Understanding Patient Service Revenue in Health Centers

Curt Degenfelder Consulting, Inc.
Understanding Patient
Service Revenue in
Health Centers
Health Center Reimbursement
• Medicaid: Cost based rate from Prospective Payment System (PPS) or alternative methodology
• Medicaid managed care: Negotiated rate with PPS wraparound protection. May be paid on a capitated (fixed monthly $ amount per member) or fee-for-service
• Medicare: Cost based rate up to Upper Payment limit (UPL)
• Medicare managed care: Negotiated rate with wraparound protection
• Medicare/Medicaid dual eligible: Medicare payment plus crossover payment
• Medicare Advantage/Medicaid dual eligible: Negotiated rate plus PPS wraparound
• SCHIP: Paid at PPS rate starting 10/1/09
• Commercial insurance: Negotiated rate
• Self – pay: Based on charges and sliding fee
Curt Degenfelder Consulting, Inc.
2
Forms of Patient Services Revenue
Each type of patient revenue can have different reimbursement schemes. These include:
• Fee-For-Service
• All-Inclusive Rate
• Prospective Payment System
• Capitation
3
Curt Degenfelder Consulting, Inc.
1
Payor Type – Medicaid
Medicaid provides medical assistance for certain individuals and families with low incomes and resources. The program is a jointly funded cooperative venture between the Federal and State governments to assist States in the provision of adequate medical care to eligible needy persons. Medicaid is the largest program providing medical and health-related services to America's poorest people (in 2007 the average enrollment in Medicaid was 41.9 million people; 61.9 million people enrollees). PPACA expands Medicaid eligibility to all residents who have been citizens for at least 5 years and who have incomes at or below 133% of the
Federal Poverty Limit.
Within broad national guidelines which the Federal government provides, each of the States:
• establishes its own eligibility standards;
• determines the type, amount, duration, and scope of services;
• sets the rate of payment for services; and
• administers its own program.
Curt Degenfelder Consulting, Inc.
4
Payor Type – Medicaid Managed Care
• Managed care plans receive a monthly primary care capitation rate for each Medicaid recipient enrolled.
• Health centers may enter into managed care agreements with managed care organizations who participate in State Medicaid programs.
Contracts between health centers and managed care service.
• The health center is required to provide all the primary care the patient needs for a defined monthly premium.
• As of 7/1/10, 39,020,325 Medicaid enrollees were in managed care nation wide, 71.45% of the total.
5
Curt Degenfelder Consulting, Inc.
Overview of PPS
• Who are the FQHCs?
• Initial PPS rate-setting methodology 2001
• FQHCs in 2001
• New FQHCs since 2001
• PPS continued rate-setting for the future
• Medicaid managed care shortfall payments (“wraparound”)
6
Curt Degenfelder Consulting, Inc.
2
Overview of PPS
• Rates established using cost data from 1999 & 2000, for health centers existing in 2001
• Rates Adjusted annually by the Medicare Economic Index (MEI)
• New Health Centers (since 2001)
– Same or similar health centers, or
– Cost Report
– Some states may allow Medicare rate on an interim basis until rate can be established using other means
• Change in Scope of Services
• Alternative Methodologies
• PPS Wraparound where managed care exists
Curt Degenfelder Consulting, Inc.
7
PPS Wrap-Around
• States required to make supplemental payments to FQHCs that subcontract
(directly or indirectly) with managed care organizations (MCOs) – particularly important in Section 1115 States where managed care is statewide.
• Supplemental payment is the difference between the payment received by the FQHC for treating the MCO enrollee and the payment to which the FQHC is entitled under the PPS.
• Incentive payments, e.g. risk pool payments are excluded from the wraparound calculation.
• Also, whether payments for non-direct medical services such as case management and administration will be figured into the wraparound calculation will also vary on a state-by-state basis.
• FQHCs are entitled to be paid at least as much as any other provider for similar services.
Curt Degenfelder Consulting, Inc.
8
Maximizing Wrap-Around
• Review managed care payment methodology and monitor “wraparound” payments
– Are you billing on a timely basis to the MCOs and to the state?
– Are you maximizing reimbursement in the form of incentive
– If approved claims need to be submitted to the state for reimbursement, are you actively submitting claims for all applicable encounters to MCOs and then tracking that those are returned as
“approved?”
9
Curt Degenfelder Consulting, Inc.
3
Setting Up Initial Medicare Billing
1.
Center gets designated as FQHC eligible
2.
Center applies to https://nppes.cms.hhs.gov/NPPES/StaticForward.do?forward=static.instructions
and gets NPI for each of its sites
3.
Center completes 855A for each of its sites, including the NPI notification letter/email and the HRSA designation letter (approval may t k 2 4 th )
4.
Center gets interim rate of $50 per visit and can begin billing
10
Curt Degenfelder Consulting, Inc.
CMS Form 855A
• Form requires completing information on health center’s identification (locations, address, etc.), legal history (including adverse rulings), ownership interest (sheet per board member with SSN), practice locations, etc.
• Copies of all:
– Professional/business licenses
– CLIA licenses
– Pharmacy licenses
– Legal Action documents
– EDI Agreements
– Articles of Incorporation/Corporate charters
– IRS Documents
– Notice of Grant Award
• Go to www.cms.hhs.gov/
– Click on Medicare; then CMS Forms
11
Curt Degenfelder Consulting, Inc.
Site Designations in Health Centers
• FQHC Medicare – Through Fiscal Intermediary by delivery site.
Must be in Federal scope of project or would be considered FQHC
Look-A-Like.
• Community Health Center – Scope of Project – PIN 2008-01
– Service site = any location where grantee either directly or through sub-recipient or established arrangement, provides primary care services to a defined service area or target
M b t bil i t h or intermittent (shelter, encampment, etc.)
• FQHC/PPS Medicaid – Varies by state:
– Some states consider only the health center organization as a site (regardless of number of delivery sites).
– Some states require FQHC Medicare designation
– Some states do not require Medicare designation, but require individual site certification
– Some states have a hybrid system
Curt Degenfelder Consulting, Inc.
12
4
Medicare FQHC Rate Setting
1.
Center completes 855A for each of its sites
2.
Center gets interim rate of $50 per visit and can begin billing
3.
Center completes a projected cost report for any twelve month period
4.
Center receives and gets paid on an interim rate
5.
Center completes a full year cost report, and
6 Rates are then trended annually by MEI gets the lesser of its actual allowable cost per visit and the upper payment limit (UPL) UPL -
$128.49 urban/ $111.21 rural 1/1/12 – 12/31/12 .
7.
Medicare reconciles actual rate to beginning of FQHC billing automatically through a remittance advice
8.
Center completes a Medicare cost report every year
13
Curt Degenfelder Consulting, Inc.
Medicare FQHC Billing
• For Medicare FQHC services, Medicare will pay 80% of the health centers rate to account for patient co-insurance. So in 2012 for an urban health center at the upper payment limit would receive $102.79 from
Medicare
• Patient coinsurance is based on 20% of charges, not of the CHC’s rate.
These charges can be reduced according to the sliding fee scale. The t k bl deductible for FQHC services ff t t ll t th f d N l
• Medicare pays 75% for behavioral health services.
14
Curt Degenfelder Consulting, Inc.
Crossover Billing
For a patient that is Medicare/Medicaid dual-eligible, Medicare is the primary insurance and Medicaid is secondary. Since it is a Medicaid visit, the health center is entitled to its full PPS rate. However, some states have interpreted that they only have to pay the 20% coinsurance. This system is somewhat similar to the wraparound for Medicaid managed care.
2012 PPS rate of $135, the could receive a crossover rate of $32.21
($135.00 - $102.79)
• In virtually every case, the state will do some sort of year-end reconciliation
(which often includes the wraparound as well)
• New health centers receiving the $50 interim Medicare FQHC rate should understand their state’s rules in preparing the reconciliation report (because actual Medicare payments do not equal expected Medicare payments)
15
Curt Degenfelder Consulting, Inc.
5
Payor Type – Commercial/Third Party
Insurance
• Employer paid health insurance.
• In most cases, these patients are above the 200% poverty level.
This suggests that any amount not covered by insurance would be considered due by the patient.
Some organizations accept the third party insurance as full payment.
• A health center may request a co-pay from the patient.
16
Curt Degenfelder Consulting, Inc.
Payor Type – Self Pay
• Section 330 regulations require that the schedule of discounts conform with the following guidelines:
– Full discount to individuals and families with incomes at or below those set forth in the most recent Federal poverty income guidelines (100 – 200% of FPL)
– No discount to individuals and families with annual incomes greater than twice those set forth in the Guidelines (>200% of FPL)
– Except that nominal fees for services may be collected from individuals with incomes at or below such levels where imposition of such fee is consistent with project goals (<100% of FPL, accounts for over half of health center self-pay patients nationwide)
• Section 330 statute further requires that “a health center has made and will continue to make every reasonable effort to secure from patients payment for services in accordance with such schedules.”
• Health centers have different set-ups in terms of sliding fee arrangements.
– Some have set fee amounts per sliding fee category
– Some have different sliding scales for different types of services
– Others have different sliding scales for some types of procedures
Curt Degenfelder Consulting, Inc.
17
Dental Services in FQHCs
• Usually paid by Medicaid at the same cost rate as medical, or sometimes on its own individual cost basis (direct + overhead)
• Not a covered service for Medicare
• Could be billed fee-for-service during the cost year
• Medicaid covered services vary by state for dental
• Dental services use the Current Dental
Terminology (CDT), a manual published by the
ADA which includes the Code on dental procedures and nomenclature and ADA claim form.
18
Curt Degenfelder Consulting, Inc.
6
Other Programs
• SCHIP – as of 10/1/09, paid at the PPS rate
• Other state programs – wide variety of reimbursement options. If they are a Medicaid extension, PPS payment rules apply
• Family planning – federal program (Title X) but broad
• Uncompensated care, bad debt, charity care, primary care expansions – oftentimes these programs are billed and paid at a per visit rate, but the health center has an allocated annual maximum payment
• Behavioral health services may have billing limits as to the number of services that can be billed monthly or annually
19
Curt Degenfelder Consulting, Inc.
Analyzing
Reimbursement
Example of Troubled Health Center
Balance Sheet
Current
Period
Prior Year
End
Change
FAV/ (UNFAV) %
Current Ratio
Working Capital
Days Cash on Hand
Days in Patient A/R
Days in A/P
0.82
($107,975)
5
109
64
1.1
$104,907
25
66
37
(0.28)
($212,882)
(20)
(43)
(27)
-25%
-103%
-80%
-65%
-64%
What are revenue cycle trends and how might they be affecting these numbers?
Curt Degenfelder Consulting, Inc.
21
7
When does the Board need to intervene with
Executive Management?
• Trends to watch for
– Overall financial instability (e.g., losing money, negative fund balance)
– Abnormally high bad debt percentage – or a trend of increasing bad debt
– Medicaid or other payor audit results in large recoupment of payments, resulting from inaccurate coding and documentation
– Days in self-pay receivables > 365
– Days in Medicaid receivables > 100
– Large shift in total volume, up or down
– Big swings in payor mix
Curt Degenfelder Consulting, Inc.
22
When does Management need to intervene in the Finance Department and Operations?
• Trends to watch for:
– Shifts in net revenue per visit
– High denial rates
– Milestones/benchmarks in the billing cycle aren’t being met
– Days in Medicaid receivables are higher than target
– Inaccurate or incomplete coding and documentation
23
Curt Degenfelder Consulting, Inc.
Reporting
•
•
High Level
Commonly review monthly reports “in total”
– Days in Accounts Receivable, Net
– Bad Debt as a Percentage of Net Patient Services Revenue
– Visit Payor Mix Analysis
– Visits by Provider
– Revenue Per Visit
Measures commonly compared against:
– Prior periods – year over year
– Budget
– Industry norms – collection percentage, days in A/R, Payor Mix
– Strategic or Annual Operating Plan
24
Curt Degenfelder Consulting, Inc.
8
Reporting on Patient Services Revenue
Less:
Contractual
Allowance and
Sliding Fee
Discounts
Net
Revenue
Allowance for
Bad Debt
Less Bad
Debt Payor
Medicaid
Fee For
Service
Medicaid MC
Medicare
Commercial/
Other
Self-Pay
Total
Charges
$ 1,130,559
$ 765,982
$ 534,083
$ 952,558
$ 1,686,866
$ 5,070,047
$ 248,050
$ 441,324
$ 280,444
$ 882,510
$ 324,658
$ 253,639
$ 79,426
$ 29,219
$ 22,827
$ 548,820
$ 1,358,059
$ 2,876,696
$ 403,738
$ 328,807
$2,193,351
$ 36,336
$ 29,593
$ 197,402
$ 803,084
$ 295,439
$ 230,811
$ 367,401
$ 299,215
$ 1,995,949
From this report can also calculate per visit figures, collection percentages, and bad debt Percentages.
Curt Degenfelder Consulting, Inc.
25
Sample Report on Revenue and Visit Activity
February-07
Private Pay
Sliding Fee
Private Insurance
Visits
1,545
706
1,154
% of
Total
Visits
27.7%
Charges
$46,860
12.7% $69,829
20.7% $139,073
Medicare FQHC
Medicare Hospital Billing
Medicaid FQHC
Medicaid Hospital Billing
698
387
1,018
38
Special Billing 6
Total Clinic 5,580
12.5%
6.9%
$64,444
$45,459
18.2% $113,206
0.7% $61,269
0.1%
100.0%
$2,804
$546,142
Less
Adjustments
-$13,313
$51,866
$22,748
-$21,773
$47,322
-$128,914
$11,349
$388
-$29,858
Less
Allowance for
Doubtful Net
Accounts Revenue
$16,454 $43,719
-$54 $18,017
-$17 $116,341
% of
Total
Revenue
7.8%
3.2%
20.8%
$0
$0
$86,217
-$1,864
-$2 $242,122
$0 $49,920
$0 $2,416
$16,382 $559,618
15.4%
-0.3%
Net
Revenue per Visit
$28.30
$25.52
$100.82
$123.52
-$4.82
43.3% $237.84
8.9% $1,313.70
0.4%
100.0%
$402.61
$100.29
Dental 304
Pharmacy 3,406
Total Other
Grand Total 9,290
$22,624
$86,115
$108,739
$654,881
$28,300
$21,683
$49,983
-$11,944
-$1,373
$6,267
$65,805
-$13,316 $72,072
$20,126 $3,065 $631,690
$20.62
$19.32
Curt Degenfelder Consulting, Inc.
26
Analyzing Trends in Patient Revenue
Reasons why revenue decreases while visits increase:
• Retroactive settlement in prior period
• Poor collections in current year
• p y y more than any other payor
• Large bad debt write-off in the current period pertaining to old receivables currently on the books
• Rate Revisions
• Improper Coding
27
Curt Degenfelder Consulting, Inc.
9
Analyzing Shifts in Payor Mix
Effects of Changes in Payor Mix
Current Period Prior Year
Medicaid
Self - Pay
Total
Visits
6,256
5,554
Payor
Mix
53%
47%
Revenue per Visit
Total
Revenue Visits
$96 $597,812 6,500
$22 $122,188 3,500
Payor
Mix
65%
35%
Revenue per Visit
Total
Revenue
$100 $650,000
$20 $70,000
11,810 100% $61 $720,000 10,000 100% $72 $720,000
28
Curt Degenfelder Consulting, Inc.
Milestone Benchmarks for FFS Claims
Processing
During Encounter
Provider Completes
Encounter Info
In 1 Day
Billed to Payor
New goal – able to charge all patients at checkout
Usually within 45 days
Claim Denied?
Payment and
Remittance Advice
Received
Paid Claim? Then in 1 Week
Use your standard correction procedures and resubmit within 2 weeks
Reconcile
Payment and
Post Cash
Curt Degenfelder Consulting, Inc.
29
Measuring Revenue Cycle Staff Productivity –
Earned Minutes
April
Khanna, Anupam
Sanchez, Lourdes
Trong, Vang
Nalbandian, Aram
Aguilar, Martha
Dejesus, Corazon
Limpiado, Marina
Total/Average
Bill Processing
Monthly
Minutes
Worked
9,240
9,240
9,240
9,240
9,240
5,544
9,240
60,984
#
486
534
600
644
Standard
Minutes - 10
4,860
5,340
6,000
6,440
667
108
688
3,727
6,670
1,080
6,880
37,270
Correct Claims
Standard
#
Minutes -
5
2
17
7
18
10
85
35
90
18
56
71
189
90
280
355
945
Denial Processing
Standard
#
Minutes -
15
3
14
1
0
45
210
-
15
2
185
17
222
30
2,775
255
3,330
Total
Standard
Minutes
4,915
5,635
6,050
6,530
6,790
4,135
7,490
41,545
Efficiency
Rate
53.2%
61.0%
65.5%
70.7%
73.5%
74.6%
81.1%
68.1%
30
Curt Degenfelder Consulting, Inc.
10
Another Look at Billing Staff Productivity
April
Average
Sanchez, Lourdes
Trong, Vang
Aguilar, Martha
Dejesus, Corazon
Limpiado, Marina
Old Performance
New Performance
Monthly
Minutes
Worked
9,240
9,240
9,240
9,240
9,240
5,544
9,240
60,984
60,984
Bill Processing
#
534
600
667
108
688
3,727
Standard
Minutes - 10
5,340
6,000
6,440
6,670
1,080
6,880
37,270
Correct Claims
#
Standard
Minutes -
5
Denial Processing
#
Standard
Minutes -
15
17
189
7
18
56
71
85
35
90
280
355
945
14
1
2
185
17
222
210
15
-
30
2,775
255
3,330
Total
Standard
Minutes
6,295
5,635
6,050
6,530
6,790
4,135
7,490
41,545
42,925
Efficiency
Rate
68.1%
61.0%
65.5%
73.5%
74.6%
81.1%
68.1%
70.4%
By getting the worst performer to average performance, or by replacing the worst performer with an average performer, the health center could increase overall efficiency from 68% to over 70%, and get over 22 hours (1,380 minutes or .15 of an FTE) of service activity from the same number of staff.
Curt Degenfelder Consulting, Inc.
31
Analyzing Patient Receivables
What are the components of the patient receivable balance?
Gross Accounts Receivable
Less: Allowance for Contractual Adjustments
Equals: Net Accounts Receivable
When looking at revenue streams or accounts receivable, it is important that the analysis is based on net revenue and net accounts receivable.
Curt Degenfelder Consulting, Inc.
32
Analyzing Patient Receivables
• The best high-level analytical tool for evaluating patient receivables is to calculate
Days in Accounts Receivable.
• This is an indicator of the amount of revenue tied up in accounts receivable. Days in accounts receivable is an indicator of the length of time between the date a patient is seen and the date payment is received.
• Days in Accounts Receivable Calculation =
Gross A/R less allowance for doubtful accounts and contractual allowances
(Revenue, net of contractual allowances and bad debt expense, less capitation revenue ÷ 365 days)
33
Curt Degenfelder Consulting, Inc.
11
Patient Receivable Reports
Revenue Maximization Accounts
Receivable Metrics – Days in A/R
Current
Period
Prior
Period
Change
FAV/ (UNFAV) %
Weighted Total Days in Patient A/R
Medicaid Fee For Service
Medicaid Managed Care
Medicare
Commercial/Other
Self-Pay
Curt Degenfelder Consulting, Inc.
79.2
72.3
54.6
72.1
72.1
119.4
66.4
66.4
53.7
78.4
65.7
82.4
(12.79)
(5.90)
-19%
-9%
(0.90) -2%
6.30 8%
(6.40)
(37.00)
-10%
-45%
34
Financial Statements vs. Billing System
• To effectively manage patient receivables, the balances in the general ledger should reconcile to the billing system.
• Test the validity of the reports generated by the billing system and used for posting to the general ledger: Reconcile current month activity (gross per the aged accounts receivable reports.
• Test the validity both in total as well as by payor source.
• A re-calculation of the allowance for bad debts should be performed and posted on a monthly basis. This give a truer picture of net accounts receivable, thus what is more realistically owed to the health center.
35
Curt Degenfelder Consulting, Inc.
Analyzing Patient Receivables
Sample Analysis – Accounts Receivable Aging Trend:
Current Month
Prior Month
Total
79,500
70,500
2 Month's Prior 60,000
Current
$ %
31-60 days
$ %
61-90 days
$ %
91-120 days
$ %
120+ days
$ %
36
Curt Degenfelder Consulting, Inc.
12
Analyzing Patient Receivables
• Analyze trends in days in accounts receivable by payor:
– Is days in A/R less than 90?
– Are certain payors not paying on a timely basis?
• Total A/R:
– Has A/R been cleaned up to recognize bad debt?
– Has self pay been cleaned up?
– Has General Ledger been reconciled to the practice management system?
Curt Degenfelder Consulting, Inc.
37
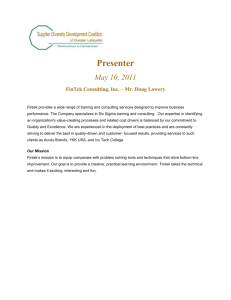
How Can You Recognize Improper Coding?
70%
60%
50%
40%
30%
UNDERCODER HEALTH CENTER
10%
0%
99211 99212 99213
National Average*
99214 99215
Undercoder
*Source: Ingenix, 2001
E&M Codes
99211
99212
99213
99214
Established Patient Visits
National Average*
% of Total
99215
Curt Degenfelder Consulting, Inc.
2.7%
20.6%
63.5%
11.3%
2.0%
Undercoder Health Center
# Visits % of Total
2,300
3,500
3,800
400
-
23.0%
35.0%
38.0%
4.0%
0.0% 38
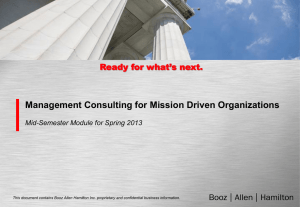
How Can You Recognize Improper Coding?
60%
50%
40%
30%
20%
10%
0%
When we add payor-based coding information, the differences may become even clearer:
Medicaid
Medicare
National
Average
99211 99212 99213 99214 99215
Commercial
Insurance
Self Pay
39
Curt Degenfelder Consulting, Inc.
13
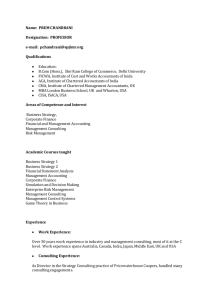
Denial Analysis
The analysis below shows the reasons why claims are denied and a sample frequency:
Reason
Charges covered under a capitated agreement
Claim not filed timely
Correct tooth info needed
Duplicate claim
Lack of authorization/referral
Lacks other info needed for adjudication
Paid current / conflicting claim
Patient ineligible
Patient ineligible (Another plan)
Patient ineligible at time of service
Provider ineligible
Service not covered - Plan
Service part of more global procedure
Unknown / Other
Total Denied Visits
#
890
506
89
5,798
% of Total
6.7%
3.8%
0.7%
43.5%
207
206
1,335
52
181
3,283
355
44
168
22
77
1.5%
10.0%
0.4%
1.4%
24.6%
2.7%
0.3%
1.3%
0.2%
0.6%
TOTALS
Curt Degenfelder Consulting, Inc.
13,323 100.0%
40
Front Desk Issues
• Training – there is frequently high turnover of front desk staff; and thus making sure that all staff understand their responsibilities is crucial
• Proper completion of registration form (make all tasks as selfexplanatory or routinized to reduce the amount of personal interpretation)
• Front desk may be the source of errors in billing system which then flow through to all other processes
• Ensuring that the correct patient is being recorded in the system
• Excessive wait times resulting from slow patient processing
• Eligibility verification
• A feedback loop with the billing department must be established so that front desk staff understand the impact of their actions.
Oftentimes the best form for the communication is a facilitated peer-to-peer interaction.
Curt Degenfelder Consulting, Inc.
41
Tracking Billing Errors Back to the Source
• Front desk
– Patient not eligible
– Incorrect demographic information, or outdated insurance coverage
– Not MCO primary care provider
• Providers
– Incorrect code
– Service not supported by diagnosis/documentation
– Service not covered
– Provider not eligible/credentialed
– NEW EHR issue…..Provider hasn’t completed Medical Record, thus claim won’t show as active in PMS
• Billing staff
– Duplicate bill
– Missing information
• Can also look at individuals
Curt Degenfelder Consulting, Inc.
42
14
Impact of Reducing Denials
Aguilar, Angie
Santana, Bonnie
Sandhu, Navjoat
Total
Monthly minutes
9,240
9,240
9,240
27,720
Patients registered
612
702
804
2,118
Earned
Minutes
4,896
5,616
6,432
16,944
Efficency
Rate
53.0%
60.8%
69.6%
61.1%
Errors Error Rate
72 11.8%
53
29
154
7.5%
3.6%
7.3% median 128 6.0%
• What are the other tasks being done by front desk staff and how do they impact efficiency and error rates?
• What is the revenue opportunity of 26 less errors per month?
• Time savings of 390 minutes (26 x 15 minutes to process each denial) per month
43
Curt Degenfelder Consulting, Inc.
15