- MBSW Online

Graphical Approaches to the Analysis of
Safety Data from Clinical Trials
Ohad Amit, Richard M. Heiberger, Peter W. Lane
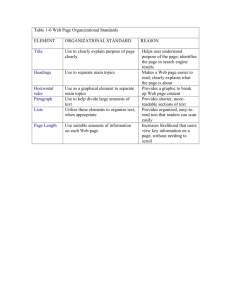
Patient safety has always been a primary focus in the development of new pharmaceutical products.
Safety issues in clinical trials are usually reported in tables.
Formal analysis of safety data is much less developed than for efficacy data.
Safety data provides an ideal opportunity to use graphical methods
•
Present concise summaries
•
Communicate main messages
•
Back up with tables as needed
Graphs can be used in
• an exploratory setting to help identify emerging safety signals.
• a confirmatory setting as a tool to elucidate known safety issues.
1
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
I spent a research leave year at GSK where I joined a company-wide team investigating graphical issues for display of clinical trial information.
We developed several graphical displays for routine safety data collected during a clinical trial, covering a broad range of graphical techniques. Many of the displays we devised are now included in the GSK software library. Our results, coauthored with Ohad Amit and Peter W. Lane of GSK, appeared in 2008 in
Pharmaceutical Statistics .
The displays focus on key safety endpoints in clinical trials
2
• the QT interval from electrocardiograms
• laboratory measurements for detecting hepatotoxicity
• adverse events of special interest.
We discuss in detail the statistical and graphical principles underlying the production and interpretation of the displays.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
We illustrate eleven specific graphical designs, many of which display the data along with statistics derived from them. Each will be discussed in detail.
•
Two are simple, comparing distributions with boxplots or cumulative plots.
4
3
2
1
0
ALAT ASAT ALKPH
Liver Function Test
Drug A (N=209) Drug B (N=405)
For ASAT, ALKPH, and ALAT, the Clinical Concern Level is >2 ULN;
For BILTOT CCL is >1.5 ULN; where ULN is the Upper Level of Normal Range
BILTOT
•
Five more display data and summaries over time, comparing information from two groups in terms of distribution (with boxplots), cumulative incidence, hazard, or simply means with error bars.
Drug A
Drug B
0
Drug A
Drug B
218
447
201
339
50
190
305
100
Days on Study
176
278
150
162
264
200
0
2
Drug A
Drug B
0.008
0.006
0.004
0.002
0.0
0
Average no. of subjects
at risk during interval
Drug A
Drug B
210
430
20
200
340
40
190
310
60 80 100 120
Days since randomization
140
180
300
180
280
170
280
170
270
160
260
160 180
93
150
13
18
200
3
•
The other four are multi-panel displays: one-dimensional and two-dimensional arrays of scatterplots, a trellis of individual profiles, and a paired dotplot displaying risk together with relative risk.
Most Frequent On−Therapy Adverse Events Sorted by Relative Risk
ALAT ALKPH ASAT
4
3
2
1
0
0 1 2 3 4 0
Drug A (N=209)
Drug B (N=405)
1 2 3 4 0 1
Baseline (/ULN)
2 3 4 0
For ASAT, ALKPH, and ALAT, the Clinical Concern Level is 2 ULN;
For BILTOT, the CCL is 1.5 ULN; where ULN is the Upper Level of Normal Range
BILTOT
1 2 3 4
3
2
1
0
3
2
1
0
3
2
1
0
0 1 2 3 0 1 2 3 0 1 2 3
ASAT (/ULN) ALAT (/ULN)
Drug A (N=209)
Drug B (N=405)
BILTOT (/ULN)
For ASAT, ALKPH, and ALAT, the Clinical Concern Level is 2 ULN;
For BILTOT CCL is 1.5 ULN; where ULN is the Upper Level of Normal Range
ARTHRALGIA
NAUSEA
ANOREXIA
HEMATURIA
INSOMNIA
VOMITING
DYSPEPSIA
WEIGHT DECREASE
PAIN
DIARRHEA
FATIGUE
FLATULENCE
DIZZINESS
ABDOMINAL PAIN
RESPIRATORY DISORDER
HEADACHE
INJURY
GASTROESOPHAGEAL REFLUX
BACK PAIN
RASH
HYPERKALEMIA
SINUSITIS
INFECTION VIRAL
UPPER RESP TRACT INFECTION
COUGHING
URINARY TRACT INFECTION
MYALGIA
MELENA
RHINITIS
BRONCHITIS
CHEST PAIN
CHRONIC OBSTRUCTIVE AIRWAY
DYSPNEA
((
((
((
((
((
((
((
((
))
))
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
))
))
(( ))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
0 10 20 30 .125
.5 1 2 4 8 16 32
TREATMENT A (N=216)
•
Percent
TREATMENT B (N=431)
Relative Risk with 95% CI
•
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Graphical displays for safety data
Richard M. Heiberger
We illustrate each of our graphs using real data from a drug development program: specifically, safety data from a large Phase III pivotal trial. This was a two-arm randomized trial comparing a fixed dose of the test drug (Drug B below) to placebo (Drug A). Following a four-week placebo run-in, patients were randomized to receive either placebo or test drug for 24 weeks. The safety data collected in this trial is typical of the type of routine safety data collection that is part of almost all Phase II and III trials of pharmaceutical products.
While the graphs were developed in the context of a randomized parallel-group trial we have provided commentary on their utility in other settings. This real dataset has been used to demonstrate key concepts that we identified as important in the evaluation of safety, but the displays were not tailored to draw specific conclusions regarding the safety profile of the test drug.
4
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
QT Interval
Richard M. Heiberger
QTc measure of heart rhythm has become pivotal
Prolonged QTc interval is treated as a surrogate for serious arrhythmia
Change from baseline considered most relevant
Change associated with drug:
• >
30 msec
→ clinical concern
• >
60 msec
→ serious clinical concern
Entire distribution is of interest, as well as tail behaviour
We propose three graphs to help evaluate QTc.
5
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 6
100
90
80
70
60
50
40
30
20
10
0
-30 -20 -10 0 10 20 30 40 50
Change in QTc interval (msec)
Note: Increase <30msec ’Normal’, 30-60msec ’Concern’, >60msec ’High’
60
Figure 1:
Empirical distribution function for maximum change in QTc
Drug A (N=215)
Drug B (N=429)
70 80 90
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
The y
-variable is the maximum change for each patient over the 24-week treatment period. Each point represents the percentage of patients on the y
-axis with a change in QTc less than or equal to the corresponding value on the x
-axis. Reference lines have been provided at 30 and 60 msec as well as at 0 msec to help the interpretation.
The distribution functions for the two treatment groups are drawn with fairly thin lines to allow assessment of small differences at the upper end; different linestyles are used as well as different colours for each treatment so that differences are obvious when the graph is printed in black and white. As can easily be seen in the graph, in this particular dataset there is little difference in how the distributions behave at the upper tail, though the distribution for the test drug is slightly less concentrated around the median than that for placebo. The proportion of patients with a maximum change less than zero is about oneninth, as expected in a trial with eight visits after baseline and no effect on
QTc.
7
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 8
Figure 2:
Boxplot of change from baseline in QTc by time and treatment
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
Figure 2 is a boxplot that displays the distribution of the changes in QTc at each time-point during treatment. The distribution of the maximum change over the entire treatment period is displayed in a “margin” at the right-hand side of the graph. Alternative or additional information can be displayed in the margin, such as derived variables like the last-observation-carried-forward
(LOCF). In addition to providing a visual summary of variability and central tendencies, this type of graphical display explicitly identifies the extreme values in the distribution. Reference lines are drawn as before at 30 and 60 msec to aid in the interpretation.
The concept of a graphical margin as used in Figure 2 is a powerful way to add extra summary information in the context of a graph, just as a tabular margin adds value to a table. It is of particular value in many graphs that show effects over time to add a lower margin as here to show the number of subjects involved in the summaries displayed at each time-point. Note that the numbers of subjects may differ among the graphs we present, because of different patterns of missing observations and different definitions of populations for the variables involved.
9
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
1
0
-1
-2
-3
-4
-5
3
2
-6
Drug A
0 2
Drug B
4 8 12 16 20 24
Week
Drug A
Drug B
216
431
210 206
423 384
199
362
191
337
184
315
176
311
169
299
Note: Vertical lines are 95% confidence limit ranges, LOCF is last observation carried forward
164
293
Figure 3:
Mean (95% CI) change from baseline in QTc by time and treatment
LOCF
214
429
10
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 11
Recent ICH guidance (ICH, 2005) on evaluation of QT prolongation has recommended the use of means and confidence intervals in summarizing QTc data; we propose Figure 3 to address those recommendations. Figure 3 displays means and associated 95% confidence intervals for change in QTc by time. The LOCF value is displayed in a margin; but, as in Figure 2, alternative values, such as the maximum change over the treatment period, can be displayed instead.
Within-group mean changes with 95% confidence intervals are displayed as bars around a point.
In a thorough QT study (see ICH, 2005) the focus is on the mean difference from placebo along with a 90% confidence interval. Mean differences from placebo and the relevant measure of variability could also be displayed using the graphical display in Figure 3.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Liver Function Tests (LFTs)
Richard M. Heiberger 12
Evaluation of hepatotoxicity has become a central part of many pharmaceutical development programs. Hepatotoxicity is evaluated through the collection of key laboratory variables, including aspartate aminotransferase (ASAT), alanine aminotransferase (ALAT), alkaline phosphatase (ALKPH) and total bilirubin
(BILTOT).
We have created graphics that summarize these variables individually and collectively. We recognize that summary statistics may be of little value in the evaluation of hepatotoxicity, so we propose graphics that aid in describing properties of the distribution and provide greater insight where it is needed: at the individual patient level.
Unlike with the QT interval, where changes over the baseline are deemed important, with liver function it is the result itself, relative to the “upper limit of normal” (ULN), which represents the clinically meaningful metric. The ULN is a value routinely specified for each variable by each laboratory, and allows the standardization of results coming from different labs with different normal ranges.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 13
Figure 4:
Distribution of ASAT by time and treatment
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Boxplots as a function of time
Richard M. Heiberger 14
We propose boxplots for each LFT measurement as a function of time (Figure
4). The maximum value over the entire treatment period is displayed in a margin at the right-hand side of the graph, and alternatives should be considered as appropriate. To better facilitate a comparison and to highlight true elevations, patients who were above the upper limit of normal at baseline are excluded from this graph. We have reduced the vertical spread of the graph by summarizing all values above twice the ULN as counts in an upper margin of the graph.
2
1
4
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
3
Richard M. Heiberger
0
ALAT ASAT ALKPH
Liver Function Test
Drug A (N=209) Drug B (N=405)
For ASAT, ALKPH, and ALAT, the Clinical Concern Level is >2 ULN;
For BILTOT CCL is >1.5 ULN; where ULN is the Upper Level of Normal Range
BILTOT
Figure 5:
Distribution of maximum liver function test values by treatment
15
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Parallel boxplots of the maximum elevation
Richard M. Heiberger 16
We propose a set of boxplots displaying the maximum elevation in each LFT over the treatment interval, side-by-side (Figure 5). This type of display allows clinicians to evaluate elevations simultaneously across LFT measurements.
Reference lines are provided at selected levels relative to the upper limit of normal. These are intended to help highlight subjects with elevations exceeding these levels and can be modified as appropriate for the disease or population under study.
An additional issue to consider when displaying multiple LFT measurements within the same plot is how to define the maximum. In Figure 5, we chose the maximum for each patient on each measurement individually. With this approach a patient’s maximum value may occur at different time-points depending on the measurement.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
ALAT ALKPH ASAT
4
3
2
1
0
0 1 2 3 4 0
Drug A (N=209)
Drug B (N=405)
1 2 3 4 0 1
Baseline (/ULN)
2 3 4 0
For ASAT, ALKPH, and ALAT, the Clinical Concern Level is 2 ULN;
For BILTOT, the CCL is 1.5 ULN; where ULN is the Upper Level of Normal Range
1
BILTOT
2 3 4
17
Figure 6:
Empirical distribution function for maximum change in QTc
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Scatterplots of LFT maximum values against baseline
Richard M. Heiberger 18
To help explain what is happening at the individual patient level, we propose two multiple-panel displays. Figure 6 is a set of scatterplots of the maximum value against baseline over the treatment period with a panel for each LFT measurement and a symbol for each treatment group. It is important to use identical scaling on the x- and y-axes. This display can be considered the graphical analogue to laboratory shift tables. Specifically, focusing on the upper left-hand quadrant of the graph allows you to note patients who were normal at baseline and have had subsequent elevations during the treatment period.
These are intended to help highlight patients with elevations exceeding levels of clinical concern. While individual points are not labelled, it may be useful to add labels (such as subject ID) for those observations above one of the levels of concern in one or both dimensions. Note that this type of graphical display is useful across a wide range of clinical trial designs.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 19
3
2
1
0
3
2
1
0
3
2
1
0
0 1 2 3 0 1 2 3 0 1 2 3
ASAT (/ULN) ALAT (/ULN)
Drug A (N=209)
Drug B (N=405)
BILTOT (/ULN)
For ASAT, ALKPH, and ALAT, the Clinical Concern Level is 2 ULN;
For BILTOT CCL is 1.5 ULN; where ULN is the Upper Level of Normal Range
Figure 7:
Matrix Display of Maximum LFT Values
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Scatterplot matrix of maximum LFT values
Richard M. Heiberger 20
A second multiple-panel display (Figure 7) represents the lower triangle of a four-by-four matrix of scatterplots of all possible combinations of the four LFT measurements. This type of display is helpful in visually identifying patients with simultaneous elevations in two liver function tests. For this graph, the maximum value for each patient on each measurement over the treatment interval is used, and reference lines are provided at selected levels relative to the upper limit of normal.
One feature that is disconcerting at first sight is the overlaying of points from one treatment by those of another. However, this can be used to advantage: by choosing to draw the Placebo points last (Drug A), the effect is to highlight any difference in distribution of the test drug compared to this standard distribution.
In this application, there is little difference to see apart from the four patients on Drug A with high ASAT values.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 21
Patient: 5152 Drug: A White Male Age: 48
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
-50 -25 0 25 50 75 100 125 150 175 200
Patient: 6850 Drug: A White Male Age: 51
-50 -25 0 25 50 75 100 125 150 175 200
ALAT ASAT ALKPH
Patient: 6416 Drug: A White Male Age: 64
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
-50 -25 0 25 50 75 100 125 150 175 200
Patient: 5269 Drug: B White Female Age: 48
5.0
4.5
4.0
3.5
3.0
2.5
2.0
1.5
1.0
0.5
0.0
-50 -25 0 25
_
50 75 100 125 150 175 200
BILTOT Study Days
Note: Clinical concern level for ALAT, ASAT and ALKPH is 2xULN, for BILTOT is 1.5xULN
Figure 8:
LFT patient profiles
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Patient profiles of LFT values
Richard M. Heiberger 22
Patient profiles of LFT values can be shown in a trellis display with several panels on a page and potentially many pages, each panel representing one patient’s data for the LFT measurements of interest. The display may usefully be restricted to just those patients whose values give cause for concern. Reference lines are provided as before. Also note that the treatment period is displayed as a thick red line at the bottom of each panel. At the individual patient level this allows the observer to see which measurements are causing concern and to what extent, to assess their temporal relationship to treatment, and to evaluate the onset and duration of the elevation.
Note that care needs to be taken when constructing multiple-panel displays to ensure that text is not made unreadable for the intended medium, as a result of packing several panels onto a page: default settings suitable for single displays usually need to be changed.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Adverse experience data
Richard M. Heiberger 23
Evaluation of adverse experience data is a critical aspect of all clinical trials.
We propose graphics for exploratory data analysis or signal identification, and for adverse experiences (AEs, also read as adverse events) that may result from a compound’s mechanism of action or events that are of special interest to regulators.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
Most Frequent On−Therapy Adverse Events Sorted by Relative Risk
24
ARTHRALGIA
NAUSEA
ANOREXIA
HEMATURIA
INSOMNIA
VOMITING
DYSPEPSIA
WEIGHT DECREASE
PAIN
DIARRHEA
FATIGUE
FLATULENCE
DIZZINESS
ABDOMINAL PAIN
RESPIRATORY DISORDER
HEADACHE
INJURY
GASTROESOPHAGEAL REFLUX
BACK PAIN
RASH
HYPERKALEMIA
SINUSITIS
INFECTION VIRAL
UPPER RESP TRACT INFECTION
COUGHING
URINARY TRACT INFECTION
MYALGIA
MELENA
RHINITIS
BRONCHITIS
CHEST PAIN
CHRONIC OBSTRUCTIVE AIRWAY
DYSPNEA ((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
((
))
))
((
((
((
((
((
((
((
((
((
(( ))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
))
0 10 20 30 .125
.5 1 2 4 8 16 32
TREATMENT A (N=216)
•
Percent
TREATMENT B (N=431)
Relative Risk with 95% CI
•
Figure 9:
Most frequent on-therapy adverse events sorted by relative risk
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
AE dotplot of incidence and relative risk
Richard M. Heiberger 25
Figure 9 is a two-panel display of the most frequently occurring AEs in the active arm of the study. The first panel displays their incidence by treatment group, with different symbols for each group. The second panel displays the relative risk of an event on the active arm relative to the placebo arm, with
95% confidence intervals as defined by Agresti (2004) for a 2
×
2 table.
If confidence intervals are presented, multiple comparison issues should be given consideration, particularly if there is interest in assessing the statistical significance of differences of the relative risk for so many types of events. However, the primary goal of this display is to highlight potential signals by providing an estimate of treatment effect and the precision of that estimate. S-Plus code for the construction of this plot is available in the online files that accompany
Heiberger and Holland (2004).
The AEs are ordered by relative risk so that events with the largest increases in risk for the active treatment are prominent at the top of the display. We do not recommend ordering alphabetically by preferred term, which is the likely default with routine programming, because that makes it more difficult to see the crucial information of relative importance of the AEs.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
AE dotplot from Excel with the RExcel interface
Richard M. Heiberger 26
Recently I have been working on the RExcel interface with Erich Neuwirth.
Our book R through Excel will be available from Springer this summer. One of the examples shows control of the AEdotplot from Excel.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 27
Figure 10:
Data on adverse events in an Excel spreadsheet.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 28
Figure 11:
Most frequent on-therapy adverse events sorted by relative risk
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 29
Figure 12:
Double-click the spreadsheet on a column title, in this case alphabetical by event name
(silly, yes, but the data may have been given to you in that sort order).
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 30
Figure 13:
The graph immediately sorts itself to match.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Time-to-event plots for AEs
Richard M. Heiberger 31
Of particular interest in AE data is the onset date of each event relative to the start of treatment. Specifically, we may want to summarize how the risk for an event is changing over time. It is both convenient and appropriate to treat AEs as time-to-event data. Unlike simple incidence rates, this approach allows evaluation of the risk as a function of time. In fact, it can be argued that the most appropriate and unbiased approach to estimating the risk of an event is through the use of statistical methodology for time-to-event data.
This approach to analyses of AE data has been advocated in several regulatory guidance documents including the Statistical Principles for Clinical Trials E9
(ICH, 1998) and the ICH Structure and Content of Clinical Study Reports
E3 (ICH, 1995). Several authors have also advocated the approach including
O’Neill (1998), Gait et al (2000) and Ioannidis and Lau (2002), and several real-life examples have demonstrated its value.
We propose two graphical displays based on non-parametric survival methods.
As there can typically be dozens of events reported in any clinical trial, we recommend that these displays be tailored around events that are of particular interest to a given compound. In our example, the particular events of interest are gastrointestinal (GI) AEs of concern.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Drug A
Drug B
Richard M. Heiberger 32
0
Drug A
Drug B
218
447
201
339
50
190
305
100
Days on Study
176
278
150
162
264
200
0
2
Figure 14:
Cumulative distribution (with SEs) of time to first AE of special interest
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 33
Figure 10 is a Kaplan-Meier plot by treatment group of the cumulative incidence of GI adverse events of concern by time. We adhered to the principles laid out by Pocock et al (2002) for display of censored survival data. Standard error bars for the cumulative incidence at selected time-points on the x
-axis have also been included. Simultaneous confidence bands may be displayed instead.
The readability and clarity of the graph should be a factor in considering whether or not to display standard error bars or confidence bands. For example, if the estimated curves are close together, the use of confidence bands may make it difficult to distinguish between the curves or between the estimated curve and the confidence bands. The graph provides a clear indication of the evolving incidence of these events as a function of time making the appropriate adjustments to the risk set as patients withdraw from the trial.
This graph is useful in many settings where there is a sufficiently long follow-up period. It can be applied across a wide range of clinical trial designs.
We have included “rug-plots” along each stepped line to characterize the distribution of censored events in each treatments, i.e. the times at which individuals withdraw from the trial. In conjunction with the steps, which represent individual adverse events, the graph therefore displays all the relevant data along with the statistical summary of cumulative incidence.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger
Drug A
Drug B
34
0.008
0.006
0.004
0.002
0.0
0
Average no. of subjects
at risk during interval
Drug A
Drug B
210
430
20
200
340
40
190
310
60 80 100 120
Days since randomization
140 160 180 200
180
300
180
280
170
280
170
270
160
260
93
150
13
18
Figure 15:
Hazard function for AEs of special interes
Graphical Approaches to the Analysis of Safety Data from Clinical Trials Richard M. Heiberger 35
A complementary display to the cumulative incidence plot is a graphical display of the hazard for each treatment group as a function of time (Figure 11). Lifetable estimates of the hazard function for each treatment group were generated and then displayed graphically along with their standard errors. The life-table analysis was based here on 10-day intervals, and the hazard displayed at the midpoint of each interval. This display is intended to provide a more direct assessment of the risk of an event occurring at any given time during the followup period.
The values provided in the lower margin give the context of the estimated hazard rates above, as seen in the earlier graphs. However, these values are not necessarily integral (unless rounded, as here), as a fundamental assumption of the life-table method is that all censoring occurs at the midpoint of an interval.
Therefore, the number of censored patients, who are assumed to be at risk for only half the interval, is multiplied by 0.5.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Discussion
Richard M. Heiberger 36
The eleven graphs described above represent our key areas of focus. There are several additional pieces of safety data that might be displayed graphically and there are several additional graphical approaches that could be considered for the endpoints discussed above. Other common safety measurements, in addition to those discussed above, consist of vital signs, additional ECG measurements, and additional clinical laboratory measurements. Although the graphics described above were not developed with these in mind, several are still applicable. We give here a brief description of how these graphics may be applied to these additional safety endpoints, and
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Conclusions—Tools
Richard M. Heiberger 37
The production of graphs has always been a time-consuming process. With the pressure of deadlines in a development project, it is essential to provide tools that take care of the details of graph construction in whatever software is used, and allow people to concentrate on selecting the right information to present. In GlaxoSmithKline we are developing standard tools for producing good-quality graphical displays. These include
• validated scripts to allow straightforward production of standard graphs like those presented here. We estimate that these will provide for only about half the graphs that are needed, on average.
• a graphical environment in which it is easier to construct ad hoc displays, and export scripts that capture the process into the standard production environment.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Conclusions—Context
Richard M. Heiberger 38
The graphical displays described above should be given prime consideration in the analysis of safety data arising from clinical trials. They allow the analyst a broad range of options to evaluate safety data. While tabular summaries of safety data can be voluminous and difficult to interpret, graphical summaries display information in a clear and concise manner. Many of these graphs display not only the summary statistics derived from analysis, but also some or all of the original data, putting the statistics into context and highlighting individual observations that are of particular concern in safety analysis.
Graphical Approaches to the Analysis of Safety Data from Clinical Trials
Acknowledgements
Richard M. Heiberger 39
We are indebted to the other members of the Graphics Team in the Biomedical and Data Sciences Division of GlaxoSmithKline: Susan P. Duke, Daniel C.
Park, Mike Colopy, Nada X. Boudiaf, Randall R. Austin, and Shi-Tao Yeh
(who programmed the SAS versions of most of the graphs). We also thank
Michael Durante for programming the S-Plus version of two of the graphs.
This talk is based on the paper:
Ohad Amit, Richard M. Heiberger, and Peter W. Lane. (2008) “Graphical Approaches to the Analysis of Safety Data from Clinical Trials”. Pharmaceutical
Statistics, 7, 1, 20-35.
http://www3.interscience.wiley.com/journal/114129388/abstract
The S-Plus/R function for the AEdotplot is included in the HH package available for S-Plus on CSAN and for R on CRAN. The RExcel example for the
AEdotplot is included with the R package for R through Excel by Richard M.
Heiberger and Erich Neuwirth to be published by Springer in August 2009.