis and ROS production in EPCs from diabetic patients; (3) In contrast, co-incubation with
cMVs from diabetic patients had the opposite effects on EPCs from healthy
subjects; (4) The expression of miR-126 in cMVs from diabetic patients was
decreased, and the expression of VEGFR2 in EPCs from healthy subjects was
decreased after co-incubation with cMVs from diabetic patients; (5) miR-126
inhibitor significantly decreased the protective effects of cMV in healthy
subjects, while the miR-126 mimic diminished the detrimental effects of
cMVs in diabetic patients. In conclusion, cMVs from diabetic patients are
detrimental to EPCs partially due to the reduction of their carried miR-126.
Supported By: National Natural Science Foundation of China (81470047)
19‑LB
Effect of Progesterone on the Development of Diabetic Nephropathy
in Streptozotocin-induced Diabetic Rats
BAHAA AL-TRAD, IBRAHEEM ASHANKYTY, Ha’il, Saudi Arabia
17‑LB
Previous studies reported that 17β-Estradiol may influence the progression of diabetic renal disease in females. The present study was intended
to provide insight into the specific effects of progesterone, the other female
sex hormone, in diabetic renal complications. Adult female wistar rats were
divided into four groups (n=5-6/group): intact control (non-diabetic, ND), intact diabetic (D), ovariectomized diabetic (OVX-D) and ovariectomized diabetic treated with progesterone (OVX-D+P; 10 mg/kg, s.c, every second day)
for 10 weeks. Diabetes was induced by a single dose injection of 55 mg/kg
streptozotocin. Diabetes was associated with increases in urinary albumin to
creatinine ratio (ACR; mean± SEM; ND, 20.5±1.6; D, 94.6±12.9 mg/g; P<0.05),
the index of glomerulosclerosis (GSI; ND, 0.16±0.08; D, 2.41±0.57; P<0.05),
the mRNA expression of TGF-β (ND, 1.12±0.31; D, 2.85±0.60; P<0.05) and
with a significant decreases in the mRNA expression of podocyte markers;
nephrin (ND, 1.26±0.41; D, 0.26±0.15; P<0.05) and podocin (ND, 0.88±0.09; D,
0.34±0.07; P<0.05). The expression and localization of TGF-β, nephrin, and
podocin were also confirmed by immunohistochemistry. In the OVX-D rats,
these changes were exacerbated while progesterone supplementation markedly attenuated the increases in the ACR (59.4±12.9 mg/g), GSI (1.05±0.31)
and TGF-β mRNA expression (1.04±0.29) compared to D and OVX-D groups.
Furthermore, the reduced expressions of nephrin and podocin in the D and
OVX-D groups were significantly reversed by progesterone supplementation
(0.45±0.16 and 0.64±0.18, respectively). These results provide evidence, for
the first time, that progesterone replacement can ameliorate renal damage
in experimental models of diabetic nephropathy through improve the renal
function; downregulation of renal expressions of TGF-β; along with amelioration of podocyte injury.
Effect of Long-Term Interventions in the Diabetes Prevention Pro‑
gram (DPP) and Its Outcome Study on Coronary Artery Calcium
(CAC)
RONALD GOLDBERG, MARINELLA TEMPROSA, VANITA R. ARODA, ELIZABETH
L. BARRETT-CONNOR, MATTHEW BUDOFF, JILL CRANDALL, DANA DABELEA,
EDWARD S. HORTON, KIEREN J. MATHER, TREVOR J. ORCHARD, DAVID S.
SCHADE, KAROL E. WATSON, Miami, FL, Rockville, MD, Hyattsville, MD, San Diego,
CA, Torrance, CA, Bronx, NY, Aurora, CO, Boston, MA, Indianapolis, IN, Pittsburgh, PA,
Albuquerque, NM, Alhambra, CA
Despite intensive management of cardiovascular (CV) risk factors, coronary heart disease remains a major cause of morbidity and mortality in
type 2 diabetes. Intervention in the prediabetic phase may have a greater
long-term impact on atherosclerosis than waiting for diabetes to develop
before intervening. The DPP demonstrated that intensive lifestyle (ILS) and
metformin (MET) reduced diabetes incidence vs. placebo (PLBO) in high risk
participants (ppts). During long term follow-up, MET ppts continued to receive study metformin and all received group lifestyle. After a mean study
duration of 14 years, we assessed subclinical atherosclerosis by CAC in 2029
ppts using multidetector CT, read centrally, as an Agatston score. For assessment of treatment and covariate effects, Tobit regression models were
used to estimate age-adjusted CAC severity expressed as log (CAC+1). At
the time of CAC assessment, 58% and 67% received lipid- and BP-lowering medications respectively, and 55% had developed diabetes. CAC was
greater in men (mean range was 39.5-66.9 in the 3 groups) than women
(4.7-5.2). While there were no overall differences in CAC between ILS, MET
and PLBO, in a pre-specified subgroup analysis, CAC was significantly lower
in MET vs. PLBO in men (ILS=58.3, MET=39.5, PLBO=66.9; p<0.05) especially
in the youngest baseline age group (25-44 yrs: MET vs. PLBO 3.0 vs. 17.6;
p<0.05) and MET was lower than ILS in subjects who had diabetes (p=0.02).
CAC prevalence (CAC>0) was also lower in men in MET vs. PLBO (ILS=85%,
MET=75%, PLBO=84%; p<0.05). In multivariate models in men, the MET associated effect on CAC was independent of age, race, baseline CV risk factors and diabetes status, but lost significance when diabetes duration was
added. Among men, lower CAC in the MET group suggests that metformin
may delay atherosclerosis development in prediabetes and in early diabetes,
independent of lipid- and BP-lowering therapy.
Supported By: King Abdulaziz City for Science and Technology (M-S-34/44)
20‑LB
Synip Phosphorylation Is Necessary for Insulin-stimulated Glut4
Translocation and Glucose Uptake in Podocyte
SHUICHI OKADA, TSUGUMICHI SAITO, EIJIRO YAMADA, YOKO SHIMODA, AYA
OSAKAI, RYO SHIBUSAWA, JUNICHI OKADA, JEFFREY E. PESSIN, MASANOBU
YAMADA, Maebashi, Japan, Bronx, NY
Previously we reported that the phosphorylation of Synip on serine 99
is required for Synip dissociation from Syntaxin4 and insulin-stimulated
Glut4 translocation in cultured 3T3-L1 adipocytes. We also reported that
the dissociated Synip remains anchored to the plasma membrane by binding to Phos­pha­tidylinositol (3,4,5)-triphosphate. Recently Synip was reported
ADA-Funded Research
For author disclosure information, see page LB98.
LB5
POSTERS
Complications—Nephropathy—
Basic and Experimental Science
Acute and Chronic
Complications
Complications—Macrovascular—Cellular
Mechanisms of Atherogenesis in Diabetes
POSTERS
Acute and Chronic
Complications
Complications—Nephropathy—Clinical and Translational Research
Complications—Nephropathy—Clinical and
Translational Research
to arrest SNARE-dependent membrane fusion as a selective t-SNARE binding inhibitor. In this study, we have newly found that Synip is expressed
in podocytes although at a somewhat lower level than in adipocytes. To
determine whether phosphorylation of Synip on serine 99 is required for
insulin-stimulated Glut4 translocation and glucose uptake in podocytes
we expressed a phosphorylation deficient Synip mutant (S99A-Synip) that
inhibited insulin-stimulated Glut4 translocation and 2-deoxyglucose uptake
in adipocytes. We confirmed that S99A-Synip significantly inhibited insulinstimulated Glut4 translocation and 2-deoxyglucose uptake in podocyte too.
We conclude that serine 99 phosphorylation of Synip is required for Glut4
translocation and glucose uptake in both adipocytes and podocytes, suggesting that defects in Synip phosphorylation may underlie insulin resistance and associated diabetic nephropathy.
A Glucose-activated Sodium Transporter in the Vasculature
23‑LB
Mesenchymal Stem Cell Therapy for Diabetic Nephropathy: A Phase
2 Randomized Controlled Trial
DAVID K. PACKHAM, IAN FRASER, PETER G. KERR, JASON LICHLITER, SILVIU
ITESCU, DONNA SKERRETT, KAREN R. SEGAL, Melbourne, Australia, Richmond,
Australia, Clayton, Australia, New York, NY
The etiology of diabetic nephropathy (DN) includes renal inflammation and
endothelial dysfunction. Allogeneic bone marrow derived mesenchymal precursor cells (MPC), can modulate both inflammatory cells and microvasculature. We conducted a randomized, placebo (PBO) controlled, dose-escalating
trial of MPC at 4 Australian sites in 30 type 2 diabetes/DN subjects (24 men,
6 women) with an estimated serum creatinine (SCr) based glomerular filtration rate (eGFR) of 20-50 ml/min/1.73/m2 and on a stable regimen of reninangiotensin inhibition. Subjects were randomized to a single IV infusion of
PBO (saline) or 150 million (M) or 300M MPCs (N=10 per group). Primary study
period was 12 w with follow-up to 60 w. Renal function was measured by
99 mTc diethylenetriamine pentaacetate (mGFR) at baseline and 12 w, and
by eGFR at all visits. Baseline mean age was 70 years, mean eGFR was
34.6, 35.7 and 34.6 ml/min/1.73/m2 for PBO, 150M and 300M, and 19/30
patients (63%) had eGFR>30. The infusions were well tolerated and there
were no treatment-related adverse events. For mGFR change from baseline
at 12 w, the adjusted least squares mean (LSM) differences (+SE) from PBO
were 4.0+2.8 ml/min1.73/m2 (+8%) for 150M and 3.9+2.8 (+8%) for 300M.
In subjects with baseline eGFR >30, the LSM difference from PBO (n=7) in
mGFR change from baseline at 12 w was 6.2+3.3 (+13%) in the pooled MPC
(n=12), p=0.07. For eGFR change from baseline at 12 w, the LSM differences
from PBO were 4.4+2.2 (+11%), p=0.05, in 150M, 1.6+2.2 (+5%) in 300M and
4.5+2.8 (+11%) in pooled MPC with baseline eGFR>30. Interleukin-6 (IL-6)
was elevated at baseline, and was reduced at 12 w in 300M vs. PBO (-0.21
vs. 2.5 pg/dl; p=0.01). Baseline IL-6 correlated with SCr and eGFR improvement at 12 w in the MPC groups (r= -0.57 and 0.50; both p<0.05) but not in
PBO. In this exploratory study, a single MPC infusion improved or stabilized
GFR over 12 w, most notably in those with baseline eGFR>30. Mechanisms
may include effects on inflammatory cytokines and renal microvasculature.
21‑LB
PAUL HANNA, CHRISTINE DURIS, KEVIN R. REGNER, JOHN D. IMIG, JULIAN H.
LOMBARD, PAULA E. NORTH, NILOOFAR M. TABATABAI, Milwaukee, WI
Diabetes is the leading cause of chronic kidney disease, and diabetic kidney
disease is the major cause of end-stage renal disease. SLC5A4 is a member of
the sodium-glucose cotransporter (SGLT) family and is known as SGLT3. However, SGLT3 is a glucose-activated sodium transporter. Rodents have two
SLC5A4-homologous genes encoding SGLT3a and SGLT3b. The physiological
role of SGLT3 is not well studied and its role in the pathogenesis of diabetes
is not known. Previously, we showed the expressions of SGLT3 mRNA and
protein in human kidney specimens and that of mRNA for SGLT3a in mouse
kidney. To investigate SGLT3 role in the kidney, we examined the localization
of SGLT3 in the human kidney tissue and compared that to that of SGLT3a in
kidneys of C57BL/6 mouse using a panel of our specific antibodies against
SGLTs. In Western blot analysis, SGLT3a antibody hybridized to ~72 kDa
protein band in mouse kidney homogenate. Immunohistochemical analysis
showed SGLT3 was strongly expressed in arterial blood vessels in the human
kidney. Similarly, in mouse kidney, strong SGLT3a signals were observed in
arteries but neither SGLT1 nor SGLT2 antibody stained the vasculature. Vascular expression of SGLT3a was also observed in mouse aorta. Next, the effect of SGLT3 agonist, imino sugar deoxynojirimycin (DNJ), was examined on
isolated mouse kidney arterioles and aortic tissue ex vivo. The results showed
that exposure to 10-150 μM DNJ caused dose-dependent vasoconstriction in
micro- and macrovasculature. This study identified the vascular localizations
of human SGLT3 and mouse SGLT3a. The results suggest that SGLT3 may play
role in the development of vascular diseases in diabetes.
24‑LB
Environmental Contaminant Perfluorooctane Sulfonate and Kidney
Function by Diabetes Status
Supported By: R01DK085031, R01ES004026, R25DK098104
BAQIYYAH CONWAY, KAREN INNES, TINA COSTACOU, JOHN ARTHUR, Morgantown, WV, Pittsburgh, PA, Charleston, SC
22‑LB
Although perfluroakyl acids are environmental contaminants linked to
certain adverse health outcomes, they are also potent oxygen transporters used in organ preservation and synthetic blood development. Data are
scarce on the effect of perfluroakyls on kidney function and chronic kidney
disease (CKD), especially in diabetes (DM). We assessed these associations
by DM status in a large cohort. Participants were from the C8 Health Project
(n=5,270 and 48,832 w/and w/out DM, respectively, age≥20 ys). eGFR was
assessed by the MDRD formula. CKD was defined as eGFR <60. Perfluorooctane sulfonate (C8s) was log-transformed before analysis. Adjusting for age
and sex, C8s was directly related w/eGFR in those w/DM and inversely in
those w/out DM (all p<0.0001; P interaction <0.0001). Further adjusting for
DM duration (in DM) BMI, HDLc, WBC, CRP, serum iron and hemoglobin (hb),
these associations remained significant (Fig. 1a). CKD was present in 21.6%
w/and 7.2% w/out DM. Fig. 1b shows the C8s - CKD associations. When
stratified by CKD, C8s was directly associated w/eGFR in CKD and inversely
in those w/out CKD (Fig. 1c) regardless of DM status. Our data suggest C8s
may have beneficial effects on kidney function in those w/CKD and DM,
conditions where low hb is common, perhaps by protecting against hypoxiainduced kidney damage. The inverse relation of C8s in those w/out CKD,
where low hb is less common, is likely due to reverse causation.
Adiponectin Alters the Kidney-Bone Axis of Mineral Balance
JOSEPH M. RUTKOWSKI, NYNKE VAN POLANEN, PHILIPP E. SCHERER, Dallas, TX
Diabetes is the primary cause of kidney failure and diabetic nephropathy is
a concurrent pathological manifestation of the obesity epidemic. The insulinsensitizing adipokine adiponectin is protective and aiding in recovery of renal
function following injury; however, unlike other adipokines, adiponectin is
reduced in obesity. High adiponectin levels have been correlated with bone
loss, suggesting an additional role in regulating mineral balance. The kidney
controls calcium and phosphate levels with disruptions leading to osteoporosis or vascular calcification. Using adiponectin knockout (KO), wildtype, and
adiponectin overexpressing transgenic (Tg) mice, we sought to identify how
adiponectin may regulate renal calcium and phosphate balance. At baseline,
adiponectin KO mice exhibited lower serum Ca2+, lower Ca2+ excretion, and
higher circulating klotho concentrations than wildtype littermates. Adiponectin-Tg mice on chow diet had markedly lower FGF23 and increased Ca2+ excretion. Challenging these mice with a 2% phosphate (Pi)-enriched diet resulted
in expected increases in serum PTH and FGF23, decreases in secreted klotho,
and, unexpectedly, increased 1, 25-vitamin D in all mice. Adiponectin-Tg mice
were, however, hyper responsive to Pi challenge exhibiting 2-fold higher serum FGF23 and concomitant increase in fractional Pi excretion. These mice
also excreted more Ca2+ with Pi-enriched diet and less klotho protein was
present in kidney. Adiponectin KO mice exhibited a 50% smaller increase in
PTH; serum FGF23 was increased, but significantly less so than in their study
mates. While all mice displayed a loss in bone mass over time, adiponectin-Tg
mice exhibited disproportionately lower bone strength and mass. Adiponectin thus alters calcium and phosphate balance and impacts renal function and
mineral excretion. This work highlights the profound effects of adipose tissue
on renal function and has identified a new mechanism by which adiponectin
may regulate bone mass.
Supported By: National Institutes of Health (R01DK55758, P01DK088761 to
P.E.S.); American Heart Association (12SDG12050287 to J.M.R.)
ADA-Funded Research
For author disclosure information, see page LB98.
LB6
Supported By: National Institutes of Health (U54GM1049)
Complications—Neuropathy
25‑LB
Elevated Soluble Urokinase-type Plasminogen Activator Is a Pre‑
dictor of Incident Renal Disease
27‑LB
SALIM S. HAYEK, SANJA SEVER, YI-AN KO, STAMATIOS LERAKIS, LAURENCE
S. SPERLING, ARSHED A. QUYYUMI, JOCHEN REISER, Atlanta, GA, Boston, MA,
Chicago, IL
Withdrawn
Background: Soluble urokinase-type plasminogen activator receptor (SuPAR) is implicated in the pathogenesis of kidney disease but whether it predicts incident renal dysfunction is unknown.
Methods: The relationship between suPAR levels and renal function was
investigated in 3683 patients recruited in the Emory Cardiovascular Biobank
(mean age 63, 66% males, 17% Blacks, 32% diabetic, median suPAR 3040
pg/mL). Creatinine at enrollment and all subsequent values acquired during
follow-up were collected. Incident kidney disease was defined as a decrease
in eGFR<60 mL/min. The relationship between suPAR levels and eGFR at
baseline and its change with time were analyzed using linear mixed modeling adjusting for clinical covariates.
Results: suPAR levels correlated with baseline levels of eGFR (r=-0.45,
p<0.0001) and urine protein (r=0.22, p<0.0001), independently of demographic and clinical characteristics. Higher suPAR levels were associated
with a more rapid decline in eGFR with time irrespective of age, diabetes
status or race (Figure 1A). Patients with the highest quartile of suPAR level
had a three-fold increased incidence of CKD (Figure 1B).
Conclusions: suPAR level is independently associated with parameters
of renal function, decrease in eGFR and incident kidney disease. Whether
suPAR is a modifiable risk factor for renal disease and therefore a potential
treatment target needs further study.
28‑LB
Role of TLR4 and HMGB1 in Changes in Pain in Type 1 and Type 2
Diabetic Animals
26‑LB
MUNMUN CHATTOPADHYAY, El Paso, TX
Peripheral sensory neuropathy is one of the most common complications of diabetes. Accumulating evidence suggests that chronic low-grade
inflammation involved in the pathogenesis of the disease. We hypothesize
that continuous release of inflammatory mediators in the peripheral nervous system causes the sensory neuropathy in diabetic animals; therefore
blocking this increase will prevent or delay the development of neuropathy.
High mobility group box 1 (HMGB1), a nuclear protein released by injured
and severely stressed cells, promotes cytokine release via its interaction
with the Toll-like receptor (TLR). In this study we investigated the changes in
cytokine/chemokine profiles in the dorsal root ganglia (DRG) and compared
the changes in behavior with treatment with TLR4 inhibitor in type 1 diabetic
(T1D) model of pain and HMGB1 inhibitor in type 2 diabetic (T2D) model of
pain. At 6 weeks after hyperglycemia, diabetic rats demonstrated significant
changes in thermal hyperalgesia manifested by a decrease in withdrawal
latency to heat, mechanical hyperalgesia measured by the Randall Sellito
method of paw pressure. Both T1D and T2D rats exhibited marked increases
in IL1β and TLR4, TNFα, pp38, HMGB1, RAGE by 6 weeks after diabetes as
Comparing Medications that Can Cause Renal Tubular Harm vs.
Nonharmful: Their Use Patterns, Health Services Utilization, and
Expenses
MARY L. DAVIS-AJAMI, JUN WU, JEFFREY C. FINK, Richmond, VA, Greenville,
SC, Baltimore, MD
The study compared population-level characteristics, individual-level
medication use, health services utilization and expenses between individuals prescribed medications that can cause renal tubular harm versus those
with any other or no medication(s) and compared them by co-existent chronic
disease in adults with pre-dialysis kidney disease. This retrospective study
used Medical Expenditure Panel Survey (MEPS) household component longitudinal files (years 2006-2012; panels: 11-16) including adults > 18 years
with pre-dialysis kidney disease. Two groups were created: 1) those prescribed medications that can cause acute tubular nephritis and/or tubular
toxicity (termed “harmful”) and 2) those with any other or no prescription
medication(s). From published work, select drugs cited as possibly inducing
ADA-Funded Research
For author disclosure information, see page LB98.
LB7
POSTERS
tubular kidney damage were used. Longitudinal weights accounted for MEPS
complex survey design. Logistic regression models assessed the likelihood of
harmful drug use. Generalized linear regression models assessed expenses.
Of 809 eligible adults with kidney disease (weighted frequency: 14,665,892
U.S. non-institutionalized population), 72% had medications termed harmful.
Of those, 47.2% and 52.8% were prescribed one and at least two harmful
medications, respectively. In co-existent chronic conditions, hypertension
dominated (72.3%), then diabetes (49.5%), coronary heart disease (33%),
arthritis (23.6%), and COPD (17.6%). Being older, from the southern U.S. region, and greater comorbidity significantly increased the likelihood of using a
drug that may induce renal tubular harm. Renally harmful drug use vs. none
showed significantly greater all-cause health services utilization and health
expenses. No significant differences existed in kidney disease-related utilization or expense. Vigilance is needed when prescribing medications in kidney
disease, particularly for comorbid conditions, the elderly, or uninsured.
Acute and Chronic
Complications
Complications—Neuropathy
POSTERS
Acute and Chronic
Complications
Complications—Neuropathy
determined by the Western blot analysis. To determine whether increased
TLR4 level is responsible for the painful neuropathy in diabetic animals, we
injected TLR4 antagonist TAK242 for 5 days at a dose of 1.5 mg/kg per day
I.P. in T1D animals. We injected HMGB1 inhibitor Glycyrrhizin for 5 days/
week up to 2 weeks at a dose of 50mg/kg per day I.P. to T2D rats. Diabetic
animals treated with TLR4 and HMGB1 inhibitors had significant decrease
in mechanical hyperalgesia. This study suggests that TLR4/HMGB1 plays
an important role in the inflammatory aspect of the painful neuropathy in
T1D and T2D animals. Understanding the mechanisms of diabetic neuropathy
may provide a novel treatment approach for this difficult-to-treat complication of diabetes.
Supported By: American Diabetes Association (7-12-BS-021 to M.C.)
29‑LB
31‑LB
Autoantibodies to Calcium Channels in Type 1 Diabetes Mediate
Oxidative Stress in Pancreatic Beta Cells
MRS-based In Vivo Biomarkers Characterizing Chronic Uncon‑
trolled Hyperglycemia at Ultra-high Field (9.4 Tesla)
DAISY MOHANASUNDARAM, DEVANGI MODI, SKYE PEARS, TOM GORDON,
MICHAEL JACKSON, Adelaide, Australia
SAKTHIVEL SEKAR, SANKAR SERAMANI, BOOMINATHAN RAMASAMY, PETER
CHENG LEE PING, KISHORE KUMAR BHAKOO, Singapore, Singapore
Type 1 diabetes (T1D) is an autoimmune disease caused by the loss of
significant numbers of functional beta cells, resulting in loss of blood glucose
regulation. Autonomic neuropathy is a common but poorly understood complication of T1D resulting in significant morbidity. Previously, we have demonstrated that autoantibodies derived from T1D patients and directed against
L type Voltage gated calcium channels (VGCC) contribute to autonomic dysfunction of the gastrointestinal tract and bladder. We further demonstrated
that these antibodies directly alter the function of the rat insulinoma line, Rin
A12, however the mechanism behind this effect was not clear. In the current
study, we have attempted to address how these anti-VGCC antibodies cause
disruption of Rin cell function, by examining the effect of anti-VGCC autoantibodies on the induction of oxidative stress in pancreatic beta cells using
a novel method. Immunoglobulin from patients and healthy controls were
purified from serum using the caprylic acid method. Rin m5F and Min 6 cells
were treated with 2’, 7’-Dichlorofluorescein Diacetate (DCFDA) at a final
concentration of 5uM for 5 min in the dark. DCFDA treated cells were then
incubated for 2 hrs at 37C with patient or control IgG at a final concentration
of 0.4 mg/ml. The cells were then analysed by flow cytometry to detect the
level of Reactive Oxygen Species production (ROS) in terms of mean DCFDA
intensity. We found a significant increase in the level of ROS production in
both Rin and MIN cells treated with patient IgG compared to cells treated
with controls. This preliminary work is the first to demonstrate that antiVGCC autoantibodies mediate a stress response in pancreatic beta cells,
and suggest that these antibodies, in addition to contributing to autonomic
dysfunction, may also form part of the immunological insult responsible for
destruction of pancreatic beta cells.
Impact of metabolic changes in the brain due to hyperglycemia and/or diabetes are poorly understood due to difficulty in measuring the brain metabolism in-vivo. Recent advances in ultra-high field MR spectroscopy allow us
to observe metabolic changes with increased spectral resolution. The study
aimed to identify in-vivo biomarker(s) of neurodegeneration due to chronic
uncontrolled hyperglycemia using a 9.4T MRI scanner. Hyperglycemia was
induced in a cohort of male Wistar rats (~300g, n=6) with STZ (60 mg/kg, IV).
Blood glucose and HbA1c levels were documented. MRS data were acquired
on 2, 6, 10, 14, 18 and 40 weeks post STZ injection employing a PRESS sequence with a voxel (2.5×4×4 mm3) localized in the hippocampus [TR/TE/
TA/NA: 4000ms/13ms/8 min/128]. Metabolite quantitation was performed
using LC Model. Amongst the various brain metabolites (glucose, glutamate,
glutamine, GABA, glutathione, myo-inositol, NAA and taurine) quantitated,
significant reduction (p<0.05) in glutathione and increase in glucose and
Myo-inositol were apparent with the progression of the condition. Glutathione has major role in sequestering free radicals and toxins from normal tissues; glutathione depletion in the brain plays a major role in oxidative stress
(Koji et al, 2013) and an accumulation of destructive free radicals, which then
progressively leads to neurodegeneration. Furthermore, myo-inositol has
been reported as a biomarker for glial cells; elevated level of myo-inositol
in the hippocampus has been associated with mild cognitive impairment in
Alzheimer’s disease (Miller et al, 1993). We report that levels of glutathione
and myo-inositol may serve as in-vivo biomarkers for identifying progressive oxidative stress and cognitive impairments respectively, as a result of
chronic uncontrolled hyperglycemia; thereby emphasizing the need for early
therapeutic interventions. Furthermore our study exemplifies the value of
1H-MR spectroscopy to characterize neuronal metabolism in-vivo.
30‑LB
Correlates of Somatic and Autonomic Neuropathy in Colombian Pa‑
tients with Type 2 Diabetes
32‑LB
Role of Peroxynitrite in the Progression of Small Nerve Fiber Func‑
tion in Diabetes Mellitus
CARLOS O. MENDIVIL, CLAUDIA R. TIQUE, ARTURO ORDUZ, JOSE L. CÁRDENAS,
JORGE E. PATIÑO, WILLIAM KATTAH, Bogotá, Colombia
JOSH EDWARDS, CAROLINA M. CASELLINI, ELLYN KORNFEIND, HENRI PARSON, IRINA G. OBROSOVA, MARK A. YOREK, AARON I. VINIK, Norfolk, VA, Baton
Rouge, LA, Iowa City, IA
Diabetic neuropathy is greatly under-recognized, and its causes insufficiently understood. We assessed factors associated with cardiovascular
autonomic neuropathy (CAN), distal symmetric polyneuropathy (DSP) and
sudomotor dysfunction (SD) in 154 patients with type 2 diabetes (DM2),
age 61.4 +/- 9.5, diabetes duration 12.2 +/- 11.4 years. CAN diagnosis was
made with the Ewing Battery of autonomic tests. DSP diagnosis was defined
as a Total Symptoms Score (TSS) ≥ 5 or a Michigan Neuropathy Disability
Score (NDS) ≥ 3. SD was diagnosed using the Neuropad® test. The overall
prevalence of CAN, DSP and SD was very high at 68.0%, 45.0% and 67.5%,
respectively. Prevalence increased across quartiles of diabetes duration for
CAN (from 56.8 to 86.3%, p-trend: 0.008), and NDS-defined DSP (from 33.3
to 58.3%, p-trend: 0.0036). Mutually-adjusted logistic models including 12
predictors showed significant associations of age (OR 1.08, 95% CI: 1.021.14) and A1c (OR 4.34, 95% CI: 1.13-16.6) with CAN. Plasma triglycerides and
BMI were significantly associated with SD. No variable was associated with
DSP. Our results highlight the extreme importance of good glycemic control
in the prevention of CAN, and suggest that in many patients with DM2 CAN
and DSP are allowed to progress over time without effective interventions.
Accumulation of nitrotyrosine (NT) has been associated with nerve dysfunction in diabetes mellitus (DM). The objective of this study was to evaluate
the relationship between NT and nerve dysfunction in healthy controls (HC),
diabetic patients with (DM-DPN) and without diabetic peripheral neuropathy
(DM-Non-DPN). We hypothesized that an association would exist between
NT levels and the progression of neuropathy. This was a two year prospective study of 60 patients (20 HC, 14 DM Non-DPN, and 26 Definite DM-DPN).
Neuropathy diagnosis was stratified according to the Toronto Consensus
guidelines. Individuals were assessed at baseline and after two years using
clinical neuropathy scores, quantitative autonomic function tests (QAFT), intraepidermal nerve fiber density (IENF), and nerve conduction studies (NCS).
Mean NT levels (pmol/mg protein) in serum were 3.17 ± 0.29 for HC, 4.22 ±
0.36 for DM Non-DPN, and 4.83 ± 0.38 for Definite DM-DPN. Mean NT levels
in diabetic subgroups were significantly higher than controls. A deterioration
of small nerve fiber (SNF) function was observed in the DM Non-DPN group
after two years for total neuropathy scores (p=0.007), neuropathy impairment scores of the lower limbs (NIS-LL) sensory scores (p=0.004) and NIS-LL
total scores (p=0.004) as well as QAFT measures of heart rate variability
(p=0.02). However, baseline NT levels, HbA1C, triglyceride levels, HDL, LDL,
and blood pressure values were found to not be predictors of SNF deterioration upon simple and multivariable regression analysis. Our findings suggest
in this preliminary study none of the traditional predictors of SNF, including
ADA-Funded Research
For author disclosure information, see page LB98.
LB8
are associated with pathologies of disease including diabetes, diabetic complications, aging, and neurodegenerative diseases. In the present work, we
found that MG significantly induced the expression of transcription factor
SP1 (specific protein 1) and NF-Y (nuclear transcription factor Y) using Cignal finder reporter array in human retinal pigment epithelial cells (ARPE-19).
Cytotoxicity were performed using the MTT assay in MG (5, 10 μM) or high
glucose (HG, 30 mM)-treated ARPE-19. According to the FACS analysis with
Annexin V staining, apoptotic cells were significantly increased in MG, HG,
and MG-HG-cotreated cells. MG induced the expressions of SP1 (1.54 fold)
and NF-Y (2.29 fold) and activated ERK1/2 and c-Jun in a dose dependent
manner in ARPE-19. The C/EBP homologous protein (CHOP), activated by
ER stress, and interaction of SP1 and NF-Y also were increased in MGtreated cells. Further, tight junction proteins such as ZO-1, occluding, and
claudin-1 were significantly increased by MG or HG. Taken together, these
results demonstrate that SP1 and NF-Y transcription factors are involved in
the regulation of ER stress and expressions of tight junction by MG or HG.
Therefore, our finding that MG triggers the expression and direct binding of
SP1 and NF-Y and MG-induced SP1 signaling pathway may serve as novel
mechanisms against diabetic retinopathy.
Supported By: National Institutes of Health
Complications—Ocular
33‑LB
Differential Gene Expression Profiling in the Retina of Diabetic
Rats
HONG-LIANG WANG, JING HAN, TIANTIAN LV, YAN WU, GAIMEI HAO, JIE HE,
WEI WANG, Beijing, China
Diabetic retinopathy (DR) is a common microvascular complication of
diabetes characterized by high disability rate and low quality of life. In this
study, we aim to investigate mRNA expression changes in the retina of rats
with diabetes induced by streptozocin (STZ) and probe into the mechanism
of DR, then provide experimental basis to the prophylaxis and treatment of
DR. Six male SD rats were randomly divided into normal group and model
group. A single intraperitoneal injection of STZ 65mg/kg was used to induce diabetic rats. The normal group was given isopyknic sodium citrate.
mRNA of the retina was extracted after 32 weeks of diabetes. The mRNA
expression changes were identified using rat genome microarrays, and gene
ontology (GO) analysis and the KyotoEncyclopedia of Genes and Genomes
(KEGG) were used to select target genes by function and pathway. Several
key up-regulated genes were CCR6, IL10RA, CXCL9, SOCS3 and TPO, which
were further validated by Quantitative Real-time PCR (qPCR). Microarray data analysis revealed that DR induced 138 genes up-regulated and 137 genes
down-regulated compared with the normal group. GO and Pathway analysis
showed that the majority of change genes were associated with cytokinecytokine receptor interaction, cellular signal transduction and neuroactive
ligand-receptor interaction. Five genes were confirmed with qPCR, consistent with the results from microarray. DR changed expression of many genes
which regulated various biological functions. These findings might advance
our understanding of the regulatory mechanisms underlying the evolution of
DR, and might provide the novel therapeutic target in DR.
Supported By: K14040
RPE Barrier Breakdown in Diabetes: Is It Real?
36‑LB
YUN-ZHENG LE, MEILI ZHU, Oklahoma City, OK
Diabetic retinopathy (DR) is traditional regarded as a microvascular
disorder. However, it is increasingly clear that the retinal pigment epithelium (RPE) plays a critical role in “vascular leakage” in DR. To investigate
the significance of RPE barrier breakdown in DR, we developed an imaging
assay for RPE barrier-specific leakage (IOVS, 52:2160). To explore the role
of the RPE barrier in diabetic macular edema (DME), a major vision loss in
DR, we examined the dynamics of fluorescein isothiocyanate (FITC)-dextran
passed through the RPE barrier in diabetic rodents. RPE barrier leakage was
measured de novo by florescent microscopy of retinal sections from diabetic
rodents injected intravenously with FITC-dextran. Computer-assisted quantification was used to determine the relative levels of RPE- or endothelial
barrier-specific leakage. The RPE barrier leakage was detected immediately
after intravenous injection of FITC-dextran, indicating that the leakage from
choroidal circulation to the retina was more efficient than that from retinal
vessels. While the RPE barrier leakage occurred everywhere, there were
clearly severe leakage sites (image: 6 mo diabetic rats). In addition, the RPE
barrier leakage appeared to be comparable, if not more, to that from the
endothelial barrier. Our data suggest a prominent role for the RPE barrier
breakdown in “vascular leakage” in DR, which provides a cellular mechanism
for DME patients with the cellular lesion near the RPE.
34‑LB
P-MST and P-YAP Decreased in Rats with Diabetic Retinopathy
JING HAN, YAN WU, TIANTIAN LV, HONGLIANG WANG, JIE HE, GAIMEI HAO,
WEI WANG, Beijing, China
The Hippo signaling pathway is a core kinase cassette that consists of
MST1/2, LATS1/2, SAV1 and MOB1. And YAP is a downstream target of this
pathway. The Hippo-YAP signaling pathway plays crucial roles in organ size
control and cancer development through modulating cell proliferation. Diabetic retinopathy is one of the most prominent complications of diabetes and
is characterized by vascular proliferation. But whether Hippo-YAP signaling
pathway altered in diabetic retinopathy is not elucidated. In this study, SD
rats were fasted for 14 hours before STZ injection. STZ was dissolved in
citrate buffer and intraperitoneally injected at 65 mg/kg body weight. Age
matched control rats received equal volume of vehicle (citrate buffer). Rats
with blood glucose levels higher than 16.7 mmol/L were considered to be
diabetic and used for studies. After diabetes was induced for 32 weeks, ocular blood flow velocities in central retinal artery were determined by Color
Doppler imaging and the eyes were isolated for retinal digest preparations
and transmission electron microscope. The expression of P-MST1/2 and
P-YAP in retinas were determined by immunohistochemistry. The results
showed that compared with normal group, the blood flow velocity in central
retinal artery decreased, basement membrane of blood vessel thickened,
capillary density increased and the ratio of endothelial cells to pericytes
elevated in diabetic group. Meanwhile P-MST1/2 distributed mainly in inner
plexiform layer and P-YAP distributed mainly in pigment epithelium layer of
retinas in rats. In diabetic group, P-MST1/2 and P-YAP decreased compared
with normal group. In conclusion, Hippo-YAP pathway maybe participates in
the process of diabetic retinopathy. These findings will contribute to provide
new mechanism underlying diabetic retinopathy and lay a foundation for improving new drugs to ameliorate diabetic retinopathy.
Supported By: American Diabetes Association (1-10-BS-94 to Y-Z.L.); National
Institutes of Health (GM104934, EY020900, EY021725); Presbyterian Health Foundation; Oklahoma Center for Adult Stem Cell Research; Choctaw Nation
37‑LB
Improvements in Diabetic Retinopathy (DR) following Ranibizumab
(RBZ) Medical Therapy
JEFFREY S. HEIER, CHIRAG P. SHAH, PIN-WEN WANG, SHAMIKA GUNE, ANNE
FUNG, Boston, MA, South San Francisco, CA
35‑LB
DR, a diabetic microvascular complication of the retina, is a leading cause
of blindness in American adults. DR worsens over time and diabetic macular
edema (DME) can develop at any stage of DR. Panretinal photocoagulation
(PRP) has been the standard of care since the early 1990s to treat proliferative DR (PDR) but leads to irreversible loss of tissue and visual field. In
Feb 2015, the FDA approved RBZ (Lucentis®) for the treatment of DR (non-
Methylglyoxal Induces Expressions of CHOP and Tight Junction via
SP1 and NF-Y Transcription Factors in ARPE-19
BO-JEONG PYUN, Daejeon, Republic of Korea
Methylglyoxal (MG), a highly reactive metabolite of glucose, is a major
cell-permeant precursor of advanced glycation end products (AGEs). AGEs
ADA-Funded Research
For author disclosure information, see page LB98.
LB9
POSTERS
NT, proved to be significant contributors of the progression of neuropathy.
Larger studies are needed to further explore the relationship between NT
levels and the progression of SNF neuropathy.
Acute and Chronic
Complications
Complications—Ocular
POSTERS
Acute and Chronic
Complications
Diabetic Dyslipidemia
proliferative DR [NPDR] and PDR) in patients (pts) with DME; the first medical
therapy to receive that label. This analysis summarizes changes in DR severity with RBZ therapy in pts with DME in RIDE and RISE, 2 parallel phase 3
trials. Pts (N = 759) were randomized to monthly 0.3 mg RBZ, 0.5 mg RBZ,
or sham injection. At mo 24, pts in the sham arm crossed over to monthly
0.5 mg RBZ. At mo 36, 500 pts entered an open label extension (OLE) and
received 0.5 mg RBZ PRN based on worsening vision and retinal thickness.
DR severity was graded on the ETDRS DR Severity Scale using color fundus
photos. Pts received PRP at investigator discretion. At mo 24, significantly
more DR improvement was observed with RBZ vs. sham: for 0.3 mg RBZ,
0.5 mg RBZ, and sham, rates of ≥ 2-step improvement were 38%, 36%, and
5%, respectively; respective rates of ≥ 3-step improvement were 13%, 15%,
and 1%. At mo 36, 12 mo after sham-arm pts crossed to active treatment,
rates of ≥ 2-step improvement were 39%, 39%, and 24% for 0.3 mg RBZ, 0.5
mg RBZ, and sham/crossover, respectively; rates of ≥ 3-step improvement
were 15%, 13%, and 4%, respectively. When pts switched to less frequent
therapy in the OLE, 75% of pts receiving some treatment and nearly 60% of
pts not receiving any RBZ injections maintained their mo 36 DR scores at
mo 48. By mo 24, 1%, 1%, and 12% of pts received PRP in the 0.3 mg RBZ,
0.5 mg RBZ, and sham arms, respectively. Monthly RBZ therapy resulted in
meaningful improvements in DR severity and decreased the need for PRP
laser when compared with sham. Some patients maintained improvements
with less-than-monthly RBZ dosing.
HOMA-R, FFA or BMI, suggesting that decreased FFA with ipragliflozin is not
a consequence for lowered blood glucose levels or enhanced beta-cell function. Significant negative correlations between the changes (Δ) of FFA and
ΔHOMA-B (R=-0.434), and positive correlations between ΔFFA and ΔHbA1c
(R=0.432) were observed only in ipragliflozin group, indicating that reduction
of FFA is linked to enhancement of beta-cell function and decreased blood
glucose levels with this drug. By contrast, no correlations were observed
between ΔFFA and ΔHOMA-R or between ΔHOMA-B and ΔHOMA-R in ipragliglozin group, implying that decreased FFA and/or increased beta-cell
function are not related to reduced insulin resistance with this drug. Taken
together, these results implicate that beta-cell function is activated partly
through reduced lipotoxicity (FFA) with ipragliflozin.
40‑LB
Acute Leptin Treatment Reduces PCSK9 in ob/ob Mice and Leptindeficient Patients
AMY E. LEVENSON, MARY HAAS, JI MIAO, REBECCA J. BROWN, RANGANATH
MUNIYAPPA, SUDHA B. BIDDINGER, Boston, MA, Bethesda, MD
Proprotein convertase subtilisin/kexin type 9 (PCSK9) promotes degradation of the Low Density Lipoprotein Receptor (LDLR), and thereby increases
serum cholesterol levels. Currently, there are several emerging pharmacotherapies aimed at inhibiting PCSK9 to decrease Low Density Lipoprotein
Cholesterol (LDL-C) in patients. However, the endogenous regulation of
PCSK9 is poorly understood. Leptin is a cytokine-like hormone that plays
a key role in the regulation of energy metabolism and body weight, as well
as in lipid metabolism. Indeed, leptin treatment has been shown to reduce
LDL-C and total plasma cholesterol in leptin deficient patients. In this study,
we examined the effects of leptin on PCSK9 expression in both leptin deficient ob/ob mice and humans with lipodystrophy, a hypoleptinemic state.
In ob/ob mice, four days of recombinant mouse leptin treatment (24 mcg/
day, delivered by an osmotic pump) decreased plasma PCSK9 concentrations (15.3±1.9 ng/mL versus 155.9±12.6 ng/mL in vehicle treated mice;
n=5/group; p=0.001). In parallel, leptin treatment decreased hepatic Pcsk9
mRNA expression by 93% (p=0.003). However, hepatic Ldlr mRNA and
LDLR protein levels were also reduced with leptin treatment, and LDL-C was
slightly increased. Lipodystrophic patients, treated for four to six months
with a synthetic leptin analog (Metreleptin, ~4.4 mg/day via subcutaneous
injection), showed a 26% decrease in plasma PCSK9 concentration (221±102
ng/mL post-leptin treatment versus 298 ± 109 ng/mL pre-leptin treatment;
n=8; p=0.008). This decrease in PCSK9 was associated with a decrease in
LDL-C (r=0.751, p=0.03). In summary, these data indicate that leptin replacement can suppress PCSK9 levels in both mice and humans. In humans, the
decrease in PCSK9 is associated with a decrease in LDL-C, suggesting that
some of the beneficial effects of leptin on plasma lipids could be mediated
by PCSK9.
Diabetic Dyslipidemia
38‑LB
Exposure to Common Food Additive Carrageenan Alone Leads to
Fasting Hyperglycemia and in Combination with High-Fat Diet Ex‑
acerbates Glucose Intolerance and Hyperlipidemia without Effect
on Weight
SUMIT BHATTACHARYYA, LEO FEFERMAN, TERRY G. UNTERMAN, JOANNE K.
TOBACMAN, Chicago, IL
Exposure to the common food additive carrageenan caused glucose
intolerance, insulin resistance, and impaired insulin signaling in human
hepatocytes and C57BL/6J mice. Current experiments were performed to
determine: the minimal amount of carrageenan which produced glucose intolerance; the impact of carrageenan in combination with high fat diet on
glucose tolerance; and whether carrageenan alone increased fasting blood
glucose and hemoglobin A1c. Carrageenan (10 µg/ml) was added to the water of C57BL/6J mice, and the impact compared to control mice on a regular
diet, mice on a high fat diet, and mice on the combination of carrageenan
and high fat diet. Carrageenan exposure led to abnormal glucose tolerance
after 6 days, and to elevated fasting blood glucose at 23 weeks. Effects of
carrageenan were similar to those in mice on the high fat diet, but without
weight gain, suggesting that carrageenan intake may be a useful mouse
model for non-obese diabetes. The combination of carrageenan and high
fat diet shortened the interval to fasting hyperglycemia and increased levels
of total cholesterol and triglycerides, compared to high fat diet alone. The
amount of carrageenan intake (~50 µg/day/25 gm mouse = 2 µg/g) is about
half the anticipated daily intake in the average adult diet (250 mg/day/60
kg adult = ~4.2 µg/kg), suggesting that carrageenan intake may contribute
to the development of diabetes in association with the Western diet and
may exacerbate the effects of the high fat diet on glucose tolerance, insulin
resistance, and hyperlipidemia.
Supported By: National Institutes of Health-National Institute of Diabetes and
Digestive and Kidney Diseases (K125K12DK094721-03)
41‑LB
American Diabetes Association 2015 and American Heart Associa‑
tion 2013 Lipid Guidelines: Are They Interchangeable?
FATEMA H. AL HAMMADI, ASMA A. AL NUAIMI, JAMILA S. AL DHUHOURI, SARAH AL SHAIKH, SARA BEULA, TAREK M. FIAD, Abu Dhabi, United Arab Emirates
Conventional practice of treating dyslipidaemia entails titration of statin therapy aiming at achieving a goal LDL-C level. Two new guidelines, the
ADA1 and the American Heart Association (AHA) 2 moved away from this
practice, instead, both introduced a risk-based decision-making on grounds
of which, either moderate-intensity (M-I) or high-intensity (H-I) statin therapy
is recommended 1, 2. This study aimed at assessing whether the 2 guidelines
yields similar rates of statin initiation and dose-intensity. In the context of
primary CVD prevention, the impact of adopting the ADA guidelines among
445 diabetics aged 40-75 years was: 1) all patients (100%) qualified for statins therapy; b) 97% of subjects were considered for H-I statin therapy. In
contrast, the impact of adopting the AHA guidelines to this age group is: 1)
all patients qualified for statins therapy; b) the proportion of patients considered for H-I and M-I statins was 56% and 46% respectively. Among the 2
other age groups e.g. 20-39 years (n=99) and >75 years (n=24), specific recommendations were made by the ADA but not by the AHA guidelines. Based
on the ADA guidelines, the proportion of patients between the ages of 20-39
years being considered for M-I and H-I statins was estimated as 36% and
30% respectively. Among the >75 years age group, 100% of patients will be
considered for statins initiation, the options being either M-I or H-I statins.
In the setting of CVD secondary prevention, all 129 patients (100%) qualified for H-I statin therapy according to both guidelines. In conclusion, the
ADA and AHA guidelines on lipid management are not interchangeable with
Supported By: American Diabetes Association (1-12-BS-216 to J.K.T.)
Effect of Ipragliflozin on Lipotoxicity and Beta Cell Function
39‑LB
EIJI KUTOH, MITSURU HIRATE, ASUKA WADA, Tokyo, Japan
Besides genetic elements, several modifiable factors are linked to betacell deterioration including chronic hyperglycemia (glucotoxicity) and elevated free fatty acid (FFA, lipotoxicity). Ipragliflozin, a SGLT-2 inhibitor, exerts its
effects by facilitating glucose excretion through the kidneys, thereby reducing glucotoxicity. However, effects of SGLT-2 inhibitors on beta-cell function
involving lipotoxicity remain unknown. The aim of this study is to explore this
question. Treatment naïve subjects with T2DM were administered either 2550 mg/day ipragliflozin (n=25) or 12.5-25 mg/day alogliptin (as a control, n=26)
monotherapy. The baseline characteristics were similar in these two groups.
At 3 months, in ipragliflozin group, significant reductions of HbA1c (from
10.35% to 8.46%, NGSP), HOMA-R (-23.9%), FFA (-33.5%) and BMI (-2.9%)
were observed, while significant increases of HOMA-B (32.8%) were noted.
In alogliptin group, similar reductions of HbA1c and increases of HOMA-B
from those of ipragliflozin were observed, while no changes were noted in
ADA-Funded Research
For author disclosure information, see page LB98.
LB10
Foot Care—Lower Extremities
42‑LB
Contrasting the Impact of the ADA 2014 and 2015 Guidelines on the
Practice of Lipid Management
MASSIMO MILANI, ADALBERTO FEDERICI, GIOVANNI FEDERICI, Milan, Italy,
Rome, Italy
FATEMA H. AL HAMMADI, ASMA A. AL NUAIMI, JAMILA S. AL DHUHOURI, SARAH AL SHAIKH, SARA BEULA, TAREK M. FIAD, Abu Dhabi, United Arab Emirates
An effective hydration of foot skin in diabetics is a relevant preventive
strategy in order to maintain a healthy foot, contributing to reduce the risk
of ulcers development. No long-term data are available regarding effects of
emollient in treating severe lower limb skin xerosis (SS) in type 2 diabetics.
We evaluated efficacy of 8-month topical urea 5% with arginine and carnosine cream (UC) in comparison with a glycerin-based cream (SEC) in type 2
diabetic patients with moderate-severe SS of feet. We assessed the effect
of UC on feet skin hydration in a randomized, assessor-blinded comparative study in 50 diabetic patients, aged 40-75 years, treated with UC (N=25)
or comparator (N=25) for 32 consecutive weeks. Primary study outcomes
were a 9-point grading Xerosis Assessment Scale (XAS) score and a 4-point
grading overall cutaneous score (OCS) evaluated at baseline, at weeks 4, 12,
and 32 by an investigator unaware of treatment allocation. In addition skin
hydration and desquamation were objectively evaluated by means of Hydr8
bio-impedance analysis device at baseline and at week 32.
Results: UC induced significantly greater hydration than SEC (p=0.01) with
a 91% reduction at week 32 in XAS score (from 5.5 to 0.5; p < 0.001) in
comparison with baseline values. After 4 weeks, compared with the SEC
treated group, XAS score in UC treated group was significantly lower (1.0 vs.
3.9; p= 0.048). At month 8 Skin hydration (+75%) and desquamation (-77%)
evaluated by Hydr8 statistically improved in UC treated subjects both in
comparison with baseline and in comparison with SEC group. Application of
urea 5%, arginine and carnosine cream for 8 consecutive months increases
skin hydration and alleviates the condition of SS in type 2 diabetic patients
in comparison with a control glycerol-based emollient cream with a greater
efficacy observed as soon as 4 weeks of treatment.
The ADA 2014 guidelines, recommended the widely practiced approach
whereby stain therapy is titrated, aiming at defined LDL-C goal1. The ADA
2015 Guidelines introduced a risk-based decision making for which moderate-intensity (M-I) or high-intensity (H-I) statin therapy is advocated2. This
study aimed at assessing the impact of adopting the ADA 2015 Guidelines
on an unselected diabetic population currently been treated in accordance
with the ADA 2014 guidelines1. Analysis included 698 diabetic patients. In
the context of primary CVD prevention, the impact of adopting the 2015 ADA
guidelines2 among diabetics aged 40-75 years (n=445) is: 1) the proportion
of patients eligible for statins increased from 87% to 100%; b) H-I statin
therapy usage increased from current level of 25% to 97%. Among the 2039 years age group (n=99), the new guidelines will result in: a) an increase
in eligibility for statin initiation from current level of 40% to 66%; b) H-I
statin use will increase from a current level of 3% to 30%. Among the >75
years age group (n=24), the new guidelines will result in: a) proportion of
statin eligible patients will increase from 92 to 100% b) in contrast to current use of H-I statins in 17% of subjects, the new ADA guidelines considers
the options of either M-I or H-I statins initiation in 100% of subjects. Among
subjects with history of CVD (n= 129), adopting the new ADA guidelines mandates that all patients (100%) being considered for H-I statin therapy (up
from 46%). In conclusion, adopting the ADA 2015 lipid guidelines will lead
to a striking increase in proportion of patients initiated on statin therapy as
well as those offered H-I statins among all age groups. The highest impact
will affect subjects aged ≤75 years, where the implementation of the new
recommendation will lead to an additional 13-26% of diabetic subjects being initiated on statin therapy as well as 3-10 fold increase in the use of H-I
statins. (1) ADA. Diabetes Care 2014;37 (Suppl 1) S14-S80. (2) ADA. Diabetes
Care 2015;38 (Suppl 1):S52.
Supported By: Isdin
45‑LB
Topical Administration of Pirfenidone Increases Healing of Chronic
Diabetic Foot Ulcers: A Randomized Crossover Study
43‑LB
MARCELA JANKA-ZIRES, ANA C. URIBE-WIECHERS, PALOMA ALMEDA-VALDES,
JOEL LOPEZ-GUTIERREZ, SONIA C. JUAREZ-COMBONI, FRANCISCO J. GOMEZPEREZ, Mexico City, Mexico
Withdrawn
Introduction: Diabetic foot is one of the most common and devastating
complications of diabetes mellitus and the most frequent cause of amputation of the lower extremity. With conventional treatment, diabetes ulcers
heal in 30% of cases in 20 weeks. Pirfenidone is a topical medication with
biological, anti-inflammatory and anti-fibrotic effects, which can be useful in
chronic diabetic foot ulcers by activating the healing process.
Methods: This is a randomized crossover study. Patients with diabetic foot
ulcer Wagner 1 or 2, with at least 4 weeks duration were randomly assigned
into two groups. Group 1 was first treated with topic pirfenidone treatment
(PT) plus conventional treatment (CT) for 8 weeks. After this period, they
continued with CT for additional 8 weeks. Patients assigned to group 2 were
first treated with CT and subsequently with PT for the remaining 8 weeks.
All patients attended the Diabetic Foot Clinic every week for 16 weeks. The
primary end points were the complete ulcer healing and the percentage of
size reduction.
Results: Final data were obtained from 36 ulcers in 27 patients, 20 men
and 7 women. The mean age was 57.4±12.5 and diabetes evolution 16.5
[14.5-23.7] years. Baseline ulcer size and depth were not different between
groups. Fifty percent of patients in treatment with PT healed before eight
weeks vs. 14.3% of patients in CT (P= 0.032). Between 8 and 16 weeks,
30.8% of patients with PT healed vs. 0% in CT group (P= 0.067). By week 8,
the reduction in ulcer size was 98% [73-100] with PT vs. 57.5% [28.9-74] with
CT, P= 0.012. By week 16, the reduction in ulcer size was 93% [42.7-100] with
PT and 20% [8-72.1] with CT (P= 0.032).
Conclusions: In diabetic chronic foot ulcers the addition of topical pirfenidone to conventional treatment is associated with a superior percentage of
ulcer healing and a significant reduction in the percentage size.
ADA-Funded Research
For author disclosure information, see page LB98.
LB11
POSTERS
44‑LB
A Urea, Arginine, and Carnosine Cream Shows Greater Efficacy in
the Treatment of Severe Feet Xerosis in Type 2 Diabetic Patients in
Comparison with Standard Emollient Glycerol Cream: A Random‑
ized, 8-Month, Assessor-blinded, Controlled Trial
Acute and Chronic
Complications
Foot Care—Lower Extremities
much greater likelihood of using H-I statins in diabetic subjects aged 4075 years when the ADA guidelines are used. Furthermore, the ADA but not
the AHA/ACC guidelines provides specific guidance on statins treatment in
the younger and the older age groups. (1) ADA. Diabetes Care 2015;38(suppl
1):S52 (2) AHA Guidelines. Circulation 2014;129(25 Suppl 2):S1-45.
Diabetes Education
Diabetes Education
48‑LB
The Beneficial Effect of Mediterranean Diet on Glycaemic Control
in Youths with Type 1 Diabetes Mellitus: A Controlled Study
46‑LB
THEOFANEIA TSACHALINA, IOANNIS KYRGIOS, EFTHIMIA EFSTRATIOU, MICHAIL MELISSINOS, KYRIAKOS KAZAKOS, ASSIMINA GALLI-TSINOPOULOU,
Thessaloniki, Greece
Mediterranean Diet (MedDiet) has been reported as an optimal diet for
the prevention of chronic diseases and maintaining good health. Despite the
fact that impact of MedDiet on type 2 diabetes and the metabolic syndrome
in adults has been previously described, no data concerning MedDiet and
young patients with type 1 diabetes mellitus (T1DM) have been reported.
American Diabetes Association’s guidelines in 2014 recommended MedDiet
for the management of T1DM. We aimed with this control study to investigate the influence of MedDiet on glycaemic control in youngsters with
T1DM. Twenty four adolescents with T1DM were consecutively enrolled and
divided to follow either a 7 day Med-style Diet or an ad libitum diet (ALD).
The two groups did not differ statistically in gender, age, BMI, glycated
haemoglobin (HbA1c) and required insulin dose (RID). Patients were asked
to perform 6 blood glucose (BG) measurements daily for 2 weeks. The first
week was for both group ALD and only 6 BG measurements. During the study
period a reduction in the second week was noted which was statistically
significant greater in the intervention group (IG), at post prandial BG values
(159 mg/dL vs. 117 mg/dL p=<0.001) at daily rates (163 mg/dL vs. 127 mg/dL
p=<0.001) hypothetical HbA1c (7.2% vs. 6.0% p=<0.001) and RID (0.96 IU/kg
vs. 0.92 IU/kg p=0.001). Also a significantly greater decrease in preprandial,
average prandial, total daily BG, hypothetical HbA1c and RID was noted in
the IG, as compared to the control group (p<0.05). As regards the 1-h and 2-h
postprandial BG, although the decrease in the IG was greater, this difference
did not reach the level of statistical significance (p>0.05). The increase in the
number of total daily hypoglycaemias tended to be greater in the IG (2.77 vs.
0.45 p=0.09). Our study demonstrates that adopting a diet containing foods
from the pyramid of MedDiet is recommended in adolescents with T1DM in
order to maintain euglycaemia which thereby reduces the risk of long-term
complications.
POSTERS
Behavioral Medicine, Clinical
Nutrition, Education, and Exercise
Withdrawn
47‑LB
Impact of a Type 2 Diabetes Education Program on Clinical Out‑
comes during Ramadan
49‑LB
The Relationship between Online Activity and Biometric Tracking
and Medication Adherence among Members with Diabetes
MAHMOUD IBRAHIM, LAURA N. MCEWEN, NAHED ALI, SAMIR H. ASSAADKHALIL, HYAM R. TANTAWI, GAMELA NASR, SHAYAN MOHAMMAD MORADI,
ALY A. MISHA’L, FIRAS A. ANNABI, EBTESAM M. BA-ESSA, SUHAD M. BAHIJRI,
JAAKKO TUOMILEHTO, WILLIAM H. HERMAN, McDonough, GA, Ann Arbor, MI,
Ismaïlia, Egypt, Alexandria, Egypt, Cairo, Egypt, Lexington, KY, Amman, Jordan, Dammam, Saudi Arabia, Jeddah, Saudi Arabia, Helsinki, Finland
MICHAEL TAITEL, JENNY JIANG, OSAYI AKINBOSOYE, GREGORY ORR, Deerfield, IL
In 2013, Walgreen Co., a national community pharmacy and retailer,
launched an online rewards program to help rewards program members
track physical activity and biometrics. In April 2014, the program expanded
to reward members for connecting devices and logging blood glucose (BG).
The study is to determine the relationship between program member engagement and adherence to oral diabetes medications (ODMs), with focus
on physical activity and BG tracking. This is a retrospective cohort study
of members newly enrolled in the Walgreens Balance Rewards for healthy
choices™ (BRhc) program between May and June 2014 who logged activities
such as steps (walking, running) and biometrics (body weight, BG) within 6
months of enrollment and filled at least one medication in 2014. Steps logged
were converted into miles on a 2,000:1 basis. Proportion of Days Covered
(PDC) was used to measure adherence and calculated from each member’s
first prescription fill date (Index) in 2014 to December 31, 2014. A total of
1,855 new BRhc members met the study criteria. Of these, 735 members
tracked their BG and 1,309 tracked steps, with 235 members logging steps
more than 1 mile/day. BRhc members who filled ODMs were older and had
more co-morbidity compared to the general BRhc member population with
any prescription in 2014 (median age = 46.9 years vs. 38.1 years; median
maintenance medication count = 5 vs. 2). Members who tracked their BG
levels had significantly higher adherence to ODMs compared to non-trackers
(82.9% vs. 77.5%; Diff = 5.4%; Increase = 6.97%, P<0.001). And, compared to
members who logged less than 1 mile/day, members who logged at least 1
mile/day over the 180-day tracking period had significantly higher adherence
to ODMs (vs. 86.4% vs. 78.5%; Diff = 7.9%; Increase = 10.05%, P<0.0001).
This study demonstrated a significant relationship between higher levels of
member engagement in healthy activities and biometric tracking through
BRhc™ program and greater adherence to prescribed ODMs.
Muslims who fast during Ramadan abstain from eating and drinking from
before dawn until after sunset. The ADA has recommended that people with
diabetes who fast receive education to achieve a safer fast. The objective
of this study was to determine if pre-Ramadan education resulted in a safer
fast for people with type 2 diabetes (T2DM). Participating clinics in Egypt,
Iran, Jordan, and Saudi Arabia were randomized to provide patients with
T2DM who intended to fast during Ramadan 2014 an individualized education program or usual care. There were 8 intervention and 8 control clinics.
The education program addressed meal planning, physical activity, blood
glucose monitoring, and acute metabolic complications, and provided an
individualized diabetes treatment plan. Pre-Ramadan surveys were administered to 1010 people, 857 (85%) of whom also completed post-Ramadan
surveys. Of these, 774 reported having T2DM and fasting during Ramadan.
In the latter group, age (mean±SD) was 48±10 years, 59% were female, BMI
was 30±4 kg/m2, and HbA1c was 8.8±1.4%. After Ramadan, those who attended clinics that provided individualized education were more likely to
have modified their diabetes treatment plan during Ramadan (97% vs. 88%,
p<0.0001), to perform self-monitoring of blood glucose at least twice daily
(70% vs. 51%, p<0.0001), and to have improved knowledge about hypoglycemic signs and symptoms (p=0.0007). Those who attended clinics that provided education also reduced their BMI (-1.1±2.4 kg/m2 vs. -0.2±1.7 kg/m2,
p<0.0001) and HbA1c (-0.7±1.1% vs. -0.1±1.3%, p<0.0001) during Ramadan
compared to those who attended control clinics. There were more mild (77%
vs. 67%, p=0.0031) and moderate (38% vs. 19%, p<0.0001) hypoglycemic
events reported by those who attended intervention clinics, however, they
reported fewer severe hypoglycemic events (23% vs. 34%, p=0.0017). In
conclusion, this individualized education and diabetes treatment program
helped patients with type 2 diabetes achieve a safer Ramadan fast.
ADA-Funded Research
For author disclosure information, see page LB98.
LB12
Exercise
KATHERINE WENTZELL, ASHLEY ATKINS, JULIE GRIFFITH, JOYCE KEADY, BRITTANY MARTIN, KERRY MILASZEWSKI, CINDY PASQUARELLO, ELLA STEPHENS,
LORI M. LAFFEL, Boston, MA
Older teens and young adults with T1D experience suboptimal glycemic
control and often miss clinic appointments; the Take Charge Clinic (TCC) was
created as a quality improvement effort to overcome these challenges. TCC
was a nurse-led weekly walk-in clinic, providing increased care accessibility
and support (in-person and by text messaging), directed at high risk young
persons with T1D, ages 16-25 with A1c >9%, missed appointments or a recent DKA episode. During the TCC, patients saw either an RN/CDE or NP for
standard diabetes education and care. A trained non-medical staff member
met briefly with each patient during the TCC to provide support; each patient
received a $10 gift card after meeting with support staff. During the 6-month
pilot, 23 young persons had 40 unique TCC encounters. Participants (35%
male, 35% pump users) had a mean age of 18.7±2.2 years, T1D duration of
9.1±4.6 years and initial A1c of 11.0±1.8%. Participants attended between 1
and 6 visits (both regular and TCC visits) during the 6 months (mean 2.3±1.6
visits, median 2 visits). Participants attending ≥2 visits (n=13) had a mean
A1c improvement of 0.45±0.8 (p=0.06). Additionally, if the study window is
extended 30 days to see effect beyond 6 months, there was a significant
improvement in A1c for this cohort (n=17) from a baseline A1c of 11.0±1.6%
to 10.3±1.2% (p=0.001). Support staff sent 118 text messages (reminders to
attend clinic, support for diabetes goals set at visits) to 20 patients and 7 patients replied with 44 texts. The clinic was designed to be walk-in, yet only 1
patient attended without scheduling. Participants reported that short-notice
appointment availability and increased visit frequency were helpful. These
pilot results suggest that the TCC for high risk young persons with T1D may
improve glycemic control; the combination of increased care accessibility,
support from non-medical staff and text messaging may enhance engagement and empowerment with care.
% IT OR IC 95%
P
Group
25.4% 3.41 1.91-5.16 0.0001
12.1% 2.49 1.29-4.77 0.005
26.0% 2.40 1.48-3.88 0.0001
19.8% 2.21 1.25-3.89 0.005
50.0% 1.41 0.89-2.27 0.141
22.0% 0.73 0.39-1.34 0.311
52‑LB
Associations between Diabetes Knowledge and Glycemic Control
among Incarcerated Persons with Diabetes
LOUISE A. REAGAN, WILLIAM BARTA, New York, NY, Storrs, CT
While there is abundant research in the community describing how factors such as knowledge about diabetes, and race/ethnicity influence glycemic control, research of this nature in the incarcerated diabetic population
is nonexistent. In order to develop effective diabetes programming and prevent complications, it is imperative that we begin to understand the factors
that influence glycemic control in this population. In a prior cross-sectional
study of 124 incarcerated persons (M age 47.3 years, SD 9.46) with diabetes
(12.9% type 1, 59.7% type 2 and 27.4% unaware of type), we found that diabetes knowledge (Spoken Knowledge for Low Literacy in Diabetes) (SKILLD)
was positively associated (p<0.001). This result is contrary to findings from
research with community dwelling individuals that has shown diabetes
knowledge to have no relationship or an inverse relationship to glycemic
control. For this secondary analysis, we hypothesized that race/ethnicity,
and length of incarceration were moderating factors on the relationship
between diabetes knowledge (SKILLD) and glycemic control (log10 HbA1c).
Participants were 93.5% male, 40% black, 37% white and 23% Latino with
77% having HS, GED or less education, M HbA1c 8.2 and on 85% on insulin.
Results confirm our hypothesis that length of incarceration and race/ethnicity moderate the association of diabetes knowledge (SKILLD) and glycemic
control. Consideration of the influence of duration of incarceration and race/
ethnicity should be explored when developing diabetes programming for incarcerated persons with diabetes.
51‑LB
Myths about Insulin Therapy in Latin Patients with Type 2 Diabetes
JUAN C. LIZARZABURU, JOSE VALERA, GABRIELA VARGAS, SOFIA VILLANES,
FLOR VENTO, LORENA VILLENA, YOBANA BELTRAN, BLANCA FUENTES, JOSE
LACA, EIKO WATANABE, LIZARDO TORRES, Lima, Peru
A barrier to insulin therapy (IT) in diabetic patients is the presence of
myths about its use. There are few publications about this topic in Latins.
We reviewed six myths described in the literature. The aim of the study was
to describe the presence of myths about IT in patients with type 2 diabetes
(T2D), at the Central Air Force Hospital in Lima-Peru. We conducted a crosssectional study from January-December of 2014. Summary statistics for 360
from 5236 T2D patients was evaluated. Patients with type 1 diabetes mellitus, gestational diabetes, illiterate were excluded. We used a survey, using Likert-scale, grouped in: agree, disagree or indifferent respect the myth.
Stepwise logistic regression was used. Of the study population with a mean
age of 67.4±10.7 years, 37.2% were on IT and 60.8% were female. The mean
disease duration was 10.3±9.2 years. In the IT group, 67.3% had received
Education in Insulin Use (EIU). We found that the most common myth was
(5) with 48%, while the myth less frequent was (2) with 13.9%. The Non-IT
group had greater presence of myths. The myth (1) was 3.4 times more present in Non-IT group regarding the IT group with p <0.05. Greater presences
of myths were in patients with non-EIU, but not significant differences regarding EIU patients among the IT group The presence of myths in the Latin
patient with T2D is high. It was higher in the patient on Non- IT than patients
on IT, but its presence was independently if they received or not education.
Exercise
53‑LB
Interrupting Prolonged Sitting Modulates Glycemic Control in
Adults with Type 2 Diabetes
PADDY C. DEMPSEY, JENNIFER M. BLANKENSHIP, NEVILLE OWEN, NORA
STRAZNICKY, NEALE COHEN, BARRY BRAUN, BRONWYN A. KINGWELL, DAVID
DUNSTAN, Melbourne, Australia, Amherst, MA, Fort Collins, CO
Interrupting prolonged sitting with light activity lowers postprandial plasma glucose in overweight/obese adults, but the effect in individuals with
type 2 diabetes (T2D) is unknown. We studied the effect of uninterrupted
sitting compared to sitting broken up by brief bouts of light intensity walking
or by simple resistance activities on glycemic control in T2D patients. In a
randomized crossover trial, inactive adults with T2D consumed a standardized eucaloric diet over 22 h (9am - 7am) while wearing a continuous glucose
monitor system for 3 x 8 h conditions (6-day washout): i) SIT: uninterrupted
sitting (control); ii) LW: sitting + 3 min bouts of light-intensity walking at 3.2
km/h every 30 min; and iii) SRA: sitting + 3 min bouts of simple resistance
activities (alternating half-squats, calf raises, brief gluteal contractions and
knee raises) every 30 min. Over 22 h, both LW and SRA significantly reduced
mean [interstitial] glucose, time in hyperglycemia (glucose > 10 mmol/L) and
glycemic variability (quantified via the SD of mean glucose and mean amplitude of glycemic excursions) relative to uninterrupted sitting (Table). These
simple interruptions to sitting significantly reduced the time in hyperglycemia, mean glucose and glycemic variability in adults with T2D. With the ubiq-
ADA-Funded Research
For author disclosure information, see page LB98.
LB13
POSTERS
Table. Myths in IT and in Non-IT Groups.
Myth
% Non-IT
Group
(1) Insulin use is similar
51.7%
that use illegal drugs.
(2) The insulin injections
25.6%
are painful.
(3) The use of insulin means
45.7%
that I will not be able to
have a normal life.
(4) The use of insulin brings
35.4%
complications such as
blindness, amputation
and even death.
(5) If I start using insulin,
58.5%
I will need to use it for
the rest of my life.
(6) The use of insulin leads
17.0%
to weight gain.
Behavioral Medicine, Clinical
Nutrition, Education, and Exercise
50‑LB
Accessible Care Model to Improve Glycemic Control in High Risk
Teens and Young Adults with Type 1 Diabetes (T1D): Lessons from
the Take Charge Clinic (TCC)
Exercise
POSTERS
Behavioral Medicine, Clinical
Nutrition, Education, and Exercise
uity of sedentary behaviours and the low adherence to structured exercise,
this approach has the potential to be beneficial and practical.
pants showed significantly higher insulin levels compared with moderately
fit (8.20±4.80 vs. 6.17±2.59 μU/ml, p=0.024) and highly fit (vs. 5.32±3.57 μU/
ml, p=0.008). Circulating adiponectin and chemerin levels were also associated with fasting insulin levels after adjustment for gender, age, stage,
and BMI. To study combined impact of adiponectin and chemerin levels on
fasting insulin levels participants were divided into four groups according
to their adiponectin and chmerin levels. Participants in high adiponectin
and low chemerin group showed lower fasting insulin level (4.79±2.14 vs.
8.49±4.64 μU/ml, p=0.006) compared with participants with low adiponectin and high chemerin levels. Multiple linear regression analysis confirmed
that adiponectin and cardiopulmonary fitness (β=-0.224, p=0.009; β=-0.267,
p=0.006) were independently associated with fasting insulin level. Our results suggest that physical fitness, adiponectin and chemerin levels may
contribute to circulating levels of insulin. Findings from the current study
may suggest that exercise influences the prognosis of colorectal cancer patients by influencing circulating levels of adiponectin and chemerin as well
as physical fitness level.
Table. (A) Participant Characteristics and (B) Effects of the Three Trial
Conditions on Glycemic Control.
(A) Participant characteristics (B) Effects of the three trial conditions on
measures of glycemic control over 22 h
Characteristic N or mean
Measure
SIT
LW
SRA
(95% CI)
of glycemic (control)
control
Number of study
14 M 10 F
Time in hyper‑
60.3
37.5
26.5
participants
glycemia (%)
(49.2, 71.3) (26.5, 48.6)** (15.5, 37.6)**
Age (yr)
62.3 (64.8, 59.8)
Time in hyper13.3
8.3
5.8
glycemia (hr)
0.8, 15.7) (5.8, 10.7)** (3.4, 8.3)**
BMI (kg/m2)
33 (34.4, 31.7)
Mean interstitial
11
9.4
8.6
glucose (mmol/L) (10.2, 11.8) (8.5, 10.2)** (7.8, 9.4)**
HbA1c (%)
7.2 (7.5, 7)
SD of mean
2.2
1.9
1.7
interstitial
(2, 2.5)
(1.7, 2.2)** (1.5, 2)**
glucose
Note: All participants were Metformin/diet
MAGE (mmol/L)
104.94
85.5
76.18
controlled individuals with type 2 diabetes.
(92.11, 117.78) (72.66, 98.34)** (63.35, 89.02)**
SD=standard deviation; MAGE=mean amplitude of glycemic
excursions. *difference from SIT (P < 0.05); **difference from SIT
(P < 0.001); Analysed using multi-level mixed models, controlling for
age and BMI. Data are mean (95% CI).
Supported By: National Research Foundation of Korea (NRF-2010-0009048);
National R&D Program for Cancer Control, Ministry of Health and Welfare, Republic of Korea (1120230)
56‑LB
Exercise Increases Insulin-induced Microvascular Recruitment in
the Myocardium during Nutrient Overload
ERIK M. VAN POELGEEST, ERIK H. SERNÉ, VICTOR W.M. VAN HINSBERGH, YVO
M. SMULDERS, FEMKE M.P. HOEVENAARS, ETTO C. ERINGA, Amsterdam, Netherlands
Supported By: National Health and Medical Research Council (1081734)
Impaired microvascular perfusion in muscle contributes to insulin resistance
and, in the heart, determines susceptibility to ischemia. In healthy individuals, insulin is known to induce vasodilatation of arterioles which subsequently
leads to an increase in muscle microvascular perfusion. This response is impaired in obese individuals, and may be improved by exercise. We studied
whether exercise prevents insulin-induced microvascular recruitment in skeletal muscle and the heart during nutrient overload. During two weeks, C57Bl/6
mice were fed chow (control), a western diet, alone (WD) or combined with
treadmill running (WD+Ex). Microvascular perfusion was studied using contrast ultrasonography during a hyperinsulinemic euglycemic clamp. In mice fed
a normal diet insulin increased microvascular blood flow in skeletal muscle
(1.00+0.29 to 1.18+0.48, p<0.05) and myocardium (1.00+0.43 to 1.39+0.61,
p<0.05). Insulin enhanced blood volume and blood velocity in myocardium,
while increasing only blood volume in skeletal muscle. Western diet reduced
peripheral insulin sensitivity and exercise partially restored that reduction
(GIR in µm/kg/min: control: 85.24+-22.92; WD: 52.07+-26.94, p<0.05; WD+Ex:
65.83+-38.57, ns). Western diet impaired insulin-induced enhancement of myo­­
cardial blood volume, and exercise prevented this impairment (1.00+0.63 to
1.05+0.51, 1.03+0.36 to 1.21+0.46, p<0.05). In skeletal muscle western diet
impaired insulin-induced increase of blood flow, but this was not prevented by
exercise. Running distance correlated with blood volume during hyperinsulinemia in myocardium (r=0.51, p=0.05), but not in skeletal muscle. Exercise did not
increase muscle perfusion in mice fed a normal diet. In conclusion, exercise
prevents western diet-induced impairment of insulin-induced microvascular
perfusion in myocardium, but not in skeletal muscle. Our findings highlight a
protective effect of exercise in the coronary microcirculation.
54‑LB
Effect of a 12-Week Home-Based Exercise Intervention on Fasting
Insulin and Adipocytokine in Colorectal Cancer Survivors: A Ran‑
domized Controlled Trial
MI KYUNG LEE, JI-YOUNG KIM, DONG-IL KIM, DONG-WOO KANG, JI-HYE PARK,
KI-YONG AHN, NAM-KYU KIM, JUSTIN Y. JEON, Seoul, Republic of Korea
High circulating insulin levels are associated with an increased risk of recurrence and mortality in early colorectal cancer (CRC). We conducted a randomized controlled trial to determine the effect of a 12-week home-based
exercise program on fasting insulin, adipocytokines, and physical function
in stage II-III CRC survivors. One hundred and twenty-three stage II-III CRC
survivors were randomly assigned to either a home-based exercise (n=62) or
usual care (n=61) group for 12 weeks. The goal of the home-based exercise
program was to increase the levels of exercise to 18 metabolic equivalent
task hours per week. The primary outcome was fasting insulin levels and
secondary outcomes were adipocytokine levels and physical function, measured by 6 minute walk test. A total of 99 (80.5%) participants completed
the trial. Intention-to-treat analysis indicated that fasting insulin level was
significantly decreased by 1.0 µU/ml (-16.67%) in exercise group while no
change was observed in the control group (between group difference, mean
-0.9, 95% CI: -1.8 to -0.01, p=0.042). Further analysis showed that tumor
necrosis factor (TNF)-α level was significantly reduced in exercise group
compared with control group (between group difference, mean -0.5, 95%
CI: -0.9 to -0.1, p=0.029). Physical function and fitness level measured by
6-min walk test, chair to standing test, and push up test were significantly
improved in the exercise group compared with control group (p<0.05).
Home-based exercise program was effective in reducing fasting insulin,
TNF-α levels and improving physical function.
57‑LB
Supported By: National Research Foundation of Korea (NRF-2010-0009048);
National R&D program for Cancer Control, Ministry of Health and Welfare, Republic of Korea (1120230), Yonsei University Research Fund of 2014
Protective Association of Physical Activity with Sexual Dysfunc‑
tion in Men with 50 or More Years of Type 1 Diabetes
55‑LB
Sexual dysfunction (SD) has been recognized in those with diabetes as an early sign of impending cardiovascular disease (CVD), as progressive vascular disease should manifest earlier in penile microvasculature than in systemic conduit
vessels. However, few protective factors have been identified for either condition. Our previous analyses demonstrated physical activity (PA) protects against
CVD in men with 50 or more years of type 1 diabetes (Joslin 50-Year Medalists)
(Adjusted OR: 0.25, 95% CI: 0.12, 0.52). SD and PA were assessed by self-report
and validated by the International Index of Erectile Function and Paffenbarger
questionnaires, respectively. Males in this cohort (46%, n=442/968) had a mean
(standard deviation) age of 67.0 (7.9) y, BMI of 26.5 (3.9) kg/m2, total cholesterol
of 148.0 (30.7) mg/dL and HbA1c of 7.0 (0.9)%. SD prevalence was 69.4% and
was associated with elevated HbA1c (7.1 vs. 6.8%, p≤0.001), higher BMI (26.8
vs. 25.5 kg/m2, p≤0.001) and lower HDL (52.0 vs. 59.0 mg/dL, p≤0.001). SD was
not associated with diabetic nephropathy, retinopathy or neuropathy (p>0.05).
PA was reported by 83.1% of males, BMI (28.4 vs. 26.1 kg/m2, p≤0.001) was
significantly higher and HDL was lower (47.0 vs. 55.0 mg/dL, p≤0.001) in those re-
STEPHANIE D’EON, LIANE TINSLEY, STEPHANIE M. HASTINGS, DAVID POBER,
GEORGE L. KING, HILLARY A. KEENAN, Boston, MA
Associations between Adiponectin, Chemerin, Physical Fitness,
and Fasting Insulin level in Colorectal Cancer Patients
KI-YONG AHN, MI KYUNG LEE, DONG-IL KIM, JIHYE PARK, JIHEE MIN, HYUK IN
YANG, JUNGA LEE, MINSUK OH, NAM-KYU KIM, JUSTIN Y. JEON, Seoul, Republic of Korea
Since high levels of insulin and insulin resistance are associated with
colorectal cancer prognosis, it is important to identify factors contributing
to fasting insulin level in colorectal cancer patients. The purpose of the current study is to investigate the associations of adiponectin, chemerin, physical fitness, and fasting insulin level in colorectal cancer patients. A total
of 123 colorectal cancer patients who completed standard treatment were
recruited. Anthropometric parameters, physical fitness, fasting insulin level,
homeostasis model assessment of insulin resistance, lipid profiles, adiponectin, and chemerin levels were measured and analyzed. Low fit particiADA-Funded Research
For author disclosure information, see page LB98.
LB14
Surprisingly, the level of ISGU was maintained high in the exercised leg on day 2
and 5. Exercise resulted in marked dephosphorylation and activation of muscle
glycogen synthase (GS) on day 1. This enhanced effect of exercise on GS was
preserved the subsequent day. Hexokinase II, but not GLUT 4, protein content
was increased (~ + 30%) in the prior exercised muscle throughout the supercompensation regime. We hypothesize that the mechanism leading to muscle
supercompensation involves enhanced ISGU mediated by enhanced capacity for
glucose phosphorylation and glucose storage. The apparent glycogen independent regulation of these events is novel and questions current thoughts on the
regulatory role of glycogen in human muscle insulin action.
Supported By: National Institutes of Health; JDRF
58‑LB
Withdrawn
Nutrition—Clinical
60‑LB
Red Wine Polyphenols as Treatment for Obesity-associated Insulin
Resistance: A Randomized, Placebo-Controlled, Double-Blind Clini‑
cal Trial
JORN WOERDEMAN, RICK I. MEIJER, ETTO C. ERINGA, YVO M. SMULDERS,
ERIK H. SERNÉ, Amsterdam, Netherlands
Red wine consumption is associated with reduced incidence of type 2 diabetes. Preclinical studies suggest that polyphenols extracted from red wine
(RWPs) favorably affect insulin sensitivity. Controversy exists whether RWPs
exert beneficial effects in humans. This study was undertaken to investigate
whether RWPs improve insulin sensitivity and post-meal glycemia in obese
volunteers. Obese (BMI>30) volunteers were randomly allocated to RWPs
600mg/day (n=14) or matched placebo (n=15) in a double-blind fashion. Subjects were investigated at baseline and after 8 weeks supplementation. Insulin
sensitivity was the primary endpoint and measured using the hyperinsulinemic-euglycemic clamp, and expressed as M-value. To study whether insulin
sensitivity was also affected in a more physiological setting, all participants
underwent a mixed meal test to measure postprandial glucose, and lipid levels
(after 4 hours). Both groups were well matched and none of the volunteers
experienced side effects. No differences were observed in weight or body fat.
Red wine polyphenols elicited no significant changes in M-value, postprandial
glucose, or postprandial lipid levels. We conclude that eight weeks of RWPs
supplementation do not improve insulin sensitivity, postprandial glycemia or
lipid levels in obese mildly insulin resistant volunteers.
Table 1. Study Results (Change from Baseline).
RWP (mean±SD
or median [IQR])
Weight (kg)
0.4 ± 2.1
Body fat (%)
-0.1 ± 2.0
M-value (mg/kg/min)
0.4 ± 1.1
AUCglucose (mmol/L*4h)
10.2 ± 116.0
Total-cholesterol (mmol/L)
0.2 [0;0.4]
HDL-cholesterol (mmol/L)
-0.04 ± 0.17
LDL-cholesterol (mmol/L)
0.2 [-0.3;0.3]
Triglycerides (mmol/L)
0.2 ± 0.8
Placebo (mean±SD p-value
or median [IQR])
0.2 ± 2.6
0.88
1.3 ± 2.4
0.13
0.3 ± 1.5
0.65
-0.9 ± 88.7
0.99
-0.1 [-0.5;0.4]
0.33
-0.03 ± 0.11
0.65
-0.3 [-0.4;0.3]
0.50
0.1 ± 0.5
0.12
Supported By: Dutch Heart Foundation (2010T041)
61‑LB
Is Exposure to Famine in Childhood and Economic Development
in Adulthood Associated with Diabetes? Two-Hit Hypothesis from
Spect-China Study
59‑LB
NINGJIAN WANG, XIAOJIN WANG, BING HAN, QIN LI, YI CHEN, CHUNFANG
ZHU, YINGCHAO CHEN, FANGZHEN XIA, XIAOQI PU, ZHEN CANG, CHAOXIA ZHU,
MENG LU, YING MENG, HUI GUO, CHI CHEN, DONGPING LIN, WEIPING TU, BIN
LI, LING HU, BINGSHUN WANG, MICHAEL D. JENSEN, YINGLI LU, Shanghai,
China, Zhejiang, China, Nanchang, China, Rochester, MN
Molecular Signaling and Insulin Sensitivity of Human Skeletal Mus‑
cle during Glycogen Supercompensation
JANNE R. HINGST, MADS BAU HANSEN, ANDERS GUDIKSEN, JESPER
BIRK, HENRIETTE PILEGAARD, BENTE KIENS, ERIK A. RICHTER, JØRGEN F.P.
WOJTASZEWSKI, Copenhagen, Denmark
Background: The middle-aged and elderly Chinese experienced severe famine between 1959 and 1962 and subsequent rapid economic development
from 1978 to now. Now diabetes has attained epidemic proportions in China.
Objective: We hypothesized that exposure to malnutrition at early age and
economic development in adulthood might increase diabetes risk.
Design: We analyzed the association of exposure to famine at different age
stages and economic development with risk of diabetes in adulthood. Our data
of 6897 adults was from population-based SPECT-China study in 2014. Among
them, 3844 adults were exposed to famine when they were between -4 (fetus)
and 37 years old and lived in areas with different economic development levels
in adulthood. Diabetes was defined as previous diagnosis by health care professionals, fasting plasma glucose ≥7.0mmol/L and/or HbA1c ≥6.5%.
The phenomenon of glycogen supercompensation after exercise is not
mechanistically understood. To investigate this, nine healthy male subjects were
studied 3 times during 5 days following knee-extensor exercise of one leg while
the other leg served as resting control. Insulin action was evaluated in each leg
by euglycemic hyperinsulinemic clamps and leg catherization on day 1 (4 h post
exercise), day 2 and day 5 (28 and 100 h post exercise, respectively) while the
subjects consumed an isocaloric carbohydrate rich diet (80% CHO) between
clamps. In the prior exercised leg glycogen content was decreased (65%, day
1), normalized (day 2) and supercompensated (+ 30%, day 5) compared to the
rested leg. Insulin stimulated glucose uptake (ISGU) was markedly (~+ 40%) increased in the exercise leg 4 h after exercise (day 1) compared to the rested leg.
ADA-Funded Research
For author disclosure information, see page LB98.
LB15
POSTERS
porting PA. Total Testosterone, sex hormone binding globulin, C-Reactive Protein
levels, as well as antilipidemic use, HbA1c and hypertension prevalence did not
differ between PA groups (p>0.05). In an unadjusted model, those who reported
being physically active were 2 times less likely to report SD (OR: 0.48, 95% CI:
0.26, 0.90). This relationship persisted with adjustment for age and CVD factors
(Adjusted OR: 0.50 (0.26, 0.96)). This analysis demonstrates a strong, protective
association of PA with SD, independent of CVD and metabolic risk factors in men
with long duration of type 1 diabetes.
Behavioral Medicine, Clinical
Nutrition, Education, and Exercise
Nutrition—Clinical
POSTERS
Behavioral Medicine, Clinical
Nutrition, Education, and Exercise
Psychosocial, Behavioral Medicine
Psychosocial, Behavioral Medicine
Results: Compared with non-exposed subjects, famine exposure during
fetal development (age -1~-4, OR 1.53, 95% CI 1.09-2.14) and childhood (age
0~9, OR 1.82, 95% CI 1.21-2.73) was associated with an increased diabetes risk after adjustment for age and sex. Further adjustment for adiposity,
insulin resistance, lipid profile and blood pressure did not attenuate this association. Living in rural area (severely affected famine area) and under high
economic status, subjects had higher diabetes risk in adulthood (OR 1.22,
95% CI 1.02-1.46 and OR 1.46, 95% CI 1.20-1.78, respectively). No interaction
was found between age classification and economic development status.
Conclusions: The rapid increase in diabetes prevalence in middle-aged
and elderly people in China may be due to the combination of severe malnutrition during fetus and childhood (age 0~9) (the first hit) and high economic
development level in adulthood (second hit). Avoiding central obesity could
overcome the second hit. Our findings are in line with the two-hit hypothesis
of diabetes etiology.
63‑LB
Physician–Patient Communication at Prescription of an Additional
Oral Agent for Type 2 Diabetes (T2D): Link Between Key Conversa‑
tion Elements, Physician Empathy, and Patient Outcomes—Insights
from the Global IntroDia™ Study
MATTHEW CAPEHORN, ANNE BELTON, SUSAN DOWN, AUS ALZAID, VICTORIA
GAMERMAN, FRIEDERIKE NAGEL, JISOO LEE, STEVEN EDELMAN, WILLIAM H.
POLONSKY, Rotherham, United Kingdom, Toronto, ON, Canada, Bridgwater, United
Kingdom, Riyadh, Saudi Arabia, Ridgefield, CT, Ingelheim, Germany, San Diego, CA
IntroDia™ is investigating physician-patient communication during the
early treatment of T2D and how such conversations may be linked to critical
patient outcomes. Here we investigate patient experiences of the “add-on”
moment, i.e. the consultation when, typically months or years after the T2D
diagnosis, another oral agent is first prescribed, and how this conversation
is associated with patient self-care and quality of life outcomes. A total of
4235 patients from 26 countries (52% male, median age 46 years) completed
a self-report survey examining the content of the conversation with their
physicians at add-on (via a 24-item scale of conversation elements specific
for add-on). Perceived physician empathy (PPE) was measured with CAHPS,
TIPS and IPC items. Current psychosocial status (WHO-5, DDS) and self-care
behavior (SDSCA) were also evaluated. Three key elements of the physician-patient conversation were identified by factor analysis - Collaborative
(e.g. “Encouraged me to ask him/her questions”), Encouraging (e.g. “Told me
that the new medication would improve my quality of life”) and Discouraging (e.g. “Told me that my diabetes was getting worse”). PPE was positively
associated with Collaborative (β=1.16, p < 0.001) and Encouraging (β=1.39,
p < 0.001) and negatively linked with Discouraging (β=-0.92, p < 0.001).
Further, PPE was associated with less diabetes distress (DDS: β=-0.39,
p < 0.001), greater well-being (WHO-5: β=0.54, p < 0.001) and better self-care
(SDSCA - exercise: β=0.56, p < 0.001; diet: β=0.94, p < 0.001; medication taking: β=0.76, p < 0.001). Thus, physician use of collaborative/encouraging conversation elements when prescribing an additional oral agent may enhance
communication with T2D patients and lead to better self-care and quality of
life. Conversely, discouraging elements may have the opposite effect.
Supported By: National Natural Science Foundation of China (81270885,
81070677); Clinical Potential Subject Construction of Shanghai Jiaotong University School of Medicine (2014); Ministry of Science and Technology in China
(2012CB524906); Science and Technology Commission of Shanghai Municipality
(14495810700); Fund for Outstanding Academic Leaders in Shanghai (12XD1403100)
62‑LB
Eugenia Dysenterica DC (Brazilian Fruit) Juices Reduce Postpran‑
dial Glucose and Insulin Plasma Concentrations
RENATA ARAUJO, ROSA FERREIRA SANTOS, LUCIANO GIACAGLIA, MARIA ELIZABETH ROSSI SILVIA, MARIA INES GENOVESE, São Paulo, Brazil
Eugenia dysenterica DC (EDDC) is a Brazilian fruit rich in polyphenols, and
previous study have shown its action on carbohydrate metabolism. This study
evaluated the effect of EDDC juices without fiber (clarified C) and with fiber (nonclarified NC) on postprandial glycaemia and insulinemia, in patients with glucose
intolerance (GI). Fourteen patients (male/female: 2/12); age ( 46 ± 8) years, were
conducted to three meal tests of 30 g of carbohydrate plus 300 mL water (Test
1), or 300 mL of C- EDDC juice (Test 2), or 300 mL of NC- EDDC juice (Test 3),
after 8 hours fasting, 7 days interval between them. Blood glucose and insulin
were measured at 0, 30, 60, 90, and 120 min for glucose and insulin, and at 0 and
120 min for Ferric reducing antioxidant power (FRAP). Data (mean ± SEM) were
analyzed by ANOVA and Friedman, p ≤0.05. The results showed that AUC were
lower in C and NC-EDDC Juices for glucose (14935 ± 1604 x 12968 ± 1237 x 12291
± 979 mg/dL/min, p ≤ 0.0001) and insulin: (6049 ± 3617 x 3710 ± 1757 x 3331 ±
1337 µU/ml/min, p ≤ 0.0013. The insulin secretion index (ΔIns0-120/Δgluc0-120)
decreased with both EDDC juices: (0.3972 ± 0.2156 x 0.2859 ± 0.1323 x 0.2692 ±
0.1020 p < 0.0035). Also, both EDDC juices increased plasma antioxidant capacity (FRAP) p < 0.05. In conclusion, C and NC-EDDC juices decreased significantly
post prandial glucose and insulin secretion index during meal tests.
Supported By: Boehringer Ingelheim/Eli Lilly and Company
64‑LB
Development and Validation of an Instrument to Measure Collabora‑
tive Goal Setting in the Care of Patients with Diabetes
HEATHER L. MORRIS, LEVENT DUMENCI, JENNIFER ELSTON LAFATA, Gainesville, FL, Richmond, VA
Despite known benefits of patient-perceived collaborative goal setting, we
have limited ability to monitor this process in practice. We developed the Patient Measure of Collaborative Goal Setting (PM-CGS) to evaluate the use of
collaborative goal setting from the patient’s perspective. A random sample of
400 patients aged 40 years or older, receiving diabetes care from the Virginia
Commonwealth University Health System between 8/2012 - 8/2013 were
mailed a survey containing potential PM-CGS items (n=41) as well as measures of patient demographics, self-efficacy, trust in their physician, and selfmanagement behaviors. Confirmatory factor analysis was used to evaluate
instrument construct validity. External validity was evaluated via a structural
equation model (SEM) that tested the association of the PM-CGS with selfmanagement behaviors. The direct and two mediated (via trust and self efficacy) pathways were tested. A total of 259 patients responded to the survey
(64% response rate), of whom 192 were eligible for inclusion. Results from
the factor analysis supported a 37-item measure of patient-perceived collaborative goal setting spanning five domains: listen and learn; share ideas;
caring relationship; measurable objective and goal achievement support (χ =
4366.13, p<.001; RMSEA = .08). Results from the SEM confirmed a relationship between the collaborative goal setting measure and self-management
(p<.001), which was partially mediated by self-efficacy (p<.05). Collaborative
goal setting can be validly measured by the 37-item PM-CGS. Use of the PMCGS can help illustrate actionable deficits in goal setting discussions.
Supported By: National Institutes of Health (1R36HS022202-01)
65‑LB
Glucose Variations Are Strongly Coupled to Sleep Disruption in
Young Adults with Type 1 Diabetes (T1DM)
SARAH S. FARABI, DAVID W. CARLEY, LAURETTA T. QUINN, Chicago, IL
Sleep quality is reduced in individuals with T1DM, which may negatively
impact ongoing disease management. Glucose variability has been postulated to impair sleep continuity in individuals with T1DM, but this has not
Supported By: CAPES; FAPESP
ADA-Funded Research
For author disclosure information, see page LB98.
LB16
Clinical Therapeutics/New Technology—Glucose Monitoring and Sensing
Supported By: National Diabetes Services Scheme; Sanofi Aventis; National
Health and Medical Research Council (1072987 to E.K.F.); National Health and
Medical Research Council (1061801 to G.R.); Centre for Eye Research
68‑LB
Smartphone Skills Enhances Cognitive Behavioral Therapy (CBT)
Intervention Addressing Adherence and Distress with Type 2 Dia‑
betes (T2D)
Supported By: American Association of Diabetes Educators
66‑LB
JUDITH A. CALLAN, GREG J. SIEGLE, LINDA SIMINERIO, KATHLEEN M. MCTIGUE,
SUSAN M. SEREIKA, Pittsburgh, PA
“It Is Definitely a Game Changer”: Closed Loop Technology in the
Home Experienced by Adults with Type 1 Diabetes
Non-adherence and distress are associated with poor clinical outcomes in
T2D. To modify negative adherence appraisals, a pilot feasibility study was
conducted using a 30-minute phone CBT intervention with a skills practice
smartphone application (app) for T2D (6 vs. 8 vs. 12 sessions or usual treatment). Outcomes included: medication adherence (measured via MEMs cap
and Morisky self-report), diabetes distress and HbA1c levels. The sample
included 12 subjects taking oral diabetes medication, aged 30 to 65 years,
HbA1c of > 8, with self-management and distress issues. Subjects were randomly assigned to equal groups of the 3 intervention conditions or usual
care. Outcome measures were collected at baseline and post-intervention.
At fourteen weeks, all subjects had a follow-up HbA1c. Subjects also documented feasibility, ease of learning, T2D-relevance, and desire to use the
app via ratings from 1 (very favorable) to 7 (very unfavorable).
CHRISTEL HENDRIECKX, JANE SPEIGHT, LUCINDA A. POOLE, AMIN SHARIFI,
MARGARET LOH, JODIE C. HORSBURGH, STEVE TRAWLEY, ALICIA J. JENKINS,
KAVITA KUMARESWARAN, RICHARD J. MACISAAC, GLENN M. WARD, PETER
COLMAN, LEON A. BACH, ANDREW KYOONG, NATALIE KURTZ, BENYAMIN
GROS­­MAN, ANIRBAN ROY, DAVID O’NEAL, Melbourne, Australia, Fitzroy, Australia, Northridge, CA
This qualitative study explored participants’ experiences after four nights
Home Closed Loop (CL) Insulin Delivery System use vs. Sensor Augmented Pump
Therapy with Low-Glucose Suspend (SAPT-LGS) in a randomised cross-over trial.
Ten adults (≥18 years) completed the trial between April 2014 and March 2015;
median age 37.5 years (range 32-62) and diabetes duration 31 years (range 8-36);
five were women. Semi-structured interviews were conducted on day five, after
four consecutive nights of CL at home. Interviews were audio-recorded, with
transcriptions imported into NVivo 10 for thematic analysis. A coding framework was developed to identify the main themes and subthemes. When asked
about the four nights’ CL experience, the most common observation was the
“flat-line,” showing stable overnight glucose levels. Although most reported
technical glitches during one or more nights, few safety concerns were raised. If
any, these related to feeling unsure whether the system would respond in time
to falling glucose. However, confidence increased when they observed how the
CL stopped insulin delivery when their glucose was trending down, how (when
switching to CL at night) the CL dealt with high glucose levels. Compared with
their current insulin pumps (and, for some, sensors), participants reported the
following benefits: less decision making, resulting in few human errors; fewer
alarms, as the CL kept glucose levels within target overnight; not having to
cope with the consequences of hypo- and hyperglycaemia (e.g. feeling sick post
event), due to less glucose variability. Participants found the CL was easy to use,
but they mentioned that this might be different for people who are less “tech
savvy.” In conclusion, participants gave a very positive evaluation of CL in the
home. They were impressed with how well the CL system responded to their
glucose levels and noted that further improvements of the technology will enhance the user’s experiences.
Table. Post-Intervention Clinical Outcomes.
CBT
HbA1c
MEM Doses
Diabetes
Duration Total
HbA1c
Adherence (Morisky5-item) Distress
(weeks) (Change) (% Change)
(%)
(% Change) (% Change)
6
-0.6o
-6.62
37.73
88.89
-17.98
8
-2.3o
-20.46
35.73
26.67
-8.33
12
-2.33
-22.34
88.69
46.67
-40.92
Usual Tx -2.15
-20.46
84.06
6.25
-36.22
Mean feasibility rating was 1.84+0.64. Subjects used the app regularly,
with mean daily actions of 33.27+19.73. Overall app rating was 3.00+2.07,
indicating they found the app highly usable. The data demonstrates feasibility and usability. All intervention subjects had improved adherence, reduced
distress, and reduced HbA1c. Usual Tx subjects had higher than usual motivation to improve clinical status.
Supported By: 8KL2TR00014608
Clinical Therapeutics/New Technology—
Glucose Monitoring and Sensing
Supported By: JDRF
67‑LB
69‑LB
What Is the Best Measure for Assessing Diabetes Distress? A Ra‑
sch Analysis Comparing the Problem Areas in Diabetes and Diabe‑
tes Distress Scale: Results from Diabetes MILES—Australia
Lanthionine Synthetase C-like Receptor 2 (LANCL2): A Novel Thera‑
peutic Target for Type 2 Diabetes
ADRIA CARBO, RAQUEL HONTECILLAS, JULIAN COOPER, RICHARD GANDOUR,
PATRICK HEIZER, MARION EHRICH, JOSEP BASSAGANYA-RIERA, Blacksburg, VA
EVA K. FENWICK, GWYN REES, ELIZABETH HOLMES-TRUSCOTT, JESSICA L.
BROWNE, FRANS POUWER, JANE SPEIGHT, East Melbourne, Australia, Melbourne, Australia, Tilburg, Netherlands
There is an urgent need for developing type 2 diabetes (T2D) drugs that
are more effective and safer than existing medications. Lanthionine Synthetase C-like Receptor 2 (LANCL2) is a novel T2D therapeutic target that
exerts potent anti-inflammatory and anti-diabetic effects. We generated
libraries of derivatives and analogs of parent LANCL2-binding compounds
61610 belonging to the class of bis (benzimidazoyl) terephthalanilides (BTTs),
and identified BT-11 as our top lead compound. Molecular modeling studies
The aim of this study was to compare the psychometric properties of the
Problem Areas In Diabetes (PAID) scale and the Diabetes Distress Scale (DDS)
to determine the optimal tool for measuring diabetes distress. A total of 3,338
adults with diabetes participated in the Diabetes MILES - Australia study, and
completed the PAID (N=1,609: n=675 type 1 diabetes; n=934 type 2 diabetes)
ADA-Funded Research
For author disclosure information, see page LB98.
LB17
POSTERS
or the DDS (N=1,705: n=693 type 1 diabetes; n=1,012 type 2 diabetes). Rasch
analysis was used to explore key parameters, namely category threshold ordering, precision, unidimensionality, item and person “fit,” targeting, and differential item functioning. In the type 2 diabetes sample, the PAID total scale
had satisfactory psychometric properties, which were optimized by the deletion of responses from persons with extreme minimum scores and ‘“misfit”
(9% and 12%, respectively), and the exclusion of item 15. However, the DDS
total scale had disordered thresholds, multidimensionality, and person misfit,
which could not be remedied by removing misfitting items or extreme scores.
All four DDS subscales failed initially to reach adequate precision; only the
Emotional burden and Regimen-related distress subscales achieved adequate
precision following removal of a substantial proportion of the sample (25%
and 11%, respectively) due to floor effects or misfit. Psychometric concerns
were similar but less marked in the type 1 diabetes sample. In conclusion,
the DDS requires substantial revisions to resolve multidimensionality and item
misfit within the total scale, and poor precision in its subscales. The results of
the present psychometric study support use of the PAID to measure diabetes
distress.
Clinical Diabetes/
Therapeutics
been systematically investigated. Actigraphy is a validated quantitative tool
used to assess sleep disruption that rarely has been used in individuals with
T1DM. Here, we employed actigraphy and continuous glucose monitoring
(CGM) to define the coupling between variations in glucose and sleep disruption in young adults with T1DM. 21 participants with T1DM (8 males),
aged 18-30, wore a CGM system and a wrist actigraph for an 8-hour overnight period. The cross correlation function was used to objectively quantify coupling between glucose and activity and to estimate the global delay
between these processes. Because this coupling is/may be both frequency
dependent and time varying, wavelet coherence analysis was employed to
capture these dynamics. The greatest mean cross-correlation (r2) was 0.44 ±
0.03 (p < 0.00005) with zero lag between glucose and activity. Mean coherence (C) was greatest for the fluctuations with periods of 10 to 20 min (0.39 ±
0.016, p < 0.00005) with very high coherence (VHC; C > 0.7,) observed for 16.2
± 3.5% of recording time (VHC%). Furthermore, hemoglobin A1c and mean
overnight glucose were negatively associated with VHC% (r = -0.45, p =0.04
for each). Among our subjects with T1DM, glucose variations accounted for
nearly half of the variance in sleep disruption measured by overnight activity, with increasing glucose aligned with increasing activity. Moreover, this
coupling was consistently strongest for rapid fluctuations and the presence
of very high coherence between glucose and activity was negatively associated with A1c and overnight mean glucose. This suggests an important
physiologic connection between glucose homeostasis and sleep continuity,
which may be weakened by poor glucose control.
Clinical Therapeutics/New Technology—Glucose Monitoring and Sensing
were used to predict LANCL2 binding and predictions were validated experimentally by Surface Plasmon Resonance (SPR) data, demonstrating that 3
top leads, strongly bind to LANCL2. Our pre-clinical efficacy studies in db/db
and diet-induced obesity (DIO) mice showed that daily oral administration
of BT-11 significantly reduces fasting blood glucose and improves glucose
normalization during a glucose tolerance test. Oral BT-11 administration significantly decreased the infiltration of macrophages and pro-inflammatory
Ly6chigh GR1+ granulocytes as well as decreasing the expression of TNFalpha and MCP1 in white adipose tissue. To assess the safety profile of
BT-11, we performed a single high-dose and a 14-day repeated daily dose
studies in rats, both of which confirmed the excellent initial safety profile of
BT-11. Rats treated with BT-11 orally during a 14-day period showed no differences in Functional Observational Battery endpoints, clinical pathology,
and histopathological examination in 15 tissues. In sum, BT-11 is a promising
LANCL2-binding anti-inflammatory and anti-diabetic drug efficacious and
safe for treating T2D.
of the time while at home use subjects demonstrated a frequency of 12.2%
for the same error threshold. The lack of variance in home use suggests that
subjects may be entering the same BG value twice when calibration. Patient SMBG testing demonstrates significantly more variability at home than
when conducted in the optimized clinical environment highlighting a lack
of precision of SMBG during actual use. Because replicate measurements
are only obtained at initial calibration, it is unknown if the observed SMBG
imprecision affects patient perception of SMBG accuracy.
Comparative Accuracy of 17 Glucometers
LAYA EKHLASPOUR, MANASI SINHA, DEBBIE MONDESIR, NORMAN LAUTSCH,
COURTNEY BALLIRO, MALLORY HILLARD, KENDRA MAGYAR, STEVEN J. RUSSELL, Boston, MA, Cambridge, MA
The accuracy of blood glucose (BG) meters is important for the detection
of dysglycemia and for calculation of insulin doses. The safety and effectiveness of automated glucose management with a bionic pancreas is also
dependent on accurate BG measurements for calibration of the continuous
glucose monitor. To evaluate the comparative accuracy of commercially
available glucometers across a wide range of reference BG and hemoglobin
values. Fresh, discarded blood samples from a hospital STAT laboratory were
spiked with a glucose solution or incubated them at 37 C to produce 351
samples with an even distribution across reference BG levels from 20 - 440
mg/dl and hemoglobin values from 9-16 g/dl. We measured the BG of each
sample with 17 different available glucometers and the reference method
(YSI 2300) at the same time. Reference whole blood measurements were
converted to plasma glucose values. We determined the mean absolute relative difference (MARD) for each glucometer and determined whether they
met ISO 2003 and 2013 criteria for accuracy. Seven meters met ISO 2003
criteria for accuracy but only 2 met ISO 2013 criteria. All meters meeting
ISO 2003 criteria had a MARD <10% and all utilize glucose dehydrogenase
chemistry. Accuracy did not differ markedly with blood hemoglobin level.
There was no correlation between accuracy and strip cost. The accuracy
of commercially available glucometers varies widely. Most of the meters
tested did not meet current accuracy criteria.
70‑LB
Patient Home Experiences Using the OneTouch Reveal® Web Ap‑
plication with the OneTouch Verio® Glucose Meter Demonstrates
Improved Glycemic Control
POSTERS
Clinical Diabetes/
Therapeutics
72‑LB
MIKE GRADY, GRAHAM WARREN, LAURENCE B. KATZ, BRIAN L. LEVY, Inverness,
United Kingdom, West Chester, PA
Cloud-connected diabetes applications enable health care professionals (HCPs) to monitor patient progress in real time and offer remote consultations. OneTouch Reveal® (OTR) is a cloud-based web application that
aggregates data from a patient’s blood glucose (BG) meter and/or insulin
pump. OTR tracks, analyzes and interprets patient blood glucose and insulin
data to help patients and HCPs make more informed treatment and lifestyle
decisions. This study assessed the experience of patients using OTR in
conjunction with the OneTouch Verio® (OTV) meter. 40 subjects with type
1 (23 T1DM) or type 2 diabetes mellitus (17 T2DM) uploaded BG meter results every 2 weeks to the OTR web application on their home computer for
12 weeks. At baseline, HCPs customized individual target BG ranges. HCPs
remotely reviewed progress using OTR and delivered telephone consultations at 4 and 8 weeks based on OTR insights. After 12 weeks, mean A1c
decreased from 8.3% to 7.9% (SD=0.725, p=0.001 paired t-test) with 25% of
subjects having an A1c reduction of ≥1.0%. In subjects with T2DM, mean BG
decreased from 175 to 161 mg/dl (p< 0.001), and the percentage of aboverange BG results decreased from 33.0% to 23.9% (p=0.002), whilst in-range
BG results increased from 65.5% to 75.0% (p=0.001). During phone consultations, 80% of subjects confirmed OTR detected out-of-range glucose
patterns, and 84% of these subjects were able to correct the underlying
pattern to get BG back in-range. 82.5% of subjects agreed OTR helped them
“see the big picture and motivated them to stick to their plan,” and 92.5%
agreed the OTV meter “made it clear when to take action.” In summary, OTR
in combination with the OTV meter enabled subjects with T1DM and T2DM
to effectively manage their diabetes and improve BG control over 12 weeks.
Real-time visibility to subject data enabled HCPs to deliver focused and effective remote consultations.
71‑LB
Imprecision of SMBG Values Used for CGM Calibration during Opti‑
mal Conditions or Home Use
ARTURO GARCIA, TOMAS WALKER, DAVID A. PRICE, San Diego, CA
As real-time continuous glucose monitoring (CGM) requires twice daily
calibrations with self-monitored blood glucose (SMBG) values patients are
repeatedly reminded of differences between the CGM and the SMBG. The
frequent comparison may impact the perception of CGM accuracy. In contrast, patients relying on SMBG rarely perform a direct comparison between
meters or sequential SMBG measurements. Initial calibration of the Dexcom
CGM, requires patients to enter 2 SMBG values, obtained from separate
fingersticks. We compared differences between the two initial calibration
SMBG values performed during clinic sessions (subjects washed their hands,
were instructed on proper blood application, and used fresh strips) and during home use. Clinic session data came from three clinical studies, 2 adult
studies with 69 subjects (n=62 T1D, n=7 T2D) and 1 pediatric study with
24 subjects (n=24 T1D). The home use data was derived Dexcom technical
support data. A total of 1126 fingerstick pairs were evaluated. The SMBG
imprecision was measured by calculating an absolute proportional error if
both SMBG values ≥ 100 mg/dl and an absolute difference error for SMBG <
100 mg/dl. The subjects in the clinical study demonstrated errors > 10%/10
mg/dl and > 20%/20 mg/dl 7.6% and 3.3% respectively; home use subjects
demonstrated a > 10%/10 mg/dl and > 20%/20 mg/dl of 17.6% and 3.6%
respectively. Clinical study subjects demonstrated 0%/0 mg/dl error 2.2%
73‑LB
Pressure-induced Sensor Attenuation Testing on a Fully Implant‑
able Continuous Glucose Monitoring System
ANDREW D. DEHENNIS, XIAOLIN WANG, SORIN IOACARA, Germantown, MD,
Bucharest, Romania
This abstract presents the results of clinical testing on a Continuous Glucose Monitoring (CGM) based on an implantable sensor to assess its susceptibility to Pressure Induced Sensor Attenuation (PISA). The system under
evaluation is composed of a long term, subcutaneously inserted sensor, a
smart wearable transmitter, and a Mobile Medical App. Although previous
reports on transcutaneous devices has shown the need to develop PISA detection capability into the CGM system, a system that is not susceptible to
PISA will not need an algorithm to detect PISA or cause pump shut-offs due
to PISA. In this study, 20 subjects with type 1 diabetes (T1DM) with mean
age 37±8 years, mean disease duration 11±6 years were implanted with the
investigational continuous glucose sensor in the upper arm for up to 90 days.
During the clinical session, which as 30 days after sensor insertion for 7
subjects and 90 days after sensor insertion for 13 subjects, pressure was
applied to the area above the implanted sensors for about 30 minutes, and
ADA-Funded Research
For author disclosure information, see page LB98.
LB18
Clinical Therapeutics/New Technology—Glucose Monitoring and Sensing
74‑LB
Frequent, Persistent CGM Use May Reduce Hypoglycemia Fear
among Individuals Treated with Intensive Insulin Regimens
JAMES J. CHAMBERLAIN, EMILY GILGEN, DANA DOPITA, Salt Lake City, UT
Fear of hypoglycemia remains a significant obstacle to achieving and
maintaining optimal glycemic control. The impact of continuous glucose
monitoring (CGM) use on hypoglycemia fear has not been well studied.
We conducted a survey to assess the concerns of individuals about hypoglycemia after one year of CGM use. This single-center study included 74
individuals treated with intensive insulin therapy: average age 42.9 years
(range: 23-71 years); 49% male; 76.6% 10-25+ years diabetes duration;
79.7% insulin pump use. Participation was restricted to individuals who used
the Dexcom G4 device to avoid confounding responses due to differences
between various CGM systems. Respondents completed a 16-item survey,
which queried them about their frequency of CGM use and primary reasons
for persistence of use. Among the 74 respondents, 58 (78.3%) reported CGM
use on most days. A notable number of these respondents (n=45, 77.6%)
reported worrying about hypoglycemia “most of the time” (n=20, 34.5%) or
“frequently” (n=25, 43.1%) prior to CGM use. After one year, no respondents
reported worrying about hypoglycemia “most of the time” and one (1.7%)
reported frequent worry, a 97.8% decrease (Figure 1). Our findings show that
frequent, persistent use of CGM reduced hypoglycemia fear among survey
respondents.
76‑LB
Continuous Glucose Monitoring at the Site of Subcutaneous (SC)
Insulin Delivery: Building a Durable Sensing Catheter
W. KENNETH WARD, SHEILA BENWARE, MATTHEW BREEN, TYLER MILHEM,
KRISTIN MORRIS, CHAD KNUTSEN, KAMESH MULLAPUDI, JOHN CONLEY, ROBERT S. CARGILL, Portland, OR, Corvallis, OR
New evidence suggests that CGM can be carried out in proximity to insulin delivery. One method of creating a combined sensing + insulin delivery device is to place thin metal electrode films on a polymer substrate that forms
the catheter wall. However, these films may not be durable. We hypothesized that depositing the thin metal films on a substantial metal foil would
increase durability. We evaluated 2 constructions of sensing catheters, each
of which were indwelled in pigs x 24 h: GEN 1: Thin metal films of Pt and Ag
deposited on a polymer. GEN 2: Thin metal films of Pt and Ag deposited over
a 12 µm thick titanium foil. We also evaluated 2 tube architectures: GEN 1:
a sharp steel needle. GEN 2: a blunt steel tube with retractable insertion
stylet. In the pigs, after a period of equilibration, high rate aspart insulin was
delivered continuously for 4 h at a rate of 0.02 u/kg/h SC. In control tubes, no
insulin was given. After explant, 3 observers graded electrode integrity and
tissue trauma using photomicrographs. Indicating electrode integrity was
greater in titanium foil devices than in thin film devices (95% +/- 3 (n=46)
vs. 76% +/- 4 (n=15), p < 0.001). Similar results were found in reference electrodes (90% +/- 4 (n=43) vs. 81% +/- 2 (n=14), p < 0.05). Mean tissue trauma
score for the blunt tubes was one-fifth that of the sharp needle. There was
no clear time-related decline of the glucose signal from the sensing tubes
through which insulin was delivered. There was a trend for sensed glucose
levels to be slightly (10-20%) lower in insulin tubes (n=19) vs. non-insulin
tubes (n=22). A base layer of titanium foil improved electrode durability in
glucose sensing tubes. Use of a retractable stylet within a blunt tube led to
a much lower mean tissue trauma score than a sharp needle. The delivery
of high basal rates of insulin via the tubes led to relatively small declines of
local glucose levels. We conclude that continuous measurement of glucose
in close proximity to the site of insulin delivery is feasible.
75‑LB
Supported By: National Institute of Diabetes and Digestive and Kidney Diseases; The Leona M. and Harry B. Helmsley Charitable Trust
Frequent CGM Use May Reduce Daily Blood Glucose Testing Fre‑
quency and Emergency Hospitalizations/Paramedic Visits
EMILY GILGEN, DANA DOPITA, JAMES J. CHAMBERLAIN, Salt Lake City, UT
Continuous glucose monitoring (CGM) is indicated as an adjunct to selfmonitoring of blood glucose (SMBG). The impact of CGM use on daily SMBG
habits has not been well studied. We assessed changes in SMBG frequency
and emergency hospitalizations/paramedic visits in individuals who frequently and persistently use CGM. This single-center study included 74
ADA-Funded Research
For author disclosure information, see page LB98.
LB19
POSTERS
individuals treated with intensive insulin therapy: average age 42.9 years
(range: 23-71 years); 49% male; 76.6% 10-25+ years diabetes duration;
79.7% insulin pump use. Participation was restricted to individuals who used
the Dexcom G4 device to avoid confounding responses due to differences
between various CGM systems. Respondents completed a 16-item survey,
which queried them about their frequency of CGM use and primary reasons
for persistence of use. Among the 74 respondents, 58 (78.3%) reported CGM
use on most days. A 50.0% reduction in average number of daily blood glucose tests was reported after 1 year of CGM use vs. prior to use. (Figure 1A).
An 85.7% reduction in the number of emergency hospitalization/paramedic
visits after 1 year of CGM use vs. prior to use was reported. (Figure 1B). Frequent, persistent CGM use was associated with notable reductions in daily
SMBG frequency and emergency hospitalizations. Reductions in emergency
hospitalizations and SMBG utilization may offset the cost of CGM without
jeopardizing patient safety.
Clinical Diabetes/
Therapeutics
upon interviewing, the subjects felt the pressure was significant. The data
analysis calculated the rate of change during the pressure tests of all the
participating subjects to detect any PISA and all the glucose rates of change
were within physiological limits, no rate of change below -4 mg/dL/minute
was seen. The summary of rate of change during the pressure test is shown
in Table 1.
Clinical Therapeutics/New Technology—Glucose Monitoring and Sensing
77‑LB
member and clinicians using pre- and post-surveys. Two sites participated
in Time in Motion (TIM) and work flow mapping; to ensure that the AGP process was an enhancement to clinical care. Both clinics had patient download
self-serve kiosks in their lobbies during this study. Patients entered minimal
data and connected the device(s) for download. Download software sent
data to the AGP cloud, clinic staff logged onto the AGP system and printed
the report. The average patient time to download from sitting down at the
computer to a complete download has historically been 4 minutes, 54 seconds. The average time to print a report by the staff is 4 minutes, 45 seconds
including time to log onto the AGP site and collect the report from the printer.
The staff time for the prior work flows was 8 minutes, 15 seconds (site 1) and
20 minutes (site 2). The AGP process saved on average 3.5 to 15 minutes per
patient. Therefore, with practices seeing on average 20 patients per clinician per day; a time savings of 3 minutes result in a per day time savings of 1
hour staff time per clinician. Clinics with 4 clinicians could expect to save 0.5
FTE medical assistant (avg. salary $30,000/yr.) by implementing a standardized AGP download. Additional time saved in the clinical encounter since
standardized AGP reporting may facilitate efficient shared decision making.
Performance of Dario Blood Glucose Monitoring System Evaluated
in a Clinical Study in Compliance with the New ISO 15197:2013 Stan‑
dard
POSTERS
Clinical Diabetes/
Therapeutics
BILLY PERY, PAUL M. ROSMAN, Caesarea, Israel, New York, NY
Blood glucose monitoring systems (BGMS) are an in basic tool for diabetes
patients. The innovative DarioTM BGMS enables convenient self-monitoring
by adding a proprietary smart phone application. We evaluated accuracy and
user performance in a clinical trial of 368 type 1 and type 2 diabetic patients,
each of whom tested fresh capillary finger prick blood glucose levels while
using this BGMS for the first time, as instructed only by the manufacturer’s
directions for using the device. Glucose value accuracy was determined in
one sample obtained from each subject measured both on the BGMS by individual subjects and by a reference analysis of the identical sample. We
documented sample collection or measurement errors. When needed, repeat sampling by each subject was limited to 3 per subject. The interval of
glucose levels tested were BGMS range 43.0-477.0 mg/dL, and YSI range
42.3-435.5 mg/dL. There were no outliers. We used all 368 lay subjects’
samples. Accuracy for this BGMS met ISO 15197:2013 criteria. Below 100
mg/dL, 97.8% of values were within ±15mg/d of YSI reference glucose values. For samples with glucose above or equal to 100 mg/dL, 96.4% of values
were within ± 15% of YSI glucose levels. Lay subject performance assessment of the Dario BGMS’ instruction clarity and usefulness showed 97.1% of
subjects found instructions easy to follow with 70.7% rating they were very
satisfied (5/5) and 26.4% rating they were satisfied (4/5). Reading the result
on the smart mobile device was rated easy to understand by 99.1% of lay
subjects, with 86.1% rated it very easy (5/5) and 13% rated it easy (4/5). If
an error message displayed on the report screen, 96.4% of lay subjects were
clear about what to do, with 50% reporting is was very clear (5/5) and 46.4%
reported it was clear (4/5). The Dario BGMS meets ISO 15197:2013 standards
for clinical performance as determined by lay user accuracy and by satisfactory experience with the BGMS instructions clarity and system utility.
Supported By: The Leona M. and Harry B. Helmsley Charitable Trust
80‑LB
Long-Term Follow-up of Sensor-augmented Pump Therapy with
Low Glucose Suspend Function (SAP-LGS) in Type 1 Diabetes (T1D)
Patients with High Risk of Hypoglycemia
ANA MARIA GOMEZ, OSCAR MUÑOZ, DIANA HENAO, EDWIN MORA, CARLOS
AUGUSTO YEPES, MARTIN RONDON, Bogotá, Colombia
To assess the efficacy and safety of long term use of SAP-LGS in T1D
patients who initiated this therapy because of hypoglycemia and poor metabolic control. The second objective was to compare the frequency of severe
hypoglycemia and perception of hypoglycemic symptoms before and after
SAP-LGS therapy. The study was an observational prospective cohort study
from August 2010 until February 2015 of T1D patients with hypoglycemia,
older than 14 years of age, who started SAP - LGS at Hospital Universitario
San Ignacio, Bogotá - Colombia. The main indication was hypoglycemia and
poor metabolic control. Demographic and clinic variables were registered as
well as A1c levels at the beginning, 3 month and 1 year follow-ups. 94 T1D
patients with hypoglycemia were included with an average baseline A1c of
8.84 ± 1.93%. The mean follow-up was 2, 2 years (range 4.5 - 1, 02 years);
sensor use was 80 - 100% of the time in 94% of the patients. At the end of
the follow-up, the decrease of A1C was statistically significant at 7.3% ±
1.03% (p<0.0001), this decrease was found at the third month of follow-up
A1c 7.6%±1.7% (p<0.0001), with decreased incidence of severe hypoglycemia in the last year to 0.02 episodes per patient per year (p= 0.0032). Only
2% of the patients presented severe hypoglycemia, which is statistically
different from the baseline (p <0.0001) and 12% of patients remain with hypoglycemia unawareness (p <0.0001) after initiating therapy. The patient
proportion at the beginning with A1C less than 7% was 16%. 87% had severe hypoglycemia. At the end of the follow-up, it was 44.7%. Only 4.8% had
severe hypoglycemia (p<0.0001) In conclusion, SAP-LGS therapy reduces in a
statistically significant quantity the severe hypoglycemic and unawareness
of hypoglycemia in T1D patients with failure to MDI and a high risk of hypoglycemia. This allows better metabolic control in a safe way. This effect was
observed early and was maintained during the follow-up time.
78‑LB
Evaluation of Hematocrit and Hypoglycemia in a University Hos‑
pital: Blood Glucose Monitoring Experience Using Retrospective
Data Analysis
RICHARD J. BALTARO, BRYAN J. DANGOTT, ROBERT J. TANENBERG, APARNA
THOMBARE, SU FAN LIN, Greenville, NC
We evaluated the effect of hematocrit on waived point of care blood
glucose values and the number of hypoglycemic events, using concurrent
main laboratory glucose and hematocrit. At Vidant Medical Center, a 941
bed university hospital, a Roche Accu-Chek II Inform blood glucose monitoring system (BGMS) is used for metabolic control. The BGMS was evaluated
using EHR data for 14 months (October 2013-December 2014). During the
sample period, there were 590,000 point of care adult patient blood glucose
tests (POC BG), 332,000 chemistry analyzer blood glucose tests (CA BG) and
332,000 hematocrit tests (HCT). We correlated all BGMS values that had
a concurrent glucose performed by laboratory chemistry analyzer (Siemens
Advia) within 3 minutes and a laboratory hematocrit (Coulter) within 6 hours.
Hypoglycemic events where defined as a POC BG laboratory < 70 mg/dl preceded by a POC BG > 180 mg/dl in the previous 6 hrs. At hematocrits < 40, the
lower the hematocrit, the higher the percent POC BG increase against the CA
BG. At lower hematocrits, the average POC BG was higher than the CA BG.
At hematocrit of <20, 88% of the POC BG values were elevated and only 12%
were decreased. The average increase bias was + 9.4%. At hematocrits > 50,
there was a slight negative bias (-1.7%). 860 hypoglycemic events were identified out of 159,416 patients for an average of 0.54% events per patient. The
patient population with hematocrit < 30 had 380 hypoglycemic events for
29,023 patients, or 1.39% events per patient. This value is almost ten times
higher than 72 hypoglycemic events for 46,528 patients with hematocrits >
40 or 0.16% events per patient. Retrospective data analysis demonstrated
increased bias of POC BG readings by lower hematocrit and the subsequent
increased incidence of hypoglycemic episodes.
81‑LB
Can Use of Continuous Glucose Monitoring (CGM) Prior to Initiating
Insulin Pump Therapy Result in Greater Glycemic Improvements?
AIMEE JOSE, RUTH SPIRAKIS, CHRISTOPHER G. PARKIN, Palo Alto, CA, Boulder
City, NV
Initiating continuous glucose monitoring (CGM) prior to insulin pump therapy has been shown to increase frequency of CGM use, however, the impact of this approach on clinical outcomes has not been well studied. In this
single-center, retrospective, pilot study, we assessed changes in HbA1c over
6 months in patients with type 1 diabetes treated with CSII and CGM. HbA1c
values at baseline (before starting CGM) and 6 months after combined device
(CGM/pump) use were available for 13 patients: 7 used CGM before pump
(BP) initiation (baseline HbA1c 7.7±1.5, age 52.3±10.6 years, 86% female,
186.1±151.0 CGM days [range: 26-441 days] before pump); 6 patients started
CGM after pump (AP) initiation (baseline HbA1c 7.9±1.1, age 45.3±14.7 years,
83% female, 75.5±93.1 pump months [range: 0-252 months] before CGM. At
6 months post CGM/pump use, BP patients showed a clinically significant
reduction in HbA1c from baseline compared with AP patients: -0.7±1.1% vs.
-0.2±1.0%, respectively. (Figure 1) Although not conclusive due to the small
sample size, our results suggest that use of CGM prior to initiation of insulin
79‑LB
Reducing Staff Time with Optimized Work Flows and Standardized
Ambulatory Glucose Profile (AGP) Reporting
DEBORAH M. MULLEN, RICHARD M. BERGENSTAL, AGP WORK FLOW STUDY
GROUP, Minneapolis, MN
This research aimed to evaluate feasibility, utility and preference of standardized cloud-based glucose reporting using AGP reports. Seven diverse
sites were recruited (n = 144 patients and 16 clinicians). Measures of AGP vs.
traditional glucose data acquisition were collected from the patient/family
ADA-Funded Research
For author disclosure information, see page LB98.
LB20
Clinical Therapeutics/New Technology—Insulins
pump therapy may lead to greater glycemic improvement. Larger studies are
needed to assess the efficacy of this approach.
kg). C-peptide secretion also improved significantly in this population with
very advanced long-standing disease.
Table.
Clinical Therapeutics/New Technology—
Insulins
Supported By: Novo Nordisk
Sustainable Effects of Basal Insulin Have Favorable Outcomes on
Fasting Blood Glucose Control in Patients with Type 2 Diabetes
YOU-PING CHAN, GUILLAUME NOEL, Oullins, France, Marcy l’Etoile, France
SHIZUKA KANEKO, YUMIKO TAHARA, YORIHIRO IWASAKI, Takatsuki, Japan
Ultra-long acting insulins, characterized by a duration of action greater
than 36 hours, are the next generation basal insulins that could potentially
provide a better glucose control by delivering an infusion-like profile insulin
at steady state following daily injection. The objective of the study was to
investigate PK and PD performances in the Dog model of a new insulin analog that has the potential to be an ultra-long acting insulin. The new insulin
is made from glargine by addition of one histidine moiety. The new molecule,
formulated with the same excipients as those used in Lantus® and at the
same molar concentration of insulin analog, has been administered subcutaneously to normal fasted beagle dogs (n=9, 10-15 Kg) and the glucose level
measured over a period of 36 hours. The study has been conducted in a
crossover manner using Lantus® as the comparator and both are administered at 4.2 nmol/kg. The glucose lowering results, displayed in Figure A,
show that the duration of action for the new molecule is at least 36 hours
compared to about 20-24 hours for Lantus®. The c-peptide corrected insulin
levels, consistent with the glucose lowering results, also last for at least 36
hours as shown in Figure B. These results suggest that the new analog has
the potential to deliver basal insulin with efficacy for at least 36 hours in
this animal model.
We investigated the difference in the sustainable effect of longer acting
formulations on blood glucose control in T2DM. We compared insulin degludec therapy (IDeg) which has the longest effect of 42 hours with conventional basal insulins (NPH, ditemir or glargine (IGla)) therapies of which the effect
is less than 24 hours. We conducted two different retrospective analyses,
1) comparison of the newly introduced IDeg and conventional insulin, and 2)
substitution of IDeg for conventional insulin. The duration needed to achieve
the target FPG and the quantity of insulin needed in both groups were analyzed. Out of 332 patients with T2DM, 114 patients (60 males, 64.4±9.8 years
old, disease duration of 7.6±7.4 years, HbA1c 10.1±2.1%, BMI 26.7±3.7, FPG
201±52 mg/dl) were newly administered IDeg once-daily, and 218 patients
(95 males, 57.4±13.0 years old, disease duration of 5.6±5.6 years, HbA1c
10.4±1.8%, BMI 27.1±4.6, FPG 200±56mg/dl) were newly administered IGla
once-daily. Patients newly treated with IDeg achieved the target FPG earlier
(6.7±6.9 days) than those with IGla (8.9±11.7 days) (p<0.01). Total doses of
IDeg (104.4±75.3 unit) needed to achieve the target FPG tended to be less
than those of IGla (122.5±93.4 unit) (NS). Sixty-nine patients undergoing conventional therapy were switched to IDeg for more than 30 days and then
switched back to conventional therapy. The average and variability (SD) of
FPG for 14 days prior to and after both switches were analyzed. After switching from conventional therapy to IDeg therapy, both the average and SD of
FPG decreased in 47.8% of patients (the average decreased in 72.4% and the
SD of FPG decreased in 68.1%), and the amount of insulin was reduced by
10%. Nocturnal hypoglycemia occurred in 1% and 5% of patients undergoing IDeg and conventional therapy, respectively. Longer active basal insulin
therapy, i.e. IDeg, provides more effective and safer control of blood glucose
in T2DM. It might also be expected to reduce medical costs.
Supported By: Japan Vascular Disease Research Foundation
Adding Liraglutide to High-Dose Insulin: Breaking the Cycle
83‑LB
ANNA VANDERHEIDEN, LINDSAY HARRISON, BEVERLEY ADAMS HUET, ILDIKO
LINGVAY, Dallas, TX, Austin, TX
Treatment with high dose insulin has become much more common in the
type 2 diabetes population. These patients often experience treatment
related weight gain and an increase in insulin resistance, leading to even
higher insulin requirements. We evaluated if addition of liraglutide is effective and safe in this difficult to control population with advanced disease.
We conducted a randomized, double-blinded, placebo-controlled study in
patients with uncontrolled (HbA1c>7.5%) type 2 diabetes using >1.5 units
of insulin/day, who received liraglutide 1.8 mg/day or matching placebo in
addition to their background insulin regimen, for a total of 6 months. All
measurements, including a 4 hr mixed meal challenge test were performed
at baseline and end of treatment. We randomized 71 patients (age 54 yrs,
diabetes duration 18 yrs, insulin treatment duration 10 yrs), 93% completed
the study. Results are in the Table. The rate of hypoglycemia (<70mg/dl) was
0.91 per person/month (ppm) in the liraglutide vs. 0.59 ppm in the placebo
group (p=0.07), this occurred in 84.9% of patients in liraglutide and 71.4%
in the placebo group (p=0.25). Addition of liraglutide to a high dose insulin
regimen significantly improved glycemic control (placebo-subtracted HbA1c
-1.0%) and caused weight loss (placebo-subtracted weight difference -2.1
85‑LB
Delay of Insulin Initiation in Patients with Type 2 Diabetes Mellitus
Inadequately Controlled on Oral Glucose-Lowering Agents (Analy‑
sis of Patient- and Physician-related Factors): A Prospective, Ob‑
servational Dipp-Factor Study in Korea
SIN GON KIM, KYOUNG SOO HA, BON JEONG KU, HO SANG SHON, DOO MAN
KIM, TAE SUN PARK, YONG-SEONG KIM, IN JOO KIM, DONG SEOP CHOI, Seoul,
Republic of Korea, Daejeon, Republic of Korea, Daegu, Republic of Korea, Jeonju,
Republic of Korea, Incheon, Republic of Korea, Busan, Republic of Korea
Objective: To assess the time to initiation of insulin therapy, and concurrently investigate both patients- and physicians-factors associated with
delaying insulin therapy in Korean patients with type 2 diabetes (T2D) uncontrolled on oral hypoglycemic agents (OHAs).
Research Design and Methods: This prospective, observational disease
registry was conducted across 69 centers in Korea. T2DM patients who had
received two or more OHAs within last 5 years, had HbA1c ≥8% in last 6
ADA-Funded Research
For author disclosure information, see page LB98.
LB21
POSTERS
A New Ultra-Long-Acting Glargine Analog with Improved Pharma‑
co-kinetic (PK) and Pharmacodynamic (PD) Profiles Compared with
Lantus®
Clinical Diabetes/
Therapeutics
84‑LB
82‑LB
Clinical Therapeutics/New Technology—Insulins
months and had not received insulin were included. Data were collected in a
data collection form during a 12-month period.
Results: Of 2,168 patients enrolled, 1,959 were evaluated and classified
as insulin-initiated or insulin-delayed group. Insulin was prescribed for only
20% of the patients during one year follow-up and less than half (44.5%) of
the patients who were on two OHAs started insulin after 6 years. Patientrelated factors for delay in insulin initiation included older age, shorter duration of diabetes, and a lower HbA1c. Physician-related factors included
age (50 ~ <60 years), gender (women), number (<1000) of patients consulted
per month, Patient refusal (33.6%) and physician’s concerns of patient’s
non-compliance (26.5%) were the other major reasons of delaying insulin
therapy. Inconvenience due to insulin therapy (51.6%) was the major reason
for patient refusal.
Conclusions: Insulin initiation is delayed in patients with T2D uncontrolled
on two or more OHAs in Korea. Patient- and physician-related factors associated with this delay need to be addressed for better diabetes management.
Supported By: Sanofi-Aventis
Supported By: Sanofi-Aventis
POSTERS
Clinical Diabetes/
Therapeutics
86‑LB
88‑LB
Use of PKPD Model to Design and Analyze Results of a Euglycemic
Clamp Study for a Very Long-Acting Insulin Analogue HM12470
Clinical Pharmacokinetics (PK) and Renal Elimination of Basal In‑
sulin Peglispro (BIL) and Its Polyethylene Glycol (PEG)-Containing
Products
YEAMIN HUH, JAHOON KANG, NARI YUN, SIYOEN KIL, JEEWOONG SON, SUNNY CHAPEL, Ann Arbor, MI, Seoul, Republic of Korea
PARAG GARHYAN, SIAK LENG CHOI, ELIZABETH S. LABELL, MARY P. KNADLER,
MELVIN J. PRINCE, Indianapolis, IN, Singapore, Singapore
HM12470 is a novel very long-acting insulin analogue developed for weekly
dosing, by conjugating a soluble insulin and a non-glycosylated Fc carrier via a
non-peptidyl linker. The extended half-life of HM12470 was confirmed in several species; mice, rats, dogs, and monkeys. Due to an expected prolonged
glucose lowering efficacy from the extended pharmacokinetic (PK) profile,
choosing the right time for a euglycemic clamp study becomes an issue to
capture an onset, peak, and offset of insulin action. The purpose of this study
is to select the timing of clamp study for a very long-acting insulin analogue
using a PKPD (pharmacodynamic) modeling. A PKPD model to describe a relationship between concentration and glucose infusion rate (GIR) of HM12460A,
another very long-acting insulin analogue having a similar molecular structure
to HM12470, was previously developed. From results of animal studies, a ratio
of HM12470 half-life (t1/2) to HM12460A t1/2 in human was predicted as 2.4 (132
hrs vs. 55 hrs). The elimination rate constant (Ke) of HM12470 was then estimated as 0.0055/hr based on the ratio of t1/2 and Ke of HM12460A (0.0132/hr).
By assuming that a base PK model structure is the same between HM12470
and HM12460A except Ke, a concentration vs. time profile of single dose of
HM12470 was predicted. The predicted concentration vs. time profile enabled
to predict a GIR vs. time profile based on an assumption that the potency of
HM12470 is the same as the one for HM12460A. Based on these predictions,
the maximum GIR is expected to be at 62 hr post-dose and the GIR is reduced
by 40% 10 days later. Therefore, performing a clamp study on day 1 and day
5 was recommended to capture an onset and elimination phase of GIR for the
ongoing Phase I study of HM12470. In conclusion, PKPD modeling could be a
useful tool to design and analyze results of a euglycemic clamp study for a very
long-acting insulin analogue, whose prolonged glucose lowering effect cannot
be fully monitored using current standard methods.
BIL is a novel basal insulin with a prolonged duration of action consisting of
insulin lispro covalently linked to 20 kDa PEG. In rats, BIL was eliminated primarily via catabolism with total-PEG (BIL and PEG-containing catabolism products)
excreted about equally via biliary and renal routes. In this analysis, BIL population
PK was evaluated using data from 15 Phase 1, 2, and 3 studies in healthy subjects
and patients with type 1 diabetes or type 2 diabetes (T2D). BIL and total-PEG
exposure and renal elimination were evaluated in a subset of T2D patients in a
26-week Phase 3 study; BIL and total-PEG were measured in urine at week 26
(n=35) and plasma (total-PEG, n=47) or serum (BIL, n=190) at week 2, 4, 12, and
26. The PK of BIL was well described by a 2-compartment model with absorption-limited first-order elimination kinetics. Rate of absorption was estimated at
0.022 hr-1, clearance was 1.79 L/h and central and peripheral volumes of distribution were 31.5 L and 23.4 L, respectively. Body weight was the only significant
predictor of BIL PK, and the effects of body weight, age, BMI, sex, race/ethnicity,
renal function and disease status were not clinically relevant. At steady state,
mean renal excretion of BIL and total-PEG was 1.6% and 23.9% of BIL dose, respectively. Serum BIL and plasma total-PEG concentrations increased over time
during dose titration and remained stable during the remainder of the dosing
period. Total-PEG plasma concentrations decreased after cessation of BIL dosing. These findings show low urinary excretion of intact BIL and suggest that in
patients with T2D the majority of total-PEG was excreted via nonrenal routes.
At steady state, total-PEG plasma concentrations did not increase over time, as
total-PEG continued to be excreted. The PK of BIL supports once-daily dosing,
and dose adjustments are not needed based on patient factors.
Supported By: Eli Lilly and Company
89‑LB
87‑LB
Basal Insulin Peglispro (BIL) Demonstrates Hepato-Preferential
Action vs. Insulin Glargine (GL) in Patients with Type 1 Diabetes
Mellitus (T1DM)
Basal Insulin Treatment in Patients with Type 2 Diabetes Uncon‑
trolled on Oral Antihyperglycemic Agents: ORBIT Study in China
LINONG JI, PUHONG ZHANG, JIANPING WENG, SATISH K. GARG, Beijing, China,
Guangzhou, China, Aurora, CO
SUNDER MUDALIAR, ROBERT R. HENRY, THEODORE P. CIARALDI, DEBRA A.
ARMSTRONG, PAIVI M. BURKE, JEREMY H. PETTUS, PARAG GARHYAN, SIAK
LENG CHOI, SCOTT J. JACOBER, MARY P. KNADLER, ERIC CHEN QUIN LAM, MELVIN J. PRINCE, NAMRATA BOSE, NIELS PORKSEN, VIKRAM P. SINHA, HELLE LINNEBJERG, San Diego, CA, Indianapolis, IN, Singapore, Singapore, Silver Spring, MD
Basal insulin (BI) treatment is usually delayed in patients with T2DM despite its proven efficacy. We report the largest 6-month prospective study in
China to evaluate the safety and glucose control after introduction of BI in
real-life in the 2nd or 3rd tier hospitals. Inadequately controlled with OADs
(A1C ≥7%), adults (N=18,995) with T2DM were enrolled at 209 hospitals (different regions of China) and had 3 visits (baseline, 3 and 6 months). Type of BI
used was at the physician’s discretion. Mean age was 55.4±10.4 years, with
6.4±5.3 diabetes duration (~50% men). Long-acting BI was most commonly
used (82.5%-visit 1, 69.9%-visit 2, 64.2%- visit 3; Figure), with intermediateacting NPH insulin used by <18% at all visits. Long-acting BI-glargine was
used by 70% at visit 1, 59% at visit 2, and 54% at visit 3 of patients, whereas
detemir was used in <13% at each visit. >70% of glargine and detemir users
continued to use the same insulin throughout the study. 40% of patients
did not change their insulin dose at all in the first 3 months. There was a
significant improvement in A1c values at 3 months, which was maintained
at 6 months (Figure). Target FBG (<7.0 mmol/L) and A1C (<7%) were achieved
in 43% and 41% of patients, respectively. Hypoglycemia was higher with
no weight gain for long-acting BI. We conclude that BI initiation in real-life
improves glucose control at 3 and 6 months in the ORBIT study.
BIL, a novel, long-acting basal insulin, has previously demonstrated
hepato‑preferential action in healthy subjects. This randomized, open-label,
4-period, crossover study evaluated effects of therapeutic (BIL and GL) and
supratherapeutic concentrations (BIL) on liver (endogenous glucose production
[EGP]) and peripheral tissues (glucose disposal rate [GDR] and lipolysis) in patients with T1DM. Patients (n=14; 22-48 years) had 4 euglycemic clamps of 8-10
hours duration with primed, continuous infusions of BIL (15.3 and 74.1 mU/min)
and GL (10 and 20 mU/m2/min). D-[3-3H]-glucose infusion assessed EGP and
GDR. To correct for differences in insulin receptor binding, equivalent human
insulin concentrations (EHIC) were calculated by dividing each insulin concentration by its Ki (binding constant) and multiplying by the Ki of human insulin.
At both low and high doses, BIL showed similar effects on EGP suppression
(endpoint EGP) compared to GL, but had an attenuated effect on GDR (endpoint
GDR) (Table). Lipolysis, assessed by free fatty acids (FFA) and glycerol, was
suppressed at low and high GL doses but only at the high BIL dose (Table).
ADA-Funded Research
For author disclosure information, see page LB98.
LB22
Clinical Therapeutics/New Technology—Insulins
91‑LB
BIL has similar hepatic activity (EGP suppression) but less peripheral activity
(GDR stimulation, lipolysis suppression) at clinically relevant concentrations
compared to GL, confirming hepato-preferential action.
Table.
Improved Glycemic Control with Lesser Daily Dose with insulin
Glargine on Retransition from Insulin Detemir
92‑LB
Ultra-Rapid-Acting/Basal Concentrated Insulin BIOD-531 Demon‑
strates Superior Postprandial Glucose Control and Potential for
Flexible Post-meal Dosing Compared with Marketed Prandial/Bas‑
al Insulins in Insulin-Resistant Patients with Type 2 Diabetes
LINDA MORROW, LORI CANNEY, PHILIP PICHOTTA, MARCUS HOMPESCH, ALAN
KRASNER, ERROL DE SOUZA, Chula Vista, CA, Danbury, CT
BIOD-531, a 400 U/ml formulation of recombinant human insulin, EDTA, citrate,
and magnesium sulfate is associated with ultra-rapid onset and basal duration
of action. Twelve subjects with type 2 diabetes who used a mean of 205 units
of insulin/day were evaluated in this randomized, four-arm cross-over study. On
separate days, following glucose standardization, each subject underwent the
following 4 treatments administered with a standardized breakfast (921 kcal)
and with a standardized dinner (963 kcal): (a) BIOD-531 immediately before
meals (pre-meal); (b) Humalog® Mix 75/25 (HMix) pre-meal; (c) Humulin® R U-500
(U-500) pre-meal; and (d) BIOD-531 20 min after the start of the meals (postmeal). The insulin dose was 1.2 U/kg with breakfast and 0.8 U/kg with dinner.
Lunch (669 kcal) was given without insulin treatment 330 min after the breakfast
dose. The primary endpoint was average glucose concentration in the breakfast
to lunch interval. BIOD-531 was associated with superior glucose control compared to HMix and U-500 during this period. The mean post-breakfast glucose
concentration (mg/dl) was 164.6±11.8 with BIOD-531 treatment compared to
179.9±10.0 with HMix (p=0.009) and 178.0±7.3 with U-500 (p=0.019). Over the
entire 24 hours of observation, pre- and post-meal BIOD-531 resulted in superior
glucose concentrations (155.7±15.7 and 149.8±11.8, respectively) compared to
pre-meal HMix (172.6±14.0, p < 0.05 for both comparisons) and comparable to
pre-meal U-500 (154.0±13.1). There were no unexpected safety findings. In summary, BIOD-531 dosed pre-meal twice daily resulted in superior prandial control
compared to HMix and U-500 in insulin-resistant patients with type 2 diabetes.
Post-meal dosing of BIOD-531 resulted in superior or comparable overall glycemic control compared to pre-meal treatment with HMix and U-500.
Supported By: Eli Lilly and Company
90‑LB
Simple Fortnightly Intravenous Nonpump Insulin Therapy to Treat
Diabetic Gastroparesis
PRASHANT K. PRAKASH, PRADEEP K. MAHESHWARI, DAYA K. HAZRA, PRABHAT K. AGRAWAL, AYUSH K. AGARWAL, Agra, India
Diabetic gastroparesis is characterised by a delay in gastric emptying after
a meal in the absence of a mechanical gastric outlet obstruction. Chronic intermittent intravenous insulin therapy (CIIIT) was originally described as delivering insulin intravenously over a 6-12 hour period in a pulsatile fashion adjusting
dosages based on frequent blood sugar monitoring and has been claimed to be
beneficial in diverse diabetic syndromes. The aim of the study was to evaluate
the efficacy of a modified non-pump insulin regime “MOD CIIIT” in patients
of diabetic gastroparesis Fifty euglycemic cases of diabetes mellitus having
signs and/or symptoms of diabetic gastroparesis not relieved with conventional pharmacotherapy were studied. 12 units of human regular insulin were
added to a half litre bottle of 5% Dextrose in 0.9% Normal Saline and infused
intravenously over a period of 6-8 hours using a microdrip set. This was repeated fortnightly The symptoms were compared at the commencement of the
study and after 6 sessions of MOD CIIIT (i.e. after 3 months) and finally after
12 sessions (6 months) by asking the patient to grade their symptoms numerically viz Belching, Bloating, Constipation, Diarrhoea, Nausea and Vomiting on
a Visual Analogue Scale (VAS) on each visit. We found that patients who were
previously refractory to conventional pharmacotherapy, showed considerable
response to MOD CIIIT with most patients giving history of improvement in
their symptoms after therapy and during follow up. The VAS scores showed
statistically significant decline in the composite score of all symptoms (p<
0.001) and HbA1c levels also remained in the euglycemic range throughout.
MOD CIIIT is extremely beneficial in patients presenting with complaints of
diabetic gastroparesis can be managed by MOD CIIIT. MOD CIIIT is a simple
and inexpensive method of delivering intermittent insulin therapy.
Inpatient Diabetes on Corticosteroids Study
93‑LB
JAMIL B. ALKHADDO, LISA FISH, AMEER KHOWAJA, Minneapolis, MN
Despite marked hyperglycemia in diabetes patients receiving corticosteroids (CS), there are no published protocols tested to address insulin management. We tested a simple protocol using NPH insulin for inpatient diabetes
(IPDM) patients on CS (Table 1). In a prospective, randomized, non-blinded
study of IPDM adults receiving CS, 31 patients have been randomized to
ADA-Funded Research
For author disclosure information, see page LB98.
LB23
POSTERS
Background: We documented lapse of glycemic control, despite higher daily
insulin dose, 2 SC injections, and increased number of daily blood glucose monitoring with less convenience on switching from Insulin Glargine (GI) to Insulin
Detemir (DI) in subjects with type 1 and type 2 DM (Iowa Medicaid 1 and 2).
Objective: Assess impact of retransition from DI to GI in subjects with
type 1 and type 2 DM.
Subjects and Methods: 8 men and 6 women with type 1 (36 ± 3 years)
and 12 men and 10 women with type 2 DM (62 ± 5 years). Duration of DM
(years) was 15 ± 2 in type 1 and 12± 3 in type 2. DI was discontinued in both
groups. Insulin Aspart (AI) was continued premeal 3 times daily in type 1 and
Metformin and SU were continued in same daily dose in type 2. GI was reinitiated at 0700-0800 AM in the same daily dose as DI. Daily dose of insulin
DI, GI and AI, no of injections, HbA1c, body Weight (BW) and hypoglycemia
(Hypo) were assessed at 6 months.
Results: Type 1 DM: Daily insulin dose, 58±6 and DI, 31±6 declined to 48±6
and GI, 23±5 units respectively (p<0.05). AI daily dose was not significantly
altered. No of injections with DI, 4.6±0.3 declined to 4.0 ±0 with GI. HbA1c,
BW and Hypo were not significantly different (GI: HbA1C, 7.2 ± 0.2; BW, 70 ± 4;
Hypo, 0.5 ± 0.2) vs. DI: HbA1c, 7.4 ± 0.3; BW, 71 ± 5 Kg; Hypo, 0.6 ± 0.2).
Type 2 DM: On transition to GI, Daily DI dose,70±11 units, no. of injections,
1.4±0.2 and HbA1c, 7.6±0.3 declined to 56±6 units, 1±0, and 7.1±0.2 (p<0.01).
No significant changes occurred in BW (93±5 with DI vs. 91±3 with GI) and
hypo (0.2±0.1 with DI vs. 0±0 with GI).
Conclusion: Insulin Glargine is more cost effective than Insulin Detemir
due to lower daily dose, less equipment, (syringes, needles, alcohol pads)
needed for once daily administration (more convenient with better quality
of life) in type 1 and type 2 Once daily blood sugar testing may further lower
cost in type 2. Thus, Insulin Glargine and Detemir are not bioequivalent and
transition from one to another may be detrimental.
Clinical Diabetes/
Therapeutics
UDAYA M. KABADI, Iowa City, IA
Clinical Therapeutics/New Technology—Insulins
date to receive either NPH insulin using the protocol or standard care (control). The mean daily blood glucose was 276.8 and 219.47 for the control and
treatment group, respectively, and the incidence of severe hyperglycemia
was lower in the intervention arm (Table 2). In conclusion, implementing an
insulin protocol in IPDM patients receiving CS is straightforward and will
increase the use of basal insulin, resulting in better glycemic control. However, optimal care may necessitate further insulin adjustment.
aAcross
the study, TI doses were individualized and ranged from 15-90 U;
therefore, calculating mean FDKP and insulin AUC, mean insulin and C-peptide
concentrations, or PK parameters were not meaningful. bFor diagnosis of URTIs,
patients had to have ≥ 3 URTI symptoms within the 24 hours prior to clinic visit
and/or on the day of clinic visit (runny nose, nasal stuffiness, sneezing, sore
throat, scratchy throat, hoarseness, cough [new onset], sinus pain/pressure,
head congestion/headache, and plugged ears/ear discomfort). cn = 19. dFor 5
patients, TI doses during and after URTI resolution were different. AUC was
normalized for these patients to the lower of the 2 TI doses; the ratio was
performed on the log-transformed normalized AUC. eDifference (after URTI −
during URTI); as differences were small and variation large, statistical analysis
was limited. AUC0-4h, AUC from 0-4 hours; Cmax, maxium serum concentration;
Cmin, minimum serum concentration; FDKP, fumaryl diketopiperazine; NA, not
applicable; tmax, time to reach Cmax.
Table 1. NPH Insulin Protocol.
NPH insulin dose with every
CS dosing
Low dose High dose
CS
CS *
Eating and 6 am to 8 pm 0.15 u/kg 0.3 u/kg
NPO or 8 PM to 6 am
0.1 u/kg 0.2 u/kg
* High dose CS defined as Prednisone > 40 mg/day, hydrocortisone >160 mg/
day, methylprednisolone > 32mg/day, and dexamethasone > 6mg/day.
Supported By: MannKind Corporation (NCT00642681); Sanofi US, Inc.; Excerpta
Medica
95‑LB
POSTERS
Clinical Diabetes/
Therapeutics
Table 2.
Total # of readings
BG 70 to 180 BG >180 BG >300 BG >400 Control
17 pts
185
34 (18.4%)
151 (81.6%)
73 (39.5%)
17 (9.2%)
Intervention
14 pts
133
46 (33.6%)
34 (63.5%)
26 (19.0%)
5 (3.6%)
New Insulin Glargine 300 U/mL (Gla-300) in Combination with Di‑
peptidyl Peptidase IV Inhibitors in T2DM (EDITION 2 and 3): Glyce‑
mic Control and Hypoglycemia
P value
RAFFAELLA BUZZETTI, JEREMY H. PETTUS, MIGUEL BRITO-SANFIEL, FERNANDO J. LAVALLE-GONZÁLEZ, ANA MERINO-TRIGO, PETER STELLA, SOAZIG CHEVALIER, JEAN-FRANÇOIS YALE, Rome, Italy, San Diego, CA, Majadahonda, Spain,
Monterrey, Mexico, Paris, France, Chilly-Mazarin, France, Montreal, QC, Canada
0.0028
0.0004
0.0001
0.0846
In people with T2DM treated with oral antihyperglycemic drugs (insulinnaïve [EDITION 3, N=878] or on basal insulin [EDITION 2, N=811]), starting
with or switching to Gla-300 provided comparable glycemic control to insulin glargine 100 U/mL (Gla-100), with a lower risk of hypoglycemia at any
time of day and during the night over 6 months. This post hoc patient-level
meta-analysis of EDITION 2 and EDITION 3 data evaluated glycemic control
and hypoglycemia with Gla-300 vs. Gla-100, with or without concomitant
DPPIVi use. Among treated patients, 107 (13%, Gla-300) and 133 (16%, Gla100) participants received DPPIVi therapy. A comparable decrease in HbA1c
from baseline to month 6 was observed for Gla-300 vs. Gla-100, irrespective
of DPPIVi use (Table). Risk of confirmed (≤70 mg/dL) or severe hypoglycemia
at any time of day (24 h) or at night (00:00–05:59 h) was consistently lower
for Gla-300 vs. Gla-100, regardless of DPPIVi use. The concomitant use of
DPPIVi did not have an impact on basal insulin dose change in the different
treatment arms. Weight gain was minimal in all groups. In conclusion, the
comparable glycemic control with less hypoglycemia at any time of day (24 h)
and during the night of Gla-300 vs. Gla-100 observed in the overall EDITION
2 and EDITION 3 study populations was consistently shown in this pooled
analysis, irrespective of administration of DPPIVi.
94‑LB
Inhalation of Insulin: Effect of Symptomatic Upper Respiratory Tract In‑
fections on Pharmacokinetic/Pharmacodynamic (PK/PD) Properties
PHILIP A. LEVIN, LUTZ HEINEMANN, ANDERS BOSS, PAUL D. ROSENBLIT, Baltimore, MD, Düsseldorf, Germany, Bridgewater, NJ, Huntington Beach, CA
Uncomplicated, acute upper respiratory tract infections (URTIs), i.e. common colds, occur in patients with diabetes at a similar frequency to the general population. We studied the effect of URTIs on the PK/PD properties of
Technosphere Insulin Inhalation Powder (TI) in patients with type 1 or type 2
diabetes (N = 20, mean age 50 years, 60% men). The trial included patients
who developed a URTI while treated with TI in a phase 3 study (see Table
for URTI definition). Patients underwent two 4-hour meal challenges during
which blood samples were drawn to measure serum FDKP (the dry powder
excipient), serum insulin, serum C-peptide, and plasma glucose. The primary
outcome was the ratio of serum FDKP AUC0-4h during URTI to after clinical
resolution of URTI symptoms (≥ 15 to ≤ 45 days). There were no significant
differences in PK parameters during URTI versus after resolution of URTI
(Table). Plasma glucose concentrations (unadjusted and baseline-corrected)
were similar during and after URTI resolution. No adverse events (including
hypoglycemia) occurred during meal challenge visits. URTIs had no impact
on the PK/PD properties of TI. However, study observations are are limited
to patients with URTI, as individuals with lower respiratory tract infection
were not studied. If a patient is unable to conduct proper inhalation they
should administer insulin subcutaneously.
Table. FDKP Ratio and Insulin/Glucose Parameters During a Meal Challenge
During and After URTI (N = 20).
During
After
Parameter, mean (SD)a
URTIb
URTI
Comparison P value
FDKP ratio AUC0-4h during URTI:
NA
NA
1.1 (0.63)c,d 0.4462
AUC0-4h after URTI (ng*min/mL)
FDKP tmax (minutes)
15.8 (26.2)c 15.5 (14.8)c −0.3 (31.97)c 0.9725
Insulin ratio AUC0-4h during URTI:
NA
NA
0.9 (0.37)c 0.1754
AUC0-4h after URTI (ng*min/mL)
Insulin tmax (minutes)
25.5 (44.42) 21.3 (25.12) −4.3 (52.12) 0.7194
Glucose Cmax (mg/dL) Baselinecorrected Cmax (mg/dL)
212.0 (65.6) 198.8 (69.7) −13.2 (75.6)e
81.0 (57.2) 69.7 (69.9) −11.3 (72.7)e
NAe
Glucose Cmin (mg/dL) Baselinecorrected Cmin (mg/dL)
(57.8)e
NAe
116.7 (41.7) 111.1 (41.2)
5.9 (14.6) 1.9 (7.9)
−5.7
−4.0 (12.5)e
Supported By: Sanofi (NCT01499095, NCT01676220)
ADA-Funded Research
For author disclosure information, see page LB98.
LB24
Clinical Therapeutics/New Technology—Insulin Delivery Systems
Clinical Therapeutics/New Technology—
Insulin Delivery Systems
98‑LB
Bi-hormonal Closed-Loop Treatment of Type 1 Diabetes with Exer‑
cise Announcement to Prevent Hypoglycemia
Introduction: Technosphere inhaled insulin (TI) recently became available for
clinical use as a non-invasive alternative to subcutaneous insulin in adult patients with diabetes. The purpose of this systematic review and meta-analysis
was to determine the efficacy, safety, and patient acceptability of TI.
Methods: We searched MEDLINE, the Cochrane Clinical Trials Register,
and the Food and Drug Administration review documents of TI through January 31, 2015 for randomized control trials that compared TI with placebo,
subcutaneous insulin, or oral anti-diabetic drugs. Two reviewers independently assessed trials for inclusion and extracted data on study characteristics, participant baseline characteristics, efficacy, and safety outcomes.
Results: 12 trials met eligibility criteria (n=5,273, mean age range 38-61).
Among patients with type 1 or insulin-requiring type 2 diabetes, hemoglobin
A1c improvement from baseline favored subcutaneous insulin over TI (net
difference 0.16% [95% CI 0.06, 0.25]). TI was associated with less weight
gain (net difference -1.6 kg [-2.1, -1.6]) and less risk of hypoglycemia (odds
ratio 0.61 [0.35, 0.92]) compared to subcutaneous insulin. There was an
increased incidence of mild, transient, dry cough in patients treated with
TI (odds ratio 7.82 [6.14, 10.15]) and greater decline in FEV1 (net difference
-0.038 liters [-0.049, -0.026]). There was no difference in quality of life or
overall patient satisfaction. Many trials were designed for non-inferiority,
which may introduce bias, and most of the trials were 24 weeks duration or
less, thus limiting assessment of long-term safety.
Conclusions: Until long-term safety data are available, TI should be reserved for non-pregnant, non-smoking, adult patients with diabetes, free of
pulmonary disease, who are needle-phobic and would otherwise delay initiating or intensifying insulin therapy. For patients who are needle-tolerant,
subcutaneous insulin appears to be a better option.
Supported By: National Institutes of Health-National Institute of Diabetes and
Digestive and Kidney Diseases (DP3DK101044-01, K23DK090133)
97‑LB
99‑LB
A Feed-Forward Control Approach Capable of Substantially Tight
Variation of Blood Glucose Level
Closed-Loop Control with DIAS vs. Sensor-Augmented Pump Thera‑
py in Adolescents and Young Adults with Type 1 Diabetes at Camp
DERRICK K. ROLLINS, YONG MEI, Ames, IA
TRANG T. LY, DANIEL CHERÑAVVSKY, MARTA SATIN-SMITH, DANIEL J. DESALVO, SATYA SHANMUGHAM, PATRICK KEITH-HYNES, MARC D. BRETON, BRUCE
A. BUCKINGHAM, Stanford, CA, Charlottesville, VA, Norfolk, VA
An artificial pancreas (AP) must be capable of tight glucose control for major disturbances. Feedforward control (FFC) has the potential to completely
cancel the effect of any disturbance that it models. Thus, our objective is
the evaluation of our novel nonlinear parametrized FFC approach that seeks
to directly nullify the effects of eating, activity and stress. In this work, 11
cases of two weeks of free-living data collection on subjects with type 1
diabetes are modeled with 13 input variables. The activity variables were
collected using the SenseWear ® Pro3 Body Monitoring System. For a FFC
model, the critical performance measure is the correlation of the measured
BGC and the fitted BGC (rfit). The average rfit values of the 11 cases for
training, validation and testing were 0.64, 0.63, and 0.61, respectively. The
closeness of the values for each of the three sets is an indication that the
models did not significantly over-fit the data on unmeasured disturbances.
To understand the potential impact of this approach at this level of rfit we
show how the variation would be reduced in the figure using the fit of Subject 11. As shown, the variability is substantially reduced, with the standard
deviation dropping from 73.9 (left plot) to 8.7 (right plot) mg/dL, a decrease
of 88.3%. Thus, an AP based on this approach has the potential to reduce the
variation to the level of those without diabetes.
The DIAS system utilizes a control to range based algorithm for glucose
control in type 1 diabetes. The system includes a Dexcom G4 sensor, a Roche
AccuCheck pump and an Android-based DIAS controller. The objective of
this study was to test the safety and efficacy of DIAS in subjects with type
1 diabetes, aged 10-35y, over 5 days at diabetes camp. There were 33 subjects randomized to either closed-loop with DIAS (intervention) or sensoraugmented pump (control) for 5 days at diabetes camp. Both groups utilized
premeal boluses. The mean±SD age of all subjects was 17.9±5.5y, A1C was
8.2±1.5% (range 6.2-11%) and insulin dose 0.9±0.3 u/kg/day. Glucose control
for the two groups is shown in the Table. The primary outcome of overall percent time in range, 70-180mg/dL, was greater with DIAS, 78.6% vs. 65.4%
in the control group, p=0.003. This was associated with both a reduction
in time spent < 70 mg/dL and > 180 mg/dL. Closed-loop control with DIAS
was effective in reducing both hypoglycemia and hyperglycemia as well as
increasing the percent time spent in range in this cohort of adolescents and
young adults with variable baseline glucose control. The improvement in glucose control was most prominent at night.
Table. Glycemic Outcomes. Results are Man±SE.
OVERALL
Control Group DIAS Closed07:00 - 07:00
(SAP) n= 16
Loop n=17
Mean glucose
156±5
143±3
Percent time between 70-180 mg/dL
65.4±5.3
78.6±2.2
Percent time between 80-150 mg/dL
46.5±3.2
60.0±2.6
Percent time < 70 mg/dL
4.2±0.8
1.8±0.4
Percent time > 180 mg/dL
30.7±3.4
19.8±2.2
Average number of meter glucose
5.4±0.8
4.0±0.7
values < 70 mg/dL
P-Value
0.040
0.003
0.002
0.008
0.011
0.212
Supported By: The Leona M. and Harry B. Helmsley Charitable Trust
ADA-Funded Research
For author disclosure information, see page LB98.
LB25
POSTERS
Exercise significantly increases the risk of hypoglycemia in individuals
with type 1 diabetes (T1D). To reduce exercise-related hypoglycemia, we
developed and tested a wireless bi-hormonal artificial pancreas system that
delivers insulin and glucagon and adjusts dosing after an exercise announcement. In random order, adult subjects with T1D underwent three 20 h sessions: open-loop (OL), closed-loop (CL), and CL with exercise announcement.
Exercise announcement stopped insulin for 30 m, then 50% reduction for
60 m and increased glucagon by 2 fold for 1.5 h. Parameters were selected
based on in silico testing using a glucoregulatory model with an exercise
component. Glucose values from a Dexcom G4 sensor were pushed every
5 m to a Google Nexus phone running the controller. Delivery commands
were sent to 2 t:slim pumps for subcutaneous insulin and glucagon infusion.
Capillary blood glucose levels were measured every 2 h during the day and
every 3 h at night. After an overnight stay, subjects exercised for 45 m at
60% VO2max. Subjects were given 2 meals and carbohydrate amounts were
entered into the controller, which automatically delivered pre-meal insulin.
Subjects wore a Zephyr heart rate monitor and accelerometer. Four (of 24
planned) adult subjects with T1D participated in 7 (of 72 planned) 20 h studies. BG during CL control was 152±46 mg/dl (mean±SEM); daytime BG was
161±51; overnight BG was 135±29. Automated delivery of glucagon successfully prevented BG values from falling below 70 mg/dL in 100% of cases.
Rescue CHO doses were given for BG values <70 mg/dL. No treatments were
needed in any of the 5 CL studies. Five treatments were needed between the
2 OL studies. Preliminary results show that automated insulin and glucagon
delivery effectively controlled glucose levels and prevented hypoglycemia,
including during and after exercise. Testing is ongoing to complete a total of
24 subjects. Future work will incorporate heart rate and accelerometry to
automatically detect exercise.
GREGORY P. WESTCOTT, ETHAN M. BALK, ANASTASSIOS G. PITTAS, Boston, MA,
Providence, RI
Clinical Diabetes/
Therapeutics
PETER G. JACOBS, JOSEPH EL YOUSSEF, NAVID RESALAT, RAVI REDDY, DEBORAH BRANIGAN, NICHOLAS PREISER, JOHN CONDON, JESSICA R. CASTLE,
Portland, OR
96‑LB
Efficacy and Safety of Technosphere Inhaled Insulin: Systematic
Review and Meta-analysis
Clinical Therapeutics/New Technology—Non-Insulin Injectables
100‑LB
weeks vs. 8.245 ± 0.72 at baseline with P ≤ 0.034), fasting C-peptide levels
(1.095 ± 0.215 at 12 weeks vs. 0.245 ± 0.069 at baseline with P ≤ 0.003)
and C-peptide response following a 75-g oral glucose tolerance test (1.817
± 0.27 at 12 weeks vs. 0.504 ± 0.065 at baseline with P ≤ 0.004). Patients of
treatment group A, exhibited significant increases in plasma level of TGF-β1
(26.18 ± 4.39 at 12 weeks vs. 3.68 ± 0.55 at baseline with P ≤ 0.001). Patients of group A, had also exhibited significant increase in plasma levels
of IL-10 from baseline of (3.8535 ± 0.662) to (13.33 ± 1.516) at 12 weeks (P ≤
0.009). Participants of the control group B did not show significant improvement in any of the previously mentioned parameters at any time point of the
study period. Administration of (CF-CB-MSCs) microvesicles is safe and can
ameliorate autoimmunity and regenerate β cell mass in T1DM patients. Trial
registration: ClinicalTrials.gov number NCT02138331.
Medtronic’s Hybrid Closed-Loop System—An Evaluation of Meal
Dosing
POSTERS
Clinical Diabetes/
Therapeutics
BENYAMIN GROSMAN, ANIRBAN ROY, GAYANE VOSKANYAN, NATALIE KURTZ,
DI WU, NEHA PARIKH, REBECCA GOTTLIEB, KRISTEN HUGHES, SARAH MCKENNEY, RONALD BRAZG, FRANCINE KAUFMAN, Northridge, CA, Renton, WA
Medtronic’s hybrid closed-loop system (HCL) requires that patients provide an estimate of the carbohydrate content of upcoming meals; the system
then calculates an appropriate meal bolus based on a pre-specified insulin:
carbohydrate ratio (CR). It was hypothesized that standardized and relatively
aggressive CRs could significantly improve the system’s performance by reducing postprandial hyperglycemia without increasing the risk of hypoglycemia. Ten subjects (4 male, mean ages 50±15) wore Medtronic’s HCL system
(composed of next generation insulin pump and sensor technologies) with
the embedded HCL algorithm for 12 consecutive days in a monitored setting. The clinical trial consisted of three phases: 4 open-loop control days,
4 days with the HCL system using the subjects’ previous pump CRs, then 4
days in HCL with CRs determined using 300 divided by the total daily dose
(300 Rule). Subjects consumed standardized meals on day 2 (open-loop), day
6 (closed-loop with previous pump CRs) and day 10 (closed-loop with CRs
using the 300 Rule). On days 2, 6, and 10, the average sensor glucose (SG)
values were 162±16, 157±12 and 148±8 mg/dL, peak post-prandial SG values
after the standardized meals were 210±44, 224±51 and 194±41 mg/dL, and
the percentage of SG values between 70-180 mg/dL range were 66±16%,
73±12%, and 79±6%, respectively. The percentage SG values <70mg/dl in
the three phases were: 1.6±1.8%, 0.4±0.45%, and 0.9±0.5%, respectively.
The average Insulin delivered in anticipation of a standard meal at day 6
and 10 were 4.75±4.4, and 5.76±4.85 U and the average CRs were 13.1±4.9
and 10.2±4.4 U/g carbohydrate, respectively. The use of a standardized and
relatively low CR resulted in higher pre-meal bolus doses and greater reductions in postprandial hyperglycemia. This was achieved without increasing
the risk of hypoglycemia in the Medtronic HCL system.
103‑LB
Withdrawn
101‑LB
Dose Safety Artificial Pancreas Controller Use in Ad Lib Living
Studies
RICHARD MAUSETH, DON MATHESON, ROBERT KIRCHER, Redmond, WA
The Dose Safety artificial pancreas fuzzy logic dosing controller (FLC) is
designed to reduce the high cognitive load on people with diabetes. In an attempt to better understand the dynamics of our FLC, we conducted sixteen 8
hour daytime ad lib living studies on five subjects in the CRC. Subjects were
asked to perform their usual daily routine as much as possible, and were
allowed to eat and exercise as they wished. Subjects had repeated studies.
No pre meal boluses or meal or exercise notifications were given. Mean CHO
intake was 110 gram range (33-190 grams). Mean exercise performed was
22 minutes range (0-84 minutes). In spite of this wide range of CHO intake
and exercise periods, 36.9% of the time the subject’s glucose was within the
70-180mg/dL range. The average glucose was 183mg/dL during the hardest
time of day to handle. For each meal we compared the FLC actual dosing
with what the subjects would have dosed. We found that the FLC delivered
68% of the subject own dosing within the first hour and 102% in the first two
hours post meal. The FLC was revised based on the subjects own dosing.
Open loop regression tests of the revised controller using the clinical data
showed that 87% of the subject’s usual dose in the first hour, again with no
pre meal bolus or meal notification. We believe this revision will significantly
improve the time in range and average blood glucose.
104‑LB
Liraglutide Causes Massive and Rapid Reduction of Cardiac Fat In‑
dependent of Weight Loss in Type 2 Diabetes
GIANLUCA IACOBELLIS, SUZY BIANCO, MAHSHID MOHSENI, Miami, FL
Epicardial adipose tissue (EAT) is a unique visceral fat depot with peculiar
anatomical, bio-molecular features and growing clinical applications. EAT
can be measured using standard ultrasound and its thickness is an accurate
marker of visceral fat and an emerging therapeutic target. EAT is higher in
subjects with type 2 diabetes when compared to controls. Liraglutide, an
analogue of glucagon-like peptide-1 (GLP-1RA) can improve glycemic control
and cause weight loss in type 2 diabetic patients. Nevertheless, whether
Liraglutide-related weight loss and improved metabolic profile can be attributed to a visceral fat loss is unknown and unexplored. We sought to test
the hypothesis that Liraglutide causes a rapid and significant reduction in
EAT in well controlled overweight/obese type 2 diabetic patients. This was
a 6-month interventional case-controlled study in type 2 diabetic subjects
with body mass index (BMI) > 27 kg/m2 and Hemoglobin A1c (HbA1c) ≤ 8% on
metformin monotherapy. Individuals were randomized in 2 groups to receive
additional Liraglutide up to 1.8 mg sc once daily or to remain on Metformin up
to 1 g twice daily. EAT thickness was measured at baseline, 3 and 6-month
follow up visits. Currently, 35 patients completed the 6-month study. In the
Liraglutide group, EAT decreased from 10.2±2 to 6.9±1.9 and 5.8±1.9 mm (p<
0.001) after 3 and 6 months, respectively, accounting for a -42% of reduction
at 6 months, whereas there was no EAT reduction in the Metformin group;
BMI decreased from 33±7 to 31.8±4 and 31.7±4 kg/m2 and HbA1c lowered
from 6.6±0.8 to 5.7±0.7 and 5.4±0.8% in the Liraglutide group, reflecting -7%
and -18% of reduction, respectively. Our preliminary results indicate that
Liraglutide causes a massive and rapid cardiac fat loss in overweight/obese
type 2 diabetic patients, independently of overall weight loss and improved
Clinical Therapeutics/New Technology—
Non-Insulin Injectables
102‑LB
Effect of Cell-Free Mesenchymal Stem Cells Microvesicles (MVs)
and Exosomes Therapy on β-Cell Mass in Type 1 Diabetes Mellitus
(T1DM)
WAEL F. NASSAR, Cairo, Egypt
Type 1 diabetes (T1D) is an immunological mediated disease. The clinical applications of cord blood stem cells and their microvesicles have been
regarded as a crucial means of intercellular communication and their ability to ameliorate autoimmunity have increased enormously in recent years.
Twenty nine T1DM patients were enrolled into two groups; (group A) 20 patients, were treated with 2 doses of cell-free cord-blood mesenchymal stem
cells derived microvesicles and (group B) 9 patients, as matching placebo
group. Participants in Group A exhibited improved HbA1c (6.67 ± 0.321 at 12
ADA-Funded Research
For author disclosure information, see page LB98.
LB26
Clinical Therapeutics/New Technology—Non-Insulin Injectables
106‑LB
glucose control. GLP-1RA effects may be therefore visceral fat specific.
These data are of great novelty and immediate clinical application.
Glucagon Receptor Antibody LY2786890 Reduced Glucose Levels in
Type 2 Diabetes Mellitus Patients
Supported By: Novo Nordisk
Glucagon levels are often elevated in type 2 diabetes mellitus (T2DM)
and may contribute to hyperglycemia. LY2786890 (LY) is a humanized IgG4
monoclonal glucagon receptor antibody that displays antagonistic activity
against the human glucagon receptor. A Phase 1, randomized, double-blind,
placebo-controlled study examined the safety and efficacy of single doses
of LY in healthy subjects (N=10, intravenous [IV] 0.05 mg/kg) and T2DM patients (N=44; IV 0.05, 0.1, 0.3, 0.55 mg/kg; subcutaneous [SC] 0.1, 0.55 mg/
kg; mean fasting blood glucose [FBG] 126 mg/dL; hemoglobin A1c 7.3%). LY
was safe and well tolerated. Hypoglycemia was infrequent and mild. Dose
dependent elevations in aminotransferase levels were seen in T2DM patients; levels returned to baseline during follow-up with no clinical signs
of liver injury or significant elevations in bilirubin or alkaline phosphatase.
Pharmacokinetic and pharmacodynamic (PD) profiles of LY supported once
weekly SC dosing. The half-life (4 to 26 days) and PD time-action were concentration dependent. Absolute bioavailability after SC administration was
estimated to be 50%. In T2DM patients, LY significantly reduced FBG (Figure)
and increased plasma glucagon up to approximately 3-fold by day 2. As seen
with oral glucagon receptor antagonists, these data demonstrate that blocking glucagon action effectively lowers blood glucose in T2DM subjects.
STEFANO DEL PRATO, JAHOON KANG, SOOMIN CHOI, WOOHYUNG LEE, OAKPIL HAN, SIYOEN KIL, KYUHOON GEE, IN YOUNG CHOI, SE CHANG KWON, MICHAEL TRAUTMANN, MARCUS HOMPESCH, Pisa, Italy, Seoul, Republic of Korea,
Hwaseong, Republic of Korea, Hamburg, Germany, Chula Vista, CA
HM11260C (HM) is a novel ultra-long acting GLP-1R agonist with a T1/2
of ~ 158 hrs. This 16-week, randomized, placebo (PBO) controlled, doubleblind parallel group study was designed to investigate efficacy, safety, and
tolerability of a range of once monthly (QM) HM doses in subjects with
T2DM. We report interim data from 86 patients (mean age 56 yrs, BMI 32.1
kg/m2, T2DM duration 95.4 months) out of 209 patients with unsatisfactory
glycemic control while on a stable dose of metformin (≥ 3 months) before entering this study. Patients were randomized to one of three HM QM doses (8,
12 and 16 mg) or PBO, followed by a 4-week titration period. Overall, all HM
doses produced remarkable reductions in HbA1c, fasting plasma glucose,
and 7-point daily glucose (Table 1). Percentage of patients on HM achieving
A1c Target < 7% was 73.3% (8 and 16 mg) and 64.3% (12 mg) vs. 22.2% on
PBO. With HM, the reduction in body weight ranged from 2.16% to 2.80% vs.
1.24% on PBO. The most frequent AEs in HM-treated patients were mild or
moderate gastrointestinal events. No increase in heart rate was recorded.
All QM doses of HM demonstrated clinically meaningful improvement in
blood glucose and body weight loss. The current results will have to be confirmed upon completion of the trial and warrant further studies to evaluate
the long-term efficacy and safety of a monthly regimen with HM in T2DM.
107‑LB
Advancing Basal Insulin Glargine with Prandial Lixisenatide QD vs.
Insulin Glulisine QD or TID in T2DM: The GetGoal-Duo2 EvidenceBased Trial (NCT01768559)
JULIO ROSENSTOCK, MARKOLF HANEFELD, SANDRO GENTILE, RONNIE ARONSON, FRANCISCO J. TINAHONES, BRUNO GUERCI, CHRISTINE ROY-DUVAL, ELISABETH SOUHAMI, MAREK WARDECKI, JENNY YE, SIMON HELLER, ON BEHALF
OF THE GETGOAL-DUO2 STUDY INVESTIGATORS, Dallas, TX, Dresden, Germany,
Naples, Italy, Toronto, ON, Canada, Málaga, Spain, Vandœuvre-lès-Nancy, France,
Paris, France, Warsaw, Poland, Bridgewater, NJ, Sheffield, United Kingdom
To provide evidence on how to advance basal insulin (BI), we explored
treatment options in poorly controlled, BI-treated (≥6 mo ± 1-3 OADs), predominantly obese adults with T2DM randomized to lixisenatide 20 µg QD (LIXI),
insulin glulisine QD (GLU-1), or GLU TID (GLU-3), all added to insulin glargine (IG)
± metformin, if HbA1c remained >7-9% after a 12-week IG optimization run-in
period after stopping other OADs. Co-primary endpoints at 26 weeks were (1)
non-inferiority (95% CI upper bound <0.4%) in HbA1c reduction with LIXI vs.
GLU-1 and (2) for LIXI vs. GLU-3, either non-inferiority in HbA1c reduction (2a) OR
superiority (one-sided α=0.025) in body weight change (2b). FPG, PPG, IG dose,
AEs, and hypoglycemia were assessed. Each arm randomized 298 pts (T2DM
duration 12 yrs, BI duration 3 yrs, weight 89 kg). All co-primary endpoints were
met as LIXI was non-inferior to GLU-1 and GLU-3 for HbA1c reductions and statistically superior to both for body weight loss (Table). Documented hypoglycemia was numerically and significantly lower with LIXI than with GLU-1 and
GLU-3, respectively. In conclusion, BI plus LIXI may become a preferred option
to advance BI, attaining meaningful glycemic targets with less hypoglycemia
and without negative impact on weight vs. prandial insulin as Basal Plus or
Basal Bolus for uncontrolled, BI-treated T2DM.
ADA-Funded Research
For author disclosure information, see page LB98.
LB27
POSTERS
Once-a-Month Treatment with HM11260C Improves Glycemic
Control in Type 2 Diabetes (T2DM)—Interim Data from a 16-Week
Study
Clinical Diabetes/
Therapeutics
RONAN P. KELLY, PARAG GARHYAN, VINCENT L. REYNOLDS, JENNIFER A. MARTIN, CHENG CAI TANG, KWEE POO YEO, THOMAS A. HARDY, Singapore, Singapore, Indianapolis, IN
105‑LB
Clinical Therapeutics/New Technology—Oral Agents
Clinical Therapeutics/New Technology—
Oral Agents
109‑LB
POSTERS
Clinical Diabetes/
Therapeutics
Withdrawn
110‑LB
Low Dose Pioglitazone on Glycemic Control and Insulin Resistance
in Type 2 Diabetes: A Randomised, Double-Blind, Clinical Trial
DEBASISH HOTA, SUJIT RAJAGOPALAN, AMITAVA CHAKRABARTI, PINAKI DUTTA, ANIL BHANSALI, Bhubaneswar, India, Chandigarh, India
Objective: To evaluate the antihyperglecemic and anti insulin sensitising
effects of low dose pioglitazone (7.5 mg) along with characterisation of its
adverse effect profile.
Methods: This was a randomised, double blind, single centre study comparing the effects of three doses (7.5 mg, 15 mg and 30 mg) of pioglitazone
over a period of 12 weeks. We recruited 90 patients who were allocated
to the three groups in (1:1:1) fashion. HbA1c, FPG, PPG, FPI, C-peptide, Adiponectin, Leptin, Weight, Waist circumference, Body fat, haematological
and biochemical parameters were measured at baseline and at the end of
12th week. ITT analysis was done.
Results: Significant reduction in HbA1c was seen with Pioglitazone 7.5 mg,
15 mg and 30 mg, with a mean reduction of -0.5 ± 0.1%, -0.6 ± 0.2 and -0.7
± 0.1 respectively. There was a significant reduction in FPG and PPG in all
three groups. Pioglitazone 7.5 was also able to cause significant reduction
in insulin, c-peptide and increase in adiponectin levels similar to its 15 mg
and 30 mg doses. Moreover, there was significantly less weight gain and
increase in body fat in the 7.5 mg group as compared to 30 mg group. There
were no changes in hepatic or renal function.
Conclusions: Pioglitazone 7.5 mg is as efficacious as higher doses of 15 mg
and 30 mg and has lesser side effects. Hence it is better to start therapy at
a lower dose of pioglitazone in patients.
108‑LB
A Monoclonal Anti-aP2 Antibody Treats Diabetes and Ameliorates
Fatty Liver Disease in Obese Mice
MEHMET FURKAN BURAK, KAREN INOUYE, ARIEL WHITE, CARL DOYLE, DAN
LIGHTWOOD, LOUISE HOWELLS, GEOFREY ODEDE, HANNA HAILU, SHAUNA
WEST, ALISON CLARGO, HELEN NEALE, RACHEL GARLISH, ADRIAN MOORE,
GÖKHAN S. HOTAMISLIGIL, Boston, MA, Slough, United Kingdom
The lipid chaperone aP2/FABP4 has been implicated in the pathology of
many immunometabolic diseases, such as diabetes and atherosclerosis.
While multiple lines of evidence also supports its involvement in human
disease, targeting aP2 for therapeutic applications have not yet been accomplished. Recent studies in our laboratory have shown that aP2 is not
simply an intracellular protein binding lipids but an active adipokine that
contributes to hyperglycemia by promoting hepatic gluconeogenesis and
interfering with peripheral insulin action. Multiple groups have now demonstrated that serum aP2 levels are markedly elevated in mouse models of
obesity, and human serum aP2 levels strongly correlate with BMI, insulin resistance, dyslipidemia, and cardiovascular risk. Importantly, blocking aP2 in
preclinical models showed strong anti-diabetic activity. These observations
raised an exciting new strategy for targeting serum aP2 to treat metabolic
disease with a monoclonal anti-aP2 antibody. Here, we report the identification of a highly effective, anti-aP2 mAb, CA33, and the characterization of
its effects in vivo. Treatment of mice with dietary or genetic obesity with
CA33 lowered fasting blood glucose levels, improved glucose metabolism,
increased systemic insulin sensitivity and reduced fat mass and liver steatosis. In hyperinsulinemic-euglycemic clamp studies, we found that the
anti-diabetic effect of CA33 was predominantly linked to the regulation of
hepatic glucose output and peripheral glucose utilization. We also examined
the properties of this antibody by structural and biochemical studies, identified its target epitopes, and demonstrated its target specificity. We conclude
that development of an anti-aP2 monoclonal antibody-mediated therapeutic
is a feasible approach and would constitute a strong candidate for the treatment of diabetes and fatty liver disease.
111‑LB
Cardiovascular Outcome Trial with Fasiglifam, a Novel Selective
GPR 40 Agonist
VENU MENON, A. MICHAEL LINCOFF, STEPHEN NICHOLLS, PRABHAKAR VISWANATHAN, DARREN K. MCGUIRE, THEODORE MAZZONE, BERNARD ZINMAN,
ANTONIO CHACRA, JOHN BETTERIDGE, JULIO ROSENSTOCK, CYRUS MEHTA,
SUSAN JASPER, JOHN MARCINAK, CLAUDIA LOPEZ, STEVEN E. NISSEN, Cleveland, OH, Adelaide, Australia, Deerfield, IL, Dallas, TX, Chicago, IL, Toronto, ON,
Canada, São Paulo, Brazil, London, United Kingdom, Cambridge, MA
Fasiglifam (FG) is a compound that potentiates glucose-stimulated insulin
secretion via selective agonism of the G protein-coupled receptor 40. We
designed a double blind, multicenter, international cardiovascular outcome
trial (CVOT). We planned to enroll approximately 5000 subjects with T2D
(HbA1c 7-10.5%) with either “high risk” factors (prior MI, symptomatic PAD,
or stroke >2 but < 24 months of enrollment) or “intermediate risk” criteria.
Trial subjects received either FG 50 mg or placebo once daily in addition
to standard of care. Subjects with ALT/AST > 3x ULN, bili > 1x ULN, HIV,
or active Hep B/C were excluded. The 10endpoint was time to first occurrence of any component of the MACE composite of CV death, MI, stroke
or hospitalization for unstable angina. The study was terminated early by
Supported By: UCB Pharmaceuticals
ADA-Funded Research
For author disclosure information, see page LB98.
LB28
Clinical Therapeutics/New Technology—Oral Agents
DMC after enrollment of 3207 subjects with a mean exposure of 221±134
days for observed risks of hepatotoxicity that appeared to outweigh potential benefits. The mean age was 63 ± 9 years, 65.5% of subjects were male,
mean HbA1c was 8.3±0.9% and mean duration of T2D was 13±8 years. At 6
months, the median HbA1c on FG decreased 0.8% compared to 0.4% with
placebo (P <0.001). The number of subjects who had elevated ALT >3×ULN
during double blind treatment was higher in the FG than in the placebo group
(32/1601 [2.0%] vs. 6/1603 [0.4%]), as were the number with elevated ALT
>5×ULN (17/1601 [1.1%] vs. 1/1603 [0.1%]) and with elevated ALT >10×ULN
(5/1601 [0.3%] vs. 1/1603[0.1%]). There were no cases of Hy’s law but 1 subject in FG arm had ALT >3xULN and total bili1.6xULN with no alternative
etiology. The 10endpoint occurred in 40 subjects (2.5%) in each arm, RR for
FG vs.placebo of 0.99 (95% CI: 0.641, 1.539), p=0.98. Whether the liver injury
represents a specific drug or class effect with this novel target remains uncertain. Rates of CV endpoints were comparable for FG and placebo groups.
Long term CVOT in T2D contribute to understanding the overall safety profile
of a compound.
and 48% (P=0.06) respectively, but had no effect on tissue ceramide
content. Increased PKC-epsilon and PKC-theta activity play a major role
in promoting liver and muscle insulin resistance and consistent with the
improvement in whole body insulin sensitivity. CRMP treatment reduced
PKC-epsilon in liver and PKC-theta activity in muscle by ~50% (P<0.05) and
70% (P<0.05) respectively. In conclusion these data support the potential
utility of CRMP for the treatment of NAFLD, NASH and T2D in the setting
of severe lipodystrophy.
114‑LB
Baricitinib in Diabetic Kidney Disease: Results from a Phase 2, Mul‑
ticenter, Randomized, Double-Blind, Placebo-Controlled Study
TRPA1 Calcium Channel Activators as Novel GLP-1 Secretagogues
JIMMY WU, OLEG G. CHEPURNY, COLIN LEECH, HUI LI, XINPING HAN, GEORGE
G. HOLZ, Hanover, NH, Syracuse, NY, Dallas, TX
Orally administrable blood glucose-lowering agents that exert their effects by stimulating GLP-1 release from intestinal L-cells may constitute
a new means by which to treat patients with diabetes mellitus. Here, we
report the synthesis, characterization, and target validation of JWU-A021,
a small molecule cycloalka[b]indole that stimulates GLP-1 release and that
is synthesized by means of a novel 3 component coupling reaction in which
each component is independently varied (Han et al., ACIE, 2012). JWU-A021
is orally bioavailable in mice, and it exerts a GLP-1 secretagogue action by
virtue of its ability to activate TRPA1 calcium channels. Using intestinal STC1 cells that express TRPA1, we find that JWU-A021 activates voltage-independent calcium currents, an effect also measurable in HEK cells transfected
with TRPA1. For both STC-1 and HEK cells, a dose-dependent, sustained, and
reversible increase of calcium concentration is measured in response to
JWU-A021, and this effect is blocked by the TRPA1 antagonists HC-030031,
A-967079, and AP-18. Using HEK cells transfected with a mutant TRPA1, we
find that JWU-A021 activates TRPA1 independently of covalent channel
modification. The binding site for JWU-A021 on TRPA1 is enantiodiscriminatory since (+)-JWU-A021 elicits a more robust response than that of (-)-JWUA021. Notably, JWU-A021 stimulates GLP-1 release from STC-1 cells (EC50
2 microM), as is also the case for the structurally related compounds JWUA019 and JWU-A020 that activate TRPA1. The GLP-1 secretagogue action of
JWU-A021 is measurable at both 5 and 25 mM extracellular glucose, and it
is potentiated by cAMP-elevating agents (forskolin, IBMX). Since G proteincoupled receptors for fatty acid amides (GPR119) and bile acids (TGR5) are
linked to cAMP production in L-cells that express TRPA1, these new findings suggest a drug treatment strategy in which cycloalka[b]indoles such as
JWU-A021 are administered in combination with a GPR119 or TGR5 agonist
so that L-cell GLP-1 secretion is fully stimulated.
Supported By: National Institutes of Health (1R01GM111638-01)
113‑LB
A Novel Extended-Release Mitochondrial Protonophore Reverses
Diabetes in Lipoatrophic Mice
ABUDUKADIER ABULIZI, RACHEL J. PERRY, NASIRI ALI, MICHAEL J. JURCZAK,
GERALD I. SHULMAN, New Haven, CT
Supported By: Eli Lilly and Company
Non-alcoholic fatty liver disease (NAFLD) is a major factor in the
pathogenesis of type 2 diabetes (T2D) and non alcoholic steatohepatitis
(NASH). Recently, we showed that a controlled-release oral formulation
of 2,4-dinitrophenol (CRMP) reversed insulin resistance, hyperglycemia as
well as hepatic steatosis and liver inflammation in rat models of T2D and
NASH without adverse effects (Perry et al. Science 2015). We hypothesized
that CRMP would also be effective in reversing insulin resistance and NAFLD/NASH in a transgenic (A-ZIP/F-1) mouse model of severe lipodystrophy. Consistent with this hypothesis we found that CRMP treatment (2mg/
kg/d x 3 wks) decreased plasma glucose and insulin concentrations in AZIP
mice by 50-60% (P<0.01) during an intraperitoneal glucose tolerance test
compared to controls. CRMP-induced improvement in glucose tolerance
and insulin sensitivity was associated with 50% reductions in liver triglyceride content and reduced liver inflammation as reflected by 30-45%
reductions in plasma AST and ALT concentrations and occurred independently of any changes in activity, food intake, energy expenditure or body
weight and was unassociated with any adverse effects. Furthermore,
CRMP reduced liver and muscle diacylglycerol content by 36% (P<0.001)
115‑LB
Comparative Effectiveness and Safety of Monotherapy and Add-on
Therapy to Metformin in Type 2 Diabetes: An Updated Systematic
Review and Meta-analysis
NISA M. MARUTHUR, EVA TSENG, LISA WILSON, SUSAN HUTFLESS, EMANNUEL IYOHA, CATALINA SUAREZ-CUERVO, ZACK BERGER, JODI SEGAL, SHARI
BOLEN, Baltimore, MD, Cleveland, OH
Given the recent approval of many new glucose-lowering drugs for type
2 diabetes, we updated the 2011 AHRQ-funded report about their comparative effectiveness. We searched the MEDLINE®, Embase™, and Cochrane
databases through July 2014 for articles evaluating the effects of monotherapy (metformin [MET], thiazolidinediones [TZDs], sulfonylureas [SUs], GLP-1
agonists, DPP-4 inhibitors, SGLT-2 inhibitors) and MET-based combinations
(MET + any other class) on long-term, intermediate, or adverse outcomes.
We included 115 new studies (total 229 studies). Cardiovascular (CV) mortality was 37-50% lower for MET compared to SUs; CV morbidity was also
ADA-Funded Research
For author disclosure information, see page LB98.
LB29
POSTERS
Diabetic kidney disease (DKD) is the foremost cause of end-stage renal
disease. New therapeutic strategies are needed as standard care fails to
prevent progressive DKD. Baricitinib (bari) is a small-molecule inhibitor of
Janus kinases 1 and 2. This ph 2 study examined if bari treatment decreased
levels of urine albumin in patients at high-risk for progressive DKD. Study
participants (n=129) received standard care and were randomized (1:1:1:1:1)
to bari (0.75 mg QD, 0.75 mg BID, 1.5 mg QD, 4 mg QD) or placebo (PBO) for
6 months (mos) followed by a washout period of 4 weeks. Baseline 24 hr
urine albumin-to-creatinine ratio (UACR) (median [interquartile range]) was
886 (488-1643) mg/g. Reductions in 24 hr UACR were observed at 3 and 6
mos (Figure). Baseline estimated glomerular filtration rate (cystatin C based)
was 49±23.2 ml/min/1.73 m2 (mean±SD) and did not change in any group.
Inflammatory markers, including urinary interferon gamma-induced protein
10 and plasma soluble tumor necrosis factor receptor 2, decreased in a dosedependent manner suggesting an anti-inflammatory mechanism to reduce
albuminuria. At 6 mos, only the highest bari dose group had a decrease in hemoglobin compared to PBO (-1.0±0.35, g/dL) (difference in LSM±SE). Adverse
events of anemia were also more frequent in bari 4 mg (8/25) vs. PBO (1/27).
These results encourage further study of bari as a new therapy for DKD.
112‑LB
Clinical Diabetes/
Therapeutics
KATHERINE TUTTLE, FRANK C. BROSIUS III, SHARON G. ADLER, MATTHIAS
KRETZLER, RAVINDRA L. MEHTA, JAMES A. TUMLIN, JIAJUN LIU, MARIA E.
SILK, TRACY E. CARDILLO, KEVIN L. DUFFIN, JOSEPH V. HAAS, WILLIAM L. MACIAS, JONATHAN M. JANES, Spokane, WA, Ann Arbor, MI, Torrance, CA, San Diego, CA, Chattanooga, TN, Indianapolis, IN
Clinical Therapeutics/New Technology—Oral Agents
lower for this comparison. Most monotherapy medications decreased HbA1c
similarly except DPP-4 inhibitors which had a lesser effect. MET-based combinations lowered HbA1c by 0.7-1% vs. MET alone. MET, GLP-1 agonists,
and SGLT-2 inhibitors caused weight loss vs. SUs and TZDs which caused
weight gain. SGLT-2 inhibitors reduced systolic blood pressure by 3-5 mm
Hg and increased the risk of genital mycotic infections vs. other drugs. SUs
increased the risk of hypoglycemia vs. other drugs; SGLT-2 inhibitors caused
less hypoglycemia than MET. MET caused more gastrointestinal side effects
vs. other drugs except GLP-1 agonists which increased vomiting vs. MET.
Evidence on microvascular and other adverse outcomes was sparse. While
the comparative long-term benefits and harms of most diabetes medications
remain unclear, the evidence suggests that MET is associated with lower
CV mortality and morbidity compared to SUs. Given the similar short-term
glycemic effects and differential effects on other outcomes of interest
(e.g., weight, hypoglycemia, GI side effects, and infections) by drug class,
our updated synthesis should help clinicians and patients choose diabetes
medications collaboratively and prioritize patient concerns related to specific benefits and harms.
2. Episodes of Hypoglycemia/pt/24 hours in CGM at start and end of therapy
Overall hypoglycemia (< 70 mg/dl)
0.28 + 0.9
0.31 + 0.6
0.05
Overall Severe hypoglycemia (< 50 mg/dl)
Nocturnal Hypoglycemia
0.05 + 0.2
0.07 + 0.2
NS
(< 70 mg/dl, 12 midnight-6 am)
0.06 + 0.2
0.09 + 0.1
NS
Nocturnal Severe hypoglycemia
(< 50 mg/dl)
0.02 + 0.0
0.03 + 0.1
NS
3. Duration of Hypoglycemia in Minutes/ 24 hrs in CGM start and end of
therapy
A: Overall hypoglycemia
All Hypoglycemia < 70 mg/dl
18.8 + 70.0 21.3 + 51.3
NS
Mild Hypoglycemia 50-69 mg/dl
8.9 + 29.2 12.1 + 25.9 0.04
Severe Hypoglycemia < 50 mg /dl
9.8 + 44.8
9.2 + 36.7
NS
B: Nocturnal Hypoglycemia (12 midnight-6 am)
All Hypoglycemia < 70 mg/
8.1 + 31.7
9.2 + 31.7
NS
Mild Nocturnal Hypoglycemia
2.6 + 10.7
4.2 + 12.4
NS
50-69 mg/dl
Severe Nocturnal Hypoglycemia
5.5 + 23.7
5.0 + 29.1
NS
< 50 mg /dl
4. Area Over the Curve (AOC) of Hypoglycemia in CGM start and end of
therapy (mg/dl.min)
A: Overall hypoglycemia AOC
All Hypoglycemia < 70 mg/dl AOC
74.5 + 317.7 71.7 + 233.8 NS
Mild Hypoglycemia 50-69 mg/dl AOC
57.6 + 243.7 56.3 + 171.3 NS
Severe Hypoglycemia < 50 mg /dl
16.9 + 75.1 15.4 + 64.3
NS
B: Nocturnal Hypoglycemia (12 midnight-6 am) AOC
All Hypoglycemia < 70 mg/dl AOC
37.4 + 156.1 35.6 + 173.7 NS
Mild Nocturnal Hypoglycemia
27.9 + 115.8 26.5 + 119.9 NS
50-69 mg/dl AOC
Severe Nocturnal Hypoglycemia
9.5 + 41.7
9.1 + 54.4
NS
< 50 mg /dl
*CGM are expressed either as combination of start and follow up data or
separately.
116‑LB
POSTERS
Clinical Diabetes/
Therapeutics
Supported By: HHSA290201200007I
Hypoglycemia (Hypo) during Therapy (Rx) of New Onset Type 2 Dia‑
betes (DM2) Patients (Pts) Presenting with Severe Hyperglycemia:
Comparison of 2 Protocols
AMBIKA AMBLEE, DANIEL LIOUS, ZACHARIAH SHEBANI, LEON FOGELFELD,
Chicago, IL
To test hypo occurrence with Continuous Glucose Monitoring (CGM) in 2
simple oral Rx in newly diagnosed DM2 pts presenting with severe hyperglycemia. Open label, RCT of 100 adult DM2 pts with blood glucose (BG) levels
of 300-450 mg/dl at a public hospital. Pts were randomized to Glipizide XL (G
group {gp}) versus (vs.) Kombiglyze XR, the saxagliptin/metformin fixed-dose
combination (K gp). Three -5 day CGM was performed at start (1st week of
Rx) and at the end of study (12 weeks). Data are available for 77 pts at start
and 53 pts at the end of the study. Baseline characteristics and glycemic
control (A1c) at the end of the study were similar, K gp 10.8 to 6.8%; G gp
11.0 to 6.9%. Hypoglycemia incidence and episodes (epi) in patients by selfmonitored BG were lower in the K gp, (8.9% vs. 25%; 4 vs. 27). The CGM data
(Table) indicate that overall incidence of hypos, the episodes of hypo/pt/24
hours and the duration of mild hypos were lower in K gp. There were hypos
at start of Rx in both gps including nocturnal and severe hypos. Glipizide XL
and Kombiglyze XR Rx improved severe hyperglycemia in newly diagnosed
DM2 patients. Hypoglycemia, including nocturnal and severe, was present
within the 1st week of therapy in both gps. The Kombiglyze XR gp had less
hypoglycemia at the end of the study. Hypoglycemia can occur early after Rx
initiation in newly diagnosed pts with severe hyperglycemia.
Supported By: AstraZeneca/Bristol-Myers Squibb
117‑LB
MARCH Sub-analysis: Influential Factors for Efficacy of Acarbose
and Metformin as Initial Therapy in Chinese Patients with Newly
Diagnosed Type 2 Diabetes
WENYING YANG, JINPING ZHANG, Beijing, China
MARCH trial demonstrated that as initial therapy for Chinese newly diagnosed T2DM patients, acarbose and metformin has similar efficacy in HbA1c
reduction and there was no difference in the proportion of patients with HbA1c
≤ 7% between those two treatment. We aimed to investigate whether specific characteristics were associated with treatment efficacy for either drug. All
patients (n=657) randomly assigned to acarbose or metformin treatment were
divided into two groups based on HbA1c levels at the end of 48 weeks followup: HbA1c <7% and HbA1c ≥7%. Univariate, multivariate, and stepwise linear
regression analysis were applied to identify factors associated with treatment efficacy. Univariate analysis revealed that the efficacy of acarbose and
metformin were influenced by baseline glucose level and the change of BMI
(P≤0.006). And the efficacy of acarbose was also associated with age, gender
and AUC of insulin, while for metformin treatment, the efficacy was also associated with baseline diastolic blood pressure, HDL-C and β cell function (HOMA-B). Multivariate and stepwise regression model analyses revealed that
lower baseline 2hPPG and more change of BMI are protect factors for efficacy
in both treatment group (P≤0.05). And the efficacy of acarbose treatment was
also increased with baseline AUC of serum insulin, while for metformin treatment, the efficacy was also increased with baseline diastolic blood pressure
and HDL-C (P≤0.05). Stepwise regression model analysis demonstrated that,
except for baseline 2hPPG and the change of BMI, lower baseline HOMA-IR
and higher AUC of serum insulin are also protect factors for HbA1c normalization for all patients (P≤0.001). Newly diagnosed T2DM patients with lower
2hPPG and HOMA-IR, higher insulin level are more likely to achieve glucose
control. And the change of BMI or body weight after acarbose or metformin
treatment is also an influential factor for treatment efficacy.
Table. *CGM Hypoglycemia Data (adjusted for 24 hours).
K Group
G Group P-value
1. Incidence of Hypoglycemia (% of Patients)
A: Overall hypoglycemia (< 70 mg/dl)
Hypoglycemia
9/44 (20.4%) 18/43 (41.8%) 0.03
(CGM at start and end of study)
—Hypoglycemia (CGM start of therapy) 4/40 (10%)
5/37 (13.5%) NS
—Hypoglycemia (CGM end of therapy) 5/25 (20%) 13/28 (46.5%) 0.04
B: Nocturnal Hypoglycemia (< 70 mg/dl from 12 midnight-6 am)
Nocturnal hypoglycemia
5/44 (11.3%) 9/43 (20.9%) NS
(CGM at start and end of study)
—Nocturnal Hypoglycemia
3/40 (7.5%) 3/37 (8.1%) NS
(CGM start of therapy)
—Nocturnal Hypoglycemia
2/25 (8%)
6/28 (21%)
NS
(CGM end of therapy)
C: Severe hypoglycemia (< 50 mg/dl)
Severe hypoglycemia
3/44 (6.8%) 5/43 (11.6%) NS
(CGM at start and end of study)
—Severe Hypoglycemia
2/40 (5%)
2/37 (5.4%) NS
(CGM start of therapy)
—Severe Hypoglycemia
1/25 (4%)
3/28 (10.7%) NS
(CGM end of therapy)
D: Severe Nocturnal hypoglycemia (< 50 mg/dl)
Nocturnal Severe hypoglycemia
3/44 (6.8%) 3/43 (6.9%) NS
(CGM at start and end of study)
— Nocturnal Severe Hypoglycemia
2/40 (5%)
2/37(5.4%) NS
(CGM start of therapy)
— Nocturnal Severe Hypoglycemia
1/25(4%)
1/28(3.5%) NS
(CGM end of therapy)
ADA-Funded Research
For author disclosure information, see page LB98.
LB30
Clinical Therapeutics/New Technology—Oral Agents
118‑LB
Table.
Influence of Baseline HbA1c, BMI, β-cell Function, and Insulin Sen‑
sitivity on the Treatment Response of Empagliflozin (EMPA) in Pa‑
tients with Type 2 Diabetes (T2DM)
MARTIN RIDDERSTRALE, ULRICH ELSASSER, CORDULA ZELLER, STEFAN HANTEL, AFSHIN SALSALI, ULI BROEDL, Gentofte, Denmark, Ingelheim, Germany, Biberach, Germany, Ridgefield, CT
EMPA, a potent, selective sodium glucose cotransporter 2 inhibitor, inhibits renal glucose reabsorption, leading to glucosuria and improved fasting
and postprandial glucose. Due to its renal mechanism of action (MOA), we
hypothesized that glucose lowering with EMPA is independent of β-cell function and insulin resistance. Using pooled data from three 24-week trials that
investigated EMPA 10 mg (n=632) and EMPA 25 mg (n=626) vs. placebo (PBO;
n=622) as monotherapy or add-on to metformin (MET) or MET+sulfonylurea,
we investigated the influence of baseline HbA1c, body mass index (BMI),
HOMA-B and HOMA-IR on change from baseline in HbA1c using 2-way interaction models. EMPA significantly reduced HbA1c from baseline vs. PBO
at week 24; in a model without interaction, mean HbA1c reductions vs. PBO
were -0.65% with EMPA 10 mg and -0.70% with EMPA 25 mg. Baseline
HbA1c had a significant influence on the treatment effect (p<0.001 for interaction). There were no interactions between treatment and baseline BMI
(p=0.606), HOMA-B (p=0.384) or HOMA-IR (p=0.199). Predicted reductions in
HbA1c based on a model including baseline HbA1c by treatment interaction
are presented in the Table. In summary, treatment effects of EMPA on HbA1c
reductions appear to be driven by baseline HbA1c and to be independent of
baseline β-cell function, insulin sensitivity and BMI.
Table.
MADANAHALLI R. JAGANNATH, MARIKUNTE V. VENKATARANGANNA, BAGGAVALLI P. SOMESH, MAMMEN O. ANUP, THARAPPEL M. ANIL, MAHESH KUMAR VERMA, KRISHNAREDDY HARSHA, RAJ GOWTHAM, PATIL A. HANSRAJ,
MUDIGERE N. LAKSHMI, PUTTREVANA M. PALLAVI, SIVAKUMARAN YOGESHWARI, ARALAKUPPE S. GOPALA, Bangalore, India
We have previously reported that CNX-013-B2, an orally administered heterodimer selective rexinoid, controlled multiple risk factors of the metabolic
syndrome in obese rodent models of disease. CNX-013-B2 did not cause edema
or fluid accumulation or hepatomegaly nor did it increase body weight in rodents. We now report the effect of long term treatment of male Zucker Diabetic
Fatty (mZDF) rats with CNX-013-B2 (10 mg/kg qd, n=10) on control of diabetes
and certain aspects of diabetic complications. CNX-013-B2 treatment provided
significant glycemic control all through the study period reaching a decrease of
67% fed (115 vs. 348 mg/dl) and 69% fasting (110 vs. 355 mg/dl) glucose compared to mZDF control animals (22nd week). This robust glycemic control translated to a steep reduction in HbA1c (4.54% vs. 14.56%) compared to control
animals. In OGTT (10th week), treatment reduced glucose AUC by 16% (32552
vs. 38524; p<0.05) and insulin AUC by 39% (769.48 vs. 1270.17; p<0.001) indicating significant improvement in insulin sensitivity. After 18 weeks treatment a
significant reduction in serum levels of oxidized LDL (45%), leptin (36%) and an
increase in adiponectin (31%) was observed even in absence of any change in
body weight. At end of study significant reduction in fasting triglyceride (TG 25%), total cholesterol (10%), liver TG (34%) and muscle TG (40%) was observed.
A significant 29 mg/dl reduction in Blood Urea Nitrogen, an increase in nerve
conductance velocity and decrease in serum levels of known cardiovascular
risk factors were observed indicating control over progression of diabetic complications. Treatment has shown a significant improvement in genes those are
involved in glucose and fat oxidation, energy expenditure and cellular stress.
Supported By: Boehringer Ingelheim/Eli Lilly and Company
119‑LB
Initial Combinations of Empagliflozin and Metformin (EMPA+MET)
in Patients with Type 2 Diabetes (T2DM)
SAMY HADJADJ, ANTE JELASKA, SHU ZHANG, THOMAS MEINICKE, HANS J.
WOERLE, ULI C. BROEDL, Poitiers, France, Ridgefield, CT, Biberach, Germany, Ingel­
heim, Germany
MET is the recommended first-line therapy for patients with T2DM, but
initial combination therapy may provide more robust glucose-lowering
efficacy. In a Phase III study, 1364 drug-naïve patients with T2DM were
randomized to EMPA 12.5mg bid+MET 1000mg bid (n=170), EMPA 12.5mg
bid+MET 500mg bid (n=170), EMPA 5mg bid+MET 1000mg bid (n=172), EMPA
5mg bid+MET 500mg bid (n=170), EMPA 25mg qd (n=168), EMPA 10mg qd
(n=172), MET 1000mg bid (n=171) or MET 500mg bid (n=171). The primary
endpoint was change from baseline in HbA1c at week 24. Key secondary
endpoints were changes from baseline in fasting plasma glucose (FPG) and
weight. EMPA+MET bid led to statistically superior and clinically meaningful
reductions in HbA1c vs. EMPA qd and MET bid doses (Table). EMPA+MET bid
led to significant reductions in FPG vs. EMPA qd and MET bid and in weight
vs. MET bid (Table). Adverse events (AEs) were reported in 56.7-66.3% of
patients across groups. Percentage of patients with confirmed hypoglycemic
AEs (glucose ≤70mg/dL and/or requiring assistance) was low in all groups
(0-1.8%); none required assistance. EMPA+MET bid significantly reduced
HbA1c vs. EMPA qd and MET bid and was well tolerated.
121‑LB
Effects of Dextromethorphan (DXM) Alone and as Add-on to Sita‑
gliptin (SITA) on Blood Glucose (BG) and Serum Insulin (INS) Con‑
centrations in Patients with Type 2 Diabetes Mellitus (T2DM) after
an Oral Glucose Tolerance Test (OGTT)
JAN MARQUARD, ALIN STIRBAN, FREIMUT SCHLIESS, FELIX SIEVERS, ALENA
WELTERS, SILKE OTTER, ANNELIE FISCHER, STEPHAN WNENDT, THOMAS
MEISSNER, TIM HEISE, ECKHARD LAMMERT, Düsseldorf, Germany, Neuss, Germany, Mönchengladbach, Germany
Recently we showed that the NMDA receptor antagonist DXM enhances
postprandial INS and oral BG tolerance in T2DM and improves islet insulin content, islet cell mass and BG control in db/db mice (Nature Medicine,
April 2015, DOI 10.1038/nm.3822). In this double-blind, placebo-controlled,
cross-over study we investigated the BG-lowering effect of 60 mg DXM and
100 mg SITA alone and the combination of DXM + SITA with an OGTT in 20
patients with T2DM. DXM 60 mg significantly reduced blood glucose excursions and increased insulin secretion versus placebo (data combined from
two clinical studies, not shown). The effects on BG were similar to those
seen with SITA alone, whereas the combination of DXM and SITA improved
both maximum blood glucose levels and early phase insulin secretion significantly better than SITA and DXM alone (Figure). All study drugs were
well tolerated without relevant adverse events. These findings confirm the
therapeutic potential of DXM alone and, in particular, in combination with
ADA-Funded Research
For author disclosure information, see page LB98.
LB31
POSTERS
120‑LB
CNX-013-B2 Provides Long-Term Glycemic Control and Has Poten‑
tial to Reduce Diabetic Complications—Studies in mZDF Rats
Clinical Diabetes/
Therapeutics
Supported By: Boehringer Ingelheim/Eli Lilly and Company
Clinical Therapeutics/New Technology—Oral Agents
DPP-IV inhibitors in patients with T2DM. This potential warrants further investigation in long-term clinical trials.
carried out for 16 weeks in 18 patients with gliclazide (60-120 mg/day) and
16 with vildagliptin (100 mg/day). Fasting and postprandial plasma glucose,
HbA1c, insulin, glucagon, soluble markers of cell adhesion (VCAM, ICAM and
E-selectin), inflammatory markers (PAI-1, TNF-alpha and IL-6) and of oxidative stress (TBAR and TAOS) were measured at the beginning and at the end
of the study. The two drugs showed significant improvement in glycemic
control There was no intergroup statistical difference in soluble markers
of cell adhesion and PAI-1. TNF-α showed a significant improvement in the
vildagliptin group compared with gliclazide (3.0±1.5 and 3.5±1, 1 pg/ml, respectively, ajusted p=0.001) and IL-6 (2 4±1.1 and 2.8±1, 1 pg/ml, respectively, ajusted p=0.005). There was also significant improvement in TBAR and
TAOS in the vildagliptin group compared with gliclazide (8.0±0.7 and 8.4±0, 9
nmol/MDA/ml, respectively, ajusted p<0.001 and 266.5±49, 4 and 264.3±34,
0μM Trolox Equivalents respectively ajusted p=0.001). Both drugs improved
glycemic control. Vildagliptin provided significant improvement in inflammatory markers TNF and IL-6 and oxidative stress markers TBAR TAOS.
FEI WANG, TIANSHENG WANG, JUNWEN ZHOU, HUILIN TANG, TRINH NHAN,
SHARON GIOVENALE, Storrs, CT, Beijing, China
POSTERS
Clinical Diabetes/
Therapeutics
124‑LB
Adverse Effects of Incretin-based Therapies on Major Cardiovascu‑
lar and Arrhythmia Events: Meta-analysis of Randomized Trials
The long-term cardiovascular safety outcome of incretin therapies remains
controversial. A meta-analysis of RCTs was conducted to quantitatively
evaluate CV safety (all cause death, CV death, myocardial infarction, stroke,
heart failure, unstable angina, and arrhythmia) of incretin therapies: sitagliptin (SIT), vildagliptin (VIL), saxagliptin (SAX), linagliptin (LIN), exenatide (EXE),
liraglutide (LIR), albiglutide (ALB), dulaglutide (DUL), and lixisenatide (LIX). A
systematic search of EMBASE, MEDLINE, Cochrane Database of Systematic Reviews, and ClinicalTrials.gov was conducted through November 2014.
From relevant reports, 99 randomized clinical trials were included. Results
were pooled via Peto methods and meta-regressions. Of 85231 participants
from 99 trial reports including 102 trial populations (26 SIT, 9 VIL, 11 SAX,
13 LIN, 8 ALO, 13 EXE, 8 LIR, 6 ALB, 3 DUL, and 5 LIX), there were a total
of 1280 all cause death events and 3455 CV events (805 CV death, 1101
myocardial infarction, 515 stroke, 626 heart failure, 253 unstable angina, 155
arrhythmias). There was a statistically significant increase in heart failure
outcomes associated with SAX (OR 1.23; 95% CI, 1.03-1.46). Compared with
controls, EXE was associated with increased risk of arrhythmia (OR 2.83;
95% CI, 1.06-7.57). SIT was associated with a significantly decreased risk
of all cause death compared to active controls (OR 0.39, 95% CI 0.18-0.82).
Other agents were not significantly associated with risk. Time-cumulative
analyses indicated that for EXE the risk for arrhythmia was evident by the
end of 2014; the evidence for heart failure risk of SAX became apparent
by 2013. Our meta-analysis indicates that EXE might be associated with increased risk of arrhythmia; and that SIT was associated with a reduced risk
of all cause death compared with other anti-diabetic agents. These results
need confirmation in long-term CV outcome trials.
122‑LB
LEZ763, a Novel GPR119 Agonist, Increases GLP-1, GIP, PYY, and
Glucagon, but Has Minimal Effects on Glucose in Patients with Type
2 Diabetes
YANLING HE, LORI DAVIS, PRAFULLA BHAD, AHMED AMER, LAURENCE COLIN,
JING-HE YAN, STUART HARRIS, ANN TAYLOR, Cambridge, MA, Burlington, ON,
Canada, East Hanover, NJ, Miami, FL
Agonists of GPR119 have been tested in patients with T2DM, although the
effects on glucose have been disappointing. The objective of this study was to
assess the effects of LEZ763, a potent and selective GPR119 agonist, on glucose and biomarkers including glucagon, insulin, C-peptide, and gut hormones
(total and active GLP-1, total GIP and PYY) in T2DM patients. A total of 96
patients were enrolled and 92 completed the study. Patients were randomized
to one of the six treatments: 25,100, 300 and 600 mg qd LEZ763, placebo, or
sitagliptin 100 mg qd for 4 weeks. At baseline and after 4 weeks of treatment,
a standardized mixed test meal was given whereafter serial blood samples
were collected up to 4-hour post dose for biomarkers measurement. LEZ763
treatment modestly decreased postprandial glucose (AUC0-4h; 3-8%), although
this was not statistically significant. Sitagliptin reduced postprandial glucose
by 14% (p<0.05). LEZ763 treatment was associated with a non-significant increase in insulin (6-15%) and C-peptide (4-9%). LEZ763 treatment increased
glucagon (22~41%; p<0.05), total GLP-1 (29-35%; p<0.01), active GLP-1 (2950%; p<0.05), total GIP (21-36%; p<0.05) and PYY (39-76%; p<0.05). Although
LEZ763 significantly increased glucagon, GLP-1, GIP and PYY, it did not significantly decrease postprandial glucose. The lack of translation of the preclinical
glycemic control of a GPR119 agonist may be, at least partially, attributed to
the increased levels of glucagon in patients with T2DM. The counter-regulation effects of glucagon in humans may be more efficient than animal models
in the context of increased levels of gut hormones and insulin. To our knowledge, this is the first report with well characterized glucagon data in T2DM
following treatment with a GPR119 agonist. GPR119 agonists may not be an
effective glucose-lowering treatment in T2DM.
125‑LB
Maintenance of Normokalemia with Sodium Zirconium Cyclosili‑
cate (ZS-9) in Diabetic Patients on RAASi from the Phase 3 Random‑
ized, Placebo-Controlled HARMONIZE Study
STEVEN N. FISHBANE, MOHAMED EL-SHAHAWY, HENRIK S. RASMUSSEN,
PHILIP T. LAVIN, BHUPINDER SINGH, ALEX YANG, WAJEH QUNIBI, Manhasset,
NY, Los Angeles, CA, Coppell, TX, Framingham, MA, San Antonio, TX
Hyperkalemia (HK) is higher in pts with diabetes mellitus (DM), limits use
of RAAS inhibitors (RAASi), and is associated with morbidity and/or mortality. Current HK treatments such as polymer resins have questionable efficacy and are limited by potentially fatal GI side effects (eg, colonic necrosis).
Sodium zirconium cyclosilicate (ZS-9) is a first in class, highly specific, nonabsorbed cation exchanger designed to trap K+ in the gut. Here we present
a subgroup analysis of DM pts on RAASi from a Phase 3 study. HARMONIZE
was a multicenter, randomized, double-blind, PBO-controlled trial in 258 HK
pts. All pts received open label 10g ZS-9 TID for 48h (acute). Pts achieving
normokalemia (NK; 3.5-5.0 mEq/L) were randomized to 5, 10, or 15g ZS-9 QD
or PBO for 28d (maintenance). RAASi dose was maintained. Of 258 enrolled
pts, 121 (47%) had DM and were on RAASi. Median time to K+ normalization
was 2.1h. Mean K+ declined from 5.6 mEq/L at baseline to 4.6 mEq/L at 48h,
with 97% of pts achieving NK at 48h. Mean K+ was maintained (28d) at 4.9,
4.5, and 4.4 mEq/L with the 5, 10, and 15g doses, respectively, vs. 5.2 mEq/L
with PBO (P<0.0001 all). In DM pts on RAASi, ZS-9 rapidly and safely normalized K+ within hours, maintained NK for 28d and was well tolerated with GI
side effects similar to PBO, suggesting that ZS-9 acts quickly and may enable
continued RAASi use in DM pts with HK.
123‑LB
Comparative Study of 16 Weeks of the Effect of Vildagliptin and
Gliclazide on Markers of Inflammation and Oxidative Stress in Dm2
Inadequately Controlled with Metformin
LILIAN L.A. CAVALCANTE, MARCELO R.N. HISSA, SERGIO B. GUIMARAES, HERMANO A.L. ROCHA, MIGUEL N. HISSA, Fortaleza, Brazil
Diabetes mellitus has a latent baseline inflammatory status and a high
oxidative stress that are intrinsically related to complications of the disease. Atherosclerosis is also an inflammatory disease and represents a
major cause of morbimortality associated with diabetes. Recent studies
have shown anti-inflammatory actions and reducing oxidative stress, in addition to improved glycemia, using incretin based therapy. To evaluate the
response from the gliclazide, second-generation sulfonylurea, and from
vildagliptin, DPP-4 inhibitor, in the inflammatory markers and in the oxidative
stress in DM2, we performed a prospective study, randomized, open-label
in 34 patients inadequately controlled with metformin. The monitoring was
ADA-Funded Research
For author disclosure information, see page LB98.
LB32
126‑LB
SHASHANK R. JOSHI, SUJOY GHOSH, PARAG SHAH, ASHOK D. JAISWAL,
PANKAJ PATEL, Mumbai, India, Kolkata, India, Ahmedabad, India
Saroglitazar is the world’s first commercially available dual PPAR α and γ
agonist which was launched in September 2013 in India. The objective of this
post-marketing surveillance study was to evaluate the safety and efficacy
of saroglitazar for 1 year follow up in clinical practice. It was a multicenter,
phase 4 study conducted all over India. Total 236 patients with diabetic
dyslipidemia who were prescribed saroglitazar 4mg daily were evaluated
for lipid and glycemic parameters at baseline, 3 month, 6 month, 9 month
and 12 month follow up. Baseline patient demographics were: age 52 ± 10
year (mean ± SD), average duration of diabetes 5.91 year, and BMI 28.8 ±
3.99 kg/m2 (mean ± SD). At baseline, 89% and 38.6% patients were reported
to be on antidiabetic and statin therapy respectively. Metformin was the
most commonly reported in 72% patients followed by sulfonylureas (66.9%),
gliptins (16.1%), insulin (20.8%) and pioglitazone (4.7%). One year treatment
with saroglitazar resulted into significant improvement in glycemic and lipid
parameters (results are shown in Table). There were no serious adverse
events reported. Saroglitazar was found to be safe, well tolerated and was
not associated with edema or weight gain. This is the first data of one year
safety and efficacy of saroglitazar in a real world setting which clearly demonstrated the dual action of glucose and lipid lowering.
Supported By: LG Life Sciences
128‑LB
Organ-specific Uptake and Elimination of Metformin Can Be Deter‑
mined In Vivo in Mice and Humans by PET-imaging Using a Novel
11C-metformin Tracer
JONAS B. JENSEN, LARS C. GORMSEN, ELIAS SUNDELIN, STEEN JAKOBSEN,
OLE L. MUNK, MIKKEL H. VENDELBO, METTE M.H. CHRISTENSEN, KIM BROSEN,
JØRGEN FROKIAER, NIELS JESSEN, Aarhus, Denmark, Odense, Denmark
Metformin is the most commonly prescribed oral anti-diabetic drug.
However, despite being in clinical use for almost 60 years the underlying
mechanisms for action remain elusive. We have therefore applied a novel
PET-tracer, 11C-metformin, to determine uptake and elimination in liver in vivo. To test the role of organic cation transporters, we used OCT1/2 knock out
mice and pharmacological inhibitors. In a second series of experiments we
have determined organ specific uptake of 11C-metformin in healthy humans.
Our results demonstrate that in mice, OCT1/2 expressions are essential for
normal uptake while MATE1 is necessary for elimination of metformin from
the liver. There is no detectable secretion of 11C-metformin to the bile after
iv-injection, but metformin is transported into duodenal enterocytes from
blood. In humans (Fig. 1) there is visible uptake in liver, kidney and salivary
glands, but no detectable uptake in brain, muscle or fat. Effective dose was
0.0095 mSv/MBq. The therapeutic effects of metformin vary considerably
from patient to patient. Determination of tissue specific uptake of metformin
can be an important tool to investigate the underlying causes and optimizing
treatment. In addition, precise determination of metformin action in specific
tissues could help clarify the mechanisms of action of metformin outside its
present indications.
Table. Effect of Saroglitazar 4 mg Once Daily on Glycemic and Lipid
Parameters at 1 Year Follow-up; All val.
Absolute
P
%
Laboratory
3 month 6 month 1 year
change value change
parameter
Baseline follow up follow up follow up at 1 year
% at 1 year
HbA1C (%)
8.5±
7.9±
7.5±
6.9±
-1.6± <0.0001 —
1.06
0.87
0.78
0.76
1.12
Fasting Plasma 179.4± 144.1± 132.6± 115.5±
-63.9± <0.0001 -32.7±
Glucose (mg/dL) 54.67
40.29
37.81
28.90
44.20
15.20
Post-prandial 252.6± 192.0± 168.8± 146.5± -106.1± <0.0001 -38.7±
Plasma Glucose 64.17
38.81
31.34
22.11
63.56
16.24
(mg/dL)
Triglycerides
316.0± 222.1± 194.9± 153.9± -162.1± <0.0001 -47.3±
(mg/dL)
139.02 70.63
66.36
50.06
136.73
16.91
LDL-C (mg/dL) 131.8± 114.8± 108.1±
96.7±
-35.1± <0.0001 -24.1±
43.78
35.55
31.9
30.13
34.2
21.72
HDL-C (mg/dL) 42.5±
43.6±
45.0±
44.8±
2.3±
0.0044 9.2±
8.74
7.18
8.20
9.11
12.09
29.59
Non HDL-C
194.0± 160.6± 147.3± 127.0±
-67.1± <0.0001 -33.4±
(mg/dL)
48.48
37.75
35.92
35.04
45.54
16.49
127‑LB
Efficacy and Safety of Gemigliptin in Type 2 Diabetes Patients with
Moderate to Severe Renal Impairment
SUN AE YOON, BYOUNG GEUN HAN, SUNG GYUN KIM, SANG YOUB HAN,
YOUNG-IL JO, KYUNG HWAN JEONG, KOOK-HWAN OH, HYOUNGCHUN PARK,
SUN-HEE PARK, SHIN-WOOK KANG, KI-RYANG NA, NAM-HO KIM, DAE RYONG
CHA, GUARD STUDY, Uijeongbu, Republic of Korea, Wonju, Republic of Korea,
Anyang, Republic of Korea, Goyang, Republic of Korea, Seoul, Republic of Korea,
Daegu, Republic of Korea, Daejeon, Republic of Korea, Gwangju, Republic of Korea,
Ansan, Republic of Korea
Supported By: Novo Nordisk Foundation
129‑LB
Activation of the cAMP-PKA Pathway Antagonizes Metformin Sup‑
pression of Hepatic Glucose Production
LING HE, EVAN CHANG, JINGHUA PENG, SALLY RADOVICK, FREDRIC E. WONDISFORD, Baltimore, MD
Gemigliptin, a potent and selective DPP-4 inhibitor, can be used without
dose reduction in renal impairment. This randomized, double blind, parallel
group Phase 3b study comprised a 12-week, placebo-controlled phase fol-
Metformin is a widely prescribed anti-diabetic agent, which is taken by
more than 150 million people worldwide. Treatment guidelines for type 2
ADA-Funded Research
For author disclosure information, see page LB98.
LB33
POSTERS
Saroglitazar in Diabetic Dyslipidemia: 1-Year Data
lowed by a 40-week, double blind active-controlled extension phase (placebo switched to linagliptin). This 12-week randomized trial investigated the
efficacy and safety of gemigliptin in type 2 diabetic patients with moderate to severe renal impairment. It was also evaluated whether gemigliptin
has renoprotective effects in these patients. A total of 132 patients were
randomized to gemigliptin (n=66) or placebo (n=66). Primary endpoint was
HbA1c change from baseline at Week 12. Baseline demographics were
similar between treatment groups (mean HbA1c 8.4%; age 62.0 years; BMI
26.2 kg/m2, duration of T2DM 16.3 years; eGFR 33.3 mL/min/1.73 m2). The
predominant background therapy was insulin (63.1%). At Week 12, adjusted
mean ± SE change HbA1c with gemigliptin was -0.83 ± 0.14% (change with
placebo 0.38 ± 0.14%; difference -1.21, 95% CI -1.54 to -0.89; p<0.0001). A
similar profile was also observed in other glycemic control parameters (FPG,
glycated albumin, and fructosamine). After 12 weeks of gemigliptin treatment, albuminuria (measured by urinary albumin creatinine ratio [UACR])
significantly decreased in the patients with micro- and macro-albuminuria.
Furthermore, urinary nephrin and type IV collagen in the gemigliptin were
also significantly reduced compared to placebo. Drug-related AEs including
hypoglycemia for gemigliptin was similar to placebo (15.2% and 12.1%, respectively). There was no meaningful change from baseline in body weight
(gemigliptin, -0.3 kg; placebo -0.2 kg). Gemigliptin improved glycemic control
and provided additional renoprotection in T2DM patients with moderate to
severe renal impairment. There was no additional risk of hypoglycemia and
no weight gain.
Clinical Diabetes/
Therapeutics
Clinical Therapeutics/New Technology—Oral Agents
Clinical Therapeutics/New Technology—Oral Agents
diabetes mellitus (T2D) recommend metformin as the initial drug. Surprisingly, about 35% of diabetic patients either lack or have a delayed response
to metformin treatment, and many patients become less responsive to metformin over time. It remains unknown how metformin resistance or insensitivity occurs. Recently, we find that therapeutic metformin concentrations
suppress glucose production in primary hepatocytes through the activation
of AMPK; and activation of the cAMP-PKA pathway negatively regulates
AMPK activity by phosphorylating the AMPKα subunit at S485, which in
turn reduces net phosphorylation at T172 and AMPK activity. Indeed, metformin failed to suppress cAMP-stimulated glucose production in primary
hepatocytes with constitutive PKA activation and to improve hyperglycemia in mice with hyperglucagonemia. Mutation of a PKA phosphorylation
site on AMPKα1 (S485A) increased both AMPKα1 phosphorylation at T172
and suppression of glucose production in primary hepatocytes treated with
metformin. Intriguingly, salicylate/aspirin prevents the phosphorylation of
AMPKα S485, blocks this cAMP-PKA negative regulation of AMPK, and improves metformin resistance. We propose that salicylate/aspirin may augment metformin’s hepatic action to suppress glucose production.
AE rates were 41.8%, 44.3%, 37.1%, 39.9%, and 37.6% with CANA 100 mg/
MET XR, CANA 300 mg/MET XR, CANA 100 and 300 mg, and MET XR with
low rates of serious AEs. Incidences of genital mycotic infections and osmotic diuresis, volume depletion, and renal-related AEs and hypoglycemia were
low, but higher in all CANA arms vs. MET XR with overall low discontinuation
rates across groups. In conclusion, initial combination therapy with CANA/
MET XR is efficacious and well tolerated in drug-naïve T2DM.
130‑LB
POSTERS
Clinical Diabetes/
Therapeutics
Supported By: National Institutes of Health
The Combination of Insulin, Liraglutide, and Dapagliflozin as Triple
Therapy for Type 1 Diabetes
NITESH D. KUHADIYA, ADITYA MEHTA, HUSAM GHANIM, JEANNE HEJNA,
ANTOINE MAKDISSI, AJAY CHAUDHURI, MANAV BATRA, PARESH DANDONA,
Buffalo, NY
We have recently demonstrated that the addition of liraglutide to insulin
significantly improves the glycemic control in patients with type 1 diabetes
(T1D). We have now investigated whether the addition of dapagliflozin, a
SGLT-2 inhibitor, which induces glycosuria, to insulin and liraglutide would
improve glycemia further. We conducted a retrospective analysis of 10 patients on continuous glucose monitoring system (CGMS) treated with this
combination. They were under treatment with insulin and had received
liraglutide for 11±2 months (baseline HbA1c: 8.01±0.22%; mean age: 56±4
years; mean age of diabetes diagnosis: 29±5 years; mean BMI: 29±1 Kg/m2;
mean body weight: 86.4±4.5 kg; mean BP: 125/75±3 mm Hg). In all patients,
dapagliflozin was started at a dose of 5 mg daily and was increased to 10
mg daily 7±1 days later. At the end of 12±1 weeks of dapagliflozin therapy,
mean HbA1c fell by 0.66±0.22% (p=0.0004); mean glucose fell by 28±2mg/
dl from a baseline of 172±9 mg/dl (p=0.016,); the daily carbohydrate intake
increased from 166±3g to 196±4g (p= 0.04); mean body weight and BMI fell
from 87±5 Kg to 85±5 Kg and 29±1 to 28±1Kg/m2, respectively (p=0.02). Total
insulin dose remained unchanged at 0.7±0.1 u/Kg daily. Percent time spent
in glycemic range of 70-160 mg/dl increased by 11±2% while that greater
than 160 mg/dl decreased by 13±3% (p<0.05 for both). There was no additional hypoglycemia (<70 mg/dl). One patient developed diabetic ketoacidosis (DKA) in spite of normal blood glucose concentrations within 48 hours
of increasing the dose of dapagliflozin to 10 mg. The dose of insulin in this
patient had declined from 0.45 to 0.39 u/kg (total dose: 32.9 to 28.5 units).
Carbohydrate intake had increased from 50 to 95g daily. We conclude that
the addition of dapagliflozin to insulin and liraglutide in patients with T1D
results in a significant improvement in glycemia. However, care would have
to be exercised in terms of the reduction in insulin dose and thus the occurrence of euglycemic DKA.
Supported By: Janssen Research and Development, LLC.
132‑LB
Exogenous GLP-1 Is Not Fully Protected by Acute DPP-4 Inhibition
EMILIE S. ANDERSEN, ASGER LUND, CAMILLA ANDREASEN, JONATAN I. BAGGER, CAROLYN DEACON, BOLETTE HARTMANN, JENS JUUL HOLST, FILIP K.
KNOP, TINA VILSBØLL, Hellerup, Denmark, Copenhagen, Denmark
Dipeptidyl peptidase-4 (DPP-4) inhibitors limit glucagon-like peptide-1
(GLP-1) degradation, and are used to treat type 2 diabetes (T2D). DPP-4 exists
in soluble and membrane-bound forms. It is unclear if plasma DPP-4 activity
levels reflect the full extent of DPP-4 inhibition in all compartments. We used
the selective inhibitor sitagliptin to explore the relationship between DPP4 activity and protection of GLP-1. On 4 separate days, subjects with T2D
(BMI: 28.8±1.4 kg/m2 [mean±SEM]; HbA1c: 43.1±2.4 mmol/mol) and matched
healthy controls (BMI: 28.1±1.2 kg/m2; HbA1c: 34.4±1.2 mmol/mol) received
continuous iv GLP-1 (1.0 pmol/kg/min) and oral sitagliptin (0 [placebo], 25,
100 or 200 mg; double-blind randomized order). Plasma DPP-4 activity was
measured by chromogenic assay, and the degree of protection of GLP-1 (assessed with specific RIAs) was used as a surrogate index of inhibition of
“total” DPP-4 activity. At steady-state, within the time period 180-360 minutes, plasma DPP-4 activity decreased dose-dependently (Table), but with
differences between DPP-4 compartments and groups, the latter possibly
due to differences in gastric emptying. Despite relatively high inhibition of
plasma DPP-4 activity, intact GLP-1 levels remained lower than total GLP-1
levels. This could suggest that membrane-bound DPP-4 was not fully inhibited. Furthermore, other enzymes, not inhibitable by sitagliptin, may also
have been responsible.
131‑LB
Initial Combination Therapy with Canagliflozin (CANA) plus Met‑
formin Extended-Release (MET XR) in Drug-Naïve Type 2 Diabetes
Mellitus (T2DM)
JULIO ROSENSTOCK, LEONARD CHUCK, MANUEL GONZÁLEZ-ORTIZ, KATE MERTON, JAGRITI CRAIG, GEORGE CAPUANO, RONG QIU, Dallas, TX, Walnut Creek,
CA, Guadalajara, Mexico, Raritan, NJ
This study assessed the efficacy and safety of initial combination therapy
with CANA, an SGLT2 inhibitor, and MET XR in drug-naïve T2DM (A1C 7.5%12.0%; N = 1186; mean age, 54.9 y; A1C, 8.8%; BMI, 32.5 kg/m2; eGFR, 88
mL/min/1.73 m2; T2DM duration, 3.3 y) randomized to CANA 100 mg/MET
XR, CANA 300 mg/MET XR, CANA 100 or 300 mg, or MET XR (titrated up
to 2000 mg/d; median dose = 2000 mg/d) for 26 weeks. Both CANA/MET
XR doses provided statistically superior A1C reductions vs. their respective
monotherapies (Fig. A). CANA 100 mg/MET XR and CANA 300 mg/MET XR
provided larger A1C reductions vs. CANA 100 and 300 mg or MET XR in patients with baseline A1C ≥9.0% (-2.4%, -2.4%, -1.9%, -2.0%, -1.8%). More
attainment of A1C <7.0% (Fig. B) and significant weight loss were seen with
both CANA/MET XR doses vs. MET XR. CANA 100 and 300 mg showed noninferiority in A1C lowering and greater body weight loss vs. MET XR. Overall
ADA-Funded Research
For author disclosure information, see page LB98.
LB34
Clinical Therapeutics/New Technology—
Pharmacologic Treatment of Complications
Health Care Delivery—
Economics
Table.
Table. Results.
Parameters
Group-1
Baseline
(Exenatide Only)
HbA1c (%)
7.9 +/- 0.54
HDL-C (mg/dL) 35.8 +/- 9.8
Triglycerides
362.9 +/- 167.2
(mg/dL)
Liver Fat Content 319.3 +/- 31.4
(dB/m)
133‑LB
Triple Therapy with Dapagliflozin (DAPA) Add-on to Saxagliptin
(SAXA) plus Metformin (MET): Characterization of the Open-Label
SAXA+MET Lead-in Period of a Phase 3 Trial
Group-1 Change
Week 24 Group 1
Group-2
Group-2
Baseline
Week 24
(Exenatide+Saroglitazar)
7.09 +/- 0.29 - 0.81
8.1 +/- 1.01
6.94 +/- 0.40
38.1 +/- 8.9 + 6.4 %
31.6 +/- 10.5
38.4 +/- 10.3
233.8 +/- 60.8 - 35.6 %
390.4 +/- 96.6 180.3 +/- 51.6
248.3 +/- 30.5 - 22.2 %
330.7 +/- 36.1
Change
Group 2
p VALUE
(changes
between groups)
- 1.16 0.09 (NS)
+ 21.5 %
0.003
- 53.8 %
0.01
202.8 +/- 28.3 - 38.7 %
<0.001
We conclude that the Exenatide-Saroglitazar combination leads to significant reductions in Liver fat content and serum triglycerides. It also raises
HDL-C significantly in these patients. This combination maybe effective at
retarding the progression of hepatic steatosis and longitudinal studies are
required to look at the long term effects of this combination.
CHANTAL MATHIEU, AURELIAN EMIL RANETTI, LARS HANSEN, HUNTGA CHEN,
RICARDO GARCIA-SANCHEZ, ALEX J. CHIN, NAYYAR IQBAL, Leuven, Belgium,
Bucharest, Romania, Princeton, NJ, Gaithersburg, MD
The 24-week efficacy and safety of DAPA versus placebo (PBO) as add-on
to SAXA+ MET in adults with type 2 diabetes (T2DM) was demonstrated
in a randomized, double-blind, phase 3 trial (NCT01646320). The 8-16 week
open-label (OL) lead-in period of this study was designed to generate a set
of uniform patients on SAXA+MET that could be randomized for double-blind
treatment. Patients on stable MET (stratum A; A1C 8.0%-11.5%, N=349) or
MET+DPP-4 inhibitor (stratum B; A1C 7.5%-10.5%, N=134) for ≥8 weeks received OL SAXA 5 mg/d+MET for 16 (stratum A) or 8 weeks (stratum B, any
DPP-4 inhibitor replaced with SAXA). Patients with inadequate glycemic
control (A1C 7%–10.5%) at week –2 before randomization were randomized
to PBO or DAPA 10 mg/d plus OL SAXA+MET. This analysis was focused on
patients in stratum A (baseline A1C 8.0%-11.5% and poorly controlled on
MET alone). At entry to the OL period (baseline), mean age was 54 years and
58% were women. Most patients (81.9%) completed the OL period. The most
common reason for not completing the OL period was not meeting study
criteria (12.3%). At OL baseline, mean (SD) A1C was 9.38% (0.91), and following the addition of SAXA, decreased to 8.06% (1.02) at week -2 (mean
change [95% CI] from baseline A1C, –1.32% [–1.46, –1.17]). At week –2, 61
patients (17.5%) achieved a therapeutic response (defined as A1C <7%), most
patients (234; 67.0%) had A1C 7.0%−10.5%, and 12 patients (3.4%) had A1C
>10.5%; an additional 42 patients (12%) had no −2 week data. During the
OL period, no hypoglycemic events were reported; 113 (32.4%) patients reported adverse events (AEs), and 5 reported serious AEs (none considered
related to treatment). The results show that 17.5% of patients with poorly
controlled T2DM and high baseline A1C of 8.0%-11.5% despite MET treatment achieved A1C <7% with the addition of SAXA. However, most patients
would require additional therapy in an effort to achieve a desired glycemic
goal of A1C <7%.
The prevalence of T2DM patients (pts) in the U.S. with A1C > 10% has
increased and is associated with a high healthcare burden. A recent trial
of ITCA 650 (continuous subcutaneous exenatide) in pts with high baseline
A1C (mean 10.9%) resulted in a 3.4% reduction in A1c at 39 weeks with 26%
of pts achieving the goal of A1C <7%. Little is known about the patterns of
treatment, adherence and change in A1C among real-world (RW) pts after
an extremely high A1C has been identified. Linked Optum-Humedica claims
and electronic medical records (1/2007-3/2014) were used to identify a RW
sample with T2DM, high baseline A1C and characteristics similar to pts in
the ITCA 650 study. Pts had 10 %< A1c≤12% (index date), and an A1C measurement 12 months later (± 3 months). Demographics, change in A1C, diabetes drug classes filled, and adherence (percent of days covered ≥80%) were
measured in the year before (baseline) and after index date (study period).
1,248 pts met study criteria. They had a mean age of 58 years, BMI of 35 kg/
m2, and A1C of 10.8%; 59% were male. At baseline, 46% of pts were adherent to diabetes drugs. 77% filled Rx for diabetes drugs at baseline: 11% metformin only, 34% other oral regimens, 28% insulin, and 6% GLP-1s. Pts taking
any diabetes drugs increased 13% points (P<0.01) from baseline and 50% of
all patients added a new drug class in the study period. Adherence increased
to 58% in the study period (P<0.01). Mean A1C declined 1.8% points from
index to 2nd A1C (mean 364 days) (P<0.01) with 16% of pts achieving A1C
goal <7. Sensitivity analyses that matched RW and trial pts yielded similar
results. While Rx fills increased in this RW study, non-adherence remained
high and reduction in A1C was modest with few pts achieving goal after a
year. New treatments that achieve greater reductions in A1C and improve
adherence at the same time are needed to more effectively treat T2DM pts
with high A1C who carry both a higher risk of complications and a higher cost
burden to the healthcare system.
Supported By: AstraZeneca
Clinical Therapeutics/New Technology—
Pharmacologic Treatment of Complications
134‑LB
Health Care Delivery—Economics
Efficacy of Exenatide-Saroglitazar Combination in Treatment of NA‑
FLD in Type 2 Diabetes
136‑LB
KIRAN PAL SINGH, MOHINISH CHHABRA, AVINAINDER SINGH, JYOTIKA MANAN, SHAKUN DABRA, Ajitgarh, India
Access to High-Acuity Care among Diabetes Patients in High De‑
ductible Insurance: A NEXT-D Study
Non Alcoholic Fatty Liver Disease (NAFLD) is commonly associated with
T2DM. Current treatment is aimed at lifestyle modifications only. Recently,
we studied the efficacy of a novel dual PPAR agonist - Saroglitazar in reversing the biochemical manifestations of MetS. Recent evidence also suggests
a role of Incretin based therapies for the management of NAFLD in diabetics.
We set out to combine these two approaches for the management of NAFLD
in diabetics. We studied the effects of Exenatide in combination with Saroglitazar on hepatic fat content and other biochemical parameters in obese
diabetics with NAFLD. 40 patients on dietary, Metformin and statin therapy
received treatment with exenatide alone (10 mcg BD) (n=20) or exenatide
and saroglitazar (4mg PO) (n=20) for 24 weeks. Age, BMI, Diabetes duration and abnormal transaminase levels were comparable between the two
groups. Hepatic steatosis was measured by Transient Elastography (Fibroscan). Other parameters including BMI, FPG, PPPG, HbA1c, lipid profile, RFT
and LFT were measured.
JAMES F. WHARAM, FANG ZHANG, EMMA B. MORTON-EGGLESTON, CHRISTINE LU, STEPHEN SOUMERAI, DENNIS ROSS-DEGNAN, Boston, MA
The Affordable Care Act (ACA) will soon make high deductible health plans
(HDHP) the predominant private insurance benefit in the U.S. No studies have
examined the impact of HDHPs on high-acuity care among diabetes (DM)
patients. We studied privately insured members of a large national health
plan. We followed DM patients from 2004-2012 and included 11,490 with
1 baseline year in traditional (≤$500 deductible) coverage whose employers then mandated transition to HDHP (≥$1000) coverage for 2 continuously
enrolled years. We performed employer- and member-level 1:1 propensity
score matching based on multiple baseline characteristics to contemporaneous DM patients continuously enrolled for 3 years whose employers offered
only traditional coverage. We assessed annual rates of emergency department (ED) visits and hospitalizations for 1 year before and 2 years after the
mandated switch from traditional to HDHPs, vs. controls. We stratified by
income and sex. We used annual difference-in-differences negative bino-
ADA-Funded Research
For author disclosure information, see page LB98.
LB35
POSTERS
GINGER S. CARLS, CHRISTIAN FROIS, EDWARD TUTTLE, MICHELLE A. BARON,
Menlo Park, CA, Boston, MA
Clinical Diabetes/
Therapeutics
135‑LB
Treatment, Adherence, and Change in A1c in Type 2 Diabetes (T2DM)
with High (>10%) HbA1c
Health Care Delivery—Economics
mial regression with generalized estimating equations to calculate adjusted
pre-to-post changes in the HDHP group vs. controls. In follow-up years 1
and 2, the overall HDHP group experienced no relative changes in ED visits (3.2% [-5.2, 11.7] and 0.0% [-8.2, -8.1], respectively) and findings were
similar across income and sex stratifications. The overall HDHP group also
demonstrated no detectable follow-up changes in hospitalizations (-2.5%
[-14.4, 9.4] and -4.7% [-16.0, 6.5], respectively). However, by follow-up year
2, low income and male HDHP members experienced pronounced relative
reductions in hospitalizations (-34.5%, [-60.5, -8.5] and (-18.9% [-32.9, -4.8],
respectively). Low income and male HDHP members with DM experienced
major reductions in access to hospital care. Male DM patients in HDHPs are
a previously overlooked vulnerable subgroup. As HDHPs expand under the
ACA, policy makers and researchers should focus on chronically ill male and
low income HDHP members.
Criteria 2 Pre-DM: 92.78% SN, 20.22% SP, 43.04% PPV, and 81.18% NPV.
Criteria 1 DM: 97.83% SN, 13.63% SP, 14.15% PPV and 97.74% NPV. Criteria
2 DM: 96.83% SN, 16.84% SP, 14.49% PPV and 97.33% NPV. This data suggests that BMI and age may be sufficient to identify eligible patients for A1C
testing, as further addition of RF added little to the sensitivity of eligibility
criteria. More importantly, a negative test (normal A1C) in an eligible patient
should not give a false sense of security and follow up should address modifiable risk factors.
Supported By: Centers for Disease Control and Prevention (U58DP002717)
139‑LB
CMS Competitive Bidding Program Disrupted Access to Diabetes
Supplies with Resultant Increased Mortality
GARY A. PUCKREIN, FARHAD ZANGENEH, GAIL NUNLEE-BLAND, LIOU XU,
CHRISTOPHER G. PARKIN, JAIME A. DAVIDSON, Washington, DC, Boulder City,
NV, Dallas, TX
Supported By: Natural Experiments in Diabetes Translation (NEXT-D) Initiative
(5U58DP002719)
The Centers for Medicare and Medicaid (CMS) implemented a trial of the
Competitive Bidding Program (CBP) for diabetes supplies in 9 test sites on
January 2011. In 2012, CMS reported the program was a success, noting
that beneficiary access to supplies was not compromised. We used CMS
data from 2009-2012 to assess the impact of CBP on acquisition of selfmonitoring of blood glucose (SMBG) supplies by Medicare beneficiaries who
acquired insulin >80% of days covered (n=529,627). The 2009 records were
separated into two cohorts; inclusion in the test sites (TEST; n=43,939) vs.
all other non-test sites (NON-TEST; n=485,688) In 2011, the percentage of
TEST beneficiaries with reduced SMBG acquisition, increased 23.0% vs.
1.7% in NON-TEST beneficiaries. The percentage of TEST vs. NON-TEST
beneficiaries with no SMBG record increased (16.7% vs. 1.2%). Migration
from full to reduced acquisition or no SMBG was associated with increased
mortality in both cohorts; however, a significantly higher percentage of TEST
vs. NON-TEST beneficiaries made this migration (p<0.0001) (Table) Acquisition of SMBG supplies was somehow disrupted in the TEST population, with
resultant increased mortality; a finding not supported by the CMS report on
adverse outcomes associated with the CBP. These data suggest that the CBP
may have had unanticipated, deleterious consequences, and argue for more
careful monitoring of CBP impact by CMS.
Use of Digital Tracking Devices in the Management of Diabetes
Mellitus: A Systemic Review and Meta-analysis
BARBARA J. GROHMANN-IZAY, MICHAEL FORISCH, Vienna, Austria
POSTERS
Clinical Diabetes/
Therapeutics
137‑LB
A systemic literature search was conducted in October 2014 to identify
randomized, controlled clinical trials investigating the effect of a digital
tracking device in diabetes mellitus type 1 (DM1) and type 2 (DM2), including
adults, adolescents and the special population of pregnant women (GDM)
compared to a conventional, usual-care approach. Included trials were
evaluated regarding outcome of clinical parameters, quality of life (QoL) and
socio-economical parameters. A meta-analysis was performed on pooled
HbA1c change from baseline reported in the trials identified during the systemic review. In this review, a total of 31 studies fulfilled the search criteria and were included in the final evaluation. Twelve (12) studies assessed
DM1, 11 DM2, 5 included both indications (DM1/DM2), and additional 3
trials evaluated GDM. Most of the trials (93.5%) compared digital tracking
devices with controls (conventional/usual care without digital tracking/telemedicine). Twenty-four (24) studies (77.4%) used a telecare approach and
2 of the included studies (6.5%) used gamification. Several studies (51.9%)
have shown that usage of a digital tracking device in diabetes management
is significantly improving metabolic control (measured by HbA1c); additional
positive effects on the lipid profile, blood pressure, QoL (including self-efficacy and adherence behaviour) and cost of care were observed. Some of
the studies failed to show significant differences between the two groups
(digital tracking device vs. controls), but it has to be noted that none of the
studies found that the use of a digital tracking device was inferior to the
conservative approach. Meta-analysis of 19 trials in the adult population
found a -0.38% difference [95% CI -0.40 to -0.37] in HbA1c between usage
of digital tracking devices and controls. Therefore, we conclude that the use
of digital tracking devices in diabetes management is effective, safe and
well accepted for different patient populations with DM.
Table. Mortality Associated with Migration from Full SMBG* to Reduced or
No SMBG.
Full
Mortality
Reduced/
Mortality
Acquisition
2011
No Record
2011
n (%)
n, (%)
n, (%)
n, (%)
Full Cohort
TEST: Full SMBG acquisition (n=7,123)
migrating to Full or Reduced/No Record:
4,014 (56.4%) 279 (7.0%) 2,306 (32.4%) 218 (9.5%)
NON-TEST: Full SMBG acquisition (n=68,742)
migrating to Full or Reduced/No Record:
47,898 (69.7%) 3,080 (6.4%) 12,618 (18.3%) 1,209 (9.6%)
Propensity Score Matched
TEST: Full SMBG acquisition (n=4,205)
migrating to Full or Reduced/No Record:
2,112 (50.2%) 133 (6.3%) 1,163 (27.7%) 102 (8.8%)
NON-TEST: Full SMBG acquisition (n=4,311)
migrating to Full or Reduced/No Record:
2,495 (57.9%) 143 (5.7%) 605 (14.0%) 60 (9.9%)
* >80% of proportion of days covered, based on 3 test strips per day.
138‑LB
Testing for Type 2 Diabetes (DM) or Prediabetes (Pre-DM) in Asymp‑
tomatic Adults: Sensitivity and Specificity of American Diabetes
Association (ADA) Eligibility Criteria Extracted from the Electronic
Health Record (EHR)
YELENA ZUBATOV, PINDAN HAO, EDWIN YOUNG, NANCY SOHLER, JEANINE
ALBU, New York, NY
140‑LB
Do Financial Incentives Improve Participation in a Workplace Dia‑
betes Management Program? Yes, but Not by Much
Since 2010 the ADA has published evidence-based demographic and
clinical risk factors (RF) for development of DM, used to optimize eligibility
for blood glucose testing (fasting glucose, OGTT or A1C) to identify previously undiagnosed DM or Pre-DM. In clinical practice, testing eligibility is
determined by the physician’s knowledge, which is often influenced by the
availability of RF data in the EHR. We identified 4,715 patients (ages 18-100,
61% female) who, between Jan 1 2012-Dec 31 2014, had a complete set
of RF documented in the EHR and subsequent A1C testing. We calculated
the sensitivity and specificity of A1C testing eligibility criteria to diagnose
the presence of DM or Pre-DM. We used Criteria 1 which defined testing
eligible as age >45 years OR age <45 AND BMI >25 and Criteria 2 which, in
addition, incorporated the other ADA RF. The data was obtained from available structured fields in the EHR (BMI, age, race/ethnicity, HTN, CVD, dyslipidemia, PCOS) and a RF Questionnaire (RFQ) filled in during the patient’s visit
with the PCP (family history, GDM, physical inactivity). Highest A1C value
documented in the EHR after the RFQ was used to identify Pre-DM and DM
(5.7-6.4% Pre-DM, >6.5% DM).
Results: Criteria 1 Pre-DM 94.18% SN (sensitivity), 16.31% SP (specificity), 42.24% PPV (positive predictive value) and 81.18% NPV (negative PV).
ZACHARY PREDMORE, EMILY HOCH, JOHN CALOYERAS, HANGSHENG LIU, Boston, MA, Santa Monica, CA
Financial incentives have become increasingly popular to improve diabetes management, but its impact in the workplace remains largely unknown.
This study used disease program eligibility and participation data from a
Fortune 500 employer for 2003 to 2011. The data set contains 3,343 diabetes
patients who were eligible for a diabetes management program, with a total
of 8,519 patient-years. In 2009, the employer imposed a $600 penalty on eligible employees who did not participate in the program. We performed a logistic regression to see whether the penalty was associated with employee
participation. The eligible employees were 81.5% male, 68.5% Caucasian,
average age of 48.3 years, and had an average Charlson Comorbidity Index
(CCI) of 0.98. The unadjusted participation rate rose from 25.9% before the
introduction of the penalty to 30.9% after. Women (31.2% vs. 27.1%, p<0.01),
those over the age of 55 (32.8% vs. 26.2%, p<0.01), and Caucasians (37.7%
vs. 28.3%, p<0.01) were most likely to participate. Additionally, participants
had higher CCI (1.16 vs. 0.91, p<0.01). After adjusting for gender, age, region,
ADA-Funded Research
For author disclosure information, see page LB98.
LB36
Pediatrics—Obesity and Type 2 Diabetes
pay type, union status, zip code median income, and CCI, the introduction
of a penalty was associated with an increase in the participation rate from
25.5% (95% CI: 24.3% - 26.7%) to 30.8% (95% CI: 29.2% - 32.5%). Several
covariates had a significant effect on participation in the program, including sex, age, region, CCI, ethnicity, and blood pressure. These findings suggest that financial penalties can increase participation in a diabetes disease
management program, but the effect size is relatively small given penalty
size, which is about 10% of typical individual insurance premium. Employers
should not expect to see large increases in participation simply by increasing
the size of financial incentives. Making programs attractive to employees or
framing incentives in a way that is acceptable to employees might be a more
effective means of increasing employee participation.
that std measures have misclassified non-adherent multidrug pts and consequently underestimated the burden of non-adherence. Estimates of medication adherence in T2DM should be based on the pt’s regimen and not simply
any diabetes medication on hand.
141‑LB
Previous studies showed that variable glucose concentration results in
greater stress in endothelial cells than hyperglycemia per se. It was also
reported that the magnitude of glycemic excursions (MAGE) was positively
related to a urinary marker of oxidative stress in adults with type 2 diabetes
(T2D). Our purpose was to determine for the first time if MAGE is associated
with oxidative and vascular stress in adolescents without overt cardiovascular disease. Boys and girls 13-21 y old classified as normal weight (NW),
obese (Ob), or with T2D (N=10-12 per group) wore a continuous glucose monitor for 5 days to determine MAGE under free-living conditions. The T2D group
was not using insulin. The Ob group had normal glucose tolerance but had
hyperinsulinemia. All participants had low habitual physical activity (6,551
± 401 steps per day measured with accelerometry) and low aerobic fitness.
MAGE was higher (p<0.01) in the T2D group (82 ± 10 mg/dl) than either the
NW (30 ± 3) or Ob (33 ± 3) groups. Several markers of oxidative and vascular
stress were also increased in the T2D group. Oxidized LDL (NW: 48.4 ± 2.0;
Ob: 58.1 ± 3.8, T2D: 70.3 ± 5.0 U/l), an atherogenic particle elevated in T2D,
was strongly correlated with MAGE (r = 0.77, p<0.01). Likewise, the vascular
stress markers E-selectin (NW: 43.5 ± 4.9; Ob: 51.8 ± 8.8, T2D: 72.8 ± 7.5 ng/
ml) and ICAM-1 (NW: 181 ± 9; Ob: 195 ± 17, T2D: 231 ± 19 ng/ml) were highest in the T2D group and positively correlated with MAGE (r = 0.50 and 0.35,
respectively, p<0.01). The glycemic control marker, sRAGE (NW: 655 ± 54;
Ob: 356 ± 48, T2D: 344 ± 44 pg/ml) was lowest in the T2D group and inversely
correlated with MAGE (r = -0.38, p<0.01). These results demonstrate that
vascular stress is present adolescents and related to MAGE. Interventions
that reduce glycemic variability in youth may reduce vascular stress and the
risk for future cardiovascular disease.
Pediatrics—Obesity and Type 2 Diabetes
143‑LB
Glycemic Variability Is Associated with Vascular Stress Markers in
Adolescents With and Without Type 2 Diabetes
YANG LU, LILIAN SERPAS, PAULINE GENTER, DAVID CAMPA, ELI IPP, Torrance, CA
Screening for diabetic retinopathy (DR) is an efficient and cost-effective tool
to prevent visual impairment in people with diabetes. Yet relatively low rates
of DR screening are common, especially in public health delivery systems. To
improve DR screening rates in a single, large safety net health center that
serves predominantly low-income minority patients in South Los Angeles, we
undertook a survey of providers (P; n=18), staff (S; n=26), and patients (Pa;
n=101) to identify barriers to DR screening. Pa were surveyed at scheduled
clinic visits. Questionnaires were tested for basic language and cultural competency prior to use. The survey revealed a low DR screening rate among Pa;
only 51% were screened in the previous year, despite 78% reporting a physician recommendation. We examined potential barriers that might explain this.
Pa acknowledged the presence of 2 or more barriers in 44%; 1 barrier in 26%,
and none in 30%. Most common barriers were depression (22% of Pa) and
financial problems (26%); 14% reported both. Other barriers identified by Pa
were language issues, lack of transportation, and time pressure (all by 15% of
Pa). Women (59%) were more likely to report barriers (p<0.01). Pa who could
not adequately explain the need for DR screening also reported more barriers (p<0.01). Pa consisted of 27% African American and 71% Latino; though
no difference was observed in the number of barriers between these groups,
African American were less likely to be screened (p<0.01). We also compared
Pa survey results with P and S combined (n=44), revealing markedly divergent
perceptions of the importance of 9 barriers (all p<0.01). In summary, many barriers acknowledged by Pa were anticipated, but the striking divergence between Pa and P/S perception of their importance was not. We conclude that
preconceived ideas of barriers to DR screening do not match actual patient
perception. To increase DR screening rates, patient communities should be
engaged to find key elements for intervention.
Supported By: University of Oklahoma Health Sciences Center
144‑LB
Longitudinal Trends in Children with Severe Early Onset Obesity
VIDHU THAKER, MOLLY MCDONALD, MICHAELA BANKS, ADRIANNE LAGE,
STAVROULA OSGANIAN, Boston, MA
Supported By: California Community Foundation
Background: The prevalence of severe childhood obesity continues to increase. There is a significant risk of cardiovascular disease (CVD) mortality
in adults with greater body mass index (BMI) velocity at ages 8-13 years.
There is little information about the longitudinal trends of BMI in children
with severe early onset obesity, who likely will be at higher risk of CVD or
metabolic morbidity and mortality.
Methods: We used a validated electronic algorithm with structured and
unstructured data to identify children with severe early onset obesity (BMI
>120% of 95th percentile at an age < 6 years) visiting the clinics at Boston
Children’s Hospital. We extracted longitudinal growth and BMI data for at
least > 3 points/child over minimum 6 months with at least one value under
6 years of age using EHR data and WebPlot digitizer software for scanned
records. We excluded outlier data points using 3 methods. The longitudinal
trends of BMI and BMI velocity were analyzed using multivariate mixed effects adaptive spline model (SAS software) and superimposition by translation and rotation model (SITAR, R software).
Results: A total of 630 children were identified for the study - primary care
(76.3%) and weight management (57.5%) clinic. The gender distribution was
even (51% girls, 49% boys) with predominantly underrepresented minorities (39% African American, 48.2% Hispanic/Latino). The median age at visit
was 89 months with an average 33 observations/child. Trend analysis was
performed on 551 children, excluding outliers and inadequate data. The BMI
velocity is higher than predicted by CDC curves, boys 1.33kg/m2/yr (SE 0.03)
and girls 1.44kg/m2/yr (SE 0.04), p < 0.05. The velocity is highest between
11-14 years of age, girls later than boys.
Conclusion: Children with early onset obesity are at a high risk of CVD
based on BMI velocity. The highest velocity is reached in later childhood
calling for early identification and intervention, especially when obesity is
established prior to 6 years of age.
142‑LB
A Regimen-based Measure of Adherence and Costs Associated
with Nonadherence to Type 2 Diabetes (T2DM) Medications
RUO-DING TAN, GINGER S. CARLS, CHRISTIAN FROIS, EDWARD TUTTLE, Menlo
Park, CA, Boston, MA
In order to achieve recommended A1c targets, many patients (pts) require
multidrug regimens, but these regimens present increased hurdles to patient
adherence. Current methods of measuring patient adherence to multidrug
regimens may overestimate adherence. This study compares a common
measure of adherence, proportion of days covered (PDC) by any diabetes
medication, with a regimen-based refinement. Linked Optum-Humedica
data (1/2007-3/2014) that included claims, electronic medical records and
A1c were extracted for adult T2DM patients with at least one diabetes drug
fill. PDC and healthcare (medical and drug) patient costs were assessed over
the most recent continuously enrolled 1 year period. We compare PDC by
any diabetes medication ≥80%, a standard measure of adherence (std),
with regimen-based PDC≥80%. Regimen-based PDC accounts for initiation,
switching, discontinuation, and stockpiling at the class level. ADA guidelines
provide rules for determining whether a switch or discontinuation reflects
standard of care or non-adherence. 26,076 patients met study criteria having a mean age of 61 years, 52% male, and a mean A1c of 7.3%. 53% of
patients had A1c <7% and mean healthcare costs of $18,041. 52% of all
pts filled multiple drug classes. The fraction of multidrug pts classified as
non-adherent increased to 57% (regimen-based) from 36% (std). The excess
healthcare cost of non-adherent multidrug pts was $3,374 (regimen-based)
vs. $1,758 (std) (P<0.0001). Excess healthcare cost for all non-adherent pts
was $3,091 (19% above adherent pts) with the regimen-based measure vs.
$2,405 (14% above adherent pts) with the std measure (P<0.001). A measure
of PDC which more closely approximates T2DM medication regimen shows
Supported By: T32DK007699, P30DK040561
ADA-Funded Research
For author disclosure information, see page LB98.
LB37
POSTERS
Barriers to Diabetic Retinal Screening: Patient Perspective Is Dif‑
ferent from Providers and Staff
Clinical Diabetes/
Therapeutics
PAUL S. DASARI, BEN S. GANDOMANI, APRIL M. TEAGUE, AMEYA PITALE, MICHAEL OTTO, KEVIN R. SHORT, Oklahoma City, OK, Norman, OK
Pediatrics—Type 1 Diabetes
Pediatrics—Type 1 Diabetes
tionship with gender, age, HbA1c, IAA at diagnosis and HLA-DQ genotypes.
The study included 636 patients with T1D aged from 0.2 to 28.3 years at
diagnosis, with a follow-up of 1.4 to 25.3 years. Among the 636 patients,
5.4% were negative for all autoantibodies at diagnosis, 11.8% were positive
for 1 autoantibody, 22.5% for 2 autoantibodies, 31.8% for 3 autoantibodies and 28.6% were positive for the 4 autoantibodies. A nearly total disappearance of ICA was observed after 5 years, of GADA after 7 years and of
IA-2A after 8 years. The susceptible genotype 0301-0302/0501-0201 was
more prevalent in patients with multiple autoantibodies and at a younger
age at diagnosis. The most frequent autoantibody among the patients was
ICA. IAA and ICA were more frequent in younger patients at diagnosis and
GADA in older patients. Male gender, younger age, higher HbA1c and the
presence of autoantibodies (especially of ICA) at diagnosis were related to
lower C-peptide levels. Male gender, older age, and positivity of IAA at diagnosis were correlated with longer persistence of ICA. Male gender was also
correlated with longer persistence of GADA. Older age, lower HbA1c and
positivity of IAA at diagnosis, as well as 0301-0302/0301-0302 genotype,
were associated with longer persistence of IA-2A. During the long follow-up
of this study (25 years), there was an association between the evolution of
the autoantibodies and age, gender, HbA1c, C-peptide, positivity of IAA at
diagnosis and HLA-DQ genotype (only for IA-2A). In conclusion, the evolution
of C-peptide was influenced by the presence of autoantibodies at diagnosis,
age, gender and HbA1c at diagnosis.
145‑LB
HOMA2β Is Predictive of the Development of Type 1 Diabetes in Tri‑
alNet Pathway to Prevention Participants
POSTERS
Clinical Diabetes/
Therapeutics
FARAH MEAH, PING XU, LINDA A. DIMEGLIO, JAY M. SOSENKO, SUSAN GEYER,
CARMELLA EVANS-MOLINA, TYPE I DIABETES TRIALNET GROUP, Indianapolis,
IN, Tampa, FL, Miami, FL
Decreases in β cell function as measured by changes in the first phase insulin response and β cell glucose sensitivity are useful predictors of progression towards type 1 diabetes (T1D) but require the performance of provocative
procedures such as intravenous and oral glucose tolerance tests (OGTT). The
homeostasis model assessment (HOMA2) online calculator is a validated
mathematical tool commonly used in type 2 diabetes research that assesses β
cell function (HOMA2β) and insulin sensitivity (HOMA2s) using fasting glucose
and insulin measurements. However, the utility of HOMA2β in predicting T1D
progression has not been previously tested. To this end, the HOMA2 calculator
was used to estimate HOMA2β in non-diabetic first-degree (age 1-45 yrs) and
second or third-degree (age 1-20 yrs) relatives of individuals with T1D who
were positive for one or more β cell autoantibodies (aab) and followed longitudinally in the TrialNet Pathway to Prevention (PTP) Cohort. A Cox proportional
hazards model was used to determine associations between HOMA2β at
study entry and time to progression to T1D with adjustment for age, HOMA2s,
and peak C-peptide on OGTT. 2,700 aab+ PTP participants entered the protocol
(mean age 19.6 ± 13.7 yrs, HOMA2β 92.8 ± 43.5, HOMA2s 143.3 ± 99.6, peak
C-peptide from OGTT 8.1 ± 3.7 ng/mL); 543 participants developed T1D during
the monitoring period. In multivariate analysis, likelihood of T1D moderately
but significantly increased with decreasing HOMA2β among all aab+ subjects
(HR 0.987; 95% CI 0.983-0.992; p<0.0001) and in subjects with multiple (≥2)
aabs (n = 475, HR 0.989; 95% CI 0.984-0.994; p<0.001). Furthermore, HOMA2β
was positively correlated with peak C-peptide (r=0.54; p<0.0001). Our results
suggest that decrements in HOMA2β may have utility in predicting progression to T1D in individuals with established autoimmunity. Future analyses will
focus on combining HOMA2β with additional metabolic and immunologic endpoints to improve T1D risk assessment.
148‑LB
Prepubertal Children Need More Bolus Insulin than Derived from
the 500-Rule
RAGNAR HANAS, KRISTIN LUNDQVIST, ANNIKA SJÖSTRAND, Uddevalla, Sweden
Objectives: The “500-rule” has been used extensively to find the insulin:
carbohydrate (IC) ratio when carbohydrate counting is practiced, both in
adults and children. Data is lacking on validating this in young children.
Methods: We initiated carbohydrate counting by finding the individual IC
for each child by dividing the carbohydrate content in grams by the insulin
dose (breakfast and other meals separately). Insulin correction factor (ISF)
was defined by the “100-rule” (100 divided by total daily insulin dose (TDD).
IC and ISF were adjusted at each visit. Data was taken from pump downloads. IC and ISF were recalculated to “rules” (IC/ISF multiplied by TDD).
Results: 21 prepubertal children aged 7.0±2.3 (±SD) (range 2-10) years with
diabetes duration 3.0±1.9 (0.5-7.7) years used the pump bolus guide for carbohydrate counting (CC) and correction boluses. 15 had started with a pump
from the onset of diabetes. Their HbA1c was 53±6 mmol/mol (7.0±0.5%), and
none had experienced severe hypoglycemia with unconsciousness or seizures since diabetes diagnosis. Their total daily dose was 0.7±0.1 U/kg/24h
(range 0.5-1.0), and their percentage basal insulin was 38±11%. The median breakfast rule was 211 (Q, quartiles 137; 285), and for other meals 434
(Q 336; 532). The median ISF rule was 113 (Q99; 127) in the morning, and 122
(Q 107; 137) during the rest of the day. There was a significant correlation
between the total daily insulin dose (U/24h) and both IC and ISF.
Conclusions: Prepubertal children seem to need more bolus insulin for
meals than calculated from the 500 rule, especially at breakfast, but less
insulin for corrections than calculated from the 100 rule. When adjusting the
bolus wizard according to the downloaded data and parent’s experience of
insulin effect, a good metabolic control can be achieved with a low rate of
severe hypoglycemia.
146‑LB
Early Identification of Cardiac Autonomic Neuropathy Using Com‑
plexity Analysis
PENELOPE KANE, PETER LARSEN, ESKO WILTSHIRE, Wellington, New Zealand
Abnormal heart rate variability (HRV), a marker of cardiac autonomic neuropathy (CAN), contributes to mortality in adults with diabetes. Traditional HRV
measures do not consistently detect abnormalities in youth with type 1 diabetes
(T1D). We aimed to assess whether complexity analysis of HRV would identify
CAN earlier than traditional methods, in youth with T1D. We studied 17 youth
with T1D [age 12.8±1.8 years, duration 4.5±2.6 years, HbA1c 7.9±1%] and 15 controls (age 12.9±1.6), with 12 lead EKGs (sampling frequency 1000Hz) recorded
continuously for 10 mins. Recordings were analysed using Labview software and
an algorithm for complexity analysis (sample entropy and detrended fluctuation
analysis), with standard methods for time-domain and spectral analysis. Clinical (auxology, BP, insulin dose) and laboratory (lipids, HbA1c, electrolytes) data,
as well as heart rate (HR) and BP responses to standing were obtained. Data
were analysed using chi-squared, student’s t or Mann Whitney-U tests and Pearson’s or Spearman’s correlation. Youth with T1D had significantly higher sample
entropy (0.149±0.011 vs. 0.136±0.014, p=0.015) than controls suggesting increased complexity in HRV, but similar detrended fluctuation analysis (0.67±0.12,
0.65±0.13, p=0.68). They had increased % high frequency (62±14% vs. 46±16%,
p=0.017) and reduced mid-frequency (18±7.5% vs. 26±1.5%, p=0.019) power on
spectral analysis, but no differences in HR or BP responses to standing or timedomain analysis of HRV. In T1D, sample entropy correlated strongly with triglycerides (TGs) (r=0.76, p=0.001) and detrended fluctuation analysis correlated
strongly with serum potassium (K+) (r= -0.86, p<0.001). Complexity analysis of
HRV may detect CAN earlier than traditional measures. Our data suggest serum
potassium and TGs may contribute to abnormal HRV. It is conceivable an interaction between abnormal HRV and serum K+ contributes to the “dead-in-bed”
syndrome in youth with T1D, which would be worth further investigation.
Supported By: Fyrbodal Research Institute
149‑LB
Antibiotic Use in Early Childhood and the Development of Type 1
Diabetes Autoimmunity: The TEDDY Study
KAISA M. KEMPPAINEN, KENDRA VEHIK, RONALD J. CANEPA, ALEXANDRIA N.
ARDISSONE, AUSTIN G. DAVIS-RICHARDSON, OLLI G. SIMELL, JORMA TOPPARI,
ANETTE-GABRIELE ZIEGLER, MARIAN REWERS, ÅKE LERNMARK, WILLIAM A.
HAGOPIAN, JIN-XIONG SHE, BEENA AKOLKAR, DESMOND SCHATZ, MARK A.
ATKINSON, MARTIN J. BLASER, JEFFREY P. KRISCHER, ERIC W. TRIPLETT, TEDDY
STUDY GROUP, Gainesville, FL, Tampa, FL, Turku, Finland, Munich, Germany, Aurora,
CO, Malmö, Sweden, Seattle, WA, Augusta, GA, Bethesda, MD, New York, NY
Antibiotic treatment can have profound effects on gut microbiota. Recent
studies have described a link between the gut microbial community and risk
of type 1 diabetes (T1D). Here the association between the appearance of
islet autoantibodies (IA) and the use of antibiotics during the first 4 years of
life in children genetically at risk for T1D is assessed. In the TEDDY study,
8495 children with T1D-associated HLA genotypes from Sweden, Finland,
Germany, and the U.S. were enrolled at 3 months of age and tested for IA
(mIAA, IA2A, GADA) every 3 months up to 48 months. Persistent autoimmunity was defined as an IA present on ≥2 consecutive visits and was confirmed
147‑LB
Evolution of Diabetes-associated Autoantibodies and of C-Peptide
Since the Onset of Type 1 Diabetes
HARRY R. DORCHY, ANDRIANA ASIMAKOPOULOU, Brussels, Belgium
The objective is to investigate the immunological markers (ICA, GADA,
IA-2A) and the residual insulin secretion (as measured by the C-peptide
levels) from the onset of diabetes, their evolution over time and their relaADA-Funded Research
For author disclosure information, see page LB98.
LB38
Pregnancy—Basic Science
Pregnancy—Clinical
in 476 subjects (5.6%) at a median age of 21.6 months. Antibiotic use (oral
or parenteral) was reported every 3 months. Cox models assessed associations between the use of common antibiotics (penicillins, cephalosporins,
and macrolides) and the instantaneous risk of developing persistent IA.
Amoxicillin use, but not other antibiotics, 3-6 months prior to seroconversion increased the risk of multiple IAs (HR=1.27, 95% CI=1.01-1.59, p=0.04).
However, cumulative use of penicillin-based antibiotics over time (HR=0.98),
in the first year (HR=1.02), in the first two years (HR=0.99), and within a year
before seroconversion (HR=1.02); or use of other antibiotics, were not significantly associated with risk of any or multiple IAs. All analyses were adjusted
for HLA, first degree relative status, gender, breastfeeding, probiotic use,
mode of delivery, maternal antibiotic use during pregnancy, country, and
season of birth. These findings suggest that amoxicillin use is associated
with the risk of developing IA in high-risk children. Further research assessing causal relationships between antibiotic use, gut microbiota, and mucosal
immunity is needed for better understanding the mechanisms involved in
T1D development.
ment could affect cellular function and development in F1 and F2 embryos.
To test this hypothesis, ICR mice (F0) were bred and assigned to control (C)
or undernutrition (UN) - 50% caloric restriction, ED 11.5 to 13.5; embryos
were collected at E13.5 for isolation of mouse embryonic fibroblasts (F1-C
and UN MEFs) for ex vivo culture. Using FACS-based analysis, we observed
a 25% reduction in the ratio of cells in G0-G1 to G2-M phase in F1-UN-MEFs.
In parallel, we observed a 17-42% reduction (P<0.05) in expression of cell
cycle regulatory genes, including cyclins and aurora kinases, and upregulation (4-9 fold) of the cell cycle regulators E2f1 and E2f4, the insulin and IGF-1
receptors. Interestingly, the MEFs isolated from F2 embryo offspring of F1UN males also displayed a 40% lower proliferation rate compared to F1-C,
despite no change in cell cycle phase. In summary, in utero undernutrition
reduces proliferation and cell cycle progression of MEFs cultured ex vivo,
and also has a striking impact to reduce proliferation in second-generation
MEFs. Together, these data indicate that intergenerational inheritance of
metabolic disease may be linked to epigenetic mechanisms perturbing transcriptional control of cellular proliferation and cell cycle regulation.
Supported By: CAPES; Ajinomoto Pharmaceuticals Co., Ltd.
152‑LB
Translocator Protein (TSPO): An Early Marker of Placental Mito‑
chondrial Dysfunction in Pregnancy Affected by Obesity
JOANNA ZHOU, LUCIANA LASSANCE GOMES, MARICELA HAGHIAC, JUDI MINIUM, PATRICK M. CATALANO, SYLVIE HAUGUEL-DE MOUZON, Cleveland, OH
150‑LB
Stress Trajectories in Newly Diagnosed Youth with Type 1 Diabetes
and Their Caregivers: The Moderating Role of Resilience
Obesity in pregnancy is associated with decreased maternal estrogen and
progesterone concentrations combined with global mitochondrial dysfunction and lower cholesterol content in placenta. The aim of this study was
to investigate mechanisms for impaired placental mitochondrial function in
early pregnancy. Maternal blood and placenta tissue were collected at voluntary termination of pregnancy (9-11 weeks of gestation) from 55 women
with BMI ranging from 21.3-54.3 and no metabolic disease. Maternal total
plasma cholesterol and progesterone were assayed by ELISA. Placental ATP
and mitochondrial cholesterol were measured via fluorometric assays. Expression of the mitochondrial cholesterol transporters, MLN64 and TSPO
were quantified by Western blot. Mitochondrial DNA copy number and
VDAC protein were assessed as markers of mitochondrial density. Plasma
progesterone was lower in obese (BMI>30) compared to normal weight
(BMI <25) women (27.9±7.0 vs. 43.3±18.9 ng/mL, p=0.001). Expression of
the outer mitochondrial membrane cholesterol transporter TSPO was 60%
lower (p=0.03) in obese compared to lean women, whereas the endosomal
cholesterol transporter, MLN64, was unchanged. Placental mitochondrial
cholesterol concentration was 20% lower in obese vs. lean (p<0.0003). Placental ATP content did not vary as a function of BMI. Placental mtDNA and
VDAC expression were unchanged, suggesting similar mitochondrial number
in lean and obese women. In conclusion, maternal obesity impairs placental mitochondrial cholesterol transport and progesterone synthesis early in
pregnancy. TSPO protein may serve as an early marker of defects in placental mitochondrial function in pregnancy affected by obesity. The resulting
impairment in intrauterine progesterone balance, may yield adverse consequences for maintenance of pregnancy and fetal development.
JOYCE P. YI-FRAZIER, KATIE COCHRANE, KATHRYN B. WHITLOCK, MICHAEL
PASCUAL, NATALIE BEAUREGARD, CONNOR MITROVICH, NEIL PANLASIGUI,
CATE PIHOKER, Seattle, WA
It is well-known that stress is associated with poor outcomes for youth
with diabetes. Less is known about the trajectory of stress over time and the
potential moderators of that stress. Resilience is a construct describing an
individual’s capacity to maintain psychological and/or physical well-being in
the face of stress, and it has been shown to buffer the negative effects of
stress in adults with diabetes. Our study proposed to explore the impact of
resilience on the trajectory of stress over the first year of diagnosis for adolescent youth with type 1 diabetes (ages 10-17) and a primary caregiver. We
assessed resilience (Connor-Davidson Resilience Scale) and stress (overall
stress rating) at time of new onset and every 3 months over the first year.
Stress trajectories were identified using semiparametric group-based trajectory modeling with backward model selection strategy and final model
selection based on minimizing Bayesian Information Criterion. Resilience
scores across time were stable for both patient and parent groups. For patients, 3 patterns of stress were identified: 1) stable low stress (n=33), 2)
stable moderate stress (n=22), and 3) stable high stress (n=5); no patterns
indicated significant change across time. Compared to the low stress group,
the moderate and high stress groups had lower baseline resilience (p’s =
.04, .03 respectively). For parents, 4 patterns of stress were identified: 1)
initial high stress quickly decreasing to stable low stress (n=4) , 2) initial high
stress, briefly decreasing to moderate stress but returning to high stress,
(n=7), 3) stable moderate stress (n=18), and 4) initial high stress decreasing
gradually to moderate stress (n=31). Parent resilience was not associated
with the parent stress trajectories. In sum, trajectories of parents’ stress
seemed much more variable over the first year than youth. However, resilience was only found to moderate stress trajectories in youth.
Supported By: National Institutes of Health (R01HD22965)
Pregnancy—Clinical
Supported By: Seattle Children’s Center for Clinical and Translational Research
153‑LB
The UPBEAT RCT: A Complex Intervention of Diet and Physical Ac‑
tivity in 1,555 Obese Pregnant Women
Pregnancy—Basic Science
LUCILLA POSTON, RUTH BELL, HELEN CROKER, KEITH M. GODFREY, ANGELA
C. FLYNN, LOUISE HAYES, NINA KHAZAEZADEH, SCOTT M. NELSON, EUGENE
OTENG-NTIM, NASHITA PATEL, STEPHEN C. ROBSON, JANE SANDALL, THOMAS A.B. SANDERS, PAUL T. SEED, NAVEED SATTAR, JANE WARDLE, MELISSA K.
WHITWORTH, ANNETTE L. BRILEY, THE UPBEAT TRIAL CONSORTIUM, London,
United Kingdom, Newcastle, United Kingdom, Southampton, United Kingdom, Glasgow, United Kingdom, Manchester, United Kingdom
151‑LB
In Utero Caloric Restriction Induces Intergenerational Cell Cycle
Dysregulation
VICENCIA M. SALES, YUSUKE ADACHI, ELIZABETH J. RADFORD, ANNE FERGUSON-SMITH, MARY-ELIZABETH PATTI, Boston, MA, Cambridge, United Kingdom
Nutrition during intrauterine development is critical for normal fetal development and metabolic health during later life and in subsequent generations. We have previously demonstrated that transient exposure to caloric
restriction during intrauterine life causes low birth weight, impaired glucose
tolerance and obesity in not only offspring mice (F1), but also in F2 offspring
of F1 males, despite no further nutritional insult. Transmission of phenotypes
via the male lineage implicates alterations in sperm. Consistent with this
hypothesis, we have recently demonstrated altered sperm methylation of F1
male mice and perturbed gene expression at differentially methylated loci in
F2 mouse embryos. We therefore hypothesized that the intrauterine environ-
The risk of gestational diabetes (GDM) increases with obesity. Numerous
interventions in obese women have focused on limiting gestational weight
gain (GWG). The UPBEAT intervention was designed to prevent GDM. 1555
obese pregnant women (mean BMI 36.3 kg/m2; 63% White, 26% Black; 78%
4th or 5th quintiles of deprivation) were randomized (15 +0 to 18+6 weeks’ gestation) to standard antenatal care or a health trainer delivered intervention
(weekly, 8 weeks) of dietary advice (focus, low glycemic index) and physical
activity. All women had an OGTT (27+0 -28+6 weeks’ gestation). Compared to
standard care, the intervention (mean 7 sessions/woman) reduced dietary
glycemic load by 26.3 units (95% CI -31.6 to -20.9) (19% lower), saturated fat
ADA-Funded Research
For author disclosure information, see page LB98.
LB39
POSTERS
Supported By: National Institutes of Health; National Institute of Diabetes
and Digestive and Kidney Diseases; National Institute of Allergy and Infectious
Diseases; Eunice Kennedy Shriver National Institute of Child Health and Human
Development; National Institute of Environmental Health Sciences; JDRF; Centers
for Disease Control and Prevention
Clinical Diabetes/
Therapeutics
Pregnancy—Clinical
155‑LB
intake (% energy) by 1.03% (-1.35 to -0.70) (8% lower) and total energy intake
by 1.08MJ (-1.36 to -0.80) (14% lower). Protein intake increased (p<0.001)
and total carbohydrate intake (p=0.02) fell. Physical activity improved by 295
(112.1 to 477.6) metabolic equivalents min/wk (21.3% higher). Maternal GWG
was reduced by 0.55 kg (-1.1 to 0.0), from 7.76 to 7.19kg and the sum of skinfold thicknesses decreased (p=0.010). Despite achieving significant changes
in dietary and physical activity behaviors, reducing GWG and improving
body composition, the intervention did not reduce GDM (IADPSG; control
26.6% vs. intervention 25.5%, -1.1% (-6.0 to 3.9)). Large for gestational age
(LGA) deliveries (>90 th customized centile, primary neonatal outcome) were
similar (control 8.3%; intervention 9.3%) as were LGA by population centiles
(11.1%,12.6%), SGA and preterm birth. BMI, ethnicity and age were similar
in participants and women who declined. UPBEAT, the largest complex intervention study to date in obese pregnant women provides a safe strategy
to improve diet, physical activity, GWG and body fat. However, in ethnically
diverse obese women of mostly low socioeconomic status, we conclude that
GDM is not preventable by an intense lifestyle intervention in pregnancy.
Differential Expression of MicroRNA in Human Umbilical Vein En‑
dothelial Cells from Infants of Diabetic Mothers
JEANIE B. TRYGGESTAD, APRIL M. TEAGUE, ANU VISHWANATH, DAVID M.
THOMPSON, YUSUKE TAKAHASHI, JIAN-XING MA, STEVEN D. CHERNAUSEK,
Oklahoma City, OK, Bangalore, India
Perinatal conditions such as diabetes mellitus (DM) have been shown to
“program” offspring for certain metabolic phenotypes later in life. The mechanisms underpinning this sequence are not well understood, but epigenetic
modification has come to the forefront as a potential mediator of the association of perinatal conditions and future cardiometabolic disease. One possible
mechanism for epigenetic modification involves micro-RNAs (miRNAs), small,
non-coding RNAs that bind to complementary sequences within 3’UTR of
messenger RNAs (mRNAs) and modulate gene expression, typically repressing translation of targeted mRNAs. The purpose of the current study was to
identify miRNAs that are differentially expressed in the human umbilical vein
endothelial cells (HUVEC) in infants of mothers with diabetes compared with
infants born to mothers with euglycemia. Total RNA including miRNAs was
extracted from freshly isolated HUVEC cells from the umbilical cords of infants born to mothers with gestational diabetes as defined by the American
Diabetes Association and infants born to mothers with normal glycemia. A microarray of 2,019 miRNA species probed for differentially expressed miRNAs.
Twenty-seven miRNA species were selected for validation by RT-PCR from the
microarray based on a significant difference between the groups or evidence
from literature. Exact permutation tests found 5 of these 27 miRNA species to
be differentially expressed (miR-126, P=0.0004; miR-30c-5p, P=0.0015; miR452-5p, P=0.0172; miR-let-7a, P=0.0004; miR-let-7g, P=0.0004). Predicted targets of these differentially expressed miRNAs include IRS1 and vascular cell
adhesion molecule 1 (VCAM1). In conclusion, we have identified 5 miRNA species that are differentially expressed in HUVECs from diabetic pregnancies.
Future work will focus on validating the targets of these miRNA and further
elucidating their impact on cardiometabolic health in the offspring.
POSTERS
Clinical Diabetes/
Therapeutics
Supported By: UK National Institute for Health Research (RP-PG-0407-10452);
GSTT/KCL Biomedical Research Centre; Chief Scientists Office, Scotland; Guys and
St. Thomas’ Charity; Tommy’s Charity
Gestational Diabetes Mellitus
154‑LB
MUSTAFA DEMIRPENCE, NUR DEMIRPENCE, ALIYE P. TÜTÜNCÜOGLU, GUZIDE
GONCA ORUK, NESIL ATALAY, AHMET GORGEL, BANU ARSLAN, HAMIYET YIL·
MAZ, MITAT BAHCECI, Izmir, Turkey, Diyarbakir, Turkey
Recent observations suggest that a defective glucose stimulated insulin
secretion by glucagon-like peptide-1 (GLP- 1) plays a role in the pathogenesis
of type 2 diabetes (T2D). Whether such a defect is impaired in Gestational
diabetes mellitus (GDM) remains to be ascertained. The aims of this study
were to evaluate how change GLP-1 levels among highly risky pregnancy
with GDM. We investigated fasting and after 75-g oral glucose tolerance
test (OGTT) GLP-1 responses in pregnant women with and without GDM.
75-g-2h OGTT was performed in 20 GDM at 25.1±7.1 weeks and 11 without GDM women 26.8±4.8 weeks of gestation, for determination of plasma
GLP-1, glucose, insulin, C-peptide levels. All of them were evaluated among
fasting blood sample. Besides glucose, insulin, c-peptide, GLP-1 levels were
also performed among both 60. and 120. minutes blood samples of OGTT.
Data analysis was performed by SPSS 15.0 package programmer. Continuous variables were presented with mean and standard deviation (SD) values.
Man Whitney U tests was performed to evaluate the statistical significance
between two different medians. p < 0.05 was accepted as statistically significant. All results were summarized (Table). Women with GDM were found
to have lower fasting GLP-1 levels than women without GDM (p=0.028).
Although it was not significant, GLP-1 levels of 60. and 120. minutes were
also lower among women with GDM. GLP-1 levels also may have a part as
decreasing in the etiopathogenesis of GDM like T2D.
Supported By: Oklahoma Shared Clinical and Translational Resources
156‑LB
The Impact of Group Compared with Individual Prenatal Care on
Gestational Diabetes Mellitus: The South Carolina Centering Preg‑
nancy Expansion Project
LIWEI CHEN, EMILY HEBERLEIN, SARAH COVINGTON-KOLB, AMY PICKLESIMER,
Clemson, SC, Greenville, SC
Centering Pregnancy group prenatal care (CPNC), a patient-centered model
of integrating medical checkups with social support and education in a group
setting, has shown promise in reducing preterm birth. However, the impact of
CPNC on gestational diabetes mellitus (GDM) has not been investigated. This
retrospective cohort study included pregnant women who received prenatal
care from 7 obstetric practices participated in the South Carolina (SC) Centering Pregnancy Expansion Project. Using SC birth certificate data linked with
Medicaid claims, we compared the incidence of GDM in women who chose
CPNC and had a live birth between August, 2013 and September, 2014 to
women from the same practices receiving standard individual prenatal care
(IPNC). We applied multivariate regressions to estimate the ORs and 95% CI
with controlling for demographic and clinical risk factors. The crude rate of
GDM was 6.42% in IPNC (N=6,807) and 4.14% in CPNC (N=604) (P=0.03). Compared to women in IPNC, women in CPNC were less likely to develop GDM
(OR=0.53; 95% CI: 0.34-0.81; P=0.003) after adjusted for age, race, education,
marital status, parity, time of entering and adequacy of prenatal care. The OR
only slightly changed and remained significant (OR=0.58; 95% CI: 0.38-0.89;
P=0.012) after additional controlling for pre-pregnancy BMI category, gestational weight gain, and gestational age. In conclusion, approximately 40%
lower risk of GDM was observed in pregnant women who received CPNC as
compared with women receiving IPNC, suggesting that Centering Pregnancy
has clinically significant benefits on reducing the occurrence of GDM.
Table. Evaluation of All Results of Women With and Without Gestational
Diabetes Mellitus.
GDM + (n=20)
GDM - (n=11)
p value
Mean±SD
Mean±SD
Age (year)
31.4±5.4
27.8±3.8
0.046
A1c (%)
5.7±0.3
5.4±0.4
0.039
GLUCOSE (mg/dl)
Fasting
88.6± 11.4
80.5±7.3
0.051
60.min
177.5 ±33.3
147.8±23.8
0.002
120.min
147.0±36.5
113.3±21.4
0.017
C-PEPTIDE (ng/mL)
Fasting
2.3±0.8
1.8±1.6
0.091
60.min
10.9±4.0
8.6±2.9
0.076
120.min
11.7±4.1
8.1±2.3
0.016
INSULIN (mU/ml)
Fasting
14.8 ±4.9
10.5±3.7
0.024
60.min
122.4 ±62.1
87.1±48.0
0.151
120.min
105.4±65.4
66.8±29.1
0.237
GLP-1
Fasting
5.5±1.8
16.0±18.3
0.028
60.min
5.9±1.9
11.5±13.9
0.237
120.min
7.7±9.8
10.1±9.8
0.434
Supported By: South Carolina Department of Health and Human Services
157‑LB
Sex of Offspring Influences DNA Methylation Patterns in Placentae
from Native American and Hispanic Women with Diabetes during
Pregnancy
SARA E. PINNEY, APRIL TEAGUE, JULIE DOBKIN, TIFFANY RUIZ, STEVEN CHERNAUSEK, REBECCA A. SIMMONS, Philadelphia, PA, Oklahoma City, OK
Offspring of mothers with diabetes during pregnancy (DDP) are at increased
risk for obesity and type 2 diabetes, which may be influenced by off‑spring sex.
The mechanisms responsible for the phenomenon are unknown. We hypothesize
that that DDP alters genome-wide DNA methylation resulting in differentially
methylated loci of genes critical to glucose homeostasis resulting in diabetes
and metabolic syndrome in the offspring. To test this hypothesis we mapped
genome-wide DNA methylation with the Infinium 450K Human Methylation Ar-
ADA-Funded Research
For author disclosure information, see page LB98.
LB40
Epidemiology—Aging
ray using a nested case-control design from a cohort of Native American and
Hispanic women with DDP. Term fetal placentae were collected and matched 1:1
with controls based on maternal age, race/ethnicity, and offspring sex. Methylation status at each probe site was determined by calculating = M/(M+U=100)
(M= methylated signal; U= unmethylated signal). Differential methylation (dm)
was calculated as Δ per pair and averaged across all samples.
development. Most of previous studies were case-control which could not
give a cut-off value for practice. This study was to investigate whether sex
hormone-binding globulin (SHGB) was a biomarker associated with GDM development in later pregnancy. This prospective cohort study was conducted
in four hospitals. A total of 713 pregnant women who visited these centers
during the first trimester (<12 weeks of gestation) between May 2013 and
May 2014 were enrolled. SHGB level were measured at 4-12 weeks of gestation. Among the 443 participants included in the final analysis, 41 (9.3%)
developed GDM. Participants were divided into 4 quartiles, according to
SHBG levels (Q1: <70.84 nmol/L, n=111; Q2: 70.84-116.35 nmol/L, n=110);
Q3: 116.35-158.49 nmol/L, n=111; Q4: >158.49 nmol/L, n=111). Among them,
15.3%,17.2%, 6.3%, and 2.7% developed GDM, respectively, in Q1, Q2, Q3,
and Q4. No differences were found between Q1 and Q2, and Q3 and Q4,
with the Q1/Q2 group showing higher rates. Finally, at SHBG >116.35 nmol/L,
GDM rates were significantly decreased. Decreased SHBG concentrations
during the first trimester may predict GDM development.
Table.
Female offspring
10
27.9 (23-33)
247
4
56 (-28% - +23%) 21 (-28.7% - +16.9%)
25
14 (19)
1 (1)
12 (16)
21 (29)
24 (33)
Supported By: Science and Information Technology of Guangzhou, China
(12C22021649)
5
0
1 (5)
0
3 (15)
17 (80)
160‑LB
Blood Levels of Glycated CD59 (GCD59) as a Novel Biomarker for
Screening and Diagnosis of Gestational Diabetes
PAMELA GHOSH, MIGUEL A. LUQUE-FERNANDEZ, ANAND VAIDYA, MICHAEL
CHOREV, CHLOE ZERA, THOMAS F. MCELRTAH, MICHELLE WILLIAMS, ELLEN W.
SEELY, JOSE HALPERIN, Boston, MA
CD59 is a membrane-anchored complement regulatory protein that inhibits
formation of the membrane attack complex (MAC). A soluble form of CD59,
shed off cell membranes, is present in human blood. We recently reported
that plasma levels of glycated CD59 (GCD59) served as a sensitive and specific
biomarker for acute and chronic glucose handling in non-pregnant individuals
(JCEM. 2014;99:999). We therefore hypothesized that plasma levels of GCD59
may represent a sensitive method to screen for impaired glucose tolerance and
gestational diabetes (GDM) in pregnant women. We conducted a prospective
study of plasma GCD59 levels in 1114 consecutive pregnant women undergoing
two-step screening for GDM at Brigham and Women’s Hospital. Normal glucose
tolerance (NGT) was defined as a 50gr glucose load test (GLT) value <140 mg/dL,
impaired glucose tolerance (IGT) as a GLT value >140 mg/dL followed by 0 or 1
abnormal value on a 100gr/3hr glucose tolerance test (OGTT), and GDM by OGTT
Carpenter-Coustan criteria. GCD59 was measured in plasma samples using a
recently reported ELISA (AJH. 2013;88-670). We used ROC curves to assess the
sensitivity and specificity of GCD59 to classify women with NGT, IGT or GDM.
Infant birth weight z-scores were calculated using population based growth
norms. Mean plasma levels of GCD59 at 24-26 weeks gestation were 0.09±0.04
units in women with NGT (n=698) and 2.9±0.1 units in women with GDM (n=126;
p< 0.0001). Plasma values of GCD59 classified with high sensitivity and specificity women with GDM (ROC curve AUC = 0.93), as well as women with IGT
and NGT (ROC AUC 0.79). Importantly, higher concentrations of maternal GCD59
were associated with higher incidence of large for gestational age newborns (zscore >2). As most pregnant women are screened for GDM using a cumbersome
testing methodology, we conclude that a one time measurement of GCD59 in the
late second trimester represents a promising new biomarker for screening and
diagnosis of impaired glucose tolerance and GDM.
cadherins, cell adhesion,
glycoprotein,
plasma membrane, metal
ion transport,
binding, cation binding, transcription regulation,
glucose metabolism,
metal binding,
transcription regulation
cation binding
In summary, DDP alters placental DNA methylation at metabolicallyrelevant loci in a sex specific manner, with more probes affected in males.
This finding may begin to explain the long-term metabolic effects of DDP
on offspring as the placenta functions to regulate the environment of the
developing fetus. Future studies will correlate site-specific methylation with
mRNA expression via RNA-Sequencing.
Supported By: American Diabetes Association (1-10-CT-09 to S.C.); National
Institutes of Health (R01DK089034-03)
158‑LB
The Effect of Maternal Nutritional Intake during Pregnancy in Obese
Women on Infant Body Composition
PRANEETA CHODAVARAPU, SHARON GROH-WARGO, DENNIS SUPER, PATRICK
M. CATALANO, Cleveland, OH
The purpose of this study was to determine the relationship of maternal nutrition in obese women on infant body composition. Healthy, obese (Body Mass Index; BMI > 25 kg/m2), pregnant women between the ages of 18 and 40 years and
8 to 16 weeks of gestational age (GA) were recruited in the antenatal clinic of
MetroHealth Medical Center. Exclusion criteria were any maternal (i.e., diabetes)
or infant (i.e. respiratory distress) illnesses. During the first and third trimesters
(GA 14.4 + 1.7 and 35.2 + 0.8 weeks), all mothers underwent a detailed nutritional
assessment (Harvard Food Frequency Questionnaire, 2007, Harvard University,
Cambridge, MA), body composition by air displacement plethysmography using
the Bod Pod (COSMED, Rome, Italy) and BMI (weight on a calibrated scale and
height using stadiometer). Infants had their body composition measured during
the first week of life by the Pea Pod (COSMED). Of the 38 mothers enrolled, the
following first trimester maternal characteristics were associated with their infant’s percent body fat (% BF): carbohydrate intake (Pearson r = + 0.346, p = 0.034
two-tail); linoleic acid (r = + 0.334, p = 0.040); maternal BMI (r = + 0.284, p = 0.084);
omega 3:6 ratio (r = - 0.280, p = 0.090) and physical activity (r = - 0.329, p = 0.044).
In a stepwise multiple regression analysis, carbohydrate intake, Omega 3:6 ratio
and physical activity in early pregnancy were independently associated with the
infant’s % BF (adjusted r squared 0.245, P = 0.006). None of the above variables
obtained in the third trimester were associated with infant’s % BF. In summary,
increased maternal carbohydrate intake, decreased omega 3:6 ratio and decreased physical activity during early but not in late pregnancy are significantly
associated with higher infant % BF.
Supported By: National Institutes of Health-National Institute of Diabetes and
Digestive and Kidney Diseases (DK095429)
Epidemiology—Aging
161‑LB
Follicle-stimulating Hormone Associates with Prediabetes and
Diabetes in Postmenopausal Women
NINGJIAN WANG, LIN KUANG, QIN LI, BING HAN, YI CHEN, CHUNFANG ZHU,
YINGCHAO CHEN, FANGZHEN XIA, ZHEN CANG, CHAOXIA ZHU, MENG LU, YING
MENG, HUI GUO, CHI CHEN, DONGPING LIN, YINGLI LU, Shanghai, China, Hangzhou, China
Objective: Follicle-stimulating hormone (FSH) was reported to be associated with obesity in pre- and post-menopausal women. Few studies concern
the association between FSH and glucose metabolism. We aim to investigate whether the variation of FSH is associated with prediabetes and diabetes in postmenopausal women.
Methods: Our data was from population-based Survey on Prevalence in
East China for Metabolic Diseases and Risk Factors (SPECT-China) (ChiCTRECS-14005052, www.chictr.org) in 2014. 1642 women ages 55-89 that were
postmenopausal and were not using hormone replacement therapy were
selected. Newly diagnosed diabetes was defined as fasting plasma glucose
159‑LB
SHBG Concentrations during the First Trimester May Predict GDM
Development
TONG ZHANG, WANGEN LI, SHAOJUAN YANG, WEIQIANG LIANG, YING LIU,
YIMEI CHEN, JIANMIN NIU, FANG WANG, ZIHAO LI, Guangzhou, China, Philadelphia, PA
Gestational diabetes mellitus (GDM) is one of most common complications of pregnancy. No well-known early pregnancy biomarker predict GDM
ADA-Funded Research
For author disclosure information, see page LB98.
LB41
POSTERS
Male offspring
8
29.2 (21-39)
465
15
Epidemiology/
Genetics
All
Pairs
18
Maternal age: mean (range)
28.4 (21-39)
# Probes with p< 0.001
277
Genes with > 1 probe with dm
5
(p<0.001)
Probes with dm > or =+/- 10% 7 (-10.5 % +11.9%)
(range)
Probes with dm > or = +/- 15%
0
Probes assigned to 5’ UTR (%)
1 (13)
Probes assigned to 3’UTR (%)
0
Probes assigned to 1st exon (%)
1 (13)
Probes assigned to TSS (%)
2 (25)
Probes assigned to gene
4 (50)
body (%)
DAVID gene function
glycoproteins,
enrichment
plasma membrane,
neuronal development
Epidemiology—Cardiovascular Disease
≥7.0mmol/L and/or HbA1c ≥6.5%. Prediabetes was defined as impaired fasting glucose (fasting plasma glucose 5.6-6.9mmol/L) or HbA1c between 5.7%
and 6.4%, or both. FSH, luteinizing hormone, total testosterone and estradiol
were measured by chemiluminescence in one central laboratory certified by
the College of American Pathologists. Multinomial logistic analyses were
used to measure the association of FSH with prediabetes and diabetes.
Results: Among the participants, 801 (48.8%) had prediabetes and 127
(7.6%) had newly-diagnosed diabetes. Increased quartiles of FSH were associated with significantly decreased odds ratios of prediabetes and diabetes (P
for trend <0.01). This association was attenuated by waist circumference and
HOMA-IR but persisted in fully adjusted model (P for trend <0.01) in which
for the lowest compared with the highest quartile of FSH, the odds ratios of
prediabetes and diabetes were 2.07 (95% CI 1.32-3.24) and 3.56 (95% CI 1.349.46).
Conclusion: Low FSH was associated with higher prevalence of prediabetes and diabetes in postmenopausal women, which was partially explained
by adiposity and insulin resistance. FSH may be a protective biomarker of
glucose metabolism in postmenopausal women.
Blood glucose and HbA1c levels were documented to characterize hyperglycemia. We report a significant increase in end diastolic volume (p<0.02),
end systolic volume (p<0.03), stroke volume (p<0.04), circumferential strain
(p<0.03) and the CURE index (p<0.03) in the diabetic rats when compared
to age matched control rats. We have characterized the functional changes
in the diabetic heart induced by chronic hyperglycemia in-vivo; exemplifying the utility of advanced CINE/tagging protocols to characterize disease
pathology and the need for early therapeutic intervention.
Supported By: National Natural Science Foundation of China (81270885,
81070677); Clinical Potential Subject Construction of Shanghai Jiaotong University School of Medicine (2014); Ministry of Science and Technology in China
(2012CB524906); Science and Technology Commission of Shanghai Municipality
(14495810700); Fund for Outstanding Academic Leaders in Shanghai (12XD1403100)
164‑LB
Risk of Hospitalization for Heart Failure with Dipeptidyl Peptidase-4
Inhibitors vs. Sulfonylureas and with Saxagliptin vs. Sitagliptin in a
U.S. Claims Database
Epidemiology—Cardiovascular Disease
ALEX Z. FU, STEPHEN JOHNSTON, JOHN SHEEHAN, AMEEN GHANNAM, KATHERINE TSAI, KATHERINE CAPPELL, ROBERT FOWLER, IFTEKHAR KALSEKAR,
Washington, DC, Bethesda, MD, Fort Washington, PA, Gaithersburg, MD
POSTERS
Epidemiology/
Genetics
162‑LB
In the SAVOR trial, the risk of hospitalization for heart failure (hHF), a component of the secondary endpoint, was increased with saxagliptin compared
to placebo. This observational cohort study used a U.S. insurance claims
database to compare the risk of hHF between patients with type 2 diabetes
mellitus (T2DM) treated with dipeptidyl peptidase-4 inhibitors (DPP-4i) vs.
sulfonylureas (SU) and between those treated with saxagliptin vs. sitagliptin. Methods followed the FDA’s Mini-Sentinel protocol for active surveillance
of antidiabetic agents. Patients initiated treatment between 8/1/2010 and
8/30/2013 and had no use of the comparator treatments in the prior 12 months
(baseline). Each comparison consisted of patients matched 1:1 on a propensity
score (nearest neighbor; caliper=0.01). Analyses were stratified by presence of
baseline cardiovascular disease (CVD). Time to hHF was compared between
matched groups using Cox models. The Table shows the study results. Among
patients with no baseline CVD, those treated with DPP-4i had significantly
(P=0.013) lower hazards of hHF compared to those treated with SU; other comparisons were statistically insignificant. In this analysis of patients with T2DM
in a real world setting, there was no evidence of increased risk of hHF for DPP4i relative to SU or for saxagliptin relative to sitagliptin.
Aboriginal Australians with Type 2 Diabetes Have a Substantially
Increased Risk of Recurrent Cardiovascular Events: The Fremantle
Diabetes Study
WENDY A. DAVIS, TIMOTHY M.E. DAVIS, Fremantle, Australia
Patients with type 2 diabetes (T2D) and a history of coronary artery disease are at increased risk of further cardiovascular disease (CVD) events. We
compared the risk of recurrent CVD events in community-based Aboriginal vs.
non-Aboriginal T2D patients after hospitalization for acute coronary syndrome
(ACS). Of 1296 patients with T2D in the longitudinal observational Fremantle
Diabetes Study recruited in 1993-1996 (mean age 64 yrs, 49% males), 422 (33%)
had a first (index) ACS hospitalization during mean±SD 14±6 years’ follow-up
from 2 years before entry to census (last contact/death/end 2012). The mean
age at index event was 71 yrs; 3% were Aboriginal. Subsequent CVD episodes
(non-fatal acute myocardial infarction (AMI)/stroke, CVD death) were identified
through validated data linkage. Nearly three-quarters of Aboriginals (73%) vs.
57% of non-Aboriginals suffered a recurrent CVD event (P=0.37). The recurrent
CVD event was an AMI in 44%, stroke in 17%, and CVD death in 39%, with no
difference by Aboriginal status (P=0.79). Aboriginals were younger at the time of
the recurrent event (63±13 vs. 77±9 years, P<0.001). In Cox proportional hazards
modelling with age as the time-scale and after adjusting for sex, Aboriginals
were nearly four times more likely to have a recurrent CVD event (hazard ratio
(95% CI): 3.77 (1.85-7.69)). During further follow-up starting from the recurrent
CVD event until end-2012, 87.5% of Aboriginals vs. 88.1% non-Aboriginals died
(P=1.00), a median [IQR] 0 [0-0.4] vs. 0 [0-1.2] years, respectively, later (P=0.78).
The incidence of recurrent CVD events after ACS hospitalization and the associated early mortality are high in community-based Australians with T2D.
Aboriginals are especially at risk, suggesting an urgent need for targeted and
culturally-sensitive strategies for prevention and management of CVD.
Table. Study Results* for Propensity Score Matched Cohorts**.
DPP-4i vs. SU
Saxa vs. Sita
No Baseline CVD
Baseline CVD
No Baseline CVD
Baseline CVD
DPP-4i SU*** DPP-4i SU*** Saxa Sita*** Saxa Sita***
N of patients****
82,019 82,019 27,259 27,259 43,402 43,402 13,042 13,042
Mean follow-up***** 171
164
187
177
181
187
206
206
N of hHF events
35
58
200
202
23
24
82
87
IR per 100 PY
0.091 0.157 1.434 1.527 0.107 0.108 1.116 1.180
HR (95% CI), P
0.585 (0.384-0.892), 0.946 (0.778-1.151), 0.990 (0.560-1.749), 0.945 (0.699-1.278),
P=0.013
P=0.58
P=0.972
P=0.712
*Sensitivity analyses of hHF risk factor subgroups and using alternative followup assumptions produced consistent results (not shown) **The propensity
score match achieved balance on all patient characteristics included in the
propensity score model (not shown). ***Reference category for HR; HR<1
indicates lower risk for DPP-4i or saxagliptin. ****Patients were matched 1:1
on a propensity score based on demographics, general clinical characteristics,
and hHF risk factors from the 1-year baseline. *****In days; patients were
followed from treatment initiation until hHF or censoring at cessation of
the initiated treatment, use of the alternative comparator treatment, loss to
follow-up, or 8/31/2013. CI=confidence interval; CVD=cardiovascular disease;
DPP-4i=dipeptidyl peptidase 4 inhibitors; hHF=hospitalization for heart
failure; HR=hazard ratio; IR=incidence rate; PY=person-years of follow-up;
Saxa=saxagliptin; Sita=sitagliptin; SU=sulfonylurea.
Supported By: Takeda Pharmaceuticals International, Inc.
163‑LB
In Vivo MR Imaging in Investigating the Effect of Hyperglycemia in
a Rodent Heart
SANKAR SERAMANI, SAKTHIVEL SEKAR, KISHORE KUMAR BHAKOO, Singapore,
Singapore
Hyperglycemia is associated with higher cardiovascular risk. The impact
of cardiac function due to hyperglycemia and/or diabetes are poorly understood in preclinical models due to difficulty in measuring the heart function
non-invasively. Advances in ultra-high field (7 Tesla) MRI allow us to observe
functional changes in a rodent heart with and without hyperglycemia. This
study aims to identify the cardiovascular risk associated with hyperglycemia with structural imaging (cine MRI) and strain assessment (MR tagging
technique). Hyperglycemia was induced in a cohort of male Wistar rats (350450g, n=6) with STZ (60 mg/kg, IV) at week 7. MRI data were collected at
week 40. Data were acquired with Bruker 7Tesla MRI scanner; GRE based
cine imaging and tagged image data was acquired on the rat heart with
the dedicated phased array cardiac coil [TR/TE: 5ms/1.7ms with 25 phases].
Supported By: AstraZeneca
ADA-Funded Research
For author disclosure information, see page LB98.
LB42
Epidemiology—Clinical—Diagnosis and Screening
Epidemiology—Diabetes Complications
Epidemiology—Clinical—Diagnosis
and Screening
spectively examined the associations between the number of nevi and risk of
T2DM among 23,748 men (1986-2010) from the Health Professionals Follow-up
Study (HPFS) and 67,050 women (1989-2010) from the Nurses’ Health Study
(NHS). Information on the numbers of melanocytic nevi on arms and the incidence of T2DM was collected by validated questionnaires. During 1,831,118
person-years of follow-up, we documented 8748 incident cases of T2DM. After adjustment for age, BMI, and other diabetes risk factors, the number of
nevi was significantly associated with increased risk of T2DM. Multivariableadjusted HRs (95% CIs) for <1, 1-5, 6-14, and ≥15 nevi were 1.00 (reference),
1.02 (0.92, 1.14), 1.10 (0.87, 1.38), and 1.70 (1.22, 2.36), respectively, for men (P
trend = 0.03) and 1.00 (reference), 1.15 (1.09, 1.21), 1.25 (1.11, 1.40), and 1.70
(1.38, 2.09), respectively, for women (P trend = 0.019). In the subgroup analyses
in the NHS, the positive relationship between nevi count and T2DM remained
significant in postmenopausal women but not in premenopausal women. Mole
count may represent a novel marker for development of T2DM in men and
postmenopausal women, indicating a possible role of levels or functions of endogenous sex steroid hormones in the pathogenesis of T2DM. Further studies
are warranted to clarify the relationship and underlying mechanisms.
165‑LB
Prevalence of Diabetes and Metabolic Syndrome in Jinuo Chinese
Adults
JIANG FUSONG, HOU XUHONG, WEIPING JIA, Shanghai, China
Background: To investigate the prevalence of diabetes and metabolic syndrome in Jinuo Chinese adults, the last established ethnic minority population in Yunnan, China.
Methods: Between January and May 2012, we conducted a cross-sectional
survey. A representative sample of 5,633 adults, aged ≥18 years, from the
Jinuo minority of Yunnan province participated in this study. After an overnight
fast, blood samples were drawn to measure fasting plasma glucose levels and
2 hours after an oral glucose-tolerance test in participants without history of
diabetes. Physical examination and laboratory tests were also performed.
Results: The age-standardized prevalence of diabetes was 7.2% in the
population (men: 10.2%; women: 4.4%). Among 297 patients with newly
diagnosed diabetes, 38.4% had raised fasting plasma glucose levels (≥7.0
mmol/L) only, 39.7% had raised 2-hour plasma glucose levels (≥11.1 mmol/L)
only, and both parameters were raised in 21.9%. The age-standardized
prevalence of prediabetes was 19.0% (men: 21.2%; women: 17.0%). Among
1070 patients with prediabetes, 42.5%, 44.0%, and 13.5% had isolated impaired fasting glucose, isolated impaired glucose tolerance and combined
impaired fasting glucose and impaired glucose tolerance, respectively. The
age-standardized prevalences of central obesity, general obesity, hypertension, dyslipidemia, and metabolic syndrome were 8.9%, 20.4%, 20.9%,
20.4%, and 33.5%, respectively.
Conclusion: Jinuo male adults have a higher prevalence of diabetes and
pre-diabetes and are prone to elevated fasting glucose levels.
Epidemiology—Diabetes Complications
168‑LB
Point-of-Care Hba1c Testing in a Clinical Setting: Performance
Analysis
Supported By: Asahi Kasei Corporation
166‑LB
Impact of Diabetes Screening in Asian Americans Based on the Re‑
vised ADA Standards of Medical Care in Diabetes 2015
DANIEL S. HSIA, SANDRA LARRIVEE, WILLIAM T. CEFALU, WILLIAM D. JOHNSON, Baton Rouge, LA
The BMI cut point for screening overweight or obese Asian Americans for
prediabetes and type 2 diabetes was changed recently from 25 kg/m2 to 23 kg/
m2 to reflect the evidence that this population is at increased risk for diabetes
at lower BMI levels relative to the general population. The purpose of this cross
sectional study was to examine screening rates using the new lower BMI cutoff
compared to the previous BMI cutoff of 25 kg/m2 in Asians participating in the
National Health and Nutrition Examination Survey (NHANES) from 2011-2012
when there was an oversampling of Non-Hispanic Asians. We hypothesized
that including Non-Hispanic Asians ≥ 45 years old at a BMI cutoff of 23 kg/m2
would significantly increase the prevalence of prediabetes and diabetes in this
population compared to a BMI of 25 kg/m2. NHANES 2011-2012 consisted of
9756 participants of which 13.1% (1282) were identified as Non-Hispanic Asian.
From this demographic group, 341 participants were identified as ≥ 45 years
old with available BMI, HbA1c, and fasting glucose data. In this subset, 45%
(155) had a BMI ≥ 25 kg/m2 compared to 69% (236) with a BMI ≥ 23 kg/m2.
Using the lower BMI cutoff, the prevalence of prediabetes and diabetes was
48.4% compared to 32.8% when using the previous BMI cutoff of ≥ 25 kg/m2.
Moreover, lowering the screening BMI increased the sensitivity of screening for
prediabetes and diabetes from 49.3% to 72.7% (p<0.0001) but decreased the
specificity from 62.3% to 37.7% (p=0.0003). Overall, the combined prevalence
of prediabetes and diabetes was 66.6% (227 of 341) in this cohort. Although this
will add additional healthcare costs due to more widespread screening, early
identification of these conditions may be beneficial for primary and secondary
prevention in this unique population. More research is indicated to determine
if this lower cutoff should apply to younger populations and to more specific
ethnic groups within the Non-Hispanic Asian demographic.
169‑LB
Bladder Cancer Risk in Relation to Exposure to Pioglitazone among
Patients with T2DM in the Pan European Multi-Database Bladder
Cancer Risk Characterisation Study
PASI KORHONEN, EDITH M. HEINTJES, RACHAEL WILLIAMS, FABIAN HOTI, SOLOMON CHRISTOPHER, MAILA MAJAK, LEANNE HOUWELING, HELEN STRONGMAN, MARIE LINDER, PAUL DOLIN, SHAHRAM BAHMANYAR, Espoo, Finland,
Utrecht, Netherlands, London, United Kingdom, Stockholm, Sweden
Supported By: National Institute of General Medical Sciences (1U54GM104940)
This observational cohort study was conducted in Finland, Netherlands,
Sweden and United Kingdom at the request of the European Medicines
Agency. The objective was to evaluate bladder cancer risk in T2DM patients
in relation to exposure to pioglitazone. A common study protocol and pooled
analysis plan was used across countries. Linked prescription, hospital, general practitioner, cancer and death registration records were used to build the
study database from the country specific datasets. To limit channelling bias,
pioglitazone exposed (n=56,337) and non-exposed were matched based on
treatment history and propensity scores accounting for variables affecting pioglitazone initiation. The hazard ratios (HR) with 95% confidence intervals (CIs)
were estimated using Cox’s model with adjustments for relevant confounders.
Follow-up was from cohort entry until first incident bladder cancer, secondary
167‑LB
Associations between Benign Cutaneous Nevi and Risk of Type 2
Diabetes Mellitus in Men and Women: Results from Two Prospec‑
tive Cohort Studies
HONGJI DAI, QI SUN, XI ZHANG, JOANN E. MANSON, FRANK B. HU, YIQING
SONG, Indianapolis, IN, Boston, MA
Previous studies suggest that the number of cutaneous nevi and type 2
diabetes mellitus (T2DM) are both associated with endogenous sex hormone
levels. However, no prospective studies have specifically examined the relationship between the number of benign cutaneous nevi and T2DM. We proADA-Funded Research
For author disclosure information, see page LB98.
LB43
POSTERS
HbA1c test reflects glycemic control over past three months, predicts diabetic complications and can be used for diabetes diagnosis and screening;
changes of 0.5-1.0% are clinically significant. Although POCT HbA1c assays may
be NGSP-certified the ADA doesn’t recommend them for diagnostic purposes.
PTS Diagnostics (Indianapolis, USA) has recently introduced POCT HbA1c monitoring system (A1cNow), NGSP and IFCC-certified, CLIA-waived, that provides
results in 5 minutes and requires a 5µl blood sample. We investigated A1cNow
performance in out clinic diabetic patients. HbA1c levels of 101 diabetic subjects were measured with A1cNow devices, using capillary blood samples, and
laboratory Tosoh G8 HPLC Analyzer (CV% from external quality assessment
of low and high HbA1c levels: 2.1 and 2.6%, respectively) using EDTA venous
blood samples. A1cNow precision was evaluated by the CV of ten replicates
in two consecutive days using low (5.4%) and high (10.0%) NOD HbA1c control
solutions (Nova-One Diagnostics, Woodland Hills, USA). Diabetic patients Tosoh results were 7.6±1.2% (range 5.3-11.0) vs. A1cNow 7.4±1.2 (5.1-10.5). The
A1cNow results correlated with laboratory results (r= 0.95, p<0.001), but mean
difference between A1cNow results minus Tosoh results was -0.24±0.39 (from
-1.6 to 1.1, p<0.001); the 95% confidence intervals (CIs) of mean difference were
-0.16 and -0.32. The relative error (bias/reference x 100) was 3.1±5.1% and
showed a non-normal distribution: skewness 0.57 and kurtosis 3.84 (p<0.0001).
The within- and between-run CVs were well <4% for both levels of control solutions. Thus, although the majority of A1cNow measurements were accurate in
comparison with results of the reference method, a small percentage (5%) of
mismatched results could lead to inappropriate medical decision. Research is in
progress to determine system factors contributing to error. A high quality POCT
could have a big impact on diabetes screening promotion as well as on diabetes
care at home, in the hospital or office setting.
Epidemiology/
Genetics
ELENA MATTEUCCI, CRISTINA CONSANI, LUCA ROSSI, LUCA DELLA BARTOLA,
OTTAVIO GIAMPIETRO, Pisa, Italy
Epidemiology—Nutrition
malignant neoplasm of bladder, death, start of other TZDs, leaving the database, end of database coverage or 30 June 2011 whichever occurred first. A
total of 283 bladder cancer cases occurred: 130 in the exposed group and 153
in the non-exposed group during a mean follow-up time of 2.9 years and 2.8
years, respectively. The pooled adjusted HR (exposed vs. non-exposed) was
0.99 (95% CI: 0.75-1.30). The dataset specific HRs varied from 0.56 (95% CI:
0.31-1.00) for Finland to 4.27 (95% CI: 1.26-14.46) for Sweden. We did not observe a trend with regard to cumulative exposure to pioglitazone. The adjusted
HRs varied from 1.10 (95% CI: 0.82-1.48) to 0.86 (95% CI: 0.44-1.66) for <18
months and >48 months of exposure and from 1.05 (95% CI: 0.77-1.42) to 0.65
(95% CI: 0.33-1.26) for 1-14,000 mg and >40,000 mg of exposure, respectively
when compared with the never exposed group. In conclusion, exposure to pioglitazone did not increase bladder cancer risk. Further analyses are needed to
explore the observed heterogeneity between datasets.
p-yrs, RR=3.29 (2.27-4.77). The risk of falls in youth with T1D diabetes was
less pronounced - RR 1.62 (1.05-2.48).
Conclusions: Youth with T1D is more likely to suffer injury, particularly in
older teenage years. Increased incidence of MVA-related injuries in youth
with T1D requires further evaluation.
Epidemiology—Nutrition
172‑LB
Pinitol-enriched Beverage Improves Mitochondrial and Endothelial
Function in Type 2 Diabetic Patients
ANTONIO HERNÁNDEZ, CELIA BAÑULS, SUSANA ROVIRA-LLOPIS, OLALLA
Rubio-Puchol, Victor M. Victor, Milagros Rocha, Valencia, Spain
Background: A limited amount of research suggests that inositol derivates
have a positive influence on glucose tolerance in type 2 diabetic patients,
but little is known about their effects on endothelial function.
Objective: To assess the anti-diabetic properties of an inositol-enriched
beverage (IEB) on glycaemic control and its influence on the endothelial function and/or redox status in type 2 diabetic subjects.
Design: This was a 12-week, double-blind randomized trial employing
nineteen diabetic subjects that receiving an IEB, containing mainly of pinitol,
4.0 g/day. Anthropometric and biochemical measurements, postprandial and
fasting nocturnal glycemia, endothelial and inflammatory parameters, and
oxidative stress markers were analyzed at baseline and after intervention.
Results: Subjects consuming IEB exhibited a significant decrease in triglyceride (8.82%) and HbA1c (4.53%) levels. Continuous glucose monitoring
system revealed a significant reduction of -9.15% and -4.24% in glucose during postprandial breakfast and dinner, respectively and of 4.52% overnight
fasting periods. It also improved endothelial function by reducing P-selectin
levels (p<0.05) and leukocyte-endothelium interactions, as there was an increase in rolling velocity and a reduction in polymorphonuclear leukocyte
adhesion (p<0.05 for both). This response was mediated by a significant
diminution in the generation of ROS determined by DFCH-DA (p<0.01).
Conclusions: The present results show that IEB supplementation induces
a significant improvement in glycemic control in diabetic subjects by improving endothelial function and intracellular redox status, which could, in turn,
reduce cardiovascular events.
170‑LB
Effects of Depression on Mortality Risk in Subjects With or With‑
out Diabetes: The National Health Insurance Service—National
Sample Cohort (2002-2010) in Korea
POSTERS
Epidemiology/
Genetics
JI A. SEO, TAE JOON KIM, JI HYE SEO, JI HEE YU, HYE JIN YOO, SIN GON KIM,
KYUNG MOOK CHOI, SEI HYUN BAIK, DONG SEOP CHOI, YOUSUNG PARK, NAN
HEE KIM, Ansan, Republic of Korea, Seoul, Republic of Korea
The aim of this study was to evaluate the effect of depression on allcause, cardiovascular and suicidal mortality among Koreans with or without
diabetes. We evaluated the mortality risk in Korean adults using the large
prospective cohort data provided by the National Health Insurance Service,
which consisted of more than one million subjects. A total of 749,051 adults
over 20 years of age at baseline of 2003 and 2004 were classified into 4
groups by the presence/absence of diabetes and depression and were followed-up until 2010. The prevalence of depression in 2003~2004 in subjects
with or without diabetes was 5.83% and 1.58%. Over 7 years, 39,603 deaths
were documented, including 6,999 deaths from cardiovascular disease and
1,906 from suicide. Compared with the reference group (no diabetes and no
depression), mortality risk was highest in those with both diabetes and depression [HR 2.09 (95% CI 1.94-2.26)]. Subjects with only depression or diabetes had modestly increased risk for death [depression only, 1.38 (95% CI
1.30-1.47); diabetes only 1.43 (1.39-1.47)]. Cardiovascular mortality showed
a similar pattern in these four groups [depression only, 1.32 (1.14 -1.53);
diabetes only, 1.47 (1.38 -1.57); both diabetes and depression, 2.28 (1.932.70)] compared to the reference group]. However, suicidal mortality was
increased in subjects with depression regardless of the presence/absence
of diabetes [depression only, 3.90 (3.18-4.77); both diabetes and depression
3.65 (2.57-5.20)]. Depression is more prevalent in those with diabetes than
without. The coexistence of diabetes and depression increased the risk for
all-cause and cardiovascular mortality.
Supported By: Fund for Health Research (PI12/01984, PI13/1025, PI13/0073)
173‑LB
Food Craving, Self-Control of Eating, and Appetite Score Were Pre‑
dictors for Weight Loss in the POUNDS Lost Trial
JENNY TONG, DENNIS HANSEMAN, CATHERINE M. CHAMPAGNE, GEORGE A.
BRAY, LU QI, DONALD A. WILLIAMSON, STEPHEN D. ANTON, FRANK M. SACKS,
Durham, NC, Cincinnati, OH, Baton Rouge, LA, Boston, MA, Gainesville, FL
171‑LB
Eating habits and food craving are strong correlates of obesity but how
psychological and behavioral factors may influence successful weight loss is
not well understood. We aimed to identify predictors for successful weight
loss over a six months time period in the Preventing Overweight Using Novel
Dietary Strategies (POUNDS Lost) trial. A total of 811 overweight and obese
participants (age 51 ± 9 y [mean ± SD], 64% female, BMI 33 ± 4 kg/m2) were
randomly assigned to one of the four diets with targeted percent energy
from fat, protein and carbohydrates as 20-15-65, 20-25-55, 40-15-45, and
40-25-35 for 2 years. Multivariable linear regression analyses as well as
partial correlation analyses were performed. Mean weight loss achieved
across all dietary conditions at 6 months was 5.8 ± 5.7 kg. There was no difference in weight loss according to dietary assignment. Greater craving for
carbohydrates and higher dietary restraint scores at baseline predicted less
weight loss, while greater craving for high fat foods and high appetite score
at baseline predicted greater weight loss at 6 months. Both greater carbohydrate and fat craving were correlated with higher intake of carbohydrates,
protein and fat as well as total calories estimated at 0 and 6 months, but only
craving of high fat foods at baseline was associated with decreased fat and
total calorie intake over the first 6 months. Higher dietary restraint at baseline was associated with less food intake at baseline independent of BMI
but was associated with increased calorie intake from 0 to 6 months. Appetite score was negatively correlated with dietary restraint. Interestingly,
higher appetite score was associated with decreased calorie intake over the
first 6 months. We conclude that while varying macronutrients in the diet did
not lead to difference in weight loss, craving for specific macronutrients and
levels of dietary restraint both predict short-term weight loss.
Higher Incidence of Injuries in Children and Adolescents with
Type 1 Diabetes
ARLETA REWERS, MOLLY NOWLAN, DANA DABELEA, GREGORY TUNG, JUSTIN
CURIE, DAWN COMSTOCK, Aurora, CO
Background: Hypoglycemia or hyperglycemia may increase the risk of injury in patients with type 1 diabetes (T1D); however little is known concerning the incidence of injuries in diabetic youth. The goal of this study was to
determine whether the risk of injury in youth with T1D differs from that in
the general population.
Material and Methods: The study population included all Colorado residents aged <20 years followed for 14 332 638 person-years, during 20002010. Annual intercensal population estimates were obtained from the state.
Cases of injury resulting in death, hospitalization or ER visit (N=34 761) were
ascertained using the population-based Colorado Trauma Registry. Injury was
classified using the ICD-9 codes. Children and adolescents with T1D among
injury cases (N=84) were identified based on a comorbidity variable. The
population of youth with T1D who were at risk for injury in 2000-2010 was
estimated based on SEARCH Colorado diabetes prevalence data.
Results: The incidence of injury in youth with T1D was significantly higher - 5.4/1000 p-yrs than that in the underlying population - 2.4 /1000 p-yrs,
RR=2.25 (95% C 1.81-2.78). Most injuries (67%) occurred in males, regardless
of diabetes status. Age-group 15-19 yrs accounted for 67% of injuries in
patients with T1D and 42% in the general population. T1D patients in this
age group experienced the greatest increase in injuries, compared to the
general population. Motor vehicle accidents (MVA) were the primary cause
of injuries in T1D patients and responsible for half of the injuries among 1519 yr olds. The incidence of MVA injuries in T1D patients - 1.8/1000 p-yrs
was significantly increased, compared to the general population - 0.6/1000
Supported By: National Institutes of Health-National Institute of Diabetes and
Digestive and Kidney Diseases
ADA-Funded Research
For author disclosure information, see page LB98.
LB44
Epidemiology—Nutrition
174‑LB
176‑LB
Genetic Predisposition to Central Obesity, Dietary Fat, and Changes
in Appetite: Preventing Overweight Using Novel Dietary Strategies
Trial (POUNDS Lost)
Randomized Trial of Multivitamin Use and Risk of Type 2 Diabetes
Mellitus in Men
Central obesity is a major risk factor for diabetes and is determined by both
genetic and environmental factors. Energy homeostasis plays a central role
in influencing body fat distribution and risk of central obesity. However, little
is known about whether genetic variants related to central obesity affect energy intake. In the 2-y Preventing Overweight Using Novel Dietary Strategies
Trial, we examined the relation between a genetics risk score (GRS) for central
obesity and changes in appetite related behaviors, and particularly assessed
interactions between the GRS and diet interventions. The GRS was created
based on 13 central obesity-associated SNPs in 742 participants. The appetiterelated traits included food craving, fullness, hunger and prospective consumption. We found a significant interaction between the central obesity GRS and
dietary fat intake in relation to 2-y changes in appetite (P-interaction=0.0009).
Individuals with high GRS had increased appetite, while those with low GRS
had decreased appetite (P=0.005) in the low-fat diet group. In subjects with
high-fat diet, there was no significant genetic effect on appetite (P=0.381). In
addition, we found that the central obesity GRS score significantly modified
the effect of dietary fat intake on 2-y changes in prospective consumption
(P-interaction=0.0005). Participants with high GRS had a greater reduction in
prospective consumption when their fat intake was high (P=0.015); but tended
to have less reduction in prospective consumption when their fat intake was
low (P=0.111). Our data suggest that participants with a high genetic risk for
central obesity might obtain more benefits in appetite and prospective consumption by choosing a hypocaloric higher-fat weight-loss-diet. This trial was
registered at clinicaltrials.gov as NCT00072995.
Supported By: Indiana University School of Medicine (to Y.S.)
175‑LB
Effects of Substituting Brown Rice for White Rice on Diabetes Risk
Factors in India: A Randomized Controlled Trial
177‑LB
Dietary Lipophilic Index and Lipophilic Load and Risk of Type 2 Dia‑
betes in the Women’s Health Study: Importance of Both Fat Quality
and Quantity
VASANTI S. MALIK, SUDHA VASUDEVAN, NICOLE M. WEDICK, RAMYA BAI,
VIJAYALAKSMI PARTHASARATHY, LAKSHMIPRIYA NAGARAJAN, KOKILA ARUMUGAM, BILING HONG, RUIFENG LI, KAMALA KRISHNASWAMY, RANJIT M.
ANJANA, DONNA SPIEGELMAN, WALTER C. WILLETT, FRANK B. HU, VISWANATHAN MOHAN, Boston, MA, Chennai, India
ERIC L. DING, KATERINA M. DE VITO, QI SUN, HONGYU WU, HANNIA CAMPOS,
EILIS J. O’REILLY, VASANTI S. MALIK, JULIE E. BURING, JOANN E. MANSON,
Cambridge, MA, Boston, MA
Background: Fatty acid fluidity may influence insulin resistance and inflammation. Traditional broad fat classification may not sufficiently describe
differing risks of fatty acids. Therefore, we investigated the association
between two novel lipid indexes of fatty acid fluidity, the Dietary Lipophilic
Index (DLI) and the Dietary Lipophilic Load (DLL), and risk of incident T2D: the
DLI reflects average fatty acid fluidity independent of quantity, while the
DLL reflects both fat intake quantity and fluidity. We also tested an a priori
hypothesis of interaction with C-reactive protein (CRP).
Methods: Study included 19,388 women in the Women’s Health Study,
who were free of major chronic diseases and metabolic conditions (diabetes,
dyslipidemia, and hypertension) at baseline. DLL was calculated by summing
across the products of each fatty acid (g/day) and its Celcius melting point.
DLI was calculated by dividing DLL by total fatty acid intake (g/day). We
calculated hazard ratios (HR) for T2D using Cox regression adjusted for established risk factors and explored interaction with CRP.
Results: There were 442 cases of incident T2D in 238,690 person-years
of follow-up. In multivariate models, DLL, but not DLI, was positively associated with an increased risk of T2D. The HR for T2D comparing extreme
quintiles of DLL was 2.55 (95% CI: 1.13-5.74), while HR for T2D comparing
extreme quintiles of DLI was 1.13 (0.50-2.55). The DLL positive association
persisted after further adjustment for polyunsaturated:saturated fat ratio
(HR=2.55, 1.13-5.74). Analyses by CRP levels (>1 vs. <=1 mg/L) suggested potential CRP effect modification of both DLI and DLL (P interaction=0.042 and
0.047, respectively), where DLL and T2D risk was stronger among high CRP.
Conclusions: The Dietary Lipophilic Load, but not Dietary Lipophilic Index,
is associated with higher risk of T2D, indicating the synergistic importance
of both fatty acid fluidity and quantity.
India has the second largest number of people with type 2 diabetes (T2D)
in the world following China. Epidemiological evidence indicates that consumption of white rice is associated with increased risk for T2D, while intake
of brown rice decreases T2D risk. However, data from trials are sparse. We
determined the effect of substituting brown rice for white rice on T2D risk
factors among adults in urban South India. Following a 1-week run-in phase,
166 overweight (BMI ≥23kg/m2) volunteers aged 25-65 years who consume
≥200 g of rice/day were enrolled in a randomized cross-over trial conducted
at the study center. The intervention consisted of a brown rice and white
rice regimen each providing 2 ad libitum meals/day, 6 days/week for 3
months with a 2-week wash-out period. Fasting measurements of glucose
metabolism, dyslipidemia and inflammation were assessed at baseline and
end of follow-up. During the intervention, no significant between-group differences were observed for markers of glycemic control or lipids. There was
less increase in high-sensitivity C-reactive protein in the brown rice (0.03
(2.12) mg/L) compared to white rice group (0.63 (2.35) mg/L) (p=0.04). Among
participants who thought brown rice was healthy, the brown rice group
gained more weight than the white rice group, while among participants
who did not think brown rice was healthy there was no difference in weight
between groups (p-for-heterogeneity=0.002). Changes in HbA1c were more
favorable in the brown rice group among those who did not think brown rice
was healthy while there was no difference among those who thought brown
rice was healthy (p-for-heterogeneity=0.01). In this 3-month trial, substituting brown rice for white rice did not appreciably improve glycemic or lipid
parameters but had a favorable effect on inflammation. Changes in body
weight and glycemia differed by perception about brown rice. Larger studies of longer duration are needed to examine the role of brown rice in T2D
prevention in India.
Supported By: American Diabetes Association (1-12-JF-13 to E.L.D.); American
Heart Association
Supported By: Fogarty International Center; National Institutes of Health
(R03TW008726)
ADA-Funded Research
For author disclosure information, see page LB98.
LB45
POSTERS
Objective: Multivitamin supplements are the most commonly used dietary
supplements in the U.S. and have been suggested as a means to prevent
type 2 diabetes. However, observational studies have shown an inconsistent association and multivitamin supplement use and type 2 diabetes. In
addition, there are no long-term randomized trials of multivitamin use that
examined its effect on diabetes risk.
Research Design and Methods: In a secondary analysis of the Physicians’
Health Study II (PHS II), a randomized, double-blind, placebo-controlled trial
of a multivitamin among 14,641 U.S. male physicians aged >=50 years, we
examined whether randomized multivitamin supplementation decreases the
risk of type 2 diabetes.
Results: Among 13,621 men free of diabetes at baseline, 1,074 incident
cases of type 2 diabetes were identified during a median follow-up of 11
years. Overall, there was no significant difference in diabetes risk between
those randomized to take a daily multivitamin and those taking a placebo
(log-rank P=0.38). There were 551 incident diabetes cases in the multivitamin supplement group and 523 in the placebo group (hazard ratio [HR], 0.98;
95% CI, 0.78-1.22; P = .83). Similarly, there was no effect of multivitamin
use on diabetes risk according to follow-up time (>0 to <5 and >=5 years of
follow-up). Stratification by known diabetes risk factors, history of coronary
heart disease, and other randomized treatments showed no significant interactions.
Conclusions: In this large, long-term randomized trial of a daily multivitamin among male physicians, a common multivitamin had no effect on the risk
of developing type 2 diabetes among initially healthy men.
Epidemiology/
Genetics
YIQING SONG, LU WANG, JOANN E. MANSON, ROBERT J. GLYNN, JULIE E. BURING, J. MICHAEL GAZIANO, HOWARD D. SESSO, Indianapolis, IN, Boston, MA
CHRISTINA-ALEXANDRA SCHULZ, TAO HUANG, YAN ZHENG, TIANGE WANG,
FRANK M. SACKS, GEROGE A. BRAY, QI LU, Malmö, Sweden, Boston, MA, Baton
Rouge, LA
Epidemiology—Other
Epidemiology—Other
180‑LB
Reduction in Diabetes Incidence Differs by Prediabetes Type in a
Randomized Translational Trial of Prevention
178‑LB
MARY BETH WEBER, HARISH RANJANI, LISA R. STAIMEZ, RANJIT M. ANJANA,
MOHAMMED K. ALI, K.M. VENKAT NARAYAN, VISWANATHAN MOHAN, Atlanta,
GA, Chennai, India
An Interleukin-6 Polymorphism May Modify Air Pollutants and Dia‑
betes Association
POSTERS
Epidemiology/
Genetics
IKENNA C. EZE, MEDEA IMBODEN, ASHISH KUMAR, ARNOLD VON ECKARD­
STEIN, DAIANA STOLZ, MARGARET GERBASE, NINO KÜNZLI, THIERRY ROCHAT,
CHRISTIAN SCHINDLER, FLORIAN KRONENBERG, NICOLE PROBST-HENSCH, Basel, Switzerland, Zurich, Switzerland, Geneva, Switzerland, Innsbruck, Austria
Based on the success of trials in people with impaired glucose tolerance
(IGT), the ADA and others issued prevention guidelines; however, real-life effectiveness of these guidelines for all prediabetes (isolated impaired fasting
glucose, iIFG, iIGT, and IFG+IGT) remains unknown. The Diabetes Community
Lifestyle Improvement Program (D-CLIP) in Chennai, India randomized adults
with iIFG, iIGT, or IFG+IGT to control (N=293) or a low-resource lifestyle modification program (N=283) based on the Diabetes Prevention Program (DPP)
plus metformin for individuals remaining at highest risk (IFG+IGT or IFG + elevated HbA1c at four months or later). Participants were 63.2% men; mean age
of 44.4 ± 9.3 years; mean BMI of 27.9 ± 3.7 kg/m2; and 30.2% had iIFG, 29.7%
had iIGT, and 40.1% had IFG+IGT. Mean follow-up was 2.54 ± 0.91 years, loss
to follow-up 9.5%, and 71.5% in the lifestyle arm needed metformin. In intention to treat analyses, the overall reduction in diabetes incidence was 32%
(Table), but intervention was less effective among iIFG compared to iIGT or
IFG+IGT. Incidence reduction was greatest among obese (-49%), male (-37%;
-24% in women) and older participants (-47% ages >50; -34% ages ≤35; -21%
ages 36-50). A DPP-like intervention plus metformin when needed reduces
diabetes incidence by a third among all people with prediabetes; however
additional prevention tools may be needed in iIFG or BMI <27.5 kg/m2.
Air pollution (AP) has been linked to type 2 diabetes (T2D) and hypothesized to act through inflammatory pathways. AP has been linked to induction of interleukin-6 gene (IL6) in the airway epithelium, and IL6 may impact
on glucose homeostasis. A recent meta-analysis showed the common polymorphism, IL6 -572G>C (rs1800795) to be associated with T2D. IL6 -572G>C
has also been shown to influence circulatory IL-6 levels. We hypothesize that
polymorphisms on IL6 may modify the association between AP and T2D. We
cross-sectionally studied 4410 follow-up participants of the Swiss Cohort
Study on Air Pollution and Lung and Heart Diseases (SAPALDIA), aged 29 to
73 years, with complete data on IL6 -572G>C genotype and covariates. We
defined diabetes as self-reported, physician-diagnosed, or diabetes medication use or non-fasting glucose >11.1mmol/L or HbA1c>0.065. Genotyping was done using 5'-nuclease Taqman assay. AP exposures were 10-year
means of particulate matter <10um in diameter (PM10) and Nitrogen dioxide
(NO2). We derived interaction terms between AP and genotype and applied
mixed logistic models to explore effect modification by IL6 -572G>C. There
were 252 diabetes cases. Minor allele frequency was 7%. IL6 -572G>C
was not associated with diabetes in our study. We observed a positive
association between AP and diabetes among homozygous carriers of the
proinflammatory major G-allele [ORPM10: 1.53 (1.22, 1.92; Pinteraction (additive):
0.031); ORNO2: 1.32 (1.15, 1.53); P: 0.042]. There was indication that the
C-allele mitigated the effect of PM10 and NO2. Sensitivity analyses showed
this effect modification to be consistent across various diabetes phenotypes when limiting case definition to each diagnostic criterion. We found
a modifying effect of IL6 -572G>C on the association between AP and diabetes in the SAPALDIA cohort. Our results are consistent with hypothesis
that AP impacts on T2D through inflammatory pathways. Further studies
are needed to determine the public health impact of these findings.
Table. Diabetes Incidence in the D-CLIP Study.
Diabetes Incidence Diabetes Incidence
Rate Control
Rate Intervention
(cases/100
(cases/100
N
person-years)
person-years)
Overall
550
14.2
9.8
BMI (kg/m2)
23-<27.5 246
10.5
8.7
≥27.5 273
19.1
10.5
Glycemic Status iIFG
166
7.2
6.5
iIGT
162
10.7
7.4
IFG+IGT 222
22.2
14.5
Relative
Reduction in
Incidence %
(95% CI)
32 (7, 50)
14 (-43, 48)
49 (23, 66)
12 (-80, 57)
31 (-31, 64)
36 (3, 57)
Number
Needed
to Treat
9.8
46.3
6.8
15.5
11.0
12.3
Supported By: International Diabetes Federation
179‑LB
Modification of Air Pollution and Diabetes Association by Genetic
Risk Score of Type 2 Diabetes Variants
181‑LB
IKENNA C. EZE, MEDEA IMBODEN, ASHISH KUMAR, ARNOLD VON ECKARDSTEIN, DAIANA STOLZ, MARGARET W. GERBASE, NINO KÜNZLI, THIERRY
ROCHAT, FLORIAN KRONENBERG, CHRISTIAN SCHINDLER, NICOLE PROBSTHENSCH, Basel, Switzerland, Zurich, Switzerland, Geneva, Switzerland, Innsbruck,
Austria
Withdrawn
Exposure to ambient air pollution has been associated with risk of type 2
diabetes (T2D). Genetic factors may influence susceptibility to environmental stressors in the aetiology of T2D. The effect of T2D genetic risk variants on susceptibility to air pollution has not been studied. Compared to
single variants, joint genetic variants contribute substantially to disease
risk. Therefore, we did cross-sectional analyses of the modifying effect of
genetic risk scores (GRS) of 46 European T2D risk variants on the association between air pollution and diabetes in 2825 participants of the Swiss
Cohort Study on Air Pollution and Lung and Heart Diseases in Adults, aged
29-73 years, with complete genetic data. T2D risk variants were identified
from genome-wide meta-analyses. Air pollution exposures were the 10-year
means of particulate matter <10µm in diameter (PM10) and Nitrogen dioxide
(NO2). Genotyping of 46 European T2D risk variants was done using Illumina
Human Omni Express Exome chip. We computed two risk scores, count-GRS
and weighted-GRS, and applied pollutant-specific interaction term with each
risk score in mixed logistic models, including subgroup analyses. Diabetes
prevalence was 5.9%. There was an increase in the association between
PM10 and diabetes across tertiles (t) of count-GRS [OR t1:1.32 (0.86, 2.01);
ORt2:1.66 (1.06, 2.61); ORt3:1.99 (1.06, 3.73); Pinteraction =0.275). We observed
a positive interaction between PM10 and count-GRS (βint=0.27; P=0.003)
among participants with chronic obstructive pulmonary disease (COPD). Although there was no evidence for effect modification of the GRS in the entire
sample, two T2D risk variants (rs1531343 near gene HMG2A and rs8043680
near PRC1) showed significant interactions with PM10 (P<0.05). We observed
similar results with weighted-GRS as well as with NO2. In conclusion, our
results suggest that genetic risk for diabetes may modify susceptibility to air
pollution. The results need follow-up in diabetes cohort consortia.
ADA-Funded Research
For author disclosure information, see page LB98.
LB46
Epidemiology—Other
182‑LB
diabetic subjects (DS) in comparison with a group of non diabetic subjects
(NDS). During the first outbreak of CKF in Haiti in 2014, the first 46 consecutive adult patients with preexisting diabetes and the first 53 consecutive
non diabetic adult patients, diagnosed with CKF in a FHADIMAC (Fondation
Haïtienne de Diabète et de Maladies Cardio-vasculaires) affiliated clinic in
Port-au-Prince, were enrolled. Clinical history, capillary fasting glycemia and
HbA1c (DCA Vantage) were used to rule out diabetes in controls. All patients
with signs/symptoms suggestive of CKF underwent whole blood immunochromatographic tests for CKF (IgM Antibodies), dengue fever (IgG and IgM
Antibodies) and plasmodium falciparum malaria (Antigen). Mean age was
53.2 and 47.4 years, 56.5% and 56.6% were women, 23.9% and 20.7% were
obese among DS and NDS respectively (NS). Mean duration of diabetes was
7.1 years; 4.3% of DS (2/46) were treated with lifestyle modifications (LM)
only, 82.6% (38/46) were on oral antidiabetic agents (OAA) and 13.0% (6/46)
on insulin. No patient with CKF had concomitant malaria or dengue fever.
Arthralgia (100 and 98.1%), fever (86.9 and 90.5%), and myalgia (80.4 and
50.9%, p<0.01) were the most frequent clinical findings in DS and NDS, respectively. Improvement of arthralgia was reported after 8 days versus 3.5
days among DS and NDS respectively (p<0.01). In DS mean fasting glycemia, based on glucose self-monitoring over 1 week, was 29.2% higher post
compared to pre CKF symptoms onset (p<0.01). This increase of glycemic
values was 1.6 times more in 32.6% of DS (15/46). Anti-diabetic medication
was titrated up in 41.3% of DS (19/46): 74.7% more for OAA, 35.5% more
for insulin, addition of OAA for both DS on LM. Our study shows a significant negative impact of CFK on glycemic control among diabetic patients.
It also suggests greater morbidity related to CKF among diabetic patients
compared with non diabetic subjects.
Life-Course Evolution of Prediabetes in Young Rural Indians
CHITTARANJAN YAJNIK, CHARUDATTA JOGLEKAR, DATTATREYA BHAT, HIMANGI LUBREE, PALLAVI YAJNIK, CAROLINE FALL, Pune, India, Southampton,
United Kingdom
The Pune Maternal Nutrition Study was set up in 1993 to study the effect
of maternal nutrition on fetal growth and programming of diabetes and cardiovascular disease. We studied mothers from before and during pregnancy,
and children from birth onwards with serial anthropometric and metabolicendocrine measurements. Fathers were also studied. At 18 years of age,
we followed 663 (94%) of possible 709 children for their glucose tolerance,
body size and composition, and other risk factors for diabetes and CVD. Average BMI was 19.1 kg/m2, and there was one girl with diabetes (possibly
monogenic). Twenty five percent had prediabetes (37% in boys and 18% in
girls) by ADA criteria (23% IFG, 10% IGT, and 5% both). At 18 years, prediabetic children had higher waist circumference (72.5 cm vs. 69.0), higher
subscutaneous abdominal fat area ( 96.9 cm2 vs. 92.9) but similar visceral
fat area when compared to NGT. They also had higher HOMA-IR (1.8 vs. 0.4),
lower insulinogenic index (1.4 vs. 1.7) and lower disposition index (63 vs. 82).
Prediabetic children had higher fasting glucose and lower disposition index
at 12 and 6 years of age, had similar anthropometry but lower gestation
(271 days vs. 273) at birth, and their mothers had lower plasma triglyceride
concentrations (128 mg% vs. 137) in pregnancy. In this world’s first lifecourse
analysis of glucose intolerance in a high risk “undernourished” population,
we highlight importance of early life beta cell impairment and programming
effect of intrauterine undernutrition and minimal prematurity. Our findings
suggest that type 2 diabetes in developing countries may have a “malnutrition related” beta-cell pathology. Current ideas of prevention of diabetes
by lifestyle interventions in adults should be revised to include the role of
intergenerational programming.
UZMA MOHAMMAD SIDDIQUI, MICHAEL THOMPSON, Worcester, MA
183‑LB
Several risk factors have been cited for the development of NODM (New
onset Diabetes Mellitus) in Liver transplant patients. Hepatitis C has been
identified as an independent risk factor for the development of NODM. We
performed a study looking for a correlation between viral loads, viral genotypes and treatment for Hepatitis C with the development and persistence
of Post transplant diabetes mellitus. This was a retrospective chart-review,
which looked at patients who underwent a Liver transplant at University
of Massachusetts (UMass) Medical Center from 6/2/2012-7/9/2014 (N=113).
The patients were followed for up to 12 months post transplant. The data
was collected from the Transplant Registry at UMass and from supporting medical records. Of the 113 patients, 6 underwent Living donor transplants (5.3%), while the rest underwent deceased donor. Indications for the
transplant included Alcohol abuse (47%), Hepatitis C (34.5%) and Hepatitis
B (0.8%), amongst other reasons. Of the total patients, 29% were diabetic
pre-transplant and hence were excluded from follow up. 7 patients died prior
to completion of the 12 month follow up. Of the 39 patients with Hepatitis
C, 12 patients had Pre-transplant diabetes. Of the remaining Hepatitis C patients, 14 (51.8%) developed NODM at 3 months post transplant, and most
of them remained diabetic a year out of transplant. Most of the patients that
developed NODM had a Hepatitis C genotype of 1a/1b. The post transplant
immunosuppressants, viral loads and treatment for Hepatitis C for these patients were also followed. The presence of NODM has been implicated in
poor outcomes in terms of graft survival and increased patient mortality. Our
ongoing study may help in identifying Liver transplant patients who are at
increased risk for Post transplant NODM and may therefore provide indication for closer observation, or even preemptive management.
Life-Course Associations of Body Fat Patterns with Diabetes and
Cardiovascular Risk Factors
CHITTARANJAN YAJNIK, ROHINI KELKAR, SUYOG JOSHI, CHARUDATTA
JOGLEKAR, MANOJ CHINCHWADKAR, CAROLINE FALL, Pune, India, Southampton, United Kingdom
The Pune Maternal Nutrition Study was set up in 1993 to study intergenerational determinants and lifecourse evolution of diabetes (DM) and
cardiovascular (CVD) risk. Serial anthropometric and DXA measurements are
available, and at 18 years of age we used MRI (mean of 3 sections 1mm apart
at L4-5 level) to study abdominal fat distribution (n=633, 95.5% of possible).
The participants had an average BMI of 19.1 kg/m2 (48.2% underweight,
5.7% overweight and obese) and DXA fat percent 21.3 (men 15.5, women
28.0). The abdominal subcutaneous fat area (SFA) was higher than the visceral (VFA) (94.1 vs. 57.7 cm2), and the two were inversely related (curvilinear
r2 =0.534, p<0.001). Men had higher VFA and women higher SFA. SFA was
directly related to socio-economic status, to parental BMI, and maternal folate , and inversely to maternal Vit D and B12 concentrations and physical
activity in pregnancy (p<0.05 for all, adjusted for age and sex). It was also
directly related to weight, length, and head circumference at birth, and fat
percent at 6, 12 and 18y. VFA had opposite relationships (p<0.05 for all). SFA
was directly and VFA inversely related to current weight, waist circumference and fat percent, but not to height. SFA was directly related to 120 min
glucose (OGTT), HOMA-IR, cholesterol, triglycerides and TLC, but inversely
to disposition index. VFA was inversely related. Hyperglycemics (IFG + IGT,
ADA criteria) had higher SFA compared to the normoglycemic (96.9 cm2 vs.
92.9 cm2, p<0.05) but similar VFA. In this world’s first description, we found
that parental BMI, maternal micronutrient nutrition and physical activity
during pregnancy were associated with subcutaneous and abdominal adiposity in adult offspring. SFA had a predisposing while VFA a protective association with glycemic and cardiovascular risk. Our results shed new light
on early life determinants of components of abdominal adiposity, and support observations that subcutaneous abdominal adiposity increases risk of
DM and CVD in SA Indians.
186‑LB
Association between Type 2 Diabetes and Prognosis in Colorectal
Cancer
JUHONG YANG, Boston, MA
Purpose: Type 2 diabetes is associated with an increased risk of colorectal
cancer (CRC) but controversial exists in its association with prognosis, as
most studies did not account for various potential confounders, such as cancer stage, physical activity and body mass index (BMI) in their analyses.
Patients and Methods: We analyzed survival by diabetes status among
1,303 patients diagnosed from 1986 to 2010 from two prospective cohort
studies: the Nurses’ Health Study (NHS) and Health Professionals Follow-Up
Study (HPFS). We used Cox proportional hazards models to calculate the
hazard ratios (HRs) for colorectal cancer specific mortality (CM) and overall
mortality (OM), after adjustment for cancer stage, tumor grade and location,
postdiagnosis smoking, aspirin usage, BMI, and physical activity. Survival
time was calculated from CRC diagnosis to death or last follow-up.
Supported By: UK Wellcome Trust; Government of India
Effects of Chikungunya Fever on Diabetes
184‑LB
EDDY JEAN-BAPTISTE, FREDERICA RAPHAEL, NANCY C. LARCO, PHILIPPE LARCO, JULIA VON OETTINGEN, RENE CHARLES, Port-au-Prince, Haiti, Boston, MA
Very few data exist regarding the effects of chikungunya fever (CKF)
on diabetic patients. This study aimed to determine the impact of CKF on
ADA-Funded Research
For author disclosure information, see page LB98.
LB47
POSTERS
Supported By: UK Wellcome Trust; Government of India
Epidemiology/
Genetics
185‑LB
Hepatitis C and New Onset Diabetes Mellitus in Liver Transplant
Patients
Epidemiology—Type 1 DiabetesGenetics—Type 1 Diabetes
Results: In 1,303 CRC patients, 107 (8.21%) were complicated with type
2 diabetes. There was no difference in cancer stage, differentiation, location, family history and gender between diabetes and non-diabetic patients.
Diabetic patients had a higher BMI and less physical activity. Comparing
diabetic patients to non-diabetic patients, the HRs for death were 0.944
(95% CI, 0.582 to 1.531, P>0.05) for CM and 1.492 (95% CI, 1.135 to 1.961,
P=0.004) for OM. Compared to those without diabetes, the HRs for OM was
1.072 (95% CI, 0.667 to 1.721, P>0.05) for patients with short-term diabetes
(<5 years), and 1.804 (95% CI, 1.305 to 2.492, P=0.003) for patients with
long-term diabetes (>5 years).
Conclusion: Diabetes especially long-term diabetes is associated with
decreased overall survival but not cancer specific survival among patients
with colorectal cancer.
Supported By: R01CA151993, K07CA190673
Epidemiology—Type 1 Diabetes
187‑LB
Who Is Not Returning? Retention of Recruited Subjects in the Type 1
Diabetes TrialNet Pathway to Prevention
189‑LB
Noninvasive Measurement of Beta Cell Function in Adult Subjects
with New Onset Type 1 Diabetes
POSTERS
Epidemiology/
Genetics
EMILY K. SIMS, DAVID BOULWARE, CARMELLA EVANS-MOLINA, CARLA J. GREEN­
BAUM, HENRY RODRIGUEZ, JEFFREY P. KRISCHER, LINDA A. DIMEGLIO, TYPE 1
DIABETES TRIALNET STUDY GROUP, Indianapolis, IN, Tampa, FL, Seattle, WA
DAVID A. BAIDAL, JASON L. GAGLIA, Boston, MA
Serum C-peptide (CP) measures during mixed meal tolerance test (MMTT)
are often used to assess beta-cell function in type 1 diabetes (T1D) clinical trials. As a noninvasive alternative, we evaluated whether urinary Cpeptide/creatinine ratio (UCPCR) correlated with CP during MMTT in newly
diagnosed (< 6 months) T1D subjects and healthy controls. Nineteen T1D
subjects (age 25±6 years, male 13/19) and 20 healthy controls (age 26±4
years, male 16/20) were enrolled. Subjects underwent standardized 2hr
MMTT. A subset of 6 T1D patients had serial MMTT over 1 year. UCPCR
was calculated from 2nd fasting and post-MMTT urine samples. We found
no significant correlation between UCPCR and fasting or MMTT CP values in
controls. By contrast, in T1D subjects fasting UCPCR correlated with fasting
CP (r=0.61, p<0.01), and post-MMTT UCPCR correlated with both 90min CP
(r=0.64, p<0.01) and CP AUC (r=0.69, p<0.01). Serial MMTT showed persistent correlations between fasting UCPCR and fasting CP (r=0.63, p=0.003),
and between post-MMTT UCPCR and 90min CP (r=0.78, p<0.001) and CP
AUC (r=0.81, p<0.001) (Fig. 1). In T1D patients UCPCR strongly correlated with
fasting CP, 90min CP, and CP AUC with correlations persisting over time, supporting use of this simple test for monitoring beta-cell function in new onset
T1D clinical trials. A nonlinear association at higher CP values may explain
the lack of significant correlations seen in controls.
The TrialNet Pathway to Prevention (PTP) screens first and second-degree
family members of persons with type 1 diabetes (T1D) to identify subjects at
high T1D risk, and enrolls eligible persons into natural history and prevention
studies. As of January 2015, PTP screened 144,476 individuals worldwide
at both clinical centers and affiliate sites. To determine which antibodypositive (Ab+) subjects were either successfully recruited into monitoring
studies or lost to follow-up, we performed multivariate logistic regressions
of PTP data. Only variables with a p value <0.05 were interpreted as having
a significant effect. First, we defined characteristics of single Ab+ subjects
on initial screen (n=4228) who failed to return for confirmatory Ab testing
(n=1191, 28.2% of recruited subjects). Older subjects, parents and children
of probands with T1D, persons recruited by affiliate sites (vs. clinical centers), racial minorities (Blacks, Native Americans, Pacific Islanders), and
Hispanics/Latinos were less likely to follow-up. We also examined which
subjects eligible for monitoring (n=4726) were not currently participating in
TN PTP monitoring visits (n=1542, 32.6% of Ab+ subjects). Again parents of
probands, racial minorities, and subjects recruited by affiliates were less
likely to continue with monitoring. Interestingly, age and ethnicity were not
predictive at this stage. Those who were 4Ab+ were most likely to return.
These data confirm clear differences between successfully recruited populations and those lost to follow-up. Future work is needed to improve retention of Ab+ participants in order to facilitate rapid enrollment and reduce
selection biases in T1D natural history and prevention studies.
Supported By: K08DK103983 (to E.K.S.)
188‑LB
Are There Gender Differences in the Management among Our Pa‑
tients with Type 1 Diabetes?
NOEMI GONZALEZ, LUCRECIA HERRANZ, ROSALIA SANCHEZ, NATALIA HILL­
MAN, BEATRIZ BARQUIEL, FELIPE PALLARDO, Madrid, Spain
Sex differences in achievement of lipid and glycemic control have been
related to worse cardiovascular outcomes in women with type 1 diabetes
(DM1). We examined if quality of care varied by gender in our Diabetes Unit
in patients without coronary heart disease. A1c, lipid profile (LDLcol, HDLcol,
total col, triglycerides) and clinical data from patients seen during 2013 were
collected from lab and clinical reports. Target Glycemic Control (TGC) was
defined as A1c <7%. Target Lipid Control (TLC) as LDLcol <100 mg/dL, HDLcol
>40 (men) or >50 (women) mg/dL and TG <150 mg/dL; Target Cardiovascular
Index (TCVI) as total chol/HDL <4 (women) or <4.5 (men). Univariate analysis
was used to compare women and men with DM1. 828 patients were included. Clinical characteristics, biochemical parameters and glycemic/ lipid
targets are shown in Table 1. Less than 40% of the patients achieved glycemic or lipid target, with no sex differences (TGC 39.3% vs. 37.7%; TLC
35.4 vs. 40.3; p=ns). 93.1% (women) and 92.8% (men) (p=0.854) had targeted
CV Index. Despite longer duration of diabetes, and less lipid lowering drugs
in women, no gender differences with regard to Target Glycemic, Lipid and
Cardiovascular Index Control were found. These results reflect an adequate
awareness about female cardiovascular risk, but an effort to improve guideline-based clinical practice is still needed independent of sex.
Genetics—Type 1 Diabetes
A RAGE Gene SNP Is Associated with Type 1 Diabetes
190‑LB
JUNNOSUKE MIURA, MANABU KAWAMOTO, YASUSHI KAWAGUCHI, SARI
HOSHINA, HIROKO TAKAIKE, MARI OSAWA, HISASHI YAMANAKA, YASUKO
UCHIGATA, Tokyo, Japan
Receptor for advanced glycation endproducts (RAGE) is related to not only
vascular damage but also immune disturbance. Therefore, we tested the association between RAGE gene SNPs and type 1 diabetes (T1D). The subjects
were 817 patients with T1D (305 men, 698 of acute onset, onset age: 19±13
years old, 119 of slowly progressive with GAD Ab+, onset age: 34±16 yrs
old). Gene polymorphisms were determined by Taqman SNP assay of known
SNPs of RAGE gene, G82S (G/A), -429T/C and -374T/A. A sixty-three bp dele-
ADA-Funded Research
For author disclosure information, see page LB98.
LB48
Genetics—Type 2 Diabetes
Table 1. Example of Variants Found.
nPOD Gene,
AA PolyPhen Minor Allele Cause of Death Histopathology
ID
Variant Change Score Frequency
6033 KCNJ11, Val290Met 1.000 0.00001648 Cerebrovascular Ins-/Gluc+ islets. Moderate Ki67+
c.868G>A
acinar cells. Acinar atrophy with
increased fibrosis
6037 MNX1, Pro356Ser 0.915 0.00006834 Cerebrovascular Ins-/Gluc+ islets, reduced size and
c.1066C>T
numbers. Mild infiltrate, Low Ki67
acinar cells. Minimal vascular
disease.
6166 LMNA, Asp300Asn 0.955 0
Anoxia
Ins+ (highly)/Gluc+ islets, numerous.
c.898G>A
Mild fatty infiltrate. Multifocal, mild
ductular dysplasia. CVD- moderate.
6173 UCP2, Met287Thr 0.990 0.00002713 Anoxia
Ins-/Gluc+ islets, reduced density.
c.860T>C
Acinar atrophy moderate to severe
with prominent nerve fibers and
diffuse chronic pancreatitis (CD3+
infiltrates).
6176 HNF1A, Thr10Met 0.965 0.00003463 Anoxia
Ins+ (weak)/Gluc+ islets, numerous
c.29C>T
but small sized. Mild acinar atrophy.
6243 GLIS3, His621Gln 0.999 0
Cerebrovascular Ins+/Gluc+ islets (reduced numbers
c.1863C>G
but present throughout), glucagon+
only islets (pseudoatrophic). Insulitis
present particularly PanTail. Low
normal Ki67 islets and acinar cells.
Hydropic degeneration in scattered
islets within most regions.
6249 INSR,
N/A
N/A N/A
Cerebrovascular Ins+/Gluc+ islets. Moderate exocrine
Multiatrophy. Global robust amyloidosis.
exonic
Multifocal, mild chronic pancreatitis.
deletion
Mild to moderate atherosclerosis
with infrequent focal calcification
within arterial walls.
6264 INSR, Val1012Met 0.992 0.00000824 DKA
Ins+ (very rare)/Gluc+ islets present.
c.3034G>A
Numerous scattered single alpha
cells or in very small islets (clusters).
Insulitis in PanBody 03 observed.
Peri-ductular, lobular fibrosis mild.
Very mild acinar atrophy.
191‑LB
Two Novel Loci in the GCKR Gene Contribute to Develop Monogenic
Diabetes
PIOTR GNYS, KAROLINA ANTOSIK, WOJCIECH MLYNARSKI, MACIEJ BOROWIEC, Łódz,’ Poland
GCKR gene encodes GKRP (Glucokinase Regulatory Protein) that is a
hepatocyte-specific protein acting as a modulator of glucokinase. We performed Sanger’s sequencing of GCKR gene among 15 patients of Polish
descent with clinical features of diabetes (Table 1). Beside already known
single nucleotide polymorphisms (rs1260320, 2293571, 1260326, 8179236,
183738110) we have found 2 novel genetic alteration. First GCKR variant c.5592G>T, was found in a patient who was initially screened for mutations
in the GCK gene. Second - c.26521A>G, was found in a patient who was analyzed throughout KCNJ11, INS and GCK gene. In both cases Sanger sequencing and MLPA technique were performed and none mutations beside those
among GCKR gene were identified. Intronic variant c.5592G>T is located
inside the sequence assigned as Long Interspersed Nuclear Elements (LINE),
which may have influence on epigenetic regulation. The second identified intronic change - c.26521A>G is a part of the sequence that binds transcription
factor CTCF. CTCF is known for being responsible for transcriptional regulation by binding to chromatin insulators and preventing interaction between
promoter and nearby enhancers and silencers. Taking into account these informations we may consider potential role and association of these changes
with patients clinical outcome. These cases brings new ways of thinking
about the role of GKRP in regulating glucose homeostasis.
Supported By: JDRF (nPOD)
Genetics—Type 2 Diabetes
193‑LB
High-Density Imputation and Trans-ethnic Association Analysis
Reveals a Novel Locus for Type 2 Diabetes Susceptibility
ANDREW P. MORRIS, Liverpool, United Kingdom
The Resource for Genetic Epidemiology Research on Adult Health and
Aging (GERA) is a large multi-ethnic population-based cohort, created for
investigating the genetic and environmental basis of common age-related
diseases, including type 2 diabetes (T2D). Participants were genotyped using
one of four custom arrays, designed to maximise coverage of common and
low-frequency variants in non-Hispanic white, East Asian, African-American
and Latino ethnicities. With these data, this study aimed to discover loci for
T2D susceptibility through high-density imputation and trans-ethnic association analysis and to evaluate the evidence for heterogeneity in allelic effects on the disease between ancestry groups. After quality control, 71,604
unrelated participants, including 9,747 T2D cases, were retained for analysis
and imputed up to the multi-ethnic reference panel (Phase 3, October 2014
release) from the 1000 Genomes Project Consortium. High-quality imputed
Supported By: 2013/09/N/NZ4/01775, TEAM-2009-3/7
The Histopathology of Monogenic Diabetes
192‑LB
DAVID CARMODY, DANIELA DEL GAUDIO, KELLY ARNDT, YING YING HU, FRANCES KOBIERNICKI, GORKA ALKORTA-ARANBURU, MARK A. ATKINSON, IRINA
KUSMARTSEVA, SIRI ATMA W. GREELEY, Chicago, IL, Gainesville, FL
Single gene mutations cause 1-2% of all diabetes but because diagnosis
relies on clinical suspicion many are unrecognized. We utilized the Network
for Pancreatic Organ Donors with Diabetes (nPOD) to allow histopathological
correlation to genetic results in cases with potential monogenic causes of
diabetes. 310 nPOD cases were considered for genetic testing if they met
either of the following: a) diabetes diagnosed under 35 years of age without
ADA-Funded Research
For author disclosure information, see page LB98.
LB49
POSTERS
detectable type 1 diabetes (T1D) antibodies or b) diagnosed with T1D but
with evidence of persistent C-peptide production >5 years after diagnosis.
Those with cystic fibrosis or a BMI >35 kg/m2 were excluded. We identified
38 cases for genetic testing; DNA of sufficient quality for analysis was available for 35 cases. DNA was isolated and samples were analyzed using an
in-house next-generation sequencing (NGS) panel including 41 genes associated with monogenic diabetes and lipodystrophy. 24 donors were negative
for variants of significance while 11 of 35 donors had variants identified within targeted genes (8 most significant shown in Table 1). Case 6176 represents
the first report of histopathology for MODY3/HNF1A (known causal variant).
6033, 6249, 6264 and 6166 require further study regarding unexpected but
plausible causes related to chronic insulin resistance/overproduction. We
demonstrate that variants within monogenic diabetes and lipodystrophy
genes are common and deleterious mutations may go unrecognized.
Epidemiology/
Genetics
tion polymorphism between -429T/C and -374T/A was determined by PCR.
These allele frequencies were compared to that of 887 healthy controls (HC)
(525 men, 39±11 yrs old). The Linkage disequilibrium (LD) analysis was done
among polymorphisms of RAGE genes. All SNPs in T1D and HC were satisfied
with Hardy-Weinberg Equilibrium. The allele frequencies (%) of T1D were
G82S G/A: 86.9/13.1, -429T/C T/C: 79.4/20.6, -374T/A A/T:76.2/23.8, and
63bp wild/del:96.7/3.3 while those of HC were G/A: 86.0/14.0, T/C: 92.1/7.9,
A/T:76.0/24.0, and 63bp wild/del: 98.0/2.0, respectively. There was significant difference in -429T/C SNP between T1D and HC (p = 1.75 x 10 -24), and the
odds ratio was 2.82 (95% CI: 2.29-3.46). The allele frequencies of acute onset
and slowly progressive T1D were -429T/C T/C: 79.5/20.5 and 80.5/19.5 (not
significant). There was significant difference in -429T/C frequency of each
T1D subclass compared with HC (p=1.39 x 10 -23 and 3.9 x10 -8). The -429T/C
allele frequencies in male and female T1D were T/C: 77.3/22.7 and 80.8/19.2
(not significant). There was significant difference in -429T/C SNP between
T1D and HC in male (p=9.28x10 -23), and in female (p=6.05 x10 -19), and these
odds ratio were 3.41 (95% CI: 2.64-4.41) and 2.77 (2.20-3.30). Pairwise LD
analyses revealed the presence of complete disequilibrium among the four
RAGE polymorphisms. There were no differences in frequencies of other
3 polymorphisms between 2 subclasses of T1D. This study indicated that
RAGE gene -429 T/C SNP was strongly associated with T1D in Japanese.
Genetics—Type 2 Diabetes
variants were tested for association with T2D in a logistic regression model,
after adjustment for sex and eigenvectors from principal components analysis to account for trans-ethnic and ancestry-specific population structure.
Common lead SNPs at ten loci attained genome-wide significant evidence
(p<5x10 -8) of association with T2D, including a novel signal mapping to
TOMM40 (p=2.8x10 -9). This gene has been previously implicated in Wolfram
Syndrome, a neurodegenerative disorder characterised by diabetes mellitus.
Across lead SNPs for the ten loci, nominal evidence of heterogeneity in allelic effects between ethnicities was observed only at TCF7L2 (pHET=0.012),
where the risk allele had the lowest T2D odds-ratio for participants of East
Asian ancestry. This study provides further evidence for the homogeneity of
allelic effects of common T2D risk variants across diverse populations, and
highlights the benefits of trans-ethnic analysis for discovery of novel loci
associated with the disease.
acid IR index (FFA-IRI; P=1.3x10-4). The TGD rate represents mainly skeletal
muscle IR; hGP indicates hepatic IR and FFA IR indicates adipose IR. ADH1B
protein was decreased with high BMI (P<0.05, N=12). In summary, decreased
adipose ADH1B expression was associated with increased obesity, whole
body IR, IR in liver, skeletal muscle and adipose tissue, and with declining
β-cell function. Interestingly, serum levels of circulating endogenous ethanol, a substrate for ADH1B, decreased with increasing OB/IR (P=0.019 with
a 7-fold increase in FPI).
Supported By: National Institutes of Health; U.S. Department of Veterans Affairs
196‑LB
PCSK2 Variant rs200711626 R430W Is Associated with Type 2 Dia‑
betes in the Amish
ALEXANDRA H. WINTERS, LAURA YERGES-ARMSTRONG, TONI I. POLLIN, IRIS
LINDBERG, Baltimore, MD
Supported By: UK Wellcome Trust (WT098017)
Prohormone convertase 2 (PC2), encoded by PCSK2, is one of two enzymes that cleave proglucagon and is the sole enzyme that cleaves mature
glucagon. In humans, noncoding variants near PCSK2 have been previously
associated with risk for and age of onset of type 2 diabetes and with variation in glucagon levels. However, coding variants in PCSK2 are rare and no
missense variants with a minor allele frequency (MAF) greater than 0.001
are present in 1000 Genomes (phase 3). The Old Order Amish (OOA) are a
genetically well-defined founder population of European descent that immigrated to the U.S. from Western Europe. The Amish Family Diabetes Study
was a study designed to identify genes associated with type 2 diabetes by
recruiting OOA individuals with type 2 diabetes and their first- and seconddegree relatives. We hypothesized that coding variants in PCSK2 would be
associated with type 2 diabetes and diabetes-related traits. There is one
coding variant found in PCSK2 in the OOA, R430W (rs200711626), with approximately 4% MAF in the OOA. This variant is greatly enriched in the OOA
as compared to other populations with 2 copies (0.04%) in 1000 genomes
and 1 copy in the NHLBI Exome Sequencing Project (0.008%). R430W is
twice as common among Amish individuals with diabetes (8.4% MAF in 137
individuals) as compared to those with normal glucose tolerance (3.7% in
578 individuals) (p=0.04). R430W also has a trend towards carriers having
increased insulin at 30 minutes of the OGTT (p=0.07) and increased HbA1c
(p=0.07). PC2 R430W shows greater enzyme activity as measured by in vitro
in cleavage of a fluorogenic substrate. We hypothesize that R430W carriers’
increased PC2 activity compared to wildtype causes increased cleavage of
proglucagon to glucagon particularly at the time of inappropriate glucagon
secretion postprandially, necessitating the higher insulin levels at 30 minutes of the OGTT. This increased glucagon may be leading to the increased
risk of type 2 diabetes.
194‑LB
TCF7L2 Overexpression and Type 2 Diabetes: Dissecting the Func‑
tion of TCF7L2 as a Regulator of Glucose Metabolism
POSTERS
Epidemiology/
Genetics
KATHLEEN A. BAILEY, MATTHEW PIRON, JONATHAN KAHN, RONALD COHEN,
GRAEME I. BELL, MATTHEW J. BRADY, MARCELO A. NOBREGA, Chicago, IL
Intronic variation within TCF7L2 is the most strongly associated genetic
determinant of T2D risk in humans. Although the majority of studies have
concentrated on the roles of TCF7L2 in pancreatic beta cells, the T2D associated interval drives TCF7L2 expression throughout a variety of peripheral
tissues with known roles in glucose metabolism. We interrogated the role
of TCF7L2 in mouse adipocytes to elucidate the peripheral contribution of
TCF7L2 signaling and identify how perturbation of this pathway could lead
to T2D risk. Utilizing a glucose intolerant humanized mouse model globally
overexpressing TCF7L2, we specifically restored endogenous expression
in adipocytes while maintaining overexpression elsewhere. We found that
restoration of TCF7L2 expression in adipocytes alone was sufficient to rescue whole-body glucose and insulin intolerance. Furthermore, we identified
restored adipocyte insulin sensitivity, proper triglyceride storage, reduced
adipocyte hypertrophy, and the prevention of ectopic lipid accumulation,
indicating that restoration of endogenous TCF7L2 expression in adipocytes
markedly improved glucose metabolism and storage, even in face of the
persistent overexpression of TCF7L2 elsewhere. These data demonstrate
that the restoration of TCF7L2 expression in adipocytes restores glucose
tolerance and metabolic health, indicating that overexpression of TCF7L2 in
adipocytes significantly contributes to the T2D state. Our study highlights
the complexities of a multi-system phenotype such as glucose metabolism
and supports a distinct and relevant role of TCF7L2 expression in adipocytes.
Further elucidation of the signaling mechanism of TCF7L2 action in adipocytes may lead to new therapeutic targets for T2D treatment.
197‑LB
Single Nucleotide Polymorphisms Associated with Clinical Out‑
comes of High-Dose Insulin Intensification in Type 2 Diabetes
195‑LB
Transcriptomic Identification of ADH1B as a Candidate Gene for
Obesity and Insulin Resistance in Human Adipose Tissue in Mexi‑
can Americans from the Veterans Administration Genetic Epidemi‑
ology Study (VAGES)
P. ANTHONY AKKARI, SUMAN DUVVURU, SREEKUMAR G. PILLAI, SUDHA S.
SHANKAR, MARK A. DEEG, HOLLY R. MARTIN, JENNAL L. JOHNSON, STEPHEN
O’RAHILLY, JEFFREY A. JACKSON, Chapel Hill, NC, Indianapolis, IN, Cambridge,
United Kingdom
This study sought to characterize relationships between gene variants
and various clinical outcomes in severely insulin-resistant patients with
type 2 diabetes after treatment intensification with high-dose human regular U-500 insulin. DNA samples were obtained from patients enrolled in a
24-week, multicenter, open-label, randomized trial in the United States. Association of clinical outcomes of 660 single nucleotide polymorphisms (SNPs)
in genes involved in metabolism and type 2 diabetes risk were tested in 211
Caucasian individuals. These outcomes included glycemic efficacy, risk of
hypoglycemia, change in body mass index, insulin dose requirements, lipid
levels, and liver and renal function. Several SNPs with P value (raw) threshold of ≤0.01 were observed in genotype-phenotype associations (Table). The
IGF-1 SNP, rs1520220, demonstrated significant associations with change in
aspartate and alanine aminotransferase levels (P <0.0001). These data show
for the first time that phenotypic responses to high-dose insulin therapy for
type 2 diabetes are linked to select genetic markers. Further validation of
these findings in prospective trials is warranted.
CHRISTOPHER P. JENKINSON, DEVJIT T. TRIPATHY, DOUGLAS T. CROMACK,
JOANNE E. CURRAN, SATISH KUMAR, MELANIE CARLESS, MUHAMMAD
ABDUL-GHANI, SOBHA PUPPALA, RECTOR ARYA, THOMAS D. DYER, DONNA
M. LEHMAN, SHIRLEY L. HU, MARCEL FOURCAUDOT, LUKE NORTON, VIDYA S.
FAROOK, JOHN BLANGERO, HARALD H. GÖRING, RALPH A. DEFRONZO, RAVINDRANATH DUGGIRALA, Edinburg, TX, San Antonio, TX, Harlingen, TX
Type 2 diabetes is a complex disease that is highly prevalent in Mexican
Americans, and is strongly associated with obesity and insulin resistance
(OB/IR). The aim of this study was to measure genome-wide gene expression
in adipose tissue to detect gene regulation associated with OB/IR in 75 unrelated Mexican Americans. Fasting RNA was extracted from adipose biopsies, and gene expression data generated using Illumina Bead Arrays (47,324
probes). Gene sets analysis identified one gene, alcohol dehydrogenase 1B
(ADH1B) with significantly enriched expression (P<10-60) as a candidate for
involvement in multiple relevant metabolic pathways. Adipocyte ADH1B was
highly and specifically expressed in adipose tissue at levels greater than in
all other tissues examined. ADH1B expression was inversely correlated with
all OB/IR variables at the tissue and whole body levels: waist circumference (P=2.8x10-9), BMI (P<0.0001), fasting plasma insulin (P<0.001), HOMAIR (P<0.01), Matsuda Index (P<0.01), β-cell function (oral disposition index
across 120 minutes of the oral glucose tolerance test (ODI1-120; OGTT)
(P=8.6x10-4), pre-T2D (impaired glucose tolerance and fasting glucose during the OGTT (P=8.6x10-5); and from the insulin clamp: total glucose disposal (P=8.6x10-10), hepatic glucose production (hGP, P=8.6x10-4) free fatty
ADA-Funded Research
For author disclosure information, see page LB98.
LB50
Genetics—Type 2 Diabetes
Table.
on genome and transcriptome variability available through GTEx, in which
whole genome sequencing has been conducted in a set of individuals (>450)
in which RNAseq has been completed on up to >30 tissues. We applied
penalized regression procedures to develop SNP-based predictors of gene
expression. We can apply these predictors in a method we term “PrediXcan”
(predicted expression scan) to any data with at least GWAS level interrogation of the genome, and test the association of genetically predicted gene
expression for a specific tissue with disease phenotypes. Thus, we conduct
a gene-based test that is mechanistic by design, robust to reverse-causality
issues, and provides an easy-to-interpret direction of effect. We applied
PrediXcan using models for 15 tissues from the GTEx project to GWAS data
from the WTCCC and Starr County (Mexican American) cohorts. Associated genes in the WTCCC analysis include TRIM66 (p = 1.7e-5, adipose), ID4
(p = 1.0e-6, small intestine), and MTMR10 (p = 3.3e-6, whole blood). In the
Starr County analysis, TOMM7 showed the most significant association in
multiple tissues (p = 1.2e-6, 6.4e-7, 1.0e-6 in skeletal muscle, adipose, and
cerebellum, respectively). Overall, we found enrichment of previously implicated T2D genes among SC and WTCCC results across several tissues as
well as significant overlap of top genes between the two studies. These
results show that more biology can be gleaned from the union of GWAS with
functional data and suggest that PrediXcan can provide new opportunities
for researchers to characterize the genetic basis of T2D.
198‑LB
Genetic Risk to Fasting Glucose Modulates Changes in Glycemic
Traits in Response to 2-Year Weight-Loss Diet Intervention: The
POUNDS Lost Trial
Supported By: National Institute of Diabetes and Digestive and Kidney Diseases
TIANGE WANG, TAO HUANG, YAN ZHENG, GEORGE A. BRAY, FRANK M. SACKS,
LU QI, Boston, MA, Baton Rouge, LA
200‑LB
We examined whether a genetic risk score (GRS) for fasting glucose modifies the long-term changes in glycemic traits in response to weight-loss diets
in the Preventing Overweight Using Novel Dietary Strategies (POUNDS Lost)
trial. A GRS was calculated based on 15 fasting glucose-associated SNPs in
733 adults. The changes in fasting glucose, insulin, homeostasis model assessment of insulin resistance (HOMA-IR) and insulin sensitivity (HOMA-S) were
assessed by GRS and diet interventions. At 6 months, in the lowest tertile of
GRS, participants assigned to low-fat diet group had less reduction in fasting
glucose, insulin, and HOMA-IR, and less increase in HOMA-S, compared with
those assigned to high-fat diet group. Opposite relations between dietary fat
and changes in glycemic traits were found in the highest tertile of GRS (Figure). The GRS-dietary fat interactions were significant on changes in glucose,
HOMA-IR and HOMA-S (P≤0.047) after adjustment for age, sex, ethnicity, and
baseline values for respective outcomes. After further adjustment for weight
loss, the GRS-dietary fat interaction on change in glucose remained significant
(P=0.013). The interactions became attenuated at 2 years due to the rebound
of glycemic traits. Individuals with higher genetic predisposition to fasting glucose may benefit more in glycemic improvement by choosing a low-fat diet.
Exome-Wide Association Study Revealed Seven Novel Variants As‑
sociated with Liver Enzymes
201‑LB
High Resolution Maps Identify Novel T2D Genes and Regulatory Hot
Spots in African Americans and Europeans
NIKOLAS MANIATIS, WINSTON LAU, FILIPPO TAMANINI, TOBY ANDREW, London, United Kingdom
High-resolution genetic maps provide refined information about the structure of linkage disequilibrium (LD) in the human genome. This information is
essential in genome-wide association studies (GWAS) and for determining
genetic differences between populations. Despite the known importance of
LD in gene mapping, most GWAS studies ignore LD when testing for association or treat it as a nuisance factor. Our GWAS method improves power
to locate genes by using genetic map distance for this task. Here we identify
new loci by 1) analysing two different ethnic populations of African-American
and Northern-European descent; 2) utilising genetic map distances that are
specific to each of these two populations; 3) integrating data from European
GWAS and adipose tissue expression profiling with the aim to co-locate loci
on these genetic maps. Two population-specific genetic maps in LD units (LDU
maps) for African-Americans and Europeans were constructed using HapMap
data. The two European T2D GWAS data were provided from the WTCCC1
and WTCCC2 and African-American from the NIDDK. Independent genomic
and adipose expression data for healthy Europeans were obtained from dbGaP
and EBI respectively. Our whole genome analysis using map distances in LDU
199‑LB
“Imputing” the Genetics of Type 2 Diabetes: Testing the Association
of Genetically Imputed Gene Expression with Type 2 Diabetes
JASON M. TORRES, HEATHER E. WHEELER, NICHOLAS W. KNOBLAUCH, KAANAN SHAH, JENNIFER E. BELOW, CRAIG L. HANIS, NANCY J. COX, HAE KYUNG
IM, Chicago, IL, Houston, TX, Nashville, TN
Recent studies have shown that a substantial part (up to 80%) of the
heritability for common diseases is attributable to DNA variation in DNAse I
hypersensitivity sites (Gusev et al. 2014. AJHG), suggesting that regulation
at the level of transcription may drive much of the common variant signal observed for common disease. Moreover, there is now a wealth of information
ADA-Funded Research
For author disclosure information, see page LB98.
LB51
POSTERS
Liver enzymes have been reported to be an index of liver injury and a marker
of fatty liver and oxidative stress. Also elevated liver enzymes have been
known to be related with type 2 diabetes, body mass index, metabolic control
and the presence of the metabolic syndrome. Therefore, finding genetic factors influencing liver enzyme levels is very important to understand individual
difference and also underlying mechanism of liver related diseases and metabolic iseases. In the last decade, numerous common variants (MAF >= 5%)
responsible for liver enzymes have been discovered by the advent of genomewide association studies (GWAS). However, rare exonic variants (MAF < 5%)
have not yet been studied for potential association with liver enzymes. In this
study, we conducted an exome-wide association study to identify rare variants
associated with liver enzymes. First, we constructed 848 samples of whole
exome reference panel using GWAS chip, exome array, and exome sequencing
data. Using whole-exome reference panel, imputation analysis was performed
on 8,529 samples of combined data consists of GWAS chip and exome array.
For imputation analysis, we used generally used pre-phasing based imputation
process using shapeit and minimac software. Subsequent association analysis
was performed on about half million imputed and genotyped variants. No new
associations were discovered at the genome-wide significance level (P < 5e-8).
At the suggestive significance level (P < 5e-6), we discovered 7 novel variants including two missense variants. Among them, six variants were located
at exonic regions of genes including LHCGR, A1CF, OBSCN, RET, COL4A1, and
KIAA1456. One novel variant was discovered at intergenic region of 10q21.1.
Epidemiology/
Genetics
YOUNG JIN KIM, YUN KYOUNG KIM, TAE-JOON PARK, SANGHOON MOON,
BONG-JO KIM, Cheongju, Republic of Korea
Genetics—Type 2 Diabetes
204‑LB
identified 93 novel genome-wide significant gene regions that are common to
both Europeans and African-Americans. More than 60% of these trans-ethnic
signals reside within <50kb of one another, demonstrating the high resolution
of our findings. Using the adipose expression data, two-thirds of the 93 loci
also appeared to regulate gene expression. Such location estimates are instrumental for designed targeted resequencing, which in turn has the potential to
bring us closer to personalised medicine and understanding what screening
can be applied to T2D patients from different ethnic backgrounds.
Exome Chip Meta-analysis Identifies Low-Frequency Variants Con‑
tributing to Body Fat Distribution
CECILIA M. LINDGREN, ANNE E. JUSTICE, HEATHER M. HIGHLAND, KRISTIN L.
YOUNG, MISA GRAFF, TUGCE KARADERI, NANCY L. HEARD-COSTA, DOROTA
PASKO, VALERIE TURCOT, YONGKE LU, LORRAINE SOUTHAM, L. ADRIENNE CUPPLES, CHING-TI LIU, CAROLINE S. FOX, THOMAS W. WINKLER, NIELS GRARUP,
ROBERT A. SCOTT, MARK I. MCCARTHY, KAREN L. MOHLKE, RUTH J.F. LOOS,
INGRID BORECKI, KARI E. NORTH, THE BBMRI CONSORTIUM, THE GOT2D CONSORTIUM, THE CHARGE CONSORTIUM, THE GIANT CONSORTIUM, Cambridge,
MA, Chapel Hill, NC, Houston, TX, Oxford, United Kingdom, Boston, MA, Exeter,
United Kingdom, Montreal, QC, Canada, New York, NY, Cambridge, United Kingdom,
Farmingham, MA, Regensburg, Germany, Copenhagen, Denmark, St. Louis, MO
Supported By: UK Medical Research Council (G0901017)
202‑LB
Obtaining More from Genome-Wide Analysis: Localisation of Novel
European-specific Genes for Type 2 Diabetes
Fat distribution, a heritable trait measured as waist to hip ratio adjusted
for BMI (WHR), is correlated with visceral adiposity (r=0.56). Aggregation of
visceral fat and unfavourable fat distribution is a predictor of increased type
2 diabetes (T2D) risk. Here, we set out to identify coding and low-frequency
variants (LFVs) (minor allele frequency, MAF<5%) associated with fat distribution across the human exome using array data from 136,404 European
ancestry (EA) and an additional 26,697 participants of other ancestries. We
meta-analyzed study specific additive models for both single variant and
gene-based results with WHR in men and women combined. Gene-based
models were defined by non-synonymous variants of MAF<5% and analyzed
using the sequence kernel association test (SKAT) method. Analyses included up to 201,126 variants with MAF<5% and 15,000 genes with >1 variant
at MAF<5%. We identified three variants in novel loci: one with MAF>5%
(intergenic) and two non-synonymous variants with MAF<5% (in KIAA0408
and RAPGEF3). The non-synonymous variant within RAPGEF3 exhibited a
much greater effect on WHR compared to common variants (beta > 0.1 versus 0.062). Our gene-based analyses also identified RAPGEF3 as significantly
associated with WHR (p<2.5e-06) after correction for multiple testing.
RAPGEF3 has been reported to be involved in the regulation of insulin secretion. Ongoing analyses include an expansion of the sample (>300,000) and
functional follow-up. These observations highlight the importance of largescale genomic studies for identifying fat distribution susceptibility variants
and provide insights into the etiology of fat distribution, and may highlight
population-specific variants that pose increased susceptibility among individuals at greater risk.
POSTERS
Epidemiology/
Genetics
WINSTON LAU, FILIPPO TAMANINI, TOBY ANDREW, NIKOLAS MANIATIS, London, United Kingdom
Although 80 loci increasing risk of type 2 diabetes (T2D) have been identified by genome-wide association studies (GWAS) in European populations, additional fine mapping is required since 1) many loci remain to be
identified given the polygenic nature of T2D; 2) the most significant genetic
markers (SNPs) associated with disease will often not be proximal to the
causal variant(s) location; and 3) the implicated genes and variant function
are often still ambivalent. We aimed to identify novel loci by using a mapping approach that utilises information from multiple markers within an analytical interval rather than assessing one SNP at a time. The markers in the
analysis are located on a genetic rather than physical map and hence the
method provides a location estimate for the causal variant. This is achieved
by exploiting high-resolution linkage disequilibrium (LD) maps in LD Units
(LDU maps) derived using the population-specific and publicly available SNPs
provided by the HapMap Project. All genome-wide significant locations for
T2D were tested for evidence that they confer risk of disease by regulating
gene expression, using fine map genomic and adipose expression data for
healthy European samples (EBI, E-TABM-1140). Using Wellcome Trust Case
Control Consortium (WTCCC) data for T2D, our whole genome analysis has
identified 17 novel gene regions specific to Europeans with genome-wide
significance. None of these signals were identified in African-Americans.
These locations were replicated using independent European Metabochip
data (WTCCC2). The majority of the 17 novel loci showed strong evidence of
being cis-eQTLs, with 11/17 co-locating to within <50kb of variant locations
that regulate neighbouring gene expression in adipose tissue. We conclude
that the integrative multi-marker analysis of GWAS data on T2D with data
on adipose expression profiling has great potential to provide refined location and functional information relating to T2D disease susceptibility.
TCF7L2 in Hypothalamic Neurogenesis in Mice and Men
205‑LB
DONNA M. LEHMAN, LI YAO, YUANHANG LIU, IRISCILLA AYALA, SWETHA MAHESULA, YIDONG CHEN, ERZSEBET KOKOVAY, San Antonio, TX
Growing evidence indicates that adult hypothalamic neurogenesis is necessary for energy homeostasis and is affected by environmental conditions.
Therapeutic interventions upon this process may be beneficial for metabolic
disorders. We are investigating involvement of TCF7L2 isoforms using human
neurons and murine neural stem cells. During murine embryonic development TCF7L2 isoforms expressed in thalamus are 34kD (dominant-negative),
58kD and 75kD (weak). Postnatally, the 34kD form is not expressed. We have
generated human iPS-derived hypothalamic NPY/AgRP neurons, analyzed
longitudinal patterns of normalized gene expression profiles across 6 time
points during development of our human neurons (Days 35-115, embryonicadult) and used cluster analysis to identify potential coordinated expression
patterns. Similar to mouse, we see 34kD, 58kD and weak 75kD TCF7L2 isoforms early and until Day 75. From Day 75-115 (presumed postnatal to adult),
only 58kD and weak 75kD are expressed. A cluster of 268 genes whose expression sharply peaks at Day 75 and then rapidly declines is enriched for
the key GO terms “synapse” and “transmission of nerve impulse” (p=1.1E-7).
Conversely, a cluster of genes whose expression sharply increases from Day
75-95 is enriched for GO terms “actin-myosin filament sliding” (p=4.3E-09)
and “extracellular matrix” (p= 7.6E-07). Several genes in both clusters have
canonical TCF7L2 binding sites. We next conducted siRNA knockdown of TCF7L2 adult isoforms in the human neurons at Day 55 resulting in expression
of only the 34kD form. GO analysis indicated up-regulation of genes involved
in synaptogenesis and neuropeptide release, and down-regulation of genes
involved in myosin networks which in turn affect neuronal migration and
plasticity. Additionally, we isolated adult neural stem cells from the murine
hypothalamus and found very weak expression of the 34kD- but high levels
of the 58kD- and 75kD isoforms of TCF7L2, suggesting that these isoforms
are important in adult hypothalamic neurogenesis as well.
203‑LB
RASGRF1 and IGF2BP2 Confer Pleiotropic Risk of Susceptibility to
Both Type 2 Diabetes and Common Myopia in Europeans
TOBY ANDREW, KRISTAL SHEHATA, WINSTON LAU, NIKOLAS MANIATIS, London, United Kingdom
Diabetic individuals are at increased risk of myopia. However, in the general population the relationship between myopia and subtle dysregulation in
glucose metabolism is unknown. It has been suggested for example, that the
rapid increased incidence of myopia observed in SE Asia - which is correlated
with many aspects of rapid urbanisation - is in part due to the widespread
adoption of a more Westernised, high-glycaemic index diet. We investigated
RASGRF1 (an established gene for myopia) and chromosome 3q26-29 (a genomic region with co-incident replicated linkage for myopia and type 2 diabetes) for evidence of pleiotropic association with common myopia and T2D. We
used population-specific, fine-scale genetic maps derived from high-resolution
HapMap data on Northern-Europeans and phenotype data for 1) type 2 diabetes (T2D) cases and controls from the Wellcome Trust Case Control Consortium, WTCCC1 (Affymetrix 500K SNPs) and WTCCC2 (Illumina MetaboChip
200K targeted SNP array) and 2) TwinsUK/dbGaP myopia samples (accession
phs000142.v1.p1 Illumina Human 610). We found 1) strong evidence of pleiotropic association at RASGRF1 (4e-06) and IGF2BP2 (2e-24). RASGRF1 has been
shown to be associated with retinal photoreceptor function and glucose metabolism. In addition to IGF2BP2 on chromosome 3q26-29, ABCC5, IQCJ and
TBL1XR1 also show evidence of pleiotropy at this locus; 2) there is a statistically significant (p=0.00003), but small phenotypic correlation between myopia and circulating plasma insulin levels in the UK population with evidence
from the twin data that most (approximately 75%) of the covariance between
these two traits is due to shared genetic factors. We conclude that shared
genetic risk factors may contribute common myopia and T2D and that IGFBP2
and RASGRF1 contribute to the (patho)physiology of both conditions with the
potential to provide new aetiological insights.
Supported By: National Institutes of Health (DK047482)
Supported By: UK Medical Research Council (G0901017)
ADA-Funded Research
For author disclosure information, see page LB98.
LB52
Immunology
206‑LB
208‑LB
Diverse Molecular Profiling Maps of Skeletal Muscle Reveal Mech‑
anistic Insights about Type 2 Diabetes
Integrated 3-D Epigenomic and Transcriptomic Analysis of EndoCbetaH1 Human Beta Cells
STEPHEN PARKER, JEROEN HUYGHE, MICHAEL ERDOS, HEIKKI KOISTENEN, PETER CHINES, RYAN WELCH, LAURA SCOTT, D. LELAND TAYLOR, BROOKE WOLFORD, HEATHER STRINGHAM, ANNE JACKSON, ANDREW BECK, HUI JIANG,
XIAOQUAN WEN, NARISU NARISU, TIMO LAKKA, RICHARD M. WATANABE,
KAREN L. MOHLKE, JAAKKO TOUMILEHTO, MICHAEL BOEHNKE, FRANCIS S.
COLLINS, Ann Arbor, MI, Bethesda, MD, Helsinki, Finland, Kuopio, Finland, Los Angeles, CA, Chapel Hill, NC
MICHAEL L. STITZEL, STEPHEN C.J. PARKER, BROOKE N. WOLFORD, XINGWANG
LI, EMALY PIECUCH, ASA THIBODEAU, ELADIO MARQUEZ, OSCAR LUO, MICHAEL ERDOS, DUYGU UCAR, YIJUN RUAN, FRANCIS S. COLLINS, Farmington,
CT, Ann Arbor, MI, Bethesda, MD
Genome-wide association studies (GWAS) and functional (epi)genomic
analyses of human pancreatic islets converged to implicate DNA sequence
variation in islet enhancers in islet dysfunction and type 2 diabetes (T2D). The
target gene(s), direction of effect, and molecular mechanism are unknown
for many T2D and metabolic trait (MT) GWAS SNPs. Integrated genomic,
epigenomic, and transcriptomic approaches offer an opportunity to answer
these questions. EndoC is the first human cell line exhibiting functional beta
cell properties. As such, it is an attractive model to study the molecular genetics and functional (epi)genomics of beta cell physiology and dysfunction.
Here, we combine deep mRNA-seq, epigenomic (ChIP-seq, ATAC-seq) and
3D epigenome (ChIA-PET) analyses with karyotyping and dense genotyping
to understand both general and allele-specific transcriptional regulation in
EndoC-betaH1. Karyotyping indicates that EndoC is a heterogeneous population of cells, with subsets harboring specific translocations. Comparison
of ChIP-seq chromatin states from multiple cell types reveals a striking
similarity between EndoC and human pancreatic islets. In particular, we find
that T2D/MT GWAS SNPs overlap EndoC enhancers. We identify general
(e.g.CTCF) and specific (e.g. PDX1) transcription factor motifs by footprinting
analysis of EndoC ATAC-seq profiles. RNA Pol2 ChIA-PET confirms published,
targeted interactions between ISL1 and multiple enhancers and identifies
~10,000 promoter-promoter, enhancer-enhancer, and enhancer-promoter
interactions genome-wide. Integration of genotyping and -omics datasets
allows us to link allelic biases in enhancers (ChIP-seq, ATAC-seq) and target
gene expression (mRNA-seq) at several sites in the genome, including several identified as T2D/MT risk SNPs and expression quantitative trait loci
(eQTL) SNPs in islets. Together, these data define the transcriptional architecture of EndoC and provide insights into beta cell transcription.
Type 2 diabetes (T2D) results from environmental and genetic factors interacting across time and multiple tissues. More than 90% of >100 variants
associated with T2D and related traits through genome wide association
studies (GWAS) occur in non-coding regions, suggesting a strong regulatory component to disease susceptibility. To understand the full spectrum
of genetic variation and regulatory element usage in T2D-relevant tissue
and across disease progression, the FUSION Study obtained skeletal muscle
biopsies from 278 well-phenotyped Finns with normal or impaired glucose
tolerance or T2D. We performed dense genotyping and imputation and constructed strand-specific mRNA-seq libraries and sequenced a total of 25.3B
fragments (mean 91.3M per sample). We identified >13k genes with expression and/or splicing quantitative trait loci (e/sQTL) (5% FDR). We produced
reference chromatin state maps across 30 cell types and reference transcriptome maps across 16 tissue types. Integrative analyses show that the
genetic regulatory architecture of skeletal muscle specific gene expression
is encoded in skeletal muscle stretch enhancers and not typical enhancers or
stretch enhancers from unrelated tissues. Our eQTL analyses identify target
genes and direction of effect of GWAS-identified T2D and related trait risk
alleles. Some of these genes are significantly differentially expressed, implicating them as key targets for therapeutic development. These rich data enable identification of diverse molecular processes involved in muscle based
insulin resistance, changes in transcription with progression towards T2D,
and reveal mechanistic insights about disease predisposition.
Supported By: American Diabetes Association (1-14-INI-07 to S.P.); National
Institute of Diabetes and Digestive and Kidney Diseases
Supported By: American Diabetes Association (1-14-INI-07 to S.C.J.P.);
4R00DK09225103, Z01HG000024, K99DK099240
209‑LB
Withdrawn
To explore novel genetic contributions toward susceptibility for type 2 diabetes (T2D), we performed a 2-stage GWAS in the Singapore Chinese Health
Study. In stage I, we genotyped 507,509 SNPs in 4678 participants including
2338 incident cases with diagnosed T2D and 2340 matching controls with
HbA1c <6.0% on the Affymetrix ASI SNP array platform. Imputation using
the 1000 genomes project was conducted for replication of known T2D SNPs
and fine-mapping. 73 of 98 known T2D SNPs (p<10-5) from the NHGRI GWAS
Catalog were associated with T2D, 24 were statistically significant (p0.80.
Combining the risk alleles into an unweighted score, we estimated a relative
risk per allele of 1.025 (p=7.5×10-10). In stage II of the GWAS, approximately
3000 SNPs, based on the stage I analysis and next generation sequencing of
+/- 50kb, 39 known T2D sites were genotyped in prevalent cases and matching controls (n=4571) from the Singapore Study. These analyses confirmed
known SNPs and identified potentially new SNPs. Pooled over two stages
we found 12 SNPs of interest after adjustment for age, sex, dialect and BMI.
6 of these were tested for replication in the AGEN consortium of 8 Asian
studies. Two SNPs replicated (p<0.05) and were specific to Asians. One SNP,
located near the PAX4 gene on chromosome 7, remained an independent
novel signal for T2D in Asians (p=0.0003). PAX4 has a critical role in fetal
development and is involved in pancreatic islet development including differentiation of beta cells. In conclusion, we have confirmed numerous known
diabetes-related SNPs in the Singapore Chinese Health Study, and identified
at least one new Asian-specific T2D SNP.
Supported By: Singapore Chinese Health Study
ADA-Funded Research
For author disclosure information, see page LB98.
LB53
POSTERS
Immunology
MYRON GROSS, MARK A. PEREIRA, CHI-YUAN HSU, RENWEI WANG, MARK
SEIELSTAD, KOH WOON PUAY, TEO YIK YING, TAI E. SHYONG, LIU JIANJUN,
HENG KHAI KOON, JIAN-MIN YUAN, REVATI KORATKAR, KENNETH BECKMAN,
NATHAN PANKRATZ, DANIEL O. STRAM, Minneapolis, MN, San Francisco, CA,
Pittsburgh, PA, Singapore, Singapore, Los Angeles, CA
Immunology/
Transplantation
207‑LB
Type 2 Diabetes Susceptibility Loci in the Singapore Chinese Health
Study
Immunology
212‑LB
210‑LB
Anti-paralemmin 2 Antibody as a Novel Antibody for Latent Autoim‑
mune Diabetes in Adults
HCELL Expression on Murine MSC Licenses Pancreatotropism and
Confers Durable Reversal of Autoimmune Diabetes in NOD Mice
MASAHIDE HMAGUCHI, KANAE MATSUSHITA, MASAHIRO YAMAZAKI, TAKUYA
FUKUDA, MICHIAKI FUKUI, NAOTO NAKAMURA, Kyoto, Japan
REZA ABDI, ROBERT SACKSTEIN, ROBERT MOORE, SHINOBU SAKAI, CONOR
BRIAN DONNELLY, MARWAN MOUNAYAR, Boston, MA
Background: The phenotype of latent autoimmune diabetes in adults
(LADA) at early stage is similar to that of type 2 diabetes mellitus in clinical practice. However, it is thought that the ability of insulin secretion from
pancreatic β cells of LADA decreases gradually in months to years. The decrease of β cell might be prevented by the induction of insulin therapy in
LADA. Therefore, it is further necessary to diagnose and treat LADA at an
early stage. Nowadays, islet specific autoantibodies such as anti-glutamic
acid decarboxylase antibody and anti-tyrosine phosphatase-like insulinomaassociated protein 2 antibody have been used for the diagnosis of LADA.
However, there are diabetic patients, in whom autoimmune reaction for β
cell might be exist, but current available islet autoantibodies were not detected. The aim of the study was to detect a novel autoantibody for diagnosing LADA.
Method: We used an unbiased whole autoantibody array to identify novel
islet autoantibodies. We developed the quantitive measurement method for
the identified antibody in sera. We evaluated the diagnostic value of the
novel antibody for diagnosing LADA in the cohort consisted with 152 patients with diabetes mellitus.
Results: Anti-paralemmin2 (PALM2) antibody was identified as a specific
autoantibody for LADA. AUC, the sensitivity, the specificity of anti-PALM2
antibody for diagnosing LADA were 0.644, 70.8%, and 100%, respectively.
The association of the level of anti-PALM2 antibody and the change of serum C-peptide immunoreactivity per year (ng/ml/year) was -0.389 (P<0.001),
although there was no significant association between the change of serum
C-peptide immunoreactivity per year and titer of anti-GAD antibody, antiIA-2 antibody, or anti-ZnT8 antibody.
Conclusion: Anti-PALM2 antibody could be a novel antibody for LADA.
Moreover, the level of anti-PALM2 antibody could predict the decrease of
insulin secretion.
Type 1 diabetes (T1D) is an immune-mediated disease resulting in destruction of insulin-producing pancreatic beta cells. Mesenchymal stem cells
(MSCs) possess potent immunomodulatory properties, garnering increasing
attention as cellular therapy for T1D and other immunologic diseases. However, MSCs generally lack homing molecules, hindering their colonization at
inflammatory sites following intravenous (IV) administration. Here we analyzed whether enforced E-selectin ligand expression on murine MSCs could
impact their effect in reversing hyperglycemia in non-obese diabetic (NOD)
mice. Though murine MSCs natively do not express the E-selectin binding
determinant sialyl Lewisx (sLex), we found that fucosyltransferase-mediated
α (1,3)-exofucosylation of murine MSCs resulted in sLex display uniquely on
cell surface CD44 thereby creating HCELL, the E-selectin-binding glycoform
of CD44. Following IV infusion into diabetic NOD mice, allogeneic HCELL+
MSCs showed 3-fold greater peri-islet infiltrates compared to buffer-treated
(i.e., HCELL-) MSCs, with distribution in proximity to E-selectin-expressing
microvessels. Exofucosylation had no effect on MSC immunosuppressive
capacity in in vitro assays, however, though engraftment was temporary for
both HCELL+ and HCELL- MSCs, administration of HCELL+ MSCs resulted
in durable reversal of hyperglycemia, whereas only transient reversal was
observed following administration of HCELL- MSCs. Notably, exofucosylation of MSCs generated from CD44-/- mice induced prominent membrane
expression of sLex, but IV administration of these MSCs into hyperglycemic
NOD mice showed no enhanced pancreatotropism or reversal of hyperglycemia. These findings provide evidence that glycan engineering to enforce
HCELL expression boosts trafficking of infused MSCs to pancreatic islets of
NOD mice and substantially improves their efficacy in reversing autoimmune
diabetes.
Supported By: American Diabetes Association (1-14-BS-001 to R.A.)
Supported By: AS262Z02103P
211‑LB
Circulating Antibodies against Glycated Serum Albumin in Diabetic
Patients
213‑LB
Identification of Tetraspanin-7 as a Major Target of Autoimmunity
in Type 1 Diabetes
POSTERS
Immunology/
Transplantation
MEYAD A. ALKARNI, Riyadh, Saudi Arabia
The enhanced glycation status of albumin under hyperglycemic conditions
leads to the occurrence of a protein that has reduced beneficial activities
and that exerts new detrimental actions. Glycated albumin (GA) appears to
be an underestimated potential index to fill the gap between self-monitoring
of blood glucose and HbA1c testing in diabetes management. Presence of
circulating antibodie (Abs) against GA will help achieve a better understanding of the impact of albumin glycation in pathological progression. The aim
of this study was to check the presence of Abs against GA in diabetic patients. If yes, to light upon its consequences. Spectrophotometry was used
to measure the changes in the spectral reading of prepared GA and the control albumin every 12 hrs. The significant hypochromicity occurred with the
albumin and glucose concentration of 400mg/100ml after 60hrs of incubation at 37Cº; which means maximum glycation of glucose with albumin had
occurred and this was confirmed by fluorometry which showed significant
quenching after 60hrs. Indirect binding ELISA was done for 120 patient’s serum samples and 40 control samples with the prepared antigen (GA) and the
overall results show significant difference among the patient groups where
the (p-value < 0.05), which mean effective binding of patients sera Abs and
the antigen (GA) was observed almost in all patients as compared to normal
samples. Formation of immune complex between GA and anti-GA Abs in
sera of patients was also confirmed by gel retardation assay and polyacrylamide gel electrophoresis. Results showed high binding between the Abs
in diabetic serum and GA. This further reiterate our contention that protein
modification may render it immunogenic. The binding patterns of diabetic
sera obtained from different patients were remarkably similar in each group,
indicating the recognition of altered confirmation of the modified protein by
circulating antibodies in diabetic patients. Thus, circulating Abs against GA
in diabetic patients were detected.
KERRY A. MCLAUGHLIN, CAROLYN C. RICHARDSON, AARTHI RAVISHANKAR,
RICHARD FELTBOWER, DIANA MORGAN, MICHAEL R. CHRISTIE, London, United
Kingdom, Leeds, United Kingdom
The presence of antibodies to multiple autoantigens confers high risk for
development of type 1 diabetes. Four major autoantigens are established
(insulin, GAD, IA-2 and ZnT8), but the molecular identity of a fifth, bound
by antibodies in 50% of diabetic children and shown only to be a 38 kDa
membrane glycoprotein (GLIMA), is unknown. Antibodies to GLIMA are detectable only by immunoprecipitation from extracts of radiolabelled islet or
neuronal cells followed by SDS-PAGE and autoradiography. The aim of this
study was to identify GLIMA to enable efficient assay of the autoantibodies.
Sera from recent onset type 1 diabetic patients were screened for GLIMA
antibodies using radiolabelled neuronal cells to identify samples with high
GLIMA immunoreactivity. Competition studies with extracts of normal
mouse tissues detected high levels of GLIMA only in islets, brain, pituitary
and lung. Membrane glycoproteins from extracts of mouse brain and lung
were purified by lectin affinity chromatography and separated by SDS-PAGE.
Brain extracts were also immunoprecipitated with sera from GLIMA positive
and negative subjects before SDS-PAGE. Regions of gels equivalent to 38
kDa for each sample were excised and treated with trypsin. Eluted peptides
were subjected to LC-MS/MS and mass data used for protein identification.
Only 3 proteins returned in database searches were detected in samples
from the brain and lung extracts, in the GLIMA antibody positive immunoprecipitate, but not the GLIMA antibody negative immunoprecipitate: actin,
G(i) subunit alpha-2 and tetraspanin-7. Whereas actin and G(i) are widely expressed, tetraspanin-7 is a multipass transmembrane protein with restricted
neuronal and islet expression, similar to GLIMA. GLIMA identity was established by demonstrating binding of tetraspanin-7 to antibodies in GLIMA
positive type 1 diabetic patients’ sera. We identify tetraspanin-7 as a major
target of autoimmunity in diabetes, allowing its exploitation for diabetes
prediction and immunotherapy.
Supported By: King Saud University
Supported By: Diabetes UK (11/0004297)
ADA-Funded Research
For author disclosure information, see page LB98.
LB54
Immunology
214‑LB
(DPP-4) is a cell surface serine protease expressed in a variety of tissue.
Inhibitors of DPP-4 are widely used in treatment of type 2 diabetes mellitus.
Accumulating data suggests that DPP-4 inhibition yields further beneficial
pleiotropic effects, but the exact mechanisms remain poorly elucidated. We
investigated whether the DPP-4 inhibitor sitagliptin affects complement activation by altering the functional activity of the lectin pathway in vitro and
in vivo. The effect of sitagliptin on the mannan-binding lectin (MBL) mediated activation of the complement system was analysed in vitro by quantifying complement protein C4b deposition onto a surface of mannan in a
time-resolved immunofluorometric assay. The effect in vivo was analysed in
plasma samples from 71 patients with acute coronary syndrome and glucose
disturbances in the BEGAMI trial, randomly assigned to sitagliptin 100 mg
(n=34) or placebo (n=37) for 12 weeks. Plasma concentrations of MBL and
levels of C4b deposition were measured at baseline and after 12 weeks of
treatment. In vitro, sitagliptin was found to inhibit the lectin pathway of
the complement system in a dose-dependent manner. 50% reduction in C4b
levels was observed with a concentration of 1 mM sitagliptin as compared
to 0.25 mM Pefabloc (a known inhibitor of the complement system). In vivo,
MBL and C4b declined significantly during 12 weeks of follow-up in both
groups (p < 0.002). The changes in C4b appeared to be driven by changes in
MBL with no significant additional effect of sitagliptin. In conclusion, sitagliptin resulted in reduced functional activity of the lectin pathway in vitro.
The mechanisms behind a potential complement inhibitory effect of sitagliptin in vivo could not be demonstrated in the present material but merits
further investigations.
EMANUELA ZAHARIEVA, ZDRAVKO KAMENOV, ELENA VIKENTIEVA, DORA
POPOVA, Sofia, Bulgaria
Toll-like receptors (TLR) activate Nuclear Factor κB pathway, implicated to
contribute to insulin resistance. This study aimed to determine expression of
TLR 4 and 2 in patients with type 2 diabetes mellitus (DM2), correlate it with
glycemia, body mass index (BMI) and waist circumference, and establish an
association with chronic complications of the disease. We included 28 patients with DM2 and 7 control persons. Multicoloured immunofluorescence
analysis with fluorochrome-conjugated monoclonal antibodies was used to
evaluate the TLR4 and TLR2 expression by classical, intermediate and nonclassical monocytes (Mo). TLR4 expression in diabetic patients is lower, compared to controls (classical - Md=1.6% vs. Md=8.7%; nonclassical - Md=0.6%,
vs. Md=4.0%; intermediate Mo: Md=2.9% vs. Md=16.2%, p<0,05) and TLR2
expression is higher (nonclassical- Md=33.1% vs. Md=12.0%; intermediate
Mo - Md=92.8% vs. Md=29.3%, p<0,05). In men with diabetes (n=10) we found
a positive correlation between TLR4 expression on classical Mo and fasting
plasma glucose, Spearman’s correlation coefficient (Sp.CC) = 0,65, p=0.042 and
also between TLR4 expression on intermediate Mo and HbA1c, Sp.CC =0.693;
p=0.026. TLR2 was not associated with glycemia (p>0,05). Both did not correlate with BMI or waist circumference (p>0,05). TLR4 expression by intermediate Mo decreases with rise of creatinine level in patients with DM2, Sp.CC
rho = -0.38; p = 0.048, and with lowering of estimated glomerular filtration
rate (eGFR) - Sp.CC rho = 0.36; p=0.049. TLR2 expression also decreases with
renal function decline (classical Mo: creatinine - Sp.CC rho = -0.64; p = 0.044;
eGFR - Sp.CC rho=0.79, p=0.007; intermediate Mo - eGFR - Sp.CC rho = 0.64,
p = 0.047). Patients with DM2 have lower expression of TLR4 although it tends
to rise with worsening of glycemia. Expression of TLR2 is higher in diabetic
patients but does not correlate with current or recent glycemia. Both tend to
decrease with progress of diabetic nephropathy, which questions the role of
innate immunity in its early stages.
Supported By: Aarhus University
217‑LB
Methyldopa Blocks HLA-DQ8 Antigen Presentation in Recent Onset
Patients with Type 1 Diabetes (T1D)
Supported By: Medical University-Sofia (83/2013)
Human leukocyte antigen (HLA) alleles confer significant genetic risk for
T1D with recent studies implicating DQ8 in its pathogenesis, making it an important target. DQ8 antigen presentation can be inhibited in animal models
with methyldopa. In this pilot study, we evaluated methyldopa treatment in
10 DQ8 positive T1D subjects, ages 18-46 years (mean 27) with < 2 years of
diabetes duration (mean 3 months). This was an open label phase 1b dose escalation study. All subjects tolerated low (500mg BID) and moderate (500mg
TID) dosages of methyldopa, while 9/10 tolerated the high dose (2-3g/day).
There was a dose dependent reduction in DQ8 stimulated IL-2 T cell response
at 1 (-32%) and 3 weeks (-39%), which returned to normal 6 weeks after
stopping therapy (Fig. 1a). The response was specific as DR4 T cell responses
were minimally effected (Fig. 1b). Patients had good glycemic control and 2
hour AUC for C-peptide following a mixed meal tolerance test at 12 weeks
was similar to baseline levels. No serious adverse events (hypotension,
DKA, or hypoglycemia) were reported throughout the study. We conclude
that methyldopa inhibits DQ8 antigen presentation in T1D. Long-term randomized double-blinded placebo controlled trials are needed to evaluate the
exact role of methyldopa in potentially preventing and/or delaying T1D onset
and preserving residual beta cell function in new-onset T1D.
215‑LB
Withdrawn
216‑LB
Effect of Dipeptidyl Peptidase-4 Inhibition on Complement Activa‑
tion in Diabetes
Supported By: JDRF; 2-SAR-2014-142-C-R
INGEBORG T. HOFFMANN-PETERSEN, JAKOB A. ØSTERGAARD, CHARLOTTE B.
HOLT, CAMILLA HAGE, KERSTIN BRISMAR, LARS RYDÉN, LINDA G. MELLBIN,
STEFFEN THIEL, TROELS K. HANSEN, Aarhus, Denmark, Stockholm, Sweden
Diabetic nephropathy remains the most common cause of end-stage renal
failure. Increasing evidence indicates that adverse activation of the complement system may damage the kidneys in diabetes. Dipeptidyl peptidase-4
ADA-Funded Research
For author disclosure information, see page LB98.
LB55
POSTERS
AARON W. MICHELS, VIRAL SHAH, SARIT POLSKY, KRISTEN MCDANIEL, AIMON
ALKANANI, SATISH K. GARG, PETER A. GOTTLIEB, Aurora, CO
Immunology/
Transplantation
Toll-like Receptors 2 and 4 in Type 2 Diabetes
TransplantationInsulin Action—Adipocyte Biology
218‑LB
tivirus, to overexpress human pancreatic and duodenal homeobox 1 (PDX1),
neurogenin 3 (NGN3) and/or forkhead box A2 (FOXA2). These genes are involved in the development of β-cells and might enhance the reprogramming
of ADSCs into pancreatic endodermal progenitors. Thereafter, multi-step
induction protocols were applied to the cells. Induction of Ins1 expression
was indicated by fluorescence. RNA was isolated from fluorescent cells to
access the expression of pancreatic hormones and other genes essential for
β-cell function by qPCR. We developed several protocols that can induce
fluorescence in up to 20% of the transduced ADSCs. Besides, cells become
cuboidal in morphology and tend to form cell clumps in the protocols using 3-D culture. The positive protocols are able to induce the expression
of pancreatic hormones (insulin and glucagon) in ADSCs that overexpress
PDX1. Co-expressions of FOXA2 and/or NGN3 with PDX1 do not significantly
increase the expression levels. However, their overexpression leads to the
expression of glucokinase (GCK), which is crucial for glucose sensing. Thus
overexpression of PDX1 alone is sufficient to induce the expression of pancreatic hormones, including insulin, in ADSCs treated with reprograming
protocols. Cell morphology and structure can also be used as a gauge of
reprogramming efficiency. While FOXA2 and NGN3 co-expression does not
increase the efficacy of reprogramming, they induce the expression of GCK
potentially enhancing other β-cell functions.
Nasal Administration of Novel Insulin Degrading Enzyme Inhibitor
Ameliorates Autoimmunity in Diabetic Animal Model
DAN FRENKEL, Tel Aviv, Israel
Islet reactive T cells are found in many diabetes patients and in first degree
relatives with a high risk to develop overt diabetes. It was also found that mice
with a high diabetes risk, non-obese diabetic (NOD) mice, routinely target classical islet. Clonally expanded T cells from the site of autoinflammatory in longterm type 1 diabetics, indicates that insulin may be the target antigen causing
autoimmune diabetes. Insulin-degrading enzyme (IDE) is a large zinc-binding
protease plays an important role in degrading insulin. Since its discovery, IDE
is considered as an important therapeutic target in diabetes reasoned that
inhibitors of IDE would be an ideal anti-diabetic therapy, as they would slow
the degradation of insulin. It was report suggest that IDE is a cellular receptor
mediating varicella-zoster virus (VZV) infection and cell-to-cell spreading. Using computational analysis we have developed an IDE inhibitor, ADT, based on
the interaction between IDE to VZV. We discovered that ADT inhibits IDE in a
dose dependent manner (IC50≈80 nM). We aim to investigate the effect of IDE
inhibitor on the development of autoimmunity in diabetes. We found that nasal
ADT21 can ameliorate diabetes in NOD mice and increase blood insulin levels,
thus allowing physiological regulation of blood glucose and insulin levels. Th17
and Th1 population are involved in the pathogenesis of autoimmune diabetes. We discovered a marked reduction in the levels of IL-17 and IFN-gamma
in spleenocytes from ADT treated mice vs. control NOD mice. Furthermore,
ADT21 reduce pro-inflammatory and increase anti-inflammatory response of B
chain peptide positive CD4+ T-cells. Our results suggest that ADT may be use
as therapeutic approach to ameliorate autoimmunity in diabetes.
Supported By: National Medical Research Council of Singapore
221‑LB
Ten-Year Outcomes after Islet Transplantation with the Edmonton
Immunosuppression Protocol in Patients with Type 1 Diabetes
MARIE CHRISTINE VANTYGHEM, JULIE KERR-CONTE, FRANÇOIS PATTOU, Lille,
France
Supported By: ISF
Remarkable short term outcome has been often reported after intraportal
islet transplantation (IT). Here we analyzed the influence of primary graft function (PGF) on 10 years metabolic outcome of IT with the Edmonton protocole in
patients with brittle type 1 diabetes (ITA) or a previous kidney graft (IAK).
Methods: Thirty-three consecutive patients (19 ITA, 14 IAK) received 2
(n=10) or 3 (n=23) infusions of allogenic islets, within a median (IQR) period
of 80 (47-145) days, Immunosuppression was induced with anti IL2rc ab, and
maintained with sirolimus and tacrolimus. PGF was defined as the value of
the Beta score (0 to 8) at 30 days after the last islet infusion, and considered as optimal when ≥7 or suboptimal when ≤6. Patients were regularly
followed up, at least every 6 months, up to 10 years. The proportions of
patients with graft function (fasting c-peptide ≥0.3 ng/L) and insulin independence were estimated with Kaplan-Meier method and compared with
Logrank Mantel-Cox test.
Results: Insulin independence was achieved after IT in 31 patients (94%),
23 (11-46) days after the last infusion. PGF was optimal in 19 patients (56%).
At the time of this report (median follow-up 8.3 years), 7 patients (21%) had
lost graft function, while 11 patients (33%) remained insulin independent for
up to 10 years, with a HbA1c of 5.8% (5.6%-6.4%) at last visit. Overall, the
proportions of patients with graft function and insulin independence were
0.82 [0.63; 0.91, 95% CI] and 0.48 [0.29; 0.64] at 5 years, and 0.76 [0.56; 0.88]
and 0.22 [0.08; 0.41] at 10 years, respectively. These outcomes were similar between ITA and IAK patients, but were significantly better in patients
with optimal vs. suboptimal PGF: 10 years graft function 0.93 [0.59; 0.99] vs.
0.57 [0.28; 0.78] (p<0001); insulin independence 0.34 [0.12; 0.58] vs. 0 [0; 0]
(p<0001).
Conclusion: Our results suggest that the long term outcome of IT depends
in the first place on initial graft function.
Transplantation
219‑LB
PI3Kα and STAT1 Regulate Human Mesenchymal Stem Cell Immune
Polarization
POSTERS
Insulin Action/
Molecular Metabolism
EIRINI KEFALOYIANNI, MARWAN MOUNAYAR, BRIAN SMITH, ZHABIZ SOLHJOU, OMAR H. MAAROUF, JAMIL AZZI, LOLA CHABTINI, PAOLO FIORINA, MOREY KRAUS, ROBERT BRIDDELL, WILLIAM FODOR, ANDREAS HERRLICH, REZA
ABDI, Boston, MA, Cambridge, MA, Hebron, KY, Madison, CT
Due to their potent immunomodulatory function, MSC have become the
focus of attention as a promising cell therapy for the treatment of various
refractory immune-mediated diseases, including type 1 diabetes. MSC response to specific inflammatory cues allows them to switch between a proinflammatory (MSC1) or anti-inflammatory (MSC2) phenotype. Regulatory
mechanisms controlling this switch remain to be defined. One characteristic
feature of MSC2 is their ability to respond to IFNγ with induction of Indoleamine 2, 3-dioxygenase (IDO), representing the key immunoregulatory molecule
released by human MSC. Here we show that STAT1 and PI3Kα pathways
interplay regulates IFNγ-induced IDO production in MSC. Chemical PI3K paninhibition, PI3Kα-specific inhibition or shRNA knockdown diminished IFNγinduced IDO production. This effect involved PI3Kα-mediated upregulation of
STAT1 protein levels and phosphorylation at Ser727. Overexpression of STAT1
or of a constitutively active PI3Kα mutant failed to induce basal IDO production, but shifted MSC into an MSC2-like phenotype by strongly enhancing IDO
production in response to IFNγ as compared to controls. STAT1 overexpression strongly enhanced MSC-mediated T-cell suppression. The same effect
could be induced using short-term pre-treatment of MSC with a chemical inhibitor of the counter player of PI3K, Phosphatase and tensin homolog (PTEN).
Finally, downregulation of STAT1 abrogated the immunosuppressive capacity
of MSC. Our results for the first time identify critical upstream signals for the
induced production of IDO in MSCs that could be manipulated therapeutically
to enhance their immunosuppressive phenotype.
Supported By: ARD
Insulin Action—Adipocyte Biology
222‑LB
Sucrose Non-fermenting Related Kinase Is an Important Regulator
of Adipose Energy Homeostasis
220‑LB
BIN FENG, YAOHUI NIE, PING JIAO, QIN HE, ARTHUR SALOMON, KIRSTEN SIGRIST, HAIYAN XU, Providence, RI
Role of Transcription Factors in Reprogramming Adipose-derived
Mesenchymal Stem Cells into Insulin-Producing Cells
Obesity has become an epidemic disease and a major risk factor for the
development of insulin resistance and type 2 diabetes. Two types of adipose
tissues exist in humans and rodents. White adipose tissue (WAT) is essential
for maintaining whole body energy homeostasis by storing excessive energy
when nutrients are in surplus and releasing free fatty acids as fuels during
energy shortage. Pathological expansion of WAT is the basis for obesity development. WAT derived inflammatory events characterized by macrophage
infiltration in obese state are considered as a causal factor for the development of obesity-related insulin resistance. In contrast, brown adipose tissue
GUODONG LI, CHUI SUN YAP, JONATHAN CALEB QUEK, SHU MENG, THUAN KAI
JELVIN SIM, SAI KIANG LIM, YONG MONG BEE, Singapore, Singapore
Generation of surrogate islet β-cells for transplantation may cure insulindependent diabetes. This study examined the efficacy of overexpressing
transcription factors, involved in pancreatic β-cell development, in the reprogramming of adipose-derived stem cells (ADSCs) into insulin-producing
cells. ADSCs isolated from the MIP-GFP mice that harbour a transgene of
GFP under control of insulin 1 (Ins1) promoter were transduced, using lenADA-Funded Research
For author disclosure information, see page LB98.
LB56
Insulin Action—Adipocyte Biology
(BAT) is a thermogenic organ and can dissipate energy as heat and enhanced
BAT function is desired for treating obesity. We recently identified SNRK as
a potential suppressor of WAT inflammation in response to over-nutrition
as well as a critical factor for adaptive thermogenesis. Our studies demonstrate that SNRK is most abundantly expressed in WAT and BAT, and the
expression levels as well as activities are significantly decreased in both
tissues in obese mice. Global SNRK deficiency is perinatal lethal and pups
can only survive for 1 day. Reduction of SNRK expression induces inflammation in cultured white adipocytes, in WAT of global SNRK heterozygous mice
and in WAT of adipose specific SNRK knockout mice. In BAT, SNRK deficiency
significantly reduces expression of UCP1, decreases mitochondria density,
and significantly reduces oxygen consumption. Furthermore, adipose specific SNRK knockout mice are obese and resistant to β3-adrenergic receptor
agonist-induced weight loss. These results indicate that SNRK is a critical
regulator to integrate nutrient input and metabolism, and SNRK deficiency
leads to WAT inflammation and impaired BAT thermogenesis.
ers. These findings suggest that 1) niacin exerts adiponectin-independent
effects on macrophage recruitment, but not macrophage number, and 2) the
absence of adiponectin alters the effect of niacin on markers of macrophage
polarity, suggesting underlying adiponectin-dependent mechanisms.
225‑LB
Withdrawn
223‑LB
A Novel Lipocalin, LCN14, Ameliorates Hyperglycemia in Diet-in‑
duced Obese Mice via Reducing Glycerol Efflux from Adipose Tis‑
sue
JIMMY TSZ-HANG LEE, ZHE HUANG, KEWU PAN, KAREN S.L. LAM, AIMIN XU,
CHI-MING WONG, Hong Kong, Hong Kong
Adipose tissue is an active endocrine organ that plays important roles
in regulating energy metabolism in various organs, and dysreguation of
adipose tissue-derived hormones may contribute to the pathogenesis of diabetic complications. In this study, we identified a novel adipokine, lipocalin
14 (LCN14), whose circulating level and expression in white adipose tissues
are severely reduced in both diet-induced and genetically diabetic mice. This
study aims to investigate whether over-expression of LCN14 could alleviate
hyperglycemia, glucose intolerance and insulin resistance in obese mice.
Mice (C57/BL6N) were fed with either chow diet (STC) or high-fat diet (HFD)
for 10 weeks, followed by infection with recombinant adeno-associated virus (rAAV) encoding LCN14, or eGFP as a control. Our findings suggest that
over-expressing LCN14 could lead to elevate circulating level of LCN14,
which increase in insulin sensitivity in major metabolic tissues, including
liver, muscle and adipose tissues. Interestingly, over-expressing LCN14 can
also lower serum glycerol level by reducing the glycerol efflux from adipose
tissue, which limited the availability of glycerol for hepatic gluconeogenesis,
and hence reversing hyperglycemia. Collectively, our results provided the
first evidence that LCN14 is a novel adipokine involved in glucose metabolism. The deficiency of LCN14 in diet-induced obese mice may contribute to
the development of hyperglycemia and insulin resistance. LCN14, therefore,
represents a promising molecular target for the development of new tools
for blood-glucose-lowering therapy.
Oncostatin M: Metabolic Friend or Foe?
226‑LB
224‑LB
High-Fat Diet-Induced Adipose Tissue Inflammation Is Attenuated
by Niacin in Both an Adiponectin-Dependent and Independent Man‑
ner
EMILY C. GRAFF, HAN FANG, DESIREE WANDERS, ROBERT L. JUDD, Auburn, AL,
Baton Rouge, LA
Chronic obesity induces adipose tissue inflammation characterized by increased adipose tissue macrophages (ATM) and dysregulation of adipocyte
function. Studies demonstrate that chronic niacin administration attenuates
obesity-induced adipose tissue inflammation and suggest that niacin alters
ATM polarity away from the classic (M1) phenotype. In addition, niacin administration increases tissue and serum adiponectin, an adipokine that promotes an alternative (M2) phenotype. Therefore, the objectives of this study
were to 1) determine if the anti-inflammatory effects of niacin are associated with increased adiponectin concentrations and 2) evaluate the effects
of niacin on markers of adipose tissue inflammation in the absence of adiponectin. Male C57BL/6 mice (wild-type, WT) and adiponectin null mice (Adipoq-/-) were maintained on a control (10% kcal as fat) or high fat diet (HFD;
60% kcal as fat). After 6 weeks, half of the mice from each group received
either vehicle (water) or niacin (360 mg/kg/day) in their drinking water for 5
weeks. Niacin treatment resulted in increased serum adiponectin in chowfed mice only. In adipose tissue of WT and Adipoq-/- mice fed a HFD, there
was increased gene expression of MCP-1 and CD68. In WT and Adipoq-/mice, niacin treatment attenuated HFD-induced increases in MCP-1 but had
no effect on CD68. HFD fed mice had increased gene expression of both M1
and M2 macrophage markers. Treatment with niacin decreased expression
of M2 markers and showed a trend towards decreased M1 markers in the
adipose tissue of WT mice fed a HFD. Interestingly, in HFD fed Adipoq-/mice, niacin significantly increased expression of both M1 and M2 mark-
Supported By: R01DK052968-15
227‑LB
NF-KappaB Inducing Kinase-mediated Adipose Tissue Inflamma‑
tion in Obesity and Type 2 Diabetes
MANDEEP BAJAJ, JONGOH KIM, ABSALON GUTIERREZ, PADMA SATHYANARA­
YANA, LAWRENCE C.B. CHAN, SEAN M. HARTIG, Houston, TX
Adipose tissue inflammation plays a key role in insulin resistance in obesity and type 2 diabetes. Enhanced levels of nuclear factor (NF)-kappaBinducing kinase (NIK), an upstream kinase in the NF-kappaB pathway, have
been implicated in the pathogenesis of chronic inflammation in diabetes.
NF-kappaB-inducing kinase is a member of the MAPK family that plays a
critical role in noncanonical NF-kappaB pathway activation and can act as
a proximal inducer of IKK complex. We have previously shown that prior
treatment of NIK-transfected myotubes with adiponectin completely attenuated NIK-induced increases in NF-kappaB binding and insulin resistance in
vitro. Furthermore, NIK could amplify the inflammatory signal by regulating
Toll-like Receptor 4 (TLR4) expression. We investigated the role of NF-kappaB-inducing kinase in adipose tissue inflammation and insulin resistance
induced by obesity and type 2 diabetes (T2DM). We studied lean nondiabetic
subjects (BMI 23.9±0.5, n=3), obese subjects (BMI 38.2±1.5, n=8), and type
ADA-Funded Research
For author disclosure information, see page LB98.
LB57
POSTERS
IL-6 and CNTF are gp130 cytokines that are well-studied in the context of
metabolic disease states. Another gp130 cytokine, oncostatin M (OSM), has
recently been shown to have some anti-diabetic properties in mice. Published studies from our lab demonstrate that OSM is produced by adipose
tissue (AT) immune cells and is highly induced in murine and human obesity
and type 2 diabetes. Our current studies demonstrate that OSM significantly
decreases insulin action in adipocytes in vitro. Acute and chronic OSM
treatment also induces pro-inflammatory and pro-fibrotic gene expression
in adipocytes. Knockdown of the OSM-specific receptor (OSMRβ) in vitro
confirms that OSMRβ mediates the biological effects of OSM in adipocytes.
These observations suggest that OSM has pro-diabetic effects. We hypothesized that loss of OSM signaling in fat cells may prevent the development
of high-fat diet-induced obesity. To address this hypothesis, we generated
adipocyte-specific OSMRβ knockout mice (OSMRβFKO). To our surprise, the
OSMRβFKO mice are insulin-resistant, which is likely due to an observed
increase in AT OSM that promotes metabolic dysfunction in non-adipocyte
cells in AT. In conclusion, our in vitro and in vivo studies in adipocytes suggest that OSM is a metabolic foe.
Insulin Action/
Molecular Metabolism
CARRIE M. ELKS, RANDALL L. MYNATT, PENG ZHAO, JACQUELINE M. STEPHENS, Baton Rouge, LA
Insulin Action—Adipocyte Biology
230‑LB
2 diabetic subjects (BMI 38.5 ± 2.5, n=5), who underwent subcutaneous adipose tissue biopsies from the lateral thigh. Adipose tissue NIK expression
was increased in obese subjects and type 2 diabetics (p<0.05) compared
with lean subjects. The increase in NIK was associated with an increase
in adipose tissue TLR4 expression in obese and type 2 diabetic subjects
compared to lean subjects (p<0.10) as well as a decrease in adipose tissue adiponectin expression (p<0.05). Plasma adiponectin was decreased in
obese (6.4±0.4 µg/ml, p<0.01) and type 2 diabetic subjects (4.4±0.4 µg/ml,
p<0.05) compared to lean controls (12.4±4.0 µg/ml). These results suggest
that adipose tissue NIK may play a key role in adipose tissue inflammation
in insulin resistant obese and type 2 diabetic subjects in association with
hypoadiponectinemia.
Functional Roles of c-Jun in KLF15-mediated White Adipocyte Dif‑
ferentiation
KYOUNG-JIN OH, ANNA PARK, Daejeon, Republic of Korea
Hyperplasia in adipose tissue plays a critical role in the development of
metabolic disorders such as obesity. Therefore, understanding the process
of adipocyte differentiation and its regulatory mechanisms is critical to
improve several pathological problems caused by excessive fat deposition
and insulin resistance. In this study, we investigated the novel role of c-Jun
in white adipocyte differentiation. Firstly, we generated stable 3T3-L1 cell
lines expressing retroviral control vector or c-Jun. Especially, differentiation
of 3T3-L1 preadipocyte cell line stably expressing c-Jun was significantly
inhibited as shown in the measurement of lipid accumulation using Oil-red O
staining and quantification of mRNA levels of adipocyte-specific markers. To
determine the relationship between c-Jun and markers of adipocyte differentiation, we compared c-Jun and their expression pattern during adipocyte
differentiation. The expression level of c-Jun was peaked at early stage of
white adipocyte differentiation to induce the proliferation of preadipocytes
and was rapidly repressed. Notably, the expression level of KLF15 was increased when there was a decrease in the expression level of c-Jun. Further, c-Jun-expressing 3T3-L1 cell line showed the decreased KLF15 mRNA
level with remarkably reduced mRNA levels of its downstream genes, such
as C/EBPα and PPARγ. In addition, c-Jun inhibited basal and glucocorticoid
receptor(GR)-induced promoter activities of KLF15. Consequentially, these
results strongly suggest that c-Jun inhibits KLF15 at the transcriptional level
to suppress adipocyte differentiation. This study proposes a novel mechanism for regulating adipocyte differentiation, and eventually would provide
clues for treatment of obesity.
Supported By: American Diabetes Association (7-13-TS-04 to M.B.)
228‑LB
Adipocyte Hypertrophy Induces Insulin Resistance Independent of
Inflammation
JAE BUM KIM, Seoul, Republic of Korea
In obesity, adipocyte hypertrophy and pro-inflammatory responses are
closely associated with the development of insulin resistance in adipose tissue. However, it is largely unknown whether adipocyte hypertrophy in the
absence of inflammation is sufficient to induce insulin resistance. Here, we
developed an in vitro model of adipocyte hypertrophy by treating adipocytes
with long-chain fatty acids. Treatment with saturated or monounsaturated
fatty acids resulted in adipocyte hypertrophy, but a pro-inflammatory response was only observed in adipocytes treated with saturated fatty acids.
Regardless of inflammation, hypertrophic adipocytes with unilocular lipid
droplets exhibited impaired insulin-dependent glucose uptake with a defect
in GLUT4 trafficking to the plasma membrane. Moreover, Toll-like receptor
4 mutant mice (C3H/HeJ) with diet-induced obesity were not protected
against insulin resistance, although they were resistant to adipose tissue
inflammation. Together, our in vitro and in vivo data suggest that adipocyte
hypertrophy alone would be sufficient to cause insulin resistance in early
obesity.
231‑LB
Insulin and Nutrients Suppress ATGL-mediated Lipolysis in Adipo‑
cytes via mTORC1, Transcription Factor Egr1, and A Lipid Droplet
Protein FSP27
MANEET SINGH, VISHWAJEET PURI, KONSTANTIN V. KANDROR, Boston, MA
One of the key physiological functions of insulin is to restrain lipolysis in
adipocytes in the post-prandial state. Failure of insulin to suppress lipolysis
has been long considered as a very serious metabolic defect and one of the
most important if not the most important causative factor of insulin resistance and diabetes mellitus. We have found that insulin controls lipolysis via
mTORC1 that represents the central energy and nutrient sensor in the cell.
mTORC1 decreases expression of the rate-limiting lipolytic enzyme, adipose
triglyceride lipase, or ATGL. Importantly, regulation of ATGL expression by
mTORC1 is conserved in evolution from yeast through Drosophila to mammals and thus should be essential for the metabolic control. However, the
mechanism of this regulation remained completely unknown. Using a genetic screen in S.cerevisiae, we have determined that the effect of mTORC1
on the expression of ATGL is mediated by the primary early growth response
transcription factor Egr1. With the help of 35S-labeling, we have found that
mTORC1 activates Egr1 expression at the level of translation via the 4E-BPmediated axis. Knock out of 4E-BP1/2 dramatically increases levels of the
Egr1 protein, suppresses ATGL gene expression, and causes a marked accumulation of triglycerides in the cell. On the contrary, knock down of Egr1 in
in 4E-BP1/2-null cells increases ATGL expression and decreases fat storage.
Unexpectedly, it turns out that the repressor activity of Egr1 toward ATGL
transcription is enhanced by the lipid droplet protein FSP27 (a.k.a. CIDEC)
that interacts with Egr1 and increases its binding to the ATGL promoter. The
analysis of the intracellular localization of FSP27 in human adipocytes reveals that it is localized not only on lipid droplets but is also present in the
cell nucleus. We hypothesize that FSP27 plays a dual role in fat metabolism
as a LD protein and a nuclear regulator of ATGL transcription.
229‑LB
Downregulation of Lipid Synthesis Occurring Early in the Process of
Insulin Resistance in Adipose Tissue
POSTERS
Insulin Action/
Molecular Metabolism
XIANCHAO XIAO, YUJIA LIU, SUYAN TIAN, XIAOKUN GANG, CHENGLIN SUN,
GUIXIA WANG, Changchun, China
Insulin resistance associates closely with obesity, type 2 diabetes mellitus and cardiovascular disease, occurring in liver, muscle and adipose tissue. Till now, mechanisms underlying insulin resistance are still not exactly
known. Besides, metabolic alteration of lipid and glucose are obscure. Purpose of this study was to distinguish gene biomarkers of insulin resistance in
adipose tissue from vast numbers of Gene Expression Omnibus (GEO) profiles
and figure out probable metabolic modification of lipid and glucose. The gene
expression datasets GSE20950 (39 samples) and GSE26637 (10 samples)
were downloaded from GEO. In the preprocess, frozen robust multiarray
analysis (fRMA) were used for background adjustment, normalization and
summarization, then converting CEL raw expression data to gene expression
values. ComBat algorithm was used to combine these two datasets, and
then abandoned probes with expression level standard deviation<0.1. Significance analysis of microarrays applied to identify differentially expressed
genes (DEGs), with false discovery rate (FDR) <0.05. As a result, 386 DEGs
were in insulin resistant group recognized compared to insulin sensitive
group, 56 of which were at lower expression level and 330 of which were
at higher expression level respectively. Bio-information and function in various signaling pathway of each DEG was confirmed in Genecards Database.
The most prominent down-regulated DEGs in insulin resistant adipose tissue were SLC27A2, AGPAT9 and ACACB, proteins expressed by which were
playing important roles in fatty acid transporting into adipocyte, triglyceride
synthesis and fatty acid synthesis. On the contrary, genes related to glucose
metabolism didn’t show any significance. In conclusion, down-regulation of
lipid synthesis is a primary metabolic transformation in non-diabetic insulin
resistant adipose tissue.
Supported By: R01DK052057
FGF-mediated Regulation of Cellular Bioenergetics
232‑LB
FARNAZ SHAMSI, RUIDAN XUE, TIAN LIAN HUANG, MATTEW D. LYNES, C. RONALD KAHN, YU-HUA TSENG, Boston, MA
Supported By: Chinese Society of Endocrinology; National Clinical Research
Center for Metabolic Diseases
Brown adipose tissue (BAT) plays a central role in regulation of energy
expenditure in response to environmental changes, such as cold and diet.
Uncoupling protein 1 (UCP1) is the key mediator of adaptive thermogenesis
through uncoupling oxidative phosphorylation from ATP production and releasing energy as heat. Increasing amount and thermogenic activity of brown
adipose tissue hold great promise for treatment of obesity-related disorders.
To discover protein(s) that can improve energy expenditure through induction
of UCP1 expression, we performed a proprietary high-throughput screen us-
ADA-Funded Research
For author disclosure information, see page LB98.
LB58
Insulin Action—Cellular and Molecular Metabolism
ing a protein library containing more than 5,000 mammalian secreted proteins in an immortalized murine brown preadipocyte cell line. The screen
identified a number of hits that can induce UCP1 mRNA expression in the
committed brown preadipocytes. Among those, we confirmed that an paracrine/autocrine fibroblast growth factor (FGF) could induce UCP1 expression in a time- and dose-dependent manner. In vivo analysis revealed that
this factor was expressed in both brown and white adipose tissue, and its
expression in BAT, subcutaneous WAT (sqWAT) and epididymal WAT (epiWAT) was upregulated by cold exposure. Additionally, FGF treatment led to
marked increase in mitochondrial activity and uncoupled respiration. Interestingly, FGF-dependent induction of UCP1 is not accompanied by enhanced
adipogenic differentiation and lipid accumulation. In conclusion, these data
have introduced a previously unknown paradigm for regulation of energy
expenditure, in which UCP1 expression and mitochondrial activity are dissociated from adipocyte differentiation and lipid accumulation.
sistance (IR) and glucose intolerance, in part, by cross-talk between innate
immune signaling and metabolic insulin signaling. We previously showed
that IRAK-1, downstream from IL-1R/TLRs, phosphorylates IRS-1 at Ser24
to cause IR. Thus, we hypothesize that absence of IRAK-1 opposes IR. Indeed, C57Bl/6J IRAK-1 k/o mice (20 wk) on normal chow had substantially
improved insulin sensitivity (glucose clamp) and glucose tolerance (IPGTT)
when compared with littermate controls (WT mice). When WT mice with
diet-induced obesity (DIO) from high fat diet (HFD; 60% kcal fat; D12492
Research Diets, Inc.) were treated with Metformin (6 wk HFD, then 6 wk
HFD + Metformin (200 mg/kg/d)), we observed comparable body weight
when compared with HFD alone (12 wk) 41 ± 1 vs. 43 ± 1 g; p < 0.2; n = 6).
Interestingly, when treated with metformin, body weight for IRAK-1 k/o mice
was significantly higher than that of WT (45 ± 2 vs. 41 ± 1; p < 0.05) suggesting
that well known effects of metformin to cause weight loss in diabetes was
absent in IRAK-1 k/o mice. As expected, metformin treatment substantially
increased insulin sensitivity in WT mice (QUICKI = 0.227 ± 0.006 vs. 0.254 ±
0.005; p < 0.005; n = 5) and glucose tolerance (IPGTT AUCg = 16700 ± 3400 vs.
22900 ± 2400 (mg/dl)·min, ANOVA for multiple comparison, p < 0.03, n = 5).
Importantly, these anti-diabetic actions of metformin were absent in metformin-treated IRAK-1 k/o mice (QUICKI = 0.234 ± 0.015 vs. 0.239 ± 0.012,
p < 0.4; IPGTT AUCg = 20800 ± 3000 vs. 25000 ± 4500 (mg/dl)·min, ANOVA
for multiple comparison: p < 0.34). Thus, we conclude that IRAK-1 is required
to mediate beneficial metabolic actions of metformin. In future studies we
will elucidate mechanism for IRAK-1 to mediate metabolic actions of metformin. Our results may lead to novel therapeutic drug targets for treatment
of T2DM.
233‑LB
IL-6 Signaling as a Critical Mediator of Healthy Adipose Tissue Ex‑
pansion
THOMAS S. MORLEY, F. THOMAS WUNDERLICH, JENS C. BRÜNING, PHILIPP E.
SCHERER, Dallas, TX, Cologne, Germany
Obesity and the concomitant insulin resistant segment of the population
is still on the rise. Plasma profiling of these individuals has demonstrated
elevated inflammatory cytokines and acute phase reactants. Specifically,
circulating IL-6 levels (an inflammatory cytokine with a plethora of known
activities), is elevated in the obese insulin-resistant population and is reflecting dysfunctional adipose tissue. A systemic elevation of inflammatory factors can induce insulin resistance. Recently however, TNF-alpha
and other inflammatory cytokines have been demonstrated to be of pivotal
importance in the healthy expansion of adipose tissue under high fat diet
(HFD) exposure. To this end, we wished to determine the in vivo role of IL-6
signaling in adipose tissue specifically with respect to the adipose tissue
homeostasis during expansion. Using a doxycycline-inducible system, we
eliminated the IL-6 receptor from adipocytes exclusively in the adult mouse
and subsequently challenged the mice with a high fat diet. HFD feeding
leads to glucose intolerance and additional metabolic dysregulation. These
results substantiate the essential contributions of inflammation in the microenvironment of the adipocyte that allow appropriate remodeling of the
tissue during HFD-induced tissue expansion.
Supported By: American Diabetes Association (1-13-BS-150 to M.J.Q.)
234‑LB
The ER-associated Degradation Adaptor Protein SEL1L Regulates
Body Weight and Glucose Homeostasis in Age-induced Obesity
HAIBO SHA, LING QI, Ithaca, NY
SEL1L is an essential adaptor protein for the E3 ligase HRD1 in the endoplasmic reticulum (ER)-associated degradation (ERAD), a universal quality-control system in the cell. Previously we have shown that mice with
adipocyte-specific SEL1L deficiency (AKO) exhibit postprandial hypertriglyceridemia. Further analyses reveal that SEL1L is indispensable for the secretion
of lipoprotein lipase (LPL), independent of its role in HRD1-mediated ERAD
and ER homeostasis. Here we further characterize AKO mice in chronic ageinduced obesity. Aged AKO mice are resistant to obesity and demonstrate
improved glucose tolerance. Gene expression analyses showed increased
unfolded protein response and autophagy in the white adipose tissue (WAT)
of AKO mice, likely in compensation for the loss of SEL1L-HRD1 arm of ERAD.
The underlying mechanisms and potential roles of SEL1L in energy metabolism and brown adipose tissue are currently under investigation.
Supported By: American Diabetes Association (07-08-JF-47, 1-12-CD-04 to L.Q);
Cornell University
Supported By: American Diabetes Association (1-13-BS-066 to D.A.G.); National
Institutes of Health-National Institute of Diabetes and Digestive and Kidney Diseases (R01DK094004)
Insulin Action—Cellular and Molecular
Metabolism
Partial Recovery of Insulin Secretion in Type 1 Diabetes?
237‑LB
ANDRZEJ S. JANUSZEWSKI, YOON HI CHO, YIK WEN LOH, DAVID O’NEAL, MARIA CRAIG, KIM C. DONAGHUE, ALICIA JENKINS, Camperdown, Australia, Westmead, Australia, Fitzroy, Australia, Sydney, Australia, Oklahoma City, OK
235‑LB
Actions of Metformin to Ameliorate Insulin Resistance and Glucose
Intolerance in Obese Mice Requires IL-1 Receptor Associated Ki‑
nase-1 (IRAK-1)
Type 1 diabetes (T1D) can be associated with low residual insulin production. T1D patients (F/M=198/167), aged 10-80 y, (mean±SD) 30±16 y, T1D
duration 16±12 y and 249 healthy controls (CON) were evaluated in a crosssectional study. HbA1c was 8.4±1.6% and 5.1±0.4% in T1D and CON respectively (p<0.00001). Plasma C-peptide levels were measured by ultra-sensitive
ELISA (Mercodia, Sweden), with a low detection limit of 1.25 pmol/L (0.0038
XIAO JIAN SUN, SOOHYUN PARK KIM, DONGMING ZHANG, LIWU LI, MICHAEL
J. QUON, Baltimore, MD, Blacksburg, VA
Metformin is first-line therapy for T2DM. Chronic inflammation mediated
by pro-inflammatory cytokines and free fatty acids contributes to insulin reADA-Funded Research
For author disclosure information, see page LB98.
LB59
POSTERS
Insulin resistance (IR) plays an important role in the pathogenesis of obesity and type 2 diabetes (T2D); however, the cellular and molecular mechanisms are still poorly understood. White adipose tissues (WAT) are the major
energy storage site and endocrine organs that regulate insulin sensitivity
via the release of adipokines. In obesity, the failure of insulin to suppress
lipolysis in adipose tissue is thought to be a major driver of IR by increasing
the flux of FFAs to liver and skeletal muscle. Recent studies revealed the
important role of de novo lipogenesis-derived bioactive lipids in systemic
insulin sensitivity. However, the importance of each mechanism in the process of T2D, and the molecular basis of AT dysfunction in obesity remains
unclear. The mechanistic target of rapamycin complex 2 (mTORC2) phosphorylates AKT at S473 and this event is thought to be required for full AKT
activity to all of its substrates. However, we recently found that mTORC2
promotes de novo lipogenesis in brown AT via the independence of the classic downstream AKT substrates. To investigate the role of mTORC2 in WAT,
we knocked out rictor (an essential subunit of mTORC2) using adiponectinCre mice (adipo; rictor). Ap2-Cre-mediated rictor gene deletion (AP2; rictor)
had no effect on fat mass, but increased lean tissue mass, suggesting that
mTORC2 in fat controls whole body growth. However, recent studies have
highlighted several caveats associated with using Ap2-Cre. While we find
some partially overlapping phenotypes with the Ap2; rictor mice, the adipo;
rictor mice exhibited many markedly different phenotypes. Adipo; rictor mice
transiently decreases fat mass, but has no significant effect on lean tissue
mass. Rictor loss has no effect muscle insulin sensitivity or glucose tolerance, but dramatically impairs insulin’s ability to suppress hepatic glucose
production suggesting an early defect in fat-liver crosstalk. However, with
age the KO mice become glucose intolerant. Thus, adipose mTORC2 plays a
pivotal role in T2D.
Insulin Action/
Molecular Metabolism
YUEFENG TANG, DAVID A. GUERTIN, Worcester, MA
Supported By: National Institutes of Health (R01DK55758, 1P01DK088761 to
P.E.S.); National Institutes of Health (T32-GM083831 to T.S.M.)
236‑LB
The Role of Adipose Tissue mTORC2 in Regulating Hepatic Insulin
Sensitivity
Insulin Action—Cellular and Molecular Metabolism
ng/mL). Undetectable C-peptide levels were expressed as ¼ of the concentration of the assay’s lowest calibrator as per manufacturer’s instructions
(Technical Note 34-0144). C-peptide in CON and T1D were 547.1±1.2 pmol/L
and 3.6±1.2 pmol/L respectively; p<0.0001. Subjects were divided into cohorts by T1D diagnosis age (≤10, 10 to ≤20 and >20 y) and T1D duration (≤10,
10 to ≤20 and >20 y). C-peptide levels are shown in the Table. Young age diagnosis (≤10 y.o.) was associated with higher rates of undetectable C-peptide,
p<0.0001 vs. combined age T1D diagnosis 10 to ≤20y.o. and >20y.o.
als not treated with lipid lowering medications were studied. Overweight/
obese individuals (BMI>25 kg/m2, n=28) were stratified based on median
glucose infusion rate (GIR) during a hyperinsulinemic-euglycemic clamp, into
insulin-sensitive and insulin-resistant groups (top vs. bottom, OIS and OIR
respectively). Lean insulin-sensitive individuals (n=23) served as a reference
group. Vastus lateralis muscle biopsies and plasma samples were collected.
Lipidomics analysis was performed by liquid chromatography, electrospray
ionization-tandem mass spectrometry. Pathway analysis of gene array
in muscle was performed in a subset (13 lean, 11 OIR, 11 OIS). Lipidomics
analyses of skeletal muscle and plasma revealed distinct signatures of excess weight and insulin resistance. Specifically, in muscle insulin resistance
was characterized by increases in C18:0 sphingolipids, including ceramide,
dihexosylceramide (DHC) and trihexosylceramide (THC), while in plasma increases in diacylglycerol (DAG), triacylglycerol (TAG) and cholesterol ester
(CE) and decreases in lysophosphatidylcholine (LPC) and lysoalkylphosphatidylcholine (LPC(O)) indicated insulin resistance independent of body weight.
An overweight/obesity lipidomic signature was only apparent in plasma and
was predominated by increased TAG and decreased plasmalogen species.
Biological pathways associated with sphingolipid metabolism were up regulated in muscle in OIR vs. OIS. These findings suggest that insulin resistance
and excess body weight exhibit discrete footprints in plasma and may serve
as a useful marker of insulin resistance independent of obesity per se.
Table. C-peptide Levels (Geometrical Mean±SEM, Age, and Gender Adjusted).
Age T1D
n T1D duration % with undetectable C-peptide
diagnosis (yrs)
(yrs)
C-peptide
(pmol/L)
≤10
62
≤10
82
2.2±1.2
≤10
61
10 to ≤20
67
3.5±1.2
≤10
34
>20
56
5.1±1.2 ‡
10 to ≤20
50
≤10
44
2.5±1.2
10 to ≤20
26
10 to ≤20
23
5.2±1.2 ‡
10 to ≤20
38
>20
21
3.1±1.2
>20
39
≤10
10
7.2±1.2
>20
17
10 to ≤20
29
2.2±1.2 ‡
>20
26
>20
31
2.5±1.2 ‡
‡ p<0.05 vs. duration ≤10 in respective age of diagnosis group.
Supported By: Diabetes Australia; Victorian Government
240‑LB
Conclusions In T1D subjects diagnosed in childhood C-peptide levels are
higher with intermediate or long T1D duration. In those diagnosed >20 yrs Cpeptide levels fall with longer T1D duration. Results are supportive of more
complete beta cell loss in younger onset T1D, and potential beta cell regeneration. Longitudinal studies are merited.
GPS2 at the Crossroad of Lipid Metabolism and Inflammation in
Mouse Adipose Tissue
CARLY T. CEDERQUIST, MARIA D. CARDAMONE, CLAUDIA LENTUCCI, VALENTINA PERISSI, Boston, MA
Obesity-associated inflammation is widely recognized as a critical factor
in the development of insulin resistance leading to T2D. However, recent
studies suggest that local recruitment of immune cells to the adipose tissue
may have some unexpected beneficial effects, such as facilitating local tissue remodeling and contributing to the disposal of excess lipids. Thus, the
critical question of whether inhibiting inflammation is a good approach in the
attempt of treating insulin resistance remains unanswered. G-protein pathway suppressor 2 (GPS2) is an inhibitor of non-proteolytic ubiquitin signaling
recently emerged as an important regulator of homeostasis and inflammatory responses in metabolic organs. Previous work from our lab and others
indicates that GPS2 complementary functions in the cytosol and the nucleus
cooperate to inhibit the expression of the pro-inflammatory gene program
under control of JNK and the TNFα signaling pathway, while promoting the
activation of key mediators of the lipolysis pathway. Here, we present the
characterization of GPS2 adipo-specific knockout (GPS2 AKO) and transgenic
(Ap2-GPS2) mouse models confirming the critical role played by GPS2 in
regulating obesity-induced inflammation and lipid metabolism in vivo. Because of increased adipose tissue lipid storage capacity, GPS2 AKO mice
placed under HFD are more obese but metabolically healthier than their wild
type littermates despite the substantial increase in immune cell infiltration
and expression of pro-inflammatory cytokines. Conversely, systemic insulin
sensitivity is not improved in the obese Ap2-GPS2 mice despite inflammation being inhibited in both adipocytes and macrophages. These results indicate that insulin resistance and inflammation are uncoupled in GPS2 mouse
models and suggest that a better understanding of the casual relationship
between obesity, inflammation, and insulin resistance is required for the design of effective therapeutic approaches against T2D.
Supported By: Diabetes Australia
238‑LB
Effect of Berberine on TLR4/IKKβ/NF-κB Signaling Pathways in
Skeletal Muscle of Obese Rats with Insulin Resistance
POSTERS
Insulin Action/
Molecular Metabolism
YIYI ZHANG, LIQIONG HOU, TIEYUN ZHAO, Chengdu, China
Recently it has been found that Berberine can play a role in blood-glucose
lowering and improving insulin resistance. The mechanism by which berberine improve insulin resistance is still not fully understood. We investigated the effect of berberine on the TLR4-IKKβ/NF-κB signaling pathway and
insulin sensitivity in skeletal muscle. Forty Wistar rats were divided into normal-diet control group (NC, n=10) and high fat diet-caused obese group (HF,
n=30). After the obese rats model was established successfully (28 weeks),
the NC group (n=10) and the obese group (HF1, n=10) were sacrificed. The
rest of obese rats were divided randomly into two groups: untreated group
(HF2, n=10) and 200 mg.kg-1.d-1 berberine-intervened group (BBR, n=10).
Two groups were sacrificed after intervening eight weeks. The expression
of Toll-like receptor-4 (TLR-4) mRNA in skeletal muscle were detected by
real time quantitative PCR. The expression of TLR-4, IκB kinaseβ (IKKβ),
phospho-IKKβ, Nuclear factor-κB (NF-κB), insulin receptor (IR), insulin receptor substrate-1 (IRS-1), phospho-IRS-1 and the tyrosine phosphorylation
of IR and IRS-1 protein in skeletal muscle were detected by Western blotting.
The results showed: 1. The mRNA and protein expression of TLR-4, phosphoIKKβ (Ser181), NF-κB increased significantly and the protein expression of
IRS-1, phospho-IRS-1 and the tyrosine phosphorylation of IR and IRS-1 protein of skeletal muscle decreased significantly in HF1 group compared with
those in NC group (all P<0.05). 2. The mRNA and protein expression of TLR4, phospho- IKKβ (Ser181), NF-κB decreased significantly and the protein
expression of IRS-1, phospho-IRS-1 and the tyrosine phosphorylation of IR
and IRS-1 protein of skeletal muscle increased significantly in BBR group
compared with those in HF2 group (all P<0.05). Our study revealed that berberine can improve insulin resistance of skeletal muscle through inhibiting
the active of the TLR4/IKKβ/NF-κB signaling pathway.
Supported By: Boston Nutrition Obesity Research Center; National Institutes of
Health (R01DK100422)
241‑LB
High-Resolution Plasma Metabolomics during Treatment of Dia‑
betic Ketoacidosis
FRANCISCO J. PASQUEL, KARAN UPPAL, J. SONYA HAW, PRIYATHAMA VEL­L ANKI,
THOMAS R. ZIEGLER, DEAN P. JONES, GUILLERMO E. UMPIERREZ, Atlanta, GA
239‑LB
Diabetic ketoacidosis (DKA) is a disorder affecting carbohydrate, fat, and
protein metabolism. High-resolution metabolomics (HRM), a new approach
to characterize metabolism with advanced liquid chromatography-mass
spectrometry (LC-MS) and data extraction methods, provides information
on thousands of known, as well as uncharacterized metabolites in human
plasma. In the present study, more than 8,000 metabolites were evaluated
in 29 adult patients with DKA. Plasma samples collected at baseline, 4 hours
after insulin infusion, and at resolution of acid-base disorder were analyzed
by HRM. Patient characteristics were as follows: 40±12 years, 62% male,
BMI 29±9 kg/m2, HbA1c 12.0±2.5%; at baseline, BG was 510±123 mg/dL,
pH 7.1 ±0.2, beta-hydroxybutyrate 7.9±3.1 mg/dL, HCO3 12.8±4.6; at DKA
Skeletal Muscle and Plasma Lipidomics Reveal Distinct Signatures
of Overweight/Obesity and Insulin Resistance in Humans
DORIT SAMOCHA-BONET, KATHERINE TONKS, ADELLE C.F. COSTER, MICHAEL
J. CHRISTOPHER, AIMIN XU, DON J. CHISHOLM, RIMA CHAUDHURI, DAVID E.
JAMES, PETER J. MEIKLE, JERRY R. GREENFIELD, Sydney, Australia, Melbourne,
Australia, Hong Kong, Hong Kong
Alterations in lipid species in muscle and plasma have been documented in
insulin-resistant obese individuals and are suggested to contribute to insulin
resistance. Whether these lipid alterations are a reflection of insulin resistance or obesity per se remains unclear. Non-diabetic sedentary individuADA-Funded Research
For author disclosure information, see page LB98.
LB60
Insulin Action—Glucose Transport and Insulin Resistance In Vitro
resolution: BG 161±60mg/dL, pH 7.33±0.03, HCO3 19.8±3.2. A total of 369
metabolites significantly differed from baseline values over time, p<0.05.
Pathway enrichment analysis showed significant changes in amino acid
metabolism (lysine, valine, leucine and isoleucine, tyrosine, and selenomethionine), B vitamin (cobalamine and pyridoxine), nucleotide (pyrimidine and
purine), and lipid (leukotriene, sterol, vitamin A) metabolism. Abundance of
Apelin-13, an adipokine involved in energy metabolism, decreased significantly during treatment. These results show complex metabolic responses
to insulin during DKA treatment. Future studies will require determination
of specific metabolites of most interest and additional investigation of the
clinical/metabolic importance of the changes in specific metabolic pathways
and their association with DKA treatment and it’s resolution.
244‑LB
Torin1 Initiates Autophagy in Cardiomyocytes in an mTOR-indepen‑
dent Manner
QUANJIANG ZHANG, E. DALE ABEL, Iowa City, IA
Phosphorylation of ULK1 by mTOR inhibits autophagy, a lysosomal-dependent process. Torin1 a potent mTOR inhibitor may induce autophagy in
concert with reduced phosphorylation of ULK1. This study initially sought to
confirm that Torin1 may initiate autophagy by inhibiting mTOR in H9C2 cells.
H9C2 cells were treated with Torin1 for 2 hrs under either nutrient replete
(NR, DMEM+10% FBS) or nutrient deplete (ND, glucose-free HBSS+0.5 mM
pyruvate). Torin1 dose-dependently deactivated mTOR and Akt signaling
as shown by dephosphorylation of mTOR at S2448, P70S6K at T389, Akt
at S473 and T308, and GSK3β at S9 (P<0.05, n≥8), without any effects on
ERK1/2 phosphorylation (P>0.05, n≥8). Torin1 increased ULK1 expression by
>3 fold, dephosphorylated ULK1 at both S757 and S555 (P<0.05, n≥8), and induced autophagy as shown by increased LC3-II content in NR (P<0.05, n≥8).
Torin1 did not significantly augment ND-induced autophagy as determined
by LC3-II content and degradation of p62 and NBR1 (P>0.05, n≥8). Insulin at
100 nM increased phosphorylated Akt and mTOR, and inhibited autophagy
in ND media (P<0.05, n≥10), which was blocked by Torin1 (P<0.05, n≥10). To
test whether Torin1-induced autophagy requires mTOR signaling, mTOR was
silenced by ~80%. Silencing mTOR neither initiated autophagy in NR condition, nor augmented ND-induced autophagy. Unexpectedly, Torin1 still induced autophagy in the absence of mTOR as shown by increased LC3-II level
and degradation of p62 (P<0.05, n≥8), in concert with reduced phosphorylation of Akt. These data show that Torin1 may increase autophagic flux in a
mTOR-independent manner, and supports our earlier observations that mTOR
might be dispensable in ND-induced autophagy in cardiomyocytes.
242‑LB
TYLER J. BREHM, WEI YING, BEIYAN ZHOU, JING XU, College Station, TX
Under obese stress, adipose tissue macrophages (ATMs) undergo a phenotypic switch from anti-inflammatory status (M2) to proinflammatory (M1)
status, a major contributor to the development of chronic tissue inflammation
and insulin resistance which are causal factors for type 2 diabetes. However,
the mechanisms underlying the control of macrophage activation statuses
have not been fully elucidated. In this study, we demonstrate that interferon
regulatory factor 6 (IRF6) exerts a profound impact on macrophage polarization. Interestingly, we observed that the expression of IRF6 was dramatically
suppressed in M2 macrophages upon IL4 stimulation, but not in LPS-activated M1 macrophages, as compared to naive (M0) macrophages. In addition,
IRF6 expression differs distinctly between lean and obese ATMs. We further
investigated the role of IRF6 using gain and loss of function strategies in a
well-defined in vitro system. Knockdown of IRF6 with a gene-specific shRNA
successfully suppressed IRF6 expression level in macrophages. Interestingly, significantly enhanced M2 responses were demonstrated by elevated
levels of the activation-related cell surface markers CD69 and CD86 and
the expression of M2-related genes including IRF4, PPARγ, Arginase1, and
IL10. Conversely, bone marrow derived macrophages (BMDMs) with ectopic
expression of IRF6 displayed blunted M2 responses in the presence of IL4,
compared to the M2 BMDMs transfected with an empty vector. In addition,
the gain or loss of IRF6 expression did not significantly affect M1 responses
of BMDMs upon LPS stimulation, suggesting the regulatory effect of IRF6
primarily acts on enhancing macrophage alternative activation. In summary,
our findings identified a novel transcription factor, IRF6, in mediating macrophage alternative activation program. Further analysis of IRF6 will provide
crucial information to understand the ATM action and their contribution to
adipose tissue function and subsequent obesity-induced chronic inflammation and insulin resistance.
Supported By: National Institutes of Health
Insulin Action—Glucose Transport and
Insulin Resistance In Vitro
245‑LB
Supported By: American Diabetes Association (1-13-JF-59 to B.Z.)
HAIYAN WANG, NAVEEN SHARMA, EDWARD B. ARIAS, GREG CARTEE, Ann Arbor, MI, Mount Pleasant, MI
243‑LB
Exercise and calorie restriction (CR) are widely used with the goal of improving insulin sensitivity in older, insulin resistant individuals, but the benefits of combining these treatments on muscle insulin signaling and action
remain poorly understood. Accordingly, we assessed the independent and
combined effects of acute exercise (3-4 hours after an exercise protocol previously demonstrated to increase insulin-stimulated glucose uptake, ISGU, in
24 mo-old rats) and chronic CR (65% of ad libitum, AL, intake beginning at 14
wk-old) on insulin signaling and ISGU in soleus of 30 mo-old rats. Soleus muscle strips, after ex vivo incubation with [3H]-2-D-deoxyglucose (2-DG) ±0.6
nM insulin, were analyzed for [3H]-2-DG accumulation (by scintillation counting) and abundance and phosphorylation of key proteins (by immunoblotting).
CR alone versus AL sedentary controls induced greater ISGU concomitant
with diet-related (CR > AL) elevations in insulin-stimulated phosphorylation
of AktSer473, AktThr308 and Akt substrate of 160 kDa (AS160) Ser588. CR
alone did not increase GLUT4 abundance or insulin-stimulated phosphorylation of the insulin receptor Tyr1146 and AS160 Thr642. Exercise alone did not
alter ISGU, GLUT4 abundance or insulin-stimulated phosphorylation of the
insulin receptor, Akt or AS160. Although CR combined with exercise versus
CR or exercise alone increased GLUT4 abundance and insulin-stimulated AktSer473 and AktThr308 phosphorylation, it did not induce further elevation
of ISGU or insulin-stimulated insulin receptor and AS160 phosphorylation
versus CR alone. These results revealed that although the soleus muscles of
old rats were highly responsive to a CR-induced enhancement of insulin signaling and action, an exercise protocol previously demonstrated to enhance
ISGU in younger rats was ineffective for increasing ISGU, either alone or
when combined with CR.
A Novel Lipid Class Improves Glucose Homeostasis through GLP-1
Receptor-Dependent and Independent Mechanisms
ISMAIL SYED, JENNIFER LEE, ALEXANDRA SONTHEIMER, PRATIK ARYAL, MARK
M. YORE, ODILE D. PERONI, MATTHEW J. KOLAR, ALAN SAGHATELIAN, BARBARA B. KAHN, Boston, MA, La Jolla, CA
Increased adipose tissue (AT) lipogenesis is associated with enhanced
insulin sensitivity but the mechanisms are unknown. Recently we discovered a novel class of endogenous anti-diabetic and anti-inflammatory lipids,
branched Fatty Acid Esters of Hydroxy Fatty Acids (FAHFAs). One FAHFA
family member, Palmitic Acid Hydroxy Stearic Acid (PAHSA), is present in
serum and nearly all tissues with highest expression in AT. PAHSAs are regulated by fasting-refeeding and high fat diet-induced obesity. PAHSAs are
reduced ~70% in AT of insulin-resistant vs. insulin-sensitive people and correlate highly with insulin sensitivity measured by euglycemic clamp. PAHSAs
improve glucose tolerance but effects on insulin sensitivity are unknown.
Aim: to determine whether PAHSA treatment improves insulin sensitivity
and if so, by what mechanism. There are multiple PAHSA isomers defined by
the position of the ester bond. Administration of 5- and 9-PAHSA by osmotic
pump in chow-fed mice for 7-8 weeks elevated serum levels of these lipids
2-3 fold. This improved insulin sensitivity (insulin tolerance test area above
curve: vehicle 4482 ± 961 vs. PAHSA 7106 ± 488) with no change in body
weight or food intake. PAHSA administration also improved glucose tolerance and augmented secretion of both insulin (vehicle 1.2 ± 0.3 vs. PAHSA
3.4 ± 0.6 ng/ml) and total GLP-1 (vehicle 17.07 ± 1.1 vs. PAHSA 24.52 ± 1.7 pM)
during GTT. The GLP-1 receptor antagonist, Exendin-(9-39) (5µg/mouse daily
X 14 days) reversed the PAHSA effects on insulin and total GLP-1 secretion
and glucose tolerance but not on insulin sensitivity. In summary, chronic administration of 5- and 9-PAHSA improves glucose tolerance through a GLP-1
Supported By: National Institutes of Health (AG-010026)
ADA-Funded Research
For author disclosure information, see page LB98.
LB61
POSTERS
Independent and Combined Effects of Calorie Restriction and Exer‑
cise on Insulin-stimulated Glucose Uptake and Insulin Signaling in
the Soleus of Old, Insulin-Resistant Rats
Insulin Action/
Molecular Metabolism
IRF6 Controls Macrophage Alternative Activation
receptor-dependent mechanism and insulin sensitivity through a separate
mechanism. Thus, PAHSAs exert beneficial effects through multiple pathways. Restoring the low PAHSA levels in people with type 2 diabetes is
likely to improve insulin and GLP1 secretion, insulin sensitivity and blood
glucose control.
Insulin Action—Signal Transduction, Insulin, and Other Hormones
Insulin Action—Signal Transduction,
Insulin, and Other Hormones
248‑LB
SORCS1 and SORCS3 Cooperate in Regulation of Glucose Homeo‑
stasis
AYGUL SUBKHANGULOVA, THOMAS WILLNOW, Berlin, Germany
246‑LB
SORCS1 and SORCS3 are members of the VPS10P-domain receptor family,
a group of endocytic and sorting receptors genetically implicated in Alzheimer’s disease (Reitz et al., 2013). SORCS1 is also genetically associated with
diabetes in humans and mouse models, and was recently shown to have a
function in insulin granule replenishment (Kebede et al., 2014). Based on the
close structural similarity of SORCS1 and SORCS3, we investigated possible
redundant functions of both proteins in control of glucose metabolism in a
novel mouse model with combined deficiency for Sorcs1 and Sorcs3. Our initial analysis documented an aggravation of phenotypes in the double mutant
line as compared to the Sorcs1 or Sorcs3 single mutant lines with glucose
intolerance in young mice (10 weeks of age), even when fed a normal chow.
In addition, Sorcs1/3-/- females showed an overall reduction in body weight,
albeit at an increased fat mass. Circulating levels of hormones (insulin, Cpeptide, leptin, glucagon) were not different between Sorcs1/3-/- mice and
their wild-type littermates. Since the brain is the main site of co-expression
of SORCS1 and 3, we currently explore a function for both proteins in central
control of energy homeostasis.
Effect of the Long-Acting Insulin Analogs Glargine and Degludec on
Cardiac Cell Signaling and Function
THORSTEN HARTMANN, NINA WRONKOWITZ, SABRINA GREULICH, MARGRIET
OUWENS, PAULUS WOHLFART, NORBERT TENNAGELS, JUERGEN ECKEL, Düsseldorf, Germany, Frankfurt, Germany
One important aspect for the long-term use of insulin analogs is cardiovascular safety data. Insulin glargine has proven to be safe in the cardiovascular outcome ORIGIN trial, while for insulin degludec (IDeg) the outcome
trial DEVOTE is ongoing. The aim of this study was to investigate insulin
glargine (IGla), its active metabolite M1 (IGlaM1) and IDeg on signaling and
contractility in three preclinical cardiovascular cellular models. In mouse
HL-1 cardiomyocytes, IDeg stimulation results in a lower Akt (Ser473) phosphorylation compared with insulin IGla and IGlaM1 after 5- and 10-min incubation. After 60-min treatment the phosphorylation was comparable to
insulin and IGlaM1. In freshly isolated adult rat ventricular cardiomyocytes
(ARVM), we observed similar increases in Akt (Ser473) phosphorylation with
insulin, IGlaM1 and IDeg after a single time point (10 min). Incubation of electrically paced ARVM with the different analogs resulted for all insulins in a
significantly increased sarcomere shortening and similarly increased contractility and relaxation velocities. The positive inotropic effect of all insulins
could be abrogated by the specific Akt inhibitor triciribine. In iPS-derived
human Cor.4U cardiomyocytes, cell viability and beating rate was monitored
with an impedance- based device up to 24 h. All insulins displayed no obvious cardio-toxicity and slightly increased the rate of spontaneous beating
1.1-1.2-fold. In conclusion, we characterized for the first time the efficacy
and safety of IGla, its metabolite M1 and IDeg, and demonstrated similar
efficacy under steady-state-conditions compared with regular insulin. In HL1 cardiomyocytes, IDeg exhibited a slower on-set of action on Akt (Ser473)
phosphorylation. Investigation may be needed to determine whether the observed kinetic difference plays a role in more complex tissue models.
249‑LB
Insulin Increases Cerebral Blood Flow in Regions Involved in Hu‑
man Feeding and Executive Function
LISA PARIKH, RENATA BELFORT DE AGUIAR, CHERYL LACADIE, DONGJU SEO,
SARITA NAIK, JANICE J. HWANG, RAJITA SINHA, R. TODD CONSTABLE, ROBERT
S. SHERWIN, New Haven, CT
Insulin’s effect on human brain activity as measured by cerebral blood
flow (CBF) remains unclear. Previous animal studies have shown an increase
in CBF with insulin administration. Human studies using positron emission
tomography detected no change in CBF after intravenous (IV) insulin infusion, while intranasal insulin increased insular cortex blood flow. To further
evaluate the effect of IV insulin on CBF, we used functional MRI (fMRI) with
pulsed arterial spin labeling to identify region-specific changes in CBF in
humans. Sixteen healthy participants (INS group: age 29+/- 8 years, BMI
24 +/- 2 kg/m2, HbA1c 5.4 +/- 0.3, weight 68 +/- 10 kg) underwent a hyperinsulinemic-euglycemic clamp during an fMRI scan. They were compared to
a control group of 16 subjects (CON group: age 28 +/- 8 years, BMI 22 +/- 2
kg/m2, HbA1c 5.1 +/- 0.3, weight 64 +/- 8 kg) that received an IV saline infusion during an fMRI scan. Cerebral blood flow was measured approximately
40 minutes after the infusion onset. Plasma glucose, insulin, and counterregulatory hormones were measured throughout both studies. At the time
of CBF measurement, plasma insulin significantly differed between both
groups (INS group: 152 +/- 40 microunits/mL and the CON group: 13 +/- 10
microunits/mL). There was a greater decline in glucagon in the INS vs. CON
group (p=0.05). Other counterregulatory hormones did not differ. CBF was
greater in the anterior cingulate gyrus, left and right putamen, and medial
frontal cortex in the INS group compared to CON group. This study shows
that elevations in circulating insulin increase CBF in a variety of brain regions
that are involved in reward, learning, executive functioning, and eating behavior. Thus, blood flow may serve as a potential biomarker of insulin’s effect
on brain activity.
Supported By: Sanofi-Aventis Deutschland GmbH
247‑LB
Identification of PP1α as an S/T-Phosphatase that Regulates AS160
Dephosphorylation in Skeletal Muscle
POSTERS
Insulin Action/
Molecular Metabolism
PRAGYA SHARMA, GREG CARTEE, Ann Arbor, MI
Akt substrate of 160 kDa (AS160; also known as TBC1D4) is a Rab GTPase
activating protein and a key regulator of insulin-stimulated GLUT4 translocation and glucose transport in skeletal muscle. Akt’s phosphorylation of
AS160 on T642 and S588 is essential for insulin’s full effect on glucose
transport. However, phosphorylation status of proteins depends on the balance of actions by kinases and phosphatases, and the specific S/T-protein
phosphatase(s) controlling AS160 dephosphorylation is (are) unknown. Accordingly, we assessed possible roles of highly expressed skeletal muscle
S/T-phosphatases (PP1, PP2A, PP2B and PP2C) on AS160 dephosphorylation.
Preliminary screening of the candidate phosphatases used an AS160 dephosphorylation assay: lysates from insulin-stimulated rat skeletal muscle
underwent a time-course incubation with several chemical phosphatase
inhibitors, followed by S588 and T642 dephosphorylation rates determined
with AS160 phosphosite-specific antibodies. PP2B and PP2C inhibitors had
no effect on either site, but okadaic acid (which at low doses inhibits PP2A,
and at high doses inhibits PP1) had dose-dependent effects (high > low dose)
on both sites. Immunoprecipitation (IP) with anti-AS160 followed by immunoblotting with antibodies against PP1 isoforms (α, β and γ) and PP2A
revealed only PP1α co-immunoprecipitated with AS160. We next performed
a dephosphorylation assay using recombinant inhibitor 2 protein (a selective
PP1 inhibitor) and found delayed dephosphorylation on both sites. Subsequently, using L6 myocytes we performed co-IP analysis, and found specific
AS160-association with PP1α, but not PP1β, PP1γ or PP2A. Finally, we used
siRNA to selectively deplete each PP1 isoform and found that knockdown
of PP1α, but not PP1β and PP1γ, caused greater AS160 phosphorylation in
insulin-stimulated L6 cells. In summary, the current study provided multiple
lines of novel evidence that PP1α regulates AS160 dephosphorylation in
skeletal muscle.
250‑LB
CD36 Mediates the Effects of Saturated and Unsaturated Fatty Ac‑
ids on Insulin Sensitivity by Direct Interaction with Insulin Receptor
Signaling Complex
DMITRI SAMOVSKI, SINJU SUNDARESAN, MEGHAN LAM, XIONG SU, NADA
ABUMRAD, St. Louis, MO
Elevated concentrations of saturated fatty acids (SFA) in plasma are associated with insulin resistance in skeletal muscle and the development of
type 2 diabetes, while the increase in circulating polyunsaturated fatty acids
(PUFA) is thought to improve insulin sensitivity and metabolic function. While
several mechanisms were proposed to explain the role of SFA in the impairment of insulin signal transduction, the underlying molecular mechanisms
that allow the discrimination between the SFA and PUFA and directly link
them to regulation of insulin sensitivity have not been elucidated. Our recent
findings identify CD36 as a key regulator of signal transduction by fatty acids
(FA). We show by co-immunoprecipitation experiments in cultured myotubes
that CD36 is directly involved in formation of membrane protein complexes
consisting of CD36, insulin receptor, Fyn kinase, c-Cbl and PI3 kinase. Binding
of saturated FA to CD36 resulted in acute (within 15 min) dissociation of the
CD36/Fyn/c-Cbl/PI3K signaling complexes and suppressed insulin-induced
Supported By: National Institutes of Health (DK071771)
ADA-Funded Research
For author disclosure information, see page LB98.
LB62
Integrated Physiology—Insulin Secretion In Vivo
253‑LB
Akt activation. Conversely, binding of PUFA to CD36 augmented the formation of the signaling complexes and enhanced insulin-induced Akt activation.
The effects of both SFA and PUFA were abolished in CD36-defeicent cells,
suggesting the direct role of CD36 in regulation of PI3K signaling pathway.
Insulin-induced activation of PI3K/Akt signaling was increased in skeletal
muscle of CD36 -/- mice, suggesting that CD36 is involved in regulation of
insulin signal transduction in-vivo. Together, our findings document a novel
role for CD36 as an FA receptor that accounts for the different effects of SFA
and PUFA on insulin signal transduction. We postulate that the persistent
elevation in circulating SFA would suppress insulin signaling through CD36,
while the increase in PUFA binding to CD36 would negate the negative effects of SFA and enhance insulin sensitivity.
Outpatient Beta Cell Function (BCF) Testing Yields Comparable
Within-Subject Variability to Inpatient BCF Testing
DOUGLAS S. LEE, MARIA T. VASSILEVA, MYRLENE STATEN, SUDHA S. SHAN­
KAR, R. PAUL ROBERTSON, RALPH RAYMOND, ROBERTO A. CALLE, DAVID A.
FRYBURG, FOR THE FOUNDATION FOR NIH BETA CELL PROJECT TEAM, Cambridge, MA, Bethesda, MD, Indianapolis, IN, Seattle, WA, Skillman, NJ, East Lyme,
CT
Prevailing practice to minimize variability in BCF testing is to admit subjects as inpatients (IP) to ensure subjects have fasted and rested overnight
prior to study. However, this is a burden on subjects, requires housing, and
adds cost. Previous results from this group reported the repeatability (indexed by within subject coefficient of variation (WSCV)) of a mixed meal
tolerance test (MMTT) and arginine stimulation test (AST) in IP subjects with
T2DM. We performed the present study to assess outpatient (OP) WSCV
and compare with earlier IP results. To do so, we assessed MMTT and AST
WSCV in a different cohort of 20 OP, overnight fasted, T2DM subjects who
had 2 MMTTs and 2 ASTs. We then compared WSCV of BCF tests in OP vs.
IP. For AST, acute insulin response to arg (AIRarg) was determined in first 5
min post Arg (5 gm IV) followed by a 60 min infusion of glucose and repeat
injection of Arg (AIRargMAX). Insulin secretory reserve (ISR)=AIRargMAXAIRarg. For MMTT, a standardized 470kCal meal was used. MMTT parameters include insulin sensitivity (Si); insulin release (Φtot); and disposition
index (DItot (=Si* Φtot)). Table shows OP (and IP for comparison) parameter
geometric mean and CV values. OP WSCV, the key measure, was similar to
IP WSCV for each parameter.
Conclusion: These BCF measures can be used for repeat testing as OP and
not require IP admission.
Table.
Integrated Physiology—Insulin Secretion
In Vivo
251‑LB
Characterization of GPR40 Knockout Rats Generated by Zinc Finger
Nucleases
JIN SHANG, MYUNG SHIN, YUE FENG, SHENG-PING WANG, XIAODONG YANG,
JULIE LAO, NINA LI, JOHN MUDGETT, LIANGSU WANG, ANDREW HOWARD,
Kenilworth, NJ
GPR40, a fatty acid sensing G protein coupled receptor, has emerged as a
promising target for type 2 diabetes. Using the zinc finger nuclease technology, we created a Wistar-Hans rat model lacking GPR40 protein. The knockout
rat carries a small deletion and insertion with a stop codon, resulting in the
premature truncation of the GPR40 protein at the region of TM2. To confirm
that the knockout rat is devoid of GPR40 activity, IPGTT was performed with
a GPR40 selective agonist. Significant reduction in glucose excursion was
observed in wild-type littermate rats but not in the homozygous knockout
rats. We further examined pancreatic islets isolated from both knockout and
wild-type rats. The effect on enhancing glucose-dependent insulin secretion
by a GPR40 selective agonist was seen in the islets isolated from wild-type
but not from the GPR40 knockout rats. Gene expression analysis confirmed
that the targeted deletion region of GPR40 was not expressed in islets.
Further, the mRNA expression levels of insulin, GLP-1R or GPR120 were not
altered in the islets of GPR40 knockout rats. The Glucose, lipid and energy
homeostasis in homozygous GPR40 null rats was characterized in comparison with wild type littermate controls with either chow or high-fat diet
feeding. Taken together, our studies demonstrate that the ZFN-generated
GPR40-/- rat will be a valuable tool for investigating GPR40 biology, and for
determining whether beneficial effects as well as safety liability mediated
by GPR40 agonists are mechanism-based.
Supported By: Foundation for the National Institutes of Health Biomarkers
Consortium
252‑LB
Long-Term Regulation of Glycemia in Rhesus Monkeys on Caloric
Restriction or Eating Ad Libitum
254‑LB
A New Model-Based Method for Estimating Hepatic and Peripheral
Insulin Clearance from Intravenous Glucose Tolerance Test Data
JOSEPH W. KEMNITZ, HELENA M. DZIADOWICZ, SHEILA GHANIAN, ROZALYN
M. ANDERSON, RICHARD WEINDRUCH, RICKI J. COLMAN, Madison, WI
ADA-Funded Research
For author disclosure information, see page LB98.
LB63
POSTERS
Insulin clearance is an important factor in the regulation of plasma insulin
concentrations and insulin action. Common methods for estimating clearance
involve measuring plasma insulin during hyperinsulinemic clamps or insulinmodified frequently sampled intravenous glucose tolerance tests (FSIGT) and
then using the insulin infusion rate to calculate clearance. These methods do
not provide information on the relative contributions of hepatic or peripheral
clearance or an estimate of clearance for endogenous insulin secretion. We
developed a mathematical model that utilized both C-peptide and insulin
measurements during FSIGT to estimate endogenous insulin secretion and
both hepatic and peripheral insulin clearance. Data from 101 black subjects
(mean (SD) BMI = 28 (4) kg/m2, age = 38 (10) yr, fasting insulin = 42 (60)
pM, SI = 3.9 (2.4) ∙ 10 -4 (µU/ml)-1min-1) were analyzed. The model provided an
excellent fit to the observed data (Figure; mean r2 = 0.88 for individual fits).
Model-estimated clearance for IV- (1.7 (0.7) L/min) and portally-delivered
(2.5 (1.1) L/min) insulin were 80-170% higher than IV clearance estimated
from previous FSIGT method (0.9 (0.5) L/min). Clearance for both IV and
portal insulin delivery were correlated with insulin sensitivity (Figure). The
method provides a promising new approach for estimating insulin clearance
in clinical studies.
Integrated
Physiology/Obesity
DAVID POLIDORI, RICHARD N. BERGMAN, ANNE SUMNER, San Diego, CA, Los
Angeles, CA, Bethesda, MD
For the past 25 years we have been assessing glycemic regulation in cohorts of male and female rhesus monkeys to evaluate the effects of moderate caloric restriction (CR) on healthspan and lifespan. Beginning ~10 yr of
age (median lifespan ~26 yr) all subjects were fed a purified diet containing
15% protein (lactalbumin), 10% fat (corn oil) and ~65% carbohydrate (sucrose, starch and dextrin), supplemented daily with fresh fruit or vegetables.
Control monkeys (C, n=38 initially, 3 currently surviving) were fed amounts of
purified diet to allow unlimited access for ~8 hr/day. Restricted monkeys (R,
n=38, 10 currently surviving) were fed 20-30% of their individualized baseline level of intake, subsequently adjusted for changes in intake by C except
to maintain health as indicated. Fasting glucose (Gb) and insulin (Ib) concentrations were measured semi-annually and additional parameters by FSIGT
and minimal modeling at 6-mo (0-10 yr), annually (11-15 yr) and bi-annually
(16 yr - present). Mean values of survivors over time (decreasing n’s) for Gb
and Ib were consistently higher for C than R (p<0.02). Insulin sensitivity (SI)
and disposition index (DI) steadily declined with advancing age for both
groups, but were greater for R (p<0.05), and glucose tolerance (KG) tended
to be improved for R (p=0.1). Insulin response to glucose (AIRG) did not differ
between groups. During the course of study, 14 C exhibited persistent Ib
greater than 90th percentile of baseline average and 5 developed fasting
hyperglycemia; only 5 and 2 of R showed these impairments, respectively.
Glycemic regulation was enhanced and preserved throughout adulthood by
moderate restriction of a relatively high sugar diet.
Integrated Physiology—Liver
257‑LB
Orphan Nuclear Receptor Estrogen-related Receptor gamma Medi‑
ates Homocysteine-induced 11β-hydroxysteroid Dehydrogenase1
Expression in Liver
KWI-HYUN BAE, AE-KYUNG MIN, JAE-HAN JEON, SUNG-WOO KIM, DONGWOOK KIM, IN-KYU LEE, KEUN-GYU PARK, Daegu, Republic of Korea
11β-Hydroxysteroid dehydrogenase1 (11β-HSD1), an enzyme converting
inactive cortisone to active cortisol, is one of the most promising target
for the treatment of metabolic syndrome including diabetes, obesity and
fatty liver. Hyperhomocysteinemia is associated with diabetes and diabetic complications, considering as an independent risk factor for cardiovascular diseases. Although homocysteine-induced endoplasmic reticulum
(ER) stress has been proposed to explain the pathological changes in diverse disease models, the precise mechanisms are still largely unknown.
In the present study, we investigated whether homocysteine-induced ER
stress leads to transcriptional activation of the estrogen-related receptor
γ (ERRγ) and 11β-HSD1. We found that homocysteine induced ER stress
response related markers, ERRγ and 11β-HSD1expression in H4IIE cells.
Tunicamycin and thapsigargin known as ER stress inducers increased hepatic ERRγ and 11β-HSD1 expression in cultured hepatocytes. To examine the potential role of ERRγ in hepatic 11β-HSD1 expression, ERRγ was
over-expressed or knock-downed by adenovirus expressing ERRγ or siRNA
against ERRγ, respectively. Overexpression of ERRγ significantly increased
11β-HSD1 expression, whereas knockdown of ERRγ expression attenuated
homocysteine-mediated induction of 11β-HSD1 expression. Moreover, an
inverse agonist of ERRγ, GSK5182, ameliorated homocysteine-mediated
11β-HSD1 induction. In conclusion, this study shows that ERRγ mediates
homocysteine-induced hepatic 11β-HSD1 expression, and suggests a novel
mechanism by which hepatic 11β-HSD1 transcription is mediated under hyperhomocysteinemia. The present study suggests that ERRγ inhibitors such
as GSK5182 has potential metabolic benefits by ameliorating homocysteine
induced hepatic 11β-HSD1 expression.
Integrated Physiology—Liver
255‑LB
The RNA Binding Protein Tristetraprolin Regulates Hepatic Metab‑
olism and the Development of Diabetes
KONRAD T. SAWICKI, MARINA BAYEVA, HSIANG-CHUN CHANG, ADAM DEJESUS, ANTHONY LEONARDI, HOSSEIN ARDEHALI, Chicago, IL
Diabetes is associated with extensive metabolic dysfunction, particularly
in glucose and fatty acid metabolism. Tristetraprolin (TTP) is a zinc finger
protein that binds to AU-rich elements in the 3’-untranslated region (UTR)
of target mRNAs, resulting in their degradation. The yeast homologs of
TTP were recently shown to regulate the mRNAs of metabolic enzymes,
and clinical studies have linked TTP expression to metabolic syndrome in
human patients. We hypothesized that TTP protects against the development of diabetes by promoting glucose oxidation through downregulation of
pyruvate dehydrogenase kinase 4 (PDK4) and reducing FA oxidation through
downregulation of peroxisome proliferator activated receptor (PPAR)-α in
the liver. TTP protein and mRNA levels were significantly reduced in the livers of db/db and high-fat diet fed mice compared to controls, suggesting
that the mRNA targets of TTP may be stabilized in diabetes. Primary hepatocytes from TTP KO mice demonstrated increased PPARα mRNA, a major
regulator of lipid metabolism compared to control mice. Consistent with
increased PPARα, rates of lipid uptake and β-oxidation were increased in
primary hepatocytes isolated from TTP KO compared to control mice. PPARα
mRNA was also significantly stabilized in TTP KO compared to control cells,
suggestive of post-transcriptional regulation by TTP. Primary hepatocytes
from TTP KO mice also demonstrated increased PDK4 mRNA, a key regulator
of glucose utilization. Consistent with increased PDK4, lactate content was
increased in primary hepatocytes from TTP KO compared to control mice. In
silico analysis revealed multiple well-conserved putative TTP-binding sites
in the 3’UTR of PPARα and PDK4, consistent with the possibility of direct
regulation of mRNA stability by TTP. We show that TTP is downregulated in
the livers of diabetic mice, and that TTP KO in primary hepatocytes increases
the levels of key metabolic enzymes, PDK4 and PPARα, both of which are
implicated in diabetes.
258‑LB
Pemt Deficiency Promotes Steatohepatitis through Sustained
Apoptosis via Clathrin Heavy Chain-p53 Mediated Transcriptional
Mechanisms
ATSUKO NAKATSUKA, KAZUTOSHI MURAKAMI, NUNOUE TOMOKAZU, SATOSHI
YAMAGUCHI, JUN EGUCHI, DAISUKE OGAWA, JUN WADA, Okayama, Japan
Phosphatidylethanolamine N-methyltransferase (pemt) catalyzes the
conversion of phosphathidylethanolamine to phosphatidylcholine, which is
critical pathway for lipoprotein metabolism, stability of cellular membranes,
and de novo choline production in the liver. We identified pemt as one of the
highly up-regulated genes in obese mice by DNA chip. To investigate the
role of pemt in metabolic syndrome, we generated pemt knockout mice and
subjected to high-fat high-sucrose (HF) diet. Although pemt-/- mice showed
obesity resistant phenotype and normal insulin sensitivity under HF diet,
prominent steatohepatitis with multiple tumors was observed. In the liver
of pemt-/- mice under HF, TUNEL-positive apoptosis cells were increased.
Histologically, accumulation of F4/80-positive macrophages and enhanced
fibrosis were also observed in pemt-/- mice under HF compared with
pemt+/+. Next, we found the novel localization of pemt in the nuclei besides
the known cellular distribution in endoplasmic reticulum. By using nuclear
extracts of the liver, clathrin heavy chain (CHC) was identified as an interactive molecule with pemt by immunoprecipitation and subsequent LC-MS/
MS analysis. We also found that pemt forms a complex with p53 and CHC
by immunoprecipitation and western blot analysis. Overexpression of pemt
suppressed p53 mediated transcriptional activity by luciferase reporter assay. In turn, the expressions of p53-target genes; cleaved caspase 3, Bax,
and p21 were increased in the liver of pemt-/- mice under HF. Our investigation revealed the deficiency of pemt resulted in increased expression of
CHC, which has been reported to promote tumor growth and angiogenesis.
In conclusion, pemt deficiency and subsequent facilitation of CHC-p53 transcriptional pathways continuously promote hepatocyte apoptosis, tissue
inflammation, and fibrosis, which ultimately lead to steatohepatitis.
Supported By: National Institutes of Health (F30DK102341 to K.T.S.)
256‑LB
Hepatokine IGFBP-2 Is Increased by PPARα during Fasting
POSTERS
Integrated
Physiology/Obesity
SEUNG-SOON IM, JAE-HOON BAE, DAE-KYU SONG, BYUNG-CHUL OH, JI-YOUNG
CHA, Daegu, Republic of Korea, Incheon, Republic of Korea
Insulin-like growth factor (IGF)-binding protein-2 (IGFBP-2), one of the
most abundant circulating IGFBPs, is known to attenuate the biological action of IGF-1. Although the effect of IGFBP-2 in preventing metabolic disorder
is well known, its regulatory mechanism remains unclear. Herein, we demonstrated the transcriptional regulation of the IGFBP-2 gene by peroxisome
proliferator-activated receptor (PPAR) α in the liver. During fasting, both
Igfbp-2 and PPARα expressions increased. Wy14,643, a selective PPARα
agonist, significantly induced IGFBP-2 gene expression in primary cultured
hepatocytes. However, IGFBP-2 gene expression in Pparα null mice was
not affected by either fasting or Wy14,643. In addition, through transient
transfection and chromatin immunoprecipitation assay in fasted livers, we
determined that PPARα bound to the putative PPAR-response element between -511 bp and -499 bp on the IGFBP-2 gene promoter, indicating that the
IGFBP-2 gene transcription is directly activated by Pparα. To explore the role
of Pparα in IGF-1 signaling, we treated primary cultured hepatocytes with
Wy14,643 and observed a decrease in the number of IGF-1 receptors and
in Akt phosphorylation. No inhibition was observed in the hepatocytes isolated from Pparα null mice. These results suggest that PPARα controls IGF-1
signaling through the upregulation of hepatic IGFBP-2 transcription during
fasting and Wy14,643 treatment.
259‑LB
NF-kB Inhibits Hepatic Insulin Sensitivity by Upregulation of cAMP
JIANPING YE, BILUN KE, ZHIYUN ZHAO, VINCENT MANGANIELLO MANGANI­
ELLO, BIN WU, Baton Rouge, LA, Bethesda, MD, Guangzhou, China
Inflammation regulates glucose and fatty acid metabolism in liver. However, the signaling pathway remains to be characterized. To this point, we
tested the role of transcription factor NF-kB in liver by inactivating the subunit p65 (RelA) gene. Liver p65 knockout mice (L-p65-KO) were generated in
Supported By: Korea Healthcare Technology R&D Project (A120864)
ADA-Funded Research
For author disclosure information, see page LB98.
LB64
Integrated Physiology—Liver
C57BL/6 gene background by crossing floxed p65 and Alb-cre mice. The NFkB inactivation did not alter growth, reproduction and body weight in mice
on the regular chow or a high fat diet (HFD). In KO mice, systemic insulin sensitivity was improved on HFD as indicated by insulin and glucose tolerance.
Hepatic insulin sensitivity was enhanced as indicated by increased pyruvate
tolerance, Akt phosphorylation and decreased expression of gluconeogenic
genes in hepatocytes. In liver of KO mice, a decrease in intracellular cAMP
was observed with reduced CREB phosphorylation. An increase in cAMP
clearance was observed with increased activity of cyclic nucleotide phosphodiesterase 3B (PDE3B), whose expression was enhanced in mRNA and
protein. p65 was found to mediate TNF-α activity to inhibit expression of
PDE3B gene at three NF-kB binding sites in the PDE3B gene promoter. Body
composition, food intake, energy expenditure, systemic and hepatic inflammation were not significantly altered in KO mice on HFD. These data suggest
that in inflammatory responses, NF-kB may inhibit hepatic insulin sensitivity by up-regulation of cAMP pathway through suppressing transcription of
PDE3B gene.
were significantly increased in the LIRKO model, both mRNA and protein
levels returned to low levels in mice lacking both liver insulin receptor and
Fox01 (LIRFKO): a) mRNA: (LIRKO 70.5±14.3 vs. LIRFKO 1.0±0.2, p=0.004,
n=6); b) protein: (LIRKO 125.5±20.6 vs. LIRFKO 5.9±0.8, p=0.0006 n=6). In
agreement with a role for serpinB1 in β-cell growth, LIRFKO mice exhibit reduced β-cell area (control 0.5±0.04 vs. LIRKO 1.75±0.35, p=0.01; control vs.
LIRFKO 0.6±0.08%, p=0.4, n=5-6) due to attenuation of β-cell proliferation
as revealed by Ki67 staining (control 0.55±0.02 vs. LIRKO 2.0±0.43, p=0.03;
control vs. LIRFKO 0.38±0.08% Ki67+ β-cells, p=0.1, n=5-6). Together, these
data implicate Fox01 as a regulator of serpinB1 in mediating β-cell compensatory response to insulin resistance.
Perilipin 5 Phosphorylation in Lipolysis of Nonadipocytes
262‑LB
MICHELLE B. TREVINO, TIMOTHY KING, SO HYUN PARK, YUI MACHIDA, SUCHARITA DUTTA, YUMI IMAI, Norfolk, VA
Adipocytes increase lipolysis through protein kinase A (PKA) mediated
phosphorylation of perilipin (PLIN) 1 that increases access and activity of lipases at lipid droplets (LD). In non-adipocytes such as hepatocytes and beta
cells, lipolysis and resultant metabolites are critical for provision of energy
and for cellular signaling including PPARa activation and augmentation of
insulin secretion. However, the regulation of lipolysis in these cells without
PLIN1 is poorly understood. PLIN5 is a LD protein increased in beta cells and
hepatocytes in fasted mice when lipolysis is important (Trevino MB, Diabetes
in press). Here, we report that serine155 (S155) of mouse PLIN5 is phosphorylated (P-PLIN5) in vivo in response to nutritional cues, and PKA resistant
S155 mutant (S155A) blunts lipolysis and expression of genes regulated by
PPARa. When P-PLIN5 was assessed in the liver from fed and 24h fasted
C57BL6 male mice by LC/ESI-MS/MS (Q-Exactive, Thermo Fisher), S155
phosphorylation (P-S155) was increased to 2.5 fold (p<0.005) in fasted liver
in which cAMP level is elevated from glucagon. PKA dependence of P-S155
was confirmed in primary hepatocytes expressing PLIN5; PKA inhibitor H89
reduced the rise of P-S155 by cAMP analog (1mM 8-Br-cAMP, p<0.005). In
beta cells, cAMP increases postprandially in response to glucose and GLP1. Expectantly, S155/P-S155 ratio was 5.3 fold (p<0.05) in islets from mice
refed 1h after fasting compared with fasted mice. S155A PLIN5 expressed in
AML12 cells blunted an increase in lipolysis upon 1mM 8-Br-cAMP treatment
(p<0.05) in agreement with recent data in COS7 cells (JBC 2015:290:1295).
Finally, 1mM 8-Br-cAMP increased the expression of PPARa and its target
genes in AML12 cells expressing WT PLIN5, while the response was blunted
in S155A AML12 cells. The above data along with our recent data (Trevino
MB, Diabetes in press) support a model that P-PLIN5 regulates lipolysis in
non-adipocytes aiding a switch in lipid metabolism during fasting in the liver
and postprandial insulin secretion in beta cells.
Supported By: DK068036
260‑LB
Leucine Synergizes with Phosphodiesterase 5 (PDE5) Inhibitors and
Metformin to Reverse Hepatic Lipid Accumulation and Inflammation
and Treat Nonalcoholic Fatty Liver Disease (NAFLD)
LIZHI FU, FENFEN LI, QIANG CAO, XIN CUI, BINGZHONG XUE, HANG SHI, ANTJE
BRUCKBAUER, MICHAEL B. ZEMEL, Atlanta, GA, Knoxville, TN
Sirt1 and AMPK regulate hepatic lipid and energy metabolism and are
therapeutic targets for NAFLD. We previously demonstrated that L-leucine
(leu) has a unique role as an allosteric activator of Sirt1, enabling synergy
with metformin (met) to increase insulin sensitivity and reverse NAFLD in
mice. PDE5 inhibitors converge on the Sirt1/AMPK pathway via eNOS/NO
signaling, and leu also synergizes with sildenafil (sild) to inhibit both steatosis and inflammation. Here we demonstrate the potential for multi-component activation of this pathway with leu (0.5 mM), met (10 M) and sild (1 nM)
to yield greater therapeutic efficacy in NAFLD. Leu-met-sild activated Sirt1
to a greater degree than leu-met or leu-sild, resulting in markedly greater
stimulation of hepatocyte fat oxidation (~60%, p<0.01) and inhibition of
palmitate-induced triglyceride accumulation (~70%, p<0.001). To evaluate
this synergy in vivo, non-alcoholic steatohepatitis (NASH) was induced in
mice via high fat diet supplemented with cholesterol and cholate (HF/ATH
diet); mice were then treated with combinations of leu (24 g/kg diet), met
(0.25 g/kg diet; <20% of therapeutic dose) and sild (25 mg/kg diet; <10%
therapeutic dose). The HF/ATH diet caused a ~6-fold increase in alanine aminotransferase (p<0.0001) which was modestly reduced by leu-met and leusild (30-40%, p<0.01) and further reduced by leu-met-sild (60%, p<0.0001).
The HF/ATH diet also caused increases in liver mass and a marked increase
in liver fat content (~7-fold, p<0.0001). Leu-met and leu-sild elicited modest
reductions in both, while the leu-met-sild combination reduced liver mass
(p<0.003) and liver fat to a significantly greater degree (38%, p=0.02). These
data demonstrate preclinical therapeutic potential for leucine combined
with sub-therapeutic levels of metformin and sildenafil in the treatment of
NAFLD and NASH.
Supported By: National Institutes of Health (R01DK090490, R01DK09049002W1)
263‑LB
ApoA1 Knockout Mice Manifest Decreased Energy Expenditure and
Are Prone to High-fat Diet-induced Whole-Body Insulin Resistance
Alterations in the expression of Apolipoprotein C3 (ApoC3) and A5 (ApoA5)
have both been shown to have effects on ectopic lipid deposition as well as
insulin action in mice and humans. However, whether alterations in Apolipoprotein A1 (ApoA1) expression can also alter ectopic lipid deposition and insulin action is unknown. In order to address this question we studied ApoA1
knockout (KO) mice or wild type (WT) mice fed a high-fat diet. ApoA1 KO mice
displayed an ~80% increase in body fat compared with WT mice (P<0.001).
Associated with the increased body fat, KO mice displayed a ~15% reduction
in energy expenditure (P<0.01). ApoA1 KO mice displayed a ~40% decrease
in plasma triglycerides (TAG) (P<0.001) and a ~80% decrease in plasma cholesterol (P<0.001), associated with a ~25% decrease in liver VLDL export
(P<0.001). In addition, KO mice displayed increased TAG and diacylglycerol
(DAG) content in both liver (~140% and ~45%, P<0.01) and skeletal muscle
(~115% and ~70%, P<0.01). Consistent with increased DAG content, PKCε
activation in liver and PKCθ activation in muscle were increased by ~60%
(P<0.01) and ~35% (P<0.01), respectively, in KO mice. To assess whole-body
insulin sensitivity, euglycemic-hyperinsulinemic clamps were performed.
The glucose infusion rate (GIR) was ~45% less in KO mice compared with
control mice (P<0.01), demonstrating impaired whole body insulin sensitivity in KO mice. This reduction in GIR was accounted by both reductions in
whole-body glucose uptake (~15%, P<0.05) and suppression of endogenous
glucose production (~65%, P<0.001) compared with WT mice. In conclusion,
these data demonstrate that absence of ApoA1 in mice promotes reductions
ABDELFATTAH EL OUAAMARI, INSUG O-SULLIVAN, WENWEI ZHANG, SHANSHAN XU, CHONG WEE LIEW, TERRY G. UNTERMAN, ROHIT N. KULKARNI, Boston, MA, Chicago, IL
We previously reported that adaptive β-cell growth in response to insulin
resistance is mediated by hepatic factors in the liver-specific insulin receptor knockout (LIRKO) mouse. Using differential proteomics, we identified
the factor as serpinB1. Here we report that the Forkhead box protein O1
(Fox01) is a transcriptional regulator of serpinB1. Liver-specific expression
of constitutively active Fox01 in transgenic mice (Tg) induced a dramatic
increase in hepatic serpinB1 mRNA (Tg 25.4±2.8 vs. control 1.5±0.2, p=0.01,
n=3-4) and protein (Tg 5.7±0.5 vs. control 0.9±0.1, p=0.008, n=3-4) levels.
Consistent with a role for Fox01 in fasting/feeding states, 18h-starved
mice show enhanced hepatic serpinB1 gene expression when compared to
mice re-fed for 6h after fasting (fasted 8.3±1.0 vs. refed 1.5±0.3, p=0.005,
n=3-4). The stimulatory action of fasting on serpinB1 mRNA levels was
blunted in mice lacking FOXO proteins in the liver (WT-fasted 8.3±1.0 vs.
KO-fasted 1.9±0.7, p=0.004, n=3-4). Furthermore, while hepatic expression
of serpinB1 mRNA (control 1.6±0.3 vs. LIRKO 70.5±14.3, p=0.005, n=5-6)
and protein (control 10.3±5.6 vs. LIRKO 125.5±20.6, p=0.0004, n=5-6) levels
ADA-Funded Research
For author disclosure information, see page LB98.
LB65
POSTERS
261‑LB
Fox01 Regulates Hepatic SerpinB1 Gene Expression and Partici‑
pates in Compensatory β-Cell Growth Response to Insulin Resis‑
tance
Integrated
Physiology/Obesity
JOAO-PAULO G. CAMPOREZ, VARMAN T. SAMUEL, KITT F. PETERSEN, MICHAEL
J. JURCZAK, GERALD I. SHULMAN, New Haven, CT
Integrated Physiology—Macronutrient Metabolism and Food Intake
Integrated Physiology—Macronutrient
Metabolism and Food Intake
in both plasma TAG and cholesterol concentrations but exacerbates high-fat
feeding-induced liver and muscle insulin resistance by decreasing energy
expenditure and increasing ectopic lipid content (TAG/DAG) in both liver and
muscle, leading to increased PKCε and PKCθ activation in these organs.
266‑LB
Loss of Insulin Receptors in Vascular Endothelial Cells Reduces In‑
sulin Signaling in Brain and Peripheral Tissues
264‑LB
Maternal Malnutrition Induces Defective Autophagy Leading to
Glycogen Accumulation in the Liver of Newborn Wistar Rats
MASAHIRO KONISHI, MASAJI SAKAGUCHI, WEIKANG CAI, CHRISTIAN RASKMADSEN, C. RONALD KAHN, Boston, MA
JUAN DE TORO-MARTÍN, ELISA FERNÁNDEZ-MILLÁN, ESTHER LIZÁRRAGAMOLLINEDO, FERNANDO ESCRIVÁ-PONS, CARMEN ÁLVAREZ-ESCOLÁ, Madrid,
Spain
Insulin resistance is central to the pathophysiology of obesity, type 2 diabetes and metabolic syndrome. Recent data indicate that insulin resistance
is also present in neurodegenerative diseases like Alzheimer’s disease. Dysfunction of insulin signaling in vascular endothelial cells may be a component
of insulin resistance. However, the effects of vascular insulin resistance on
insulin action in brain and other tissues are not fully understood. In this
study, we investigated effects of insulin receptor (IR) knockout specifically
in vascular endothelial cells (EndoIR-KO mice) by breeding mice with a cre
transgene driven by the VE-Cadherin promoter and IRlox/lox mice. Following
intravenous insulin injection (5U), phosphorylation of IR and Akt in interscapular BAT and soleus muscle was decreased in EndoIR-KO by 66% and 58%,
respectively, while signaling in liver was not altered. In control mice, insulin
also induced phosphorylation of IR in the prefrontal cortex, hippocampus and
hypothalamus, and these were attenuated in EndoIR-KO mice by 46%, 90%
and 82% with no change in IR protein levels. In EndoIR-KO mice, food intake
was greater than control by 18% under random fed. In addition, the glucoselowering response to intraperitoneal insulin injection (0.75 U/kg) was significantly delayed (latency of half-maximal reduction: 10.1±1.2 vs. 23.4±5.0
min in control and EndoIR-KO), while maximal glucose reduction levels were
similar. Thus, loss of IR specifically in vascular endothelial cells negatively
affects insulin signaling and functions in brain, skeletal muscle and fat, but
not liver. These results suggest that transendothelial transit of circulating
insulin via insulin receptors in vascular endothelial cells is a rate-limiting
factor for onset of insulin action, especially in brain, skeletal muscle and fat
which are separated from the circulation by vascular endothelial cells with
tight junctions preventing rapid access of insulin to the target cells.
Among the mechanisms by which an adverse intrauterine environment
could increase the susceptibility to develop type 2 diabetes in the adulthood,
defective hepatic autophagy has emerged as a potential contributor to this
pathology. We then focused this work on glycogen autophagy during the
perinatal period. We developed a model of global food-restriction achieved
by restricting maternal nutrition from the last third of gestation onwards
to 35% of ad libitum intake. A caesarean was practised just before birth
and changes in liver glycogen and in autophagic markers were measured
during the first 3 and 6h of life. No caloric intake was permitted, and the
newborns were maintained at 37º C. At birth, offspring from undernourished
dams (U) exhibited increased liver glycogen (2.5-fold) content than controls
(C). The amount of liver glycogen precipitously diminished at 3 and 6h in C
rats whereas it remained significantly elevated in U neonates, which also
showed a lower phosphorylation of AMPKα at both 3 and 6h. Consequently,
mTOR activation was enhanced in U livers. Atg7 was significantly decreased
at both times in U livers. Importantly, C livers showed a marked induction of
LC3BII conversion between 3 and 6h while in U animals LC3 lipidation was
markedly reduced. Impairment of the autophagic flux was confirmed by the
accumulation of p62 in the liver of U rats. In agreement with the increased
autophagic activity in C neonates, quantitative electron microscopy showed
abundant autophagic vesicles containing glycogen and almost no cytoplasmic glycogen in C livers. In contrast, the number of autophagic vesicles was
clearly reduced in U newborns after 6h of fasting and vast areas of cytoplasmic glycogen were observed. These results highlight that maternal undernutrition lead to defective hepatic autophagy in the offspring and consequently
could compromise hepatic metabolic function, favouring insulin resistance
development in the adulthood.
Supported By: National Institutes of Health (R01DK031036)
267‑LB
CD47 Regulates Adipose Tissue Lipolysis by Suppressing cGMP/
PKG Signaling
Supported By: MINECO (BFU2011/25420); CIBERDEM (ISCIII); CAM (S2010/
BMD-2423)
HEATHER L. NORMAN-BURGDOLF, SHUXIA WANG, Lexington, KY
CD47 is a ubiquitously expressed transmembrane cell receptor involved
in immune cell regulation, self-recognition, and cell signaling. Specifically,
CD47 regulates the cyclic GMP (cGMP)/protein kinase G (PKG) pathway by
suppressing soluble guanylyl cyclase (sGC)-dependent activation of cGMP
and downstream PKG activity. Recently, this specific pathway has been
identified as a key regulatory mechanism for the browning phenomenon associated with healthy adipocyte function including lipolysis, mitochondrial
biogenesis, and UCP1 activation. Although CD47 has been well characterized in cancer and ischemia models, adipose tissue expression has never
been explored. In the current study we determined the effect of CD47 on
adipocyte lipolysis. First, male 8-week old CD47 deficient and wildtype (WT)
littermate controls were exposed to a cold tolerance test (CTT, 4° C) for 6
hours and plasma free glycerol levels were measured. Ex vivo lipolysis of
both perigonadal and subcutaneous depots from either CD47 deficient or
WT mice in basal or 10uM isoproterenol-treated conditions were assayed.
In addition, in vitro studies with fully differentiated 3T3-L1 cells treated with
a combination of cGMP agonist and/or CD47 functional blocking antibody
were completed. We found that CD47 deficient mice had a significant increase in plasma free glycerol after 6-hour CTT (p<.05). Similarly, CD47 deficient perigonadal (p=.0514) and subcutaneous (p<.01) tissue explants had
elevated free glycerol release with both vehicle and 10uM isoproterenol
treatments compared with WT tissue explants. In vitro data showed differentiated 3T3-L1 cells treated with either 8-cCPT-cGMP and/or anti-CD47
blocking antibody exhibited increased lipolysis compared to controls (p<.05).
These studies suggest CD47 plays a novel role in regulating adipocyte lipolysis specifically by suppressing cGMP/PKG signaling.
265‑LB
Targeted Induction of Ceramide Degradation Reveals Roles for Ce‑
ramides in Nonalcoholic Fatty Liver Disease and Glucose Metabo‑
lism
POSTERS
Integrated
Physiology/Obesity
JONATHAN XIA, WILLIAM HOLLAND, PHILIPP SCHERER, Dallas, TX
Sphingolipids have garnered attention for their role in insulin resistance
and lipotoxic cell death. Aberrant accumulation of ceramides correlates with
hepatic insulin resistance and steatosis. We recently demonstrated that the
insulin sensitizing and cytoprotective actions of adiponectin are linked to the
deacylation of ceramides, mediated by adiponectin receptors. To further investigate the tissue-specific effects of local changes in ceramidase activity,
we have developed transgenic mice inducibly expressing acid ceramidase,
to trigger the deacylation of ceramides. This represents the first inducible
genetic model that acutely manipulates ceramides in adult mouse tissues,
allowing us to directly assess the impact of ceramide lowering on insulin
sensitivity. Hepatic overexpression of acid ceramidase prevents hepatic
steatosis and prompts improvements in insulin action in liver and adipose
tissue. Conversely, overexpression of acid ceramidase within adipose tissue
prevents hepatic steatosis and insulin resistance. Induction of ceramidase
activity in either tissue promotes a lowering of hepatic ceramide and reduced activation of the ceramide-activated atypical protein kinase C isoform
PKC-zeta. Ceramides induce hepatic lipid uptake via PKC-zeta induced activation of CD36, thereby promoting hepatic steatosis. These observations
suggest the existence of a rapidly acting “cross-talk” between liver and
adipose tissue sphingolipids, critically regulating glucose metabolism and
hepatic lipid uptake.
Supported By: T32DK007778-14
Supported By: R01DK55758, 1P01DK088761, F30DK100095091
ADA-Funded Research
For author disclosure information, see page LB98.
LB66
Integrated Physiology—Muscle
268‑LB
270‑LB
T Lymphocytes Are Critically Involved in Diet-induced Lipid Me‑
tabolism in the Liver
Pyruvate Dehydrogenase Kinase 4 Mediates Free Fatty Acid-in‑
duced Mitochondrial Dysfunction and Insulin Resistance in Skel‑
etal Muscle: Identification of a Novel Regulator of Insulin Signaling
by Quantitative Proteomics
MARIA MOISIDOU, SEVASTI KARALIOTA, KOSTANTIA KODELLA, ELISAVET
KODELLA, STAMATIS THEOHARIS, DIMITRIS SKOKOS, MARK SLEEMAN, KATIA
KARALIS, Athens, Greece, Tarrytown, NY, Melbourne, Australia
KENTARO MURAKAMI, MASAKI YAMABI, MASAYUKI OHTA, MALLARY HOIDAL,
MARY C. WHELAN, IWAO YAMADA, PIERO RICCHIUTO, MASANORI AIKAWA,
SASHA SINGH, KEN MIZUNO, Boston, MA
Hepatic deposition of lipids, or liver steatosis, is a cardinal sign of starvation as well as hypercaloric diets, such as high-fat diet, and obesity. Emerging evidence demonstrates the critical role of immune cells in metabolic
processes, and the impact of immunometabolism in the pathogenesis of a
variety of diseases. The aim of this study was to elucidate the role of lymphocytes in diet-induced non-alcoholic fatty liver disease, NAFLD. Histology
of the livers of Rag1-/- mice, either following starvation for 24hrs or high-fat
diet for ten weeks, had normal morphology. In contrast, profound steatosis was detected in the livers from wild-type mice following either dietary
intervention. Gene expression analysis of liver tissues identified activation
of genes involved in lipid oxidation pathway in the Rag1-/- and significant
decrease of genes involved in the glyconeogenesis pathway, compared to
the wild type mice. In support of the above, indirect calorimetry analysis
under normal feeding states showed significant decrease in the respiratory
exchange ratio of the Rag1-/- mice, reflecting more efficient lipid versus
carbohydrate utilization. Adoptive transfer of CD8+, but not CD4+, T cells
rescued the phenotype of the Rag1-/- liver indicating the critical role of these
cells in lipid metabolism in the liver. The mechanism(s) driving this effect are
still unclear, with preliminary evidence indicating altered autophagy as a putative critical node in this process. In summary, our results provide evidence
for the critical role of lymphocytes in diet-induced hepatic lipid metabolism
and raise the possibility of immunotherapy against liver steatosis, a common
side effect of various therapeutic interventions or pathological processes.
Increased levels of free fatty acids (FFA) in plasma are associated with
insulin resistance-related disorders and diseases such as obesity and type 2
diabetes mellitus (T2DM). These high levels of plasma FFA play an important
role in the development of insulin resistance. Although the evidence suggests that mitochondrial dysfunction by FFA in skeletal muscle cells play
an important role in insulin signaling impairment, the mechanisms involved
in insulin resistance induced by FFA remain incompletely understood. To
determine how FFA induces mitochondrial dysfunction and impairs insulin
signaling in skeletal muscle, we isolated mitochondrial proteins from C2C12
myotubes treated with palmitate, oleate, or bovine serum albumin (control)
for 24 hours before insulin stimulation, and performed quantitative proteomic analysis using the isobaric tandem mass tagging system (TMTTM).
Palmitate significantly increased or decreased 226 mitochondrial proteins
in C2C12 myotubes. Specifically, palmitate stimulation markedly induced
pyruvate dehydrogenase kinase 4 (PDK4) (1.6-fold vs. control). Moreover, enforced expression of PDK4 decreased phopsphorylation of AKT (pAKT/AKT,
-19% vs. control) and citrate synthase activity (-12% vs. control) under insulin stimulation conditions in C2C12 myotubes. In addition, PDK4 expression
decreased mtDNA levels (-25% vs. control P=0.035). These results indicate
that, in skeletal muscles, FFA may modulate insulin sensitivity and mitochondrial function via PDK4, leading to insulin resistance. In conclusion, PDK4
may be a novel therapeutic target for obesity or T2DM.
Supported By: Synergasia; HRAKLEITOS
Supported By: Kowa Company, Ltd.
Integrated Physiology—Muscle
271‑LB
Mechanism by which Caloric Restriction Improves Insulin Sensitiv‑
ity in Sedentary Obese Adults
269‑LB
Caloric restriction (CR) improves insulin sensitivity and reduces the incidence of diabetes in obese individuals. The underlying mechanisms whereby
CR improves insulin sensitivity are not clear. We evaluated the effect of
16-weeks of CR on whole-body insulin sensitivity by pancreatic clamp before and after CR in 11 obese participants (BMI=35 kg/m2) in comparison
with a matched control period (CON, N=9, BMI=34 kg/m2). Participants in
the CR group lost on average 10.1 ± 1.2% of total bodyweight, while no
change was found in the CON group (+0.8 ± 0.6%). Compared to CON, CR
increased the glucose infusion rate required to maintain euglycemia during hyperinsulinemia that fully suppressed endogenous glucose production
(p < 0.0001). This improvement in peripheral insulin sensitivity was not accompanied by changes in skeletal muscle mitochondrial oxidative capacity
or oxidant emissions, nor was there changes in skeletal muscle ceramide,
diacylglycerol, or amino acid metabolite levels. However, the CR induced
improvement in insulin sensitivity occurred in concert with increased post
absorptive whole body lipid oxidation and reduced levels of skeletal muscle
thioredoxin-interacting protein (TXNIP) expression following hyperinsulinemia. Furthermore, the changes in TXNIP expression correlated with changes
in whole body insulin sensitivity for all participants over the 16-week period.
Together these results support a likely role of TXNIP in CR induced improvement in insulin sensitivity.
Mitochondria (Mito) play key roles in cellular metabolism and bioenergetics, the execution of cell-death and intracellular signaling. Due to the
multiplicity of Mito functions it has been documented that Mito dysfunction is implicated in the genesis and development of many different human
pathologies, including type 2 diabetes (T2D). A key transducer in energy
conservation and reactive oxygen species signaling is the mitochondrial H+ATP synthase. Its physiological inhibitor, the Mito ATPase Inhibitory Factor 1
(IF1) acts as a master regulator of energy metabolism, playing a crucial role
in metabolic adaptation to enhanced aerobic glycolysis. In cancer, IF1 overexpression triggers Mito hyperpolarization and the subsequent production
of superoxide radicals, resulting in a cellular adaptive response that includes
resistance to cell death. Despite the emerging role of Mito bioenergetics
in controlling skeletal muscle (SkM) metabolism during T2D, the basic cell
biology of IF1 and its’ involvement in this pathology remain basically unknown. We compared the expression of IF1 and other proteins regulating the
structure/activity of Mito in SkM biopsies from obese (BMI>30) type 2 diabetic (O-T2D), lean (BMI <27) diabetic (nO-T2D), obese non diabetic (O-nT2D)
and lean non diabetic (nO-nT2D) subjects, correlating the protein expression
with BMI, FI, FG and HOMA-IR parameters. We found a significant increase
(180%) in the expression of IF1 in obese subjects, regardless of the presence
of T2D. However, a reduction (80% of nT2D) in β-F1 ATPase, the catalytic
subunit of the H+-ATP synthase, was present in O-T2D compared to healthy
subjects. T2D subjects presented higher levels of the mitochondrial redox
sensor SOD2 and a tendency for a negative regulation of the Mito fusion
controller OPA1. In conclusion, our data support the hypothesis that obesity
and T2D can contribute in different ways to perturbations in the SkM Mito
network, thus facilitating muscle dysfunction.
Supported By: R01DK41973 (to K.S.N.); U24DK100469; DK50456; T32DK007198
(to M.L.J.); KL2TR000136-07 (to M.L.J.); KL2RR024151 (to B.I.); T32DK007352 (to
M.M.R., A.R.K.); UL1TR000135; Mayo Foundation; Murdock-Dole Professorship (to
K.S.N.)
Supported By: U.S. Department of Veterans Affairs; National Institutes of Health
ADA-Funded Research
For author disclosure information, see page LB98.
LB67
POSTERS
LAURA FORMENTINI, ALEXANDER J. RYAN, LESLIE CARTER, JOSE M. CUEZVA,
THEODORE P. CIARALDI, ROBERT R. HENRY, Madrid, Spain, La Jolla, CA, San Diego, CA
Integrated
Physiology/Obesity
MATTHEW L. JOHNSON, KLAUS DISTELMAIER, IAN LANZA, BRIAN IRVING,
MATTHEW M. ROBINSON, ADAM R. KONOPKA, GERALD I. SHULMAN, K. SREEKUMARAN NAIR, Rochester, MN, New Haven, CT
Effects of Type 2 Diabetes and Obesity on the Expression of Mito‑
chondrial Proteins in Skeletal Muscle
Integrated Physiology—Other Hormones
Integrated Physiology—Other Hormones
proteolytically derived peptides could modulate insulin release. After establishing the presence of VGF in β-cell lines, we screened the effect of several
C-terminal VGF-derived peptides, including TLQP-21 and TLQP-62, on glucose
stimulated insulin secretion (GSIS) in beta-cell lines and on glucose tolerance in vivo. TLQP-62 increased insulin secretion in several insulinoma cell
lines in both low and high glucose conditions. Conversely, TLQP-21 only had
weak effect at the low glucose concentration while mildly, but significantly,
potentiated GSIS in vitro. We also found that the mechanism of action of
TLQP-62-stimulated insulin secretion is via increased intracellular calcium
mobilization and fast expression of the insulin 1 gene. Furthermore, we compared the efficacy of the two peptides in improving glucose homeostasis in
vivo in mice. TLQP-62, but not TLQP-21, dose-dependently improved glucose
tolerance in the glucose tolerance test. Together, our findings suggest that
TLQP-62 is the most potent VGF peptide on insulin secretion and glucose
homeostasis. Further studies are required to understand its mechanism of
action. Our study suggests that TLQP-62 can be considered a novel strong
insulinotropic peptide that can be targeted for innovative anti-diabetic drug
discovery programs.
272‑LB
Understanding the Mechanism of Cholesterol Lowering Effect of
GLP1-R/GCGR Co-agonists
LI-PING SUN, HONG-PING GUAN, XIAODONG YANG, MICHELE PACHANSKI,
SHENG-PING WANG, CARLOS G. RODRÍGUEZ, ANDREA NAWROCKI, STEVE PREVIS, LIANGSU WANG, PAUL CARRINGTON, Kenilworth, NJ
The glucose-lowering and anti-obesity effects of GLP-1R/GCGR co-agonist
have been demonstrated in preclinical rodent and NHP models and are now
being tested in the clinic. The lipid-lowering efficacy, especially the decrease
in LDL cholesterol, has been demonstrated with dosing of GLP-1R/GCGR coagonist. Here, using a pair feeding scheme in the Oxymax metabolic system,
we showed that GLP-1R/GCGR co-agonist lowered plasma cholesterol levels
independent of body weight loss in mice. Specifically, glucagon signaling
was responsible for the plasma cholesterol lowering. In contrast to wildtype mice, GLP-1R/GCGR co-agonist did not change plasma cholesterol levels in LDLR knockout mice. Western blot analysis showed that LDLR protein
level in liver was increased. We further demonstrated that GLP-1R/GCGR coagonist promoted uptake of fluorescently labeled DIL-LDL in primary human
hepatocytes in a dose-dependent manner, while liraglutide did not. Using a
D2O tracer study, we have shown that GLP-1/GCGR co-agonist decreased
levels of newly synthesized cholesterol in liver and secretion of newly made
cholesterol in plasma in wild-type mice. The D2O tracer study was repeated
in LDLR knockout mice and the GLP-1/GCGR co-agonist also inhibited newly
synthesized cholesterol in liver of this model. Using dual 13C-cholesterol and
D6-cholesterol tracers dosed i.v. and p.o., respectively, we have shown that
GLP-1/GCGR co-agonist did not affect intestinal cholesterol absorption. In
conclusion, GLP-1/GCGR co-agonist lowers plasma cholesterol level by decreasing hepatic cholesterol synthesis and increasing LDLR-mediated lipoprotein uptake primarily through the glucagon signaling.
Supported By: Minnesota Partnership for Biotechnology and Medical Genomics
(to A.B.); National Institutes of Health-National Institute of Diabetes and Digestive
and Kidney Diseases (DK102496 to A.B.); Ministry of Education, University and
Research (to R.P.)
275‑LB
Preserved Enteroendocrine Secretion after Meal Challenge across
Glucose Tolerance (GT): Lack of Correlation with Beta Cell Function
(BCF)
HARTMUT RUETTEN, MATHIAS GEBAUER, RALPH H. RAYMOND, R. PAUL ROBERTSON, PETER SAVAGE, SUDHA S. SHANKAR, DARKO STEFANOVSKI, MARIA
T. VASSILEVA, ADRIAN VELLA, KATHRYN F. WRIGHT, DAVID A. FRYBURG, FOR
FOUNDATION FOR NIH BETA CELL PROJECT TEAM, Frankfurt, Germany, Skillman,
NJ, Seattle, WA, Bethesda, MD, Indianapolis, IN, Philadelphia, PA, Rochester, MN,
East Lyme, CT
273‑LB
Although it is known that meal ingestion stimulates gut enteroendocrine
secretion (ES) and BCF, the relationship between ES and BCF is not known
across GT populations. In studies examining BCF in subjects with normal
glucose tolerance (NGT), prediabetes (PDM), and type 2 DM (T2DM), total
and active GLP-1, GIP, PYY, and glucagon (glgn) were measured before and
after a mixed meal (MTT). We hypothesized that these responses were associated with BCF. ES was assessed in overnight fasted subjects before and
30, 60 and 120 min after 470 kCal MTT. Table summarizes responses preand 30-min post MTT. Parameters of insulin secretion (Φtot) and sensitivity
(SI) and disposition index (DItot) were estimated using minimal model. BCF:
ES association was conducted using Spearman’s Rank correlations. Before
the MTT, ES was generally higher for T2DM versus NGT and PDM. MTT increased total and active GLP-1, GIP and PYY at 30 min. Changes were generally comparable across GT populations except glgn which showed increases
across the GT Populations NGT<PDM<T2DM (ANOVA p<0.001). Corr analysis
revealed no strong relationships between ES at baseline or 30 min postMTT, with SI, Φtot or DItot.
Conclusion: ES is not impaired after MTT in PDM and T2DM, yet there is
no apparent correlation between ES and BCF, suggesting a defect in BCF
rather than the ES in PDM and T2DM.
Table.
Investigating Translation of Kisspeptin as a Target Engagement Bio‑
marker for Glucagon and GLP1/GCGR Receptor Co-agonists
POSTERS
Integrated
Physiology/Obesity
FRANKLIN LIU, JULIE LAO, HAIHONG ZHOU, CARLOS G. RODRIGUEZ, LEI CHEN,
ERIC MUISE, MICHAEL E. LASSMAN, ANDREA NAWROCKI, STEPHEN PREVIS,
DAVID E. KELLEY, SANDRA C. SOUZA, Kenilworth, NJ, Rahway, NJ
Glucagon-like peptide 1 and glucagon receptor (GLP1R/GCGR) co-agonism
has been investigated for the treatment of T2D. While there are methods for
assessing GLP1 activation, less is known about surrogate markers for GCGR
activation. It has been recently reported that glucagon stimulates production of Kisspeptin (Kiss) (Cell Metab 2014, 19:667) and Kiss was shown to be
elevated in serum of humans with T2D and serum and livers in mouse models of metabolic dysfunction. These observations suggest Kiss is a potential
biomarker for GCGR activation, and our laboratory investigated the use of
Kiss to monitor GCGR target engagement. In agreement with reported in
vivo data, Kiss mRNA levels were increased in the liver of DIO mice acutely
treated with GLP1R/GCGR co-agonists relative to vehicle or GLP1R agonists.
In cultured primary mouse hepatocytes, based on mRNA expression data,
Kiss was among the top 10 predicted secreted proteins acutely regulated
by glucagon, oxyntomodulin and GLP1R/GCGR co-agonists. Increased Kiss
mRNA expression was stimulated by glucagon in human hepatocytes and
consistent with GCGR specificity, this increase was blocked by a GCGR
antagonist. A LC/MS assay developed for Kiss quantification determined
that plasma Kiss levels were elevated in T2D compared to healthy donors,
but not to the level previously reported. Unexpectedly, human hepatocytes
treated with GLP1R/GCGR co-agonists failed to increase Kiss mRNA expression, raising questions on the utility of circulating Kiss as a biomarker for
GCGR agonism in clinical studies. Evaluation of Kiss in humans treated with
glucagon or GCGR agonists may determine the utility of Kiss as a biomarker
for GCGR activation and increase understanding the metabolic role of Kiss
in mice vs. humans.
274‑LB
Role of C-terminal VGF-derived Peptides on Insulin Secretion and
Glucose Homeostasis
CHERYL CERO, PAMELA PETROCCHI-PASSERI, ALESSANDRO CUTARELLI, CLAUDIO FRANK, CINZIA SEVERINI, ROBERTA POSSENTI, ALESSANDRO BARTOLOMUCCI, Minneapolis, MN, Rome, Italy
Supported By: Foundation for the National Institutes of Health Biomarkers Consortium
One of the most common features of early type 2 diabetes mellitus
(T2DM) is low insulin secretion for the degree of insulin sensitivity which
is commonly reduced in this disease. The abundant presence of the granin
protein VGF (nonacronymic) in pancreatic islets suggests that some of its
ADA-Funded Research
For author disclosure information, see page LB98.
LB68
Integrated Physiology—Other Hormones
276‑LB
GLP-1R with GLP-1, Exendin-4 (Ex4) or Liraglutide (Lira) for 0, 5, 10, 15, 30, or
60 minutes (all 100nM). No differences in ACC or ERK1/2 phosphorylation
were observed between these GLP-1R agonists. Ongoing experiments are
testing effects of these GLP-1R agonists on Akt, AMPK, and CREB phosphorylation. We then tested the hypothesis that GLP-1R agonists may differentially target specific hypothalamic nuclei. Food intake was measured in
response to targeted injections of GLP-1 vs. Ex4 into the ARC, paraventricular nucleus (PVN) or ventromedial hypothalamus (VMH) in C57Bl/6 mice. Our
results demonstrate that Ex4 suppressed food intake when targeted to the
ARC, PVN, and VMH in a dose-dependent manner while GLP-1 only reduced
food intake when targeted to the PVN, but with a magnitude lower than Ex4.
In sum, our preliminary data indicate that different GLP-1R agonists do not
engage distinct signaling pathways in POMC neurons of the ARC. Instead,
the anorectic potential of GLP-1R agonists may be determined by the brain
region engaged by these peptides. Further studies will investigate other
signaling cascades as well as other brain regions to further elucidate the
mechanisms underlying Glp-1r agonist differences in anorectic potency.
Insulin-like Peptide 5 (INSL5) in Patients with Type 2 Diabetes
JENNY E. BLAU, MARY F. WALTER, VIVIANA BAUMAN, KRISTINA I. ROTHER,
Bethesda, MD
Insulin-like peptide 5 (INSL5), a member of the insulin/relaxin superfamily, is a product of enteroendocrine L cells, known to secrete glucagon-like
peptide 1 (GLP-1). INSL5 and its receptor have recently been proposed as
targets for diabetes drug development due to the glucose dependent, direct
insulinotrophic effect on beta cells (shown in vitro studies in rodent islets)
and due to INSL5’s potential auto/paracrine effect on promoting GLP-1 secretion. Little is known about INSL5’s function and regulation in humans. We
tested 13 healthy, normal weight and obese individuals with and without
type 2 diabetes mellitus (T2DM). INSL5 was measured with an RIA (Phoenix
Pharmaceuticals, range 20-2560 pg/ml) after an overnight fast (>8 hours),
and in 2 subjects after 16 and 60 hours of continued fasting. Eight participants underwent an oral glucose tolerance test (OGTT). In non-diabetic lean
and obese individuals (n=8), concentrations were at or below the lower limit
of detection and remained undetectable after a prolonged fast. In contrast,
in patients with T2DM, INSL5 was detectable (n=5) and increased with glucose administration. The highest value (163 pg/mL) was found in an obese
patient with poorly controlled T2DM (BMI 36 kg/m2, HbA1c 10.6%). Based
on these preliminary results, we hypothesize that INSL5 may play a compensatory role in individuals with T2DM to counterbalance the prevailing
relative insulin deficiency.
Supported By: American Diabetes Association (1-14-CD-01 to J.E.A.)
279‑LB
GIP (3-30) Is a Potent Glucose-dependent Insulinotropic Polypep‑
tide (GIP) Receptor Antagonist In Vitro and In Vivo
LÆRKE S. HANSEN, ALEXANDER H. SPARRE-ULRICH, BERIT SVENDSEN, MIKKEL
CHRISTENSEN, BOLETTE HARTMANN, FILIP K. KNOP, JENS JUUL HOLST, METTE
M. ROSENKILDE, Copenhagen, Denmark, Hellerup, Denmark
277‑LB
The intestinal hormone glucose-dependent insulinotropic polypeptide
(GIP) functions within lipid, bone, and glucose homeostasis. The human GIP
receptor (hGIP R) is GαS-coupled and 7TM family B. High affinity ligands will
be important tools to explore the role of GIP in adiposity, osteogenesis, and
glucose homeostasis. hGIP (1-30) is suggested to be a naturally occurring
GIP variant in humans. We here show that hGIP (3-30) - a presumed DPP-IVdegradation product of hGIP (1-30), is a potent antagonist in vitro and in vivo
with high affinity to the human GIP R. All in vitro assays were performed on
transiently transfected COS-7 cells expressing hGIP R. Radiolabeled 125IhGIP (1-42) was used for competition binding, and cAMP-accumulation was
measured using an enzyme fragment assay. In situ pancreas perfusions in
rats were performed with a single-pass system (10 mM glucose) through
arteries and collected effluent from the portal vein. hGIP (3-30) displaced
125I-hGIP (1-42) with high affinity (IC50 of 2.6nM [logIC50 -8.6±0.04, n=12),
thus with an affinity close to hGIP (1-30) and hGIP (1-42) (IC50 of 0.89nM
and 0.67nM). In the cAMP assay, hGIP (3-30) did not stimulate hGIP R but
showed potent antagonistic properties with a dose-dependent right-shift
of the hGIP (1-42) dose-response curve on 4-fold for 100nM hGIP (3-30).
Schild plot analysis revealed competitive antagonistic properties of hGIP (330) with a Ki of 15nM (Hill-slope 0.93±0.02). The antagonistic property was
confirmed in pancreas perfusion studies, where 100nM hGIP (3-30) reduced
glucagon and significantly somatostatin secretion induced by 1nM GIP (1-42),
whereas it stimulated de novo and potentiated hGIP (1-42)-induced insulin
secretion. GIP (3-30) is a highly potent competitive antagonist of the hGIP
receptor. Given its presumed presence in the human body, it could serve as
tool compound for further elucidation of the GIP physiology and thereby in
turn for future pharmacological intervention of this system.
Sleeve Gastrectomy Improves the Glycemic State in a Glucose In‑
tolerant Lipocalin Prostaglandin D2 Synthase (L-PGDS) Knockout
Mouse Model
SUNIL KUMAR, RAYMOND G. LAU, THOMAS PALAIA, CHRISTOPHER E. HALL,
KENETH HALL, COLLIN BRATHWAITE, LOUIS RAGOLIA, Mineola, NY
Sleeve gastrectomy (SG), ameliorates metabolic complications in obese
and diabetic subjects. Recently, L-PGDS has been considered an emerging
target for diabetes and metabolic disorders; however, the mechanism involved in the regulation of glucose metabolism is not fully understood yet. As
per our previous studies, L-PGDS knockout mice showed accelerated glucose
intolerance and insulin resistance. Therefore, in this study, we examined the
role of L-PGDS in diabetes and metabolic syndrome using L-PGDS knockout
(KO) mice which underwent sleeve gastrectomy (SG). The aim of the study
was to determine the effect of sleeve gastrectomy on the glucose intolerated L-PGDS knockout mice model. L-PGDS knockout mice were divided into
two groups, sham surgery (n=4) and sleeve gastrectomy (n=4). Mice were
kept on diabetogenic diet and all the fasting parameters were measured 12
weeks post surgery. Data were analyzed by unpaired t-test with the significance (p<0.05). Results of our oral glucose tolerance test with the challenge
of 2gm/kg glucose dose showed significant glycemic improvement in the SG
group compared to the sham group and clearly depicted the beneficial effect
of sleeve gastrectomy. Surprisingly, there was no difference in fasting insulin level in both the groups. Bile acid and peptide YY levels in the SG group
were significantly increased by 2.7 fold and 3.7 fold respectively, compared
to sham group. We measured the pre and post surgery weight in both the
groups and found that the SG group gained 16.5% less weight compared to
the sham group. Leptin levels were also increased by 8.4% in the SG group
compared to the sham group. Collectively, based on the present results, it can
be concluded that SG ameliorated metabolic disorder in glucose intolerated
L-PGDS knockout mice model and proved the strong correlation between LPGDS and sleeve gastrectomy. Further studies need to be performed to find
the actual mechanism of action of L-PGDS in sleeve gastrectomy.
278‑LB
Activation of GPR119 highly expressed in pancreas and intestine is known
to be involved in glucose and lipid metabolism. There are few reports on
chronic efficacy in disease animal model and some GPR119 agonists suggested an issue on loss of effect after repeated administration. To demonstrate the long-term efficacy of our novel GPR119 agonist therefore, DA-1241
was administered for 10 weeks in a progressive diabetic mice model induced
by streptozotocin (STZ) injection with a high-fat diet (HF) feeding to causes
dysregulation of glucose and lipid metabolism. HF/STZ control mice showed
overt hyperglycemia, while DA-1241 treatment significantly suppressed
blood glucose rise from two weeks after administration and its efficacy persisted during the rest of the treatment period. Hypertriglycemia and fatty
liver were attenuated by DA-1241 treatment as well, indicating simultaneous
glucose and lipid control at the same dose. Preserved islet structure and
higher beta cell mass in DA-1241-treated group support its glucose-lowering
effect. However, GSK263A, an another GPR119 agonist, showed no signifi-
Probing Mechanisms for the Differential Anorectic Effects of Glu‑
cagon-like Peptide-1 (GLP-1) Receptor (GLP1R) Agonists
JACOB D. BROWN, MELISSA A. BURMEISTER, JENNIFER E. AYALA, JULIO E.
AYALA, Orlando, FL
GLP-1 is a gut hormone known for its insulinotropic and satiety-promoting
effects. Type 2 diabetes therapies that elevate GLP-1 levels (DPP-4 inhibitors) are weight neutral while GLP-1 mimetics (e.g. Exenatide, Liraglutide)
cause weight loss via reduced food intake. Using cell-based and in vivo
methods, we aimed to elucidate the mechanism underlying this divergence
in anorectic effects between GLP-1R agonists. We hypothesized that GLP-1
and GLP-1 mimetics induce divergent intracellular signaling cascades in satiety-promoting proopiomelanocortin (POMC) neurons of the arcuate nucleus
(ARC). We tested this by measuring phosphorylation of acetyl CoA carboxylase (ACC) and ERK1/2 after treating POMC-derived cells overexpressing the
ADA-Funded Research
For author disclosure information, see page LB98.
LB69
POSTERS
MI-KYUNG KIM, TAE HYOUNG KIM, YE-HWANG CHEONG, YU NA CHAE, ILHOON JUNG, KWAN-HOO LEE, SEUL MIN CHOI, JAE SUNG YANG, MOON-HO
SON, KYUNG KOO KANG, Yongin, Republic of Korea
Integrated
Physiology/Obesity
280‑LB
Long-Term Treatment of DA-1241, a Novel GPR119 Agonist, Improved
Glucose Control via Preserved Beta Cell Mass in a Progressive Dia‑
betic Mice Model
Obesity—Animal
cant effects on glucose control and pancreatic beta cell mass, with only a
trend of a decrease in hepatic triglycerides. Then we investigated underlying
mechanisms of the effect on beta cells. DA-1241 protected beta cells from
death caused by endoplasmic reticulum stress through reducing the expression of stress molecules and stimulated beta cell replication, which may partially account for the higher beta cell mass in DA-1241-treated HF/STZ mice.
Taken together, this study suggested that i) DA-1241 has a chronic glucoselowering effect without tachyphylaxis issue, ii) the metabolic improvement
on glucose and lipid by DA-1241 treatment can be observed at a same dose
level, and iii) DA-1241 has a direct beneficial effect on pancreatic beta cells,
which may partially contribute to its anti-diabetic effect.
impaired. It is possible that hepatic FGF21 inhibits lipolysis while promotes
lipid uptake in adipocytes. These data collectively suggest that circulating
FGF21 is mainly derived from the liver. Hepatic FGF21 regulates lipid metabolism in adipocytes, and therefore protects mice against diet-induced
hyperglycemia and insulin resistance possibly via reducing ectopic lipid accumulation in non-adipose tissues such as the liver and skeletal muscles.
Supported By: Collaborative Research Fund Group Research Projects of Hong
Kong
283‑LB
Liraglutide Reduces Lipogenetic Signals in Visceral Adipose of Db/
db Mice with AMPK Activation and A Akt Suppression
YIMIN SHAO, GEHENG YUAN, JUNQING ZHANG, XIAOHUI GUO, San Diego, CA,
Beijing, China
Obesity—Animal
Liraglutide, a glucagon-like peptide-1 (GLP-1) analogue, has been proved to
reduce body weight and visceral adipose tissue (VAT) in human studies. In
this study, we aimed at examining lipogenetic signals changes in VAT after
weight-loss with liraglutide in db/db mice. The mice were divided into 2 groups:
liraglutide-treated group (n=14, 8-week old, fasting glucose>10mmol/l, liraglutide 300μg/kg twice a day for 4 weeks) and control group (n=14, saline).
We found body weight gain, food intake were reduced after liraglutide treatment (p<0.05). Compared to the control group, the VAT weights were significantly lower in the treated group (2.32±0.37g vs. 3.20±0.30g, p<0.01) than
that in control group. In VAT, compared with control group, the lipogenetic
transcription factors peroxisome proliferator-activated receptor-γ (PPARγ)
and CCAAT/enhancer-binding protein-α (C/EBPα) expressions were both reduced with phospho-Adenosine 5’-monophosphate-activated protein kinase
(pAMPK) and phospho-acetyl-CoA carboxylase (pACC) increased 3.5-fold
and 2.31-fold respectively, while the phospho-serine/threonine kinase Akt
(pAkt) and phospho-p38 mitogen-activated protein kinase (pP38MAPK) were
reduced 0.38-fold and 0.62-fold respectively (p<0.01). In conclusion, VAT was
reduced after weight loss with AMPK activation and Akt suppression with
liraglutide treatment, which was associated with reduction of lipogenetic
process in VAT.
281‑LB
Withdrawn
284‑LB
Lipoprotein Lipase Represses SND1, a Novel SREBP-regulated
Gene, to Improve the Adipose Tissue Phenotype of Mice
BEIBEI ZHU, PHILIP A. KERN, BRIAN S. FINLIN, Lexington, KY
Lipoprotein lipase (LpL) hydrolyzes the triglyceride core of lipoproteins and
also acts as a bridge to allow for the uptake of the hydrolyzed cholesterolrich remnant particle. Transgenic mice that express LpL in adipose tissue
under the control of the adiponectin promoter (AdipoQ-LpL) have improved
glucose metabolism when challenged with a high fat diet. This is mediated
by an improved adipose phenotype, including increased expression of the
anti-inflammatory adipokine adiponectin. To identify the mechanism for
reduced inflammation, we performed a microarray on adipose tissue from
mice challenged with a high fat diet for 10-days. Pathway analysis of the
microarray revealed that genes regulated by sterol regulated elementbinding protein (SREBP) transcription factors were repressed; this could
be caused by increased remnant uptake by the transgene. One of the most
significantly repressed genes was SND1 (P<0.001). Since SND1 is implicated
in cholesterol metabolism in the liver, we determined whether it is also an
SREBP-regulated gene in adipocytes by treating differentiated 3T3L1 adipocytes with SREBP2 siRNA. This treatment significantly repressed SND1
mRNA 2.2 fold (P=0.015). Since SND1 is pro-inflammatory in the liver, we
next determined whether reducing SND1 would dampen adipocyte inflammatory responses. We treated differentiated 3T3L1 adipocytes with control or SND1 siRNA and then treated the cells with 100 ng/mL recombinant
tumor necrosis factor (TNF) alpha. The SND1 siRNA treated cells had 1.9
fold lower MCP1 expression in response to TNF alpha than control siRNA
treated adipocytes (P<0.05). Consistent with this, IL-1 beta, IL-6, and TNF alpha were also lower in SND1 siRNA treated adipocytes (P<0.05). These data
suggest that SND1 is an important link between SREBP2 and inflammation
in adipocytes. Reducing SND1 by inhibiting the SREBP2 pathway in adipose
tissue may be part of the mechanism of improved adipose tissue function in
AdipoQ-LpL mice.
282‑LB
Hepatic FGF21 Protects Mice against Diet-Induced Lipid Dys­
regulation and Insulin Resistance
POSTERS
Integrated
Physiology/Obesity
ZHE HUANG, TSZ-HANG LEE, CHI-MING WONG, KAREN SIU-LING LAM, AIMIN
XU, Hong Kong, China
Fibroblast growth factor 21 (FGF21) is a potent metabolic hormone produced by a number of organs. It has been shown to confer multiple metabolic benefits on obesity. Therapeutic administration of FGF21 or its analog
protects against diet-induced obesity and hyperglycemia in both rodents and
humans. However, the physiological roles of FGF21 remain ambiguous. Since
the liver is the major source of circulating FGF21, we propose that the endocrine actions of FGF21 derived from the liver may account for its metabolic
effects on lipid metabolism. We therefore generated the liver-specific FGF21
KO (LiverKO) mice by utilizing the Cre-loxP recombination system. LiverKO
mice and their age-matched wild-type (WT) littermates were fed a high fat
diet (HFD) for 20 weeks and assessed for the metabolic phenotypes. Circulating FGF21 was significantly elevated in WT mice during fasting or HFD
feeding. However, this elevation of circulating FGF21 was completely abolished in LiverKO mice, suggesting the liver is the major source of circulating
FGF21. LiverKO mice treated with HFD showed a significant reduction in body
fat mass when compared to WT mice, as revealed by NMR body composition analyzer suggesting resistance to obesity was mainly attributed to the
loss of hepatic FGF21. Interestingly, although LiverKO mice were leaner, they
developed more severe glucose intolerance and insulin resistance after HFD
feeding as shown by GTT and ITT. In addition, LiverKO mice had higher serum
triglyceride and free fatty acid levels suggesting that lipid homeostasis is
Supported By: P20GM103527-06; DK039176; UL1TR000117; DK071349
ADA-Funded Research
For author disclosure information, see page LB98.
LB70
Obesity—Animal
285‑LB
anti-obesity and anti-diabetic properties. SR4 increased mitochondrial respiration, dissipated mitochondrial membrane potential, induced mitochondrial
swelling, and depleted ATP in cells and liver mitochondria. Oral feeding of SR4
significantly reduced body weight gain, prevented hyperlipidemia and insulin
resistance, and improved glycemic control in both high fat-diet induced obese
and diabetic db/db mice. SR4 treatment also decreased liver triglycerides and
prevented hepatic steatosis in both animal models. Mitochondrial uncoupling
by SR4 results to activation of AMPK, leading to the phosphorylation and inhibition of acetyl-CoA carboxylase, an inhibitor of mitochondrial β-oxidation.
Gene analyses by real time PCR showed SR4 significantly suppressed the
mRNA expression of several lipogenic genes as well as gluconeogenic genes
in the liver of obese mice. RNA sequencing results showed that 689 genes
were differentially expressed in liver of db/db mice after SR4 treatment (122
upregulated, 567 downregulated). Gene ontology analysis by DAVID indicated
up-regulated amino acid metabolism and down-regulated cell division and cell
cycle processes. These data demonstrates that SR4 may be a promising compound for treatment of T2DM and obesity.
The Anti-obesity Action of ACAM by Modulating the Dynamics of
Cell Adhesion and Actin Polymerization in Adipocytes
KAZUTOSHI MURAKAMI, JUN EGUCHI, ATSUKO NAKATSUKA, TOMOKAZU
NUNOUE, JUN WADA, Okayama, Japan
We identified adipocyte adhesion molecule (ACAM) which belongs to CTX
gene family. ACAM is predominantly expressed in white adipose tissues and
up-regulated in obese subjects. Two immunoglobulin-like domains exist in extracellular segment and they are involved in the adhesion process and homophilic
aggregation of the cells. To explore the functional role of ACAM in obesity, we
generated ACAM transgenic (Tg) mice driven by aP2 promoter. Under high fat
high sucrose (HFHS) diet, the increase in body weight was significantly reduced
in Tg mice compared with wild type (WT) mice and the fat pad weight and adipocyte size in Tg mice were reduced. In glucose tolerance and insulin sensitivity
tests, plasma glucose levels were significantly lower in Tg mice. To further give
insights into the mechanism for the reduction of lipid accumulation in adipose
tissues, we investigated the role of ACAM by using 3T3-L1 cells and Tg mice. As
a result, we identified γ-actin as interacting proteins forming protein complexes
with ACAM. Next, we investigated the expression of ACAM and polymerized
form of actin (F-actin) by Phalloidin staining. In WT mice under HFHS diet, both
F-actin and ACAM were faintly stained surrounding the adipocytes in epididymal
adipose tissues, while they colocalized and accentuated in a patchy fashion. By
transmission electron microscopy, in WT mice under HFHS diet the distance of
plasma membranes between adjacent adipocytes was ~100-200 nm. In contrast,
we confirmed the zone with an intercellular space of ~10-20 nm, the structure
of zonula adherens, in Tg mice fed HFHS diet. By immunoelectron microscopy,
the zonula adherens was associated with immunogold particles when the sections were stained with γ-actin or ACAM-specific antibodies. In conclusion, the
ACAM-mediated homophilic adhesion of adipocytes and formation of zonula adherens promoted the actin polymerization inhibited the adipocyte hypertrophy,
which resulted in the improvement of obesity.
Supported By: Isaac and Jacquelin Moradi; City of Hope National Medical
Center; Beckman Research Institute
Blood Glucose Control by AgRP Neurons and Glutamate
288‑LB
AYKUT G. ÜNER, GABRIEL H.M. GONÇALVES, WENJING LI, MATHEUS PORCE­
BAN, ONUR KEÇIK, NICOLE CARON, MILENA SCHÖNKE, ERIC DELPIRE, KENJI
SAKIMURA, YOUNG-BUM KIM, CHRISTIAN BJØRBÆK, Boston, MA, Nashville,
TN, Niigata, Japan
This study investigates the role of N-methyl-d-aspartate receptors (NMDARs) in agouti-related peptide (AgRP) and pro-opiomelanocortin (POMC)
neurons on glucose homeostasis. Hypothalamic AgRP and POMC neurons play
critical roles in control of energy balance. These neurons can also orchestrate
beneficial blood glucose control, but the underlying processes are not understood. NMDARs typically consist of the obligatory GluN1 subunit and different
GluN2 subunits, the latter exerting differential effects on channel activity and
neuronal functions. Glutamatergic input via NMDARs is pivotal for regulation
of neuronal activity and plasticity. Currently, the role of NMDARs and specific
GluN2 subunits in AgRP and POMC neurons on glucose homeostasis regulation is unknown. To investigate this, we used cre-lox technology to delete
GluN2A or GluN2B from AgRP or POMC neurons in mice. We show that loss of
GluN2B from AgRP neurons reduces body weight, fat mass, and food intake,
whereas GluN2B in POMC neurons and GluN2A in AgRP or POMC neurons are
not required for normal energy balance. Deletion of GluN2B in AgRP neurons
reduces the number of AgRP neurons and dendritic length. Remarkably, loss
of GluN2B in AgRP neurons of the obese and severely diabetic Lepob/ob mice
fully corrects hyperglycemia, without influencing body weight and food intake.
These mice are also more sensitive to leptin’s anti-obesity actions. Finally, to
selectively assess the ability of neuronal activity to control blood glucose balance, we activated AgRP neurons by DREADD (designer receptors exclusively
activated by designer drug) technology and observed an increase in fasted
glucose levels in lean mice. The results show that GluN2B-NMDARs in AgRP
neurons can regulate body weight and blood glucose levels, and suggests that
these effects involve altered AgRP neuronal activity/structure and modulation
of central leptin action. Inhibition of GluN2B-NMDARs in AgRP neurons may be
considered an avenue for development of novel anti-diabetes and anti-obesity
therapies.
Supported By: Japan Ministry of Education, Culture, Sports, Science and Technology (26461362)
286‑LB
Female Mice Fed a Western Diet Demonstrate Mineralocorticoid
Receptor-mediated Ultrastructural Remodeling of Perivascular
Adipose Tissue and Aortic Stiffness
MELVIN HAYDEN, VINCENT DEMARCO, JAMES R. SOWERS, Columbia, MO
Perivascular adipose tissue (PVAT) is considered to be more than a mechanical structural support of the aorta vasculature and is capable of producing
aldosterone. To explore diet-related changes in PVAT female mice were fed a
high fat/high fructose (western) diet (WD) for 16 weeks. Descending thoracic
aortas with intact PVAT were examined by transmission electron microscopic
(TEM). WD fed mice developed in vivo aortic stiffness, as demonstrated by an
increase in pulse wave velocity, and endothelial and vascular smooth muscle
stiffness, assessed ex vivo by atomic force microscopy. PVAT tissue was
comprised of white-like (WAT) and brown-like adipose tissue (BAT) with BAT
adipocytes predominating. In the WD mice, PVAT remodeling consisted of attenuation of the innermost region of WAT adipocytes, increases in mast cells,
lymphocytes and macrophages and collagen deposition, all of which were
prevented with low-dose spironolactone (LSp). In concert with these TEM
changes, LSp attenuated the WD-induced increase in aortic stiffness. Because aortic stiffening may be the nexus between cardiovascular, kidney and
cerebral vascular disease, especially in obese, insulin resistant and diabetic
women, these TEM and functional findings may have translational importance
to the current obesity epidemic which is driven by consumption of a WD.
Clc-5 Deficient Mice, a Novel Murine Model for Investigating the
Role of Gut Microbiota in Obesity and Metabolic Syndrome
YING DONG, SHI JIN, XUHANG LI, Baltimore, MD
We have identified Clc-5 knockout (Clc-5KO) mice as a completely novel animal
model of obesity and metabolic syndromes. Clc-5 (chloride channel 5) functions
primarily as an electrogenic 2Cl-/1H+exchanger. A phenotype of Clc-5 deficient
mice is strikingly similar to human Dent’s disease. Recently, we have identified
a unique and previously unrecognized phenotype of Clc-5KO mice: they are all
(100%) markedly obese on regular diet, with a body weight 25-35% higher than
age-matched WT mice. QNMR showed that Clc-5KO mice were constituted of
21% of total body fat (only 7% in WT). MRI analysis indicated a dramatic increase in both subcutaneous and visceral (abdominal) fats. All Clc-5KO exhibited
glucose intolerance and >3-fold elevated levels of systemic proinflammatory IL-6
and MCP-1 (than WT), remarkably similar to those in human obesity. They also
exhibit a 3-10-fold increase in the expression of a panel of diabetes/obesityrelated genes in the liver, including PPARγ, LXRα, RXRα, CD36, SRA (class A
scavenger receptor), leptin-R, SREBP2, AMPKβ, and GHRP-R, all of which are the
hallmarks of metabolic syndromes. More surprisingly, Clc-5KO mice had similar
food assumption as the age-matched WT, suggesting that they acquire a more
287‑LB
SR4, a Novel Mitochondrial Uncoupler, Improves Metabolic Altera‑
tions in Obese and Diabetic Mice
JAMES L. FIGAROLA, JYOTSANA SINGHAL, GEORGE W. ROGER, CHARLES WARDEN, LU YANG, XIWEI WU, TIMOTHY SYNOLD, SHARAD S. SINGHAL, DAVID
HORNE, SAMUEL RAHBAR, ARTHUR RIGGS, Duarte, CA, Billerica, MA
The number of people suffering from type 2 diabetes mellitus (T2DM) is
skyrocketing worldwide and has been closely linked to the soaring obesity
epidemic. T2DM if left untreated, can cause severe and sometimes fatal complications. Most current treatments ameliorate the hyperglycemic symptom
of the disease but are not effective in correcting its underlying cause. Development of new drugs with new mechanisms of action, in particular those
targeting the cause of insulin resistance, is important to improve diabetes
therapy. Recent studies have shown that targeting mitochondrial respiration,
specifically by mild uncoupling agents, is very promising in treating T2DM
symptoms. Here, we show that SR4 is a novel mitochondrial uncoupler with
ADA-Funded Research
For author disclosure information, see page LB98.
LB71
POSTERS
289‑LB
Supported By: National Institutes of Health (R01HL073101, R01HL107910); U.S.
Department of Veterans Affairs (to J.R.S.)
Integrated
Physiology/Obesity
Supported By: National Institutes of Health (R01DK94040 to C.B.)
Obesity—Animal
efficient dietary energy harvesting mechanism. We found a weakened bacterial
killing capacity of the macrophages in Clc-5KO compared to those in WT. Cocaging littermate WT with Clc-5KO mice led to a marked improvement of glucose
intolerance and decreased body fats in Clc-5KO mice while an impaired glucose
intolerance in WT. These data clearly indicate that it is the altered intestinal flora
that enable the Clc-5KO mice a higher energy-harvesting efficiency from dietary
foods, while the WT microbiota can diminish this efficiency. We conclude that
Clc-5 plays a critical and previously unrecognized role in lipid/glucose metabolism via modulating gut flora, and Clc-5KO mice can be used as a novel model of
obesity, diabetes or metabolic syndromes.
creased immune cell infiltration in fat depots preserves metabolic health in
obesity remains though unclear. Accordingly, we studied the role of endothelial expressed P-selectin in insulin sensitivity in mice with DIO. Wild-type
(WT) and P-selectin deficient (Psel-/-) C57BL/6 mice were given ad libitum
access to either a low fat (10% fat) or a high fat (60% fat) chow for 16 weeks.
No differences in total body weight gain, adiposity, or fasting plasma glucose were recorded between the WT and Psel-/- (p<0.01 vs. low fat WT).
Mice were then studied by intravital microscopy (IVM) to measure kinetics
of leukocyte rolling (LR) and leukocyte adhesion (LA) in the microcirculation
of the mesenteric fat pads. In WT mice, administration of high fat food increased LR and LA in the visceral fat microcirculation (p<0.001 vs. low fat
WT). In contrast, high fat feeding failed to increase LR and LA in P-sel-/- mice
(NS vs. low fat WT). High fat fed WT and Psel-/- mice showed no differences in glucose tolerance tests and insulin sensitivity tests (p<0.01 vs. low
fat WT). Fasting insulin levels were elevated in both WT and Psel-/- DIO
mice (p<0.05 vs. low fat WT). Serum TNFa concentrations were significantly
elevated in WT high fat fed mice as compared to both WT low fat fed and
Psel-/- high fat fed mice (p<0.05). Taken together, these data indicate that Pselectin deletion protects against local and systemic inflammation following
high fat feeding but has no effect on insulin sensitivity. These data suggest
that blockade of immune cell accumulation in visceral adipose depots alone
may not reduce insulin resistance associated with obesity.
Supported By: National Institutes of Health-National Institute of Diabetes and
Digestive and Kidney Diseases
290‑LB
Withdrawn
Supported By: R01DK096521 (to R.S)
293‑LB
Myeloperoxidase Downregulates Adiponectin Receptor Signaling
in Endothelial Cells via Activation of Calpain
ZIENAB A. ETWEBI, ROSARIO SCALIA, Philadelphia, PA
Obesity and type 2 diabetes mellitus have been associated with insulin
resistance, and chronic low-grade inflammation. Myeloperoxidase (MPO)
is a peroxidase enzyme secreted by activated neutrophils, which is associated with endothelial dysfunction and, more recently, insulin resistance. The
calcium dependent protease calpain has also been associated with insulin
resistance and type 2 diabetes. Accordingly, we tested the hypothesis that
MPO downregulates adiponectin receptor function in endothelial cells via
activation of calpain. Mouse lung microvascular endothelial cells (MMVEC)
were stimulated with 10 nM MPO for 30, 60, 120, 180, 240 minutes. Levels
of adiponectin receptor 2 (AdipoR2) and calpain, along with the downstream
target of adiponectin signaling 5’ AMP activated protein kinase (AMPK),
were measured by immunoblot analyses. MPO time dependently decreased
AdipoR2 abundance (P<0.0001) while significantly increased µ-calpain activity (p<0.0001). Pretreatment of MMVECs with the selective calpain inhibitor
ZLLAl (100 µM) prevent MPO-induced calpain activation (P<0.0001 vs. MPO
alone), and preserved AdipoR2 abundance (P<0.01 vs. MPO alone). Inhibition
of calpain activity also increased AMPK phosphorylation levels in the face
of MPO (p<0.001 versus MPO alone). At the transcriptional level, we found
evidence of increased AdipoR2 mRNA levels in MMVEC exposed to MPO.
Taken together, our data first demonstrate a role for calpain in the downregulation of adiponectin receptor signaling in states of leukocyte-mediated
endothelial inflammation.
291‑LB
Actin Filament-associated Protein 1 Is a Novel Regulator of Glucose
and Lipid Metabolism
POSTERS
Integrated
Physiology/Obesity
JAYDE T. HOOVEN, JOSEPH MAUCERI, STEPHEN J. COLLINS, HOLLY CORKILL,
JESS M. CUNNICK, YOUNGJIN CHO, Scranton, PA
With the current epidemic of obesity leading to an increase in the prevalence of type 2 diabetes, the discovery of the new molecular mechanisms
that regulate lipid and glucose metabolism is vital to the development of
therapeutic interventions. Recent studies have shown that members of the
Src family of kinases contribute to numerous physiological functions including the regulation of glucose homeostasis and lipid metabolism. Actin Filament Associated Protein 1 (AFAP1) is an adaptor protein of Src family kinases,
including Src and Fyn. We have shown that AFAP1 physiologically regulates
the activity of Src. We now show, that in mice that no longer express AFAP1,
glucose tolerance and insulin sensitivity are enhanced compared to wild
type controls. Furthermore, the average weight and visceral adiposity of the
AFAP1 knockout mouse is reduced. Interestingly, mice no longer expressing AFAP1L2, an isoform of AFAP1, also show improved glucose tolerance
and reduced total body fat compared to wild type mice (International Mouse
Phenotyping Consortium). These findings suggest that AFAP1 regulates glucose utilization and lipid storage in response to insulin and that AFAP1 may
provide a therapeutic target for the treatment of diabetes.
Supported By: R01DK096521 (to R.S.)
294‑LB
The Role of the Duffy Antigen Receptor for Chemokines in Meta‑
bolic Disease
TYLER W. BENSON, TAPAN K. CHATTERJEE, DANIEL S. WEINTRAUB, ORISHE­
BAWO B. POPOOLA, BRAIN STANSFIELD, KAN HUI YIEW, MATTHEW J. CROWE,
JAMES MINTZ, JULIA BRITTAIN, DAVID W. STEPP, VLADIMIR BOGDONOV, NEAL
L. WEINTRAUB, Augusta, GA, Cincinnati, OH
Inflammation in adipose tissues contributes to obesity-related insulin resistance and metabolic disease, a growing worldwide problem. The Duffy Antigen
Receptor for Chemokines (DARC) is expressed on erythrocytes and regulates
inflammation by binding chemokines such as MCP-1 to buffer inflammatory
responses. DARC allele variants protect against malaria and are prevalent in
certain African and Asian populations. We hypothesized that genetic deletion
of DARC would augment adipose tissue inflammation and glucose intolerance
in the setting of diet-induced obesity. Eight week-old male Wild Type (WT)
and DARC-/- mice (C57BL/6 background) were maintained either on chow diet
or switched to high fat diet (HFD, 60% calories from fat) for up to 24 weeks.
Thereafter, metabolic phenotyping was performed, mice were subsequently
euthanized, and tissues and blood were collected for analysis. Food intake,
energy expenditure and locomotion during HFD were similar between WT
and DARC-/- mice, leading to equivalent body-weight gain and adipose tissue
mass. Compared to WT mice, HFD-fed DARC-/- mice exhibited lower plasma
levels of the DARC-bound cytokines MCP-1, CCL11 and CXCL5, but higher adi-
292‑LB
P-Selectin Deficiency Does Not Attenuate Insulin Resistance in
Obesity
KYLE PRESTON, ROSARIO SCALIA, Philadelphia, PA
The relationship between inflammation and the metabolic complications
associated with diet induced obesity (DIO) remains poorly understood. Recent studies show that deletion of the high-affinity counter-receptor for
P-selectin, P-selectin glycoprotein ligand-1 (PSGL-1), attenuates immune
cell infiltration into fat depots of chronically high fat fed mice. Whether deADA-Funded Research
For author disclosure information, see page LB98.
LB72
Obesity—Human
pose tissue MCP-1 mRNA expression, greater numbers of adipose tissue macrophages, and significantly larger adipocytes in the visceral adipose depots,
implying enhanced adipose tissue inflammation. In addition, glucose tolerance
and insulin sensitivity were significantly more impaired in DARC-/- mice compared to WT mice on HFD. We conclude that loss of DARC predisposes to
HFD-induced adipose tissue inflammation and metabolic disease. These novel
findings may be pertinent to the pathogenesis of obesity-related metabolic
disease in populations that commonly express DARC allele variants.
and genistein could be a strategy for promoting insulin sensitivity and preventing
the pathogenesis of type 2 diabetes.
Supported By: American Diabetes Association (11-BS-84 to D.L.);
1R01AT00707701
297‑LB
Pellino3 Deficiency Improves Diet-induced Hepatic Steatosis and
Inflammation
JUNG-HUN LEE, JIN-SIK BAE, YUN-SEUNG JUNG, SUNTAEK HONG, JI-YOUNG
CHA, Incheon, Republic of Korea
295‑LB
Obesity-related inflammation has been implicated in the pathogenesis of
insulin resistance, which is a hallmark of type 2 diabetes. In this study, we
investigated the potential role of E3 ubiquitin ligase Pellino 3 on obesity, inflammation, and insulin resistance. Pellino3 deficient and wild-type mice were
fed high fat diet to study the impact of Pellino3 deficiency on the development
of obesity and insulin resistance. We determined various metabolic profiles,
glucose clearance and insulin sensitivity. We also determined the mechanism
by which Pellino3 deficiency affects the expression of genes involved in energy metabolism, insulin signaling, and inflammation. After feeding a high-fat
diet (HFD) for 10-17 weeks, Pellino3 deficient mice showed less weight gain
and adiposity than wild-type controls. Pellino3 deficiency improved hepatic
steatosis, glucose tolerance and insulin sensitivity. The decreased hepatic
TG content in HFD-fed Pellino3 deficient mice was associated with altered
expression of genes involved in fatty acid synthesis and fatty acid uptake,
cholesterol efflux, and fatty acid β-oxidation, indicative of altered liver physiology. In addition, Pellino3 deficient mice displayed a marked suppression of
the c-Jun NH2-terminal kinase (JNK) activation by high fat diet, accompanied
by decreased expression of inflammatory cytokines. These data suggest that
in a HFD context, Pellino3 deficiency protects against diet induced obesity and
its associated metabolic dysregulation, in part through a decrease in hepatic
lipid accumulation and a decrease in systemic inflammation.
PARP14 Plays a Key Role in Adipocyte Differentiation: A Potential
Novel Target for Obesity
NORIYUKI INOUE, HIROSHI IWATA, TAKUYA HARA, ANDREW MLYNARCHIK,
MALLARY HOIDAL, MARY WHELAN, KEN MIZUNO, MASANORI AIKAWA, Boston, MA
We recently reported that poly ADP ribose polymerase 14 (PARP14), a monoribosylation enzyme, induces pro-inflammatory activation of macrophages
and promotes the progression of arterial disease in mice. We found that not
only hematopoietic cells but also adipocytes express PARP14. Adipose tissue
of obese mice expressed higher levels of PARP14 mRNA than did lean mice
(3.6-folds, p<0.001, n=6-8/group). We thus hypothesized that PARP14 associates with molecular mechanisms for obesity. PARP14 protein levels increased
during the differentiation of 3T3-L1 cells into adipocytes. Enforced expression
of PARP14 enhanced PPARγ transcriptional activity in the luciferase system
for the PPARs response element PPRE (3.0-folds, p<0.05). Ribosylation assays
demonstrated that PARP14 directly ribosylates PPARγ. These results indicate
that PARP14 and PPARγ interact with each other. PARP14 silencing suppressed
adipocyte differentiation in 3T3-L1. Moreover, mouse embryonic fibroblasts
(MEFs) extracted from PARP14-deficient mice did not induce adipocyte differentiation unlike control MEFs (p<0.001, Fig. A and B). These findings suggest
that ADP-ribosylation of PPARγ by PARP14 regulates adipocyte differentiation,
indicating that PARP14 may be a novel therapeutic target for obesity.
Supported By: Ministry of Food and Drug Safety (14182MFDS978)
Obesity—Human
298‑LB
Human Beige Adipocytes Generated from Capillary Networks Di‑
rectly Improve Systemic Metabolic Homeostasis
Supported By: Kowa Company, Ltd.
296‑LB
Long-Term Effects of Phytochemicals Genisteinn, Sulforaphane,
and Kaempferol on Insulin Resistance in Diet-induced Obese Mice
HANA ALKHALIDY, JING LUO, AIHUA WANG, KYUNG-SHIN SUH, WEI ZHEN,
DONGMIN LIU, Blacksburg, VA
Insulin resistance and a progressive decline in functional β-cell mass are hallmarks of developing type 2 diabetes (T2D). Thus, searching for natural, low-cost
compounds to simultaneously target these two defects could be a promising
strategy to prevent the pathogenesis of T2D. Here, we found that natural compounds sulforaphane and kaempferol improve insulin sensitivity by increasing
energy metabolism and glucose uptake in skeletal muscle cells in vitro, while isoflavone genistein promotes pancreatic beta-cell function and glucose tolerance
in mice. We further show that oral administration of genistein (G), sulforaphane
(S), G in combination with Kaempferol (K) (G+K), or G+S significantly improved
glucose and insulin sensitivity in high-fat diet (HFD)-fed obese mice. Notably,
G+S is more potent than any other treatments in controlling blood glucose, while
treatment with either G+K or G+S completely restored insulin sensitivity to the
levels comparable to those of lean mice. These desirable metabolic effects
produced by these treatments were not due to changes in body weight or fat
deposit in obese mice. However, we observed that obese mice also treated with
compounds ultimately developed the similar magnitude of hyperglycemia and
insulin resistance as the control obese mice after mice were fed the HFD for over
16 weeks. These results suggest that a combination therapy with sulforaphane
Supported By: National Institutes of Health (R01DK089101, R24OD018259,
R01DK089185); American Heart Association (12FTF11260010)
ADA-Funded Research
For author disclosure information, see page LB98.
LB73
POSTERS
Adipose tissue is composed of white adipocytes, which are specialized for
energy storage, and brown adipocytes, which are specialized for thermogenesis.
Recent studies have revealed a new class of thermogenic adipocytes arising
within white adipose tissue in response to adrenergic stimulation or cold exposure, a phenomenon known as browning. These beige adipocytes are present in human adults and their abundance correlates with a lean phenotype and
reduced risk of metabolic diseases. To understand the mechanisms underlying
browning and metabolic benefit, it is necessary to identity the progenitors of
beige cells, the mechanisms that control their proliferation and differentiation,
and the features underling their association with improved metabolism. Numerous studies in mouse have shown that adipocyte progenitors reside within the
capillaries of adipose tissue depots. To determine whether adipocyte progenitors also reside within human adipose tissue capillaries we have used an in vitro
system in which hydrogels and pro-angiogenic conditions are used to expand
human subcutaneous adipose tissue capillary networks. We find that the growth
of adipose tissue capillaries is accompanied by proliferation of adipocyte progenitors, identified by single cell cloning. Unexpectedly, these progenitors give
rise to beige adipocytes with expression of UCP1, as well as of other brown
adipose tissue-specific genes, resulting in a thermogenic phenotype characterized by augmented uncoupled oxygen consumption. When implanted into mice,
adipocytes derived from human progenitors integrate into the circulatory system, as assessed by the presence of human adiponectin in the mouse circulation,
and the mice implanted with human beige adipocytes display improved glucose
tolerance. In summary, our results have identified functional human beige adipocyte progenitors residing within capillary networks, enabling their biochemical
and functional characterization.
Integrated
Physiology/Obesity
SO YUN MIN, RAZIEL ROJAS-RODRIGUEZ, JAMIE KADY, MINWOO NAM, MARCUS COOPER, TIMOTHY FITZGIBBONS, MICHAEL A. BREHM, SILVIA COR­VERA,
Worcester, MA
Obesity—Human
299‑LB
the Band and LCD group. Fasting glucose levels decreased dramatically after
surgery (RYGB=112±8 to 94±5mg/dL, SG=110±5 to 88±3mg/dL; Band=103±4
to 97±3mg/dL) but had returned to baseline levels in the LCD group (116±12
to 113±14mg/dL) by 1 year. At 2 months, metabolic adaptation was observed
in all surgery groups (SG=-164±62kcal; RYGB=-216±48kcal; Band=-186±66kcal;
all P<0.05), a reduction which persisted only in the RYGB group (-183±35kcal) at
1 year. No metabolic adaptation was observed in the LCD group at 2 months or
1 year. There were no associations between the degree of metabolic adaptation and % weight loss or changes in circulating leptin, T3 and T4 in any of the
groups studied. In conclusion, despite a large metabolic adaptation occurring 2
months after SG, Band and RYGB, only RYGB had persistent metabolic adaptation after one year. Our results suggest that there are unique mechanisms of
RYGB in decreasing energy expenditure which require further investigation.
Impact of Sulfonylurea (SFU) Use on Weight Loss (WL) Achieved
with Lorcaserin (LOR)
CAROLINE M. APOVIAN, RANDI FAIN, ALAN GLICKLICH, TONY MA, WILLIAM
SHANAHAN, Boston, MA, Woodcliff Lake, NJ, San Diego, CA
LOR is a 5-HT2C receptor agonist indicated for chronic weight management
in obese patients (pts)/overweight pts w/ ≥1 comorbidity. In Phase 3 trials, WL
w/LOR was lower in pts w/type 2 diabetes (T2DM) than in those w/o T2DM,
which may be due to the weight-gaining effect of SFUs. This post-hoc analysis
focuses on the effect of LOR on WL and glycemic parameters (GPs) stratified
by SFU use in the BLOOM-DM trial, where T2DM pts were treated w/LOR 10
mg BID or placebo (PBO) for 52 wks. Pts were taking SFU alone (+SFU/-MET
[metformin]), MET alone (-SFU/+MET), or both (+SFU/+MET). In the unstratified
population, LOR showed significant improvements vs. PBO for all WL and GPs
evaluated, and for the majority of these in the stratified populations (Table 1).
However, categorical and absolute WL was less in pts taking LOR+SFU w/or
w/o MET vs. pts taking LOR+MET alone. In contrast, pts taking LOR+SFU w/
or w/o MET achieved greater improvements in HbA1c and FPG vs. pts taking
MET alone. This analysis suggests that reduced efficacy of LOR on WL in pts
w/T2DM may be due, in part, to SFU use. Pts on MET but not taking SFUs had
WL comparable to previously published data in pts w/o T2DM.
Supported By: Ethicon Endo-Surgery, Inc.
301‑LB
Established BMI-associated Genetic Variants and Their Longitudi‑
nal Associations with Cardiometabolic Traits: The GLACIER Study
SHAFQAT AHMAD, ALAITZ POVEDA, DMITRY SHUNGIN, INÊS BARROSO, GÖRAN
HALLMANS, FRIDA RENSTRÖM, PAUL W. FRANKS, Malmö, Sweden, Umeå, Sweden, Cambridge, United Kingdom
Recent genome-wide meta-analyses have reported associations of 97 independent loci with body mass index (BMI). We tested whether these loci are
also associated with 10-year changes in BMI and other cardiometabolic traits in
the GLACIER Study, a population-based prospective cohort study from northern
Sweden. For the current follow-up analyses, complete data on 3,541 GLACIER
Study participants was available. The GRS was calculated by summing the BMIassociated alleles at each genetic variant. The degree to which genetic predisposition to obesity, conveyed by these variants, impacts other cardiometabolic risk
markers was determined by testing genetic associations with 10-year changes
in a variety of clinical markers (blood concentrations of fasting and 2-h glucoses,
triglycerides, total cholesterol, and systolic and diastolic blood pressures) were
tested separately and combined using principal components analysis. Cross-trait
associations (suggestive of pleiotropy and mediation) of 97 BMI-associated genetic variants/or a GRS comprised of these variants with cardiometabolic traits
were tested by comparing genetic associations with a given trait with/without
adjustment for BMI. Regression models were adjusted for baseline age, age2,
fasting time (where relevant), sex, follow-up time, and population substructure.
The GRS was significantly associated with higher BMI (P=1.2 x 10-39), triglycerides (P=0.002), SBP (P=0.037) and DBP (P=0.008) at baseline without BMI
adjustment. At 10 years follow-up, the GRS was significantly associated with increased BMI (P=0.018) and decreased total cholesterol concentration (P=0.039),
the latter of which was without BMI adjustment. Collectively, established BMIassociated variants convey modest time-dependent associations with long-term
changes in BMI and serum total cholesterol. These findings suggest a role for
effect-modification by factors that change with time.
Supported By: Novo Nordisk (to P.W.F.); Swedish Research Council (to P.W.F.);
Swedish Heart Lung Foundation (to P.W.F.); Skåne Health Authority (to P.W.F.);
Basque Government (to A.P.)
302‑LB
In Vivo Assessment of Adipocyte Cellular Kinetics in Abdominal
and Femoral Subcutaneous Adipose Tissue in Women
URSULA WHITE, MARK FITCH, MARC HELLERSTEIN, ERIC RAVUSSIN, Baton
Rouge, LA, Berkeley, CA
Adipose tissue (AT) distribution, rather than overall excess adiposity, may
be a better determinant of metabolic health. Upper body fat is classically
associated with the complications of obesity, while lower body fat may be
somewhat protective. Studies suggest that fat expansion involves depot specific cellular mechanisms. We assessed in vivo adipogenesis in subcutaneous
AT from the abdominal (scABD) and femoral (scFEM) depots using the 8 week
incorporation of deuterium (2H) into the DNA of adipocytes and preadipocytes
in 25 obese women (14 Black; 11 White; 31 ± 6 years; BMI 32.6 ± 2.7 kg/m2;
44.3 ± 4.1% body fat). Measures of new DNA synthesis denote cell formation
or proliferation in the adipose depots. Cellular preadipocyte and adipocyte
formation rates both correlated positively with overall % body fat (p < .05).
Notably, preadipocytes and adipocytes had higher proliferation rates in the
scFEM depot relative to the scABD (*p< .05; ***p< .001 in Figure). Also, the
proliferation rate of adipocytes was positively correlated to that of preadipocytes in each depot. This in vivo method will prove useful to assess adipocyte
kinetics in relation to body composition or in response to a variety of interventions, such as diet, exercise or pharmacological treatment.
Supported By: Eisai Inc.
POSTERS
Integrated
Physiology/Obesity
Table. Mean Changes in WL and GPs in All Pts and Pts Stratified by SFU and
MET Use Following 52 Wks of LOR Treatment (MITT/LOCF).
LOR
PBO
Alla +SFUb -SFU +SFU Alla +SFUb -SFU +SFU
-MET +MET +MET
-MET +MET +MET
Weight loss (%)
n
251
19
125 107 248
22
123 103
≥5%
37.5 26.3 43.2* 32.7† 16.1
9.1 16.3 17.5
≥10%
16.3 15.8 20.8* 11.2† 4.4
0
3.3
6.8
Weight (kg)
n
251
19
125 107 248
22
123 103
Baseline mean 103.5 103.2 104.9 102.0 102.3 98.9 101.7 103.6
Change from
-4.9 -4.7 -5.7* -4.1† -1.9 -0.7 -1.7 -2.3
baseline
HbA1c (%)
n
238
16
122 100 232
21
115
96
Baseline mean 8.1
8.1
7.8
8.3
8.0
8.2
8.0
8.1
Change from
-0.9 -1.0 -0.9* -1.0† -0.4 -0.4 -0.5 -0.4
baseline
FPG (mg/dL)
n
242
19
117 106 244
22
122 100
Baseline mean 163.3 169.1 154.3 172.8 160.0 162.7 161.4 157.6
Change from -29.2 -36.4 -23.8* -33.8‡ -11.3 -7.6 -13.0 -10.1
baseline
ap<0.0001 vs. PBO for all comparisons (previously reported data of mean/
mean change from baseline are presented for each parameter); bp-values not
provided for +SFU/-MET group due to small sample size. *p≤0.001 vs. PBO
-SFU/+MET; †p<0.001 vs. PBO +SFU/+MET; ‡p=0.002 vs. PBO +SFU/+MET.
FPG=fasting plasma glucose; HbA1c=glycated hemoglobin; LOR=lorcaserin;
MET=metformin; MITT/LOCF=modified intent-to-treat/last-observation-carriedforward; PBO=placebo; SFU=sulfonylurea.
300‑LB
Metabolic Adaptation Persists 1 Year after Gastric Bypass, but Not
Sleeve or Band Bariatric Surgery
CHARMAINE TAM, LEANNE M. REDMAN, FRANK GREENWAY, ERIC RAVUSSIN,
Sydney, Australia, Baton Rouge, LA
Weight loss often results in metabolic adaptation, i.e. a decrease in energy expenditure larger than that expected on the basis of the loss in fat-free
mass and fat mass. Preclinical data suggests that metabolic adaptation may
be blunted in response to bariatric surgery, but it is not known whether this
differs with the type of surgery. In this study, we assessed sedentary energy expenditure (24hEE) in a metabolic chamber at baseline, 2 months and
1 year after Roux-en-Y bypass (RYGB), sleeve gastrectomy (SG), gastric band
(Band) or low-calorie diet (LCD) (n=32: 29F/3M; 4 with diabetes; age=45.8±12.1y;
BMI=48.1±9.0kg/m2). Metabolic adaptation at follow-up was calculated as the
difference between measured energy expenditures and energy expenditures
predicted from body composition, sex and age at baseline. Data are presented
as mean±SEM. After 1 year, SG and RYGB groups had achieved similar weight
loss (SG=-35.6±3.1%; RYGB=-36.0±3.1%), with -17.6±1.8% and -3.0±1.6% in
Supported By: National Institutes of Health-National Institute of Diabetes and
Digestive and Kidney Diseases (R01DK090607-S)
ADA-Funded Research
For author disclosure information, see page LB98.
LB74
Obesity—Human
304‑LB
HNF4A Regulates Betatrophin during the Progression of Insulin Re‑
sistance
CAROLINE BONNER, VALÉRY GMYR, VIOLETA RAVERDY, GURVAN QUENIAT,
ERICKA MOERMAN, CÉDRIC BEAUCAMPS, NATHALIE DELALLEAU, JULIEN
THEVENET, AMAR ABDERRAHMANI, ROBERT CAIAZZO, JULIE KERR-CONTE,
FRANÇOIS PATTOU, Lille, France
Insulin resistance (IR) is associated with beta cell expansion in adults,
and a failure to do so in response to metabolic demand is a key feature of
type 2 diabetes (T2D). Studies in mice suggest that circulating betatrophin
(C19orf80 gene) link IR and beta cell functional mass, but the mechanisms
involved are unclear. Since Hepatocyte-Nuclear-Factor-4-alpha (HNF4A) is a
key regulator of important hepatic genes, we hypothesized whether HNF4A
was required to regulate betatrophin during IR.
In a cross sectionnal clinical
study C19orf80 mRNA expression was induced in the liver by IR and correlated with serum betatrophin concentrations, body mass index, and beta
cell functional mass, as estimated by HOMA-B. In contrast, and despite IR,
there was a significant decline in betatrophin in T2D subjects. Similar biphasic gene expression patterns were identified for HNF4A, and putative binding sites for HNF4A were identified on the C19orf80 promoter. In patients
with grade 3 obesity, surgical weight loss was associated with a simultaneous decrease in betatrophin serum levels, IR and HOMA-B. Collectively,
these findings suggest that hepatic HNF4A is a critical transcription factor
required for betatrophin liver expression and secretion, in close relation with
IR and beta cell mass function, which is lost during T2D.
303‑LB
Significant Effects of HM11260C on Body Weight over 20 Weeks in
Obese Subjects without Diabetes: A Randomized, Double-Blind,
Placebo-Controlled Study
RICHARD E. PRATLEY, JAHOON KANG, PANKYUNG KIM, EUNHWA KWAK,
OAKPIL HAN, SIYOEN KIL, KYUHOON GEE, IN YOUNG CHOI, SE CHANG KWON,
MICHAEL TRAUTMANN, MARCUS HOMPESCH, Orlando, FL, Seoul, Republic of
Korea, Chula Vista, CA
305‑LB
Spleen Attenuation Was Correlated with Intramuscular Adipose
Tissue in Skeletal Muscle at Steady State and during Exercise
KYUNG AH HAN, KYUNG WAN MIN, HONG KYU LEE, Seoul, Republic of Korea
Spleen enlargement was commonly seen in patients with nonalcoholic
fatty liver. Ectopic lipids can be depleted during exercise. We hypothesized
that spleen as another site of ectopic fat deposition is related to the intramuscular adipose tissue in skeletal muscle or hepatic steatosis and also with
insulin sensitivity in type 2 diabetes. We assessed BMI, total abdominal
ADA-Funded Research
For author disclosure information, see page LB98.
LB75
POSTERS
Integrated
Physiology/Obesity
HM11260C (HM) is a novel long acting GLP-1R agonist with a T1/2 of ~ 158
hrs resulting in a flat PK profile. This 20-week, randomized, double-blind, placebo (PBO) controlled, parallel group study was designed to evaluate the
efficacy, safety, and tolerability of once a week (QW) or every other week
(Q2W) doses of HM in obese subjects without diabetes. 297 subjects (mean
age 43.4 yrs and BMI 35.5 kg/m2) were randomized to one of four HM doses
(4 mg QW, 6 mg QW, 6 mg Q2W, or 8 mg Q2W) or to PBO. HM was administered subcutaneously for 20 weeks. The diet and exercise regimens
remained unchanged during the study. The body weight loss with HM 4mg
QW, 6 mg QW, 6 mg Q2W and 8 mg Q2W was 6.2 kg, 7.8 kg, 7.0 kg and 7.1
kg (LS Mean, p<0.0001 all HM treatment groups), whereas the body weight
gain was observed with PBO (0.8 kg). More subjects in the HM treatment
groups achieved significant body weight loss ≥5% or ≥10%, and the mean
reductions in waist circumference and BMI from baseline were greater, compared with PBO. The most frequent adverse events were gastrointestinal
events which were observed relatively frequently and increased injection
site reactions which were less common (Table 1). In conclusion, all doses
of HM meaningfully reduced body weight and were well tolerated. These
results warrant further studies to assess titration schemes as well as the
long-term efficacy and safety of HM in obesity.
Obesity—Human
(TAF), subcutaneous fat (SAF) and visceral fat (VAF), liver and spleen attenuation (HA and SA), intramuscular adipose tissue (IMAT), at midthigh level
using computed tomography, and measured circulating retinol binding protein 4 (RBP4), adiponectin/leptin ratio (ALR), free fatty acid (FFA), and insulin
sensitivity by homeostatic model assessment insulin resistance (HOMA-IR)
at baseline, and after 12 week exercise program. Total 56 women with type 2
diabetes (age 56±2 years; BMI 27.1±3.1 kg/m2) completed the lifestyle modification program including exercise. BMI decreased to 26.3±3.2 kg/m2 after
intervention. SA was correlated with visceral fat (r=-.302, p=0.02), IMAT (r=.314, p=0.016), adiponectin/leptin ratio (r=-.366, p=0.005), RBP-4 (r=-.262,
p=0.047), HOMA-IR (r=-.265, p=0.044), but not with TAF, SAF, LA or FFA. at
baseline. SA was also correlated with visceral fat (r=-.302, p=0.02), IMAT
(r=-.314, p=0.016), ALR (r=-.366, p=0.005), RBP-4 (r=-.262, p=0.047), HOMAIR (r=-.265, p=0.044), but not with TAF, SAF, LA or FFA at 3 month. Change of
SA from baseline was also correlated with change of IMAT (r=.231, p=0.045).
In conclusion, spleen attenuation was connected with intramuscular adipose
tissue and insulin resistance at steady-state, and during exercise. It suggested that spleen might be the another site of ectopic fat deposition in
type 2 diabetes.
subgroups had broadly comparable adverse events (AEs). In both liraglutide
3.0 mg subgroups (BMI< or ≥35) a greater proportion of subjects had nausea (34 vs. 32%) and vomiting (11% vs. 20%) than placebo (nausea: 12 vs.
15%; vomiting: 8% vs. 4%). Documented symptomatic hypoglycemia (FPG
≤70 mg/dL) rates were similar with liraglutide 3.0 mg in both BMI subgroups
(1.07 vs. 0.70 events/PYE), as was severe hypoglycemia, seen in 3 subjects
with concomitant SU. In summary, effects of liraglutide 3.0 mg, as adjunct to
Dand E, on weight loss, associated metabolic effects and safety profile were
consistent across predefined baseline BMI subgroups.
Table.
306‑LB
Leptin Secretion Is Modified by C-Peptide in Human Visceral Adi‑
pose Tissue
SARA GARCIA-SERRANO, CAROLINA GUTIERREZ-REPISO, FRANCISCA RODRIGUEZ-PACHECO, EVA GARCIA-ESCOBAR, JUAN GARCIA-ARNES, SERGIO
VALDES, MONTSERRAT GONZALO, JUAN F. COBOS-BRAVO, FRANCISCO J.
MORENO-RUIZ, ALBERTO RODRIGUEZ-CAÑETE, EDUARDO GARCIA FUENTES,
Málaga, Spain
Supported By: Novo Nordisk
308‑LB
Contribution of Low-Frequency Variants to Variation in Body Mass
Index (BMI)
RUTH J.F. LOOS, VALERIE TURCOT, YINGCHANG LU, HEATHER M. HIGHLAND,
TODD L. EDWARDS, TONU ESKO, MARIELISA GRAFF, ANNE E. JUSTICE, M.
CAROLINA MEDINA-GOMEZ, CLAUDIA SCHURMANN, ROBERT A. SCOTT, K. SIN
LO, SUTESH S. SIVAPALARATNAM, LORRAINE SOUTHAM, KATHY STIRRUPS,
THOMAS W. WINKLER, HANIEH YAGHOOTKAR, KRISTIN L. YOUNG, L. ADRIENNE
CUPPLES, TIMOTHY M. FRAYLING, JOEL N. HIRSCHHORN, GUILLAUME LETTRE,
CECILIA M. LINDGREN, KARI E. NORTH, INGRID BORECKI, BBMRI, GOT2D,
CHARGE, GIANT CONSORTIUM, New York, NY, Montreal, QC, Canada, Houston, TX,
Nashville, TN, Tartu, Estonia, Chapel Hill, NC, Rotterdam, Netherlands, Cambridge,
United Kingdom, Amsterdam, Netherlands, Hinxton, United Kingdom, Regensburg,
Germany, Exeter, United Kingdom, Boston, MA, Cambridge, MA, St. Louis, MO
Over 95 BMI-associated loci have been identified by genome-wide association studies (GWAS), the vast majority of which are common and have
small effects. While low-frequency exonic variants are known to cause
extreme and early-onset obesity, little is known about their role in obesity susceptibility in the general population. To estimate the contribution
of low-frequency (MAF < 5%) single nucleotide variants (SNV) to BMI, we
performed a meta-analysis of exome array data in up to 249,395 individuals
of predominantly European ancestry from 79 studies. In each study, association was tested between ~ 250,000 SNVs and inverse normally transformed
residuals of BMI, adjusted for age and sex. Study-specific association results were combined using inverse variance-weighted meta-analysis. Associations for 3 low-frequency variants reached array-wide significance (P
< 5x10-7). A rare nonsynonymous SNV (MAF = 0.04%, Val830Ile) in an unknown protein-coding gene (KIAA0754, P = 4.8x10-7) increases BMI by ~2.5
kg.m-2 (or ~7.2 kg for a 1.7m-tall person). A second SNV, in the first intron of
GPR61 (3.7%, P = 2.8x10-21, ~1.0 kg/allele), is flanked by a more common coding SNV (6.6%, P = 1.3x10-10, ~500 g/allele) in SYPL2. While fine-mapping is
needed to determine the causal gene in this locus, GPR61 is a strong biological candidate as GRP61-deficient mice exhibit obesity and hyperphagia. The
third SNV is a missense variant (3.7%, Pro180Ser) in ZBTB7B (P = 3.8x10-8,
650 g/allele), located at the downstream-end of a long-range association
peak (1Mb) of common SNVs (MAF > 25%) that include coding variants in
EFNA1 and UBQLN4. Conditional analyses and functional follow-up to determine whether the low-frequency and common SNVs represent independent
signals are ongoing. We conclude that large-scale meta-analyses of exome
array data will uncover low frequency SNVs with effects larger than the
common GWAS-identified loci. Ongoing analyses include an expansion of
the sample (> 450,000), gene-based analyses and functional follow-up.
Supported By: Consejería de Economia, Innovacion, Ciencia y Empresa de la
Junta de Andalucía, Spain (CTS-8081)
POSTERS
Integrated
Physiology/Obesity
C-peptide has been found to be a bioactive peptide, acting as a hormone
independent of insulin. C-peptide could be involved in the regulation of the
synthesis of different adipocytokines in human adipose tissue. We aim to
determine whether C-peptide levels could be associated with leptin levels.
First, we analyzed the association between serum C-peptide and leptin levels with an intravenous glucose tolerance test (IVGTT). After, we performed
an in vitro study in human visceral adipose tissue (VAT) to analyze the effect of C-peptide on leptin secretion. C-peptide significantly correlated with
different variables: glucose (r=0.342, p<0.0001), insulin (r=0.605, p<0.0001),
insulin sensitivity (SI) (r=-0.500, p=0.0001), area under curve of insulin (AUCI)
(r=0.448, p=0.003) and leptin (r=0.370, p<0.0001). C-peptide was associated in a multiple regression analysis model with leptin (p=0.011, β=0.476)
and insulin levels (p<0.001, β=0.556) (R2=0.640) after adjusting the model
for age, gender, body mass index (BMI), glucose and SI. The AUCC-peptide
correlated significantly with different variables: insulin (r=0.291, p=0.041),
AUCI (r=0.512, p<0.0001) and leptin (r=0.470, p=0.001). In a multiple linear regression model, the AUCC-peptide was associated with BMI (p=0.006; β=0.514), leptin (p=0.003; β=0.572), SI (p=0.021; β=-0.441) and AUCI (p=0.019,
β=-0.304) (R2=0.630) after adjusting the model for age, gender, glucose and
insulin. We found a significant increase in leptin secretion into the medium
after a 24 hours incubation with 10 nM C-peptide (p=0.043) in human VAT
explants from non-obese subjects, with no significant effect with 1 nM Cpeptide. In human VAT explants from morbidly obese subjects, 1 and 10 nM
C-peptide induced an increased in leptin secretion (p=0.037 and p=0.047,
respectively). In conclusion, we found a relation between serum C peptide
and leptin. Also, we found that C-peptide has an effect on leptin secretion.
307‑LB
Liraglutide 3.0 mg Efficacy and Safety by Baseline BMI in the SCALE
Diabetes Trial: Post-hoc Analysis
VANITA R. ARODA, JULIO ROSENSTOCK, JOANNA UDDÉN HEMMINGSSON,
MELANIE DAVIES, TRINE V. SKJØTH, BIRGITTE CLAUDIUS, HAROLD BAYS,
Hyattsville, MD, Dallas, TX, Stockholm, Sweden, Leicester, United Kingdom, Søborg,
Denmark, Louisville, KY
SCALE Diabetes (NCT01272232) randomized 846 adults (age 54.9 y, M
50%, BMI 37 kg/m2, A1C 7.9%, T2D duration 7.3 y) 2:1:1 to liraglutide 3.0 mg,
1.8 mg, or placebo as adjunct to diet and exercise (D and E) for 56 wk. This
analysis compared efficacy and safety results for individuals with baseline
BMI < or ≥35 kg/m2 treated with liraglutide 3.0 mg for weight management
or placebo. Data are LS means (efficacy) or observed means (LOCF). Overall
withdrawals rates were 23.4% for liraglutide 3.0 mg vs. 34.0% for placebo.
At 56 wk, greater mean and categorical weight loss, and greater improvements in glycemic parameters, SBP, and IWQoL-Lite physical function score
were seen with liraglutide 3.0 mg vs. placebo in both subgroups. Treatment
effects were independent of baseline BMI subgroup (p>0.05) (Table). BMI
ADA-Funded Research
For author disclosure information, see page LB98.
LB76
Obesity—Human
309‑LB
311‑LB
Blood Lead Level Associates with Higher Body Mass Index and
Prevalence of Obesity in Chinese Women
Weight Loss after Gastric Bypass Surgery in Human Obesity Re‑
veals Novel Changes in Skeletal Muscle Proteome
YINGLI LU, NINGJIAN WANG, CHI CHEN, XIAOMIN NIE, BING HAN, QIN LI, YI
CHEN, CHUNFANG ZHU, YINGCHAO CHEN, FANGZHEN XIA, XIAOQI PU, ZHEN
CANG, CHAOXIA ZHU, MENG LU, YING MENG, HUI GUO, DONGPING LIN, Shanghai, China
LATOYA E. CAMPBELL, PAUL R. LANGLAIS, SAMANTHA E. DAY, JOON YOUNG
KIM, TONYA R. BENJAMIN, ELENA A. DE FILIPPIS, LAWRENCE J. MANDARINO,
JAMES A. MADURA II, LORI R. ROUST, DAWN K. COLETTA, Tempe, AZ, Scottsdale, AZ, Phoenix, AZ
Objective: Lead may be an endocrine and metabolism disrupter. Limited
studies have explored the association between blood lead level (BLL) and
obesity and there is few Investigations of BLL in general adults in China. We
aimed to investigate the relationship of BLL with body mass index (BMI) and
obesity in Chinese adults.
Methods: Our data were population based and from 16 sites in East China.
5558 adults were enrolled with a mean±SD age of 53±13 years. BLL was
measured by atomic absorption spectrometry. Obesity was defined as BMI
≥30kg/m2 and overweight as 25≤BMI<30kg/m2. The associations of BLL
with BMI were analyzed by linear regression and association of BLL with
obesity and overweight by multinomial logistic regression analyses.
Results: Medians (interquartile range) of BLL were 44.0μg/L (29.0-62.2)
for men and 37.8μg/L (25.1-54.4) for women. In women BLL was significantly
correlated with BMI but in men this correlation was not observed. In linear
regression, after full adjustment for age, residence area, economic status,
smoking, diabetes, dyslipidemia and hypertension, BMI was still associated
with BLL (β=0.006, P<0.01) in women. In fully adjusted model by logistic
regression analyses, BLL significantly associated with obesity, not overweight in women. Odds ratio (95% confidence interval) of obesity for each
1-standard deviation increment of log-transformed BLL was 1.28 (1.07-1.53)
in women and 0.94 (0.77-1.16) in men.
Conclusions: BLLs in Chinese adults were much higher than those in developed countries. BLL associated with higher BMI and prevalence of obesity
in Chinese women. Concerted efforts are warranted to reduce adult lead
exposure in China.
Weight loss after roux-en-Y gastric bypass (RYGB) is associated with improvements in skeletal muscle insulin sensitivity. However, the molecular
mechanisms to explain this phenomenon are not entirely clear. Here, we investigated the role of obesity and weight loss after RYGB on the human skeletal muscle proteome. Muscle biopsies were obtained basally from seven
insulin-resistant morbidly obese (BMI >40 kg/m2) female subjects (45.1±3.6
years) pre and 3 months post-RYGB with euglycemic hyperinsulinemic
clamps to assess insulin sensitivity. Four age-matched (48.5±4.7 years) lean
(BMI <25 kg/m2) insulin sensitive (M value: 7.8±0.5 mg/kg.min) females were
studied for comparative purposes. Significant improvements in fasting plasma glucose: 104.2±7.8 vs. 86.7±3.1 mg/dl, BMI: 42.1±2.2 vs. 35.3±1.8 kg/m2
and M value: 2.6±0.4 vs. 3.6 ±0.4 mg/kg·min were demonstrated in the pre
vs. post-RYGB, all P<0.05. Quantitative mass spectroscopy analysis of the
skeletal muscle identified 2,877 quantifiable proteins. Firstly, we identified
that 395 proteins exhibited significantly altered expression levels between
the lean vs. obese pre-RYGB analysis, and KEGG pathway analysis revealed
patterns of decreased abundance in ribosomal and oxidative phosphorylation proteins in obesity. Secondly, we demonstrated that the expression of
280 proteins differed significantly in the pre versus post-RYGB analysis, and
49 proteins were normalized to levels observed in the lean healthy females
following weight loss after RYGB. The weight loss after RYGB revealed an
increased abundance and normalization of ribosomal, MAP kinase and collagen proteins. Our results provide evidence that obesity and weight loss after
RYGB have a dynamic effect on the skeletal muscle proteome.
Supported By: Mayo Clinic-Arizona State University
Supported By: National Natural Science Foundation of China (81270885,
81070677); Clinical Potential Subject Construction of Shanghai Jiaotong University School of Medicine (2014); Ministry of Science and Technology in China
(2012CB524906); Science and Technology Commission of Shanghai Municipality
(14495810700); Fund for Outstanding Academic Leaders in Shanghai (12XD1403100)
312‑LB
Withdrawn
310‑LB
Jejunal De Novo Lipogenesis and Lipoproteins Synthesis Is Altered
in Morbidly Obese Subjects with High Insulin Resistance
Integrated
Physiology/Obesity
The dyslipidemia associated with type 2 diabetes mellitus (T2DM) is an
important risk factor for atherosclerotic cardiovascular disease. However,
until now little attention has been paid to the role that the intestine might
play in these metabolic diseases. The aim of this research was to determine
the relation between insulin resistance and intestinal de novo lipogenesis/
lipoprotein synthesis in morbidly obese subjects. Jejunal mRNA expression
of different genes involved in the intestinal de novo lipogenesis/lipoprotein
synthesis was analyzed in three groups of morbidly obese subjects: with
low insulin resistance (MO-low-IR), with high insulin resistance (MO-highIR) (both groups without treatment for T2DM), and with T2DM and treatment with metformin (MO-metf-T2DM). In the MO-high-IR group, apo A-IV
(p=0.016), ACLY (p=0.045), PDHB (p=0.043) and SREBP-1c (p=0.019) mRNA
expression levels were significantly higher and ACC1 (p=0.011) and FAS
(p=0.042) significantly lower than in the MO-low-IR group. When the MOlow-IR and MO-metf-T2DM groups were compared, these significant differences were maintained in ACLY (p=0.043) and PDHB (p=0.042) mRNA
expression levels. Between the MO-high-IR and MO-metf-T2DM groups,
there are only significant differences in FAS mRNA expression (p=0.049).
HOMA-IR correlated with apo A-IV (r=0.530; p=0.004), DGAT2 (r=0.411,
p=0.033), PDHB (r=0.495, p=0.019), SREBP-1c (r=0.540; p=0.002), ACLY mRNA expression (r=0.605; p=0.006). In conclusion, the jejunum of MO-high-IR
has a decreased mRNA expression of genes involved in de novo fatty acid
synthesis and an increase of genes involved in acetyl-CoA and lipoprotein
synthesis. This effect is attenuated by metformin.
Supported By: Instituto de Salud Carlos III (PI12/00338)
ADA-Funded Research
For author disclosure information, see page LB98.
LB77
POSTERS
CAROLINA GUTIERREZ-REPISO, FRANCISCA RODRIGUEZ-PACHECO, JUAN GARCIA-ARNES, SERGIO VALDES, MONTSERRAT GONZALO, FRANCISCO J. MORENO-RUIZ, ALBERTO RODRIGUEZ-CAÑETE, MIGUEL A. ALAMINOS, GUILLERMO
ALCAIN-MARTINEZ, LUIS VAZQUEZ-PEDREÑO, SARA GARCIA-SERRANO, EDUARDO GARCIA FUENTES, Málaga, Spain
Obesity—Human
313‑LB
315‑LB
The Different Contributions of β-Cell Dysfunction and Insulin Resis‑
tance to the Progression of Type 2 Diabetes in Obese and Non­obese
Chinese People
Preoperative Prediction of Type 2 Diabetes Mellitus Remission af‑
ter Bariatric Surgery: Retrospective Validation of Diabetes Remis‑
sion Scoring Tool (DiaRem)
JIA LIU, YING WANG, YANJIN HU, YUAN XU, SONG LENG, GUANG WANG, Beijing,
China
DANIEL J. LIN, ROHAN LAKHANI, RANGANATHA RAO, JENNY ABRAHAM,
NEHA SHAH, LOUISE HALDER, HARPAL S. RANDEVA, THOMAS M. BARBER,
NARASIMHA MURTHY, VINOD MENON, SUDHESH KUMAR, NARENDRA L.
REDDY, Coventry, United Kingdom
β-cell dysfunction plays a prominent role in type 2 diabetes (T2D) etiology, and obesity is a major cause of insulin resistance and T2D. This study
aimed to assess the different roles of β-cell dysfunction and insulin resistance in the progression from normal glucose tolerance to T2D in obese and
non-obese Chinese people. A total of 3254 participants aged ≥ 25 years,
including 1,843 healthy controls and 1,411 newly diagnosed T2D patients
were recruited. All participants were categorized into the non-obese control, obese control, non-obese T2D and obese T2D groups. The obese subjects had higher homeostasis model assessment of insulin resistance and
β-cell function (HOMA-IR and HOMA-β) than the non-obese ones, whether
in the control group or the T2D group (all P<0.01). Higher HOMA-IR and lower
HOMA-β were observed in non-obese T2D patients when compared with
non-obese controls (all P<0.01). The obese T2D group had lower HOMA-β
than the obese control group (P<0.01). There was no significant difference
in HOMA-IR between the obese T2D and obese control groups. The decline
of β-cell function, together with persistent insulin resistance, accounts for
the progression from normal glucose tolerance to T2D in obese people, while
the decline in β-cell function mainly contributes to the progression in nonobese people.
DiaRem score is a preoperative prediction tool of type 2 diabetes (T2D)
remission after Roux-en-Y gastric bypass (RYGB). This study aimed to extend
the validation of DiaRem score to sleeve gastrectomy (SG) and laparoscopic
adjustable gastric band (LAGB) surgeries. A retrospective study of bariatric
patients at a University hospital involving consecutive patients undergoing
RYGB, SG, and LAGB, between February 2009 and July 2014 was undertaken
utilizing UK National Bariatric Surgery Registry. Preoperative predictors and
post-operative T2D status at 12 months were obtained from electronic and
case note records. DiaRem (weighted factors: age, HbA1c, T2D drugs, insulin
use) was applied and stratified into 5 categories (0-2, 3-7, 8-12, 13-17, 18-22).
T2D remission was defined using ADA’s 2009 criteria (HbA1c {%}: Complete
<6.0; Partial 6.0-6.5; no remission >6.5). Out of 248 patients, 81 T2D patients
(♂:22, ♀:59 female; Mean age 49 years {range 29-71}, Mean BMI 49.1 kg/
m2 {37.4-64}) underwent 42 SG, 24 LAGB, and 15 RYGB. At 12 months, 54%
(44/81) were in T2D remission; 12% (10/81) in partial remission, 34% (27/81)
in non-remission. On DiaRem stratification, T2D remission for SG: 0-2 (80%,
n=15), 3-7 (92%, n=13), 8-12 (20%, n=5), 13-17 (0%, n=8), and 18-22 (0%, n=1);
for LAGB: 0-2 (50%, n=6), 3-7 (31%, n=13), 8-12 (0%, n=2), 13-17 (0%, n=2),
and 18-22 (0%, n=1); for RYGB: 0-2 (100%, n=4), 3-7 (83%, n=6), 8-12 (100%,
n=1), 13-17 (100% n=2), 18-22 (0%, n=2). DiaRem score cut off ≤7 showed
remission in SG 86%, LAGB 37%, and RYGB 90%. Pearson correlation for
DiaRem scores with SG (r= -0.91); LAGB (r= -0.67), and RYGB (r= -0.63). DiaRem score reliably predicted T2D remission rates in SG and RYGB, and was
unreliable in LAGB. Proposed score ≤7 predicted high remission probability
in SG and RYGB. Strong negative correlation in SG indicated that DiaRem
score can be successfully applied in SG group of patients.
316‑LB
Aberrant Expression of IR-B, the Metabolic Isoform of Insulin Re‑
ceptor, in Endometrial Cancer and Hyperplasia
Supported By: Major National Basic Research Program of P.R. China
(2011CB503904); National Natural Science Foundation of China (81270369,
81070244, 30770873); Beijing Natural Science Foundation (7142060)
FARRAH SALEH, CLARE A. FLANNERY, GINA CHOE, KATHERINE ARAQUE, TERESA WOOD, HUGH S. TAYLOR, New Haven, CT, Newark, NJ
Obesity is a risk factor for endometrial hyperplasia and cancer, suggesting
that hyperinsulinemia may contribute to pathogenesis. The insulin receptor
splice variant IR-B is known for metabolic activity versus IR-A which is known
for mitogenic activity. We previously found IR-B is 2-fold higher in secretory
than proliferative endometrium, and insulin regulates glycogen synthesis in
endometrial glands, which secrete glycogen in preparation for implantation.
Thus, we hypothesized that IR-B expression is regulated by progesterone,
and may be reduced by hyperinsulinema. Given obesity-driven risk, we also
investigated IR-B in hyperplasia and adenocarcinoma. IR-B mRNA was quantified in normal proliferative (n=25) and secretory (n=18) endometrium from
women of mean BMI 29 kg/m2, endometrial hyperplasia (n=5, BMI 34), and
adenocarcinoma (n=11, BMI 37) by qRT-PCR. IR-B was also quantified in primary endometrial epithelial and stromal cells (n=4) treated with estradiol
10nM, progesterone 1µM, E+P, or insulin 1 or 100nM. IR-B was not altered by
either estradiol or progesterone in vitro (p=NS). IR-B expression and BMI did
not correlate in either cycle phase, and IR-B was not significantly changed by
insulin in primary cells at either concentration (p=NS). In hyperplasia, mean
IR-B was 5.5-fold higher than normal proliferative (p<0.001) and 2.8-fold
higher than secretory endometrium (p=0.007). In adenocarcinoma, IR-B was
3-fold higher than the proliferative tissue (p<0.01) but similar to the secretory phase (p=NS). We show that IR-B likely has a physiological role in the
endometrium during the secretory phase, but surprisingly was not regulated
directly by sex steroids. IR-B was not altered by insulin in vitro, nor correlated to BMI, a clinical indicator of hyperinsulinemia. Higher IR-B expression in
endometrial hyperplasia and cancer is consistent with increased metabolic
activity, and may reflect a contribution of IR-B in abnormal proliferation.
314‑LB
Metabolic Syndrome: Is Waist Circumference the Correct “Entrance
Criteria?”
POSTERS
Integrated
Physiology/Obesity
KATRINE DRAGSBÆK, JESPER S. NEERGAARD, MORTEN KARSDAL, CLAUS
CHRISTIANSEN, Herlev, Denmark
Large waist circumference (WC) has become the “entrance criteria” for
defining metabolic syndrome (MS) used to identify patients at greater risk
of developing cardiovascular diseases (CVD) and type 2 diabetes (T2DM).
This study aimed to investigate the risk of developing CVD and T2DM based
on number of metabolic risk factors rather than WC in subjects stratified on
BMI and body composition. Demographics, DEXA scans and serum samples
were collected from 1999-2001 on 5855 women aged 73.1±6.3. CVD and
T2DM diagnoses were collected from Danish National Disease Registries
primo 2015. Stratification was made on body composition (central/peripheral (C/P) fat mass ratio stratified into quartiles, Q1-Q4) and BMI (<18.5,
18.5-24.9, 25.0-29.9, ≥30). Metabolic health was assessed by triglycerides,
HDL-cholesterol, blood pressure, and fasting glucose. The presence of MS
and number of abnormalities were assessed by International Diabetes
Federation criteria. Subjects diagnosed prior to enrollment were excluded
from analysis. Incidence and relative risks (RR) for development of CVD and
T2DM in subjects with ≥2 MS risk factors were calculated for all BMI and
body composition groups. The RR for developing CVD and T2DM were increased within all groups regardless of BMI or body composition for subjects
having ≥2 MS risk factors. RR for CVD stratified on body composition: Q1:
RR=1.22 (95% CI: 1.05-3.53), Q2: RR=1.18 (1.06-1.31), Q3: RR=1.25 (1.14-1.36),
Q4: RR=1.12 (0.95-1.26). RR for T2DM stratified on body composition: Q1:
RR=1.44 (0.79-2.64), Q2: RR=4.26 (3.82-4.76), Q3: RR=2.64 (2.41-2.89), Q4:
RR=2.74 (2.37-3.16). The incidence of T2DM increased significantly with both
increasing C/P ratio and BMI. However, CVD incidence did not increase significantly between weight groups emphasizing that number of risk factors,
rather than BMI or body composition, are the denominator for CVD outcome.
Number of risk factors rather than WC should be used for optimal identification of patients at increased risk of CVD due to MS.
Supported By: National Institutes of Health-Eunice Kennedy Shriver National
Institute of Child Health and Human Development
Supported By: Danish National Research Foundation
ADA-Funded Research
For author disclosure information, see page LB98.
LB78
Islet Biology—Apoptosis
317‑LB
319‑LB
Exenatide Blunts the Thermic Effect of Food in Nondiabetic Women
Development of a Novel Broad Range, Highly Specific and Highly
Sensitive Chemiluminescent ELISA Assay for Measuring Glucagon
in Blood-derived Samples
NATASHA KASID, SOPHIE COMTE-PERRET, ELENA TOSCHI, JULIET R. TRIPALDI,
TAHEREH GHORBANI, ELEFTHERIA MARATOS FLIER, JODY DUSHAY, Boston, MA
Exenatide, a glucagon-like peptide 1 receptor agonist, causes increased
satiety and weight loss through peripheral and central mechanisms not
fully understood. We are conducting a randomized, single-blind, placebocontrolled study investigating weight change with BID exenatide versus
hypocaloric diet in non-diabetic women with BMI 28-48kg/m2. Subjects
receiving exenatide follow an ad lib diet while those in the diet arm follow
a hypocaloric diet and administer BID injections of placebo. Subjects who
lose ≥ 5% body weight at 3 months continue treatment for 1 year. To date,
35% of subjects randomized to exenatide (E) lost 5.5% (range 5.2-9.8) body
weight at 3 months and 7.1% (4.6-10.3) at 6 months. In the diet (D) group,
34% of subjects lost 6.4% (5.4-9.6) body weight at 3 months and 9.7%
(5.2-12.9) at 6 months. Nausea assessed by visual analog scale was similar in both groups. Resting metabolic rate (RMR) measured by indirect
calorimetry decreased by a similar degree in both groups at 3 months
(E-8.6% [(0.0-18.3%]), D-6.5% ([0.5-17.0%]) p = 0.93) and at 6 months (E-5.0%
([0.2-14.4]), D-2.4% ([-5.5-5.4]), p = 0.17). The thermic effect of food (TEF) following ingestion of 240ml Boost ® was measured by indirect calorimetry.
At baseline, E and D subjects had a similar postprandial increase in RMR
(E 13.1%, D 13.7%, p=0.87). At 3 months, D subjects maintained the increase
in RMR while E subjects demonstrated significant blunting (P 11.1%, E 3.3%,
p = 0.004). The postprandial increase in RMR was maintained at 6 months
in D but not E subjects (P 11.3%, E 2.8%, p = 0.077). Blunting of TEF in E
subjects and preservation of TEF in D subjects were independent of weight
loss. We find that a similar proportion of subjects randomized to E versus D
are early responders and weight loss is independent of nausea. Exenatide
is associated with blunting of TEF compared to hypocaloric diet. This effect
is maintained at 6 months and is independent of weight loss. The effect of
exenatide on TEF may be related to delayed gastric emptying or mechanisms
not fully understood.
NIRAJA PATEL, SEAMUS WEBB, JAMES LULO, JULIE DONALDSON, COLLIN
SHAW, CHRIS WISHERD, STACY DION, MARTIN BLANKFARD, Salem, NH
Glucagon is a well-known and important peptide hormone which has been
demonstrated to play a vital role in many biological functions, particularly
gluconeogenesis and glycogenolysis. The glucagon peptide is conserved
in all mammals. Glucagon is secreted from α-cells in the pancreas in response to low circulating glucose levels. Glucagon levels in normal patients
can range from 50-250pg/mL (14-72 pM) depending upon food intake. The
main function of glucagon is to act as a counter-regulatory hormone to insulin. Because of this, glucagon is an attractive and popular biological target
with regard to glucose homeostasis. Glucagon is part of a larger proglucagon protein which is enzymatically cleaved to form smaller, related peptides with various biological functions. The ability to accurately quantitate
glucagon levels across a large dynamic range, using a reasonable sample
size is highly desirable to any researcher. The Glucagon Chemiluminescence
ELISA, developed by ALPCO, offers researchers a robust and highly specific
assay for measuring glucagon in serum, EDTA-treated plasma, and heparintreated plasma. Using a sample size of 50µL or less, the assay demonstrates
a high degree of sensitivity (approximately 20pg/mL (5.7pM)) without any
substantial cross-reactivity to other associated proteins/peptides, particularly oxyntomodulin (no cross-reactivity up to 100ng/mL (22nM)). No matrix
interferences were observed, as determined by spike and recovery as well
as dilutional linearity tests in the noted matrices, giving the end user confidence in the accuracy and consistency of the results in each experiment. The
assay was designed with the end user in mind and allows for a simple, quick,
and reliable method for accurate quantitation of glucagon in test samples.
Islet Biology—Apoptosis
Supported By: AstraZeneca
320‑LB
318‑LB
Assessing a Potential Protective Action of Glibenclamide against
Streptozotocin-induced Beta Cell Damage In Vivo
Histone Mark Modifications of Depot-specific Genes in Human Adi‑
pose Tissue
YUMIKO NAKAMURA, JOSEPH BRYAN, Seattle, WA
ADELINE DIVOUX, TIMOTHY OSBORNE, STEVEN R. SMITH, Orlando, FL, Winter
Park, FL
321‑LB
DJ-1 Protects Pancreatic Beta Cells from Cytokine and Strepto­
zotocin-mediated Diabetes
DEEPAK JAIN, DANIEL EBERHARD, JAN EGLINGER, ECKHARD LAMMERT, Lund,
Sweden, Düsseldorf, Germany
DJ-1 is an anti-oxidant protein, highly expressed in pancreatic islet and
known to play an important role in maintenance of glucose tolerance in
mice. Pancreatic islets are highly prone to oxidative stress owing to low
expression of anti-oxidant enzymes. The purpose of the present study was
to evaluate the role of DJ-1 under challenging oxidative stress environment
ADA-Funded Research
For author disclosure information, see page LB98.
LB79
POSTERS
Increased lower body fat is associated with reduced cardiometabolic risk.
The molecular basis for depot differences in gluteal (G-Fat) compared with
abdominal (A-Fat) subcutaneous adipocyte function is poorly understood.
Our recent studies profiling gene expression in these two depots identified
major differences in the expression of HOX genes. These differences are
maintained in vitro during preadipocyte differentiation, suggesting that epigenetic differences are likely to play a major role in phenotypic differences
between A-Fat and G-Fat. We prepared chromatin from cultured preadipocytes that were isolated from A-Fat and G-Fat of 5 obese women and
evaluated by ChIP-qPCR histone H3K4 and H3K27 trimethylation (activation
and repression marks, respectively) patterns within the 5’ flanking region
of the HOXA3, HOXA5, HOXB8, HOXC13 and HOTAIR genes. mRNA expression was evaluated by RT-qPCR. We first confirmed that HOXA3, HOXA5 and
HOXB8 genes were up-regulated in abdominal preadipocytes, HOXC13 and
HOTAIR up-regulated in gluteal cells. H3K4me3 was significantly enriched
at the HOXA3, HOXA5 and HOXB8 promoter regions in abdominal preadipocytes compared to gluteal preadipocytes. H3K27me3 was decreased at the
same promoter regions. Conversely, analysis of the promoter region of the
HOTAIR gene revealed an enrichment of H3K4me3 level and a decrease of
the H3K27me3 level in the gluteal cells compared to the abdominal counterparts. In summary, H3K4me3 and H3K27me3 marks matched the observed
differential HOX gene expression between A-Fat and G-Fat. These genespecific chromatin data provide new evidence that specific epigenetic histone modifications play an important role in gene expression differences in
A-Fat vs. G-Fat. Because HOTAIR associates with the PRC2 repression complex that adds the H3K27me3 mark to chromatin, these findings also support
and extend our earlier work implicating HOTAIR, as a potential upstream
regulator of several other downstream epigenetic events in adipose tissue.
Islet Biology/
Insulin Secretion
Sulfonylureas, through their inhibitory action on SUR1/ABCC8, the regulatory subunit of SUR1/Kir6.2-type KATP channels in pancreatic beta cells,
stimulate insulin secretion and have been a therapy for type 2 diabetes for
>50 years. Recent work shows SUR1 also partners with TRPM4/TRPM4,
a Ca2+-activated, non-selective cation channel inhibited by ATP which is
widely expressed including in beta cells. Inhibition of SUR1/TRPM4 channels by glibenclamide (GBC) or knockout of SUR1 has beneficial effects in
multiple models of CNS trauma, thus we asked if GBC might protect beta
cells from acute damage due to streptozotocin (STZ). Continuous twice daily
administration of GBC to C57/Bl6 mice reduced blood sugar transiently, but
animals became insensitive to GBC and were euglycemic within two days.
Administration of high (200 mg/Kg x 1) or low (50 mg/Kg x 5) dose STZ produced hyperglycemia (>400 mg/dl) in controls while GBC-treated animals
remained euglycemic and minimal changes in islet morphology. Insulin values were dramatically reduced with STZ alone, but showed no significant
changes in GBC/STZ treated animals implying elevated insulin is not a major
factor in maintaining euglycemia. SUR1-/- mice were partially protected
from STZ; added GBC had no effect, i.e., GBC protected wildtype beta cells
more effectively than total deletion of SUR1. We attempted to implicate
TRPM4 by administering flufenamic acid (FA), a semi-selective antagonist of
TRPM4 channels. FA, given 12 hours after STZ, partially protected as judged
by reduced hyperglycemia. The results are consistent with the idea that GBC
inhibition of the stimulatory actions of SUR1 on Kir6.2/KCNJ11 and TRPM4
channels by GBC reduces STZ-induced changes in cation flux that contribute
to beta cell death.
Islet Biology—Beta Cell—Development and Postnatal Growth
by treating DJ-1 K.O. mice with multiple low-doses of streptozotocin (MLDS)
treatment. Streptozotocin (STZ) is a beta cell toxin, which kills beta cells by
both necrosis and apoptosis and also generates oxidative stress. Compared
to controls, DJ-1 K.O. mice were severely glucose intolerant following the
MLDS treatment. Insulin levels were significantly reduced, and fasting and
random blood glucose concentrations were significantly higher in DJ-1 K.O.
mice compared to controls. Beta cell death and apoptosis were significantly
increased in DJ-1 K.O. mice, and DJ-1 K.O. islets were more susceptible for
cytokine-induced apoptosis. There was a drastic reduction in number of insulin secretory granules as well as in the number of mitochondria in DJ-1
K.O. animals compared to controls. We also observed increase in beta cell
death and apoptotic cells as measured by calcein-ethidium bromide and
TUNEL staining after STZ treatment in the absence of DJ-1 protein. Accordingly treatment of isolated islets with streptozotocin from wild type mice led
to increase in DJ-1 protein expression, indicating its protective role against
the toxin. Taken together our results revealed that DJ-1 could alleviate the
toxic effect of STZ treatment leading to balanced beta cell death, however
under oxidative stress conditions in the absence of DJ-1 protein, a combined
effect of increased ROS production, insulin degranulation, and disturbance
of mitochondrial number and morphology culminates in unbalanced increase
in cell death and therefore a suboptimal release of insulin upon glucose
stimulation.
As nutrient-sensing GPCRs are well described to contribute to aspects of
β cell function, we examined the role of FFAR2 in regulating an important
aspect of β cell function, β cell mass. We conducted morphometric analysis
of β cell mass in neonatal (1 day, P1), adolescent (21 days, P21) and adult
(26 weeks) wild type (WT) and Ffar2-/- mice. These data revealed diminished β cell mass in Ffar2-/- mice at all time points, suggesting a role for
FFAR2 in the regulation of β cell mass and development. We next examined
β cell proliferation by immunohistochemistry and probed for β cell death
using serum unmethylated preproinsulin DNA as a biomarker of β cell death.
We observed increased β cell proliferation, accompanied by a simultaneous
increase in β cell death in Ffar2-/- mice at P21, but not P1 or 26 weeks. To
determine whether Ffar2 deletion imparts an intrinsic impairment in β cell
proliferation, we analyzed ex vivo β cell proliferation in WT and Ffar2-/- islets, and observed no differences in proliferation at basal conditions or in
response to prolactin (PRL) or Exendin-4, two potent stimulators of β cell
proliferation. Taken together, these data suggest that genetic deletion of
Ffar2 leads to impaired β cell mass during prenatal development, as well
as an imbalance of β cell death and renewal during adolescence, resulting
in impaired β cell mass into adulthood. However, genetic deletion of Ffar2
does not appear to affect the overall proliferative capacity of the β cell in
response to well-known mediators of β cell proliferation. Future studies are
needed to directly examine the role and mechanism by which FFAR2 mediates the development, survival, and maintenance of β cell mass.
Islet Biology—Beta Cell—Development and
Postnatal Growth
324‑LB
Activation of GLP-1 and Gastrin Signaling in Glp-1r-Overexpress‑
ing Mice Induces β-Cell Neogenesis and Maturation
322‑LB
SHUGO SASAKI, TAKESHI MIYATSUKA, MITSUYOSHI TAKAHARA, FUMIYO KUBO, KAZUYUKI MIYASHITA, YUICHI YAMAMOTO, TETSUYUKI YASUDA, YOSHIYA
KAWAGUCHI, HARUHIKO AKIYAMA, HIDEAKI KANETO, TAKA-AKI MATSUOKA,
HIROTAKA WATADA, IICHIRO SHIMOMURA, Osaka, Japan, Tokyo, Japan, Kyoto,
Japan, Gifu, Japan
Beta Cell Targeted Gene Delivery for Enhanced Beta Cell Prolifera­
tion
BRIAN LU, STACEY LEBER, KIRAN KURMI, JASON M. TONNE, TOSHIE SAKUMA,
MIGUEL MUNOZ-GOMEZ, MOUSTAFA EL KHATIB, EGON J. JACOBUS AMBULUDI, YOGISH C. KUDVA, YASUHIRO IKEDA, Rochester, MN
Lineage conversion of non-β-cells into insulin-producing cells has been
proposed as a therapy for the cure of diabetes. Whereas GLP-1 and its derivatives have been shown to induce β-cell neogenesis in vitro and β-cell
mass expansion in vivo, there has been no direct evidence that the activation of GLP-1 signaling actually regulates cell fate decisions in vivo. We
therefore aimed to clarify the role of the GLP-1 receptor (GLP-1R) in β-cell
differentiation. In the 2014 annual meeting, we reported the development
of new mouse model in which GLP-1 receptor (GLP-1R) can be induced in a
time- and tissue-specific manner (CAG-CAT-GLP-1R) and analyzed exocrineto-β reprogramming using Sox9-CreER; CAG-CAT-GLP-1R (SC; GLP-1R) and
Sox9-CreER; ROSA26-lacZ (SC;lacZ) mice. Here, we further investigated
the extent to which the newly-generated β cells have been reprogrammed
and how GLP-1 and gastrin induces the exocrine-to-β reprogramming. The
overexpression of GLP-1R, together with gastrin and exendin-4 promoted
formation of islet-like clusters, whereas exendin-4 alone or gastrin alone
failed to induce the cluster formation. Over 80% of newly-generated insulinproducing cells in SC; GLP-1R mice were positive for Pdx1, Nkx6.1 and Mafa,
but negative for amylase and other endocrine hormones. In addition, they
were positive for urocortin3. These results suggest that newly-generated
insulin-producing cells partially acquired characteristics of mature β cells.
On the other hand, the treatment with exndin-9-39 (GLP-1R antagonist) deteriorated the efficiency of β-cell neogenesis in SC; GLP-1R mice treated with
gastrin alone, suggesting that the β-cell neogenesis by gastrin is partially
mediated through GLP-1 signaling pathway. Thus, activation of GLP-1 and
gastrin signaling induces β-cell neogenesis and maturation in the exocrine
lineage, which may hence lead to a potential therapy to cure diabetes by
generating surrogate β cells.
Type 2 diabetes mellitus (T2DM) is characterized by a combination of relative insulin deficiency, beta-cell dysfunction, and beta-cell death. T2DM has
become a major health issue worldwide. Current treatments for T2DM cannot offer the same level of glycemic control as healthy, insulin-producing
beta-cells. Increasing the number of beta-cells should increase total insulin
production and lower blood glucose. As beta-cells mostly regenerate by
replication from existing beta-cells, increasing beta-cell proliferation should
increase beta-cell mass. Based on the success of glucokinase activators in
increasing beta-cell proliferation, we sought to induce beta-cell proliferation
by AAV-mediated beta-cell targeted glucokinase gene delivery. Young and
aged C57BL/6J mice maintained on normal diet or high fat diet (HFD) were
given an intraperitoneal injection of promoter-restricted AAV8 expressing
liver glucokinase (GCK) under the mouse insulin 2 promoter. Following injection, we saw markedly increased liver GCK expression in the pancreas.
Beta-cell proliferation was increased in all treated groups compared to control (young mice, 2-fold; aged mice, 6-fold; aged HFD mice, 3-fold), and mice
maintained on HFD showed improvements in glucose tolerance tests (p<0.02
by 60 minutes). These data support the use of glucokinase gene delivery for
enhanced beta-cell proliferation. Prompted by the reports of betatrophin,
we also sought to induce beta-cell proliferation by AAV-mediated delivery
of betatrophin. Young and aged C57BL/6J mice maintained on normal diet
or HFD were given an intraperitoneal injection of promoter-restricted AAV8
expressing betatrophin under the cytomegalovirus (CMV) promoter or the
elastase (ELS) promoter. We saw largely negative results with betatrophin
gene delivery (no significant beta-cell proliferation with CMV promoter;
2-fold beta-cell proliferation in aged HFD mice with ELS promoter). Our data
do not support the use of betatrophin for enhancing beta-cell proliferation.
325‑LB
Supported By: Mayo Foundation; Eisenberg Stem Cell Trust; Mayo Center for
Regenerative Medicine
Multiple MicroRNAs Coordinately Regulate Beta Cell Proliferation
through Targeting MeCP2
POSTERS
Islet Biology/
Insulin Secretion
323‑LB
SUDHIR GOPAL TATTIKOTA, FERDINAND VON MEYENN, THOMAS RATHJEN,
ADITYA KHEDKAR, JEAN HAUSSER, NORBERT EICHNER, VARUN K. PANDEY,
UMA D. KABRA, BÉATRICE CHANE-WOON-MING, MATTHIAS SURY, MATTHIAS
SELBACH, ROBERT P. ZINZEN, MIHAELA ZAVOLAN, LENA ELIASSON, MATTHIAS
TSCHÖP, MARTIN JASTROCH, SÉBASTIEN PFEFFER, GUNTER MEISTER, WOLF
REIK, SEBASTIAN KADENER, ADRIAN BIRD, MARC FRIEDLÄNDER, MATTHEW N.
POY, Berlin, Germany, Babraham, United Kingdom, Basel, Switzerland, Regensburg,
Germany, Jerusalem, Israel, Munich, Germany, Strasbourg, France, Malmö, Sweden,
Cambridge, United Kingdom, Edinburgh, United Kingdom, Stockholm, Sweden
Genetic Deletion of FFAR2 Results in Impaired β-Cell Mass
STEPHANIE R. VILLA, MEDHA PRIYADARSHINI, MICHAEL R. BRODSKY, ANTHONY R. ANGUEIRA, ROCKANN MOSSER, SARAH TERSEY, RAGHAVENDRA G.
MIRMIRA, MAUREEN A. GANNON, BRIAN T. LAYDEN, Chicago, IL, Nashville, TN,
Indianapolis, IN
Free Fatty Acid Receptor 2 (FFAR2) is a G protein-coupled receptor (GPCR)
activated by short chain fatty acids, in particular acetate. This receptor is
expressed in many metabolically relevant tissues such as adipose, gut, and
pancreatic islets. Reports of increased expression in pancreatic islets during insulin resistance suggest FFAR2 involvement in β cell compensation.
Numerous pathways including the microRNA (miRNA) pathway within the
pancreatic beta cell have been implicated in regulating its function during
states of insulin resistance and type 2 diabetes (T2D). Here in this study, we
ADA-Funded Research
For author disclosure information, see page LB98.
LB80
Islet Biology—Beta Cell—Stimulus-Secretion Coupling and Metabolism
show that global alterations in miRNA expression in the islets of hyperglycemic and insulin resistant ob/ob mice are reversed after restoration of insulin sensitivity indicating miRNAs respond to changes in metabolic demand.
We found that the expression levels of miR-184, a known regulator of beta
cell growth and function, were increased upon fasting while on the other
hand, high extracellular glucose concentrations suppressed its expression
in mouse pancreatic islets. Furthermore, we also uncovered an additional
cluster of miRNAs that includes miR-152 to be regulated in the islets according to insulin sensitivity. Computational analyses predicted that this cluster
potentially targets several important genes including Pten and Methyl CpG
binding protein 2 (MeCP2), a gene previously implicated in Rett’s syndrome.
In the pancreatic islets of doxycycline induced transgenic mice overexpressing miR-152 (dox-152) specifically in the beta cells, we in deed observed reduced MeCP2 protein expression indicating it is a direct target of miR-152. In
addition, analyses of the pancreases derived from either dox-152 transgenic
or MeCP2 knockout (MeCP2KO) mice revealed a significant increase in the
pancreatic beta cell mass. Together, these results highlight the adaptive role
of the miRNA pathway and demonstrate the presence of multiple miRNAs
coordinately promoting beta cell function in response to hyperglycemia and
insulin resistance.
negative cells are dedifferentiated hormone-producing cells, possibly representing a sub-population of beta cells, some of which transdifferentiated
to somatostatin- or glucagon-immunoreactive cells. The data are consistent
with a model in which pancreatic endocrine cells lose their terminally differentiated features in T1D, possibly implicating a process of beta cell dedifferentiation in the pathogenesis of the disease.
Supported By: German Center for Diabetes Research
Islet Biology—Beta Cell—
Stimulus-Secretion Coupling and
Metabolism
328‑LB
Roles of the Circadian Clock in Alpha- and Beta-Cell Transcriptome
and Hormone Secretion in Mouse and Human Pancreatic Islet
CHARNA DIBNER, Geneva, Switzerland
Circadian oscillation of biological processes has been described in organisms ranging from photosynthetic bacteria to vertebrate. There is growing
evidence for a connection between metabolic syndromes, including diabetes, and the circadian clockwork. We have established triple reporter mouse
allowing isolating pure alpha- and beta-cells (proGlucagon-Venus and Insulin-Cherry reporters), and characterize circadian rhythm in thus isolated cells
(Per2::luciferase reporter). Employing this model, we identified subsets of
islet genes expressed in a circadian manner in both alpha- and beta-cells,
and those oscillating in alpha- or beta-cells only. This data shed a new light
on the alpha- and beta-cell differential circadian transcriptome. Importantly,
we show that circadian clock is indispensable for proper insulin secretion by
analyzing blood insulin content in clock proficient and deficient mice. Moreover, siClock mediated clock disruption in human islet resulted in decreased
secretion levels of both insulin and glucagon, highlighting importance of
functional clock for the proper function of human islet. Disruption of the temporal programming of physiology, as occurs during shift work, jet lag, and
ageing, has detrimental effects on human health. It is thus of major importance identifying the physiological basis of circadian rhythmicity. Our study
highlights the importance of alpha- and beta-cell circadian oscillator, their
impact on islet transcriptome and function, and sheds light on the cross-talk
between alpha- and beta-cell clocks in mouse and human model systems.
By dissecting the rodent and human pancreas oscillator function we hope to
advance the understanding of clockwork connection to T2D.
326‑LB
Changes in Beta Cell Differentiation in Response to Glucolipotoxic
Stress
CHRISTINA REERS, GERALDINE PARENTY, KAIHUI HU HE, MARTIN SCHNEIDER,
STEFANIE SCHREIBER, THERESA KLISCH, ANNA GUHL, MATTHIAS AUSTEN,
Göttingen, Germany
Recent findings suppose that beta-cell dedifferentiation significantly contributes to the apparent loss of beta-cell mass in T2D and possibly also T1D.
Agents preserving or restoring the mature beta-cell phenotype have the
potential to be complementary to existing therapeutic options and to delay
or stop disease progression. Our goal was to establish the response of rat
islet beta-cell differentiation marker expression to glucolipotoxic stress. We
have emphasized quantification of molecular differentiation markers with
relevance in human T2D and diabetic animal models. As MafA is a sensitive
marker of beta-cell maturity, we have quantified changes in nuclear MafA
expression in insulin-positive beta-cells after 48h of glucolipotoxic challenge (25 mM glucose + 250 µM palmitate) by fluorescent imaging. Image
analysis was conducted with Image J based scripts. Reduction of nuclear
MafA expression upon stress stimulus in primary rat cells was 0.35 ± 0.5%
MafA+/Ins+ cells vs. 70 ± 5% MafA+/Ins+ cells in controls (p <0.001; n=15
experiments). A similar setup was established as secondary assay with human primary beta-cells (34 ± 6% MafA+/Ins+ cells upon stress stimulus vs.
57 ± 15% MafA+/Ins+ cells in controls, p <0.05; n= 5 experiments). Loss of
MafA expression in stressed rat beta-cells was completely reversible after
72h of recovery in normal culture medium. We have identified compounds
which were able to prevent loss of glucolipotoxicity induced loss of MafA
expression. A subset of these compounds also prevented dedifferentiation
in human islet beta-cells. In conclusion, preservation of beta-cell dedifferentiation may translate into improved beta-cell function. Our findings confirm
that agents which prevent loss of beta cell dedifferentiation marker expression could be promising candidate beta-cell protective agents active both in
rodents and in humans.
Supported By: SNRF; European Foundation for the Study of Diabetes
329‑LB
A Novel GLP-1 Receptor Interacting Protein ATP6ap2 Regulates In‑
sulin Secretion in Pancreatic Beta Cells
327‑LB
Pancreatic Endocrine Cell Dedifferentiation in Type 1 Diabetes
ANNA-MARIA ORDELHEIDE, HANS-ULRICH HÄRING, DOMENICO ACCILI, Tübingen, Germany, New York, NY
In type 2 diabetes (T2D), pancreatic beta cell failure is associated with
beta cell dedifferentiation. It’s not known whether dedifferentiation also
occurs in type 1 diabetes (T1D). To answer this question, we analyzed pancreatic tissue sections from 11 controls and 16 T1D donors from the nPOD database. To assess dedifferentiation, we performed immunohistochemistry
with insulin, glucagon, somatostatin, and a newly identified marker of beta
cell dedifferentiation, aldehyde dehydrogenase isoform 1A3 (ALDH1A3). In
control islets, we detected insulin-, glucagon, and somatostatin-producing
cells. We identified two sub-populations of ALDH1A3-immunoreactive cells,
one that was hormone-positive and one that was hormone-negative. In T1D
subjects, insulin-immunoreactive cells were rare. In contrast, the number of
glucagon-positive cells rose threefold, as did the number of somatostatinpositive cells. The number of ALDH1A3-immunoreactive/hormone-positive
cells increased in T1D in a manner commensurate with the overall increase.
The number of ALDH1A3-immunoreactive/hormone-negative cells also increased. Interestingly, we also saw rare residual beta cells with ALDH1A3
immunoreactivity in T1D. We suggest that ALDH1A3-positive/hormone-
Supported By: Novo Nordisk; Canadian Institutes of Health Research
ADA-Funded Research
For author disclosure information, see page LB98.
LB81
POSTERS
GLP1 activates its receptor, GLP1R, to enhance insulin secretion. The activation and transduction of GLP1R requires complex interactions with a host
of accessory proteins, most of which remain largely unknown. In this study,
we used a membrane-based split ubiquitin yeast two-hybrid (MYTH) assay
to identify novel GLP1R interactors in both mouse and a human islets. Among
these, the V-type ATPase associated protein 6 (ATP6ap2), was identified in
both mouse and human islet screens. ATP6ap2 was shown to be abundant
in in islets where it was primarily localized to beta cells. When GLP1R and
ATP6ap2 were co-expressed in beta cells, GLP1R was shown to directly interact with ATP6ap2, as assessed by co-immunoprecipitation. In INS-1 cells,
overexpression of ATP6ap2 did not affect insulin secretion, however, siRNA
knockdown decreased both glucose stimulated- and GLP1-induced insulin
secretion (GIIS). Decreases in GIIS were accompanied by attenuated GLP1
stimulated cAMP accumulation. Since ATP6ap2 is a subunit required for VATPase assembly of insulin granules, it has been reported to be involved in
granule acidification. In accordance with this, we observed impaired insulin
granule acidification upon ATP6ap2 knock-down but paradoxically increased
proinsulin secretion. Importantly ATP6ap2 is also known as the renin receptor, and we further show that it mediates renin’s insulinotropic properties in
beta cells. Taken together our findings identify a group of proteins that interact with the GLP1R. We further show that one interactor, ATP6ap2, plays
a novel dual role in beta cells, modulating both GLP1R signalling and insulin
processing to affect insulin secretion.
Islet Biology/
Insulin Secretion
FEIHAN F. DAI, ALPANA BHATTACHARJEE, YING LIU, MING ZHANG, XINYE WANG,
MICHAEL B. WHEELER, Toronto, ON, Canada
Islet Biology—Beta Cell—Stimulus-Secretion Coupling and Metabolism
330‑LB
(GSIS) from pancreatic beta cells. However, a debate has existed since the
1970’s concerning whether or not beta-cell cAMP signaling is essential for
glucose alone to stimulate insulin secretion. Here we report that GSIS from
isolated human and rat islets is cAMP-dependent, as revealed through the
use of a highly membrane permeable para-acetoxybenzyl (pAB) ester prodrug that is a derivative of the cAMP antagonist Rp-cAMPS. Kinetic assays of
perifused islets demonstrate that pretreatment of human or rat islets with
10 micromolar Rp-8-Br-cAMPS-pAB leads to a marked inhibition (up to 80%)
of first-phase GSIS, as measured in response to a step-wise increase of glucose concentration. In contrast, second-phase GSIS is inhibited to a smaller
extent, and neither phase of GSIS is affected by a negative control pAB
compound. Using an assay for cAMP-regulated gene expression, or an assay
for A-kinase activity reporter activation, we validate that in living cells, low
micromolar concentrations of Rp-8-Br-cAMPS-pAB inhibit cAMP-dependent
protein kinase (PKA) activation. BRET analysis also validates that Rp-8-BrcAMPS-pAB inhibits PKA dissociation and therefore activation under conditions in which the holoenzyme’s C-alpha catalytic subunit is reconstituted
with the type 1 or type 2 regulatory subunit isoforms. Novel actions of RpcAMPS-based analogs to antagonize cAMP sensor Epac1 and Epac2 activation are also validated in an in vitro Rap1 activation assay, or in a FRET assay
using genetically-encoded biosensors. Thus, in addition to revealing the
cAMP-dependence of first-phase GSIS, these findings establish a pAB-based
chemistry for the synthesis of highly membrane permeable prodrug derivatives of Rp-cAMPS that act with micromolar or even nanomolar potency to
inhibit cAMP signaling in living cells.
Utility of Mip-CreERT Mice with Artifactual Expression of Human
Growth Hormone in Pancreatic Beta Cell Research
DANIEL OROPEZA, NATHALIE JOUVET, LIONEL BUDRY, KHALIL BOUYAKDAN,
SARAH SCZELECKI, GABRIELLE PERRON, VALERIE BERGERON, JOSHUA C.
NEUMAN, HARPREET BRAR, RACHEL FENSKE, CLEMENCE MEUNIER, JULIE LACOMBE, JONATHAN E. CAMPBELL, MICHELLE E. KIMPLE, DANIEL J. DRUCKER,
ROBERT A. SCREATON, VINCENT POITOUT, MATHIEU FERRON, THIERRY ALQUIER,
JENNIFER L. ESTALL, Montreal, QC, Canada, Madison, WI, Toronto, ON, Canada, Ottawa, ON, Canada
There is growing concern over confounding artifacts associated with beta-cell-specific Cre-recombinase transgenic models, raising questions about
their general usefulness in research. The inducible beta-cell-specific transgenic (MIP-CreERT1Lphi) mouse was designed to circumvent many of these issues and we investigated whether this tool effectively addressed concerns
of ectopic expression and disruption of glucose metabolism. Recombinase
activity was absent from the CNS using a reporter line and high-resolution
microscopy. Despite increased pancreatic insulin content, MIP-CreERT mice
on chow diet had normal blood glucose levels, glucose tolerance and insulin
sensitivity, and equivalent insulin secretion in response to glucose in vivo and
in vitro. Unexpectedly, MIP-CreERT mice were protected from high-fat/STZinduced hyperglycemia and this was not due to inhibition of STZ-mediated
beta-cell death. Ectopic human growth hormone (hGH) was highly expressed
in MIP-CreERT islets, potentially explaining increased insulin content, islet
number and mass following high-fat/STZ. However, circulating insulin levels
remained similar to controls, while STZ-associated increases in alpha-cell
number and serum glucagon were significantly blunted by presence of the
transgene. These studies reveal important new insight into the strengths
and limitations of using the MIP-CreERT mouse line for beta-cell research.
Supported By: American Diabetes Association (7-12-BS-077 to G.G.H.); National
Institutes of Health-National Institute of Diabetes and Digestive and Kidney Diseases (R01DK069575)
333‑LB
Supported By: Canadian Diabetes Association (OG3123843JE)
Serotonin Is a Paracrine Signal that Stimulates Insulin Secretion in
Human Pancreatic Islets
331‑LB
β-catenin Is Required for Incretin Potentiated Insulin Secretion
from Pancreatic β-Cells and Regulates Insulin Vesicle Localization
JOANA ALMACA, JUDITH T. MOLINA, DANUSA MENEGAZ, ALEJANDRO CAICEDO, Miami, FL
Endocrine cells and neurons share many features despite their different
embryonic origins. In particular, islet beta cells share with serotonergic
neurons a common ability to synthesize, store and release serotonin (5-HT;
Ohta Y et al (2011) Diabetes). 5-HT has been shown to play an important role
in mouse islet plasticity. For instance, under conditions of higher metabolic
demand such as pregnancy, 5-HT stimulates beta cell proliferation (Kim et
al (2010) Nat Med) and glucose-stimulated insulin secretion (Ohara-Imaizumi
M (2013) PNAS) in pregnant mice. The role of 5-HT as a local paracrine signal
in human islets is not known. We found that a subset of beta cells contained
high levels of 5-HT in islets of non-pregnant human donors, which contrasts
with low levels of 5-HT found in isles of non-pregnant mice. Human beta
cells also expressed tryptophan hydroxylase isoform 1 (Tph1), the rate-limiting enzyme for 5-HT biosynthesis in nonneuronal tissues, and produced 5-HT
in vitro, as suggested by a significant decrease in the number of 5-HT positive cells after islet incubation with the Tph inhibitor p-chlorophenylalanine.
Using 5-HT biosensors, we observed that, besides synthesizing and storing
5-HT, human islets were also able to release 5-HT in a glucose-dependent
and pulsatile manner that resembles insulin secretion. To determine if 5-HT
has any autocrine/paracrine effect, we examined in perifusion studies how
exogenous 5-HT affects glucose-stimulated insulin secretion from human
islets. 5-HT (0.1, 1 μM) amplified glucose-induced insulin secretion. This effect was not mediated by the 5-HT receptors 5-HT2 or 5-HT3 as cytoplasmic
calcium levels in intact human islets or in dispersed human beta cells did not
change upon 5-HT application. 5-HT can bind as well to other G-protein coupled receptors (5-HT1, 5-HT4-7) that use cAMP as intracellular messenger.
We are currently identifying which 5-HT receptors are expressed in human
islet cells and mediate the stimulatory effect on insulin secretion.
BRIE SORRENSON, EMMANUELLE COGNARD, WILLIAM E. HUGHES, YANYUN
FU, WEIPING HAN, PETER SHEPHERD, Auckland, New Zealand, Sydney, Australia,
Singapore, Singapore
We recently provided evidence that modulating the Wnt signaling factor
-catenin in the INS-1E -cell model affects glucose-stimulated insulin secretion and found that the levels of -catenin can be dynamically regulated in
these cells by changes in glucose levels. Here we have extended our preliminary findings to investigate whether -catenin is also required for the effect
of incretin hormones and whether it has a role in the acute events regulating
insulin secretory vesicle trafficking. We found that reducing -catenin levels using siRNA knockdown attenuates GSIS in a range of -cell models and
blocks the ability of GLP-1 to potentiate this. This could be mimicked in both
-cell models and isolated islets by short-term exposure to the -catenin inhibitory drug pyrvinium, suggesting that -catenin is required for the processes
regulating trafficking and/or release of pre-existing insulin granules rather
than for those regulated by gene expression. This was further supported by
the finding that short-term treatment with a GSK3 inhibitor, which is known
to increase -catenin levels, results in an increase in insulin secretion. Using total internal reflectance fluorescence (TIRF) microscopy, we found that
-catenin is required for the glucose- and incretin- induced depletion of insulin
vesicles from near the plasma membrane and that lack of -catenin perturbs
insulin vesicle release from the cell periphery. We found that overexpression
of the transcriptional co-activator of β-catenin, TCF7L2, attenuated insulin
secretion, which implies the importance of β-catenin in insulin secretion is
not solely due to transcriptional effects. Overall we present a requirement
for -catenin in the mechanisms that are involved in modulating insulin secretory vesicle localization and/or fusion.
POSTERS
Islet Biology/
Insulin Secretion
Supported By: Health Research Council of New Zealand; National Heart Foundation of New Zealand
334‑LB
Preserving Pdx1 Expression in Diabetic β-Cells Improves Glycemic
Control In Vivo
332‑LB
YUICHI YAMAMOTO, TAKESHI MIYATSUKA, KAZUYUKI MIYASHITA, SHUGO
SASAKI, FUMIYO KUBO, NAOKI SHIMO, TETSUYUKI YASUDA, TAKAAKI MATSU­
OKA, HIDEAKI KANETO, IICHIRO SHIMOMURA, Suita, Japan, Tokyo, Japan, Osaka,
Japan
Rp-cAMPS-pAB Prodrugs Reveal the cAMP Dependence of Human
and Rat Islet First-Phase Glucose-stimulated Insulin Secretion
COLIN A. LEECH, FRANK SCHWEDE, OLEG G. CHEPURNY, MELANIE KAUFHOLZ,
DANIELA BERTINETTI, YINGMIN ZHU, FANG MEI, XIAODONG CHENG, JOCELYN
E. MANNING FOX, PATRICK E. MACDONALD, HANS-G GENIESER, FRIEDRICH W.
HERBERG, GEORGE G. HOLZ, Syracuse, NY, Bremen, Germany, Kassel, Germany,
Houston, TX, Edmonton, AB, Canada
Pdx1 has been shown to play a crucial role in maintaining mature β-cell
function, regulating several β-cell-related genes, such as insulin and Slc2a2
(Glut2). In addition, Pdx1 expression levels are compromised in the islets of
human diabetic patients and rodent models. When we quantified the expression levels of Pdx1 in islets of Ins2Akita (Ins2Wt/C96Y) mice, in which
a dominant mutation in the Ins2 gene causes β-cell failure, Pdx1 was sig-
Adenosine-3’,5’-cyclic monophosphate (cAMP) elevating agents such as
the incretin hormone GLP-1 potentiate glucose-stimulated insulin secretion
ADA-Funded Research
For author disclosure information, see page LB98.
LB82
Islet Biology—Beta Cell—Stimulus-Secretion Coupling and Metabolism
nificantly decreased compared with control Ins2Wt/Wt littermates (p=0.03).
To test whether preserving expression of Pdx1 affects the phenotypes of
Ins2Akita mice, we generated a transgenic mouse “Pdx1-CreER; CAG-CATPdx1 (βPdx1)” that conditionally and specifically expressed Pdx1 in β cells,
and crossed βPdx1 mice with Ins2Akita mice. In the islets of βPdx1; Ins2Akita mice, over 80% of β cells expressed transgenic Pdx1, which was detected
by immunohistochemistry for FLAG-tag epitope (Miyatsuka et al. Genes Dev
20, 1435-1440, 2006). The βPdx1; Ins2Akita mice at 8 weeks of age exhibited significantly lower HbA1c (5.1 ± 0.3 vs. 7.1 ± 1.1, p=0.01) and fasting
plasma glucose levels (258.0 ± 23.6 vs. 333.4 ± 58.2, p=0.04), compared with
the control Ins2Akita littermates. Furthermore, real-time PCR revealed that
glucokinase (Gck) was upregulated in βPdx1; Ins2Akita mice compared with
Ins2Akita littermates. Thus, sustained expression of Pdx1 improved glucose
profile of diabetic Ins2Akita mice, suggesting the critical role of Pdx1 in regulating β-cell function under diabetic conditions.
ATP usage. During acute regulation of insulin secretion by cytochrome c and
L-type calcium channels, flux of electrons from cytochrome c to H2O2 ensure
that secretion is only sensitive to changes in extracellular glucose and not
energy needs of the cell.
Supported By: American Diabetes Association (1-13-IN-53, 1-15-IN-65 to I.S.)
337‑LB
Changes in Glucose-stimulated Insulin Secretion and TORC1 Sig‑
naling in Response to Glucolipotoxicity
KAREL A. ERION, BARBARA E. CORKEY, JUDE T. DEENEY, LUCIA E. RAMEH, Boston, MA
The metabolic stress caused by diet-induced obesity is accompanied by
insulin hypersecretion. In cultured cells, exposure to high levels of glucose
and/or fatty acids can result in metabolic stress or glucolipotoxicity (GLT).
GLT increase basal insulin secretion through ROS, although the molecular
mechanisms involved are not clear. Target of Rapamycin Complex 1 (TORC1)
is a kinase complex involved in the regulation of anabolic processes that
control cell mass in response to nutrients and growth factors. A high fat
diet results in elevated TORC1 activity in peripheral tissues as well as in
b-cells. Hyperactivation of TORC1 in b-cells by knockout of the TORC1 inhibitor Tsc2 results in hyperinsulinemia. Conversely, TORC1 inhibition by rapamycin treatment of isolated islets inhibits insulin secretion and prevents
adaptation to hyperglycemia in obese mice. In order to better understand the
molecular mechanisms that contribute to GLT-induced insulin hypersecretion, we examined the effects of chronic exposure to high glucose on TORC1
signaling in b-cells. INS-1 cells were cultured in low (4 mM) or high (11 mM)
glucose to mimic the normoglycemic or hyperglycemic state, respectively.
Cells cultured in high glucose had increased basal insulin secretion and a
left shift in the glucose concentration dependency for insulin secretion, as
compared to cells in low glucose. Phosphorylation of the TORC1 substrate
p70S6K and S6 was significantly lower in cells cultured under low glucose,
but the fold response to growth factor and amino acid stimulation was increased, as compared to cells in high glucose. In addition, cells cultured in
high glucose had increased phosphorylation of PIP4k, a novel substrate for
TORC1. PIP4k localized to Golgi in INS-1 cells cultured in 4 mM glucose, but
in 11 mM glucose, PIP4k localized to cytoplasmic vesicles. Together, these
results indicate that TORC1 signaling is affected by GLT and may contribute
to hyperinsulinemia in obese patients.
335‑LB
Investigating the Role of the Zinc Transporting Protein ZnT8 in the
Pathogenesis of Type 2 Diabetes
KRISTINA NORDÉN, DEEPAK JAIN, JULIA BROSNAN, ANN-MARIE LA RONDERICHARD, JENS LAGERSTEDT, Lund, Sweden, Boston, MA
The zinc transporting protein ZnT8, encoded by the SLC30A8 gene, is
located in the membranes of the insulin secretory granules (ISG). A single
nucleotide polymorphism (SNP), introducing a switch from a tryptophan (W)
to an arginine (R) at amino acid position 325 in this protein, has by genome
wide association studies been linked to an increased risk of developing type
2 diabetes (T2D). The amino acid switch is believed to confer an altered zinc
transporting capacity of the ZnT8 protein. This would induce a local effect
on the zinc dependent packing, and storage of the insulin hexamers in the
ISGs and potentially also affect peripheral tissues due to an increased hepatic clearance of the secreted insulin. Additionally, and surprisingly, lossof-function mutations in the SLC30A8 gene have recently been shown to
confer protection against T2D in human subjects. In order to investigate the
effect of the SNP on ZnT8 structure and function we have set up production of this protein in insect cells utilizing the Baculovirus Expression Vector
System (BEVS). Protein carrying either a W or an R at position 325 has been
successfully expressed and membranes from the ZnT8 producing cells have
been isolated. To be able to evaluate the zinc transporting capacity of the
ZnT8 variants, these membranes have been incorporated into giant unilamellar vesicles (GUVs). By employing fluorescently labeled antibodies we can
show that the recombinantly expressed ZnT8 protein is properly inserted
into the lipid bilayer of the GUVs and that it is evenly distributed over the
surface of the vesicles. A major advantage with the GUV-approach is that a
defined chemical composition of the lumenal and exterior environment with
regard to, e.g., pH, ions, and fluorescent zinc probes, can be established that
allow for detailed kinetic analyses of ZnT8 variant-specific zinc fluxes.
338‑LB
The GEFs Kalirin/Trio Contribute to Beta-granule Remodeling and
Exocytosis
Insulin secretion from pancreatic β cells is a finely tuned integration of
metabolic events and signaling pathways that regulate the fusion competence of granules. Newly synthesized, immature granules (ISGs) undergo
maturation that includes content removal and association with the F-actin
rich cortex. Together these events contribute to granule competence for exocytosis. Because the Rho GDP/GTP exchange factors (GEFs) Kalirin and Trio
regulate vesicular budding from ISGs in non β cells, we targeted the GEFs by
small molecule inhibitors or genetic ablation and characterized proinsulin/
insulin release by direct exocytosis or vesicular budding. Inhibition of activity (Kalirin/Trio) or Kalirin depletion stabilized phalloidin stained F-actin to
the actin depolymerizing toxin cytochalasin D and simultaneously impaired
glucose stimulated hormone output. Delivery of viral protein VSVG to the
plasma membrane (constitutive secretion) was intact; release of newly synthesized proinsulin/insulin through constitutive-like vesicular budding, was
attenuated. Membrane depolarization or stimulation with high glucose plus
the incretin GLP-1 bypassed Kalirin/Trio requirement. Islet exposure to these
secretagogues under basal conditions, including pharmacological manipulations of the submembrane actin barrier did not restore constitutive-like
secretions. We conclude that exocytosis of granules already at the plasma
membrane (first-phase) and the second sustained phase that depends on
newly recruited “Restless Newcomers” can bypass Kalirin/Trio function.
The relatively stronger reliance on GEF activity for newly made granules and
ISG derived vesicles suggests that organelle localized, Kalirin/Trio targets
are molecular mediators of exocytosis.
336‑LB
Interaction of L-type Calcium Channels with Cytochrome c and H2O2
in the Regulation of Insulin Secretion by Pancreatic Beta Cells
ADAM S. NEAL, HUILIANG ZHANG, AUSTIN ROUNTREE, KELLY KERNAN, WILLIAM OSBORNE, WANG WANG, IAN SWEET, Seattle, WA
The redox state of cytochrome c plays a signaling role in the regulation of
insulin secretion over and above its role in transferring electrons in the electron transport chain. The redox state of the protein is exquisitely sensitive
to glucose, while being unaffected by energy usage and changes in cytosolic
calcium. These intrinsic mechanisms are unique to the beta cell and their
impairment has been shown to lead to impaired glucose-stimulated insulin
secretion. We tested the hypothesis that the critical stability of cytochrome
c occurs through buffering of electron flow to H2O2. Real time experiments
were carried out using a perifusion system loaded with islets or INS-1 cells.
Genetically-encoded sensors (HyPer), in the presence and absence of catalase, were used to measure H2O2. Buffering of reduced cytochrome c by
production of H2O2 was tested by measuring cytochrome c, H2O2 and oxygen consumption in response to agents affecting cytosolic calcium via either
L-type calcium channels or calcium release from the endoplasmic reticulum.
During exposure of cells to agents that altered calcium influx through L-type
calcium channels (including diazoxide, nimodipine, BayK 8644 and potassium) H2O2 generation was inversely proportional to changes in calcium influx
and proportional to the flow of electrons from cytochrome c away from respiration. Consistent with studies where calcium from L-type calcium channels had preferential access to machinery regulating exocytosis, increased
cytosolic calcium induced by a blocker of SERCA (thapsigargin) had little
affect on H2O2. Calcium-mediated flow of electrons from cytochrome c to
H2O2 accounts for the stability of reduced cytochrome c during changes in
ADA-Funded Research
For author disclosure information, see page LB98.
LB83
POSTERS
REGINA KULIAWAT, Bronx, NY
Islet Biology/
Insulin Secretion
Supported By: National Institutes of Health (DK63219, DK035914)
Islet Biology—Signal Transduction
Islet Biology—Signal Transduction
diet (HFD) for 14 weeks. We observed no difference in starved or glucose-induced insulin levels between CD-fed control and Dox-treated mice. 14 weeks
of HFD feeding resulted in elevated starved insulin levels in control mice but
not in NOX5-expressing mice. Glucose injection increased insulin levels by
50% in control HFD-fed mice but failed to induce insulin secretion in NOX5
transgenic mice. In vitro, islets isolated from control HFD-fed mice showed
a 1.5 fold increase in insulin secretion upon glucose exposure. By contrast,
islets derived from Dox-treated HFD-fed mice lacked glucose-induced insulin response. Taken together, our data demonstrate that elevated levels of
NOX5-derived ROS might contribute to deteriorated β-cell function and design NOX5 as a potential therapeutic target to maintain insulin secretion in
obese and diabetic patients.
339‑LB
Regulation of Polypyrimidine-Tract Binding Protein Expression by
Insulin Signaling Pathway in Pancreatic β-Cell
JEONG JAE SHIN, JIHYE KIM, JUNG SEOK KIM, JUN GI RHO, WOOK KIM, Suwon,
Republic of Korea
Polypyrimidine tract-binding protein 1 (PTBP1), also named hnRNP I, stabilizes preproinsulin mRNA by binding to the 3’-UTR in pancreatic β cells.
However, the underlying mechanism that regulates PTBP1 expression in
pancreatic β-cells is not clear. We now report that PTBP1 is present in both
mouse and human pancreatic β cells, where its levels are regulated by the
insulin receptor (IR) signaling pathway. PTBP1 abundance in immortalized β
cells isolated from the pancreas of wild-type (βIRWT) mice was significantly
higher and more glucose-inducible than that in β cells isolated from an insulin receptor (IR)-null (βIRKO) mouse. Consistently, treatment with insulin
elevated PTBP1 levels in βIRWT cells, but not in βIRKO. These findings were
also true in other β-cell lines (MIN6 and βTC6). In sum, our results identify
insulin as a pivotal regulator of PTBP1 expression in pancreatic β cells.
Supported By: Ernst and Lucie Schmidheiny Foundation; Société Francophone
de Diabète
342‑LB
Mitochondrial GTP Contributes to ChREBP Activity and Susceptibil‑
ity to Cell Death in INS-1-derived Cell Lines
LEE B. HONIG, BENNETT J. DAVENPORT, NAGESHA G. KONDEGOWDA, ANILA K.
MADIRAJU, REBECCA L. PONGRATZ, RUPANGI C. VASAVADA, DIRK HOMANN,
RICHARD G. KIBBEY, DONALD SCOTT, New York, NY, New Haven, CT
340‑LB
Carbohydrate Response Element Binding Protein (ChREBP) is a glucosesensing transcription factor necessary for a glucose-stimulated proliferation
in pancreatic beta cells, a process that drives adaptive beta cell mass expansion. ChREBP also drives Txnip expression, leading to apoptosis in response
to glucolipotoxicity. The mechanisms of activation or inhibition of ChREBP
activity are poorly understood, but important for beta cell function. We
aimed to determine if mitochondrial GTP (mtGTP) influences ChREBP activity
via generation of cytoplasmic phosphoenolpyruvate (PEP). By RT-PCR and
BrdU staining, respectively, we found that INS-1-derived 832/13 cells overexpressing the ATP isoform of Succinyl CoA Synthetase (SCS-ATP, reduced
relative mtGTP) exhibit attenuated glucose-stimulated gene expression and
proliferation compared to controls (both by ~25%, p <0.05, n=3). ChREBP
Beta promoter activity was significantly decreased in response to glucose in
SCS-ATP cells compared to 832/13 cells (~45%, p<0.01, n=3). Interestingly,
SCS-ATP cells had significantly lower relative Txnip mRNA expression (54%,
p<0.01, n=5). Upon exposure to 20 mM glucose and 0.5 mM palmitate, SCSATP overexpression conferred resistance to glucolipotoxicity as per FACS
Annexin V staining (50%, p<0.05, n=4) and cleaved caspase 3 immunostaining (42%, p<0.05, n=3). Exposure of SCS-ATP cells to cytokines resulted in
significant protection from cell death (66%, p=0.0001, n=4). Conversely,
overexpression of the GTP-binding isoform (SCS-GTP, increased mtGTP) resulted in an upward trend of glucose-stimulated gene expression, ChREBP
Beta and LPK promoter activity. The rates of both glucose-stimulated proliferation and response to cell death were found to be comparable to controls.
In conclusion, mtGTP was identified as a potential novel regulator of ChREBP
activity in INS-1 832/13 cells, possibly through the generation of PEP and the
formation of an ATP-regenerating system.
EphA4-mediated Juxtacrine Signaling Regulates Glucagon Secre‑
tion through Changes in F-Actin Density
TROY HUTCHENS, DAVID W. PISTON, Nashville, TN, St. Louis, MO
The therapeutic success of insulin in the clinical management of diabetes
has led to a robust understanding of the molecular mechanisms underlying
β-cell function and insulin secretion. However, the cellular and molecular
mechanisms underlying α-cell function and glucagon secretion remain poorly understood despite the critical role that dysfunctional glucagon secretion
and hyperglucagonemia play in the pathophysiology of diabetes. Glucagon
secretion from flow-sorted α-cells is increased over that from islets, and
it is not inhibited by glucose elevation, similar to what is seen in diabetes.
These data suggest that intra-islet signaling, through either paracrine or juxtacrine pathways, plays an important role in the tonic inhibition of glucagon
secretion. Here, we present new data in support of novel juxtacrine-mediated regulation of glucagon secretion where contact-dependent signaling
through the EphA4 receptor is responsible for tonic inhibition of glucagon
secretion by maintaining a dense F-actin network. In isolated islets, stimulation of EphA signaling results in a 41±8% decrease in glucagon secretion and
a 11±3% increase in α-cell F-actin density. Conversely, inhibition of EphA
signaling and EphA4-specific signaling results in a 212±63% and 99±38% increase in glucagon secretion respectively, with a 44±2% decrease in α-cell
F-actin density associated with inhibited EphA signaling. α-cell-specific
knockout of EphA4 results in a 53±6% increase in glucagon secretion from
isolated islets and a 32±5% decrease in α-cell F-actin density. Restoring
EphA signaling in sorted α-cells corrects glucagon hypersecretion and
restores normal glucose-inhibition of glucagon secretion, reducing glucagon secretion by 81±2% at high glucose. This juxtacrine-mediated model
of glucagon secretion opens a new pathway for therapeutically targeting
glucagon secretion, an important step in addressing the multiple hormone
dysfunctions of diabetes.
Supported By: F30DK098838; T32GM07347; R01DK098659
341‑LB
Beta Cell–specific Overexpression of the NADPH Oxidase 5 (NOX5)
Deteriorates Islet Function in High-Fat Diet-exposed Mice
POSTERS
Islet Biology/
Insulin Secretion
CHRISTELLE VEYRAT-DUREBEX, DOMENICO BOSCO, KARIM BOUZAKRI, CAROLINE AROUS, GERHARD CHRISTOFORI, CHRISTOPHER KENNEDY, ILDIKO SZANTO, Geneva, Switzerland, Basel, Switzerland, Ottawa, ON, Canada
RReactive oxygen species (ROS) play important roles in islet insulin secretion and β-cell survival. NADPH oxidases (NOX-es) are ROS-producing
enzymes that are present in islets. NOX5 is a particular isoform expressed in
human but not in rodents, and its activity is induced by Ca2+, a major regulator of insulin secretion. We applied RT-PCR in isolated human islets and validated expression of NOX2, NOX4 and NOX5 mRNAs. In situ hybridization on
pancreatic sections confirmed the presence of NOX5 mRNA in the majority
of islet cells. Real-time PCR demonstrated an upregulation of NOX5 in islets
upon hyperglycemic (16.7mM) incubation. In line with these results, immunofluorescence detected NOX5 labeling in insulin-positive cells in dispersed
human islets in the presence of 16.7mM glucose, though not in direct colocalization with insulin-containing vesicles. To investigate the role of NOX5 in
insulin secretion, we created mice with doxycycline-inducible, β-cell specific
expression of NOX5. Mice were provided or not with doxycycline (Dox) and
then were administered either a control chow (CD) or a high-fat containing
ADA-Funded Research
For author disclosure information, see page LB98.
LB84
Abdominal adiposity 183‑LB
Aboriginal Australians 162‑LB
Acarbose 117‑LB
Actin polymerization 285‑LB
Acute myocardial infarction 13‑LB
Add-on therapy 115‑LB
Adeno-associated virus 223‑LB
Adherence 49‑LB, 135‑LB
Adipocyte 226‑LB, 234‑LB, 267‑LB
Adipocyte hypertrophy 228‑LB
Adipocyte progenitors 298‑LB
Adipocyte protein 2 108‑LB
Adiponectin 22‑LB, 55‑LB, 224‑LB, 227‑LB
Adiponectin signaling 293‑LB
Adipose 222‑LB
Adipose inflammation 294‑LB
Adipose tissue 233‑LB, 240‑LB, 302‑LB
Adipose tissue distribution 318‑LB
Adipose triglyceride lipase 231‑LB
Adolescent 146‑LB
AFAP1 291‑LB
Affordable Care Act 136‑LB
Aging 252‑LB
AGP standardized glucose reporting 79‑LB
AgRP neurons 288‑LB
Air pollution 179‑LB
Akita mouse 334‑LB
ALDH1A3 327‑LB
All-cause mortality 7‑LB
Alpha-cell glucagon secretion 340‑LB
Antibiotic 149‑LB
Aortic stiffness 286‑LB
ApoA1 263‑LB
Apoptosis 258‑LB, 321‑LB
Arginine 253‑LB
Artificial pancreas 97‑LB, 98‑LB, 100‑LB, 101‑LB
AS160 247‑LB
Association mapping 201‑LB
Atherosclerosis 1‑LB
Autoantibodies 29‑LB
Autoantigen 213‑LB
Autoimmune diabetes 102‑LB
Autoimmunity 218‑LB
Autonomic neuropathy 29‑LB, 30‑LB, 146‑LB
Autophagy 244‑LB, 264‑LB
Bariatric surgery 300‑LB, 311‑LB, 315‑LB
Basal insulin 87‑LB
Basal insulin peglispro 88‑LB, 89‑LB
Berberine 238‑LB
Beta catenin 331‑LB
Beta cell 280‑LB, 323‑LB, 342‑LB
Beta cell dedifferentiation 327‑LB
Beta cell differentiation 326‑LB
Beta cell dysfunction 313‑LB
Beta cell function 145‑LB
Beta cell neogenesis 324‑LB
Beta cell proliferation 322‑LB, 325‑LB
Betatrophin 304‑LB
Blood glucose monitoring 77‑LB, 78‑LB
Body weight 317‑LB
Brown adipose tissue 232‑LB
Brown rice 175‑LB
Caloric restriction 245‑LB, 252‑LB, 271‑LB
cAMP-PKA 129‑LB
Canagliflozin 131‑LB
Carbohydrate counting 148‑LB
Cardiac safety 246‑LB
Cardiometabolic traits 301‑LB
Cardiovascular complications 6‑LB
Cardiovascular diseases 314‑LB
Cardiovascular magnetic resonance 163‑LB
Cardiovascular outcomes 111‑LB
Carrageenan 38‑LB
Cell adhesion 285‑LB, 292‑LB
Cell cycle 151‑LB
Ceramides 265‑LB
Cerebral blood flow 249‑LB
Chikungunya 184‑LB
Childhood obesity 144‑LB
ChREBP 342‑LB
Chronic hyperglycemia 31‑LB, 163‑LB
Chronic kidney disease 25‑LB
Circadian clock 328‑LB
Circulating microvesicles 16‑LB
Clc-5 289‑LB
Clinical studies 100‑LB
Closed-loop 99‑LB
Closed-loop control 101‑LB
Closed-loop technology 66‑LB
CLOUD 70‑LB
CNX-013-B2 120‑LB
Collaborative goal setting 64‑LB
Colorectal cancer 186‑LB
Colorectal cancer survivor 54‑LB
Comparative effectiveness 115‑LB
Complement 216‑LB
Continuous glucose monitoring 74‑LB, 75‑LB,
80‑LB, 81‑LB, 116‑LB, 143‑LB
Continuous subcutaneous insulin infusion 81‑LB
Controlled-release mitochondrial protonophore
113‑LB
Coronary artery calcium 17‑LB
Coronary artery disease 10‑LB
Corticosteroids 93‑LB
Cost savings 79‑LB
C-peptide 147‑LB, 237‑LB, 306‑LB
Cutaneous nevi 167‑LB
Cyclic adenosine monophosphate 332‑LB
Cyclin-dependent kinase inhibitor 2A 10‑LB
Cytochrome c 336‑LB
Depression 170‑LB
Dextromethorphan 121‑LB
Diabetes 28‑LB, 61‑LB, 121‑LB, 161‑LB, 165‑LB,
167‑LB, 170‑LB, 211‑LB, 214‑LB, 255‑LB,
257‑LB
Diabetes distress 67‑LB
Diabetes duration 237‑LB
Diabetes knowledge 52‑LB
Diabetes management software 70‑LB
Diabetes remission 315‑LB
Diabetes risk factors 175‑LB
Diabetes screening in Asian Americans 166‑LB
Diabetes-associated autoantibodies 147‑LB
Diabetic dyslipidemia 126‑LB
Diabetic foot ulcers 45‑LB
Diabetic ketoacidosis 241‑LB
Diabetic kidney disease 114‑LB
Diabetic nephropathy 19‑LB, 23‑LB
Diabetic neuropathy 30‑LB
Diabetic retinopathy 33‑LB, 34‑LB, 37‑LB
Diagnostic marker 213‑LB
Digital tracking device 49‑LB, 137‑LB
Dipeptidyl peptidase 4 132‑LB, 164‑LB
Disease management 140‑LB
LB85
DJ-1 321‑LB
DPP-4 inhibitor 95‑LB, 127‑LB, 133‑LB, 216‑LB
Drug transport 128‑LB
Dumping syndrome 4‑LB
Dyslipidemia 41‑LB, 42‑LB
Early pregnancy 152‑LB
Ectopic fat 305‑LB
Education 47‑LB
Effects of metformin and lifestyle interventions
17‑LB
Emollient 44‑LB
Empagliflozin 118‑LB, 119‑LB
Employee wellness 140‑LB
EndoC 208‑LB
Endometrial cancer 316‑LB
Endoplasmic-reticulum-associated protein
degradation 234‑LB
Endothelial progenitor cells 16‑LB
Enteroendocrine 275‑LB
Epidemiology 178‑LB, 179‑LB
Epigenetics 151‑LB
eQTL mapping 202‑LB
Exenatide 134‑LB, 317‑LB
Exercise 53‑LB, 54‑LB, 56‑LB, 98‑LB
Exocytosis 332‑LB
Exome chip 204‑LB
Exome variation 308‑LB
Exonic rare variant 200‑LB
Famine exposure 61‑LB
Fasting 47‑LB
Fasting blood glucose 82‑LB
Fasting hyperglycemia 38‑LB
Fatty acids 177‑LB, 250‑LB
Fibroblast growth factor 21 282‑LB
Fibroblast growth factor 23 22‑LB
Fitness 55‑LB
Follicle-stimulating hormone 161‑LB
Food craving 173‑LB
Free fatty acid 270‑LB
Free fatty acid receptor 2 323‑LB
Functional foods 172‑LB
Functional MRI 249‑LB
Gastric inhibitory polypeptide 279‑LB
Gastroparesis 90‑LB
GCGR 272‑LB
GCKR 191‑LB
Gemigliptin 127‑LB
Gender differences 188‑LB
Gene delivery 322‑LB
Gene expression 199‑LB
Gene expression omnibus 229‑LB
Gene-diet intervention 198‑LB
Gene-environment interactions 174‑LB
Genetic risk score 198‑LB, 301‑LB
Genome-wide association study 193‑LB, 207‑LB
Genomics 199‑LB
Gestational diabetes 155‑LB, 156‑LB, 157‑LB,
159‑LB, 160‑LB
Glargine analog 84‑LB
Glibenclamide 320‑LB
GLP-1 18‑LB, 105‑LB, 154‑LB, 272‑LB, 276‑LB,
303‑LB, 307‑LB
GLP-1 agents 130‑LB
GLP-1 receptor 324‑LB, 329‑LB
GLP-1 receptor agonists 107‑LB
GLP-1 secretagogues 112‑LB
Glucagon 2‑LB, 122‑LB, 196‑LB, 273‑LB, 319‑LB
SUBJECT INDEX
SUBJECT Index
SUBJECT INDEX
Glucagon like peptide-1 132‑LB
Glucagon receptor antibody 106‑LB
Glucagon-like peptide-1 analogues 104‑LB
Glucolipotoxicity 337‑LB
Glucose intolerance 248‑LB
Glucose monitoring 73‑LB
Glucose oxidation 6‑LB
Glucose sensor 76‑LB
Glucose transport 245‑LB
Glucose variation 65‑LB
GluN2B 288‑LB
Glycan engineering 210‑LB
Glycated albumin 211‑LB
Glycated CD59 160‑LB
Glycemia 62‑LB
Glycemic control 53‑LB, 91‑LB, 110‑LB, 184‑LB
Glycogen 264‑LB
Glycogen Supercompensation 59‑LB
GPR119 122‑LB, 280‑LB
GPR40 251‑LB
Granule maturation 338‑LB
Group prenatal care 156‑LB
Guidelines 41‑LB, 42‑LB
HbA1c 168‑LB
Health insurance 136‑LB
Health services utilization and expense 26‑LB
Healthcare costs 142‑LB
Heart failure 164‑LB
Hepatic steatosis 297‑LB
Hepatitis C 185‑LB
Hepatocyte nuclear factor-4-alpha 304‑LB
Hepato-preferential insulin action 89‑LB
High dose insulin 83‑LB
High risk adolescents and young adults 50‑LB
Hippo 34‑LB
Histone modifications 318‑LB
Histopathology 192‑LB
Homocysteine 257‑LB
Hospital diabetes management 3‑LB
Human beige adipocytes 298‑LB
Human islet 333‑LB
Human leukocyte antigen 217‑LB
Human regular U-500 insulin 197‑LB
Hyperkalemia 125‑LB
Hypoglycemia 1‑LB, 3‑LB, 78‑LB, 116‑LB
Hypoglycemia overtreatment 5‑LB
Hypothalamic neurogenesis 205‑LB
IGFBP-2 256‑LB
IL6 polymorphism 178‑LB
Immune cell 292‑LB
Immunosuppression 219‑LB
Immunotherapy 217‑LB
Implantable sensor 73‑LB
In vivo adipogenesis 302‑LB
Incarceration 52‑LB
Incretin 275‑LB, 278‑LB
Incretin based therapies 124‑LB
Infant body composition 158‑LB
Inflammation 28‑LB, 123‑LB, 228‑LB, 233‑LB,
240‑LB, 259‑LB, 284‑LB
Inhaled insulin 96‑LB
Injuries 171‑LB
Inpatient diabetes 93‑LB
Insulin 85‑LB, 231‑LB
Insulin action 254‑LB
Insulin analogs 246‑LB
Insulin clearance 254‑LB
Insulin delivery 76‑LB
Insulin glargine 91‑LB, 95‑LB
Insulin pump 148‑LB
Insulin receptor 316‑LB
Insulin receptor knockout 266‑LB
Insulin resistance 20‑LB, 227‑LB, 229‑LB, 235‑LB,
236‑LB, 238‑LB, 239‑LB, 250‑LB, 259‑LB,
261‑LB, 263‑LB, 296‑LB, 310‑LB, 313‑LB
Insulin secretion 331‑LB, 336‑LB
Insulin sensitivity 60‑LB, 271‑LB
Insulin therapy 51‑LB
Insulin-degrading enzyme 218‑LB
Insulin-dependent diabetes mellitus 96‑LB
Insulinization 11‑LB
Insulin-like peptide 5 (INSL5) 276‑LB
Insulin-producing cells 220‑LB
Integrated omics 208‑LB
Interacting proteins 329‑LB
Interferon regulatory factor 6 242‑LB
Interleukin-1 receptor-associated kinase 235‑LB
Intestine 310‑LB
Intracellular calcium 274‑LB
Islet 251‑LB
Islet transplantation 221‑LB
Kidney function 24‑LB
Kisspeptin 273‑LB
LANCL2 69‑LB
Latent autoimmune diabetes in adults 212‑LB
Lead exposure 309‑LB
Leakage 36‑LB
Leptin 40‑LB, 306‑LB
Life course 182‑LB, 183‑LB
Lifestyle trials 180‑LB
Linkage disequilibrium genetic maps 201‑LB,
202‑LB
Lipid dysregulation 282‑LB
Lipidomics 239‑LB
Lipids 243‑LB
Lipocalin 223‑LB
Lipogenesis 283‑LB
Lipolysis 262‑LB
Lipoprotein 284‑LB
Lipotoxicity 39‑LB
Liraglutide 4‑LB, 83‑LB
Liver 261‑LB
Liver enzyme 200‑LB
Long-acting insulin 84‑LB, 86‑LB
Long-term 221‑LB
Long-term type 1 diabetes 57‑LB
Lorcaserin 299‑LB
Low-dose Pioglitazone 110‑LB
L-PGDS 277‑LB
MafA 326‑LB
Maternal nutritional intake 158‑LB
Meal tolerance test 253‑LB
Measurement imprecision 71‑LB
Measuring glucagon 319‑LB
Medicare 139‑LB
Medication adherence 142‑LB
Medication safety renal tubular harm 26‑LB
Mediterranean diet 48‑LB
Membrane fluidity and inflammation 177‑LB
Mesenchymal precursor cell 23‑LB
Mesenchymal stem cells 219‑LB, 220‑LB
Metaanalysis 124‑LB
Metabolic adaptation 300‑LB
Metabolic disorder 294‑LB
Metabolic memory 8‑LB
Metabolic syndrome 314‑LB
Metabolism 268‑LB
Metabolomics 241‑LB
Metformin 117‑LB, 128‑LB, 129‑LB, 131‑LB
Methylglyoxal 35‑LB
Microarray 33‑LB
MicroRNA 8‑LB, 55‑LB, 325‑LB
LB86
Mitochondria 269‑LB, 270‑LB
Mitochondrial dysfunction 287‑LB
Monoclonal antibody 108‑LB
Monogenic diabetes 191‑LB, 192‑LB
MR spectroscopy 31‑LB
mTOR complex 2 236‑LB
Multi-ethnic cohort study 193‑LB
Multivitamin 176‑LB
Muscle 206‑LB
Muscle perfusion 56‑LB
Myeloperoxidase 293‑LB
Myopia 203‑LB
Myths 51‑LB
NADPH oxidase 5 341‑LB
NASH 258‑LB
Niacin 224‑LB
Nitrotyrosine 32‑LB
Non-alcoholic fatty liver disease 134‑LB, 260‑LB
Non-alcoholic steatohepatitis 113‑LB, 260‑LB
Novel basal insulin 82‑LB
Obesity 152‑LB, 195‑LB, 222‑LB, 278‑LB, 289‑LB,
303‑LB, 308‑LB, 309‑LB
Obesity in pregnancy 153‑LB
Obesity-related kidney disease 18‑LB
Observational multinational study 169‑LB
Overexpression 194‑LB
Oxidative stress 172‑LB
Paralemmin 212‑LB
PARP14 295‑LB
PCSK2 196‑LB
PCSK9 40‑LB
Pdx1 334‑LB
Pediatrics 143‑LB
Pellino 297‑LB
Perfluorocarobons 24‑LB
Perilipin 5 262‑LB
Pharmacogenetics 197‑LB
Pharmacokinetics 106‑LB
Phosphatases 247‑LB
Phosphodiesterase type 5 inhibitor 7‑LB, 9‑LB
Physician communication 63‑LB
Pioglitazone 169‑LB
Pirfenidone 45‑LB
PKPD model 86‑LB
Plasminogen activator inhibitor-1 12‑LB
Pleiotropy 203‑LB
Point-of-care testing 168‑LB
Polarization 242‑LB
Polyethylene glycol 88‑LB
Polypyrimidine tract-binding protein 339‑LB
Postprandial 62‑LB
Prandial insulin 92‑LB
Prediabetes 14‑LB, 182‑LB
Prevalence 165‑LB
Progesterone 19‑LB
Proinsulin secretion 338‑LB
Race 15‑LB
Racial disparities 141‑LB
RAGE gene 190‑LB
Randomized Clinical Trial 111‑LB, 153‑LB
Ranibizumab 37‑LB
Rapid-acting insulins 107‑LB
Rasch analysis 67‑LB
Reactive oxygen species 341‑LB
Real-world use 87‑LB
Recurrent cardiovascular events 162‑LB
Red wine polyphenols 60‑LB
Renin-angiotensin-aldosterone system 125‑LB
Resilience 150‑LB
Retinal screening 141‑LB
Retinoid X receptor agonist 120‑LB
Src kinases 291‑LB
Starvation 268‑LB
Streptozotocin 320‑LB
Stress 150‑LB
Structural equation model 64‑LB
Sulfonylurea 299‑LB
Sulforaphane 296‑LB
suPAR 25‑LB
Synip 20‑LB
Systemic review 137‑LB
Technology-smart phone app 68‑LB
Technosphere insulin inhalation powder 94‑LB
TEDDY 149‑LB
Testosterone 9‑LB
Therapeutic 69‑LB
Toll-like receptors 214‑LB
TORC1 337‑LB
Torin1 244‑LB
Transcription 206‑LB
Transcription factor 7–like 2 194‑LB, 205‑LB
Transcriptional regulation for adipogenesis 230‑LB
Translational research 180‑LB
Transplant 185‑LB
Trial net 187‑LB
LB87
TRPA1 agonists 112‑LB
Type 1 diabetes 48‑LB, 50‑LB, 171‑LB, 188‑LB,
190‑LB
Type 2 diabetes 119‑LB, 176‑LB, 186‑LB, 195‑LB,
207‑LB
UCP1 232‑LB
Ultra-rapid insulin 92‑LB
Uncontrolled diabetes 135‑LB
Uncoupling 287‑LB
Upper respiratory tract infections 94‑LB
Urinary C-peptide 189‑LB
User’s perspectives 66‑LB
Vascular endothelial cells 266‑LB
Vascular smooth muscle cells 12‑LB
Vascular tone 21‑LB
Vildagliptin 123‑LB
Visceral adipose tissue 283‑LB
Visceral fat 104‑LB
Waist to hip ratio 204‑LB
Weight loss 173‑LB
Within-visit blood pressure variability 14‑LB
Zinc transport in beta cells 335-LB
SUBJECT INDEX
Ribosylation 295‑LB
RNA-binding proteins 255‑LB
RPE barrier 36‑LB
Saroglitazar 126‑LB
Saxagliptin 133‑LB
Self-monitoring of blood glucose 71‑LB, 139‑LB
Self-reported outcomes 63‑LB
Sensor augmented pump therapy 80‑LB
Serotonin 333‑LB
Severe hypoglycemia 2‑LB
Sex hormone-binding globulin 159‑LB
Sexual dysfunction 57‑LB
SGLT-2 Inhibitor 39‑LB, 118‑LB, 130‑LB
SGLT-3 21‑LB
SHARE 5‑LB
Sitagliptin 13‑LB
Skeletal muscle 269‑LB
Skeletal muscle proteome 311‑LB
Skin xerosis 44‑LB
Sleep 65‑LB
Sleeve gastrectomy 277‑LB
Small fiber neuropathy 32‑LB
Sorcs 248‑LB
Spleen attenuation 305‑LB
ABSTRACT Author Index
ABSTRACT AUTHOR INDEX
The number following the name refers to the abstract number, not the page number. A number in bold beside an author’s name indicates the
presenting author.
Abderrahmani, Amar 304‑LB
Abdi, Reza 210‑LB, 219‑LB
Abdul-Ghani, Muhammad 195‑LB
Abel, E. Dale 244‑LB
Abraham, Jenny 315‑LB
Abulizi, Abudukadier 113‑LB
Abumrad, Nada 250‑LB
Accili, Domenico 327‑LB
Adachi, Yusuke 151‑LB
Adams Huet, Beverley 83‑LB
Adler, Sharon G. 114‑LB
Adrion, Christine 13‑LB
Agarwal, Ayush K. 90‑LB
Agrawal, Prabhat K. 90‑LB
Ahmad, Shafqat 301‑LB
Ahn, Ki-Yong 54‑LB, 55‑LB
Aikawa, Masanori 270‑LB, 295‑LB
Ajena, Aboajela 16‑LB
Akinbosoye, Osayi 49‑LB
Akiyama, Haruhiko 324‑LB
Akkari, P. Anthony 197‑LB
Akolkar, Beena 149‑LB
Al Dhuhouri, Jamila S. 41‑LB, 42‑LB
Al Hammadi, Fatema H. 41‑LB, 42‑LB
Al Nuaimi, Asma A. 41‑LB, 42‑LB
Al Shaikh, Sarah 41‑LB, 42‑LB
Alaminos, Miguel A. 310‑LB
Albu, Jeanine 138‑LB
Alcain-Martinez, Guillermo 310‑LB
Ali, Mohammed K. 180‑LB
Ali, Nahed 47‑LB
Ali, Nasiri 113‑LB
Alkanani, Aimon 217‑LB
Alkarni, Meyad A. 211‑LB
Alkhaddo, Jamil B. 93‑LB
Alkhalidy, Hana 296‑LB
Alkorta-Aranburu, Gorka 192‑LB
Almaca, Joana 333‑LB
Almeda-Valdes, Paloma 45‑LB
Alquier, Thierry 330‑LB
Al-Trad, Bahaa 19‑LB
Álvarez-Escolá, Carmen 264‑LB
Alzaid, Aus 63‑LB
Amblee, Ambika 116‑LB
Amer, Ahmed 122‑LB
Ammar, Hala 16‑LB
Andersen, Emilie S. 132‑LB
Anderson, Rozalyn M. 252‑LB
Andreasen, Camilla 132‑LB
Andrew, Toby 201‑LB, 202‑LB, 203‑LB
Angueira, Anthony R. 323‑LB
Anil, Tharappel M. 120‑LB
Anjana, Ranjit M. 175‑LB, 180‑LB
Annabi, Firas A. 47‑LB
Anton, Stephen D. 173‑LB
Antosik, Karolina 191‑LB
Anup, Mammen O. 120‑LB
Apovian, Caroline M. 299‑LB
Araque, Katherine 316‑LB
Araujo, Renata 62‑LB
Ardehali, Hossein 255‑LB
Ardissone, Alexandria N. 149‑LB
Arias, Edward B. 245‑LB
Armstrong, Debra A. 89‑LB
Arndt, Kelly 192‑LB
Aroda, Vanita R. 17‑LB, 307‑LB
Aronson, Ronnie 107‑LB
Arous, Caroline 341‑LB
Arslan, Banu 154‑LB
Arthur, John 24‑LB
Arumugam, Kokila 175‑LB
Arya, Rector 195‑LB
Aryal, Pratik 243‑LB
Ashankyty, Ibraheem 19‑LB
Asimakopoulou, Andriana 147‑LB
Assaad-Khalil, Samir H. 47‑LB
Atalay, Nesil 154‑LB
Atkins, Ashley 50‑LB
Atkinson, Mark A. 149‑LB, 192‑LB
Austen, Matthias 326‑LB
Ayala, Iriscilla 205‑LB
Ayala, Jennifer E. 278‑LB
Ayala, Julio E. 278‑LB
Azzi, Jamil 219‑LB
Bach, Leon A. 66‑LB
Bae, Jae-Hoon 256‑LB
Bae, Jin-Sik 297‑LB
Bae, Kwi-Hyun 257‑LB
Bae, Su Ah 3‑LB
Ba-Essa, Ebtesam M. 47‑LB
Bagger, Jonatan I. 132‑LB
Bahceci, Mitat 154‑LB
Bahijri, Suhad M. 47‑LB
Bahmanyar, Shahram 169‑LB
Bahn, Gideon 1‑LB
Bai, Ramya 175‑LB
Baidal, David A. 189‑LB
Baik, Sei Hyun 170‑LB
Bailey, Kathleen A. 194‑LB
Bajaj, Mandeep 227‑LB
Balk, Ethan M. 96‑LB
Balliro, Courtney 72‑LB
Balo, Andrew 5‑LB
Baltaro, Richard J. 78‑LB
Banks, Michaela 144‑LB
Bañuls, Celia 172‑LB
Barber, Thomas M. 315‑LB
Baron, Michelle A. 135‑LB
Barquiel, Beatriz 188‑LB
Barrett-Connor, Elizabeth L. 17‑LB
Barroso, Inês 301‑LB
Barta, William 52‑LB
Bartolomucci, Alessandro 274‑LB
Bassaganya-Riera, Josep 69‑LB
Batra, Manav 130‑LB
Bauman, Viviana 276‑LB
Bayeva, Marina 255‑LB
Bays, Harold 307‑LB
Beaucamps, Cédric 304‑LB
Beauregard, Natalie 150‑LB
Beck, Andrew 206‑LB
Becker, Alexander 13‑LB
Beckman, Kenneth 207‑LB
Bee, Yong Mong 220‑LB
Beeravolu, Swathi 3‑LB
Belfort De Aguiar, Renata 249‑LB
Bell, Graeme I. 194‑LB
Bell, Ruth 153‑LB
LB88
Below, Jennifer E. 199‑LB
Belton, Anne 63‑LB
Beltran, Yobana 51‑LB
Benjamin, Tonya R. 311‑LB
Benson, Tyler W. 294‑LB
Benware, Sheila 76‑LB
Bergenstal, Richard M. 79‑LB
Berger, Zack 115‑LB
Bergeron, Valerie 330‑LB
Bergman, Richard N. 254‑LB
Bertinetti, Daniela 332‑LB
Betteridge, John 111‑LB
Beula, Sara 41‑LB, 42‑LB
Bhad, Prafulla 122‑LB
Bhakoo, Kishore Kumar 31‑LB, 163‑LB
Bhansali, Anil 110‑LB
Bhat, Dattatreya 182‑LB
Bhatt, Deepak L. 15‑LB
Bhattacharjee, Alpana 329‑LB
Bhattacharyya, Sumit 38‑LB
Bianco, Suzy 104‑LB
Biddinger, Sudha B. 40‑LB
Bihl, Ji C. 16‑LB
Bird, Adrian 325‑LB
Birk, Jesper 59‑LB
Bjørbæk, Christian 288‑LB
Blangero, John 195‑LB
Blankenship, Jennifer M. 53‑LB
Blankfard, Martin 319‑LB
Blaser, Martin J. 149‑LB
Blau, Jenny E. 276‑LB
Boehnke, Michael 206‑LB
Bogdonov, Vladimir 294‑LB
Bohnett, Lucas 5‑LB
Bolen, Shari 115‑LB
Bonner, Caroline 304‑LB
Borecki, Ingrid 204‑LB, 308‑LB
Borowiec, Maciej 191‑LB
Bosco, Domenico 341‑LB
Bose, Namrata 89‑LB
Boss, Anders 94‑LB
Bouchaert, Emanuel 10‑LB
Boulware, David 187‑LB
Bouyakdan, Khalil 330‑LB
Bouzakri, Karim 341‑LB
Brady, Matthew J. 194‑LB
Branigan, Deborah 98‑LB
Brar, Harpreet 330‑LB
Brathwaite, Collin 277‑LB
Braun, Barry 53‑LB
Bray, George 173‑LB, 174‑LB, 198‑LB
Brazg, Ronald 100‑LB
Breen, Matthew 76‑LB
Brehm, Michael A. 298‑LB
Brehm, Tyler J. 242‑LB
Brenner, Christoph 13‑LB
Breton, Marc D. 99‑LB
Briddell, Robert 219‑LB
Briley, Annette L. 153‑LB
Brismar, Kerstin 216‑LB
Brito-Sanfiel, Miguel 95‑LB
Brittain, Julia 294‑LB
Brodsky, Michael R. 323‑LB
Broedl, Uli 118‑LB,
Charles, Rene 184‑LB
Chatterjee, Tapan K. 294‑LB
Chattopadhyay, Munmun 28‑LB
Chaudhuri, Ajay 130‑LB
Chaudhuri, Rima 239‑LB
Chen, Chi 61‑LB, 161‑LB, 309‑LB
Chen, Hong-Chi 12‑LB
Chen, Huntga 133‑LB
Chen, Lei 273‑LB
Chen, Liwei 156‑LB
Chen, Lulu 8‑LB
Chen, Yanfang 16‑LB
Chen, Yi 61‑LB, 161‑LB, 309‑LB
Chen, Yidong 205‑LB
Chen, Yimei 159‑LB
Chen, Yingchao 61‑LB, 161‑LB, 309‑LB
Cheng Lee Ping, Peter 31‑LB
Cheng, Xiaodong 332‑LB
Cheong, Ye-Hwang 280‑LB
Chepurny, Oleg G. 112‑LB, 332‑LB
Chernausek, Steven 155-LB,157‑LB
Cherñavvsky, Daniel 99‑LB
Chevalier, Soazig 95‑LB
Chhabra, Mohinish 134‑LB
Chin, Alex J. 133‑LB
Chinchwadkar, Manoj 183‑LB
Chines, Peter 206‑LB
Chisholm, Don J. 239‑LB
Cho, Yoon Hi 237‑LB
Cho, Youngjin 291‑LB
Chodavarapu, Praneeta 158‑LB
Choe, Gina 316‑LB
Choi, Dong Seop 85-LB,170‑LB
Choi, In Young 105‑LB, 303‑LB
Choi, Kyung Mook 170‑LB
Choi, Seul Min 280‑LB
Choi, Siak Leng 88‑LB, 89‑LB
Choi, Soomin 105‑LB
Chorev, Michael 160‑LB
Christensen, Mette M. 128‑LB
Christensen, Mikkel 279‑LB
Christiansen, Claus 314‑LB
Christie, Michael R. 213‑LB
Christofori, Gerhard 341‑LB
Christopher, Michael J. 239‑LB
Christopher, Solomon 169‑LB
Chuck, Leonard 131‑LB
Ciaraldi, Theodore P. 89‑LB, 269‑LB
Clargo, Alison 108‑LB
Claudius, Birgitte 307‑LB
Cobos-Bravo, Juan F. 306‑LB
Cochrane, Katie 150‑LB
Cognard, Emmanuelle 331‑LB
Cohen, Neale 53‑LB
Cohen, Ronald 194‑LB
Coletta, Dawn K. 311‑LB
Colin, Laurence 122‑LB
Collins, Francis S. 206‑LB, 208‑LB
Collins, Stephen J. 291‑LB
Colman, Peter 66‑LB
Colman, Ricki J. 252‑LB
Comstock, Dawn 171‑LB
Comte-Perret, Sophie 317‑LB
Condon, John 98‑LB
Conley, John 76‑LB
Consani, Cristina 168‑LB
Constable, R.T. 249‑LB
Conway, Baqiyyah 24‑LB
Cooper, Julian 69‑LB
Cooper, Marcus 298‑LB
Corkey, Barbara E. 337‑LB
LB89
Corkill, Holly 291‑LB
Corvera, Silvia 298‑LB
Costacou, Tina 24‑LB
Coster, Adelle C. 239‑LB
Covington-Kolb, Sarah 156‑LB
Cox, Nancy J. 199‑LB
Craig, Jagriti 131‑LB
Craig, Maria 237‑LB
Crandall, Jill 17‑LB
Croker, Helen 153‑LB
Cromack, Douglas T. 195‑LB
Crowe, Matthew J. 294‑LB
Cudejko, Céline 10‑LB
Cuezva, Jose M. 269‑LB
Cui, Xin 260‑LB
Cunnick, Jess M. 291‑LB
Cupples, L. Adrienne 204‑LB, 308‑LB
Curie, Justin 171‑LB
Curran, Joanne E. 195‑LB
Cutarelli, Alessandro 274‑LB
Dabelea, Dana 17‑LB, 171‑LB
Dabra, Shakun 134‑LB
Dagogo-Jack, Samuel 15‑LB
Dai, Feihan F. 329‑LB
Dai, Hongji 167‑LB
Dandona, Paresh 130‑LB
Dangott, Bryan J. 78‑LB
Dasari, Paul S. 143‑LB
Davenport, Bennett J. 342‑LB
Davidson, Jaime A. 139‑LB
Davies, Melanie 307‑LB
Davis, Lori 122‑LB
Davis, Timothy M. 162‑LB
Davis, Wendy A. 162‑LB
Davis-Ajami, Mary L. 26‑LB
Davis-Richardson, Austin G. 149‑LB
Day, Samantha E. 311‑LB
De Filippis, Elena A. 311‑LB
De Souza, Errol 2‑LB, 92‑LB
de Toro-Martín, Juan 264‑LB
De Vito, Katerina M. 177‑LB
Deacon, Carolyn 132‑LB
Deeg, Mark A. 197‑LB
Deeney, Jude T. 337‑LB
DeFronzo, Ralph A. 195‑LB
Dehennis, Andrew D. 73‑LB
DeJesus, Adam 255‑LB
Del Gaudio, Daniela 192‑LB
Del Prato, Stefano 105‑LB
Delalleau, Nathalie 304‑LB
Della Bartola, Luca 168‑LB
Delpire, Eric 288‑LB
DeMarco, Vincent 286‑LB
Demirpence, Mustafa 154‑LB
Demirpence, Nur 154‑LB
Dempsey, Paddy C. 53‑LB
D’Eon, Stephanie 57‑LB
DeSalvo, Daniel J. 99‑LB
Dibner, Charna 328‑LB
DiMeglio, Linda A. 145‑LB, 187‑LB
Ding, Eric L. 177‑LB
Dion, Stacy 319‑LB
Distelmaier, Klaus 271‑LB
Divoux, Adeline 318‑LB
do Bem, Daniela A. 11‑LB
Dobkin, Julie 157‑LB
Dolin, Paul 169‑LB
Donaghue, Kim C. 237‑LB
Donaldson, Julie 319‑LB
Dong, Ying 289‑LB
Donnelly, Conor Brian 210‑LB
ABSTRACT AUTHOR INDEX
Brosen, Kim 128‑LB
Brosius III, Frank C. 114‑LB
Brosnan, Julia 335‑LB
Brown, Jacob D. 278‑LB
Brown, Rebecca J. 40‑LB
Browne, Jessica L. 67‑LB
Bruckbauer, Antje 260‑LB
Brüning, Jens C. 233‑LB
Bryan, Joseph 320‑LB
Buckingham, Bruce A. 99‑LB
Budoff, Matthew 17‑LB
Budry, Lionel 330‑LB
Burak, Mehmet Furkan 108‑LB
Buring, Julie E. 176‑LB, 177‑LB
Burke, Paivi M. 89‑LB
Burmeister, Melissa A. 278‑LB
Burns, Cheryl 3‑LB
Buzzetti, Raffaella 95‑LB
Cai, Weikang 266‑LB
Caiazzo, Robert 304‑LB
Caicedo, Alejandro 333‑LB
Callan, Judith A. 68‑LB
Calle, Roberto A. 253‑LB
Caloyeras, John 140‑LB
Campa, David 141‑LB
Campbell, Jonathan E. 330‑LB
Campbell, Latoya E. 311‑LB
Camporez, Joao-Paulo G. 263‑LB
Campos, Hannia 177‑LB
Campos, Maribel 14‑LB
Canepa, Ronald J. 149‑LB
Cang, Zhen 61‑LB, 161‑LB, 309‑LB
Canney, Lori 2‑LB, 92‑LB
Cao, Qiang 260‑LB
Capehorn, Matthew 63‑LB
Cappell, Katherine 164‑LB
Capuano, George 131‑LB
Carbo, Adria 69‑LB
Cardamone, Maria D. 240‑LB
Cárdenas, Jose L. 30‑LB
Cardillo, Tracy E. 114‑LB
Cargill, Robert S. 76‑LB
Carless, Melanie 195‑LB
Carley, David W. 65‑LB
Carls, Ginger S. 135‑LB, 142‑LB
Carmody, David 192‑LB
Caron, Nicole 288‑LB
Carrington, Paul 272‑LB
Cartee, Greg 245‑LB, 247‑LB
Carter, Leslie 269‑LB
Casellini, Carolina M. 32‑LB
Castle, Jessica R. 98‑LB
Catalano, Patrick M. 152‑LB, 158‑LB
Cavalcante, Lilian L. 123‑LB
Cederquist, Carly T. 240‑LB
Cefalu, William T. 166‑LB
Cero, Cheryl 274‑LB
Cha, Dae Ryong 127‑LB
Cha, Ji-Young 256‑LB, 297‑LB
Chabtini, Lola 219‑LB
Chacra, Antonio 111‑LB
Chae, Yu Na 280‑LB
Chakrabarti, Amitava 110‑LB
Chamberlain, James J. 74‑LB, 75‑LB
Champagne, Catherine M. 173‑LB
Chan, Lawrence C. 227‑LB
Chan, You-Ping 84‑LB
Chane-Woon-Ming, Béatrice 325‑LB
Chang, Evan 129‑LB
Chang, Hsiang-Chun 255‑LB
Chapel, Sunny 86‑LB
ABSTRACT AUTHOR INDEX
Dopita, Dana 74‑LB, 75‑LB
Dorchy, Harry R. 147‑LB
Down, Susan 63‑LB
Doyle, Carl 108‑LB
Dragsbæk, Katrine 314‑LB
Drucker, Daniel J. 330‑LB
Duffin, Kevin L. 114‑LB
Duggirala, Ravindranath 195‑LB
Dumenci, Levent 64‑LB
Dunstan, David 53‑LB
Duris, Christine 21‑LB
Dushay, Jody 317‑LB
Dutta, Pinaki 110‑LB
Dutta, Sucharita 262‑LB
Duvvuru, Suman 197‑LB
Dyer, Thomas D. 195‑LB
Dziadowicz, Helena M. 252‑LB
Eberhard, Daniel 321‑LB
Eckel, Juergen 246‑LB
Edelman, Steven 63‑LB
Edwards, Josh 32‑LB
Edwards, Todd L. 308‑LB
Efstratiou, Efthimia 48‑LB
Eglinger, Jan 321‑LB
Eguchi, Jun 258‑LB, 285‑LB
Ehrich, Marion 69‑LB
Eichner, Norbert 325‑LB
Ekhlaspour, Laya 72‑LB
El Khatib, Moustafa 322‑LB
El Ouaamari, Abdelfattah 261‑LB
El Youssef, Joseph 98‑LB
Eliasson, Lena 325‑LB
Elks, Carrie M. 226‑LB
Elsasser, Ulrich 118‑LB
El-Shahawy, Mohamed 125‑LB
Elston Lafata, Jennifer 64‑LB
Erdos, Michael 206‑LB, 208‑LB
Eringa, Etto C. 56‑LB, 60‑LB
Erion, Karel A. 337‑LB
Escrivá-Pons, Fernando 264‑LB
Esko, Tonu 308‑LB
Estall, Jennifer L. 330‑LB
Etwebi, Zienab A. 293‑LB
Evans-Molina, Carmella 145‑LB, 187‑LB
Eze, Ikenna C. 178‑LB, 179‑LB
Fain, Randi 299‑LB
Fall, Caroline 182‑LB, 183‑LB
Fang, Han 224‑LB
Farabi, Sarah S. 65‑LB
Farook, Vidya S. 195‑LB
Federici, Adalberto 44‑LB
Federici, Giovanni 44‑LB
Feferman, Leo 38‑LB
Feltbower, Richard 213‑LB
Feng, Bin 222‑LB
Feng, Yue 251‑LB
Fenske, Rachel 330‑LB
Fenwick, Eva K. 67‑LB
Ferguson-Smith, Anne 151‑LB
Fernández-Millán, Elisa 264‑LB
Ferron, Mathieu 330‑LB
Fiad, Tarek M. 41‑LB, 42‑LB
Figarola, James L. 287‑LB
Fink, Jeffrey C. 26‑LB
Finlin, Brian S. 284‑LB
Fiorina, Paolo 219‑LB
Fischer, Annelie 121‑LB
Fish, Lisa 93‑LB
Fishbane, Steven N. 125‑LB
Fitch, Mark 302‑LB
Fitzgibbons, Timothy 298‑LB
Flannery, Clare A. 316‑LB
Flynn, Angela C. 153‑LB
Fodor, William 219‑LB
Fogelfeld, Leon 116‑LB
Forisch, Michael 137‑LB
Formentini, Laura 269‑LB
Fourcaudot, Marcel 195‑LB
Fowler, Robert 164‑LB
Fox, Caroline S. 204‑LB
Frank, Claudio 274‑LB
Franks, Paul W. 301‑LB
Franz, Wolfgang-Michael 13‑LB
Fraser, Ian 23‑LB
Frayling, Timothy M. 308‑LB
Frenkel, Dan 218‑LB
Friedländer, Marc 325‑LB
Frois, Christian 135‑LB, 142‑LB
Frokiaer, Jørgen 128‑LB
Fryburg, David A. 253‑LB, 275‑LB
Fu, Alex Z. 164‑LB
Fu, Lizhi 260‑LB
Fu, Yanyun 331‑LB
Fuentes, Blanca 51‑LB
Fukuda, Takuya 212‑LB
Fukui, Michiaki 212‑LB
Fung, Anne 37‑LB
Fusong, Jiang 165‑LB
Gaglia, Jason L. 189‑LB
Galli-Tsinopoulou, Assimina 48‑LB
Gamerman, Victoria 63‑LB
Gandomani, Ben S. 143‑LB
Gandour, Richard 69‑LB
Gang, Xiaokun 229‑LB
Gannon, Maureen A. 323‑LB
Garcia Fuentes, Eduardo 306‑LB, 310‑LB
Garcia, Arturo 71‑LB
Garcia-Arnes, Juan 306‑LB, 310‑LB
Garcia-Escobar, Eva 306‑LB
Garcia-Sanchez, Ricardo 133‑LB
Garcia-Serrano, Sara 306‑LB, 310‑LB
Garg, Satish K. 87‑LB, 217‑LB
Garhyan, Parag 88‑LB, 89‑LB, 106‑LB
Garlish, Rachel 108‑LB
Gaziano, J.M. 176‑LB
Gebauer, Mathias 275‑LB
Gee, Kyuhoon 105‑LB, 303‑LB
Genieser, Hans-G 332‑LB
Genovese, Maria I. 62‑LB
Genter, Pauline 141‑LB
Gentile, Sandro 107‑LB
Gerbase, Margaret 178‑LB, 179‑LB
Geyer, Susan 145‑LB
Ghanian, Sheila 252‑LB
Ghanim, Husam 130‑LB
Ghannam, Ameen 164‑LB
Ghorbani, Tahereh 317‑LB
Ghosh, Pamela 160‑LB
Ghosh, Sujoy 126‑LB
Giacaglia, Luciano 62‑LB
Giampietro, Ottavio 168‑LB
Gilgen, Emily 74‑LB, 75‑LB
Giovenale, Sharon 124‑LB
Glicklich, Alan 299‑LB
Glynn, Robert J. 176‑LB
Gmyr, Valéry 304‑LB
Gnys, Piotr 191‑LB
Godfrey, Keith M. 153‑LB
Goldberg, Ronald 17‑LB
Gomez, Ana Maria 80‑LB
Gomez-Perez, Francisco J. 45‑LB
Gonçalves, Gabriel H. 288‑LB
LB90
Gonçalves, Nadmy A. 11‑LB
Gonçalves, Rita de Cássia R. 11‑LB
Gonzalez, Noemi 188‑LB
González-Ortiz, Manuel 131‑LB
Gonzalo, Montserrat 306‑LB, 310‑LB
Gopala, Aralakuppe S. 120‑LB
Gordon, Tom 29‑LB
Gorgel, Ahmet 154‑LB
Göring, Harald H. 195‑LB
Gormsen, Lars C. 128‑LB
Gottlieb, Peter A. 217‑LB
Gottlieb, Rebecca 100‑LB
Gowtham, Raj 120‑LB
Grabmaier, Ulrich 13‑LB
Grady, Mike 70‑LB
Graff, Emily C. 224‑LB
Graff, Marielisa 308‑LB
Graff, Misa 204‑LB
Grarup, Niels 204‑LB
Greeley, Siri Atma W. 192‑LB
Greenbaum, Carla J. 187‑LB
Greenfield, Jerry R. 239‑LB
Greenway, Frank 300‑LB
Greulich, Sabrina 246‑LB
Griffith, Julie 50‑LB
Grohmann-Izay, Barbara J. 137‑LB
Groh-Wargo, Sharon 158‑LB
Grosman, Benyamin 66‑LB, 100‑LB
Gross, Myron 207‑LB
Guan, Hong-Ping 272‑LB
Guan, Meiping 18‑LB
Gudiksen, Anders 59‑LB
Guerci, Bruno 107‑LB
Guertin, David A. 236‑LB
Guhl, Anna 326‑LB
Guimaraes, Sergio B. 123‑LB
Gune, Shamika 37‑LB
Guo, Hui 61‑LB, 161‑LB, 309‑LB
Guo, Xiaohui 283‑LB
Gutierrez, Absalon 227‑LB
Gutierrez-Repiso, Carolina 306‑LB, 310‑LB
Ha, Kyoung Soo 85‑LB
Haas, Joseph V. 114‑LB
Haas, Mary 40‑LB
Hackett, Geoffrey I. 7‑LB, 9‑LB
Hadjadj, Samy 119‑LB
Hage, Camilla 216‑LB
Haghiac, Maricela 152‑LB
Hagopian, William A. 149‑LB
Hailu, Hanna 108‑LB
Halder, Louise 315‑LB
Hall, Christopher E. 277‑LB
Hall, Keneth 277‑LB
Hallmans, Göran 301‑LB
Halperin, Jose 160‑LB
Han, Bing 61‑LB, 161‑LB, 309‑LB
Han, Byoung Geun 127‑LB
Han, Jing 33‑LB, 34‑LB
Han, Kyung Ah 305‑LB
Han, Oak Pil 105‑LB, 303‑LB
Han, Sang Youb 127‑LB
Han, Weiping 331‑LB
Han, Xinping 112‑LB
Hanas, Ragnar 148‑LB
Hanefeld, Markolf 107‑LB
Hanis, Craig L. 199‑LB
Hanna, Paul 21‑LB
Hannpu, Sarah 10‑LB
Hanseman, Dennis 173‑LB
Hansen, Lærke S. 279‑LB
Hansen, Lars 133‑LB
Hooven, Jayde T. 291‑LB
Horne, David 287‑LB
Horsburgh, Jodie C. 66‑LB
Horton, Edward S. 17‑LB
Hoshina, Sari 190‑LB
Hota, Debasish 110‑LB
Hotamisligil, Gökhan S. 108‑LB
Hoti, Fabian 169‑LB
Hou, Liqiong 238‑LB
Houweling, Leanne 169‑LB
Howard, Andrew 251‑LB
Howells, Louise 108‑LB
Hsia, Daniel S. 166‑LB
Hsiao, Jong-Kai 12‑LB
Hsu, Chi-Yuan 207‑LB
Hu He, Kaihui 326‑LB
Hu, Frank B. 167‑LB, 175‑LB
Hu, Ling 61‑LB
Hu, Shirley L. 195‑LB
Hu, Yanjin 313‑LB
Hu, Ying Ying 192‑LB
Huang, Tao 174‑LB, 198‑LB
Huang, Tian Lian 232‑LB
Huang, Zhe 223‑LB, 282‑LB
Hughes, Kristen 100‑LB
Hughes, William E. 331‑LB
Huh, Yeamin 86‑LB
Hutchens, Troy 340‑LB
Hutfless, Susan 115‑LB
Huyghe, Jeroen 206‑LB
Hwang, Janice J. 249‑LB
Iacobellis, Gianluca 104‑LB
Ibrahim, Mahmoud 47‑LB
Ikeda, Yasuhiro 322‑LB
Im, Hae Kyung 199‑LB
Im, Kyung Ah 15‑LB
Im, Seung-Soon 256‑LB
Imai, Yumi 262‑LB
Imboden, Medea 178‑LB, 179‑LB
Imig, John D. 21‑LB
Innes, Karen 24‑LB
Inoue, Noriyuki 295‑LB
Inouye, Karen 108‑LB
Ioacara, Sorin 73‑LB
Ipp, Eli 141‑LB
Iqbal, Nayyar 133‑LB
Irving, Brian 271‑LB
Itescu, Silviu 23‑LB
Iwasaki, Yorihiro 82‑LB
Iwata, Hiroshi 295‑LB
Iyoha, Emannuel 115‑LB
Jackson, Anne 206‑LB
Jackson, Jeffrey A. 197‑LB
Jackson, Michael 29‑LB
Jacober, Scott J. 89‑LB
Jacobs, Peter G. 98‑LB
Jacobus Ambuludi, Egon J. 322‑LB
Jaffar, Amina 3‑LB
Jagannath, Madanahalli R. 120‑LB
Jain, Deepak 321‑LB, 335‑LB
Jaiswal, Ashok D. 126‑LB
Jakobsen, Steen 128‑LB
Jakoby, Michael G. 3‑LB
James, David E. 239‑LB
Janes, Jonathan M. 114‑LB
Janka-Zires, Marcela 45‑LB
Januszewski, Andrzej S. 237‑LB
Jasper, Susan 111‑LB
Jastroch, Martin 325‑LB
Jean-Baptiste, Eddy 184‑LB
Jelaska, Ante 119‑LB
LB91
Jenkins, Alicia 6‑LB, 237‑LB
Jenkinson, Christopher P. 195‑LB
Jensen, Jonas B. 128‑LB
Jensen, Michael D. 61‑LB
Jeon, Jae-Han 257‑LB
Jeon, Justin Y. 54‑LB, 55‑LB
Jeong, Kyung Hwan 127‑LB
Jessen, Niels 128‑LB
Ji, Linong 87‑LB
Jia, Weiping 165‑LB
Jiang, Hui 206‑LB
Jiang, Jenny 49‑LB
Jianjun, Liu 207‑LB
Jiao, Ping 222‑LB
Jin, Shi 289‑LB
Jo, Young-II 127‑LB
Joglekar, Charudatta 182‑LB, 183‑LB
Johnson, Jennal L. 197‑LB
Johnson, Matthew L. 271‑LB
Johnson, William D. 166‑LB
Johnston, Stephen 164‑LB
Jones, Dean P. 241‑LB
Jose, Aimee 81‑LB
Joshi, Shashank R. 126‑LB
Joshi, Suyog 183‑LB
Joshipura, Kaumudi J. 14‑LB
Jouvet, Nathalie 330‑LB
Juarez-Comboni, Sonia C. 45‑LB
Judd, Robert L. 224‑LB
Jung, II-Hoon 280‑LB
Jung, Yun-Seung 297‑LB
Jurczak, Michael J. 113‑LB, 263‑LB
Justice, Anne E. 204‑LB, 308‑LB
Kabadi, Udaya M. 91‑LB
Kabra, Uma D. 325‑LB
Kadener, Sebastian 325‑LB
Kady, Jamie 298‑LB
Kahn, Barbara B. 243‑LB
Kahn, C. Ronald 232‑LB, 266‑LB
Kahn, Jonathan 194‑LB
Kalsekar, Iftekhar 164‑LB
Kamenov, Zdravko 214‑LB
Kandror, Konstantin V. 231‑LB
Kane, Penelope 146‑LB
Kaneko, Shizuka 82‑LB
Kaneto, Hideaki 324‑LB, 334‑LB
Kang, Dong-Woo 54‑LB
Kang, Jahoon 86‑LB, 105‑LB, 303‑LB
Kang, Kyung Koo 280‑LB
Kang, Shin-Wook 127‑LB
Karaderi, Tugce 204‑LB
Karaliota, Sevasti 268‑LB
Karalis, Katia 268‑LB
Karsdal, Morten 314‑LB
Kasid, Natasha 317‑LB
Kattah, William 30‑LB
Katz, Laurence B. 70‑LB
Kaufholz, Melanie 332‑LB
Kaufman, Francine 100‑LB
Kawaguchi, Yasushi 190‑LB
Kawaguchi, Yoshiya 324‑LB
Kawamoto, Manabu 190‑LB
Kazakos, Kyriakos 48‑LB
Ke, Bilun 259‑LB
Keady, Joyce 50‑LB
Keçik, Onur 288‑LB
Keenan, Hillary A. 57‑LB
Kefaloyianni, Eirini 219‑LB
Keith-Hynes, Patrick 99‑LB
Kelkar, Rohini 183‑LB
Kelley, David E. 273‑LB
ABSTRACT AUTHOR INDEX
Hansen, Mads Bau 59‑LB
Hansen, Troels K. 216‑LB
Hansraj, Patil A. 120‑LB
Hantel, Stefan 118‑LB
Hao, Gaimei 33‑LB, 34‑LB
Hao, Pindan 138‑LB
Hara, Takuya 295‑LB
Hardy, Thomas A. 106‑LB
Häring, Hans-Ulrich 327‑LB
Harris, Stuart 122‑LB
Harrison, Lindsay 83‑LB
Harsha, Krishna Reddy 120‑LB
Hartig, Sean M. 227‑LB
Hartmann, Bolette 132‑LB, 279‑LB
Hartmann, Thorsten 246‑LB
Hastings, Stephanie M. 57‑LB
Hauguel-de Mouzon, Sylvie 152‑LB
Hausser, Jean 325‑LB
Haw, J.S. 241‑LB
Hayden, Melvin 286‑LB
Hayek, Salim S. 25‑LB
Hayes, Louise 153‑LB
Hazra, Daya K. 90‑LB
He, Jie 33‑LB, 34‑LB
He, Ling 129‑LB
He, Qin 222‑LB
He, Yan Ling 122‑LB
Heard-Costa, Nancy L. 204‑LB
Heberlein, Emily 156‑LB
Heier, Jeffrey S. 37‑LB
Heinemann, Lutz 94‑LB
Heintjes, Edith M. 169‑LB
Heise, Tim 121‑LB
Heizer, Patrick 69‑LB
Hejna, Jeanne 130‑LB
Heller, Simon 107‑LB
Hellerstein, Marc 302‑LB
Henao, Diana 80‑LB
Hendrieckx, Christel 66‑LB
Henry, Robert R. 89‑LB, 269‑LB
Herberg, Friedrich W. 332‑LB
Herman, William H. 47‑LB
Hernández, Antonio 172‑LB
Herranz, Lucrecia 188‑LB
Herrlich, Andreas 219‑LB
Highland, Heather M. 204‑LB, 308‑LB
Hillard, Mallory 72‑LB
Hillman, Natalia 188‑LB
Hingst, Janne R. 59‑LB
HIrate, Mitsuru 39‑LB
Hirschhorn, Joel N. 308‑LB
Hirshberg, Boaz 15‑LB
Hissa, Marcelo R. 123‑LB
Hissa, Miguel N. 123‑LB
Hmaguchi, Masahide 212‑LB
Hoch, Emily 140‑LB
Hoevenaars, Femke M. 56‑LB
Hoffmann, Ellen 13‑LB
Hoffmann-Petersen, Ingeborg T. 216‑LB
Hoidal, Mallary 270‑LB, 295‑LB
Holland, William 265‑LB
Holmes-Truscott, Elizabeth 67‑LB
Holst, Jens Juul 132‑LB, 279‑LB
Holt, Charlotte B. 216‑LB
Holz, George G. 112‑LB, 332‑LB
Homann, Dirk 342‑LB
Hompesch, Marcus 2‑LB, 92‑LB, 105‑LB, 303‑LB
Hong, Biling 175‑LB
Hong, Suntaek 297‑LB
Honig, Lee B. 342‑LB
Hontecillas, Raquel 69‑LB
ABSTRACT AUTHOR INDEX
Kelly, Ronan P. 106‑LB
Kemnitz, Joseph W. 252‑LB
Kemppainen, Kaisa M. 149‑LB
Kennedy, Christopher 341‑LB
Kern, Philip A. 284‑LB
Kernan, Kelly 336‑LB
Kerr, Peter G. 23‑LB
Kerr-Conte, Julie 221‑LB, 304‑LB
Kesireddy, Veena 3‑LB
Khai Koon, Heng 207‑LB
Khazaezadeh, Nina 153‑LB
Khedkar, Aditya 325‑LB
Khowaja, Ameer 93‑LB
Kibbey, Richard G. 342‑LB
Kiens, Bente 59‑LB
Kil, Siyoen 86‑LB, 105‑LB, 303‑LB
Kim, Bong-Jo 200‑LB
Kim, Dong-II 54‑LB, 55‑LB
Kim, Dong-Wook 257‑LB
Kim, Doo Man 85‑LB
Kim, In Joo 85‑LB
Kim, Jae Bum 228‑LB
Kim, Jihye 339‑LB
Kim, Ji-Young 54‑LB
Kim, Jongoh 227‑LB
Kim, Joon Young 311‑LB
Kim, Jung Seok 339‑LB
Kim, Mi-Kyung 280‑LB
Kim, Nam-Ho 127‑LB
Kim, Nam-Kyu 54‑LB, 55‑LB
Kim, Nan Hee 170‑LB
Kim, Pankyung 303‑LB
Kim, Sin Gon 85‑LB, 170‑LB
Kim, Soohyun Park 235‑LB
Kim, Sung Gyun 127‑LB
Kim, Sung-Woo 257‑LB
Kim, Tae Hyoung 280‑LB
Kim, Tae Joon 170‑LB
Kim, Wook 339‑LB
Kim, Yong-Seong 85‑LB
Kim, Young Jin 200‑LB
Kim, Young-Bum 288‑LB
Kim, Yun Kyoung 200‑LB
Kimple, Michelle E. 330‑LB
King, George L. 57‑LB
King, Timothy 262‑LB
Kingwell, Bronwyn A. 53‑LB
Kircher, Robert 101‑LB
Klisch, Theresa 326‑LB
Knadler, Mary P. 88‑LB, 89‑LB
Knoblauch, Nicholas W. 199‑LB
Knop, Filip K. 132‑LB, 279‑LB
Knutsen, Chad 76‑LB
Ko, Yi-An 25‑LB
Kobiernicki, Frances 192‑LB
Kodella, Elisavet 268‑LB
Kodella, Kostantia 268‑LB
Koistenen, Heikki 206‑LB
Kokovay, Erzsebet 205‑LB
Kolar, Matthew J. 243‑LB
Kondegowda, Nagesha G. 342‑LB
Konishi, Masahiro 266‑LB
Konopka, Adam R. 271‑LB
Koratkar, Revati 207‑LB
Korhonen, Pasi 169‑LB
Kornfeind, Ellyn 32‑LB
Koroscil, Thomas M. 16‑LB
Krasner, Alan 2‑LB, 92‑LB
Kraus, Morey 219‑LB
Kretzler, Matthias 114‑LB
Krischer, Jeffrey P. 149‑LB, 187‑LB
Krishnaswamy, Kamala 175‑LB
Kronenberg, Florian 178‑LB, 179‑LB
Ku, Bon Jeong 85‑LB
Kuang, Lin 161‑LB
Kubo, Fumiyo 324‑LB, 334‑LB
Kudva, Yogish C. 322‑LB
Kuhadiya, Nitesh D. 130‑LB
Kuliawat, Regina 338‑LB
Kulkarni, Rohit N. 261‑LB
Kumar, Ashish 178‑LB, 179‑LB
Kumar, Satish 195‑LB
Kumar, Sudhesh 315‑LB
Kumar, Sunil 277‑LB
Kumareswaran, Kavita 66‑LB
Künzli, Nino 178‑LB, 179‑LB
Kurmi, Kiran 322‑LB
Kurtz, Natalie 66‑LB, 100‑LB
Kusmartseva, Irina 192‑LB
Kutoh, Eiji 39‑LB
Kwak, Eunhwa 303‑LB
Kwon, Se Chang 105‑LB, 303‑LB
Kyoong, Andrew 66‑LB
Kyrgios, Ioannis 48‑LB
La Ronde-Richard, Ann-Marie 335‑LB
LaBell, Elizabeth S. 88‑LB
Laca, Jose 51‑LB
Lacadie, Cheryl 249‑LB
Lacombe, Julie 330‑LB
Laffel, Lori M. 50‑LB
Lage, Adrianne 144‑LB
Lagerstedt, Jens 335‑LB
Lakhani, Rohan 315‑LB
Lakka, Timo 206‑LB
Lakshmi, Mudigere N. 120‑LB
Lam, Eric Chen Quin 89‑LB
Lam, Karen Siu-Ling 223‑LB, 282‑LB
Lam, Meghan 250‑LB
Lammert, Eckhard 121‑LB, 321‑LB
Langlais, Paul R. 311‑LB
Lanza, Ian 271‑LB
Lao, Julie 251‑LB, 273‑LB
Larco, Nancy C. 184‑LB
Larco, Philippe 184‑LB
Larrivee, Sandra 166‑LB
Larsen, Peter 146‑LB
Lassance Gomes, Luciana 152‑LB
Lassman, Michael E. 273‑LB
Lau, Raymond G. 277‑LB
Lau, Winston 201‑LB, 202‑LB, 203‑LB
Lautsch, Norman 72‑LB
Lavalle-González, Fernando J. 95‑LB
Lavin, Philip T. 125‑LB
Layden, Brian T. 323‑LB
Le, Yun-Zheng 36‑LB
Leach, Jake 5‑LB
Leber, Alexander 13‑LB
Leber, Stacey 322‑LB
Lee, Douglas S. 253‑LB
Lee, Hong Kyu 305‑LB
Lee, In-Kyu 257‑LB
Lee, Jennifer 243‑LB
Lee, Jimmy Tsz-Hang 223‑LB
Lee, Jisoo 63‑LB
Lee, Junga 55‑LB
Lee, Jung-Hun 297‑LB
Lee, Kwan-Hoo 280‑LB
Lee, Mi Kyung 54‑LB, 55‑LB
Lee, Tsz-Hang 282‑LB
Lee, Woohyung 105‑LB
Leech, Colin 112‑LB, 332‑LB
Lehman, Donna M. 195‑LB, 205‑LB
LB92
Leiter, Lawrence A. 15‑LB
Leng, Jiyan 6‑LB
Leng, Song 313‑LB
Lentucci, Claudia 240‑LB
Leonardi, Anthony 255‑LB
Lerakis, Stamatios 25‑LB
Lernmark, Åke 149‑LB
Lettre, Guillaume 308‑LB
Levenson, Amy E. 40‑LB
Levin, Philip A. 94‑LB
Levy, Brian L. 70‑LB
Li, Bin 61‑LB
Li, Fenfen 260‑LB
Li, Guo Dong 220‑LB
Li, Hui 112‑LB
Li, Ji 6‑LB
Li, Liwu 235‑LB
Li, Nina 251‑LB
Li, Qin 61‑LB, 161‑LB, 309‑LB
Li, Ruifeng 175‑LB
Li, Wangen 159‑LB
Li, Wenjing 288‑LB
Li, Xingwang 208‑LB
Li, Xuhang 289‑LB
Li, Zihao 159‑LB
Liang, Weiqiang 159‑LB
Liao, Yi-Chun 12‑LB
Liao, Yunfei 8‑LB
Lichliter, Jason 23‑LB
Liew, Chong Wee 261‑LB
Lightwood, Dan 108‑LB
Lim, Sai Kiang 220‑LB
Lin, Daniel J. 315‑LB
Lin, Dongping 61‑LB, 161‑LB, 309‑LB
Lin, Su F. 78‑LB
Lin, Yung-Chieh 12‑LB
Lincoff, A.M. 111‑LB
Lindberg, Iris 196‑LB
Linder, Marie 169‑LB
Lindgren, Cecilia M. 204‑LB, 308‑LB
Lingvay, Ildiko 83‑LB
Linnebjerg, Helle 89‑LB
Lious, Daniel 116‑LB
Liu, Ching-Ti 204‑LB
Liu, Dongmin 296‑LB
Liu, Franklin 273‑LB
Liu, Hangsheng 140‑LB
Liu, Jia 313‑LB
Liu, Jiajun 114‑LB
Liu, Quan 6‑LB
Liu, Ying 159‑LB, 329‑LB
Liu, Yuanhang 205‑LB
Liu, Yujia 229‑LB
Lizárraga-Mollinedo, Esther 264‑LB
Lizarzaburu, Juan C. 51‑LB
Lo, K. Sin 308‑LB
Loh, Margaret 66‑LB
Loh, Yik Wen 237‑LB
Lombard, Julian H. 21‑LB
Loos, Ruth J. 204‑LB, 308‑LB
Lopez, Claudia 111‑LB
Lopez-Gutierrez, Joel 45‑LB
Lu, Brian 322‑LB
Lu, Christine 136‑LB
Lu, Meng 61‑LB, 161‑LB, 309‑LB
Lu, Qi 174‑LB
Lu, Yang 141‑LB
Lu, Yingchang 308‑LB
Lu, Yingli 61‑LB, 161‑LB, 309‑LB
Lu, Yongke 204‑LB
Lubree, Himangi 182‑LB
Meissner, Thomas 121‑LB
Meister, Gunter 325‑LB
Melissinos, Michail 48‑LB
Mellbin, Linda G. 216‑LB
Mendivil, Carlos O. 30‑LB
Menegaz, Danusa 333‑LB
Meng, Shu 220‑LB
Meng, Ying 61‑LB, 161‑LB, 309‑LB
Menon, Venu 111‑LB
Menon, Vinod 315‑LB
Merino-Trigo, Ana 95‑LB
Merton, Kate 131‑LB
Meunier, Clemence 330‑LB
Miao, Ji 40‑LB
Michels, Aaron W. 217‑LB
Milani, Massimo 44‑LB
Milaszewski, Kerry 50‑LB
Milhem, Tyler 76‑LB
Min, Ae-Kyung 257‑LB
Min, Jihee 55‑LB
Min, Kyung Wan 305‑LB
Min, So Yun 298‑LB
Minium, Judi 152‑LB
Mintz, James 294‑LB
Mirmira, Raghavendra G. 323‑LB
Misha’l, Aly A. 47‑LB
Mitrovich, Connor 150‑LB
Miura, Junnosuke 190‑LB
Miyashita, Kazuyuki 324‑LB, 334‑LB
Miyatsuka, Takeshi 324‑LB, 334‑LB
Mizuno, Ken 270‑LB, 295‑LB
Mlynarchik, Andrew 295‑LB
Mlynarski, Wojciech 191‑LB
Modi, Devangi 29‑LB
Moerman, Ericka 304‑LB
Mohammad Moradi, Shayan 47‑LB
Mohan, Viswanathan 175‑LB, 180‑LB
Mohanasundaram, Daisy 29‑LB
Mohlke, Karen L. 204‑LB, 206‑LB
Mohseni, Mahshid 104‑LB
Moisidou, Maria 268‑LB
Molina, Judith T. 333‑LB
Mondesir, Debbie 72‑LB
Moon, Sanghoon 200‑LB
Moore, Adrian 108‑LB
Moore, Robert 210‑LB
Mora, Edwin 80‑LB
Moreno-Ruiz, Francisco J. 306‑LB, 310‑LB
Morgan, Diana 213‑LB
Morley, Thomas S. 233‑LB
Morris, Andrew P. 193‑LB
Morris, Heather L. 64‑LB
Morris, Kristin 76‑LB
Morrow, Linda 2‑LB, 92‑LB
Morton-Eggleston, Emma B. 136‑LB
Mosser, Rockann 323‑LB
Mounayar, Marwan 210‑LB, 219‑LB
Mudaliar, Sunder 89‑LB
Mudgett, John 251‑LB
Muise, Eric 273‑LB
Mullapudi, Kamesh 76‑LB
Mullen, Deborah M. 79‑LB
Muniyappa, Ranganath 40‑LB
Munk, Ole L. 128‑LB
Muñoz, Oscar 80‑LB
Munoz-Gomez, Miguel 322‑LB
Munoz-Torres, Francisco 14‑LB
Murakami, Kazutoshi 258‑LB, 285‑LB
Murakami, Kentaro 270‑LB
Murthy, Narasimha 315‑LB
Mynatt, Randall L. 226‑LB
LB93
Na, Ki-Ryang 127‑LB
Nagarajan, Lakshmipriya 175‑LB
Nagel, Friederike 63‑LB
Naik, Sarita 249‑LB
Nair, K. Sreekumaran 271‑LB
Nakamura, Katherine 5‑LB
Nakamura, Naoto 212‑LB
Nakamura, Yumiko 320‑LB
Nakatsuka, Atsuko 258‑LB, 285‑LB
Nam, Minwoo 298‑LB
Narayan, K.M. Venkat 180‑LB
Narisu, Narisu 206‑LB
Nasr, Gamela 47‑LB
Nassar, Wael F. 102‑LB
Nawrocki, Andrea 272‑LB, 273‑LB
Neal, Adam S. 336‑LB
Neale, Helen 108‑LB
Neergaard, Jesper S. 314‑LB
Nelson, Scott M. 153‑LB
Neuman, Joshua C. 330‑LB
Nhan, Trinh 124‑LB
Nicholls, Stephen 111‑LB
Nie, Xiaomin 309‑LB
Nie, Yaohui 222‑LB
Nissen, Steven E. 111‑LB
Niu, Jianmin 159‑LB
Nobrega, Marcelo A. 194‑LB
Noel, Guillaume 84‑LB
Nordén, Kristina 335‑LB
Norman-Burgdolf, Heather L. 267‑LB
North, Kari E. 204‑LB, 308‑LB
North, Paula E. 21‑LB
Norton, Luke 195‑LB
Nowlan, Molly 171‑LB
Nunlee-Bland, Gail 139‑LB
Nunoue, Tomokazu 285‑LB
Obrosova, Irina G. 32‑LB
Odede, Geofrey 108‑LB
Ogawa, Daisuke 258‑LB
Oh, Byung-Chul 256‑LB
Oh, Kook-Hwan 127‑LB
Oh, Kyoung-Jin 230‑LB
Oh, Minsuk 55‑LB
Ohta, Masayuki 270‑LB
Okada, Junichi 20‑LB
Okada, Shuichi 20‑LB
O’Neal, David 237‑LB, 66‑LB
O’Rahilly, Stephen 197‑LB
Orchard, Trevor J. 17‑LB
Ordelheide, Anna-Maria 327‑LB
Orduz, Arturo 30‑LB
O’Reilly, Eilis J. 177‑LB
Oropeza, Daniel 330‑LB
Orr, Gregory 49‑LB
Oruk, Guzide Gonca 154‑LB
Osakai, Aya 20‑LB
Osawa, Mari 190‑LB
Osborne, Timothy 318‑LB
Osborne, William 336‑LB
Osei, Kwame 15‑LB
Osganian, Stavroula 144‑LB
Østergaard, Jakob A. 216‑LB
O-Sullivan, In Sug 261‑LB
Oteng-Ntim, Eugene 153‑LB
Otter, Silke 121‑LB
Otto, Michael 143‑LB
Ouwens, Margriet 246‑LB
Owen, Neville 53‑LB
Pachanski, Michele 272‑LB
Packham, David K. 23‑LB
Palaia, Thomas 277‑LB
ABSTRACT AUTHOR INDEX
Lucas, Anthony 10‑LB
Lulo, James 319‑LB
Lund, Asger 132‑LB
Lundqvist, Kristin 148‑LB
Luo, Jing 296‑LB
Luo, Oscar 208‑LB
Luque-Fernandez, Miguel A. 160‑LB
Lv, Tiantian 33‑LB, 34‑LB
Ly, Trang T. 99‑LB
Lynes, Mattew D. 232‑LB
Lyv, Fuping 18‑LB
Ma, Jian-Xing 155‑LB
Ma, Tony 299‑LB
Ma, Xiaotang 16‑LB
Maarouf, Omar H. 219‑LB
MacDonald, Patrick E. 332‑LB
Machida, Yui 262‑LB
Macias, William L. 114‑LB
MacIsaac, Richard J. 66‑LB
Madiraju, Anila K. 342‑LB
Madura II, James A. 311‑LB
Magyar, Kendra 72‑LB
Maheshwari, Pradeep K. 90‑LB
Mahesula, Swetha 205‑LB
Majak, Maila 169‑LB
Makdissi, Antoine 130‑LB
Malik, Vasanti S. 175‑LB, 177‑LB
Mallikarjuna, Shwetha 3‑LB
Manan, Jyotika 134‑LB
Mandarino, Lawrence J. 311‑LB
Manganiello, Vincent Manganiello 259‑LB
Maniatis, Nikolas 201‑LB, 202‑LB, 203‑LB
Manning Fox, Jocelyn E. 332‑LB
Mansmann, Ulrich 13‑LB
Manson, JoAnn E. 167‑LB, 176‑LB, 177‑LB
Maratos Flier, Eleftheria 317‑LB
Marcinak, John 111‑LB
Marquard, Jan 121‑LB
Marquez, Eladio 208‑LB
Martin, Brittany 50‑LB
Martin, Holly R. 197‑LB
Martin, Jennifer A. 106‑LB
Maruthur, Nisa M. 115‑LB
Mather, Kieren J. 17‑LB
Matheson, Don 101‑LB
Mathieu, Chantal 133‑LB
Matsuoka, Taka-Aki 324‑LB,
Matsushita, Kanae 212‑LB
Matteucci, Elena 168‑LB
Mauceri, Joseph 291‑LB
Mauseth, Richard 101‑LB
Mazzone, Theodore 111‑LB
McCarthy, Mark I. 204‑LB
McDaniel, Kristen 217‑LB
Mcdonald, Molly 144‑LB
McElrtah, Thomas F. 160‑LB
McEwen, Laura N. 47‑LB
McGuire, Darren K. 111‑LB
McKenney, Sarah 100‑LB
McLaughlin, Kerry A. 213‑LB
McTigue, Kathleen M. 68‑LB
Meah, Farah 145‑LB
Medina-Gomez, M.C. 308‑LB
Mehta, Aditya 130‑LB
Mehta, Cyrus 111‑LB
Mehta, Ravindra L. 114‑LB
Mei, Fang 332‑LB
Mei, Yong 97‑LB
Meijer, Rick I. 60‑LB
Meikle, Peter J. 239‑LB
Meinicke, Thomas 119‑LB
ABSTRACT AUTHOR INDEX
Pallardo, Felipe 188‑LB
Pallavi, Puttrevana M. 120‑LB
Pan, Kewu 223‑LB
Pandey, Varun K 325‑LB
Pankratz, Nathan 207‑LB
Panlasigui, Neil 150‑LB
Parenty, Geraldine 326‑LB
Pargal, Summi 3‑LB
Parikh, Lisa 249‑LB
Parikh, Neha 100‑LB
Park, Anna 230‑LB
Park, Hyoungchun 127‑LB
Park, Ji-Hye 54‑LB, 55‑LB
Park, Keun-Gyu 257‑LB
Park, So Hyun 262‑LB
Park, Sun-Hee 127‑LB
Park, Tae-Joon 200-LB
Park, Tae Sun 85‑LB
Park, Yousung 170‑LB
Parker, Stephen 206‑LB, 208‑LB
Parkin, Christopher G. 81‑LB, 139‑LB
Parson, Henri 32‑LB
Parthasarathy, Vijayalaksmi 175‑LB
Pascual, Michael 150‑LB
Pasko, Dorota 204‑LB
Pasquarello, Cindy 50‑LB
Pasquel, Francisco J. 241‑LB
Patel, Nashita 153‑LB
Patel, Niraja 319‑LB
Patel, Pankaj 126‑LB
Patiño, Jorge E. 30‑LB
Patti, Mary-Elizabeth 151‑LB
Pattou, François 221‑LB, 304‑LB
Paumelle, Réjane 10‑LB
Pears, Skye 29‑LB
Peng, Jinghua 129‑LB
Pereira, Mark A. 207‑LB
Perissi, Valentina 240‑LB
Peroni, Odile D. 243‑LB
Perron, Gabrielle 330‑LB
Perry, Rachel J. 113‑LB
Pery, Billy 77‑LB
Pessin, Jeffrey E. 20‑LB
Petersen, Kitt F. 263‑LB
Petri, Renata T. 11‑LB
Petrocchi-Passeri, Pamela 274‑LB
Pettus, Jeremy H. 89‑LB, 95‑LB
Pfeffer, Sébastien 325‑LB
Pichotta, Philip 2‑LB, 92‑LB
Picklesimer, Amy 156‑LB
Piecuch, Emaly 208‑LB
Pihoker, Cate 150‑LB
Pilegaard, Henriette 59‑LB
Pillai, Sreekumar G. 197‑LB
Pinney, Sara E. 157‑LB
Piron, Matthew 194‑LB
Piston, David W. 340‑LB
Pitale, Ameya 143‑LB
Pittas, Anastassios G. 96‑LB
Pober, David 57‑LB
Poitout, Vincent 330‑LB
Polidori, David 254‑LB
Pollin, Toni I. 196‑LB
Polonsky, William H. 63‑LB
Polsky, Sarit 217‑LB
Pongratz, Rebecca L. 342‑LB
Poole, Lucinda A. 66‑LB
Popoola, Orishebawo B. 294‑LB
Popova, Dora 214‑LB
Porceban, Matheus 288‑LB
Porksen, Niels 89‑LB
Possenti, Roberta 274‑LB
Poston, Lucilla 153‑LB
Pouwer, Frans 67‑LB
Poveda, Alaitz 301‑LB
Poy, Matthew N. 325‑LB
Prakash, Prashant K. 90‑LB
Pratley, Richard E. 303‑LB
Predmore, Zachary 140‑LB
Preiser, Nicholas 98‑LB
Preston, Kyle 292‑LB
Previs, Stephen 273‑LB
Previs, Steve 272‑LB
Price, David A. 71‑LB
Prince, Melvin J. 88‑LB, 89‑LB
Priyadarshini, Medha 323‑LB
Probst-Hensch, Nicole 178‑LB, 179‑LB
Pu, Xiaoqi 61‑LB, 309‑LB
Puckrein, Gary A. 139‑LB
Puppala, Sobha 195‑LB
Puri, Vishwajeet 231‑LB
Pyun, Bo-Jeong 35‑LB
Qi, Ling 234‑LB
Qi, Lu 173‑LB, 198‑LB
Qiu, Rong 131‑LB
Quek, Jonathan Caleb 220‑LB
Queniat, Gurvan 304‑LB
Quinn, Lauretta T. 65‑LB
Qunibi, Wajeh 125‑LB
Quon, Michael J. 235‑LB
Quyyumi, Arshed A. 25‑LB
Radford, Elizabeth J. 151‑LB
Radovick, Sally 129‑LB
Ragolia, Louis 277‑LB
Rahbar, Samuel 287‑LB
Rajagopalan, Sujit 110‑LB
Ramasamy, Boominathan 31‑LB
Rameh, Lucia E. 337‑LB
Randeva, Harpal S. 315‑LB
Ranetti, Aurelian Emil 133‑LB
Ranjani, Harish 180‑LB
Rao, Ranganatha 315‑LB
Raphael, Frederica 184‑LB
Rask-Madsen, Christian 266‑LB
Rasmussen, Henrik S. 125‑LB
Rathjen, Thomas 325‑LB
Raverdy, Violeta 304‑LB
Ravishankar, Aarthi 213‑LB
Ravussin, Eric 300‑LB, 302‑LB
Raymond, Ralph 253‑LB, 275‑LB
Raz, Itamar 15‑LB
Read, Linda 3‑LB
Reagan, Louise A. 52‑LB
Reaven, Peter D. 1‑LB
Reddy, Narendra L. 315‑LB
Reddy, Ravi 98‑LB
Redman, Leanne M. 300‑LB
Reers, Christina 326‑LB
Rees, Gwyn 67‑LB
Regner, Kevin R. 21‑LB
Reik, Wolf 325‑LB
Reiser, Jochen 25‑LB
Renström, Frida 301‑LB
Resalat, Navid 98‑LB
Rewers, Arleta 171‑LB
Rewers, Marian 149‑LB
Reynolds, Vincent L. 106‑LB
Rho, Jun Gi 339‑LB
Ricchiuto, Piero 270‑LB
Richardson, Carolyn C. 213‑LB
Richter, Erik A. 59‑LB
Ridderstrale, Martin 118‑LB
LB94
Riggs, Arthur 287‑LB
Rivera, Alba D. 14‑LB
Robertson, R. Paul 253‑LB, 275‑LB
Robinson, Matthew M. 271‑LB
Robson, Stephen C. 153‑LB
Rocha, Hermano A. 123‑LB
Rocha, Milagros 172‑LB
Rochat, Thierry 178‑LB, 179‑LB
Rodríguez, Carlos G. 272‑LB, 273‑LB
Rodriguez, Henry 187‑LB
Rodriguez-Cañete, Alberto 306‑LB, 310‑LB
Rodriguez-Pacheco, Francisca 306‑LB, 310‑LB
Roger, George W. 287‑LB
Rojas-Rodriguez, Raziel 298‑LB
Rollins, Derrick K. 97‑LB
Rondon, Martin 80‑LB
Rosenblit, Paul D. 94‑LB
Rosenkilde, Mette M. 279‑LB
Rosenstock, Julio 107‑LB, 111‑LB, 131‑LB,
307‑LB
Rosman, Paul M. 77‑LB
Ross-Degnan, Dennis 136‑LB
Rossi, Luca 168‑LB
Rother, Kristina I. 276‑LB
Rountree, Austin 336‑LB
Roust, Lori R. 311‑LB
Rovira-Llopis, Susana 172‑LB
Roy, Anirban 100‑LB, 66‑LB
Roy-Duval, Christine 107‑LB
Ruan, Yijun 208‑LB
Rubio-Puchol, Olalla 172‑LB
Ruetten, Hartmut 275‑LB
Ruiz, Tiffany 157‑LB
Russell, Steven J. 72‑LB
Rutkowski, Joseph M. 22‑LB
Ryan, Alexander J. 269‑LB
Rydén, Lars 216‑LB
Sacks, Frank M. 173‑LB, 174‑LB, 198‑LB
Sackstein, Robert 210‑LB
Saghatelian, Alan 243‑LB
Saito, Tsugumichi 20‑LB
Sakaguchi, Masaji 266‑LB
Sakai, Shinobu 210‑LB
Sakimura, Kenji 288‑LB
Sakuma, Toshie 322‑LB
Saleh, Farrah 316‑LB
Sales, Vicencia M. 151‑LB
Salomon, Arthur 222‑LB
Salsali, Afshin 118‑LB
Samocha-Bonet, Dorit 239‑LB
Samovski, Dmitri 250‑LB
Samuel, Varman T. 263‑LB
Sanchez, Rosalia 188‑LB
Sandall, Jane 153‑LB
Sanders, Thomas A. 153‑LB
Santos, Rosa F. 62‑LB
Saremi, Aramesh 1‑LB
Sasaki, Shugo 324‑LB, 334‑LB
Sathyanarayana, Padma 227‑LB
Satin-Smith, Marta 99‑LB
Sattar, Naveed 153‑LB
Savage, Peter 275‑LB
Sawicki, Konrad T. 255‑LB
Scalia, Rosario 292‑LB, 293‑LB
Schade, David S. 17‑LB
Schalkwijk, Casper G 10‑LB
Schatz, Desmond 149‑LB
Scherer, Philipp E. 22‑LB, 233‑LB, 265‑LB
Schindler, Christian 178‑LB, 179‑LB
Schliess, Freimut 121‑LB
Schneider, Martin 326‑LB
Simmons, Rebecca A. 157‑LB
Sims, Emily K. 187‑LB
Singh, Avinainder 134‑LB
Singh, Bhupinder 125‑LB
Singh, Kiran P. 134‑LB
Singh, Maneet 231‑LB
Singh, Sasha 270‑LB
Singhal, Jyotsana 287‑LB
Singhal, Sharad S. 287‑LB
Sinha, Manasi 72‑LB
Sinha, Rajita 249‑LB
Sinha, Vikram P. 89‑LB
Sivapalaratnam, Sutesh S. 308‑LB
Sjöstrand, Annika 148‑LB
Skerrett, Donna 23‑LB
Skjøth, Trine V. 307‑LB
Skokos, Dimitris 268‑LB
Sleeman, Mark 268‑LB
Smith, Brian 219‑LB
Smith, Steven R. 318‑LB
Smulders, Yvo M. 56‑LB, 60‑LB
Sohler, Nancy 138‑LB
Sohn, Hae-Young 13‑LB
Solhjou, Zhabiz 219‑LB
Somesh, Baggavalli P. 120‑LB
Son, Jee Woong 86‑LB
Son, Moon-Ho 280‑LB
Song, Dae-Kyu 256‑LB
Song, Yiqing 167‑LB, 176‑LB
Sontheimer, Alexandra 243‑LB
Sorrenson, Brie 331‑LB
Sosenko, Jay M. 145‑LB
Souhami, Elisabeth 107‑LB
Soumerai, Stephen 136‑LB
Southam, Lorraine 204‑LB, 308‑LB
Souza, Sandra C. 273‑LB
Sowers, James R. 286‑LB
Sparre-Ulrich, Alexander H. 279‑LB
Speight, Jane 66‑LB, 67‑LB
Sperling, Laurence S. 25‑LB
Spiegelman, Donna 175‑LB
Spirakis, Ruth 81‑LB
Staels, Bart 10‑LB
Staimez, Lisa R. 180‑LB
Stansfield, Brain 294‑LB
Staten, Myrlene 253‑LB
Stefanovski, Darko 275‑LB
Steinbeck, Gerhard 13‑LB
Stella, Peter 95‑LB
Stephens, Ella 50‑LB
Stephens, Jacqueline M. 226‑LB
Stepp, David W. 294‑LB
Stier, Christine K. 4‑LB
Stirban, Alin 121‑LB
Stirrups, Kathy 308‑LB
Stitzel, Michael L. 208‑LB
Stolz, Daiana 178‑LB, 179‑LB
Stram, Daniel O. 207‑LB
Straznicky, Nora 53‑LB
Stringham, Heather 206‑LB
Strongman, Helen 169‑LB
Su, Xiong 250‑LB
Suarez-Cuervo, Catalina 115‑LB
Subkhangulova, Aygul 248‑LB
Suh, Kyung-Shin 296‑LB
Sumner, Anne 254‑LB
Sun, Chenglin 229‑LB
Sun, Li-Ping 272‑LB
Sun, Qi 167‑LB, 177‑LB
Sun, Wanqing 6‑LB
Sun, Xiao Jian 235‑LB
LB95
Sundaresan, Sinju 250‑LB
Sundelin, Elias 128‑LB
Super, Dennis 158‑LB
Sury, Matthias 325‑LB
Svendsen, Berit 279‑LB
Sweet, Ian 336‑LB
Syed, Ismail 243‑LB
Synold, Timothy 287‑LB
Szanto, Ildiko 341‑LB
Tabatabai, Niloofar M. 21‑LB
Tahara, Yumiko 82‑LB
Tailleux, Anne 10‑LB
Taitel, Michael 49‑LB
Takahara, Mitsuyoshi 324‑LB
Takahashi, Yusuke 155‑LB
Takaike, Hiroko 190‑LB
Tam, Charmaine 300‑LB
Tamanini, Filippo 201‑LB, 202‑LB
Tan, Ruo-Ding 142‑LB
Tanenberg, Robert J. 78‑LB
Tang, Cheng Cai 106‑LB
Tang, Huilin 124‑LB
Tang, Yuefeng 236‑LB
Tantawi, Hyam R. 47‑LB
Tattikota, Sudhir Gopal 325‑LB
Taylor, Ann 122‑LB
Taylor, D.L. 206‑LB
Taylor, Hugh S. 316‑LB
Teague, April M. 143‑LB, 155‑LB, 157‑LB
Temprosa, Marinella 17‑LB
Tennagels, Norbert 246‑LB
Tersey, Sarah 323‑LB
Thaker, Vidhu 144‑LB
Theisen, Daniel 13‑LB
Theiss, Hans D. 13‑LB
Theoharis, Stamatis 268‑LB
Thevenet, Julien 304‑LB
Thibodeau, Asa 208‑LB
Thiel, Steffen 216‑LB
Thombare, Aparna 78‑LB
Thompson, David M. 155‑LB
Thompson, Michael 185‑LB
Tian, Suyan 229‑LB
Tinahones, Francisco J. 107‑LB
Tinsley, Liane 57‑LB
Tique, Claudia R. 30‑LB
Tobacman, Joanne K. 38‑LB
Tomokazu, Nunoue 258‑LB
Tong, Jenny 173‑LB
Tonks, Katherine 239‑LB
Tonne, Jason M. 322‑LB
Toppari, Jorma 149‑LB
Torres, Jason M. 199‑LB
Torres, Lizardo 51‑LB
Toschi, Elena 317‑LB
Toumilehto, Jaakko 206‑LB
Trautmann, Michael 105‑LB, 303‑LB
Trawley, Steve 66‑LB
Trevino, Michelle B. 262‑LB
Tripaldi, Juliet R. 317‑LB
Tripathy, Devjit T. 195‑LB
Triplett, Eric W. 149‑LB
Tryggestad, Jeanie B. 155‑LB
Tsachalina, Theofaneia 48‑LB
Tsai, Katherine 164‑LB
Tschöp, Matthias 325‑LB
Tseng, Eva 115‑LB
Tseng, Yu-Hua 232‑LB
Tu, Weiping 61‑LB
Tumlin, James A. 114‑LB
Tung, Gregory 171‑LB
ABSTRACT AUTHOR INDEX
Schönke, Milena 288‑LB
Schreiber, Stefanie 326‑LB
Schulz, Christina-Alexandra 174‑LB
Schurmann, Claudia 308‑LB
Schwede, Frank 332‑LB
Scirica, Benjamin M. 15‑LB
Scott, Donald 342‑LB
Scott, Laura 206‑LB
Scott, Robert A. 204‑LB, 308‑LB
Screaton, Robert A. 330‑LB
Sczelecki, Sarah 330‑LB
Seed, Paul T. 153‑LB
Seely, Ellen W. 160‑LB
Segal, Jodi 115‑LB
Segal, Karen R. 23‑LB
Seielstad, Mark 207‑LB
Sekar, Sakthivel 63‑LB, 131‑LB
Selbach, Matthias 325‑LB
Seo, Dongju 249‑LB
Seo, Ji A. 170‑LB
Seo, Ji Hye 170‑LB
Seramani, Sankar 31‑LB, 163‑LB
Sereika, Susan M. 68‑LB
Serné, Erik H. 56‑LB, 60‑LB
Serpas, Lilian 141‑LB
Sesso, Howard D. 176‑LB
Sever, Sanja 25‑LB
Severini, Cinzia 274‑LB
Sha, Haibo 234‑LB
Shah, Chirag P. 37‑LB
Shah, Kaanan 199‑LB
Shah, Neha 315‑LB
Shah, Parag 126‑LB
Shah, Viral 217‑LB
Shamsi, Farnaz 232‑LB
Shanahan, William 299‑LB
Shang, Jin 251‑LB
Shankar, Sudha S. 197‑LB, 253‑LB, 275‑LB
Shanmugham, Satya 99‑LB
Shao, Yimin 283‑LB
Sharifi, Amin 66‑LB
Sharma, Naveen 245‑LB
Sharma, Pragya 247‑LB
Shaw, Collin 319‑LB
She, Jin-Xiong 149‑LB
Shebani, Zachariah 116‑LB
Sheehan, John 164‑LB
Shehata, Kristal 203‑LB
Shepherd, Peter 331‑LB
Sherwin, Robert S. 249‑LB
Shi, Hang 260‑LB
Shibusawa, Ryo 20‑LB
Shimo, Naoki 334‑LB
Shimoda, Yoko 20‑LB
Shimomura, Iichiro 324‑LB, 334‑LB
Shin, Jeong Jae 339‑LB
Shin, Myung 251‑LB
Shon, Ho Sang 85‑LB
Short, Kevin R. 143‑LB
Shulman, Gerald I. 113‑LB, 263‑LB, 271‑LB
Shungin, Dmitry 301‑LB
Shyong, Tai E. 207‑LB
Siddiqui, Uzma Mohammad 185‑LB
Siegle, Greg J. 68‑LB
Sievers, Felix 121‑LB
Sigrist, Kirsten 222‑LB
Silk, Maria E. 114‑LB
Silvia, Maria Elizabeth R. 62‑LB
Sim, Thuan Kai Jelvin 220‑LB
Simell, Olli G. 149‑LB
Siminerio, Linda 68‑LB
ABSTRACT AUTHOR INDEX
Tuomilehto, Jaakko 47‑LB
Turcot, Valerie 204‑LB, 308‑LB
Tuttle, Edward 135‑LB, 142‑LB
Tuttle, Katherine 114‑LB
Tütüncüoglu, Aliye P. 154‑LB
Ucar, Duygu 208‑LB
Uchigata, Yasuko 190‑LB
Uddén Hemmingsson, Joanna 307‑LB
Umpierrez, Guillermo E. 241‑LB
Üner, Aykut G. 288‑LB
Unterman, Terry G. 38‑LB, 261‑LB
Uppal, Karan 241‑LB
Uribe-Bruce, Liliana 2‑LB
Uribe-Wiechers, Ana C. 45‑LB
Vaidya, Anand 160‑LB
Valdes, Jorge 5‑LB
Valdes, Sergio 306‑LB, 310‑LB
Valera, Jose 51‑LB
van Hinsbergh, Victor W. 56‑LB
van Poelgeest, Erik M. 56‑LB
van Polanen, Nynke 22‑LB
Vander Heiden, Anna 83‑LB
Vanhoutte, Jonathan 10‑LB
Vantyghem, Marie Christine 221‑LB
Vargas, Gabriela 51‑LB
Vasavada, Rupangi C. 342‑LB
Vassileva, Maria T. 253‑LB, 275‑LB
Vasudevan, Sudha 175‑LB
Vazquez-Pedreño, Luis 310‑LB
Vehik, Kendra 149‑LB
Vella, Adrian 275‑LB
Vellanki, Priyathama 241‑LB
Vendelbo, Mikkel H. 128‑LB
Venkataranganna, Marikunte V. 120‑LB
Vento, Flor 51‑LB
Verma, Mahesh K. 120‑LB
Veyrat-Durebex, Christelle 341‑LB
Victor, Victor M. 172‑LB
Vikentieva, Elena 214‑LB
Villa, Stephanie R. 323‑LB
Villanes, Sofia 51‑LB
VIllena, Lorena 51‑LB
Vilsbøll, Tina 132‑LB
Vinik, Aaron I. 32‑LB
Vishwanath, Anu 155‑LB
Viswanathan, Prabhakar 111‑LB
von Eckardstein, Arnold 178‑LB, 179‑LB
von Meyenn, Ferdinand 325‑LB
von Oettingen, Julia 184‑LB
von Ziegler, Franz 13‑LB
Voskanyan, Gayane 100‑LB
Wada, Asuka 39‑LB
Wada, Jun 258‑LB, 285‑LB
Walker, Tomas 5‑LB, 71‑LB
Walter, Mary F. 276‑LB
Wanders, Desiree 224‑LB
Wang, Aihua 296‑LB
Wang, Bingshun 61‑LB
Wang, Fang 159‑LB
Wang, Fei 124‑LB
Wang, Guang 313‑LB
Wang, Guixia 229‑LB
Wang, Haiyan 245‑LB
Wang, Hong-Liang 33‑LB, 34‑LB
Wang, Liangsu 251‑LB, 272‑LB
Wang, Lu 176‑LB
Wang, Ningjian 61‑LB, 161‑LB, 309‑LB
Wang, Pin-Wen 37‑LB
Wang, Renwei 207‑LB
Wang, Sheng-Ping 251‑LB, 272‑LB
Wang, Shuxia 267‑LB
Wang, Tiange 174‑LB, 198‑LB
Wang, Tiansheng 124‑LB
Wang, Wang 336‑LB
Wang, Wei 33‑LB, 34‑LB
Wang, Xiaojin 61‑LB
Wang, Xiaolin 73‑LB
Wang, Xinye 329‑LB
Wang, Ying 313‑LB
Ward, Glenn M. 66‑LB
Ward, W. Kenneth 76‑LB
Wardecki, Marek 107‑LB
Warden, Charles 287‑LB
Wardle, Jane 153‑LB
Warren, Graham 70‑LB
Watada, Hirotaka 324‑LB
Watanabe, Eiko 51‑LB
Watanabe, Richard M. 206‑LB
Watson, Karol E. 17‑LB
Webb, Seamus 319‑LB
Weber, Mary Beth 180‑LB
Wedick, Nicole M. 175‑LB
Weindruch, Richard 252‑LB
Weintraub, Daniel S. 294‑LB
Weintraub, Neal L. 294‑LB
Welch, Ryan 206‑LB
Welters, Alena 121‑LB
Wen, Xiaoquan 206‑LB
Weng, Jianping 87‑LB
Wentzell, Katherine 50‑LB
West, Shauna 108‑LB
Westcott, Gregory P. 96‑LB
Wharam, James F. 136‑LB
Wheeler, Heather E. 199‑LB
Wheeler, Michael B. 329‑LB
Whelan, Mary 270‑LB, 295‑LB
White, Ariel 108‑LB
White, Ursula 302‑LB
Whitlock, Kathryn B. 150‑LB
Whitworth, Melissa K. 153‑LB
Willett, Walter C. 175‑LB
Williams, Michelle 160‑LB
Williams, Rachael 169‑LB
Williamson, Donald A. 173‑LB
Willnow, Thomas 248‑LB
Wilson, Lisa 115‑LB
Wiltshire, Esko 146‑LB
Winkler, Thomas W. 204‑LB, 308‑LB
Winters, Alexandra H. 196‑LB
Wisherd, Chris 319‑LB
Wnendt, Stephan 121‑LB
Woerdeman, Jorn 60‑LB
Woerle, Hans J. 119‑LB
Wohlfart, Paulus 246‑LB
Wojtaszewski, Jørgen F.P. 59‑LB
Wolford, Brooke 206‑LB, 208‑LB
Wondisford, Fredric E. 129‑LB
Wong, Chi-Ming 223‑LB, 282‑LB
Wood, Teresa 316‑LB
Woon Puay, Koh 207‑LB
Wouters, Kristiaan 10‑LB
Wright, Kathryn F. 275‑LB
Wronkowitz, Nina 246‑LB
Wu, Bin 259‑LB
Wu, Di 100‑LB
Wu, Hongyu 177‑LB
Wu, Jimmy 112‑LB
Wu, Jun 26‑LB
Wu, Xiwei 287‑LB
Wu, Yan 33‑LB, 34‑LB
Wunderlich, F.T. 233‑LB
Xia, Fangzhen 61‑LB, 161‑LB, 309‑LB
LB96
Xia, Jonathan 265‑LB
Xiao, Xianchao 229‑LB
Xu, Aimin 223‑LB, 239‑LB, 282‑LB
Xu, Haiyan 222‑LB
Xu, Jing 242‑LB
Xu, Liou 139‑LB
Xu, Ping 145‑LB
Xu, Shanshan 261‑LB
Xu, Yuan 313‑LB
Xue, Bingzhong 260‑LB
Xue, Ruidan 232‑LB
Xue, Yaoming 18‑LB
Xuhong, Hou 165‑LB
Yaghootkar, Hanieh 308‑LB
Yajnik, Chittaranjan 182‑LB, 183‑LB
Yajnik, Pallavi 182‑LB
Yale, Jean-François 95‑LB
Yamabi, Masaki 270‑LB
Yamada, Eijiro 20‑LB
Yamada, Iwao 270‑LB
Yamada, Masanobu 20‑LB
Yamaguchi, Satoshi 258‑LB
Yamamoto, Yuichi 324‑LB, 334‑LB
Yamanaka, Hisashi 190‑LB
Yamazaki, Masahiro 212‑LB
Yan, Jing-He 122‑LB
Yang, Alex 125‑LB
Yang, Hyuk In 55‑LB
Yang, Jae Sung 280‑LB
Yang, Juhong 186‑LB
Yang, Lu 287‑LB
Yang, Shaojuan 159‑LB
Yang, Wenying 117‑LB
Yang, Xiaodong 251‑LB, 272‑LB
Yao, Li 205‑LB
Yap, Chui Sun 220‑LB
Yasuda, Tetsuyuki 324‑LB, 334‑LB
Ye, Jenny 107‑LB
Ye, Jianping 259‑LB
Yeo, Kwee Poo 106‑LB
Yepes, Carlos A. 80‑LB
Yerges-Armstrong, Laura 196‑LB
Yiew, Kan Hui 294‑LB
Yi-Frazier, Joyce P. 150‑LB
Yik Ying, Teo 207‑LB
Yilmaz, Hamiyet 154‑LB
Ying, Wei 242‑LB
Yogeshwari, Sivakumaran 120‑LB
Yoo, Hye Jin 170‑LB
Yoon, Sun Ae 127‑LB
Yore, Mark M. 243‑LB
Yorek, Mark A. 32‑LB
Young, Edwin 138‑LB
Young, Kristin L. 204‑LB, 308‑LB
Yu, Ji Hee 170‑LB
Yuan, Geheng 283‑LB
Yuan, Jian-Min 207‑LB
Yun, Nari 86‑LB
Zaharieva, Emanuela 214‑LB
Zangeneh, Farhad 139‑LB
Zavolan, Mihaela 325‑LB
Zeller, Cordula 118‑LB
Zemel, Michael B. 260‑LB
Zeng, Yanmei 18‑LB
Zera, Chloe 160‑LB
Zevallos, Juan C. 14‑LB
Zhang, Dongming 235‑LB
Zhang, Fang 136‑LB
Zhang, Huiliang 336‑LB
Zhang, Jinping 117‑LB
Zhang, Junqing 283‑LB
Zhao, Zhiyun 259‑LB
Zhen, Wei 296‑LB
Zheng, Yan 174‑LB, 198‑LB
Zheng, Yang 6‑LB
Zhong, Xueyu 8‑LB
Zhou, Beiyan 242‑LB
Zhou, Haihong 273‑LB
Zhou, Joanna 152‑LB
Zhou, Junwen 124‑LB
Zhu, Beibei 284‑LB
LB97
Zhu, Chaoxia 61‑LB, 161‑LB, 309‑LB
Zhu, Chunfang 61‑LB, 161‑LB, 309‑LB
Zhu, Meili 36‑LB
Zhu, Yingmin 332‑LB
Ziegler, Anette-Gabriele 149‑LB
Ziegler, Thomas R. 241‑LB
Zinman, Bernard 111‑LB
Zinzen, Robert P. 325‑LB
Zubatov, Yelena 138‑LB
ABSTRACT AUTHOR INDEX
Zhang, Ming 329‑LB
Zhang, Puhong 87‑LB
Zhang, Quanjiang 244‑LB
Zhang, Shu 119‑LB
Zhang, Tong 159‑LB
Zhang, Wenwei 261‑LB
Zhang, Xi 167‑LB
Zhang, Yiyi 238‑LB
Zhao, Peng 226‑LB
Zhao, Tieyun 238‑LB
ABSTRACT Author DISCLOSURE INFORMATION
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
AUTHOR
Abderrahmani, Amar ���������������������������� Disclosed no conflict of interest.
Abdi, Reza �������������������������������������������� Disclosed no conflict of interest.
Abdul-Ghani, Muhammad �������������������� Disclosed no conflict of interest.
Abel, E. Dale ���������������������������������������� Disclosed no conflict of interest.
Abraham, Jenny ����������������������������������� Disclosed no conflict of interest.
Abulizi, Abudukadier ���������������������������� Disclosed no conflict of interest.
Abumrad, Nada ������������������������������������ Disclosed no conflict of interest.
Accili, Domenico ���������������������������������� Disclosed no conflict of interest.
Adachi, Yusuke ������������������������������������� Employee: Ajinomoto Group.
Adams Huet, Beverley ������������������������� Disclosed no conflict of interest.
Adler, Sharon G. ����������������������������������� Advisory Panel: Baxter, Eli Lilly and Company; Consultant:
Baxter, Eli Lilly and Company, Retrophin; Research
Support: Baxter, Eli Lilly and Company, Retrophin.
Adrion, Christine ���������������������������������� Disclosed no conflict of interest.
Agarwal, Ayush K. �������������������������������� Disclosed no conflict of interest.
Agrawal, Prabhat K. ����������������������������� Disclosed no conflict of interest.
Ahmad, Shafqat ����������������������������������� Disclosed no conflict of interest.
Ahn, Ki-Yong ���������������������������������������� Disclosed no conflict of interest.
Aikawa, Masanori �������������������������������� Research Support: Kowa Pharmaceuticals.
Ajena, Aboajela ����������������������������������� Disclosed no conflict of interest.
Akinbosoye, Osayi �������������������������������� Disclosed no conflict of interest.
Akiyama, Haruhiko ������������������������������� Disclosed no conflict of interest.
Akkari, P. Anthony �������������������������������� Consultant: Eli Lilly and Company; Employee: Cabernet
Pharmaceuticals.
Akolkar, Beena ������������������������������������� Disclosed no conflict of interest.
Al Dhuhouri, Jamila S. ������������������������� Disclosed no conflict of interest.
Al Hammadi, Fatema H. ����������������������� Disclosed no conflict of interest.
Al Nuaimi, Asma A. ����������������������������� Disclosed no conflict of interest.
Al Shaikh, Sarah ���������������������������������� Disclosed no conflict of interest.
Alaminos, Miguel A. ���������������������������� Disclosed no conflict of interest.
Albu, Jeanine ��������������������������������������� Research Support: Merck & Co., Inc., Novo Nordisk Inc.,
Weight Watchers International, Inc.
Alcain-Martinez, Guillermo ������������������ Disclosed no conflict of interest.
Ali, Mohammed K. ������������������������������� Disclosed no conflict of interest.
Ali, Nahed �������������������������������������������� Disclosed no conflict of interest.
Ali, Nasiri ��������������������������������������������� Disclosed no conflict of interest.
Alkanani, Aimon ����������������������������������� Disclosed no conflict of interest.
Alkarni, Meyad A. �������������������������������� Disclosed no conflict of interest.
Alkhaddo, Jamil B. ������������������������������� Research Support: Eli Lilly and Company.
Alkhalidy, Hana ������������������������������������ Disclosed no conflict of interest.
Alkorta-Aranburu, Gorka ���������������������� Disclosed no conflict of interest.
Almaca, Joana ������������������������������������� Disclosed no conflict of interest.
Almeda-Valdes, Paloma ����������������������� Disclosed no conflict of interest.
Alquier, Thierry ������������������������������������� Disclosed no conflict of interest.
Al-Trad, Bahaa �������������������������������������� Disclosed no conflict of interest.
Álvarez-Escolá, Carmen ����������������������� Disclosed no conflict of interest.
Alzaid, Aus ������������������������������������������� Advisory Panel: AstraZeneca, Boehringer Ingelheim,
Hikma, Janssen, Merck Serono, Takeda; Speaker’s
Bureau: AstraZeneca, Boehringer Ingelheim, Hikma,
Janssen, Merck Serono, Novo Nordisk.
Amblee, Ambika ����������������������������������� Research Support: AstraZeneca Pharmaceuticals LP.
Amer, Ahmed ���������������������������������������� Employee: Novartis Pharmaceuticals Corporation.
Ammar, Hala ����������������������������������������� Disclosed no conflict of interest.
Andersen, Emilie S. ������������������������������ Disclosed no conflict of interest.
Anderson, Rozalyn M. �������������������������� Disclosed no conflict of interest.
Andreasen, Camilla ������������������������������ Disclosed no conflict of interest.
Andrew, Toby ���������������������������������������� Disclosed no conflict of interest.
Angueira, Anthony R. ��������������������������� Disclosed no conflict of interest.
Anil, Tharappel M. ������������������������������� Disclosed no conflict of interest.
Anjana, Ranjit M. ��������������������������������� Disclosed no conflict of interest.
Annabi, Firas A. ������������������������������������ Disclosed no conflict of interest.
Anton, Stephen D. �������������������������������� Disclosed no conflict of interest.
Antosik, Karolina ���������������������������������� Disclosed no conflict of interest.
Anup, Mammen O. ������������������������������� Disclosed no conflict of interest.
Apovian, Caroline M. ��������������������������� Consultant: Amylin, Arena, EnteroMedics, Johnson
and Johnson, Merck, Novo Nordisk, Nutrisystem,
Orexigen, Sanofi-Aventis, Zafgen; Research
Support: Amylin, Aspire Bariatrics, Dr. Robert C. and
Veronica Atkins Foundation, Eli Lilly, GI Dynamics,
MetaProteomics, MYOS Corporation, Orexigen, Pfizer,
Sanofi-Aventis; Speaker’s Bureau: Takeda.
Araque, Katherine �������������������������������� Disclosed no conflict of interest.
Araujo, Renata ������������������������������������� Disclosed no conflict of interest.
Ardehali, Hossein ��������������������������������� Disclosed no conflict of interest.
Ardissone, Alexandria N. ��������������������� Disclosed no conflict of interest.
Arias, Edward B. ���������������������������������� Disclosed no conflict of interest.
Armstrong, Debra A. ���������������������������� Disclosed no conflict of interest.
Arndt, Kelly ������������������������������������������ Disclosed no conflict of interest.
RELATIONSHIP/COMPANY
Aroda, Vanita R. ����������������������������������� Consultant: Novo Nordisk Inc., Sanofi U.S., VeraLight, Inc.;
Research Support: Aegerion Pharmaceuticals, Inc.,
Amylin Pharmaceuticals, LLC., Bayhill Therapeutics,
Concert Pharmaceuticals, GlaxoSmithKline, Interkrin
Therapeutics, Merck & Co., Inc., Novo Nordisk
Inc., Roche USA, Sanofi U.S., Shionogi Inc., Takeda
Pharmaceuticals U.S.A., Inc., VeraLight, Inc.
Aronson, Ronnie ����������������������������������� Advisory Panel: Janssen Pharmaceuticals, Novo
Nordisk, Inc., Sanofi; Consultant: AstraZeneca
Pharmaceuticals LP, Bristol-Myers Squibb Company,
Medtronic, Sanofi, Takeda Pharmaceutical
Company Ltd; Other Relationship: AstraZeneca
Pharmaceuticals LP, BD Medical Diabetes Care,
Boehringer Ingelheim Pharmaceuticals, Inc., BristolMyers Squibb Company, Novo Nordisk, Inc., Sanofi,
Takeda Pharmaceutical Company Ltd.; Research
Support: Abbott Laboratories, Inc., Andromeda
Biotech Ltd, AstraZeneca Pharmaceuticals LP, BD
Medical Diabetes Care, Boehringer Ingelheim
Pharmaceuticals, Inc., Bristol-Myers Squibb Company,
ConjuChem, Diartis Pharmaceuticals, Eli Lilly and
Company, Essem Research, GlaxoSmithKline, ICON,
Janssen Pharmaceuticals, Medpace, Medtronic,
Merck, Novartis Pharmaceuticals Corporation, Novo
Nordisk, Inc., Piramal BD, Quintiles, Regeneron
Pharmaceuticals, Roche Pharmaceuticals, Sanofi,
Takeda Pharmaceutical Company Ltd, Tolerx.
Arous, Caroline ������������������������������������ Disclosed no conflict of interest.
Arslan, Banu ����������������������������������������� Disclosed no conflict of interest.
Arthur, John ������������������������������������������ Disclosed no conflict of interest.
Arumugam, Kokila �������������������������������� Disclosed no conflict of interest.
Arya, Rector ����������������������������������������� Disclosed no conflict of interest.
Aryal, Pratik ������������������������������������������ Disclosed no conflict of interest.
Ashankyty, Ibraheem ���������������������������� Disclosed no conflict of interest.
Asimakopoulou, Andriana �������������������� Disclosed no conflict of interest.
Assaad-Khalil, Samir H. ����������������������� Disclosed no conflict of interest.
Atalay, Nesil ����������������������������������������� Disclosed no conflict of interest.
Atkins, Ashley �������������������������������������� Disclosed no conflict of interest.
Atkinson, Mark A. �������������������������������� Disclosed no conflict of interest.
Austen, Matthias ��������������������������������� Disclosed no conflict of interest.
Ayala, Iriscilla ��������������������������������������� Disclosed no conflict of interest.
Ayala, Jennifer E. ��������������������������������� Disclosed no conflict of interest.
Ayala, Julio E. �������������������������������������� Disclosed no conflict of interest.
Azzi, Jamil �������������������������������������������� Disclosed no conflict of interest.
Bach, Leon A. ��������������������������������������� Speaker’s Bureau: Sanofi.
Bae, Jae-Hoon ������������������������������������� Disclosed no conflict of interest.
Bae, Jin-Sik ������������������������������������������ Disclosed no conflict of interest.
Bae, Kwi-Hyun ������������������������������������� Disclosed no conflict of interest.
Bae, Su Ah ������������������������������������������� Disclosed no conflict of interest.
Ba-Essa, Ebtesam M. ��������������������������� Disclosed no conflict of interest.
Bagger, Jonatan I. �������������������������������� Disclosed no conflict of interest.
Bahceci, Mitat �������������������������������������� Disclosed no conflict of interest.
Bahijri, Suhad M. ��������������������������������� Disclosed no conflict of interest.
Bahmanyar, Shahram ��������������������������� Research Support: Centre for Pharmacoepidemiology (CPE)
at Karolinska Institute has contracts with several
pharmaceutical companies and performs research for
them through research grants.
Bahn, Gideon ���������������������������������������� Disclosed no conflict of interest.
Bai, Ramya ������������������������������������������� Disclosed no conflict of interest.
Baidal, David A. ����������������������������������� Disclosed no conflict of interest.
Baik, Sei Hyun �������������������������������������� Disclosed no conflict of interest.
Bailey, Kathleen A. ������������������������������� Disclosed no conflict of interest.
Bajaj, Mandeep ������������������������������������ Advisory Panel: Genentech, Inc.; Research Support:
American Diabetes Association, AstraZeneca,
Boehringer Ingelheim Pharmaceuticals, Inc.,
Bristol-Myers Squibb, Eli Lilly and Company, Novo
Nordisk Inc.; Speaker’s Bureau: Sanofi U.S., Takeda
Pharmaceuticals U.S.A., Inc.
Balk, Ethan M. �������������������������������������� Disclosed no conflict of interest.
Balliro, Courtney ���������������������������������� Disclosed no conflict of interest.
Balo, Andrew ��������������������������������������� Employee: Dexcom, Inc.
Baltaro, Richard J. ������������������������������� Disclosed no conflict of interest.
Banks, Michaela ���������������������������������� Disclosed no conflict of interest.
Bañuls, Celia ���������������������������������������� Disclosed no conflict of interest.
Barber, Thomas M. ������������������������������� Disclosed no conflict of interest.
Baron, Michelle A. ������������������������������� Employee: Intarcia Therapeutics, Inc.
Barquiel, Beatriz ����������������������������������� Disclosed no conflict of interest.
Barrett-Connor, Elizabeth L. ����������������� Disclosed no conflict of interest.
LB98
RELATIONSHIP/COMPANY
AUTHOR
Barroso, Inês ���������������������������������������� Disclosed no conflict of interest.
Barta, William �������������������������������������� Disclosed no conflict of interest.
Bartolomucci, Alessandro �������������������� Disclosed no conflict of interest.
Bassaganya-Riera, Josep �������������������� Disclosed no conflict of interest.
Batra, Manav ��������������������������������������� Disclosed no conflict of interest.
Bauman, Viviana ���������������������������������� Disclosed no conflict of interest.
Bayeva, Marina ������������������������������������ Disclosed no conflict of interest.
Bays, Harold ����������������������������������������� Consultant: Amgen Inc., AstraZeneca Pharmaceuticals
LP, Bristol-Myers Squibb Company, Catabasis
Pharmaceuticals, Inc., Daiichi-Sankyo Co., Ltd.,
Eisai Co., Ltd., Isis Pharmaceuticals, Inc., Merck
& Co., Inc., Novartis Corporation, Omthera, Vivus
Inc., WPU Therapeutics; Research Support: Alere,
Amarin Pharma, Inc., Amgen Inc., Ardea, Arisaph,
AstraZeneca Pharmaceuticals LP, Boehringer
Ingelheim Pharmaceuticals, Inc., Bristol-Myers
Squibb Company, Californian Raisin Board, Catabasis
Pharmaceuticals, Inc., Cymabay, Eisai Co., Ltd.,
Elcelyx Therapeutics, Inc., Eli Lilly and Company,
Esperion Therapeutics, Inc., Forest Pharmaceuticals,
Inc., Gilead, Given, GlaxoSmithKline, Hanmi, High
Point Pharmaceuticals LLC, Hisun, Hoffman-La
Roche Limited, Home Access, Janssen Research &
Development LLC, Merck & Co., Inc., Metabolex,
Nektar, Novartis Pharmaceuticals Corporation, Novo
Nordisk Inc., Omthera, Orexigen Therapeutics, Inc.,
Pfizer Inc., Pronova, Regeneron Pharmaceuticals, Inc.,
Sanofi U.S., Takeda Pharmaceuticals U.S.A., Inc.,
TIMI, TransTech Pharma, LLC., Trygg, Vivus Inc.,WPU
Pharmaceuticals.
Beaucamps, Cédric ������������������������������ Disclosed no conflict of interest.
Beauregard, Natalie ����������������������������� Disclosed no conflict of interest.
Beck, Andrew ��������������������������������������� Disclosed no conflict of interest.
Becker, Alexander �������������������������������� Disclosed no conflict of interest.
Beckman, Kenneth ������������������������������� Disclosed no conflict of interest.
Bee, Yong Mong ����������������������������������� Disclosed no conflict of interest.
Beeravolu, Swathi �������������������������������� Disclosed no conflict of interest.
Belfort De Aguiar, Renata �������������������� Disclosed no conflict of interest.
Bell, Graeme I. ������������������������������������� Disclosed no conflict of interest.
Bell, Ruth ���������������������������������������������� Disclosed no conflict of interest.
Below, Jennifer E. �������������������������������� Disclosed no conflict of interest.
Belton, Anne ���������������������������������������� Advisory Panel: Boehringer Ingelheim, Sanofi; Consultant:
Abbott, Lifescan Canada.
Beltran, Yobana ������������������������������������ Disclosed no conflict of interest.
Benjamin, Tonya R. ������������������������������� Disclosed no conflict of interest.
Benson, Tyler W. ���������������������������������� Disclosed no conflict of interest.
Benware, Sheila ����������������������������������� Employee: Pacific Diabetes Technologies, Inc.; Stock/
Shareholder: Pacific Diabetes Technologies, Inc.
Bergenstal, Richard M. ������������������������ Employee: Abbott Diabetes Care, Bayer, DexCom, Johnson
& Johnson, Medtronic and Roche.
Berger, Zack ������������������������������������������ Disclosed no conflict of interest.
Bergeron, Valerie ��������������������������������� Disclosed no conflict of interest.
Bergman, Richard N. ���������������������������� Disclosed no conflict of interest.
Bertinetti, Daniela �������������������������������� Disclosed no conflict of interest.
Betteridge, John ���������������������������������� Disclosed no conflict of interest.
Beula, Sara ������������������������������������������� Disclosed no conflict of interest.
Bhad, Prafulla ��������������������������������������� Employee: Novartis Pharmaceuticals Corporation.
Bhakoo, Kishore Kumar ������������������������ Disclosed no conflict of interest.
Bhansali, Anil ��������������������������������������� Disclosed no conflict of interest.
Bhat, Dattatreya ����������������������������������� Disclosed no conflict of interest.
Bhatt, Deepak L. ����������������������������������� Research Support: AstraZeneca Pharmaceuticals LP.
Bhattacharjee, Alpana ������������������������� Disclosed no conflict of interest.
Bhattacharyya, Sumit ��������������������������� Disclosed no conflict of interest.
Bianco, Suzy ����������������������������������������� Disclosed no conflict of interest.
Biddinger, Sudha B. ������������������������������ Disclosed no conflict of interest.
Bihl, Ji C. ���������������������������������������������� Disclosed no conflict of interest.
Bird, Adrian ������������������������������������������ Disclosed no conflict of interest.
Birk, Jesper ������������������������������������������ Disclosed no conflict of interest.
Bjørbæk, Christian ������������������������������� Disclosed no conflict of interest.
Blangero, John ������������������������������������� Disclosed no conflict of interest.
Blankenship, Jennifer M. ��������������������� Disclosed no conflict of interest.
Blankfard, Martin ��������������������������������� Disclosed no conflict of interest.
Blaser, Martin J. ����������������������������������� Disclosed no conflict of interest.
Blau, Jenny E. �������������������������������������� Disclosed no conflict of interest.
Boehnke, Michael �������������������������������� Disclosed no conflict of interest.
Bogdonov, Vladimir ������������������������������ Disclosed no conflict of interest.
Bohnett, Lucas ������������������������������������� Employee: Dexcom, Inc.
Bolen, Shari ������������������������������������������ Disclosed no conflict of interest.
Bonner, Caroline ����������������������������������� Disclosed no conflict of interest.
Borecki, Ingrid �������������������������������������� Disclosed no conflict of interest.
Borowiec, Maciej ��������������������������������� Disclosed no conflict of interest.
Bosco, Domenico ��������������������������������� Disclosed no conflict of interest.
Bose, Namrata ������������������������������������� Disclosed no conflict of interest.
RELATIONSHIP/COMPANY
Bouchaert, Emanuel ����������������������������� Disclosed no conflict of interest.
Boulware, David ����������������������������������� Disclosed no conflict of interest.
Bouyakdan, Khalil �������������������������������� Disclosed no conflict of interest.
Bouzakri, Karim ������������������������������������ Disclosed no conflict of interest.
Brady, Matthew J. ������������������������������� Disclosed no conflict of interest.
Branigan, Deborah ������������������������������� Disclosed no conflict of interest.
Brar, Harpreet ��������������������������������������� Disclosed no conflict of interest.
Brathwaite, Collin �������������������������������� Disclosed no conflict of interest.
Braun, Barry ����������������������������������������� Disclosed no conflict of interest.
Bray, George ����������������������������������������� Disclosed no conflict of interest.
Brazg, Ronald ��������������������������������������� Research Support: Medtronic MiniMed, Inc.
Breen, Matthew ����������������������������������� Employee: Pacific Diabetes Technologies, Inc.; Stock/
Shareholder: Pacific Diabetes Technologies, Inc.
Brehm, Michael A. ������������������������������� Disclosed no conflict of interest.
Brehm, Tyler J. ������������������������������������� Disclosed no conflict of interest.
Brenner, Christoph �������������������������������� Disclosed no conflict of interest.
Breton, Marc D. ������������������������������������ Research Support: Animas Corporation, BD MedicalDiabetes Care, Dexcom, Inc., Insulet Corporation,
LifeScan, Inc., Sanofi U.S., Tandem Diabetes Care,
Inc.
Briddell, Robert ������������������������������������ Disclosed no conflict of interest.
Briley, Annette L. ���������������������������������� Disclosed no conflict of interest.
Brismar, Kerstin ������������������������������������ Disclosed no conflict of interest.
Brito-Sanfiel, Miguel ���������������������������� Advisory Panel: Janssen, MSD; Speaker’s Bureau: Abbott,
AstraZeneca, Eli Lilly, MSD, Novo Nordisk.
Brittain, Julia ��������������������������������������� Disclosed no conflict of interest.
Brodsky, Michael R. ����������������������������� Disclosed no conflict of interest.
Broedl, Uli �������������������������������������������� Employee: Boehringer Ingelheim GmbH.
Brosen, Kim ������������������������������������������ Disclosed no conflict of interest.
Brosius III, Frank C. ������������������������������ Consultant: Eli Lilly and Company, Merck & Co., Inc.;
Research Support: Takeda Pharmaceuticals U.S.A.,
Inc.
Brosnan, Julia �������������������������������������� Disclosed no conflict of interest.
Brown, Jacob D. ����������������������������������� Disclosed no conflict of interest.
Brown, Rebecca J. ������������������������������� Disclosed no conflict of interest.
Browne, Jessica L. ������������������������������� Disclosed no conflict of interest.
Bruckbauer, Antje ��������������������������������� Employee: NuSirt Biopharma; Stock/Shareholder: NuSirt
Bopharma.
Brüning, Jens C. ����������������������������������� Disclosed no conflict of interest.
Bryan, Joseph �������������������������������������� Disclosed no conflict of interest.
Buckingham, Bruce A. �������������������������� Advisory Panel: BD Medical-Diabetes Care, Medtronic
MiniMed, Inc., Novo Nordisk Inc., Sanofi U.S.,
Tandem Diabetes Care, Inc., Unomedical; Research
Support: Bayer HealthCare, Dexcom, Inc., Insulet
Corporation, LifeScan, Inc., Medtronic MiniMed, Inc.,
Tandem Diabetes Care, Inc., The Leona M. and Harry
B. Helmsley Charitable Trust, Unomedical.
Budoff, Matthew ���������������������������������� Disclosed no conflict of interest.
Budry, Lionel ����������������������������������������� Employee: Novartis AG.
Burak, Mehmet Furkan ������������������������� Disclosed no conflict of interest.
Buring, Julie E. ������������������������������������� Disclosed no conflict of interest.
Burke, Paivi M. ������������������������������������� Disclosed no conflict of interest.
Burmeister, Melissa A. ������������������������� Disclosed no conflict of interest.
Burns, Cheryl ���������������������������������������� Disclosed no conflict of interest.
Buzzetti, Raffaella �������������������������������� Advisory Panel: Eli Lilly, Sanofi; Board Member: Abbott,
Takeda; Speaker’s Bureau: AstraZeneca, Eli Lilly,
Medtronic, Novartis, Novo Nordisk, Sanofi, Takeda.
Cai, Weikang ���������������������������������������� Disclosed no conflict of interest.
Caiazzo, Robert ������������������������������������ Disclosed no conflict of interest.
Caicedo, Alejandro ������������������������������� Disclosed no conflict of interest.
Callan, Judith A. ���������������������������������� Disclosed no conflict of interest.
Calle, Roberto A. ���������������������������������� Employee: Pfizer Inc.; Stock/Shareholder: Pfizer Inc.
Caloyeras, John ����������������������������������� Employee: Amgen Inc.; Stock/Shareholder: Amgen Inc.
Campa, David ��������������������������������������� Disclosed no conflict of interest.
Campbell, Jonathan E. ������������������������� Disclosed no conflict of interest.
Campbell, Latoya E. ����������������������������� Disclosed no conflict of interest.
Camporez, Joao-Paulo G. ��������������������� Disclosed no conflict of interest.
Campos, Hannia ����������������������������������� Disclosed no conflict of interest.
Campos, Maribel ���������������������������������� Disclosed no conflict of interest.
Canepa, Ronald J. �������������������������������� Disclosed no conflict of interest.
Cang, Zhen ������������������������������������������� Disclosed no conflict of interest.
Canney, Lori ������������������������������������������ Employee: Biodel Inc.; Stock/Shareholder: Biodel Inc.
Cao, Qiang �������������������������������������������� Disclosed no conflict of interest.
Capehorn, Matthew ����������������������������� Advisory Panel: Boehringer Ingelheim, Eli Lilly, Merck
Sharp & Dohme, Novo Nordisk; Research Support:
Cambridge Weight Plan, Lighter Life, Novo Nordisk;
Speaker’s Bureau: Boehringer Ingelheim, Eli Lilly,
Merck Sharp & Dohme; Stock/Shareholder: RIO
Weight Management Ltd.
Cappell, Katherine ������������������������������� Employee: Truven Health Analytics.
Capuano, George ��������������������������������� Employee: Janssen Research & Development, LLC.
Carbo, Adria ����������������������������������������� Disclosed no conflict of interest.
Cardamone, Maria D. ��������������������������� Disclosed no conflict of interest.
LB99
AUTHOR DISCLOSURE
AUTHOR
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
Cárdenas, Jose L. ��������������������������������� Disclosed no conflict of interest.
Cardillo, Tracy E. ����������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Cargill, Robert S. ���������������������������������� Employee: Pacific Diabetes Technologies, Inc.; Stock/
Shareholder: Pacific Diabetes Technologies, Inc.
Carless, Melanie ���������������������������������� Disclosed no conflict of interest.
Carley, David W. ����������������������������������� Disclosed no conflict of interest.
Carls, Ginger S. ������������������������������������ Consultant: Intarcia Therapeutics, Inc.
Carmody, David ������������������������������������ Disclosed no conflict of interest.
Caron, Nicole ��������������������������������������� Disclosed no conflict of interest.
Carrington, Paul ����������������������������������� Disclosed no conflict of interest.
Cartee, Greg ����������������������������������������� Disclosed no conflict of interest.
Carter, Leslie ���������������������������������������� Disclosed no conflict of interest.
Casellini, Carolina M. �������������������������� Disclosed no conflict of interest.
Castle, Jessica R. ��������������������������������� Advisory Panel: Biodel Inc., Novo Nordisk Inc.; Speaker’s
Bureau: Dexcom, Inc, Roche Diagnostics; Stock/
Shareholder: Pacific Diabetes Technologies.
Catalano, Patrick M. ���������������������������� Disclosed no conflict of interest.
Cavalcante, Lilian L.A. ������������������������� Disclosed no conflict of interest.
Cederquist, Carly T. ������������������������������ Disclosed no conflict of interest.
Cefalu, William T. ��������������������������������� Disclosed no conflict of interest.
Cero, Cheryl ������������������������������������������ Disclosed no conflict of interest.
Cha, Dae Ryong ������������������������������������ Disclosed no conflict of interest.
Cha, Ji-Young ��������������������������������������� Disclosed no conflict of interest.
Chabtini, Lola ��������������������������������������� Disclosed no conflict of interest.
Chacra, Antonio ����������������������������������� Disclosed no conflict of interest.
Chae, Yu Na ������������������������������������������ Disclosed no conflict of interest.
Chakrabarti, Amitava ��������������������������� Disclosed no conflict of interest.
Chamberlain, James J. ������������������������ Speaker’s Bureau: AstraZeneca, Bristol-Myers Squibb,
Janssen Pharmaceutical Companies of Johnson &
Johnson, Sanofi U.S.
Champagne, Catherine M. ������������������� Disclosed no conflict of interest.
Chan, Lawrence C.B. ���������������������������� Disclosed no conflict of interest.
Chan, You-Ping ������������������������������������� Disclosed no conflict of interest.
Chane-Woon-Ming, Béatrice ��������������� Disclosed no conflict of interest.
Chang, Evan ����������������������������������������� Disclosed no conflict of interest.
Chang, Hsiang-Chun ���������������������������� Disclosed no conflict of interest.
Chapel, Sunny �������������������������������������� Disclosed no conflict of interest.
Charles, Rene ��������������������������������������� Disclosed no conflict of interest.
Chatterjee, Tapan K. ����������������������������� Disclosed no conflict of interest.
Chattopadhyay, Munmun ��������������������� Disclosed no conflict of interest.
Chaudhuri, Ajay ������������������������������������ Disclosed no conflict of interest.
Chaudhuri, Rima ����������������������������������� Disclosed no conflict of interest.
Chen, Chi ���������������������������������������������� Disclosed no conflict of interest.
Chen, Hong-Chi ������������������������������������ Disclosed no conflict of interest.
Chen, Huntga ��������������������������������������� Employee: AstraZeneca Pharmaceuticals LP.
Chen, Lei ���������������������������������������������� Employee: Merck & Co., Inc.
Chen, Liwei ������������������������������������������ Disclosed no conflict of interest.
Chen, Lulu �������������������������������������������� Disclosed no conflict of interest.
Chen, Yanfang �������������������������������������� Disclosed no conflict of interest.
Chen, Yi ������������������������������������������������ Disclosed no conflict of interest.
Chen, Yidong ���������������������������������������� Disclosed no conflict of interest.
Chen, Yimei ������������������������������������������ Disclosed no conflict of interest.
Chen, Yingchao ������������������������������������ Disclosed no conflict of interest.
Cheng Lee Ping, Peter �������������������������� Disclosed no conflict of interest.
Cheng, Xiaodong ���������������������������������� Disclosed no conflict of interest.
Cheong, Ye-Hwang ������������������������������ Disclosed no conflict of interest.
Chepurny, Oleg G. �������������������������������� Disclosed no conflict of interest.
Chernausek, Steven ����������������������������� Disclosed no conflict of interest.
Cherñavvsky, Daniel ����������������������������� Research Support: Dexcom, Inc.
Chevalier, Soazig ���������������������������������� Employee: Sanofi; Stock/Shareholder: Sanofi.
Chhabra, Mohinish ������������������������������� Disclosed no conflict of interest.
Chin, Alex J. ����������������������������������������� Employee: AstraZeneca Pharmaceuticals LP, self.
Chinchwadkar, Manoj �������������������������� Disclosed no conflict of interest.
Chines, Peter ���������������������������������������� Disclosed no conflict of interest.
Chisholm, Don J. ���������������������������������� Disclosed no conflict of interest.
Cho, Yoon Hi ����������������������������������������� Disclosed no conflict of interest.
Cho, Youngjin ��������������������������������������� Disclosed no conflict of interest.
Chodavarapu, Praneeta ������������������������ Disclosed no conflict of interest.
Choe, Gina �������������������������������������������� Disclosed no conflict of interest.
Choi, Dong Seop ���������������������������������� Disclosed no conflict of interest.
Choi, In Young �������������������������������������� Disclosed no conflict of interest.
Choi, Kyung Mook �������������������������������� Disclosed no conflict of interest.
Choi, Seul Min ������������������������������������� Disclosed no conflict of interest.
Choi, Siak Leng ������������������������������������ Employee: Eli Lilly and Company.
Choi, Soomin ���������������������������������������� Disclosed no conflict of interest.
Chorev, Michael ����������������������������������� Stock/Shareholder: Mellitus, LLC.
Christensen, Mette M.H. ��������������������� Disclosed no conflict of interest.
Christensen, Mikkel ����������������������������� Disclosed no conflict of interest.
Christiansen, Claus ������������������������������ Stock/Shareholder: Nordic Bioscience.
Christie, Michael R. ����������������������������� Disclosed no conflict of interest.
Christofori, Gerhard ����������������������������� Disclosed no conflict of interest.
Christopher, Michael J. ������������������������ Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Christopher, Solomon ��������������������������� Employee: EPID Research performs financially supported
studies for several pharmaceutical companies
including Takeda Development Centre Europe.
Chuck, Leonard ������������������������������������� Disclosed no conflict of interest.
Ciaraldi, Theodore P. ���������������������������� Consultant: Shionogi Inc.
Clargo, Alison ��������������������������������������� Employee: UCB Pharma.
Claudius, Birgitte ��������������������������������� Employee: Novo Nordisk A/S; Stock/Shareholder: Novo
Nordisk A/S.
Cobos-Bravo, Juan F. ���������������������������� Disclosed no conflict of interest.
Cochrane, Katie ������������������������������������ Disclosed no conflict of interest.
Cognard, Emmanuelle �������������������������� Disclosed no conflict of interest.
Cohen, Neale ��������������������������������������� Disclosed no conflict of interest.
Cohen, Ronald �������������������������������������� Disclosed no conflict of interest.
Coletta, Dawn K. ���������������������������������� Disclosed no conflict of interest.
Colin, Laurence ������������������������������������ Employee: Novartis Pharmaceuticals Corporation.
Collins, Francis S. ��������������������������������� Disclosed no conflict of interest.
Collins, Stephen J. ������������������������������� Disclosed no conflict of interest.
Colman, Peter ��������������������������������������� Disclosed no conflict of interest.
Colman, Ricki J. ����������������������������������� Disclosed no conflict of interest.
Comstock, Dawn ���������������������������������� Disclosed no conflict of interest.
Comte-Perret, Sophie ��������������������������� Disclosed no conflict of interest.
Condon, John ��������������������������������������� Disclosed no conflict of interest.
Conley, John ����������������������������������������� Stock/Shareholder: Pacific Diabetes Technologies, Inc.
Consani, Cristina ���������������������������������� Disclosed no conflict of interest.
Constable, R. Todd ������������������������������� Disclosed no conflict of interest.
Conway, Baqiyyah �������������������������������� Disclosed no conflict of interest.
Cooper, Julian �������������������������������������� Disclosed no conflict of interest.
Cooper, Marcus ������������������������������������ Disclosed no conflict of interest.
Corkey, Barbara E. �������������������������������� Disclosed no conflict of interest.
Corkill, Holly ����������������������������������������� Disclosed no conflict of interest.
Corvera, Silvia �������������������������������������� Disclosed no conflict of interest.
Costacou, Tina �������������������������������������� Disclosed no conflict of interest.
Coster, Adelle C.F. �������������������������������� Disclosed no conflict of interest.
Covington-Kolb, Sarah ������������������������� Disclosed no conflict of interest.
Cox, Nancy J. ��������������������������������������� Disclosed no conflict of interest.
Craig, Jagriti ���������������������������������������� Employee: Janssen Research & Development, LLC.
Craig, Maria ����������������������������������������� Disclosed no conflict of interest.
Crandall, Jill ����������������������������������������� Disclosed no conflict of interest.
Croker, Helen ���������������������������������������� Disclosed no conflict of interest.
Cromack, Douglas T. ����������������������������� Disclosed no conflict of interest.
Crowe, Matthew J. ������������������������������ Disclosed no conflict of interest.
Cudejko, Céline ������������������������������������ Disclosed no conflict of interest.
Cuezva, Jose M. ����������������������������������� Disclosed no conflict of interest.
Cui, Xin ������������������������������������������������� Disclosed no conflict of interest.
Cunnick, Jess M. ���������������������������������� Disclosed no conflict of interest.
Cupples, L. Adrienne ���������������������������� Disclosed no conflict of interest.
Curie, Justin ����������������������������������������� Disclosed no conflict of interest.
Curran, Joanne E. ��������������������������������� Disclosed no conflict of interest.
Cutarelli, Alessandro ��������������������������� Disclosed no conflict of interest.
Dabelea, Dana ������������������������������������� Disclosed no conflict of interest.
Dabra, Shakun �������������������������������������� Disclosed no conflict of interest.
Dagogo-Jack, Samuel �������������������������� Consultant: Boehringer Ingelheim Pharmaceuticals,
Inc., Merck & Co.,Inc., Novo Nordisk Inc.; Research
Support: AstraZeneca, Boehringer Ingelheim GmbH,
Bristol-Myers Squibb, Novo Nordisk Inc.
Dai, Feihan F. ���������������������������������������� Disclosed no conflict of interest.
Dai, Hongji ������������������������������������������� Disclosed no conflict of interest.
Dandona, Paresh ���������������������������������� Disclosed no conflict of interest.
Dangott, Bryan J. ��������������������������������� Disclosed no conflict of interest.
Dasari, Paul S. �������������������������������������� Disclosed no conflict of interest.
Davenport, Bennett J. �������������������������� Disclosed no conflict of interest.
Davidson, Jaime A. ������������������������������ Disclosed no conflict of interest.
Davies, Melanie ����������������������������������� Advisory Panel: AstraZeneca Pharmaceuticals LP,
Boehringer Ingelheim GmbH, Eli Lilly and Company,
Janssen Research & Development LLC, Merck Sharp
& Dohme, Novo Nordisk A/S, Sanofi U.S.; Consultant:
AstraZeneca Pharmaceuticals LP, Boehringer
Ingelheim GmbH, Eli Lilly and Company, Janssen
Research & Development LLC, Merck Sharp & Dohme,
Novo Nordisk A/S, Sanofi U.S; Research Support: Eli
Lilly and Company, Novo Nordisk A/S, Sanofi U.S.;
Speaker’s Bureau: AstraZeneca Pharmaceuticals LP,
Boehringer Ingelheim GmbH, Eli Lilly and Company,
Janssen Research & Development LLC, Merck Sharp
& Dohme, Mitsubishi Tanabe Pharma Corporation.,
Novo Nordisk A/S, Sanofi U.S.
Davis, Lori �������������������������������������������� Disclosed no conflict of interest.
Davis, Timothy M.E. ����������������������������� Advisory Panel: Merck Sharp & Dohme, Novo Nordisk
A/S; Research Support: Merck Sharp & Dohme, Novo
Nordisk A/S, Sanofi U.S., Takeda Pharmaceutical
Company Limited; Speaker’s Bureau: AstraZeneca,
Boehringer Ingelheim GmbH, Bristol-Myers Squibb, Eli
Lilly and Company, Janssen Pharmaceutical Companies
LB100
RELATIONSHIP/COMPANY
of Johnson & Johnson, Merck Sharp & Dohme,
Novartis Pharmaceuticals Corporation, Novo Nordisk
A/S, Takeda Pharmaceutical Company Limited.
Davis, Wendy A. ����������������������������������� Advisory Panel: Merck Sharp & Dohme, Novo Nordisk
A/S; Research Support: Merck Sharp & Dohme, Novo
Nordisk A/S, Sanofi U.S., Takeda Pharmaceutical
Company Limited; Speaker’s Bureau: AstraZeneca,
Boehringer Ingelheim GmbH, Bristol-Myers Squibb,
Eli Lilly and Company, Janssen Pharmaceutical
Companies of Johnson & Johnson, Merck Sharp
& Dohme, Novartis Pharmaceuticals Corporation,
Novo Nordisk A/S, Takeda Pharmaceutical Company
Limited.
Davis-Ajami, Mary L. ��������������������������� Disclosed no conflict of interest.
Davis-Richardson, Austin G. ���������������� Disclosed no conflict of interest.
Day, Samantha E. ��������������������������������� Disclosed no conflict of interest.
De Filippis, Elena A. ����������������������������� Disclosed no conflict of interest.
De Souza, Errol ������������������������������������� Board Member: Biodel Inc.; Employee: Biodel Inc.; Stock/
Shareholder: Biodel Inc.
de Toro-Martín, Juan ��������������������������� Disclosed no conflict of interest.
De Vito, Katerina M. ���������������������������� Disclosed no conflict of interest.
Deacon, Carolyn ����������������������������������� Advisory Panel: Bristol-Myers Squibb Company, Takeda
Pharmaceutical Company Limited; Other Relationship:
Merck Sharp & Dohme, Prosidion.
Deeg, Mark A. �������������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Deeney, Jude T. ������������������������������������ Disclosed no conflict of interest.
DeFronzo, Ralph A. ������������������������������� Disclosed no conflict of interest.
Dehennis, Andrew D. ��������������������������� Disclosed no conflict of interest.
DeJesus, Adam ������������������������������������ Disclosed no conflict of interest.
Del Gaudio, Daniela ����������������������������� Disclosed no conflict of interest.
Del Prato, Stefano �������������������������������� Disclosed no conflict of interest.
Delalleau, Nathalie ������������������������������ Disclosed no conflict of interest.
Della Bartola, Luca ������������������������������� Disclosed no conflict of interest.
Delpire, Eric ������������������������������������������ Disclosed no conflict of interest.
DeMarco, Vincent �������������������������������� Disclosed no conflict of interest.
Demirpence, Mustafa �������������������������� Disclosed no conflict of interest.
Demirpence, Nur ���������������������������������� Disclosed no conflict of interest.
Dempsey, Paddy C. ������������������������������� Disclosed no conflict of interest.
D’Eon, Stephanie ��������������������������������� Disclosed no conflict of interest.
DeSalvo, Daniel J. ������������������������������� Disclosed no conflict of interest.
Dibner, Charna �������������������������������������� Disclosed no conflict of interest.
DiMeglio, Linda A. ������������������������������� Disclosed no conflict of interest.
Ding, Eric L. ������������������������������������������ Disclosed no conflict of interest.
Dion, Stacy ������������������������������������������� Disclosed no conflict of interest.
Distelmaier, Klaus �������������������������������� Disclosed no conflict of interest.
Divoux, Adeline ������������������������������������ Disclosed no conflict of interest.
Do Bem, Daniela Amg �������������������������� Disclosed no conflict of interest.
Dobkin, Julie ���������������������������������������� Disclosed no conflict of interest.
Dolin, Paul �������������������������������������������� Employee: Takeda Development Centre Europe.
Donaghue, Kim C. �������������������������������� Disclosed no conflict of interest.
Donaldson, Julie ���������������������������������� Disclosed no conflict of interest.
Dong, Ying �������������������������������������������� Disclosed no conflict of interest.
Donnelly, Conor Brian �������������������������� Disclosed no conflict of interest.
Dopita, Dana ���������������������������������������� Other Relationship: Animas Corporation, Insulet
Corporation, Medtronic MiniMed, Inc., Tandem
Diabetes Care, Inc.
Dorchy, Harry R. ����������������������������������� Disclosed no conflict of interest.
Down, Susan ���������������������������������������� Advisory Panel: Abbott, Astra Zeneca, Boehringer
Ingelheim, Bristol-Myers Squibb, Eli Lilly, Novo
Nordisk, Johnson and Johnson, Sanofi; Board
Member: Forum for Injection Technique; Speaker’s
Bureau: OmniaMed, SB Communications.
Doyle, Carl �������������������������������������������� Employee: UCB Pharma.
Dragsbæk, Katrine ������������������������������� Disclosed no conflict of interest.
Drucker, Daniel J. ��������������������������������� Disclosed no conflict of interest.
Duffin, Kevin L. ������������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Duggirala, Ravindranath ���������������������� Disclosed no conflict of interest.
Dumenci, Levent ���������������������������������� Disclosed no conflict of interest.
Dunstan, David ������������������������������������� Disclosed no conflict of interest.
Duris, Christine ������������������������������������ Disclosed no conflict of interest.
Dushay, Jody ���������������������������������������� Advisory Panel: Janssen Pharmaceutical Companies of
Johnson & Johnson.
Dutta, Pinaki ����������������������������������������� Disclosed no conflict of interest.
Dutta, Sucharita ����������������������������������� Disclosed no conflict of interest.
Duvvuru, Suman ����������������������������������� Employee: Eli Lilly and Company.
Dyer, Thomas D. ����������������������������������� Disclosed no conflict of interest.
Dziadowicz, Helena M. ������������������������ Disclosed no conflict of interest.
Eberhard, Daniel ���������������������������������� Disclosed no conflict of interest.
Eckel, Juergen �������������������������������������� Research Support: Sanofi-Aventis Deutschland GmbH.
Edelman, Steven ���������������������������������� Advisory Panel: Boehringer Ingelheim, Eli Lilly; Speaker’s
Bureau: Boehringer Ingelheim, EIi Lilly.
AUTHOR
RELATIONSHIP/COMPANY
Edwards, Josh �������������������������������������� Disclosed no conflict of interest.
Edwards, Todd L. ���������������������������������� Disclosed no conflict of interest.
Efstratiou, Efthimia ������������������������������ Disclosed no conflict of interest.
Eglinger, Jan ����������������������������������������� Disclosed no conflict of interest.
Eguchi, Jun ������������������������������������������� Disclosed no conflict of interest.
Ehrich, Marion �������������������������������������� Disclosed no conflict of interest.
Eichner, Norbert ����������������������������������� Disclosed no conflict of interest.
Ekhlaspour, Laya ����������������������������������� Disclosed no conflict of interest.
El Khatib, Moustafa ����������������������������� Disclosed no conflict of interest.
El Ouaamari, Abdelfattah �������������������� Disclosed no conflict of interest.
El Youssef, Joseph ������������������������������� Disclosed no conflict of interest.
Eliasson, Lena �������������������������������������� Disclosed no conflict of interest.
Elks, Carrie M. �������������������������������������� Disclosed no conflict of interest.
Elsasser, Ulrich ������������������������������������� Employee: Boehringer Ingelheim GmbH.
El-Shahawy, Mohamed ������������������������ Advisory Panel: ZS Pharma, Inc.; Research Support:
Amgen Inc., Celgene Corporation, GlaxoSmithKline,
Sandoz, Inc., Takeda Pharmaceuticals U.S.A., Inc., ZS
Pharma, Inc.
Elston Lafata, Jennifer ������������������������� Disclosed no conflict of interest.
Erdos, Michael ������������������������������������� Disclosed no conflict of interest.
Eringa, Etto C. �������������������������������������� Disclosed no conflict of interest.
Erion, Karel A. �������������������������������������� Disclosed no conflict of interest.
Escrivá-Pons, Fernando ������������������������ Disclosed no conflict of interest.
Esko, Tonu �������������������������������������������� Disclosed no conflict of interest.
Estall, Jennifer L. ��������������������������������� Disclosed no conflict of interest.
Etwebi, Zienab A. ��������������������������������� Disclosed no conflict of interest.
Evans-Molina, Carmella ����������������������� Disclosed no conflict of interest.
Eze, Ikenna C. ��������������������������������������� Disclosed no conflict of interest.
Fain, Randi ������������������������������������������� Employee: Eisai Inc.
Fall, Caroline ���������������������������������������� Disclosed no conflict of interest.
Fang, Han ��������������������������������������������� Disclosed no conflict of interest.
Farabi, Sarah S. ������������������������������������ Disclosed no conflict of interest.
Farook, Vidya S. ������������������������������������ Disclosed no conflict of interest.
Federici, Adalberto ������������������������������� Disclosed no conflict of interest.
Federici, Giovanni �������������������������������� Disclosed no conflict of interest.
Feferman, Leo �������������������������������������� Disclosed no conflict of interest.
Feltbower, Richard ������������������������������� Disclosed no conflict of interest.
Feng, Bin ���������������������������������������������� Disclosed no conflict of interest.
Feng, Yue ���������������������������������������������� Employee: Merck & Co., Inc.
Fenske, Rachel ������������������������������������� Disclosed no conflict of interest.
Fenwick, Eva K. ������������������������������������ Disclosed no conflict of interest.
Ferguson-Smith, Anne ������������������������� Disclosed no conflict of interest.
Fernández-Millán, Elisa ����������������������� Disclosed no conflict of interest.
Ferron, Mathieu ����������������������������������� Disclosed no conflict of interest.
Fiad, Tarek M. ��������������������������������������� Disclosed no conflict of interest.
Figarola, James L. �������������������������������� Disclosed no conflict of interest.
Fink, Jeffrey C. ������������������������������������� Disclosed no conflict of interest.
Finlin, Brian S. �������������������������������������� Disclosed no conflict of interest.
Fiorina, Paolo ��������������������������������������� Disclosed no conflict of interest.
Fischer, Annelie ������������������������������������ Disclosed no conflict of interest.
Fish, Lisa ���������������������������������������������� Research Support: Eli Lilly and Company.
Fishbane, Steven N. ����������������������������� Advisory Panel: ZS Pharma, Inc.; Research Support: ZS
Pharma, Inc.
Fitch, Mark ������������������������������������������� Disclosed no conflict of interest.
Fitzgibbons, Timothy ���������������������������� Disclosed no conflict of interest.
Flannery, Clare A. ��������������������������������� Disclosed no conflict of interest.
Flynn, Angela C. ����������������������������������� Disclosed no conflict of interest.
Fodor, William �������������������������������������� Disclosed no conflict of interest.
Fogelfeld, Leon ������������������������������������� Research Support: AstraZeneca Pharmaceuticals LP, Bayer
HealthCare, Boehringer Ingelheim Pharmaceuticals,
Inc., Bristol-Myers Squibb Company, Calibra,
Genkyotex, GlaxoSmithKline, Grifols USA, LLC, Merck
& Co., Inc., Sanofi U.S.
Forisch, Michael ����������������������������������� Disclosed no conflict of interest.
Formentini, Laura ��������������������������������� Disclosed no conflict of interest.
Fourcaudot, Marcel ������������������������������ Disclosed no conflict of interest.
Fowler, Robert �������������������������������������� Employee: Truven Health Analytics.
Fox, Caroline S. ������������������������������������ Disclosed no conflict of interest.
Frank, Claudio �������������������������������������� Disclosed no conflict of interest.
Franks, Paul W. ������������������������������������ Disclosed no conflict of interest.
Franz, Wolfgang-Michael ��������������������� Speaker’s Bureau: MSD.
Fraser, Ian ��������������������������������������������� Disclosed no conflict of interest.
Frayling, Timothy M. ���������������������������� Disclosed no conflict of interest.
Frenkel, Dan ����������������������������������������� Disclosed no conflict of interest.
Friedländer, Marc ��������������������������������� Disclosed no conflict of interest.
Frois, Christian ������������������������������������� Consultant: Intarcia Therapeutics, Inc.
Frokiaer, Jørgen ������������������������������������ Disclosed no conflict of interest.
Fryburg, David A. ���������������������������������� Stock/Shareholder: Pfizer Inc.
Fu, Alex Z. �������������������������������������������� Consultant: Truven Health Analytics, AstraZeneca.
Fu, Lizhi ������������������������������������������������ Disclosed no conflict of interest.
Fu, Yanyun �������������������������������������������� Disclosed no conflict of interest.
Fuentes, Blanca ������������������������������������ Disclosed no conflict of interest.
Fukuda, Takuya ������������������������������������� Disclosed no conflict of interest.
LB101
AUTHOR DISCLOSURE
AUTHOR
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
Fukui, Michiaki ������������������������������������� Disclosed no conflict of interest.
Fung, Anne ������������������������������������������� Employee: Genentech, Inc.
Fusong, Jiang ��������������������������������������� Disclosed no conflict of interest.
Gaglia, Jason L. ����������������������������������� Disclosed no conflict of interest.
Galli-Tsinopoulou, Assimina ���������������� Disclosed no conflict of interest.
Gamerman, Victoria ����������������������������� Employee: Boehringer Ingelheim Pharmaceuticals Inc.
Gandomani, Ben S. ������������������������������ Disclosed no conflict of interest.
Gandour, Richard ���������������������������������� Disclosed no conflict of interest.
Gang, Xiaokun �������������������������������������� Disclosed no conflict of interest.
Gannon, Maureen A. ���������������������������� Disclosed no conflict of interest.
Garcia Fuentes, Eduardo ���������������������� Disclosed no conflict of interest.
Garcia, Arturo ��������������������������������������� Employee: Dexcom, Inc.
Garcia-Arnes, Juan ������������������������������ Disclosed no conflict of interest.
Garcia-Escobar, Eva ������������������������������ Disclosed no conflict of interest.
Garcia-Sanchez, Ricardo ���������������������� Employee: AstraZeneca Pharmaceuticals LP, self.
Garcia-Serrano, Sara ��������������������������� Disclosed no conflict of interest.
Garg, Satish K. ������������������������������������� Consultant: Medtronic, Inc., Eli Lilly and Company,
Roche USA, Sanofi U.S.; Research Support: Eli Lilly
and Company, Halozyme Therapeutics, Lexicon
Pharmaceuticals, Inc., MannKind Corporation, Merck
& Co., Inc., Novo Nordisk Inc., Sanofi U.S.
Garhyan, Parag ������������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company, Eli Lilly and Company.
Garlish, Rachel ������������������������������������� Employee: UCB Pharma.
Gaziano, J. Michael ����������������������������� Research Support: Pfizer Inc.
Gebauer, Mathias ��������������������������������� Employee: Sanofi U.S.; Stock/Shareholder: Sanofi U.S.
Gee, Kyuhoon ��������������������������������������� Disclosed no conflict of interest.
Genieser, Hans-G ��������������������������������� Disclosed no conflict of interest.
Genovese, Maria Ines �������������������������� Disclosed no conflict of interest.
Genter, Pauline ������������������������������������� Disclosed no conflict of interest.
Gentile, Sandro ������������������������������������ Board Member: Sanofi; Consultant: Roche Diagnostics.
Gerbase, Margaret ������������������������������� Disclosed no conflict of interest.
Geyer, Susan ���������������������������������������� Disclosed no conflict of interest.
Ghanian, Sheila ������������������������������������ Disclosed no conflict of interest.
Ghanim, Husam ������������������������������������ Disclosed no conflict of interest.
Ghannam, Ameen �������������������������������� Employee: AstraZeneca Pharmaceuticals LP.
Ghorbani, Tahereh �������������������������������� Disclosed no conflict of interest.
Ghosh, Pamela ������������������������������������� Disclosed no conflict of interest.
Ghosh, Sujoy ���������������������������������������� Advisory Panel: Zydus Cadila.
Giacaglia, Luciano �������������������������������� Disclosed no conflict of interest.
Giampietro, Ottavio ������������������������������ Disclosed no conflict of interest.
Gilbert, Matthew ��������������������������������� Disclosed no conflict of interest.
Gilgen, Emily ���������������������������������������� Other Relationship: Animas Corporation, Asante
Solutions, Inc., Insulet Corporation, Medtronic
MiniMed, Inc., Roche Diagnostics, Tandem Diabetes
Care, Inc.
Giovenale, Sharon �������������������������������� Disclosed no conflict of interest.
Glicklich, Alan �������������������������������������� Employee: Arena.
Glynn, Robert J. ����������������������������������� Disclosed no conflict of interest.
Gmyr, Valéry ����������������������������������������� Disclosed no conflict of interest.
Gnys, Piotr �������������������������������������������� Disclosed no conflict of interest.
Godfrey, Keith M. ��������������������������������� Research Support: Abbott Nutrition, Danone, Inc., Nestec.
Goldberg, Ronald ��������������������������������� Disclosed no conflict of interest.
Gomez, Ana Maria ������������������������������� Research Support: Novartis Pharmaceuticals Corporation;
Speaker’s Bureau: AstraZeneca, Bristol-Myers Squibb,
Eli Lilly and Company, Medtronic MiniMed, Inc., Novo
Nordisk Inc.
Gomez-Perez, Francisco J. ������������������� Disclosed no conflict of interest.
Gonçalves, Gabriel H.M. ���������������������� Disclosed no conflict of interest.
Gonçalves, Nadmy A.Z. ������������������������ Disclosed no conflict of interest.
Gonçalves, Rita de Cássia R. ��������������� Disclosed no conflict of interest.
Gonzalez, Noemi ���������������������������������� Disclosed no conflict of interest.
González-Ortiz, Manuel ������������������������ Disclosed no conflict of interest.
Gonzalo, Montserrat ���������������������������� Disclosed no conflict of interest.
Gopala, Aralakuppe S. ������������������������� Disclosed no conflict of interest.
Gordon, Tom ����������������������������������������� Disclosed no conflict of interest.
Gorgel, Ahmet �������������������������������������� Disclosed no conflict of interest.
Göring, Harald H. ��������������������������������� Disclosed no conflict of interest.
Gormsen, Lars C. ���������������������������������� Disclosed no conflict of interest.
Gottlieb, Peter A. ��������������������������������� Disclosed no conflict of interest.
Gottlieb, Rebecca ��������������������������������� Employee: Medtronic MiniMed, Inc.; Stock/Shareholder:
Medtronic, Inc.
Gowtham, Raj �������������������������������������� Disclosed no conflict of interest.
Grabmaier, Ulrich ��������������������������������� Disclosed no conflict of interest.
Grady, Mike ������������������������������������������ Employee: LifeScan, Inc.
Graff, Emily C. �������������������������������������� Disclosed no conflict of interest.
Graff, Marielisa ������������������������������������ Disclosed no conflict of interest.
Graff, Misa ������������������������������������������� Disclosed no conflict of interest.
Grarup, Niels ���������������������������������������� Disclosed no conflict of interest.
Greeley, Siri Atma W. �������������������������� Disclosed no conflict of interest.
Greenbaum, Carla J. ���������������������������� Disclosed no conflict of interest.
Greenfield, Jerry R. ������������������������������ Disclosed no conflict of interest.
Greenway, Frank ���������������������������������� Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Greulich, Sabrina ��������������������������������� Disclosed no conflict of interest.
Griffith, Julie ���������������������������������������� Disclosed no conflict of interest.
Grohmann-Izay, Barbara J. ������������������� Disclosed no conflict of interest.
Groh-Wargo, Sharon ���������������������������� Disclosed no conflict of interest.
Grosman, Benyamin ����������������������������� Employee: Medtronic MiniMed, Inc.
Gross, Myron ���������������������������������������� Disclosed no conflict of interest.
Guan, Hong-Ping ���������������������������������� Disclosed no conflict of interest.
Guan, Meiping ������������������������������������� Disclosed no conflict of interest.
Gudiksen, Anders ��������������������������������� Disclosed no conflict of interest.
Guerci, Bruno ��������������������������������������� Advisory Panel: Abbott, Boehringer Ingelheim, Eli Lilly,
Novartis; Board Member: AstraZeneca, Bristol-Myers
Squibb, GlaxoSmithKline, Novo Nordisk, Roche
Diagnostic, Sanofi; Research Support: Dinno Santé,
Eli Lilly, Medtronic, MSD, Novartis, Novo Nordisk,
Janssen, Johnson & Johnson, Sanofi, Vitalaire.
Guertin, David A. ���������������������������������� Disclosed no conflict of interest.
Guhl, Anna ������������������������������������������� Disclosed no conflict of interest.
Guimaraes, Sergio B. ��������������������������� Disclosed no conflict of interest.
Gune, Shamika ������������������������������������� Employee: Genentech, Inc.
Guo, Hui ����������������������������������������������� Disclosed no conflict of interest.
Guo, Xiaohui ����������������������������������������� Disclosed no conflict of interest.
Gutierrez, Absalon ������������������������������� Disclosed no conflict of interest.
Gutierrez-Repiso, Carolina ������������������� Disclosed no conflict of interest.
Ha, Kyoung Soo ������������������������������������ Disclosed no conflict of interest.
Haas, Joseph V. ������������������������������������ Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Haas, Mary ������������������������������������������� Disclosed no conflict of interest.
Hackett, Geoffrey I. ������������������������������ Research Support: Bayer HealthCare, Bayer.
Hadjadj, Samy �������������������������������������� Board Member: AstraZeneca, Bristol-Myers Squibb,
Sanofi U.S.; Consultant: AstraZeneca, Boehringer
Ingelheim GmbH, Bristol-Myers Squibb, Eli Lilly and
Company, Novo Nordisk Inc., Sanofi U.S., Servier;
Speaker’s Bureau: AstraZeneca, Boehringer Ingelheim
GmbH, Bristol-Myers Squibb, Eli Lilly and Company,
Novo Nordisk Inc., Servier.
Hage, Camilla ��������������������������������������� Disclosed no conflict of interest.
Haghiac, Maricela �������������������������������� Disclosed no conflict of interest.
Hagopian, William A. ��������������������������� Disclosed no conflict of interest.
Hailu, Hanna ���������������������������������������� Employee: UCB Pharma.
Halder, Louise ��������������������������������������� Disclosed no conflict of interest.
Hall, Christopher E. ������������������������������ Disclosed no conflict of interest.
Hall, Keneth ����������������������������������������� Disclosed no conflict of interest.
Hallmans, Göran ���������������������������������� Disclosed no conflict of interest.
Halperin, Jose �������������������������������������� Stock/Shareholder: Mellitus, LLC.
Han, Bing ���������������������������������������������� Disclosed no conflict of interest.
Han, Byoung Geun ������������������������������� Disclosed no conflict of interest.
Han, Jing ���������������������������������������������� Disclosed no conflict of interest.
Han, Kyung Ah ������������������������������������� Disclosed no conflict of interest.
Han, OakPil ������������������������������������������� Disclosed no conflict of interest.
Han, Sang Youb ������������������������������������ Disclosed no conflict of interest.
Han, Weiping ��������������������������������������� Disclosed no conflict of interest.
Han, Xinping ����������������������������������������� Disclosed no conflict of interest.
Hanas, Ragnar �������������������������������������� Advisory Panel: Abbott, Lillly; Consultant: BMC,
Medtronic, NovoNordisk; Speaker’s Bureau: Abbott,
Menarini, Roche.
Hanefeld, Markolf �������������������������������� Advisory Panel: Bristol-Myers Squibb Company,
GlaxoSmithKline, Sanofi, Takeda Pharmaceuticals
USA, Inc.; Speaker’s Bureau: Bayer HealthCare
LLC, Eli Lilly and Company, GlaxoSmithKline, Roche
Pharmaceuticals, Sanofi, Takeda Pharmaceuticals
USA, Inc.
Hanis, Craig L. �������������������������������������� Disclosed no conflict of interest.
Hanna, Paul ������������������������������������������ Disclosed no conflict of interest.
Hannpu, Sarah ������������������������������������� Disclosed no conflict of interest.
Hanseman, Dennis ������������������������������� Disclosed no conflict of interest.
Hansen, Lærke S. ��������������������������������� Disclosed no conflict of interest.
Hansen, Lars ���������������������������������������� Employee: Bristol-Myers Squibb Company, self.
Hansen, Mads Bau ������������������������������� Disclosed no conflict of interest.
Hansen, Troels K. ��������������������������������� Disclosed no conflict of interest.
Hansraj, Patil A. ����������������������������������� Disclosed no conflict of interest.
Hantel, Stefan �������������������������������������� Employee: Boehringer Ingelheim GmbH.
Hao, Gaimei ����������������������������������������� Disclosed no conflict of interest.
Hao, Pindan ������������������������������������������ Disclosed no conflict of interest.
Hara, Takuya ����������������������������������������� Employee: Kowa Pharmaceuticals.
Hardy, Thomas A. ��������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Häring, Hans-Ulrich ������������������������������ Disclosed no conflict of interest.
Harris, Stuart ���������������������������������������� Disclosed no conflict of interest.
Harrison, Lindsay ��������������������������������� Disclosed no conflict of interest.
Harsha, Krishna Reddy ������������������������� Disclosed no conflict of interest.
Hartig, Sean M. ������������������������������������ Disclosed no conflict of interest.
Hartmann, Bolette �������������������������������� Disclosed no conflict of interest.
Hartmann, Thorsten ����������������������������� Disclosed no conflict of interest.
LB102
RELATIONSHIP/COMPANY
Hastings, Stephanie M. ����������������������� Disclosed no conflict of interest.
Hauguel-de Mouzon, Sylvie ����������������� Disclosed no conflict of interest.
Hausser, Jean ��������������������������������������� Disclosed no conflict of interest.
Haw, J. Sonya �������������������������������������� Disclosed no conflict of interest.
Hayden, Melvin ������������������������������������ Disclosed no conflict of interest.
Hayek, Salim S. ������������������������������������ Disclosed no conflict of interest.
Hayes, Louise ��������������������������������������� Disclosed no conflict of interest.
Hazra, Daya K. �������������������������������������� Advisory Panel: USV.
He, Jie �������������������������������������������������� Disclosed no conflict of interest.
He, Ling ������������������������������������������������ Disclosed no conflict of interest.
He, Qin ������������������������������������������������� Disclosed no conflict of interest.
He, Yan Ling ����������������������������������������� Employee: Novartis Pharmaceuticals Corporation.
Heard-Costa, Nancy L. ������������������������� Disclosed no conflict of interest.
Heberlein, Emily ����������������������������������� Disclosed no conflict of interest.
Heier, Jeffrey S. ����������������������������������� Consultant: Aerpio, Allergan, Inc., Genentech, Inc.,
Kala Pharmaceuticals, Regeneron Pharmaceuticals,
Inc.; Research Support: Genentech, Inc., Kala
Pharmaceuticals, Ophthotech, Regeneron
Pharmaceuticals, Inc., Stealth Biotherapeutics.
Heinemann, Lutz ���������������������������������� Advisory Panel: Biodel Inc., Eli Lilly and Company,
Halozyme Therapeutics, Novo Nordisk, Sanofi;
Employee: Science & Co.; Other Relationship: Profil
Institut for Clinical Research, Profil Institut für
Stoffwechselforschung.
Heintjes, Edith M. �������������������������������� Other Relationship: Takeda Development Centre Europe.
Heise, Tim �������������������������������������������� Disclosed no conflict of interest.
Heizer, Patrick ��������������������������������������� Disclosed no conflict of interest.
Hejna, Jeanne �������������������������������������� Disclosed no conflict of interest.
Heller, Simon ���������������������������������������� Advisory Panel: AstraZeneca; Consultant: Eli Lilly, Novo
Nordisk, Takeda; Speaker’s Bureau: Boeringher
Ingelheim, Eli Lilly, Novo Nordisk, Takeda.
Hellerstein, Marc ��������������������������������� Disclosed no conflict of interest.
Henao, Diana ��������������������������������������� Disclosed no conflict of interest.
Hendrieckx, Christel ����������������������������� Disclosed no conflict of interest.
Henry, Robert R. ����������������������������������� Advisory Panel: Amgen Inc., AstraZeneca Pharmaceuticals
LP, Boehringer Ingelheim GmbH, Bristol-Myers
Squibb Company, Elcelyx Therapeutics, Inc., Gilead,
Intarcia Therapeutics, Inc., Janssen Pharmaceutical
Companies of Johnson & Johnson, Merck & Co., Inc.,
Novo Nordisk Inc., Sanofi U.S., Vivus Inc.; Consultant:
Alere, Boehringer Ingelheim GmbH, Clin Met, Eisai
Co., Ltd., Gilead, Intarcia Therapeutics, Inc., Isis
Pharmaceuticals, Inc., Janssen Pharmaceutical
Companies of Johnson & Johnson, Sanofi U.S.;
Research Support: Eli Lilly and Company, Hitachi,
Sanofi U.S., Viacyte.
Herberg, Friedrich W. ��������������������������� Disclosed no conflict of interest.
Herman, William H. ����������������������������� Disclosed no conflict of interest.
Hernández, Antonio ����������������������������� Disclosed no conflict of interest.
Herranz, Lucrecia ��������������������������������� Disclosed no conflict of interest.
Herrlich, Andreas ��������������������������������� Disclosed no conflict of interest.
Highland, Heather M. �������������������������� Disclosed no conflict of interest.
Hillard, Mallory ������������������������������������ Disclosed no conflict of interest.
Hillman, Natalia ����������������������������������� Disclosed no conflict of interest.
Hingst, Janne R. ����������������������������������� Disclosed no conflict of interest.
HIrate, Mitsuru ������������������������������������� Disclosed no conflict of interest.
Hirschhorn, Joel N. ������������������������������ Disclosed no conflict of interest.
Hirshberg, Boaz ������������������������������������ Employee: AstraZeneca Pharmaceuticals LP.
Hissa, Marcelo R.N. ����������������������������� Disclosed no conflict of interest.
Hissa, Miguel N. ���������������������������������� Disclosed no conflict of interest.
Hmaguchi, Masahide ��������������������������� Disclosed no conflict of interest.
Hoch, Emily ������������������������������������������ Disclosed no conflict of interest.
Hoevenaars, Femke M.P. ���������������������� Disclosed no conflict of interest.
Hoffmann, Ellen ����������������������������������� Disclosed no conflict of interest.
Hoffmann-Petersen, Ingeborg T. ���������� Disclosed no conflict of interest.
Hoidal, Mallary ������������������������������������ Disclosed no conflict of interest.
Holland, William ���������������������������������� Disclosed no conflict of interest.
Holmes-Truscott, Elizabeth ������������������ Disclosed no conflict of interest.
Holst, Jens Juul ����������������������������������� Consultant: Merck Sharp & Dohme, Novartis
Pharmaceuticals Corporation, Novo Nordisk A/S,
Roche USA; Other Relationship: GlaxoSmithKline,
Merck Sharp & Dohme, Novo Nordisk A/S.
Holt, Charlotte B. ��������������������������������� Disclosed no conflict of interest.
Holz, George G. ������������������������������������ Disclosed no conflict of interest.
Homann, Dirk ��������������������������������������� Disclosed no conflict of interest.
Hompesch, Marcus ������������������������������ Employee: Profil Institute for Clinical Research, Inc.;
Stock/Shareholder: Profil Institute for Clinical
Research, Inc.
Hong, Biling ������������������������������������������ Disclosed no conflict of interest.
Hong, Suntaek �������������������������������������� Disclosed no conflict of interest.
Honig, Lee B. ���������������������������������������� Disclosed no conflict of interest.
Hontecillas, Raquel ������������������������������ Disclosed no conflict of interest.
Hooven, Jayde T. ���������������������������������� Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Horne, David ���������������������������������������� Disclosed no conflict of interest.
Horsburgh, Jodie C. ����������������������������� Disclosed no conflict of interest.
Horton, Edward S. �������������������������������� Disclosed no conflict of interest.
Hoshina, Sari ���������������������������������������� Disclosed no conflict of interest.
Hota, Debasish ������������������������������������� Disclosed no conflict of interest.
Hotamisligil, Gökhan S. ����������������������� Research Support: UCB Pharma.
Hoti, Fabian ������������������������������������������ Employee: EPID Research performs financially supported
studies for several pharmaceutical companies
including Takeda Development Centre Europe.
Hou, Liqiong ����������������������������������������� Disclosed no conflict of interest.
Houweling, Leanne ������������������������������ Employee: Takeda Development Centre Europe.
Howard, Andrew ���������������������������������� Employee: Merck & Co., Inc.
Howells, Louise ������������������������������������ Employee: UCB Pharma.
Hsia, Daniel S. ������������������������������������� Disclosed no conflict of interest.
Hsiao, Jong-Kai ������������������������������������ Disclosed no conflict of interest.
Hsu, Chi-Yuan ��������������������������������������� Disclosed no conflict of interest.
Hu He, Kaihui ��������������������������������������� Disclosed no conflict of interest.
Hu, Frank B. ������������������������������������������ Disclosed no conflict of interest.
Hu, Ling ������������������������������������������������ Disclosed no conflict of interest.
Hu, Shirley L. ���������������������������������������� Disclosed no conflict of interest.
Hu, Yanjin ��������������������������������������������� Disclosed no conflict of interest.
Hu, Ying Ying ���������������������������������������� Disclosed no conflict of interest.
Huang, Tao ������������������������������������������� Disclosed no conflict of interest.
Huang, Tian Lian ���������������������������������� Disclosed no conflict of interest.
Huang, Zhe ������������������������������������������� Disclosed no conflict of interest.
Hughes, Kristen ������������������������������������ Research Support: Medtronic MiniMed, Inc.
Hughes, William E. ������������������������������ Disclosed no conflict of interest.
Huh, Yeamin ����������������������������������������� Disclosed no conflict of interest.
Hutchens, Troy �������������������������������������� Disclosed no conflict of interest.
Hutfless, Susan ������������������������������������ Disclosed no conflict of interest.
Huyghe, Jeroen ������������������������������������ Disclosed no conflict of interest.
Hwang, Janice J. ��������������������������������� Disclosed no conflict of interest.
Iacobellis, Gianluca ������������������������������ Disclosed no conflict of interest.
Ibrahim, Mahmoud ������������������������������� Disclosed no conflict of interest.
Ikeda, Yasuhiro ������������������������������������� Disclosed no conflict of interest.
Im, Hae Kyung �������������������������������������� Disclosed no conflict of interest.
Im, Kyung Ah ���������������������������������������� Disclosed no conflict of interest.
Im, Seung-Soon ������������������������������������ Disclosed no conflict of interest.
Imai, Yumi ��������������������������������������������� Disclosed no conflict of interest.
Imboden, Medea ���������������������������������� Disclosed no conflict of interest.
Imig, John D. ���������������������������������������� Disclosed no conflict of interest.
Innes, Karen ����������������������������������������� Disclosed no conflict of interest.
Inoue, Noriyuki ������������������������������������� Employee: Kowa Pharmaceuticals.
Inouye, Karen ��������������������������������������� Disclosed no conflict of interest.
Ioacara, Sorin ��������������������������������������� Disclosed no conflict of interest.
Ipp, Eli �������������������������������������������������� Research Support: Bristol-Myers Squibb Company,
California Community Foundation, Novo Nordisk Inc.
Iqbal, Nayyar ���������������������������������������� Employee: Bristol-Myers Squibb Company.
Irving, Brian ������������������������������������������ Disclosed no conflict of interest.
Itescu, Silviu ����������������������������������������� Employee: Mesoblast Inc.
Iwasaki, Yorihiro ���������������������������������� Disclosed no conflict of interest.
Iwata, Hiroshi ��������������������������������������� Disclosed no conflict of interest.
Iyoha, Emannuel ����������������������������������� Disclosed no conflict of interest.
Jackson, Anne �������������������������������������� Disclosed no conflict of interest.
Jackson, Jeffrey A. ������������������������������ Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Jackson, Michael ��������������������������������� Disclosed no conflict of interest.
Jacober, Scott J. ���������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Jacobs, Peter G. ����������������������������������� Board Member: Pacific Diabetes Technologies; Research
Support: National Institute of Diabetes and Digestive
and Kidney Diseases; Stock/Shareholder: Pacific
Diabetes Technologies.
Jacobus Ambuludi, Egon J. ����������������� Disclosed no conflict of interest.
Jaffar, Amina ���������������������������������������� Disclosed no conflict of interest.
Jagannath, Madanahalli R. ����������������� Disclosed no conflict of interest.
Jain, Deepak ���������������������������������������� Disclosed no conflict of interest.
Jaiswal, Ashok D. �������������������������������� Employee: Cadila Healthcare Ltd.
Jakobsen, Steen ���������������������������������� Disclosed no conflict of interest.
Jakoby, Michael G. ������������������������������ Speaker’s Bureau: Sanofi U.S.
James, David E ������������������������������������ Disclosed no conflict of interest.
Janes, Jonathan M. ����������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Janka-Zires, Marcela ��������������������������� Disclosed no conflict of interest.
Januszewski, Andrzej S. ���������������������� Disclosed no conflict of interest.
Jasper, Susan ��������������������������������������� Disclosed no conflict of interest.
Jastroch, Martin ���������������������������������� Disclosed no conflict of interest.
Jean-Baptiste, Eddy ����������������������������� Disclosed no conflict of interest.
Jelaska, Ante ��������������������������������������� Employee: Boehringer Ingelheim Pharmaceuticals, Inc.
Jenkins, Alicia J. ���������������������������������� Research Support: Abbott, Medtronic, Inc., Sanofi Aventis.
Jenkinson, Christopher P. ��������������������� Disclosed no conflict of interest.
Jensen, Jonas B. ���������������������������������� Disclosed no conflict of interest.
Jensen, Michael D. ������������������������������ Disclosed no conflict of interest.
LB103
AUTHOR DISCLOSURE
AUTHOR
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
Jeon, Jae-Han �������������������������������������� Disclosed no conflict of interest.
Jeon, Justin Y. �������������������������������������� Disclosed no conflict of interest.
Jeong, Kyung Hwan ����������������������������� Disclosed no conflict of interest.
Jessen, Niels ��������������������������������������� Disclosed no conflict of interest.
Ji, Linong ���������������������������������������������� Consultant: Bayer HealthCare, Bristol-Myers Squibb
Company, Eli Lilly and Company, Merck & Co., Inc.,
Novartis Corporation, Novo Nordisk Inc., Roche USA,
Sanofi U.S.; Research Support: Roche USA, Sanofi U.S.
Jia, Weiping ����������������������������������������� Disclosed no conflict of interest.
Jiang, Hui ��������������������������������������������� Disclosed no conflict of interest.
Jiang, Jenny ����������������������������������������� Disclosed no conflict of interest.
Jianjun, Liu ������������������������������������������� Disclosed no conflict of interest.
Jiao, Ping ��������������������������������������������� Disclosed no conflict of interest.
Jin, Shi ������������������������������������������������� Disclosed no conflict of interest.
Jo, Young-II ������������������������������������������ Disclosed no conflict of interest.
Joglekar, Charudatta ���������������������������� Disclosed no conflict of interest.
Johnson, Jennal L. ������������������������������� Employee: Eli Lilly and Company.
Johnson, Matthew L. ��������������������������� Disclosed no conflict of interest.
Johnson, William D. ���������������������������� Disclosed no conflict of interest.
Johnston, Stephen ������������������������������� Employee: Truven Health Analytics.
Jones, Dean P. �������������������������������������� Disclosed no conflict of interest.
Jose, Aimee ����������������������������������������� Disclosed no conflict of interest.
Joshi, Shashank R. ������������������������������� Consultant: Bayer Zydus Pharma, Zydus Cadila; Speaker’s
Bureau: Abbott, Emcure, Franco Indian, Johnson &
Johnson, Marico, MSD, Novartis, Novo Nordisk, PHFI,
Ranbaxy, Roche, Sanofi, USV.
Joshi, Suyog ����������������������������������������� Disclosed no conflict of interest.
Joshipura, Kaumudi J. ������������������������� Disclosed no conflict of interest.
Jouvet, Nathalie ���������������������������������� Disclosed no conflict of interest.
Juarez-Comboni, Sonia C. �������������������� Disclosed no conflict of interest.
Judd, Robert L. ������������������������������������� Disclosed no conflict of interest.
Jung, II-Hoon ���������������������������������������� Disclosed no conflict of interest.
Jung, Yun-Seung ���������������������������������� Disclosed no conflict of interest.
Jurczak, Michael J. ������������������������������ Disclosed no conflict of interest.
Justice, Anne E. ����������������������������������� Disclosed no conflict of interest.
Kabadi, Udaya M. �������������������������������� Advisory Panel: Sanofi U.S.; Speaker’s Bureau: Sanofi U.S.
Kabra, Uma D. �������������������������������������� Disclosed no conflict of interest.
Kadener, Sebastian ������������������������������ Disclosed no conflict of interest.
Kady, Jamie ������������������������������������������ Disclosed no conflict of interest.
Kahn, Barbara B. ���������������������������������� Disclosed no conflict of interest.
Kahn, C. Ronald ������������������������������������ Disclosed no conflict of interest.
Kahn, Jonathan ������������������������������������ Disclosed no conflict of interest.
Kalsekar, Iftekhar ��������������������������������� Employee: AstraZeneca Pharmaceuticals LP.
Kamenov, Zdravko �������������������������������� Disclosed no conflict of interest.
Kandror, Konstantin V. �������������������������� Disclosed no conflict of interest.
Kane, Penelope ������������������������������������ Disclosed no conflict of interest.
Kaneko, Shizuka ����������������������������������� Advisory Panel: Astellas Pharma US, Inc., Novo Nordisk
Inc., Taisho Pharmaceutical Co., Ltd., Takeda
Pharmaceutical Company Limited; Speaker’s Bureau:
Astellas Pharma US, Inc., AstraZeneca, Bristol-Myers
Squibb, Eli Lilly Japan K.K., Johnson & Johnson,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Novo Nordisk Inc.,
Sumimoto Dainippon Pharma Co., Ltd., Taisho
Pharmaceutical Co., Ltd., Takeda Pharmaceutical
Company Limited.
Kaneto, Hideaki ������������������������������������ Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Daiichi-Sankyo Co., Ltd., Eli
Lilly Japan K.K., Kissei Pharmaceutical Co., Ltd.,
Kowa Pharmaceuticals, Merck Sharp & Dohme,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Novo Nordisk Inc., Ono
Pharmaceutical Co., Ltd., Sanofi U.S., Shionogi Inc.,
Takeda Pharmaceutical Company Limited.
Kang, Dong-Woo ���������������������������������� Disclosed no conflict of interest.
Kang, Jahoon ��������������������������������������� Disclosed no conflict of interest.
Kang, Kyung Koo ���������������������������������� Disclosed no conflict of interest.
Kang, Shin-Wook ��������������������������������� Disclosed no conflict of interest.
Karaderi, Tugce ������������������������������������ Disclosed no conflict of interest.
Karaliota, Sevasti ��������������������������������� Disclosed no conflict of interest.
Karalis, Katia ���������������������������������������� Disclosed no conflict of interest.
Karsdal, Morten ����������������������������������� Stock/Shareholder: Nordic Bioscience.
Kasid, Natasha ������������������������������������� Disclosed no conflict of interest.
Kattah, William ������������������������������������ Disclosed no conflict of interest.
Katz, Laurence B. ��������������������������������� Employee: LifeScan, Inc.
Kaufholz, Melanie �������������������������������� Disclosed no conflict of interest.
Kaufman, Francine ������������������������������� Employee: Medtronic MiniMed, Inc.; Stock/Shareholder:
Medtronic, Inc.
Kawaguchi, Yasushi ����������������������������� Disclosed no conflict of interest.
Kawaguchi, Yoshiya ����������������������������� Disclosed no conflict of interest.
Kawamoto, Manabu ���������������������������� Disclosed no conflict of interest.
Kazakos, Kyriakos �������������������������������� Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Ke, Bilun ����������������������������������������������� Disclosed no conflict of interest.
Keady, Joyce ���������������������������������������� Disclosed no conflict of interest.
Keçik, Onur ������������������������������������������� Disclosed no conflict of interest.
Keenan, Hillary A. �������������������������������� Disclosed no conflict of interest.
Kefaloyianni, Eirini ������������������������������� Disclosed no conflict of interest.
Keith-Hynes, Patrick ����������������������������� Disclosed no conflict of interest.
Kelkar, Rohini ��������������������������������������� Disclosed no conflict of interest.
Kelley, David E. ������������������������������������ Employee: Merck & Co., Inc.
Kelly, Ronan P. �������������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Kemnitz, Joseph W. ����������������������������� Disclosed no conflict of interest.
Kemppainen, Kaisa M. ������������������������� Disclosed no conflict of interest.
Kennedy, Christopher ��������������������������� Disclosed no conflict of interest.
Kern, Philip A. �������������������������������������� Disclosed no conflict of interest.
Kernan, Kelly ���������������������������������������� Disclosed no conflict of interest.
Kerr, Peter G. ���������������������������������������� Advisory Panel: Fresenius, Amgen Inc.
Kerr-Conte, Julie ���������������������������������� Disclosed no conflict of interest.
Kesireddy, Veena ���������������������������������� Disclosed no conflict of interest.
Khai Koon, Heng ���������������������������������� Disclosed no conflict of interest.
Khazaezadeh, Nina ������������������������������ Disclosed no conflict of interest.
Khedkar, Aditya ������������������������������������ Disclosed no conflict of interest.
Khowaja, Ameer ���������������������������������� Research Support: Eli Lilly and Company.
Kibbey, Richard G. �������������������������������� Disclosed no conflict of interest.
Kiens, Bente ����������������������������������������� Disclosed no conflict of interest.
Kil, Siyoen �������������������������������������������� Disclosed no conflict of interest.
Kim, Bong-Jo ���������������������������������������� Disclosed no conflict of interest.
Kim, Dong-II ����������������������������������������� Disclosed no conflict of interest.
Kim, Dong-Wook ���������������������������������� Disclosed no conflict of interest.
Kim, Doo Man �������������������������������������� Disclosed no conflict of interest.
Kim, In Joo ������������������������������������������� Disclosed no conflict of interest.
Kim, Jae Bum ��������������������������������������� Disclosed no conflict of interest.
Kim, Jihye �������������������������������������������� Disclosed no conflict of interest.
Kim, Ji-Young ��������������������������������������� Disclosed no conflict of interest.
Kim, Jongoh ����������������������������������������� Disclosed no conflict of interest.
Kim, Joon Young ���������������������������������� Disclosed no conflict of interest.
Kim, Jung Seok ������������������������������������ Disclosed no conflict of interest.
Kim, Mi-Kyung ������������������������������������� Disclosed no conflict of interest.
Kim, Nam-Ho ���������������������������������������� Disclosed no conflict of interest.
Kim, Nam-Kyu �������������������������������������� Disclosed no conflict of interest.
Kim, Nan Hee ��������������������������������������� Disclosed no conflict of interest.
Kim, Pankyung �������������������������������������� Disclosed no conflict of interest.
Kim, Sin Gon ���������������������������������������� Disclosed no conflict of interest.
Kim, Soohyun Park ������������������������������� Disclosed no conflict of interest.
Kim, Sung Gyun ������������������������������������ Disclosed no conflict of interest.
Kim, Sung-Woo ������������������������������������ Disclosed no conflict of interest.
Kim, Tae Hyoung ���������������������������������� Disclosed no conflict of interest.
Kim, Tae Joon ��������������������������������������� Disclosed no conflict of interest.
Kim, Wook �������������������������������������������� Disclosed no conflict of interest.
Kim, Yong-Seong ���������������������������������� Disclosed no conflict of interest.
Kim, Young Jin ������������������������������������� Disclosed no conflict of interest.
Kim, Young-Bum ����������������������������������� Disclosed no conflict of interest.
Kim, Yun Kyoung ���������������������������������� Disclosed no conflict of interest.
Kimple, Michelle E. ������������������������������ Disclosed no conflict of interest.
King, George L. ������������������������������������� Disclosed no conflict of interest.
King, Timothy ��������������������������������������� Disclosed no conflict of interest.
Kingwell, Bronwyn A. �������������������������� Disclosed no conflict of interest.
Kircher, Robert �������������������������������������� Employee: Dose Safety Inc.; Stock/Shareholder: Dose
Safety Inc.
Klisch, Theresa ������������������������������������� Disclosed no conflict of interest.
Knadler, Mary P. ����������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Knoblauch, Nicholas W. ����������������������� Disclosed no conflict of interest.
Knop, Filip K. ���������������������������������������� Consultant: AstraZeneca Pharmaceuticals LP, Boehringer
Ingelheim Pharmaceuticals, Inc., Bristol-Myers Squibb
Company, Eli Lilly and Company, Gilead, Merck Sharp
& Dohme, Novo Nordisk A/S, Sanofi U.S., Zealand
Pharma A/S; Research Support: Novo Nordisk A/S,
Sanofi U.S.
Knutsen, Chad �������������������������������������� Employee: Pacific Diabetes Technologies, Inc.; Stock/
Shareholder: Pacific Diabetes Technologies, Inc.
Ko, Yi-An ���������������������������������������������� Disclosed no conflict of interest.
Kobiernicki, Frances ����������������������������� Disclosed no conflict of interest.
Kodella, Elisavet ���������������������������������� Disclosed no conflict of interest.
Kodella, Kostantia �������������������������������� Disclosed no conflict of interest.
Koistenen, Heikki ��������������������������������� Disclosed no conflict of interest.
Kokovay, Erzsebet �������������������������������� Disclosed no conflict of interest.
Kolar, Matthew J. �������������������������������� Disclosed no conflict of interest.
Kondegowda, Nagesha G. ������������������� Disclosed no conflict of interest.
Konishi, Masahiro �������������������������������� Disclosed no conflict of interest.
Konopka, Adam R. �������������������������������� Disclosed no conflict of interest.
Kooy, Adriaan ��������������������������������������� Disclosed no conflict of interest.
Koratkar, Revati ������������������������������������ Disclosed no conflict of interest.
Korhonen, Pasi ������������������������������������� Employee: Takeda Development Centre Europe.
LB104
RELATIONSHIP/COMPANY
Kornfeind, Ellyn ������������������������������������ Disclosed no conflict of interest.
Koroscil, Thomas M. ���������������������������� Disclosed no conflict of interest.
Krasner, Alan ���������������������������������������� Employee: Biodel Inc.; Stock/Shareholder: Biodel Inc.
Kraus, Morey ���������������������������������������� Disclosed no conflict of interest.
Kretzler, Matthias ��������������������������������� Consultant: Abbvie, AstraZeneca Pharmaceuticals LP,
Boehringer Ingelheim Pharmaceuticals, Inc., Eli Lilly
and Company, Novo Nordisk Inc., Pfizer Inc.; Research
Support: Abbvie, AstraZeneca Pharmaceuticals LP,
Boehringer Ingelheim Pharmaceuticals, Inc., Eli Lilly
and Company, Novo Nordisk Inc., Pfizer Inc.
Krischer, Jeffrey P. �������������������������������� Disclosed no conflict of interest.
Krishnaswamy, Kamala ������������������������ Disclosed no conflict of interest.
Kronenberg, Florian ������������������������������ Disclosed no conflict of interest.
Ku, Bon Jeong �������������������������������������� Disclosed no conflict of interest.
Kuang, Lin �������������������������������������������� Disclosed no conflict of interest.
Kubo, Fumiyo ���������������������������������������� Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Bristol-Myers Squibb Company,
Daiichi-Sankyo Co., Ltd., Eli Lilly Japan K.K.,
Johnson & Johnson, Kissei Pharmaceutical Co., Ltd.,
Merck Sharp & Dohme, Mitsubishi Tanabe Pharma
Corporation, Novartis Corporation, Novo Nordisk Inc.,
Ono Pharmaceutical Co., Ltd., Sanofi U.S., Sumimoto
Dainippon Pharma Co., Ltd., Takeda Pharmaceutical
Company Limited.
Kudva, Yogish C. ���������������������������������� Disclosed no conflict of interest.
Kuhadiya, Nitesh D. ����������������������������� Disclosed no conflict of interest.
Kuliawat, Regina ���������������������������������� Disclosed no conflict of interest.
Kulkarni, Rohit N. ��������������������������������� Disclosed no conflict of interest.
Kumar, Ashish �������������������������������������� Disclosed no conflict of interest.
Kumar, Satish ��������������������������������������� Disclosed no conflict of interest.
Kumar, Sudhesh ����������������������������������� Disclosed no conflict of interest.
Kumar, Sunil ����������������������������������������� Disclosed no conflict of interest.
Kumareswaran, Kavita ������������������������� Speaker’s Bureau: Astra Zeneca, Eli Lilly, Medtronic, Inc.,
MSD, Sanofi U.S., Takeda.
Künzli, Nino ������������������������������������������ Disclosed no conflict of interest.
Kurmi, Kiran ����������������������������������������� Disclosed no conflict of interest.
Kurtz, Natalie ��������������������������������������� Employee: Medtronic MiniMed, Inc.; Stock/Shareholder:
Medtronic, Inc.
Kusmartseva, Irina ������������������������������� Disclosed no conflict of interest.
Kutoh, Eiji ��������������������������������������������� Disclosed no conflict of interest.
Kwak, Eunhwa ������������������������������������� Disclosed no conflict of interest.
Kwon, Se Chang ����������������������������������� Disclosed no conflict of interest.
Kyoong, Andrew ����������������������������������� Disclosed no conflict of interest.
Kyrgios, Ioannis ������������������������������������ Disclosed no conflict of interest.
La Ronde-Richard, Ann-Marie ������������� Disclosed no conflict of interest.
LaBell, Elizabeth S. ������������������������������ Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Laca, Jose �������������������������������������������� Disclosed no conflict of interest.
Lacadie, Cheryl ������������������������������������� Disclosed no conflict of interest.
Lacombe, Julie ������������������������������������� Disclosed no conflict of interest.
Laffel, Lori M. ��������������������������������������� Advisory Panel: Animas Corporation, AstraZeneca,
Boehringer Ingelheim Pharmaceuticals, Inc., BristolMyers Squibb, Dexcom, Inc., Eli Lilly and Company,
Johnson & Johnson, LifeScan, Inc., Menarini Group,
Novo Nordisk Inc., Oshadi Drug Administration,
Roche Diagnostics, Sanofi U.S.; Consultant: Animas
Corporation, AstraZeneca, Boehringer Ingelheim
Pharmaceuticals, Inc., Bristol-Myers Squibb, Dexcom,
Inc., Eli Lilly and Company, Johnson & Johnson,
LifeScan, Inc., Menarini Group, Novo Nordisk Inc.,
Oshadi Drug Administration, Roche Diagnostics, Sanofi
U.S.; Research Support: Bayer HealthCare, Boehringer
Ingelheim Pharmaceuticals, Inc., Dexcom, Inc.
Lage, Adrianne ������������������������������������� Disclosed no conflict of interest.
Lagerstedt, Jens ���������������������������������� Disclosed no conflict of interest.
Lakhani, Rohan ������������������������������������� Disclosed no conflict of interest.
Lakka, Timo ������������������������������������������ Disclosed no conflict of interest.
Lakshmi, Mudigere N. �������������������������� Disclosed no conflict of interest.
Lam, Eric Chen Quin ����������������������������� Employee: Eli Lilly and Company.
Lam, Karen Siu-Ling ����������������������������� Disclosed no conflict of interest.
Lam, Meghan ��������������������������������������� Disclosed no conflict of interest.
Lammert, Eckhard �������������������������������� Other Relationship: Author persue the patent application
WO 2013/029762 A1.
Langlais, Paul R. ����������������������������������� Disclosed no conflict of interest.
Lanza, Ian ��������������������������������������������� Disclosed no conflict of interest.
Lao, Julie ���������������������������������������������� Employee: Merck & Co., Inc.
Larco, Nancy C. ������������������������������������ Disclosed no conflict of interest.
Larco, Philippe �������������������������������������� Disclosed no conflict of interest.
Larrivee, Sandra ����������������������������������� Disclosed no conflict of interest.
Larsen, Peter ���������������������������������������� Disclosed no conflict of interest.
Lassance Gomes, Luciana �������������������� Disclosed no conflict of interest.
Lassman, Michael E. ���������������������������� Employee: Merck & Co., Inc.
AUTHOR
RELATIONSHIP/COMPANY
Lau, Raymond G. ���������������������������������� Disclosed no conflict of interest.
Lau, Winston ���������������������������������������� Disclosed no conflict of interest.
Lautsch, Norman ���������������������������������� Disclosed no conflict of interest.
Lavalle-González, Fernando J. ������������� Advisory Panel: AstraZeneca, Boehringer Ingelheim, Eli
Lilly, Janssen, Novo Nordisk, Sanofi; Board Member:
AstraZeneca, Boehringer Ingelheim, Janssen, Novo
Nordisk, Sanofi; Research Support: Boehringer
Ingelheim, Janssen, Novo Nordisk, Sanofi; Speaker’s
Bureau: AstraZeneca, Boehringer Ingelheim, Eli Lilly,
Janssen, MSD, Novo Nordisk, Sanofi.
Lavin, Philip T. �������������������������������������� Research Support: ZS Pharma, Inc.; Stock/Shareholder: ZS
Pharma, Inc.
Layden, Brian T. ������������������������������������ Disclosed no conflict of interest.
Le, Yun-Zheng ��������������������������������������� Disclosed no conflict of interest.
Leach, Jake ������������������������������������������ Employee: Dexcom, Inc.
Leber, Alexander ���������������������������������� Disclosed no conflict of interest.
Leber, Stacey ���������������������������������������� Disclosed no conflict of interest.
Lee, Douglas S. ������������������������������������ Employee: Pfizer Inc.; Stock/Shareholder: Pfizer Inc.
Lee, Hong Kyu �������������������������������������� Disclosed no conflict of interest.
Lee, In-Kyu ������������������������������������������� Disclosed no conflict of interest.
Lee, Jennifer ���������������������������������������� Disclosed no conflict of interest.
Lee, Jimmy Tsz-Hang ��������������������������� Disclosed no conflict of interest.
Lee, Jisoo ��������������������������������������������� Employee: Boehringer Ingelheim Pharma GmbH & Co. KG.
Lee, Junga �������������������������������������������� Disclosed no conflict of interest.
Lee, Jung-Hun �������������������������������������� Disclosed no conflict of interest.
Lee, Kwan-Hoo ������������������������������������� Disclosed no conflict of interest.
Lee, Mi Kyung �������������������������������������� Disclosed no conflict of interest.
Lee, Tsz-Hang ��������������������������������������� Disclosed no conflict of interest.
Lee, Woohyung ������������������������������������ Disclosed no conflict of interest.
Leech, Colin ������������������������������������������ Disclosed no conflict of interest.
Lehman, Donna M. ������������������������������� Disclosed no conflict of interest.
Leiter, Lawrence A. ������������������������������ Research Support: AstraZeneca Pharmaceuticals LP.
Leng, Jiyan ������������������������������������������� Disclosed no conflict of interest.
Leng, Song ������������������������������������������� Disclosed no conflict of interest.
Lentucci, Claudia ���������������������������������� Disclosed no conflict of interest.
Leonardi, Anthony �������������������������������� Disclosed no conflict of interest.
Lerakis, Stamatios ������������������������������� Disclosed no conflict of interest.
Lernmark, Åke �������������������������������������� Disclosed no conflict of interest.
Lettre, Guillaume ��������������������������������� Disclosed no conflict of interest.
Levenson, Amy E. ��������������������������������� Disclosed no conflict of interest.
Levin, Philip A. ������������������������������������� Advisory Panel: Novo Nordisk Inc., Sanofi U.S.;
Consultant: Novo Nordisk Inc., Sanofi U.S.; Research
Support: Amylin Pharmaceuticals, LLC., Eli Lilly and
Company, Novo Nordisk Inc., Sanofi U.S.; Speaker’s
Bureau: Amylin Pharmaceuticals, LLC., Boehringer
Ingelheim Pharmaceuticals, Inc., Eli Lilly and
Company, GlaxoSmithKline, Novo Nordisk Inc.
Levy, Brian L. ���������������������������������������� Employee: LifeScan, Inc.
Li, Bin ��������������������������������������������������� Disclosed no conflict of interest.
Li, Fenfen ���������������������������������������������� Disclosed no conflict of interest.
Li, GuoDong ������������������������������������������ Disclosed no conflict of interest.
Li, Hui ��������������������������������������������������� Disclosed no conflict of interest.
Li, Ji ������������������������������������������������������ Disclosed no conflict of interest.
Li, Liwu ������������������������������������������������� Disclosed no conflict of interest.
Li, Nina ������������������������������������������������� Employee: Merck & Co., Inc.
Li, Qin ��������������������������������������������������� Disclosed no conflict of interest.
Li, Ruifeng �������������������������������������������� Disclosed no conflict of interest.
Li, Wangen ������������������������������������������� Disclosed no conflict of interest.
Li, Wenjing ������������������������������������������� Disclosed no conflict of interest.
Li, Xingwang ���������������������������������������� Disclosed no conflict of interest.
Li, Xuhang �������������������������������������������� Disclosed no conflict of interest.
Li, Zihao ������������������������������������������������ Disclosed no conflict of interest.
Liang, Weiqiang ����������������������������������� Disclosed no conflict of interest.
Liao, Yi-Chun ���������������������������������������� Disclosed no conflict of interest.
Liao, Yunfei ������������������������������������������� Disclosed no conflict of interest.
Lichliter, Jason ������������������������������������� Disclosed no conflict of interest.
Liew, Chong Wee ��������������������������������� Disclosed no conflict of interest.
Lightwood, Dan ������������������������������������ Employee: UCB Pharma.
Lim, Sai Kiang �������������������������������������� Disclosed no conflict of interest.
Lin, Daniel J. ���������������������������������������� Disclosed no conflict of interest.
Lin, Dongping ��������������������������������������� Disclosed no conflict of interest.
Lin, Su Fan �������������������������������������������� Disclosed no conflict of interest.
Lin, Yung-Chieh ������������������������������������ Disclosed no conflict of interest.
Lincoff, A. Michael ������������������������������� Disclosed no conflict of interest.
Lindberg, Iris ���������������������������������������� Disclosed no conflict of interest.
Linder, Marie ���������������������������������������� Research Support: Centre for Pharmacoepidemiology (CPE)
at Karolinska Institute has contracts with several
pharmaceutical companies and performs research for
them through research grants.
Lindgren, Cecilia M. ����������������������������� Disclosed no conflict of interest.
Lingvay, Ildiko ��������������������������������������� Consultant: AstraZeneca Pharmaceuticals LP, Novo
Nordisk Inc.; Other Relationship: Sanofi U.S., Editorial.;
Research Support: GID, Novo Nordisk Inc., Pfizer Inc.
LB105
AUTHOR DISCLOSURE
AUTHOR
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
AUTHOR
Linnebjerg, Helle ���������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Lious, Daniel ���������������������������������������� Disclosed no conflict of interest.
Liu, Ching-Ti ����������������������������������������� Disclosed no conflict of interest.
Liu, Dongmin ���������������������������������������� Disclosed no conflict of interest.
Liu, Franklin ������������������������������������������ Employee: Merck & Co., Inc.
Liu, Hangsheng ������������������������������������ Disclosed no conflict of interest.
Liu, Jia �������������������������������������������������� Disclosed no conflict of interest.
Liu, Jiajun ��������������������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Liu, Quan ���������������������������������������������� Disclosed no conflict of interest.
Liu, Ying ������������������������������������������������ Disclosed no conflict of interest.
Liu, Yuanhang ��������������������������������������� Disclosed no conflict of interest.
Liu, Yujia ����������������������������������������������� Disclosed no conflict of interest.
Lizárraga-Mollinedo, Esther ����������������� Disclosed no conflict of interest.
Lizarzaburu, Juan C. ����������������������������� Disclosed no conflict of interest.
Lo, K. Sin ���������������������������������������������� Disclosed no conflict of interest.
Loh, Margaret �������������������������������������� Disclosed no conflict of interest.
Loh, Yik Wen ���������������������������������������� Disclosed no conflict of interest.
Lombard, Julian H. ������������������������������� Disclosed no conflict of interest.
Loos, Ruth J.F. �������������������������������������� Disclosed no conflict of interest.
Lopez, Claudia �������������������������������������� Disclosed no conflict of interest.
Lopez-Gutierrez, Joel ��������������������������� Disclosed no conflict of interest.
Lu, Brian ����������������������������������������������� Disclosed no conflict of interest.
Lu, Christine ����������������������������������������� Disclosed no conflict of interest.
Lu, Meng ���������������������������������������������� Disclosed no conflict of interest.
Lu, Qi ���������������������������������������������������� Disclosed no conflict of interest.
Lu, Yang ������������������������������������������������ Disclosed no conflict of interest.
Lu, Yingchang ��������������������������������������� Disclosed no conflict of interest.
Lu, Yingli ����������������������������������������������� Disclosed no conflict of interest.
Lu, Yongke �������������������������������������������� Disclosed no conflict of interest.
Lubree, Himangi ����������������������������������� Disclosed no conflict of interest.
Lucas, Anthony ������������������������������������� Disclosed no conflict of interest.
Lulo, James ������������������������������������������ Disclosed no conflict of interest.
Lund, Asger ������������������������������������������ Disclosed no conflict of interest.
Lundqvist, Kristin ��������������������������������� Disclosed no conflict of interest.
Luo, Jing ����������������������������������������������� Disclosed no conflict of interest.
Luo, Oscar �������������������������������������������� Disclosed no conflict of interest.
Luque-Fernandez, Miguel A. ���������������� Disclosed no conflict of interest.
Lv, Tiantian ������������������������������������������� Disclosed no conflict of interest.
Ly, Trang T. �������������������������������������������� Disclosed no conflict of interest.
Lynes, Mattew D. ��������������������������������� Disclosed no conflict of interest.
Lyv, Fuping �������������������������������������������� Disclosed no conflict of interest.
Ma, Jian-Xing �������������������������������������� Disclosed no conflict of interest.
Ma, Tony ����������������������������������������������� Employee: Eisai Inc.
Ma, Xiaotang ��������������������������������������� Disclosed no conflict of interest.
Maarouf, Omar H. �������������������������������� Disclosed no conflict of interest.
MacDonald, Patrick E. �������������������������� Disclosed no conflict of interest.
Machida, Yui ���������������������������������������� Disclosed no conflict of interest.
Macias, William L. ������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
MacIsaac, Richard J. ��������������������������� Disclosed no conflict of interest.
Madiraju, Anila K. �������������������������������� Disclosed no conflict of interest.
Madura II, James A. ���������������������������� Disclosed no conflict of interest.
Magyar, Kendra ������������������������������������ Disclosed no conflict of interest.
Maheshwari, Pradeep K. ��������������������� Disclosed no conflict of interest.
Mahesula, Swetha ������������������������������� Disclosed no conflict of interest.
Majak, Maila ���������������������������������������� Employee: EPID Research performs financially supported
studies for several pharmaceutical companies
including Takeda Development Centre Europe.
Makdissi, Antoine �������������������������������� Disclosed no conflict of interest.
Malik, Vasanti S. ���������������������������������� Disclosed no conflict of interest.
Mallikarjuna, Shwetha ������������������������ Disclosed no conflict of interest.
Manan, Jyotika ������������������������������������ Disclosed no conflict of interest.
Mandarino, Lawrence J. ���������������������� Disclosed no conflict of interest.
Manganiello, Vincent Manganiello ����� Disclosed no conflict of interest.
Maniatis, Nikolas ��������������������������������� Disclosed no conflict of interest.
Manning Fox, Jocelyn E. ���������������������� Disclosed no conflict of interest.
Mansmann, Ulrich �������������������������������� Disclosed no conflict of interest.
Manson, JoAnn E. �������������������������������� Other Relationship: Pfizer Inc.
Maratos Flier, Eleftheria ���������������������� Advisory Panel: Novo Nordisk Inc., Sanofi.
Marcinak, John ������������������������������������ Disclosed no conflict of interest.
Marquard, Jan ������������������������������������� Other Relationship: Author persue the patent application
WO 2013/029762 A1.
Marquez, Eladio ����������������������������������� Disclosed no conflict of interest.
Martin, Brittany ������������������������������������ Disclosed no conflict of interest.
Martin, Holly R. ������������������������������������ Employee: Eli Lilly and Company.
Martin, Jennifer A. ������������������������������ Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Maruthur, Nisa M. �������������������������������� Disclosed no conflict of interest.
Mather, Kieren J. ��������������������������������� Consultant: Boehringer Ingelheim GmbH, Sanofi U.S.;
Research Support: Abbott, Boehringer Ingelheim Co., Ltd,
Merck & Co., Inc., Nippon, Novo Nordisk A/S, Sanofi U.S.
RELATIONSHIP/COMPANY
Matheson, Don ������������������������������������ Employee: Dose Safety Inc.; Stock/Shareholder: Dose
Safety Inc.
Mathieu, Chantal ��������������������������������� Advisory Panel: AstraZeneca Pharmaceuticals LP,
Boehringer Ingelheim Pharmaceuticals, Inc., BristolMyers Squibb Company, Eli Lilly and Company,
Hanmi, Johnson & Johnson, MannKind Corporation,
Merck Sharp & Dohme, Novartis Pharmaceuticals
Corporation, Novo Nordisk Inc., Pfizer Inc., Sanofi
U.S.; Speaker’s Bureau: AstraZeneca Pharmaceuticals
LP, Eli Lilly and Company, Merck Sharp & Dohme,
Novartis Pharmaceuticals Corporation, Novo Nordisk
Inc., Sanofi U.S.
Matsuoka, Takaaki ������������������������������� Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Daiichi-Sankyo Co., Ltd., Eli
Lilly Japan K.K., Kissei Pharmaceutical Co., Ltd.,
Kowa Pharmaceuticals, Merck Sharp & Dohme,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Novo Nordisk Inc., Ono
Pharmaceutical Co., Ltd., Sanofi U.S., Shionogi Inc.,
Takeda Pharmaceutical Company Limited.
Matsushita, Kanae ������������������������������� Disclosed no conflict of interest.
Matteucci, Elena ���������������������������������� Disclosed no conflict of interest.
Mauceri, Joseph ���������������������������������� Disclosed no conflict of interest.
Mauseth, Richard ��������������������������������� Employee: Dose Safety Inc.; Stock/Shareholder: Dose
Safety Inc.
Mazzone, Theodore ������������������������������ Disclosed no conflict of interest.
McCarthy, Mark I. �������������������������������� Disclosed no conflict of interest.
McDaniel, Kristen �������������������������������� Disclosed no conflict of interest.
Mcdonald, Molly ���������������������������������� Disclosed no conflict of interest.
McElrtah, Thomas F. ����������������������������� Disclosed no conflict of interest.
McEwen, Laura N. ������������������������������� Disclosed no conflict of interest.
McGuire, Darren K. ������������������������������ Disclosed no conflict of interest.
McKenney, Sarah ��������������������������������� Research Support: Medtronic MiniMed, Inc.
McLaughlin, Kerry A. ��������������������������� Disclosed no conflict of interest.
McTigue, Kathleen M. ������������������������� Disclosed no conflict of interest.
Meah, Farah ����������������������������������������� Disclosed no conflict of interest.
Medina-Gomez, M. Carolina ���������������� Disclosed no conflict of interest.
Mehta, Aditya �������������������������������������� Disclosed no conflict of interest.
Mehta, Cyrus ���������������������������������������� Disclosed no conflict of interest.
Mehta, Ravindra L. ������������������������������� Advisory Panel: Abbvie, AM Pharma, Ardea, Eli Lilly and
Company; Consultant: Astellas Pharma US, Baxter,
CSL Behring, Inc., Eli Lilly and Company, Ferring
Research, GlaxoSmithKline, Isis Pharmaceuticals, Inc.,
Sanofi-Aventis, Sova; Research Support: International
Safety Adverse Events Consortium, Thrasos
Therapeutics; Stock/Shareholder: Astute Inc.
Mei, Yong ��������������������������������������������� Disclosed no conflict of interest.
Meijer, Rick I. ��������������������������������������� Disclosed no conflict of interest.
Meikle, Peter J. ������������������������������������ Disclosed no conflict of interest.
Meinicke, Thomas �������������������������������� Employee: Boehringer Ingelheim GmbH.
Meissner, Thomas �������������������������������� Other Relationship: Author persue the patent application
WO 2013/029762 A1.
Meister, Gunter ������������������������������������ Disclosed no conflict of interest.
Melissinos, Michail ����������������������������� Disclosed no conflict of interest.
Mellbin, Linda G. ���������������������������������� Research Support: MSD, Sanofi Aventis.
Mendivil, Carlos O. ������������������������������ Disclosed no conflict of interest.
Menegaz, Danusa �������������������������������� Disclosed no conflict of interest.
Meng, Shu �������������������������������������������� Disclosed no conflict of interest.
Meng, Ying ������������������������������������������� Disclosed no conflict of interest.
Menon, Venu ���������������������������������������� Disclosed no conflict of interest.
Menon, Vinod ��������������������������������������� Disclosed no conflict of interest.
Merino-Trigo, Ana �������������������������������� Employee: Sanofi.
Merton, Kate ���������������������������������������� Employee: Janssen Research & Development, LLC.
Meunier, Clemence ������������������������������ Disclosed no conflict of interest.
Miao, Ji ������������������������������������������������ Disclosed no conflict of interest.
Michels, Aaron W. ������������������������������� Disclosed no conflict of interest.
Milani, Massimo ���������������������������������� Employee: Isdin.
Milaszewski, Kerry ������������������������������� Consultant: Eli Lilly and Company.
Milhem, Tyler ��������������������������������������� Employee: Pacific Diabetes Technologies, Inc.; Stock/
Shareholder: Pacific Diabetes Technologies, Inc.
Min, Ae-Kyung ������������������������������������� Disclosed no conflict of interest.
Min, Jihee �������������������������������������������� Disclosed no conflict of interest.
Min, Kyung Wan ���������������������������������� Disclosed no conflict of interest.
Min, So Yun ������������������������������������������ Disclosed no conflict of interest.
Minium, Judi ���������������������������������������� Disclosed no conflict of interest.
Mintz, James ��������������������������������������� Disclosed no conflict of interest.
Mirmira, Raghavendra G. ��������������������� Disclosed no conflict of interest.
Misha’l, Aly A. ������������������������������������� Disclosed no conflict of interest.
Mitrovich, Connor �������������������������������� Disclosed no conflict of interest.
Miura, Junnosuke �������������������������������� Disclosed no conflict of interest.
Miyashita, Kazuyuki ����������������������������� Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
LB106
RELATIONSHIP/COMPANY
Pharmaceuticals, Inc., Bristol-Myers Squibb Company,
Daiichi-Sankyo Co., Ltd., Eli Lilly Japan K.K., Johnson
& Johnson, Kissei Pharmaceutical Co., Merck Sharp
& Dohme, Mitsubishi Tanabe Pharma Corporation,
Novartis Pharmaceuticals Corporation, Novo Nordisk
Inc.,Ltd., Ono Pharmaceutical Co., Ltd., Sanofi U.S.,
Sumimoto Dainippon Pharma Co., Ltd., Takeda
Pharmaceutical Company Limited.
Miyatsuka, Takeshi ������������������������������ Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Bristol-Myers Squibb Company,
Daiichi-Sankyo Co., Ltd., Dainippon Pharma Co.,
Ltd., Eli Lilly Japan K.K, Johnson & Johnson, Kissei
Pharmaceutical Co., Ltd., Merck Sharp & Dohme,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Novo Nordisk Inc., Ono
Pharmaceutical Co., Sanofi U.S., Sumimoto, Ltd.,
Takeda Pharmaceutical Company Limited.
Mizuno, Ken ����������������������������������������� Employee: Kowa Pharmaceuticals.
Mlynarchik, Andrew ����������������������������� Disclosed no conflict of interest.
Mlynarski, Wojciech ���������������������������� Disclosed no conflict of interest.
Modi, Devangi �������������������������������������� Disclosed no conflict of interest.
Moerman, Ericka ���������������������������������� Disclosed no conflict of interest.
Mohammad Moradi, Shayan ��������������� Disclosed no conflict of interest.
Mohan, Viswanathan ��������������������������� Disclosed no conflict of interest.
Mohanasundaram, Daisy ��������������������� Disclosed no conflict of interest.
Mohlke, Karen L. ���������������������������������� Disclosed no conflict of interest.
Mohseni, Mahshid ������������������������������� Disclosed no conflict of interest.
Moisidou, Maria ���������������������������������� Disclosed no conflict of interest.
Molina, Judith T. ���������������������������������� Disclosed no conflict of interest.
Mondesir, Debbie ��������������������������������� Disclosed no conflict of interest.
Moon, Sanghoon ���������������������������������� Disclosed no conflict of interest.
Moore, Adrian �������������������������������������� Employee: UCB Pharma.
Moore, Robert �������������������������������������� Disclosed no conflict of interest.
Mora, Edwin ����������������������������������������� Disclosed no conflict of interest.
Moreno-Ruiz, Francisco J. ������������������� Disclosed no conflict of interest.
Morgan, Diana ������������������������������������� Disclosed no conflict of interest.
Morley, Thomas S. ������������������������������� Disclosed no conflict of interest.
Morris, Andrew P. ��������������������������������� Disclosed no conflict of interest.
Morris, Heather L. �������������������������������� Disclosed no conflict of interest.
Morris, Kristin �������������������������������������� Employee: Pacific Diabetes Technologies, Inc.; Stock/
Shareholder: Pacific Diabetes Technologies, Inc.
Morrow, Linda �������������������������������������� Employee: Profil Institute for Clinical Research, Inc.;
Stock/Shareholder: Profil Institute for Clinical
Research, Inc.
Morton-Eggleston, Emma B. ���������������� Disclosed no conflict of interest.
Mosser, Rockann ���������������������������������� Disclosed no conflict of interest.
Mounayar, Marwan ������������������������������ Disclosed no conflict of interest.
Mudaliar, Sunder ���������������������������������� Advisory Panel: AstraZeneca Pharmaceuticals LP;
Consultant: AstraZeneca Pharmaceuticals LP;
Research Support: AstraZeneca Pharmaceuticals
LP, Cebix, Inc., Intarcia Therapeutics, Inc., Janssen
Research & Development LLC; Speaker’s Bureau:
AstraZeneca Pharmaceuticals LP.
Mudgett, John ������������������������������������� Employee: Merck & Co., Inc.
Muise, Eric ������������������������������������������� Employee: Merck & Co., Inc.
Mullapudi, Kamesh ������������������������������ Disclosed no conflict of interest.
Mullen, Deborah M. ����������������������������� Disclosed no conflict of interest.
Muniyappa, Ranganath ������������������������ Disclosed no conflict of interest.
Munk, Ole L. ����������������������������������������� Disclosed no conflict of interest.
Muñoz, Oscar ��������������������������������������� Disclosed no conflict of interest.
Munoz-Gomez, Miguel ������������������������� Disclosed no conflict of interest.
Munoz-Torres, Francisco ���������������������� Disclosed no conflict of interest.
Murakami, Kazutoshi ��������������������������� Disclosed no conflict of interest.
Murakami, Kentaro ������������������������������ Employee: Kowa Pharmaceuticals.
Murthy, Narasimha ������������������������������ Disclosed no conflict of interest.
Mynatt, Randall L. �������������������������������� Research Support: American Diabetes Association.
Na, Ki-Ryang ���������������������������������������� Disclosed no conflict of interest.
Nagarajan, Lakshmipriya ��������������������� Disclosed no conflict of interest.
Nagel, Friederike ���������������������������������� Employee: Boehringer Ingelheim Pharma GmbH & Co. KG.
Naik, Sarita ������������������������������������������ Disclosed no conflict of interest.
Nair, K. Sreekumaran ��������������������������� Disclosed no conflict of interest.
Nakamura, Katherine ��������������������������� Employee: Dexcom, Inc.
Nakamura, Naoto ��������������������������������� Disclosed no conflict of interest.
Nakamura, Yumiko ������������������������������� Disclosed no conflict of interest.
Nakatsuka, Atsuko ������������������������������� Disclosed no conflict of interest.
Nam, Minwoo �������������������������������������� Disclosed no conflict of interest.
Narayan, K.M. Venkat �������������������������� Disclosed no conflict of interest.
Narisu, Narisu �������������������������������������� Disclosed no conflict of interest.
Nasr, Gamela ���������������������������������������� Disclosed no conflict of interest.
Nassar, Wael F. ������������������������������������ Disclosed no conflict of interest.
Nawrocki, Andrea �������������������������������� Employee: Merck & Co., Inc.
Neal, Adam S. �������������������������������������� Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Neale, Helen ���������������������������������������� Employee: UCB Pharma.
Neergaard, Jesper S. ��������������������������� Disclosed no conflict of interest.
Nelson, Scott M. ���������������������������������� Advisory Panel: Roche Diagnostics; Research Support:
Roche Diagnostics; Speaker’s Bureau: Roche
Diagnostics.
Neuman, Joshua C. ������������������������������ Disclosed no conflict of interest.
Nhan, Trinh ������������������������������������������� Disclosed no conflict of interest.
Nicholls, Stephen ��������������������������������� Disclosed no conflict of interest.
Nie, Xiaomin ���������������������������������������� Disclosed no conflict of interest.
Nie, Yaohui ������������������������������������������� Disclosed no conflict of interest.
Nissen, Steven E. ��������������������������������� Disclosed no conflict of interest.
Niu, Jianmin ����������������������������������������� Disclosed no conflict of interest.
Nobrega, Marcelo A. ��������������������������� Disclosed no conflict of interest.
Noel, Guillaume ����������������������������������� Disclosed no conflict of interest.
Nordén, Kristina ����������������������������������� Disclosed no conflict of interest.
Norman-Burgdolf, Heather L. ��������������� Disclosed no conflict of interest.
North, Kari E. ���������������������������������������� Disclosed no conflict of interest.
North, Paula E. ������������������������������������� Disclosed no conflict of interest.
Norton, Luke ����������������������������������������� Disclosed no conflict of interest.
Nowlan, Molly ������������������������������������� Disclosed no conflict of interest.
Nunlee-Bland, Gail ������������������������������� Disclosed no conflict of interest.
Nunoue, Tomokazu ������������������������������� Disclosed no conflict of interest.
Obrosova, Irina G. �������������������������������� Disclosed no conflict of interest.
Odede, Geofrey ������������������������������������ Employee: UCB Pharma.
Ogawa, Daisuke ����������������������������������� Disclosed no conflict of interest.
Oh, Byung-Chul ������������������������������������ Disclosed no conflict of interest.
Oh, Kook-Hwan ������������������������������������ Disclosed no conflict of interest.
Oh, Kyoung-Jin ������������������������������������� Disclosed no conflict of interest.
Oh, Minsuk ������������������������������������������� Disclosed no conflict of interest.
Ohta, Masayuki ������������������������������������ Employee: Kowa Pharmaceuticals.
Okada, Junichi ������������������������������������� Disclosed no conflict of interest.
Okada, Shuichi ������������������������������������� Disclosed no conflict of interest.
O’Neal, David ��������������������������������������� Disclosed no conflict of interest.
O’Rahilly, Stephen �������������������������������� Disclosed no conflict of interest.
Orchard, Trevor J. ��������������������������������� Disclosed no conflict of interest.
Ordelheide, Anna-Maria ���������������������� Disclosed no conflict of interest.
Orduz, Arturo ���������������������������������������� Disclosed no conflict of interest.
O’Reilly, Eilis J. ������������������������������������ Disclosed no conflict of interest.
Oropeza, Daniel ������������������������������������ Disclosed no conflict of interest.
Orr, Gregory ������������������������������������������ Disclosed no conflict of interest.
Oruk, Guzide Gonca ������������������������������ Disclosed no conflict of interest.
Osakai, Aya ������������������������������������������ Disclosed no conflict of interest.
Osawa, Mari ���������������������������������������� Disclosed no conflict of interest.
Osborne, Timothy ��������������������������������� Disclosed no conflict of interest.
Osborne, William ��������������������������������� Disclosed no conflict of interest.
Osei, Kwame ���������������������������������������� Consultant: Merck & Co., Inc.; Research Support:
AstraZeneca Pharmaceuticals LP.
Osganian, Stavroula ����������������������������� Disclosed no conflict of interest.
Østergaard, Jakob A. ��������������������������� Disclosed no conflict of interest.
O-Sullivan, InSug ��������������������������������� Disclosed no conflict of interest.
Oteng-Ntim, Eugene ���������������������������� Disclosed no conflict of interest.
Otter, Silke �������������������������������������������� Disclosed no conflict of interest.
Otto, Michael ��������������������������������������� Disclosed no conflict of interest.
Ouwens, Margriet �������������������������������� Disclosed no conflict of interest.
Owen, Neville �������������������������������������� Disclosed no conflict of interest.
Pachanski, Michele ������������������������������ Disclosed no conflict of interest.
Packham, David K. ������������������������������� Consultant: Nephrogenex, ZN Pharma.
Palaia, Thomas ������������������������������������� Disclosed no conflict of interest.
Pallardo, Felipe ������������������������������������ Disclosed no conflict of interest.
Pallavi, Puttrevana M. �������������������������� Disclosed no conflict of interest.
Pan, Kewu �������������������������������������������� Disclosed no conflict of interest.
Pandey, Varun K. ���������������������������������� Disclosed no conflict of interest.
Pankratz, Nathan ���������������������������������� Disclosed no conflict of interest.
Panlasigui, Neil ������������������������������������ Disclosed no conflict of interest.
Parenty, Geraldine �������������������������������� Disclosed no conflict of interest.
Pargal, Summi �������������������������������������� Disclosed no conflict of interest.
Parikh, Lisa ������������������������������������������� Disclosed no conflict of interest.
Parikh, Neha ����������������������������������������� Employee: Medtronic MiniMed, Inc.
Park, Anna �������������������������������������������� Disclosed no conflict of interest.
Park, Hyoungchun �������������������������������� Disclosed no conflict of interest.
Park, Ji-Hye ������������������������������������������ Disclosed no conflict of interest.
Park, Keun-Gyu ������������������������������������� Disclosed no conflict of interest.
Park, So Hyun ��������������������������������������� Disclosed no conflict of interest.
Park, Sun-Hee �������������������������������������� Disclosed no conflict of interest.
Park, Tae Sun ���������������������������������������� Disclosed no conflict of interest.
Park, Tae-Joon �������������������������������������� Disclosed no conflict of interest.
Park, Yousung ��������������������������������������� Disclosed no conflict of interest.
Parker, Stephen ������������������������������������ Disclosed no conflict of interest.
Parker, Stephen C.J. ����������������������������� Disclosed no conflict of interest.
Parkin, Christopher G. �������������������������� Consultant: Animas Corporation, Asante Solutions, Inc.,
CeQur SA, Dexcom, Inc., Roche Diagnostics, Sanofi U.S.
Parson, Henri ���������������������������������������� Disclosed no conflict of interest.
Parthasarathy, Vijayalaksmi ����������������� Disclosed no conflict of interest.
LB107
AUTHOR DISCLOSURE
AUTHOR
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
Pascual, Michael ���������������������������������� Disclosed no conflict of interest.
Pasko, Dorota ��������������������������������������� Disclosed no conflict of interest.
Pasquarello, Cindy ������������������������������� Disclosed no conflict of interest.
Pasquel, Francisco J. ��������������������������� Disclosed no conflict of interest.
Patel, Nashita �������������������������������������� Disclosed no conflict of interest.
Patel, Niraja ����������������������������������������� Disclosed no conflict of interest.
Patel, Pankaj ���������������������������������������� Employee: Cadila Healthcare Ltd.
Patiño, Jorge E. ������������������������������������ Disclosed no conflict of interest.
Patti, Mary-Elizabeth ��������������������������� Consultant: Defined Health, Diasome, Foodminds, LLC;
Research Support: American Diabetes Association,
Ajinomoto Group, National Institute of Diabetes
and Digestive and Kidney Diseases, Janssen
Pharmaceutical Companies of Johnson & Johnson,
MedImmune, Nuclea, Sanofi U.S.
Pattou, François ����������������������������������� Disclosed no conflict of interest.
Paumelle, Réjane ��������������������������������� Disclosed no conflict of interest.
Pears, Skye ������������������������������������������� Disclosed no conflict of interest.
Peng, Jinghua �������������������������������������� Disclosed no conflict of interest.
Pereira, Mark A. ����������������������������������� Disclosed no conflict of interest.
Perissi, Valentina ��������������������������������� Disclosed no conflict of interest.
Peroni, Odile D. ������������������������������������ Disclosed no conflict of interest.
Perron, Gabrielle ���������������������������������� Disclosed no conflict of interest.
Perry, Rachel J. ������������������������������������ Disclosed no conflict of interest.
Pery, Billy ���������������������������������������������� Employee: LabStyle Innovations, Ltd.
Pessin, Jeffrey E. ��������������������������������� Disclosed no conflict of interest.
Petersen, Kitt F. ������������������������������������ Disclosed no conflict of interest.
Petri, Renata T. ������������������������������������� Disclosed no conflict of interest.
Petrocchi-Passeri, Pamela ������������������� Disclosed no conflict of interest.
Pettus, Jeremy H. ��������������������������������� Advisory Panel: Sanofi U.S, Tandem Diabetes Care, Inc.;
Consultant: Sanofi U.S.; Speaker’s Bureau: Dexcom,
Inc., Johnson & Johnson.
Pfeffer, Sébastien ��������������������������������� Disclosed no conflict of interest.
Pichotta, Philip ������������������������������������� Employee: Biodel Inc.; Stock/Shareholder: Biodel Inc.
Picklesimer, Amy ���������������������������������� Disclosed no conflict of interest.
Piecuch, Emaly ������������������������������������� Disclosed no conflict of interest.
Pihoker, Cate ���������������������������������������� Disclosed no conflict of interest.
Pilegaard, Henriette ����������������������������� Disclosed no conflict of interest.
Pillai, Sreekumar G. ����������������������������� Employee: Eli Lilly and Company.
Pinney, Sara E. ������������������������������������� Disclosed no conflict of interest.
Piron, Matthew ������������������������������������ Disclosed no conflict of interest.
Piston, David W. ����������������������������������� Disclosed no conflict of interest.
Pitale, Ameya ��������������������������������������� Disclosed no conflict of interest.
Pittas, Anastassios G. �������������������������� Disclosed no conflict of interest.
Pober, David ����������������������������������������� Disclosed no conflict of interest.
Poitout, Vincent ������������������������������������ Disclosed no conflict of interest.
Polidori, David �������������������������������������� Employee: Janssen Research & Development LLC.
Pollin, Toni I. ����������������������������������������� Disclosed no conflict of interest.
Polonsky, William H. ���������������������������� Advisory Panel: Novo Nordisk, RocheSanofi, Sanofi;
Consultant: Abbott, Boehringer Ingelheim, Dexcom,
Eli Lilly, Novo Nordisk, Roche, Sanofi.
Polsky, Sarit ������������������������������������������ Disclosed no conflict of interest.
Pongratz, Rebecca L. ���������������������������� Disclosed no conflict of interest.
Poole, Lucinda A. ��������������������������������� Disclosed no conflict of interest.
Popoola, Orishebawo B. ����������������������� Disclosed no conflict of interest.
Popova, Dora ���������������������������������������� Disclosed no conflict of interest.
Porceban, Matheus ������������������������������ Disclosed no conflict of interest.
Porksen, Niels �������������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Possenti, Roberta ��������������������������������� Disclosed no conflict of interest.
Poston, Lucilla �������������������������������������� Research Support: Abbott Nutrition.
Pouwer, Frans ��������������������������������������� Disclosed no conflict of interest.
Poveda, Alaitz �������������������������������������� Disclosed no conflict of interest.
Poy, Matthew N. ���������������������������������� Disclosed no conflict of interest.
Prakash, Prashant K. ���������������������������� Disclosed no conflict of interest.
Pratley, Richard E. �������������������������������� Disclosed no conflict of interest.
Predmore, Zachary ������������������������������� Disclosed no conflict of interest.
Preiser, Nicholas ���������������������������������� Disclosed no conflict of interest.
Preston, Kyle ���������������������������������������� Disclosed no conflict of interest.
Previs, Stephen ������������������������������������ Employee: Merck & Co., Inc.
Previs, Steve ���������������������������������������� Disclosed no conflict of interest.
Price, David A. �������������������������������������� Employee: Dexcom, Inc.
Prince, Melvin J. ���������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Priyadarshini, Medha ��������������������������� Disclosed no conflict of interest.
Probst-Hensch, Nicole ������������������������� Disclosed no conflict of interest.
Pu, Xiaoqi ��������������������������������������������� Disclosed no conflict of interest.
Puckrein, Gary A. ���������������������������������� Disclosed no conflict of interest.
Puppala, Sobha ������������������������������������ Disclosed no conflict of interest.
Puri, Vishwajeet ����������������������������������� Disclosed no conflict of interest.
Pyun, Bo-Jeong ������������������������������������ Disclosed no conflict of interest.
Qi, Ling ������������������������������������������������� Disclosed no conflict of interest.
Qi, Lu ���������������������������������������������������� Disclosed no conflict of interest.
Qiu, Rong ���������������������������������������������� Employee: Janssen Research & Development, LLC.
AUTHOR
RELATIONSHIP/COMPANY
Quek, Jonathan Caleb �������������������������� Disclosed no conflict of interest.
Queniat, Gurvan ����������������������������������� Disclosed no conflict of interest.
Quinn, Lauretta T. ��������������������������������� Disclosed no conflict of interest.
Qunibi, Wajeh �������������������������������������� Other Relationship: UpToDate; Research Support: ZS
Pharma, Inc.
Quon, Michael J. ���������������������������������� Disclosed no conflict of interest.
Quyyumi, Arshed A. ����������������������������� Disclosed no conflict of interest.
Radford, Elizabeth J. ���������������������������� Disclosed no conflict of interest.
Radovick, Sally ������������������������������������� Disclosed no conflict of interest.
Ragolia, Louis ��������������������������������������� Disclosed no conflict of interest.
Rahbar, Samuel ������������������������������������ Disclosed no conflict of interest.
Rajagopalan, Sujit �������������������������������� Disclosed no conflict of interest.
Ramasamy, Boominathan �������������������� Disclosed no conflict of interest.
Rameh, Lucia E. ������������������������������������ Disclosed no conflict of interest.
Randeva, Harpal S. ������������������������������ Disclosed no conflict of interest.
Ranetti, Aurelian Emil �������������������������� Advisory Panel: National Ethical Commission for the
drug’s clinical study; Research Support: Eli Lilly and
Company, Pfizer Inc., Servier; Speaker’s Bureau:
Abbott, Alfa Wasserman, Eli Lilly and Company.
Ranjani, Harish ������������������������������������� Disclosed no conflict of interest.
Rao, Ranganatha ���������������������������������� Disclosed no conflict of interest.
Raphael, Frederica ������������������������������� Disclosed no conflict of interest.
Rask-Madsen, Christian ����������������������� Disclosed no conflict of interest.
Rasmussen, Henrik S. �������������������������� Employee: ZS Pharma, Inc.; Stock/Shareholder: ZS
Pharma, Inc.
Rathjen, Thomas ���������������������������������� Disclosed no conflict of interest.
Raverdy, Violeta ����������������������������������� Disclosed no conflict of interest.
Ravishankar, Aarthi ������������������������������ Disclosed no conflict of interest.
Ravussin, Eric ��������������������������������������� Advisory Panel: Genentech, Inc., Novo Nordisk Inc.
Raymond, Ralph H. ������������������������������� Stock/Shareholder: Bristol-Myers Squibb Company.
Raz, Itamar ������������������������������������������� Research Support: AstraZeneca Pharmaceuticals LP.
Read, Linda ������������������������������������������ Disclosed no conflict of interest.
Reagan, Louise A. �������������������������������� Disclosed no conflict of interest.
Reaven, Peter D. ���������������������������������� Disclosed no conflict of interest.
Reddy, Narendra L. ������������������������������� Disclosed no conflict of interest.
Reddy, Ravi ������������������������������������������� Disclosed no conflict of interest.
Redman, Leanne M. ����������������������������� Disclosed no conflict of interest.
Reers, Christina ������������������������������������ Disclosed no conflict of interest.
Rees, Gwyn ������������������������������������������ Disclosed no conflict of interest.
Regner, Kevin R. ����������������������������������� Disclosed no conflict of interest.
Reik, Wolf ��������������������������������������������� Disclosed no conflict of interest.
Reiser, Jochen �������������������������������������� Other Relationship: Co-founders of TRISAQ, a
biopharmaceutical company aimed to develop new
therapies for kidney disease.
Renström, Frida ������������������������������������ Disclosed no conflict of interest.
Resalat, Navid �������������������������������������� Disclosed no conflict of interest.
Rewers, Arleta ������������������������������������� Disclosed no conflict of interest.
Rewers, Marian ����������������������������������� Disclosed no conflict of interest.
Reynolds, Vincent L. ����������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Rho, Jun Gi ������������������������������������������� Disclosed no conflict of interest.
Ricchiuto, Piero ������������������������������������ Disclosed no conflict of interest.
Richardson, Carolyn C. ������������������������� Disclosed no conflict of interest.
Richter, Erik A. �������������������������������������� Disclosed no conflict of interest.
Ridderstrale, Martin ����������������������������� Employee: Steno Diabetes Center A/S; Speaker’s Bureau:
Boehringer Ingelheim GmbH, Eli Lilly and Company,
GlaxoSmithKline, Johnson & Johnson, Medtronic,
Inc., Merck & Co., Inc., Novartis, Novo Nordisk A/S,
Roche Diagnostics, Sanofi-Aventis.
Riggs, Arthur ���������������������������������������� Disclosed no conflict of interest.
Rivera, Alba D. ������������������������������������� Disclosed no conflict of interest.
Robertson, R. Paul �������������������������������� Disclosed no conflict of interest.
Robinson, Matthew M. ������������������������ Disclosed no conflict of interest.
Robson, Stephen C. ������������������������������ Disclosed no conflict of interest.
Rocha, Hermano A.L. ��������������������������� Disclosed no conflict of interest.
Rocha, Milagros ����������������������������������� Disclosed no conflict of interest.
Rochat, Thierry ������������������������������������� Disclosed no conflict of interest.
Rodriguez, Carlos G. ����������������������������� Employee: Merck & Co., Inc.
Rodriguez, Henry ���������������������������������� Disclosed no conflict of interest.
Rodriguez-Cañete, Alberto ������������������� Disclosed no conflict of interest.
Rodriguez-Pacheco, Francisca ������������� Disclosed no conflict of interest.
Roger, George W. ��������������������������������� Disclosed no conflict of interest.
Rojas-Rodriguez, Raziel ����������������������� Disclosed no conflict of interest.
Rollins, Derrick K. ��������������������������������� Disclosed no conflict of interest.
Rondon, Martin ������������������������������������ Disclosed no conflict of interest.
Rosenblit, Paul D. ��������������������������������� Advisory Panel: Eli Lilly and CompanyJanssen; Research
Support: Abbott, Amgen Inc., Dexcom, Inc., Eli
Lilly and Company, MannKind Corporation, Merck,
Novo Nordisk Inc., Orexigen Therapeutics, Inc.,
Pfizer Inc.; Speaker’s Bureau: Abbott, AstraZeneca,
GlaxoSmithKline, Janssen, KOWA, Merck, Novo
Nordisk Inc., Takeda, Pfizer Inc.
Rosenkilde, Mette M. �������������������������� Disclosed no conflict of interest.
LB108
RELATIONSHIP/COMPANY
Rosenstock, Julio ��������������������������������� Advisory Panel: Boehringer Ingelheim, Bristol-Myers
Squibb, GlaxoSmithKline, Johnson & Johnson,
Lexicon, Roche; Consultant: Boehringer Ingelheim,
Bristol-Myers Squibb, GlaxoSmithKline, Johnson
& Johnson, Lexicon, Roche; Research Support:
AstraZeneca, Boehringer Ingelheim, Bristol-Myers
Squibb, GlaxoSmithKline, Johnson & Johnson,
Lexicon, Pfizer, Roche.
Rosman, Paul M. ���������������������������������� Advisory Panel: LabStyle Innovations Ltd; Consultant:
LabStyle Innovations Ltd; Research Support:
LabStuke Innovations Ltd; Speaker’s Bureau: LabStyle
Innovations Ltd.
Ross-Degnan, Dennis ��������������������������� Disclosed no conflict of interest.
Rossi, Luca ������������������������������������������� Disclosed no conflict of interest.
Rother, Kristina I. ���������������������������������� Disclosed no conflict of interest.
Rountree, Austin ���������������������������������� Disclosed no conflict of interest.
Roust, Lori R. ���������������������������������������� Disclosed no conflict of interest.
Rovira-Llopis, Susana �������������������������� Disclosed no conflict of interest.
Roy, Anirban ����������������������������������������� Employee: Medtronic, Inc.; Stock/Shareholder: Medtronic,
Inc.
Roy-Duval, Christine ���������������������������� Employee: Sanofi; Stock/Shareholder: Sanofi.
Ruan, Yijun ������������������������������������������� Disclosed no conflict of interest.
Rubio-Puchol, Olalla ����������������������������� Disclosed no conflict of interest.
Ruetten, Hartmut ��������������������������������� Employee: Sanofi U.S.; Stock/Shareholder: Sanofi U.S.
Ruiz, Tiffany ������������������������������������������ Disclosed no conflict of interest.
Russell, Steven J. �������������������������������� Advisory Panel: Tandem Diabetes Care, Inc.; Consultant:
Medtronic, Inc., Sanofi U.S.; Other Relationship:
Abbott Diabetes Care, Dexcom, Inc., Eli Lilly and
Company, Insulet Corporation, Medtronic, Inc., Sanofi
U.S., Tandem Diabetes Care, Inc.; Research Support:
Abbott Diabetes Care, Inc.
Rutkowski, Joseph M. ������������������������� Disclosed no conflict of interest.
Ryan, Alexander J. ������������������������������� Disclosed no conflict of interest.
Rydén, Lars ������������������������������������������� Consultant: Astra Zeneca, Bristol-Myers Squibb Company,
Hoffman-La Roche Limited; Research Support: Astra
Zeneca, Hoffman-La Roche Limited.
Sacks, Frank M. ������������������������������������ Disclosed no conflict of interest.
Sackstein, Robert ��������������������������������� Disclosed no conflict of interest.
Saghatelian, Alan �������������������������������� Disclosed no conflict of interest.
Saito, Tsugumichi ��������������������������������� Disclosed no conflict of interest.
Sakaguchi, Masaji ������������������������������� Disclosed no conflict of interest.
Sakai, Shinobu ������������������������������������� Disclosed no conflict of interest.
Sakimura, Kenji ������������������������������������ Disclosed no conflict of interest.
Sakuma, Toshie ������������������������������������ Disclosed no conflict of interest.
Saleh, Farrah ���������������������������������������� Disclosed no conflict of interest.
Sales, Vicencia M. ������������������������������� Disclosed no conflict of interest.
Salomon, Arthur ����������������������������������� Disclosed no conflict of interest.
Salsali, Afshin �������������������������������������� Employee: Boehringer Ingelheim GmbH.
Samocha-Bonet, Dorit �������������������������� Disclosed no conflict of interest.
Samovski, Dmitri ���������������������������������� Disclosed no conflict of interest.
Samuel, Varman T. ������������������������������� Disclosed no conflict of interest.
Sanchez, Rosalia ���������������������������������� Disclosed no conflict of interest.
Sandall, Jane ��������������������������������������� Disclosed no conflict of interest.
Sanders, Thomas A.B. �������������������������� Advisory Panel: Global Dairy Platform, Heinz PLC,
Malaysian Palm Oil Board; Consultant: Natural
Hydration Council.
Santos, Rosa Ferreira ��������������������������� Disclosed no conflict of interest.
Saremi, Aramesh ��������������������������������� Disclosed no conflict of interest.
Sasaki, Shugo �������������������������������������� Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Bristol-Myers Squibb Company,
Daiichi-Sankyo Co., Ltd., Eli Lilly Japan K.K.,
Johnson & Johnson, Kissei Pharmaceutical Co., Ltd.,
Merck Sharp & Dohme, Mitsubishi Tanabe Pharma
Corporation, Novartis Pharmaceuticals Corporation,
Novo Nordisk Inc., Ono Pharmaceutical Co., Ltd.,
Sanofi U.S., Sumimoto Dainippon Pharma Co., Ltd.,
Takeda Pharmaceutical Company Limited.
Sathyanarayana, Padma ���������������������� Disclosed no conflict of interest.
Satin-Smith, Marta ������������������������������ Disclosed no conflict of interest.
Sattar, Naveed ������������������������������������� Consultant: AstraZeneca, Boehringer Ingelheim GmbH,
Bristol-Myers Squibb, Sanofi U.S.
Savage, Peter ��������������������������������������� Disclosed no conflict of interest.
Sawicki, Konrad T. �������������������������������� Disclosed no conflict of interest.
Scalia, Rosario ������������������������������������� Disclosed no conflict of interest.
Schade, David S. ���������������������������������� Disclosed no conflict of interest.
Schalkwijk, Casper G. �������������������������� Disclosed no conflict of interest.
Schatz, Desmond ��������������������������������� Disclosed no conflict of interest.
Scherer, Philipp ������������������������������������ Disclosed no conflict of interest.
Schindler, Christian ������������������������������ Disclosed no conflict of interest.
Schliess, Freimut ���������������������������������� Disclosed no conflict of interest.
Schneider, Martin ��������������������������������� Disclosed no conflict of interest.
Schönke, Milena ���������������������������������� Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Schreiber, Stefanie ������������������������������� Disclosed no conflict of interest.
Schulz, Christina-Alexandra ����������������� Disclosed no conflict of interest.
Schurmann, Claudia ����������������������������� Disclosed no conflict of interest.
Schwede, Frank ������������������������������������ Disclosed no conflict of interest.
Scirica, Benjamin M. ���������������������������� Research Support: AstraZeneca Pharmaceuticals LP.
Scott, Donald ��������������������������������������� Disclosed no conflict of interest.
Scott, Laura ������������������������������������������ Disclosed no conflict of interest.
Scott, Robert A. ������������������������������������ Disclosed no conflict of interest.
Screaton, Robert A. ������������������������������ Disclosed no conflict of interest.
Sczelecki, Sarah ����������������������������������� Disclosed no conflict of interest.
Seed, Paul T. ����������������������������������������� Disclosed no conflict of interest.
Seely, Ellen W. ������������������������������������� Disclosed no conflict of interest.
Segal, Jodi ������������������������������������������� Disclosed no conflict of interest.
Segal, Karen R. ������������������������������������ Employee: Mesoblast Inc.
Seielstad, Mark ������������������������������������ Disclosed no conflict of interest.
Sekar, Sakthivel ������������������������������������ Disclosed no conflict of interest.
Selbach, Matthias �������������������������������� Disclosed no conflict of interest.
Seo, Dongju ������������������������������������������ Disclosed no conflict of interest.
Seo, Ji A. ���������������������������������������������� Disclosed no conflict of interest.
Seo, Ji Hye ������������������������������������������� Disclosed no conflict of interest.
Seramani, Sankar ��������������������������������� Disclosed no conflict of interest.
Sereika, Susan M. �������������������������������� Disclosed no conflict of interest.
Serné, Erik H. ��������������������������������������� Disclosed no conflict of interest.
Serpas, Lilian ��������������������������������������� Disclosed no conflict of interest.
Sesso, Howard D. �������������������������������� Research Support: Pfizer Inc.
Sever, Sanja ����������������������������������������� Other Relationship: Co-founder of TRISAQ, a
biopharmaceutical company aimed to develop new
therapies for kidney disease.
Severini, Cinzia ������������������������������������ Disclosed no conflict of interest.
Sha, Haibo �������������������������������������������� Disclosed no conflict of interest.
Shah, Chirag P. ������������������������������������� Consultant: Regeneron Pharmaceuticals, Inc.
Shah, Kaanan ��������������������������������������� Disclosed no conflict of interest.
Shah, Neha ������������������������������������������ Disclosed no conflict of interest.
Shah, Parag ������������������������������������������ Disclosed no conflict of interest.
Shah, Viral �������������������������������������������� Disclosed no conflict of interest.
Shamsi, Farnaz ������������������������������������� Disclosed no conflict of interest.
Shanahan, William ������������������������������ Employee: Arena Pharmaceuticals.
Shang, Jin �������������������������������������������� Employee: Merck & Co., Inc.
Shankar, Sudha S. �������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Shanmugham, Satya ���������������������������� Disclosed no conflict of interest.
Shao, Yimin ������������������������������������������ Disclosed no conflict of interest.
Sharifi, Amin ���������������������������������������� Disclosed no conflict of interest.
Sharma, Naveen ���������������������������������� Disclosed no conflict of interest.
Sharma, Pragya ������������������������������������ Disclosed no conflict of interest.
Shaw, Collin ����������������������������������������� Disclosed no conflict of interest.
She, Jin-Xiong �������������������������������������� Disclosed no conflict of interest.
Shebani, Zachariah ������������������������������ Disclosed no conflict of interest.
Sheehan, John ������������������������������������� Employee: AstraZeneca Pharmaceuticals LP.
Shehata, Kristal ����������������������������������� Disclosed no conflict of interest.
Shepherd, Peter ����������������������������������� Disclosed no conflict of interest.
Sherwin, Robert S. ������������������������������� Advisory Panel: AstraZeneca Pharmaceuticals LP;
Consultant: Bristol-Myers Squibb Company, Eli Lilly
and Company, McKinsey & Company, Merck & Co.,
Inc., Novartis Pharmaceuticals Corporation; Other
Relationship: MannKind Corporation, Merck & Co.,
Inc., Novartis Pharmaceuticals Corporation; Research
Support: Merck & Co., Inc.
Shi, Hang ���������������������������������������������� Research Support: NuSirt Biopharma.
Shibusawa, Ryo ����������������������������������� Disclosed no conflict of interest.
Shimo, Naoki ���������������������������������������� Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Bristol-Myers Squibb Company,
Daiichi-Sankyo Co., Ltd., Eli Lilly and Company,
Johnson & Johnson, Kissei Pharmaceutical Co., Ltd.,
Merck Sharp & Dohme, Mitsubishi Tanabe Pharma
Corporation, Novartis Pharmaceuticals Corporation,
Novo Nordisk Inc., Ono Pharmaceutical Co., Ltd.,
Sanofi U.S., Sumimoto Dainippon Pharma Co., Ltd.,
Takeda Pharmaceutical Company Limited.
Shimoda, Yoko ������������������������������������� Disclosed no conflict of interest.
Shimomura, Iichiro ������������������������������� Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Daiichi-Sankyo Co., Ltd., Eli
Lilly Japan K.K., Kissei Pharmaceutical Co., Ltd.,
Kowa Pharmaceuticals, Merck Sharp & Dohme,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Novo Nordisk A/S, Ono
Pharmaceutical Co., Ltd., Sanofi U.S., Shionogi Inc.,
Takeda Pharmaceutical Company Limited.
Shin, Jeong Jae ����������������������������������� Disclosed no conflict of interest.
Shin, Myung ����������������������������������������� Employee: Merck & Co., Inc.
Shon, Ho Sang ������������������������������������� Disclosed no conflict of interest.
LB109
AUTHOR DISCLOSURE
AUTHOR
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
Short, Kevin R. ������������������������������������� Disclosed no conflict of interest.
Shulman, Gerald I. ������������������������������� Disclosed no conflict of interest.
Shungin, Dmitry ����������������������������������� Disclosed no conflict of interest.
Shyong, Tai E. ��������������������������������������� Disclosed no conflict of interest.
Siddiqui, Uzma Mohammad ����������������� Disclosed no conflict of interest.
Siegle, Greg J. ������������������������������������� Disclosed no conflict of interest.
Sievers, Felix ���������������������������������������� Disclosed no conflict of interest.
Sigrist, Kirsten ������������������������������������� Disclosed no conflict of interest.
Silk, Maria E. ���������������������������������������� Employee: Eli Lilly and Company; Stock/Shareholder: Eli
Lilly and Company.
Silvia, Maria Elizabeth Rossi ��������������� Disclosed no conflict of interest.
Sim, Thuan Kai Jelvin �������������������������� Disclosed no conflict of interest.
Simell, Olli G. ��������������������������������������� Disclosed no conflict of interest.
Siminerio, Linda ����������������������������������� Disclosed no conflict of interest.
Simmons, Rebecca A. �������������������������� Disclosed no conflict of interest.
Sims, Emily K. �������������������������������������� Disclosed no conflict of interest.
Singh, Avinainder ��������������������������������� Disclosed no conflict of interest.
Singh, Bhupinder ���������������������������������� Employee: ZS Pharma, Inc.; Stock/Shareholder: ZS
Pharma, Inc.
Singh, Kiran Pal ������������������������������������ Disclosed no conflict of interest.
Singh, Maneet ������������������������������������� Disclosed no conflict of interest.
Singh, Sasha ���������������������������������������� Disclosed no conflict of interest.
Singhal, Jyotsana �������������������������������� Disclosed no conflict of interest.
Singhal, Sharad S. ������������������������������� Disclosed no conflict of interest.
Sinha, Manasi �������������������������������������� Disclosed no conflict of interest.
Sinha, Rajita ����������������������������������������� Disclosed no conflict of interest.
Sinha, Vikram P. ������������������������������������ Employee: MacroGenics, Inc.
Sivapalaratnam, Sutesh S. ������������������ Disclosed no conflict of interest.
Sjöstrand, Annika ��������������������������������� Disclosed no conflict of interest.
Skerrett, Donna ������������������������������������ Employee: Mesoblast Inc.
Skjøth, Trine V. �������������������������������������� Employee: Novo Nordisk A/S; Stock/Shareholder: Novo
Nordisk A/S.
Skokos, Dimitris ����������������������������������� Disclosed no conflict of interest.
Sleeman, Mark ������������������������������������� Disclosed no conflict of interest.
Smith, Brian ����������������������������������������� Disclosed no conflict of interest.
Smith, Steven R. ���������������������������������� Disclosed no conflict of interest.
Smulders, Yvo M. ��������������������������������� Disclosed no conflict of interest.
Sohler, Nancy ��������������������������������������� Disclosed no conflict of interest.
Sohn, Hae-Young ��������������������������������� Disclosed no conflict of interest.
Solhjou, Zhabiz ������������������������������������� Disclosed no conflict of interest.
Somesh, Baggavalli P. �������������������������� Disclosed no conflict of interest.
Son, Jee Woong ����������������������������������� Disclosed no conflict of interest.
Son, Moon-Ho �������������������������������������� Disclosed no conflict of interest.
Song, Dae-Kyu ������������������������������������� Disclosed no conflict of interest.
Song, Yiqing ����������������������������������������� Disclosed no conflict of interest.
Sontheimer, Alexandra ������������������������� Disclosed no conflict of interest.
Sorrenson, Brie ������������������������������������ Disclosed no conflict of interest.
Sosenko, Jay M. ���������������������������������� Disclosed no conflict of interest.
Souhami, Elisabeth ������������������������������ Employee: Sanofi; Stock/Shareholder: Sanofi.
Soumerai, Stephen ������������������������������ Disclosed no conflict of interest.
Southam, Lorraine �������������������������������� Disclosed no conflict of interest.
Souza, Sandra C. ���������������������������������� Employee: Merck & Co., Inc.
Sowers, James R. �������������������������������� Disclosed no conflict of interest.
Sparre-Ulrich, Alexander H. ����������������� Disclosed no conflict of interest.
Speight, Jane ��������������������������������������� Disclosed no conflict of interest.
Sperling, Laurence S. ��������������������������� Disclosed no conflict of interest.
Spiegelman, Donna ������������������������������ Disclosed no conflict of interest.
Spirakis, Ruth ��������������������������������������� Disclosed no conflict of interest.
Staels, Bart ������������������������������������������ Disclosed no conflict of interest.
Staimez, Lisa R. ������������������������������������ Disclosed no conflict of interest.
Stansfield, Brain ����������������������������������� Disclosed no conflict of interest.
Staten, Myrlene ����������������������������������� Disclosed no conflict of interest.
Stefanovski, Darko ������������������������������� Disclosed no conflict of interest.
Steinbeck, Gerhard ������������������������������ Disclosed no conflict of interest.
Stella, Peter ����������������������������������������� Employee: Sanofi.
Stephens, Ella �������������������������������������� Disclosed no conflict of interest.
Stephens, Jacqueline M. ��������������������� Disclosed no conflict of interest.
Stepp, David W. ����������������������������������� Disclosed no conflict of interest.
Stier, Christine K. ��������������������������������� Disclosed no conflict of interest.
Stirban, Alin ����������������������������������������� Disclosed no conflict of interest.
Stirrups, Kathy ������������������������������������� Disclosed no conflict of interest.
Stitzel, Michael L. �������������������������������� Disclosed no conflict of interest.
Stolz, Daiana ���������������������������������������� Disclosed no conflict of interest.
Stram, Daniel O. ����������������������������������� Disclosed no conflict of interest.
Straznicky, Nora ����������������������������������� Disclosed no conflict of interest.
Stringham, Heather ������������������������������ Disclosed no conflict of interest.
Strongman, Helen �������������������������������� Employee: Clinical Practice Research Datalink Group
performs financially supported studies for several
pharmaceutical companies including Takeda
Development Centre Europe.
Su, Xiong ���������������������������������������������� Disclosed no conflict of interest.
Suarez-Cuervo, Catalina ���������������������� Disclosed no conflict of interest.
Subkhangulova, Aygul �������������������������� Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Suh, Kyung-Shin ����������������������������������� Disclosed no conflict of interest.
Sumner, Anne ��������������������������������������� Disclosed no conflict of interest.
Sun, Chenglin ��������������������������������������� Disclosed no conflict of interest.
Sun, Li-Ping ������������������������������������������ Disclosed no conflict of interest.
Sun, Qi �������������������������������������������������� Disclosed no conflict of interest.
Sun, Wanqing ��������������������������������������� Disclosed no conflict of interest.
Sun, Xiao Jian �������������������������������������� Disclosed no conflict of interest.
Sundaresan, Sinju �������������������������������� Disclosed no conflict of interest.
Sundelin, Elias ������������������������������������� Disclosed no conflict of interest.
Super, Dennis ��������������������������������������� Disclosed no conflict of interest.
Sury, Matthias �������������������������������������� Disclosed no conflict of interest.
Svendsen, Berit ������������������������������������ Disclosed no conflict of interest.
Sweet, Ian �������������������������������������������� Disclosed no conflict of interest.
Syed, Ismail ������������������������������������������ Disclosed no conflict of interest.
Synold, Timothy ������������������������������������ Disclosed no conflict of interest.
Szanto, Ildiko ���������������������������������������� Disclosed no conflict of interest.
Tabatabai, Niloofar M. ������������������������� Disclosed no conflict of interest.
Tahara, Yumiko ������������������������������������� Disclosed no conflict of interest.
Tailleux, Anne ��������������������������������������� Disclosed no conflict of interest.
Taitel, Michael ������������������������������������� Disclosed no conflict of interest.
Takahara, Mitsuyoshi ��������������������������� Research Support: Astellas Pharma US, Inc., Boston
Scientific Corporation, Johnson & Johnson,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Otsuka Pharmaceutical
Co., Ltd., Sanofi U.S., Takeda Pharmaceutical
Company Limited.
Takahashi, Yusuke �������������������������������� Disclosed no conflict of interest.
Takaike, Hiroko ������������������������������������� Disclosed no conflict of interest.
Tam, Charmaine ����������������������������������� Disclosed no conflict of interest.
Tamanini, Filippo ���������������������������������� Disclosed no conflict of interest.
Tan, Ruo-Ding ��������������������������������������� Consultant: Intarcia Therapeutics, Inc.
Tanenberg, Robert J. ���������������������������� Disclosed no conflict of interest.
Tang, Cheng Cai ����������������������������������� Employee: Eli Lilly and Company.
Tang, Huilin ������������������������������������������ Disclosed no conflict of interest.
Tang, Yuefeng ��������������������������������������� Disclosed no conflict of interest.
Tantawi, Hyam R. ��������������������������������� Disclosed no conflict of interest.
Tattikota, Sudhir Gopal ������������������������ Disclosed no conflict of interest.
Taylor, Ann �������������������������������������������� Employee: Novartis Pharmaceuticals Corporation.
Taylor, D. Leland ����������������������������������� Disclosed no conflict of interest.
Taylor, Hugh S. ������������������������������������� Disclosed no conflict of interest.
Teague, April ���������������������������������������� Disclosed no conflict of interest.
Temprosa, Marinella ���������������������������� Disclosed no conflict of interest.
Tennagels, Norbert ������������������������������� Employee: Sanofi-Aventis Deutschland GmbH.
Tersey, Sarah ���������������������������������������� Disclosed no conflict of interest.
Thaker, Vidhu ���������������������������������������� Disclosed no conflict of interest.
Theisen, Daniel ������������������������������������ Disclosed no conflict of interest.
Theiss, Hans D. ������������������������������������ Disclosed no conflict of interest.
Theoharis, Stamatis ����������������������������� Disclosed no conflict of interest.
Thevenet, Julien ���������������������������������� Disclosed no conflict of interest.
Thibodeau, Asa ������������������������������������ Disclosed no conflict of interest.
Thiel, Steffen ��������������������������������������� Disclosed no conflict of interest.
Thombare, Aparna ������������������������������� Disclosed no conflict of interest.
Thompson, David M. ���������������������������� Disclosed no conflict of interest.
Thompson, Michael ����������������������������� Disclosed no conflict of interest.
Tian, Suyan ������������������������������������������� Disclosed no conflict of interest.
Tinahones, Francisco J. ������������������������ Advisory Panel: AstraZeneca Pharmaceuticals LP,
Boehringer Ingelheim Pharmaceuticals, Inc., BristolMyers Squibb Company, Eli Lilly and Company,
GlaxoSmithKline, Hoffman LaRoche, Merck, Merck
Sharp & Dohme Limited, Novartis Pharmaceuticals
Corporation, Novo Nordisk, Inc., Sanofi; Consultant:
AstraZeneca Pharmaceuticals LP, Boehringer
Ingelheim Pharmaceuticals, Inc., Bristol-Myers Squibb
Company, Eli Lilly and Company, GlaxoSmithKline,
Hoffman LaRoche, Merck, Merck Sharp & Dohme
Limited, Novartis Pharmaceuticals Corporation, Novo
Nordisk, Inc., Sanofi; Research Support: AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Bristol-Myers Squibb Company,
Eli Lilly and Company, GlaxoSmithKline, Hoffman
LaRoche, Merck, Merck Sharp & Dohme Limited,
Novartis Pharmaceuticals Corporation, Novo Nordisk,
Inc., Sanofi.
Tinsley, Liane ���������������������������������������� Disclosed no conflict of interest.
Tique, Claudia R. ���������������������������������� Disclosed no conflict of interest.
Tobacman, Joanne K. ��������������������������� Disclosed no conflict of interest.
Tomokazu, Nunoue ������������������������������� Disclosed no conflict of interest.
Tong, Jenny ������������������������������������������ Disclosed no conflict of interest.
Tonks, Katherine ����������������������������������� Disclosed no conflict of interest.
Tonne, Jason M. ����������������������������������� Disclosed no conflict of interest.
Toppari, Jorma ������������������������������������� Disclosed no conflict of interest.
Torres, Jason M. ���������������������������������� Disclosed no conflict of interest.
Torres, Lizardo �������������������������������������� Disclosed no conflict of interest.
LB110
RELATIONSHIP/COMPANY
AUTHOR
Toschi, Elena ���������������������������������������� Disclosed no conflict of interest.
Toumilehto, Jaakko ������������������������������ Disclosed no conflict of interest.
Trautmann, Michael ����������������������������� Disclosed no conflict of interest.
Trawley, Steve �������������������������������������� Disclosed no conflict of interest.
Trevino, Michelle B. ����������������������������� Disclosed no conflict of interest.
Tripaldi, Juliet R. ���������������������������������� Disclosed no conflict of interest.
Tripathy, Devjit T. ���������������������������������� Disclosed no conflict of interest.
Triplett, Eric W. ������������������������������������� Disclosed no conflict of interest.
Tryggestad, Jeanie B. ��������������������������� Disclosed no conflict of interest.
Tsachalina, Theofaneia ������������������������ Disclosed no conflict of interest.
Tsai, Katherine ������������������������������������� Employee: MedImmune, LLC.
Tschöp, Matthias ���������������������������������� Disclosed no conflict of interest.
Tseng, Eva �������������������������������������������� Disclosed no conflict of interest.
Tseng, Yu-Hua �������������������������������������� Disclosed no conflict of interest.
Tu, Weiping ������������������������������������������ Disclosed no conflict of interest.
Tumlin, James A. ���������������������������������� Advisory Panel: Eli Lilly and Company; Consultant: Eli
Lilly and Company; Research Support: Eli Lilly and
Company, Genkyotex, Gilead, Janssen Pharmaceutical
Companies of Johnson & Johnson, Mallinckrodt
Pharmaceuticals.
Tung, Gregory ��������������������������������������� Disclosed no conflict of interest.
Tuomilehto, Jaakko ������������������������������ Disclosed no conflict of interest.
Turcot, Valerie �������������������������������������� Disclosed no conflict of interest.
Tuttle, Edward �������������������������������������� Consultant: Intarcia Therapeutics, Inc.
Tuttle, Katherine ����������������������������������� Consultant: Amgen Inc., Eli Lilly and Company, NOXXON
Pharma AG.
Tütüncüoglu, Aliye P. ���������������������������� Disclosed no conflict of interest.
Ucar, Duygu ������������������������������������������ Disclosed no conflict of interest.
Uchigata, Yasuko ��������������������������������� Disclosed no conflict of interest.
Uddén Hemmingsson, Joanna ������������� Advisory Panel: Novo Nordisk A/S, Sanofi U.S.; Other
Relationship: Novo Nordisk A/S, Sanofi U.S.;
Research Support: InfoCare.
Umpierrez, Guillermo E. ����������������������� Consultant: Boehringer Ingelheim Pharmaceuticals, Inc.,
Merck Sharp & Dohme, Novo Nordisk Inc., Regeneron
Pharmaceuticals, Inc., Sanofi U.S.; Research Support:
Boehringer Ingelheim Pharmaceuticals, Inc., Merck
Sharp & Dohme, National Institutes of Health, Novo
Nordisk Inc., Regeneron Pharmaceuticals, Inc., Sanofi
U.S.
Üner, Aykut G. �������������������������������������� Disclosed no conflict of interest.
Unterman, Terry G. ������������������������������� Disclosed no conflict of interest.
Uppal, Karan ���������������������������������������� Disclosed no conflict of interest.
Uribe-Bruce, Liliana ����������������������������� Employee: Profil Institute for Clinical Research, Inc.
Uribe-Wiechers, Ana C. ����������������������� Disclosed no conflict of interest.
Vaidya, Anand �������������������������������������� Disclosed no conflict of interest.
Valdes, Jorge ��������������������������������������� Employee: Dexcom, Inc.
Valdes, Sergio �������������������������������������� Disclosed no conflict of interest.
Valera, Jose ����������������������������������������� Disclosed no conflict of interest.
van Hinsbergh, Victor W.M. ����������������� Disclosed no conflict of interest.
van Poelgeest, Erik M. ������������������������� Disclosed no conflict of interest.
van Polanen, Nynke ����������������������������� Disclosed no conflict of interest.
VanderHeiden, Anna ���������������������������� Disclosed no conflict of interest.
Vanhoutte, Jonathan ���������������������������� Disclosed no conflict of interest.
Vantyghem, Marie Christine ���������������� Disclosed no conflict of interest.
Vargas, Gabriela ����������������������������������� Disclosed no conflict of interest.
Vasavada, Rupangi C. �������������������������� Disclosed no conflict of interest.
Vassileva, Maria T. ������������������������������� Disclosed no conflict of interest.
Vasudevan, Sudha �������������������������������� Disclosed no conflict of interest.
Vazquez-Pedreño, Luis ������������������������� Disclosed no conflict of interest.
Vehik, Kendra ��������������������������������������� Disclosed no conflict of interest.
Vella, Adrian ����������������������������������������� Consultant: Bristol-Myers Squibb Company, Genentech,
Inc., Novartis Pharmaceuticals Corporation, Sanofi
U.S., XOMA Corporation; Research Support: BioKier,
Daiichi-Sankyo Co., Ltd., GI Dynamics, Inc., Merck &
Co., Inc., Novartis Pharmaceuticals Corporation.
Vellanki, Priyathama ���������������������������� Disclosed no conflict of interest.
Vendelbo, Mikkel H. ����������������������������� Disclosed no conflict of interest.
Venkataranganna, Marikunte V. ����������� Disclosed no conflict of interest.
Vento, Flor �������������������������������������������� Disclosed no conflict of interest.
Verma, Mahesh Kumar ������������������������ Disclosed no conflict of interest.
Veyrat-Durebex, Christelle ������������������� Disclosed no conflict of interest.
Victor, Victor M. ����������������������������������� Disclosed no conflict of interest.
Vikentieva, Elena ���������������������������������� Disclosed no conflict of interest.
Villa, Stephanie R. �������������������������������� Disclosed no conflict of interest.
Villanes, Sofia �������������������������������������� Disclosed no conflict of interest.
VIllena, Lorena ������������������������������������� Disclosed no conflict of interest.
Vilsbøll, Tina ����������������������������������������� Advisory Panel: AstraZeneca Pharmaceuticals LP,
Boehringer Ingelheim Pharmaceuticals, Inc.,
Bristol-Myers Squibb Company, Eli Lilly and
Company, GI Dynamics, Inc., Merck Sharp & Dohme,
Novo Nordisk A/S, Sanofi Pasteur SA, Takeda
Pharmaceutical Company Limited; Consultant:
AstraZeneca Pharmaceuticals LP, Boehringer
RELATIONSHIP/COMPANY
Ingelheim Pharmaceuticals, Inc., Bristol-Myers
Squibb Company, Eli Lilly and Company, Merck
Sharp & Dohme, Novartis AG, Novo Nordisk A/S,
Sanofi Pasteur SA, Takeda Pharmaceutical Company
Limited, Zealand Pharma A/S; Speaker’s Bureau:
AstraZeneca Pharmaceuticals LP, Boehringer
Ingelheim Pharmaceuticals, Inc., Bristol-Myers Squibb
Company, Eli Lilly and Company, Merck Sharp &
Dohme, Novo Nordisk A/S, Sanofi Pasteur SA, Takeda
Pharmaceutical Company Limited, Zealand Pharma
A/S.
Vinik, Aaron I. ��������������������������������������� Advisory Panel: Merck Sharp & Dohme, Pfizer Inc.;
Consultant: Isis Pharmaceuticals, Inc., Merck Sharp
& Dohme, NeuroMetrix, Inc., Pamlab-A Nestle
Health Science Company, Pfizer Inc.; Research
Support: American Diabetes Association, Impeto
Medical, Ipsen Bioscience, Inc., Intarcia Therapeutics,
Inc., National Institutes of Health, Novo Nordisk
Inc., Sanofi U.S., ViroMed Laboratories Inc., VM
Biopharma, Pfizer Inc.; Speaker’s Bureau: Merck Sharp
& Dohme, Pamlab-A Nestle Health Science Company.
Vishwanath, Anu ���������������������������������� Disclosed no conflict of interest.
Viswanathan, Prabhakar ���������������������� Disclosed no conflict of interest.
von Eckardstein, Arnold ����������������������� Disclosed no conflict of interest.
von Meyenn, Ferdinand ����������������������� Disclosed no conflict of interest.
von Oettingen, Julia ����������������������������� Disclosed no conflict of interest.
von Ziegler, Franz ��������������������������������� Disclosed no conflict of interest.
Voskanyan, Gayane ������������������������������ Employee: Medtronic MiniMed, Inc.; Stock/Shareholder:
Medtronic, Inc.
Wada, Asuka ���������������������������������������� Disclosed no conflict of interest.
Wada, Jun �������������������������������������������� Disclosed no conflict of interest.
Walker, Tomas �������������������������������������� Employee: Dexcom, Inc.
Walter, Mary F. ������������������������������������� Disclosed no conflict of interest.
Wanders, Desiree �������������������������������� Disclosed no conflict of interest.
Wang, Aihua ���������������������������������������� Disclosed no conflict of interest.
Wang, Bingshun ����������������������������������� Disclosed no conflict of interest.
Wang, Fang ������������������������������������������ Disclosed no conflict of interest.
Wang, Fei ��������������������������������������������� Disclosed no conflict of interest.
Wang, Guang ��������������������������������������� Disclosed no conflict of interest.
Wang, Guixia ���������������������������������������� Disclosed no conflict of interest.
Wang, Haiyan ��������������������������������������� Disclosed no conflict of interest.
Wang, Hongliang ��������������������������������� Disclosed no conflict of interest.
Wang, Liangsu ������������������������������������� Employee: Merck & Co., Inc.
Wang, Lu ���������������������������������������������� Disclosed no conflict of interest.
Wang, Ningjian ������������������������������������ Disclosed no conflict of interest.
Wang, Pin-Wen ������������������������������������ Employee: Genentech, Inc.
Wang, Renwei �������������������������������������� Disclosed no conflict of interest.
Wang, Sheng-Ping ������������������������������� Employee: Merck & Co., Inc.
Wang, Shuxia ��������������������������������������� Disclosed no conflict of interest.
Wang, Tiange ��������������������������������������� Disclosed no conflict of interest.
Wang, Tiansheng ��������������������������������� Disclosed no conflict of interest.
Wang, Wang ���������������������������������������� Disclosed no conflict of interest.
Wang, Wei ������������������������������������������� Disclosed no conflict of interest.
Wang, Xiaojin ��������������������������������������� Disclosed no conflict of interest.
Wang, Xiaolin ��������������������������������������� Disclosed no conflict of interest.
Wang, Xinye ����������������������������������������� Disclosed no conflict of interest.
Wang, Ying ������������������������������������������� Disclosed no conflict of interest.
Ward, Glenn M. ������������������������������������ Disclosed no conflict of interest.
Ward, W. Kenneth �������������������������������� Advisory Panel: Xeris Pharmaceuticals, Inc.; Employee:
Pacific Diabetes Technologies, Inc.; Stock/
Shareholder: Pacific Diabetes Technologies, Inc.
Wardecki, Marek ���������������������������������� Employee: Sanofi; Stock/Shareholder: Sanofi.
Warden, Charles ���������������������������������� Disclosed no conflict of interest.
Wardle, Jane ���������������������������������������� Disclosed no conflict of interest.
Warren, Graham ����������������������������������� Employee: LifeScan, Inc.
Watada, Hirotaka ��������������������������������� Research Support: Astellas Pharma US, Inc., AstraZeneca
Pharmaceuticals LP, Boehringer Ingelheim
Pharmaceuticals, Inc., Daiichi-Sankyo Co., Ltd.,
Eli Lilly Japan K.K., Johnson & Johnson, Kissei
Pharmaceutical Co., Ltd., Merck Sharp & Dohme,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Novo Nordisk Inc.,
Ono Pharmaceutical Co., Ltd., Sanofi U.S., Takeda
Pharmaceutical Company Limited.
Watanabe, Eiko ������������������������������������ Disclosed no conflict of interest.
Watanabe, Richard M. ������������������������� Disclosed no conflict of interest.
Watson, Karol E. ���������������������������������� Disclosed no conflict of interest.
Webb, Seamus ������������������������������������� Disclosed no conflict of interest.
Weber, Mary Beth �������������������������������� Disclosed no conflict of interest.
Wedick, Nicole M. ������������������������������� Disclosed no conflict of interest.
Weindruch, Richard ������������������������������ Disclosed no conflict of interest.
Weintraub, Daniel S. ���������������������������� Disclosed no conflict of interest.
Weintraub, Neal L. ������������������������������� Disclosed no conflict of interest.
LB111
AUTHOR DISCLOSURE
AUTHOR
AUTHOR DISCLOSURE
AUTHOR
RELATIONSHIP/COMPANY
Welch, Ryan ����������������������������������������� Disclosed no conflict of interest.
Welters, Alena ������������������������������������� Disclosed no conflict of interest.
Wen, Xiaoquan ������������������������������������� Disclosed no conflict of interest.
Weng, Jianping ������������������������������������ Disclosed no conflict of interest.
Wentzell, Katherine ����������������������������� Disclosed no conflict of interest.
West, Shauna ��������������������������������������� Employee: UCB Pharma.
Westcott, Gregory P. ���������������������������� Disclosed no conflict of interest.
Wharam, James F. ������������������������������� Disclosed no conflict of interest.
Wheeler, Heather E. ����������������������������� Disclosed no conflict of interest.
Wheeler, Michael B. ���������������������������� Disclosed no conflict of interest.
Whelan, Mary �������������������������������������� Disclosed no conflict of interest.
White, Ariel ������������������������������������������ Disclosed no conflict of interest.
White, Ursula ��������������������������������������� Disclosed no conflict of interest.
Whitlock, Kathryn B. ���������������������������� Disclosed no conflict of interest.
Whitworth, Melissa K. ������������������������� Disclosed no conflict of interest.
Willett, Walter C. ��������������������������������� Disclosed no conflict of interest.
Williams, Michelle ������������������������������� Disclosed no conflict of interest.
Williams, Rachael �������������������������������� Employee: Clinical Practice Research Datalink Group
performs financially supported studies for several
pharmaceutical companies including Takeda
Development Centre Europe.
Williamson, Donald A. ������������������������� Disclosed no conflict of interest.
Willnow, Thomas ��������������������������������� Disclosed no conflict of interest.
Wilson, Lisa ����������������������������������������� Disclosed no conflict of interest.
Wiltshire, Esko ������������������������������������� Disclosed no conflict of interest.
Winkler, Thomas W. ����������������������������� Disclosed no conflict of interest.
Winters, Alexandra H. ������������������������� Disclosed no conflict of interest.
Wisherd, Chris ������������������������������������� Disclosed no conflict of interest.
Wnendt, Stephan ��������������������������������� Disclosed no conflict of interest.
Woerdeman, Jorn �������������������������������� Disclosed no conflict of interest.
Woerle, Hans J. ����������������������������������� Employee: Boehringer Ingelheim GmbH.
Wohlfart, Paulus ���������������������������������� Employee: Sanofi-Aventis Deutschland GmbH.
Wojtaszewski, Jørgen F.P. �������������������� Disclosed no conflict of interest.
Wolford, Brooke ����������������������������������� Disclosed no conflict of interest.
Wondisford, Fredric E. �������������������������� Disclosed no conflict of interest.
Wong, Chi-Ming ����������������������������������� Disclosed no conflict of interest.
Wood, Teresa ��������������������������������������� Disclosed no conflict of interest.
Woon Puay, Koh ����������������������������������� Disclosed no conflict of interest.
Wouters, Kristiaan ������������������������������� Disclosed no conflict of interest.
Wright, Kathryn F. �������������������������������� Stock/Shareholder: Pfizer Inc.
Wronkowitz, Nina �������������������������������� Disclosed no conflict of interest.
Wu, Bin ������������������������������������������������� Disclosed no conflict of interest.
Wu, Di �������������������������������������������������� Employee: Medtronic MiniMed, Inc.
Wu, Hongyu ������������������������������������������ Disclosed no conflict of interest.
Wu, Jimmy ������������������������������������������� Disclosed no conflict of interest.
Wu, Jun ������������������������������������������������ Disclosed no conflict of interest.
Wu, Xiwei ��������������������������������������������� Disclosed no conflict of interest.
Wu, Yan ������������������������������������������������ Disclosed no conflict of interest.
Wunderlich, F. Thomas ������������������������� Disclosed no conflict of interest.
Xia, Fangzhen ��������������������������������������� Disclosed no conflict of interest.
Xia, Jonathan ��������������������������������������� Disclosed no conflict of interest.
Xiao, Xianchao ������������������������������������� Disclosed no conflict of interest.
Xu, Aimin ���������������������������������������������� Disclosed no conflict of interest.
Xu, Haiyan �������������������������������������������� Disclosed no conflict of interest.
Xu, Jing ������������������������������������������������ Disclosed no conflict of interest.
Xu, Liou ������������������������������������������������ Disclosed no conflict of interest.
Xu, Ping ������������������������������������������������ Disclosed no conflict of interest.
Xu, Shanshan ��������������������������������������� Disclosed no conflict of interest.
Xu, Yuan ����������������������������������������������� Disclosed no conflict of interest.
Xue, Bingzhong ������������������������������������ Research Support: NuSirt Biopharma.
Xue, Ruidan ������������������������������������������ Disclosed no conflict of interest.
Xue, Yaoming ��������������������������������������� Disclosed no conflict of interest.
Xuhong, Hou ����������������������������������������� Disclosed no conflict of interest.
Yaghootkar, Hanieh ������������������������������ Disclosed no conflict of interest.
Yajnik, Chittaranjan ������������������������������ Disclosed no conflict of interest.
Yajnik, Pallavi ��������������������������������������� Disclosed no conflict of interest.
Yale, Jean-François ������������������������������ Advisory Panel: Abbott, AstraZeneca, Bayer, Boehringer
Ingelheim, Eli Lilly, Janssen, Medtronic, Merck, Novo
Nordisk, Sanofi; Research Support: AstraZeneca,
Boehringer Ingelheim, Eli Lilly, Janssen, Medtronic,
Merck, Novo Nordisk, Sanofi; Speaker’s Bureau:
Abbott, AstraZeneca, Bayer, Boehringer Ingelheim,
Eli Lilly, Janssen, Medtronic, Merck, Novo Nordisk,
Sanofi.
Yamabi, Masaki ����������������������������������� Employee: Kowa Pharmaceuticals.
Yamada, Eijiro �������������������������������������� Disclosed no conflict of interest.
Yamada, Iwao �������������������������������������� Employee: Kowa Pharmaceuticals.
Yamada, Masanobu ����������������������������� Disclosed no conflict of interest.
Yamaguchi, Satoshi ����������������������������� Disclosed no conflict of interest.
Yamamoto, Yuichi �������������������������������� Research Support: Astellas Pharma US, Inc.,
AstraZeneca Pharmaceuticals LP, Boehringer
Ingelheim Pharmaceuticals, Inc., Bristol-Myers
Squibb Company, Daiichi-Sankyo Co., Ltd., Eli
AUTHOR
RELATIONSHIP/COMPANY
Lilly Japan K.K., Johnson & Johnson, Kissei
Pharmaceutical Co., Ltd., Merck Sharp & Dohme,
Mitsubishi Tanabe Pharma Corporation, Novartis
Pharmaceuticals Corporation, Novo Nordisk Inc.,
Ono Pharmaceutical Co., Ltd., Sanofi U.S., Sumimoto
Dainippon Pharma Co., Ltd., Takeda Pharmaceutical
Company Limited.
Yamanaka, Hisashi ������������������������������� Disclosed no conflict of interest.
Yamazaki, Masahiro ����������������������������� Disclosed no conflict of interest.
Yan, Jing-He ����������������������������������������� Employee: Novartis Pharmaceuticals Corporation.
Yang, Alex �������������������������������������������� Consultant: ZS Pharma, Inc.; Stock/Shareholder: ZS
Pharma, Inc.
Yang, Hyuk In ��������������������������������������� Disclosed no conflict of interest.
Yang, Jae Sung ������������������������������������ Disclosed no conflict of interest.
Yang, Juhong ��������������������������������������� Disclosed no conflict of interest.
Yang, Lu ������������������������������������������������ Disclosed no conflict of interest.
Yang, Shaojuan ������������������������������������ Disclosed no conflict of interest.
Yang, Wenying ������������������������������������� Disclosed no conflict of interest.
Yang, Xiaodong ������������������������������������ Employee: Merck & Co., Inc.
Yao, Li ��������������������������������������������������� Disclosed no conflict of interest.
Yap, Chui Sun ��������������������������������������� Disclosed no conflict of interest.
Yasuda, Tetsuyuki ��������������������������������� Disclosed no conflict of interest.
Ye, Jenny ���������������������������������������������� Employee: Sanofi; Stock/Shareholder: Sanofi.
Ye, Jianping ����������������������������������������� Disclosed no conflict of interest.
Yeo, Kwee Poo ������������������������������������� Employee: Eli Lilly and Company.
Yepes, Carlos Augusto ������������������������� Speaker’s Bureau: Eli Lilly and Company, Medtronic
MiniMed, Inc., Novo Nordisk Inc.
Yerges-Armstrong, Laura ��������������������� Disclosed no conflict of interest.
Yiew, Kan Hui ��������������������������������������� Disclosed no conflict of interest.
Yi-Frazier, Joyce P. �������������������������������� Disclosed no conflict of interest.
Yik Ying, Teo ����������������������������������������� Disclosed no conflict of interest.
Yilmaz, Hamiyet ����������������������������������� Disclosed no conflict of interest.
Ying, Wei ���������������������������������������������� Disclosed no conflict of interest.
Yogeshwari, Sivakumaran ������������������� Disclosed no conflict of interest.
Yoo, Hye Jin ����������������������������������������� Disclosed no conflict of interest.
Yoon, Sun Ae ���������������������������������������� Disclosed no conflict of interest.
Yore, Mark M. �������������������������������������� Disclosed no conflict of interest.
Yorek, Mark A. ������������������������������������� Disclosed no conflict of interest.
Young, Edwin ��������������������������������������� Disclosed no conflict of interest.
Young, Kristin L. ����������������������������������� Disclosed no conflict of interest.
Yu, Ji Hee ��������������������������������������������� Disclosed no conflict of interest.
Yuan, Geheng ��������������������������������������� Disclosed no conflict of interest.
Yuan, Jian-Min ������������������������������������� Disclosed no conflict of interest.
Yun, Nari ����������������������������������������������� Disclosed no conflict of interest.
Zaharieva, Emanuela ��������������������������� Disclosed no conflict of interest.
Zangeneh, Farhad �������������������������������� Disclosed no conflict of interest.
Zavolan, Mihaela ��������������������������������� Disclosed no conflict of interest.
Zeller, Cordula �������������������������������������� Employee: Boehringer Ingelheim GmbH.
Zemel, Michael B. �������������������������������� Board Member: NuSirt Biopharma; Employee: NuSirt
Biopharma; Stock/Shareholder: NuSirt Bopharma.
Zeng, Yanmei ��������������������������������������� Disclosed no conflict of interest.
Zera, Chloe ������������������������������������������� Disclosed no conflict of interest.
Zevallos, Juan C. ���������������������������������� Disclosed no conflict of interest.
Zhang, Dongming ��������������������������������� Disclosed no conflict of interest.
Zhang, Fang ������������������������������������������ Disclosed no conflict of interest.
Zhang, Huiliang ������������������������������������ Disclosed no conflict of interest.
Zhang, Jinping ������������������������������������� Disclosed no conflict of interest.
Zhang, Junqing ������������������������������������ Disclosed no conflict of interest.
Zhang, Ming ����������������������������������������� Disclosed no conflict of interest.
Zhang, Puhong ������������������������������������� Disclosed no conflict of interest.
Zhang, Quanjiang ��������������������������������� Disclosed no conflict of interest.
Zhang, Shu ������������������������������������������� Employee: Boehringer Ingelheim Pharmaceuticals, Inc.
Zhang, Tong ������������������������������������������ Disclosed no conflict of interest.
Zhang, Wenwei ������������������������������������ Disclosed no conflict of interest.
Zhang, Xi ���������������������������������������������� Disclosed no conflict of interest.
Zhang, Yiyi �������������������������������������������� Disclosed no conflict of interest.
Zhao, Peng ������������������������������������������� Disclosed no conflict of interest.
Zhao, Tieyun ����������������������������������������� Disclosed no conflict of interest.
Zhao, Zhiyun ����������������������������������������� Disclosed no conflict of interest.
Zhen, Wei ��������������������������������������������� Disclosed no conflict of interest.
Zheng, Yan ������������������������������������������� Disclosed no conflict of interest.
Zheng, Yang ����������������������������������������� Disclosed no conflict of interest.
Zhong, Xueyu ��������������������������������������� Disclosed no conflict of interest.
Zhou, Beiyan ���������������������������������������� Disclosed no conflict of interest.
Zhou, Haihong �������������������������������������� Employee: Merck & Co., Inc.
Zhou, Joanna ��������������������������������������� Disclosed no conflict of interest.
Zhou, Junwen �������������������������������������� Disclosed no conflict of interest.
Zhu, Beibei ������������������������������������������� Disclosed no conflict of interest.
Zhu, Chaoxia ���������������������������������������� Disclosed no conflict of interest.
Zhu, Chunfang �������������������������������������� Disclosed no conflict of interest.
Zhu, Meili ��������������������������������������������� Disclosed no conflict of interest.
Zhu, Yingmin ���������������������������������������� Disclosed no conflict of interest.
Ziegler, Anette-Gabriele ����������������������� Disclosed no conflict of interest.
LB112
RELATIONSHIP/COMPANY
Ziegler, Thomas R. �������������������������������� Consultant: Abbott, Baxter; Research Support: Abbott,
National Institutes of Health.
Zinman, Bernard ����������������������������������� Disclosed no conflict of interest.
AUTHOR
RELATIONSHIP/COMPANY
Zinzen, Robert P. ����������������������������������� Disclosed no conflict of interest.
Zubatov, Yelena ������������������������������������ Disclosed no conflict of interest.
AUTHOR DISCLOSURE
AUTHOR
LB113