CREDIT:
2.0
Continuing Education
EARN CE CREDIT FOR THIS ACTIVITY AT WWW.DRUGTOPICS.COM
AN ONGOING CE PROGRAM OF THE UNIVERSITY OF CONNECTICUT
SCHOOL OF PHARMACY AND DRUG TOPICS
educationaL oBJectiVeS
Goal: To assist pharmacists and pharmacy
technicians in understanding the impact of
electronic health record (EHR) systems on
pharmacy practice, as the use of EHR systems
continues to increase.
After participating in this activity, pharmacists
will be able to:
● Summarize the impact on pharmacy practice
of the new HHS rules governing the use of
electronic health record (EHR) systems.
● Identify the ways in which EHR systems will
increase the efficiency of pharmacy practice
with respect to continuity of care, formulary
checks, drug-to-drug and drug-to-allergy
interactions, and medication reconciliation.
● Summarize the challenges pharmacists face
as EHR systems come into increasingly
wider use.
● Apply the process of pharmacists using
EHRs to case scenarios
The University of Connecticut School of
Pharmacy is accredited by the Accreditation
Council for Pharmacy Education as a provider
of continuing pharmacy education.
Pharmacists are eligible to participate in both the
knowledge-based and application-based activities,
and will receive up to 0.2 CEUs (2 contact hours) for
completing the activity/activities, passing the quiz/
quizzes with a grade of 70% or better, and completing
an online evaluation. Statements of credit are available
via the online system.
Pharmacy technicians are eligible to participate in
the knowledge-based activity and will receive 0.1
CEU (1 contact hour) for completing the activity,
passing the quiz with a grade of 70% or better, and
completing the online evaluation. Statements of
credit are available via the online system.
ACPE #0009-9999-12-007-H04-P/T (Part 1)
ACPE #0009-9999-12-008-HO4-P (Part 2)
Grant Funding: Funding for this activity was provided by:
Cephalon; Endo Pharmaceuticals, Inc.; Purdue Pharma L.P.
Activity Fee: There is no fee for these activities.
Initial release date: 4/10/2012
Expiration date: 4/10/2014
To obtain immediate CPE credit, take the test online
at www.drugtopics.com/cpe. Just click on the link you
find under Free CPE Activities, which will take you to
the CPE site. For first-time users, please complete the
registration page. For those already registered, log
in, find, and click on this lesson. Test results will be
displayed immediately. Complete the evaluation form
and you will receive a printable statement of credit by
e-mail, showing your earned CPE credit.
For questions concerning the online CPE activities,
e-mail: cpehelp@advanstar.com.
the impact of electronic
health records on
pharmacy practice
Rachelle Spiro, RPh, FASCP
DIRECTOR, PHARMACY E-HEALTH INFORMATION TECHNOLOGY COLLABORATIVE, ALEXANDRIA, VA; CEO
AND PRESIDENT, SPIRO CONSULTING, INC., LAS VEGAS, NV
W
ith the American Recovery
and Reinvestment Act (ARRA),
which was signed into law in
2009, Congress set ambitious goals for
the nation to integrate information technology into healthcare delivery.1,2 A segment
of ARRA, the Health Information Technology for Economic and Clinical Health Act
(HITECH), authorized incentive payments
through Medicare and Medicaid to providers that use certified electronic health
records (EHRs) to achieve specified improvements in healthcare delivery and
implement a nationwide EHR system by
2014.3
At the bill’s enactment in 2009, only
11.9% of hospitals made any use of EHRs,
with only 2% meeting what would be stage
1 meaningful use criteria.4 Only 21.8% of
office-based physicians had basic electronic
systems and only 6.9% had fully functional
electronic systems.5 The U.S. Department
of Health & Human Services (HHS) finalized the meaningful use criteria for the first
2 years of the 3-stage incentive program
in mid 2010.5 The bill’s health information
technology (HIT) component followed the
earlier Office of the National Coordinator
(ONC) for Health Information Technology
created by presidential executive order in
Faculty: Rachelle Spiro, RPh, FaScP
Ms. Spiro is Director, Pharmacy e-Health Information Technology Collaborative, Alexandria, VA, and CEO
and President, Spiro Consulting, Inc., Las Vegas, NV. Editorial assistance was provided by Deborah
Kaplan. Ms. Kaplan’s revisions were reviewed and approved by Ms. Spiro.
Faculty Disclosure: Ms. Spiro has no actual or potential conflict of interest associated with this article.
Disclosure of Discussions of Off-Label and Investigational Uses of Drugs: This activity may contain discussion
of unlabeled/unapproved use of drugs. The content and views presented in this educational program are
those of the faculty and do not necessarily represent those of Drug Topics or University of Connecticut
School of Pharmacy. Please refer to the official prescribing information for each product for discussion
of approved indications, contraindications, and warnings.
46
Drug topics
April 2012
DrugTopics .c om
GETTY IMAGES/PHOTODISC/MACIEJ FROLOW
After participating in this activity, pharmacy
technicians will be able to:
● Recognize the impact on pharmacy practice
of the new HHS rules governing the use of
EHR systems.
● Identify the ways in which EHR systems will
increase the efficiency of pharmacy practice
with respect to continuity of care, formulary
checks, drug-to-drug and drug-to-allergy
interactions, and medication reconciliation.
● Recognize the challenges pharmacists face as
EHR systems come into increasingly wider use.
continuing education
glossary of terms
ACO
ADEs
ARRA
CAH
CCD
CDS
CMR
CMS
CPOE
CPT
DEA
EHR
EMR
EPCS
ePHR
Accountable care
organization
Adverse drug events
American Recovery and
Reinvestment Act
Critical access hospital
Continuity-of-care document
Clinical decision support
Comprehensive medication
review
Center for Medicare and
Medicaid Services
Computerized provider order
entry
Current procedural
terminology
Drug Enforcement Agency
Electronic health record
Electronic medical record
Electronic prescribing for
controlled substances
Electronic personal health
record
U.S. Department of Health &
Human Services
Health Insurance Portability
and Accountability Act
Health Information
Technology for Economic
Clinical Health
Health information exchange
Health information
technology
Health Level Seven
Long-term care
Medical therapy management
Office of the National
Coordinator
Primary care physician (or
provider)
Personal health record
Pharmacy management
system
Pharmacy/pharmacist
provider electronic health
record
Abstract
The American Recovery and Reinvestment Act of 2009 set ambitious goals for
the nation to integrate information technology into healthcare delivery. The
Health Information Technology for Economic and Clinical Health Act segment of
the bill provides incentives for Medicare and Medicaid providers to use certified
electronic health records (EHRs) to achieve specified improvements in healthcare
and implement a nationwide EHR system by 2014. Meaningful use criteria
are being promulgated in 3 stages. Medicare and Medicaid incentive payments
will total $27 billion over a 10-year period with $17 billion designated for
EHR development. Pharmacists will not receive direct funding or incentives but
pharmacy schools may receive grants for incorporating electronic personal health
technology into clinical education. The nation’s goal for EHRs is to reduce costs
through less paperwork, improved safety, and reduced duplication of testing, and
improve health by gathering a patient’s entire health information in a single
location. Electronic connectivity through e-prescribing—the paperless, real-time
transmission of standardized prescription data among prescribers, pharmacies,
and payers—places pharmacists squarely within the healthcare technology team.
The Pharmacy e-Health Information Technology (HIT) Collaborative, a group of
9 national pharmacy organizations and associate members, advocates integrating
the pharmacist’s role of providing patient care services into the national HIT
interoperable framework. The greatest challenge that pharmacists face in the new
era of electronic health information is to be recognized by Medicare and Medicaid
as eligible providers of medication-related patient care services and as meaningful
use contributors to electronic health information.
The primary goals of improving the nation’s HIT infrastructure are to:
• Ensure protection and privacy of
HIPAA
healthcare information;
• Improve patient care by reducing
HITECH
medical errors;
• Reduce costs by removing administrative
barriers that result in duplicative claims
HIE
and services; and
HIT
• Improve coordination of care among
healthcare providers.
HL7
To achieve these goals, as much as $27
LTC
billion over 10 years was designated in MediMTM
care and Medicaid incentive payments for
ONC
eligible providers who use EHRs and demonstrate “meaningful use” of HIT.3 In addition,
HIT systems have to be certified as meetPCP
ing certain technologic standards. A total of
$19 billion was designated to implement HIT
PHR
regional health information exchange (HIE)
PMS
networks.1,3 Of this amount, $17 billion includes the incentive payments to physicians
PP-EHR
and hospitals to develop personal healthcare
records by 2014. The remaining $2 billion
is allocated to developing and improving the
2004.6 ONC works with the Center for Medi- nation’s HIT infrastructure.1,3
care and Medicaid Services (CMS) to set the
The Congressional Research Service
policies relevant to incentive payments under expects that the incentives will promote
meaningful use requirements.7
EHR use in 70% of hospitals and 90% of
HHS
DrugTopics .c om
physician offices by 2019.8 The Congressional Budget Office has projected that
HITECH will reduce federal and private sector spending on health services during the
next decade by tens of billions of dollars
by increasing efficiency.9 By October 2011,
$1.2 billion incentives had been paid.7 Preliminary data for 2011 show the use of
EHRs growing, but the goals for 2019 are
considered ambitious.10
Pharmacists will not receive direct funding or incentives for adopting electronic
medical record technology. Pharmacy
schools, however, are included among the
list of approved graduate schools that may
receive grants for incorporating electronic
personal health technology into clinical education.1 Stage 1 of the 3-stage meaningful
use program launched in 2010 focuses
on the integration of electronic healthcare
among patients, providers, government
agencies, and insurers. There are 25 Medicare and Medicaid meaningful use criteria,
of which eligible professionals must adopt
15 professional core objectives to qualify
for the incentives (Table 1, page 48).7
Eligible professionals can receive as much
as $44,000 over a 5-year period through
Medicare. For Medicaid, eligible professionApril 2012
Drug topics
47
eLectRonic HeaLtH RecoRdS
Continuing Education
TABLE 1
TABLE 2
proFessional core oBJecTives required For Medicare and
Medicaid incenTives
1. Use CPOE
2. Implement drug-drug and drug-allergy interaction checks
3. Maintain an up-to-date problem list of current and active diagnoses
4. Generate and transmit permissible prescriptions electronically
5. Maintain an active medications list
6. Maintain an active medications allergy list
7. Record demographics (preferred language, gender, race, ethnicity, date of birth)
8. Record vital signs and chart changes (height, weight, blood pressure, BMI, growth charts for
children aged 2 to 20 years)
9. Record smoking status for patients aged 13 years or older
10. Report ambulatory clinical quality measures
11. Implement clinical decision support rule as determined by the eligible professional
12. Provide patients with an electronic copy of their health information
13. Provide clinical summaries for patients for each office visit
14. Capability to exchange key clinical information electronically (eg, problem list, medication list,
diagnostic test results) among care providers and patient-authorized entities
15. Protect electronic health information by use of certified technology
Abbreviations: BMI, body mass index; CPOE, computerized provider order entry.
Source: Ref 7
als can receive as much as $63,750 over 6
years.11 The first incentives were scheduled
for October 2011 based on 2010 performance. By 2015, physicians who are not
using certified EHRs could be penalized by
Medicare and Medicaid.12
In February 2012, federal officials released the stage 2 guidelines for meaningful use.11 The proposed stage 2 rules,
which are undergoing review at this time,
require physicians and hospitals to significantly increase their use of electronic
health information, as well as better engage patients and improve the transferability of records.13 The meaningful use
approach requires identification of standards structured in uniform ways so that
EHR systems can deliver the information
just as commonly used automated teller
machines depend on uniformly structured
data.7 If data cannot be captured uniformly, electronic systems cannot communicate or are not interoperable.14,15 Stage 2
meaningful usage will require that at least
60% of patients have their medications
and laboratory tests ordered electronically
instead of the 30% required by the stage
1 regulations. The government is placing
48
Drug topics
April 2012
emphasis on having electronic systems
that are interoperable or can communicate with each other. Thus, the 2012
stage 2 rules require that systems be able
to transfer patient information including a
patient’s notes, medications list, allergies,
and diagnostic and laboratory test results
across platforms. The information should
also be available to patients to view their
records online as well as download and
transfer information. Additionally, patients
should be able to communicate with their
physicians through a secure, online system or patient portal.13
integrating pharmacy
health information in
u.s. healthcare
Often the terms electronic medical record
(EMR) and electronic health record (EHR)
technology are used interchangeably.
EHR is defined as “an electronic record of
health-related information on an individual
that is created, gathered, managed, and
consulted by authorized healthcare clinicians and staff.”11 The personal health
record (PHR) is defined as “an electronic
record of individually identifiable health
BeneFiTs oF MeaningFul
use oF ehrs
By adopting EHRs in a meaningful
way, healthcare providers can:
» Know more about their patients.
Information in EHRs can be used to
coordinate and improve the quality
of patient care.
» Make better decisions. With more
comprehensive information readily
and securely available, healthcare
providers will have the information
they need about treatments and
conditions – even best practices for
patient populations – when making
treatment decisions.
» Save money. EHRs require an
initial investment of time and
money, but healthcare providers
who have implemented them have
reported reductions in the amount
of time spent locating paper files,
transcribing, and spending time on
the phone with labs or pharmacies;
more accurate coding; and
reductions in reporting burden.
Abbreviations: EHR, electronic health record.
Source: Ref 11
information on an individual that can be
drawn from multiple sources and that is
managed, shared, and controlled by and
for the individual.”11 The EHR differs from
the EMR in that it contains information that
is shared among healthcare providers using
interoperability standards.6 The EHR is an
individual patient’s medical record in digital,
interoperable format that includes the patient’s demographics, medical history, allergies, medications, progress notes, laboratory and diagnostic test results, scans, and
advance directives. It contains data from
many sources and can communicate with
various health and medical entities.6
An electronic tool that is initiated by the
patient is the electronic personal health record (ePHR).6 In contrast to the EHR, which
is generated by healthcare providers, the
ePHR can be generated by physicians, patients, hospitals, pharmacies, and other
sources but is managed by the patient.11
Ultimately, it is the ePHR that healthcare
analysts consider the best electronic tool
to address concerns about privacy issues
DrugTopics .c om
continuing education
with electronic health information.16
The nation’s goal for EHRs is to reduce
costs through less paperwork, improved safety, reduced duplication of testing, and improve
health by gathering a patient’s entire health
information in a single location. Additionally,
EHRs can compute the information. For example, a qualified EHR not only contains a
record of a patient’s medications or allergies
but also automatically checks for problems
whenever a new medication is prescribed and
alerts the clinician to potential conflicts.7 The
meaningful use of EHRs and HIEs can help
clinicians provide higher quality and safer care
for their patients (Table 2, page 48).11
For the purposes of the Medicare and
Medicaid incentive programs, eligible professionals, eligible hospitals, and critical access hospitals (CAHs) must use certified
EHR technology. The federal government
has established certification standards
consistent with requirements for meaningful use.17 Certified EHR technology gives
assurance to purchasers and other users
that an EHR system or module offers the
necessary technologic capability, functionality, and security to help them meet the
meaningful use criteria. Certification also
helps providers and patients be confident
that the electronic HIT products and systems they use are secure, can maintain
data confidentially, and can work with other
systems to share information.11
The PP-EHR is the pharmacy/pharmacist provider electronic health record. The
Pharmacy e-HIT Collaborative, a group of
9 national pharmacy organizations and associate members, continues to work with
national EHR certification organizations and
pharmacy system vendors to assure that
the PP-EHR functionality is adopted with
the development of certification criteria to
meet the meaningful use of EHR concepts
related to pharmacy services.18 Members
of the Collaborative were involved in working
with a joint Health Level Seven (HL7) and National Council for Prescription Drug Programs
(NCPDP) work group in the development of
the PP-EHR functional profile, an HL7 functional profile that represents “the functionality required and desired for a care setting or
application, or reflect the functionality incorporated in a vendor’s EHR system.”18
To elaborate further, from a standards
perspective, all EHRs follow HL7 functionalDrugTopics .c om
TABLE 3
inTerneT resources For
e-prescriBing
www.cms.hhs.gov/eprescribing
www.ehealthinitiative.org
www.himss.org
www.nationalerx.com
www.surescripts.com
ity. Each provider type can adopt a standard
HL7 EHR functional profile (e.g., pharmacists can adopt a pharmacist EHR specific
for documentation of pharmacist-provided
patient care information). These are different from claims-based standards used by
pharmacists for billing prescriptions such
as NCPDP version D.0.
Each provider
type can adopt a
standard HL7 EHR
functional profile.
e-prescribing: use,
benefits, challenges
Electronic connectivity through electronic
(e)-prescribing—the paperless, real-time
transmission of standardized prescription
data among prescribers, pharmacies, and
payers—places pharmacists squarely
within the healthcare technology team.19
E-prescribing communicates medications
history, new prescriptions, changes, refills,
and other prescription data. In 2000, the
Institute of Medicine recommended that
e-prescribing be in place for all prescriptions by 2010. Although short of that goal,
by 2010 more than 300 million prescrip-
tions were being routed electronically.20
More than half of office-based physicians
in the United States are reported to use
e-prescribing.21 The number of pharmacies connected electronically also continues to increase. According to Surescripts,
91% of community pharmacies in the
United States in 2010 were connected
for prescription routing compared with
76% in 2008. For independently owned
pharmacies, 73% were connected in 2010
compared with 46% in 2008.20
A national survey reported that community pharmacists and technicians were generally satisfied with e-prescribing because
of the improved legibility of electronic prescriptions and more efficient processing.22
Pharmacists in the survey also noted that
refill prescriptions and new prescriptions
required less staff time. Prescribing errors
were the most commonly cited negative
feature of e-prescribing, particularly those
which called for a wrong drug or gave erroneous directions.22
In more than 100 interviews with physician practices and pharmacies nationwide
this past year, researchers at the Center
for Studying Health System Change noted
flaws and inconsistencies concentrated in
3 critical areas in e-prescriptions. These include prescription renewals, connectivity between physician offices and mail-order pharmacies, and manual entry of prescription
information by pharmacists.23 Moreover,
pharmacies and physicians report duplicate or conflicting messages. Significantly,
short-cut features fail to aid that message
and communication fields that complete
automatically often require follow-up calls
or manual entry by pharmacists to clarify a
physician’s orders, verify quantities and sig
codes (pharmacy terminology), or provide
patient-friendly instructions.23
One barrier to e-prescribing—maintenance of a parallel paper system for controlled substances—essentially ended
pause&ponder
according to a national survey, community pharmacists
and technicians were generally satisfied with
e-prescribing because of the improved legibility of
electronic prescriptions. However, are you still following
up frequently with physicians to clarify orders?
April 2012
Drug topics
49
eLectRonic HeaLtH RecoRdS
Continuing Education
TABLE 4
TABLE 5
10 goals For pharMacy inTegraTion in healThcare sysTeM
vocaBulary sTandards
For elecTronic healTh
inForMaTion (code seTs)
1. Ensure HIT supports pharmacists in healthcare service delivery
2. Achieve integration of clinical data with electronic prescription (e-prescribing) information
3. Advocate pharmacist recognition in existing programs and policies
4. Ensure HIT infrastructure includes and supports MTM services
5. Integrate pharmacist-delivered immunizations into the EHR
6. Achieve recognition of pharmacists as meaningful users of EHR quality measures
7. Advance system vendor EHR certification
8. Promote pharmacist adoption and use of HIT and EHRs
9. Achieve integration of pharmacies and pharmacists into health information exchanges
10. Establish the value and effective use of HIT solutions by pharmacists
Abbreviations: EHR, electronic health record; HIT, health information technology; MTM, medication therapy management.
Source: Ref 18
when the prohibition against e-prescribing
for controlled substances (EPCS) was
amended in 2010 when the U.S. Drug Enforcement Administration (DEA) issued new
regulations that provide practitioners with
the option of EPCS. The revised DEA regulations also permit pharmacies to receive,
dispense, and archive electronic prescriptions.24 It is important to note, however, that
not all states have authorized EPCS, particularly Schedule II controlled substances.
For more information on e-prescribing,
please consult the websites listed in Table
3, page 49.
EHr systems increase
efficiency of pharmacy
practice, improving patient
outcomes
The Pharmacy e-HIT Collaborative advocates integrating the pharmacist’s role of
providing patient care services into the
national HIT interoperable framework.18
The Collaborative has issued a 10-goal
plan entitled “The Roadmap for Pharmacy
Health Information Technology Integration in U.S. Health Care” to promote the
inclusion of pharmacists as recognized
providers of the CMS HIT strategy (Table
4).18 The Collaborative states that pharmacists have an important role in optimal
therapeutic outcomes and safe and costeffective medication use and that the clinical services of pharmacists are a critical
component of the U.S. healthcare system.
For example, the ability to report adverse
drug events (ADEs) within the EHR and integrate reports on a national level allows
for tracking ADEs and early identification
of potentially dangerous medication side
effects.18
Medication therapy management (MTM),
which can optimize therapeutic outcomes
for individual patients, is a unique area of
contribution for pharmacy.25 Pharmacists
are key information providers in MTM, including medication reconciliation and care
transitions, medication adherence, medication monitoring, medication safety, and
evaluation of medication errors.18
MTM core elements include: medication
therapy review; personal medication record;
medication-related action plan; intervention
and referral; and documentation.18 Sharing
components of MTM between providers by
means of the continuity-of-care document
(CCD) demonstrates the value of meaningful use of the EHR by pharmacists. The
pause&ponder
Pharmacists have an important role in optimal
therapeutic outcomes and safe and cost-effective
medication use. are pharmacists in your practice setting
utilized appropriately to help during transitions of care?
50
Drug topics
April 2012
Codes sets are used for encoding
data elements, such as medical
concepts, diagnoses, or procedures.
(Nonmedical code sets, also known
as administrative code sets, encode
nonmedical data, including ZIP code,
state abbreviations.)
» Clinical terms. Systematized
Nomenclature of Medicine Clinical
Terms (SNOMED CT)
» Diagnosis codes: ICD-10 (coding
for all providers covered by the
Health Insurance Portability and
Accountability Act (HIPAA)
» Laboratory test results. Logical
Observation Identifiers Names and
Codes (LOINC)
» Medications. RxNorm, a standardized
nomenclature for clinical drugs and
drug delivery devices, is produced by
the National Library of Medicine.
» Immunizations. Code set for
vaccines administered (CVX)
Source: Ref 7
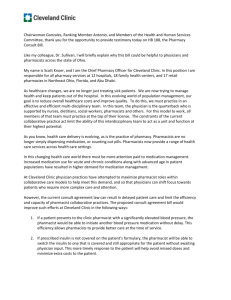
MTM core elements service model illustrates how pharmacists can interface with
the patient care process (Figure 1, page
51). The process begins with medication
therapy review. The patient interview is
conducted and a database with patient
information is created. Medications are reviewed for indication, effectiveness, safety,
and adherence. A list of medication-related problems is generated and prioritized,
generating a MTM plan. Intervention and/
or referrals involve patient, physician, pharmacist, or other healthcare professionals.
It is estimated that more than half of
medication errors occur during patient care
transitions.26 The proposed 2012 stage 2
meaningful use objectives require that medication reconciliation be conducted by 65%
of care transitions by the receiving providers.18 Therefore, medication reconciliation
at transitions of care should be part of the
EHR documentation process in all practice
settings.18 At a minimum the following information should be communicated electronically to pharmacists at transitions of care:
medications list, medical condition, and allerDrugTopics .c om
continuing education
FIGURE 1
The Medication Therapy Management Core Elements Service Model
The diagram depicts how the MTM Core Elements (❖) interface with the patient care process to create an MTM Service Model.
❖
MEDICATION THERAPY REVIEW
❖
INTERVENTION AND/OR REFERRAL
Interview patient and create
a database with patient
information
Possible referral of patient
to physician, another pharmacist or other healthcare
professional
Review medications for indication, effectiveness, safety, and
adherence
Interventions directly with patients
List medication-related
problem(s) & Prioritize
Create a plan
❖
Implement
Plan
Interventions via collaboration
Create/Communicate
PERSONAL
MEDICATION
RECORD (PMR)
Create/Communicate
MEDICATIONRELATED ACTION
PLAN (MAP)
❖
Complete/Communicate
& Conduct
Physician and other healthcare
professionals
❖
DOCUMENTATION &
FOLLOW-UP
Used with permission. Copyright © 2008 by the American Pharmacists Association and the National Association of Chain Drug Stores Foundation. All rights reserved.
Source: Ref 18
gies. For optimal medication management,
pharmacists should receive the full content
of the CCD including laboratory values, prescriber information, and medication history.18
The process of medication reconciliation
includes comparing a patient’s medication
orders to all the medications that the patient has been taking, and it should be undertaken at every transition of care in which
new medications are ordered or existing orders are rewritten. The principles of medication reconciliation must be incorporated
into EHR systems, and to ensure that it is
done appropriately, professional guidelines
should be implemented and overseen by
pharmacists.18
Medication adherence is a basic component of comprehensive MTM. The Collaborative states that with access to electronic
health information from the CCD, pharmacists and other providers can better assess medication adherence outcomes and
address medication-related problems such
as drug-drug and drug-allergy interactions.18
Further, CMS recognizes the role of
pharmacists as MTM providers under the
Medicare Part D program. This includes
pharmacist-provided education counseling
for beneficiaries, compliance programs
such as refill reminders and special packaging, and detection of adverse events and
patterns of prescription drug overuse and
DrugTopics .c om
under use. Because of their professional
knowledge and capabilities, pharmacists
should be recognized as meaningful users
of the EHR in matters of Medicare Part D.18
Challenges pharmacists
face as EHR systems come
into increasingly wider use
The greatest challenge that pharmacists
face in the new era of electronic health
information is to be recognized as eligible
providers by Medicare and Medicaid and
by accountable care organizations (ACOs)
of medication-related patient care services
and as meaningful users and contributors
to EHR. As a first step, the Collaborative
of pharmacy organizations urges that
e-prescribing be adopted in all practice
settings. Further, pharmacists should
exchange clinical information with each
other and other healthcare providers in a
bidirectional manner. Pharmacists need
to work with pharmacy system vendors to
set communications standards and build
awareness of the standardized certified
pharmacist EHR functional profile.18 Such
alliances support meaningful use and enable pharmacies to support improvements
in care, safety, cost, and health outcomes.
A recent example of such collaboration
is the announcement by Walgreens that all
of the 7,800 Walgreens and Duane Reade
pharmacies and 350 Take Care Clinics
nationwide will use the Surescripts clinical
interoperability network to deliver immunization records to the patient’s primary care
provider.27 Currently, records such as inpharmacy immunizations have been sent
to physicians by fax or traditional mail. By
using the electronic network, pharmacists
and pharmacy healthcare providers contribute to the compilation of more complete
medical histories for their patients.27
In the 2011-2012 flu season, more
than 27,000 certified immunizing pharmacists, nurse practitioners, and physician
assistants at Walgreens and Duane Reade
pharmacies and Take Care Clinics administered more than 5.5 million immunizations.
Surescripts will use a standard format to
capture immunization details and send
the record to the patient’s primary care
physician in whatever form the provider is
able to receive it, electronically or via fax
or mail. Physicians using a Surescriptscertified EHR, however, will have the option of receiving immunization records via
the Surescripts Clinical Interoperability
Network.27
The pharmacy profession is actively
contributing to quality patient care through
MTM services that identify and prevent
medication-related problems, improve medication use, and optimize individual patient
April 2012
Drug topics
51
eLectRonic HeaLtH RecoRdS
Continuing Education
therapeutic outcomes. As MTM programs
continue to expand within the healthcare
system, however, the lack of standardization for documentation and billing of MTM
services is limiting its use and is a barrier
to MTM service delivery for patients.28 To
allow for the interchange of electronic information, pharmacists need to champion
e-prescribing standards and use current
procedural terminology (CPT) billing codes
for MTM services.6 Table 5 (page 50) identifies common code sets.7
Pharmacy organizations large and small
must recognize that implementing HIT requires designing workflow management to
overcome the disruption that arrives with
new technologic practices.6 The negative
impact of HIT implementation on care processes, workflow, and safety is known and
was the subject of a Joint Commission alert
in 2008.29 Stresses placed on healthcare
providers and staff when workflow is compromised by new technology systems can
produce technology-related adverse events.6
The USP MEDMARX for 2006 reported that
one-quarter of more than 175,000 medication errors involved some aspect of computer technology.30 For example, an actual increased risk for HIT-related medication errors
was reported in a study of a computerized
provider order entry (CPOE) system.31 Examples included fragmented CPOE displays
that conveyed erroneous information about
patient medications and orders.
To evaluate the effects of CPOE with
clinical decision support (CDS) on ADEs,
researchers reviewed the medical literature
for original investigations, randomized and
nonrandomized clinical trials, and observational studies.32 They found studies that
identified the type of computer system
used, drug categories evaluated, types of
ADEs measured, and clinical outcomes.
Of the 543 citations identified, 10 studies
met inclusion criteria. These studies were
grouped into categories based on their setDownload or take the test online at
www.drugtopics.com/cpe
once there, click on the link below
Free cpE Activities
52
Drug topics
April 2012
ting: hospital or ambulatory; no studies
related to the long-term care setting were
identified. In 5 (50%) of the 10 studies,
CPOE with CDS contributed to a statistically significant decrease in ADEs (P ≤.05).
Four studies (40%) reported a nonstatistically significant reduction in ADE rates, and
1 study (10%) demonstrated no change in
ADE rates.32
At a study at a 700-bed academic medical center in Chicago, clinical staff pharmacists saved all orders that contained a prescribing error for a week in early 2002.33
The investigators classified drug class,
error type, proximal cause, phase of hospitalization, and potential for patient harm
and rated the likelihood that CPOE would
have prevented the prescribing error. A total
of 1,111 prescribing errors were identified
(62.4 errors per 1,000 medication orders),
most occurring on admission (64%). Of
these, 30.8% were rated clinically significant and were most frequently related to
anti-infective medication orders, incorrect
dose, and medication knowledge deficiency. Of all verified prescribing errors, 64.4%
were rated as likely to be prevented with
CPOE (including 43% of potentially harmful
errors), 13.2% unlikely to be prevented with
CPOE, and 22.4% possibly prevented with
CPOE depending on specific CPOE system
characteristics. The investigators concluded
that although prescribing errors are common in the hospital setting, CPOE systems
could improve practitioner prescribing. The
design and implementation of a CPOE system should focus on errors with the greatest potential for patient harm. Pharmacist
involvement, in addition to a CPOE system
with advanced CDS, is vital for medication
safety.33
conclusion
As members of the electronically connected healthcare team, pharmacists
have the unique knowledge, expertise,
and responsibility to assume a significant
role in electronic health information. And
as governments and the healthcare community develop strategic plans for the
widespread adoption of HIT, pharmacists
must use their knowledge of information
systems and the medication use process
to ensure that the new technologies lead
to better patient outcomes.
References
1. American Recovery and Reinvestment Act of 2009.
http://www.recovery.gov/About/Pages/The_Act.
aspx#act. Accessed March 20, 2012.
2. Gold MR, McLaughlin CG, Devers KJ, Berenson
RA, Bovbjerg RR. Obtaining providers’ ‘buy-in’ and
establishing effective means of information exchange
will be critical to HITECH’s success. Health Aff
(Millwood). 2012;31(3):514–526.
3. Health Information Technology for Economic and
Clinical Health (HITECH) Act, Title XIII of Division A and
Title IV of Division B of the American Recovery and
Reinvestment Act of 2009 (ARRA), Pub. L. No. 1115 (Feb. 17, 2009), codified at 42 U.S.C. §§300jj et
seq.; §§17901 et seq. Updated September 28, 2011.
http://healthit.hhs.gov/portal/server.pt/community/
healthit_hhs_gov__regulations_and_guidance/1496.
Accessed March 20, 2012.
4. Jha AK, DesRoches CM, Kralovec PD, Joshi MS. A progress
report on electronic health records in US hospitals. Health
Aff (Millwood). 2010;29(10):1951–1957.
5. Hsiao C-J, Hing E, Socey TC, Cai B. Electronic medical
record/electronic health record systems of office-based
physicians: United States, 2009 and preliminary 2010
state estimates. Health E-Stats. Hyattsville, MD: National
Center for Health Statistics. 2010. http://www.cdc.
gov/nchs/data/hestat/emr_ehr_09/emr_ehr_09.pdf.
Accessed March 20, 2012.
6. Webster L, Spiro RF. A new world for pharmacy.
Pharmacy Today. 2010;16:32–44.
7. Centers for Medicare and Medicaid Services. CMS EMR
meaningful use overview. Baltimore, MD: CMS. Last
modified December 8, 2011. https://www.cms.gov/
EHRIncentivePrograms/01_Overview.asp#TopOfPage.
Accessed March 20, 2012.
8. Redhead CS. The Health Information Technology for
Economic and Clinical Health (HITECH) Act: CRS report
for Congress. Washington, DC: Congressional Research
Service; February 23, 2009.
9. Stark P. Congressional intent for the HITECH act. Am J
Manag Care. 2010;16(12 Suppl HIT):SP24-SP28.
10. Hsiao C-J, Hing E, Socey TC, Cai B. Electronic health record
systems and intent to apply for meaningful use incentives
among office-based physician practices, United States
2001–2011. Hyattsville, MD: National Center for Health
Statistics; 2011, Data Brief No. 79. Revised February 8,
2012. http://www.cdc.gov/nchs/data/databriefs/DB79.pdf.
Accessed March 20, 2012.
11. U.S. Department of Health & Human Services. Office
of the National Coordinator for Health Information
Technology. Health IT. Washington, DC: HHS. Updated
February 18, 2011. http://www.healthit.hhs.gov/.
Accessed March 20, 2012.
12. Healthcare Finance News. Eligible provider
meaningful use criteria. December 31, 2009. www.
healthcarefinancenews.com/news/eligible-providermeaningful-use-criteria. Accessed March 20, 2012.
13. Torres C. Electronic health records program advances
to ‘stage 2.’ Capsules, KHN blog. Kaiser Health News,
February 24, 2012. http://capsules.kaiserhealthnews.
org/index.php/2012/02/health-it-coordinator-releaseof- stage-2-guidelines-a-push-ahead/. Accessed March
20, 2012.
14. Diamond CC, Shirky C. Health information technology:
A few years of magical thinking? Health Aff (Millwood).
2008;27(5):383–390.
15. Hammond WE, Bailey C, Boucher P, Spohr M, Whitaker
P. Connecting information to improve health. Health Aff
(Millwood). 2010;29(2):284–288.
16. Healthcare Information and Management Systems
Society. HIMSS’ PHR and ePHR definition and position
statement. http://www.himss.org/asp/topics_news_item.
asp?cid=67200&tid=34. Accessed March 20, 2012.
17. Bean C. Certification programs. Presentation at: Office
of the National Coordinator for Health Information
DrugTopics .c om
continuing education
Technology Annual Meeting; Washington, DC,
November 16–18, 2011.
18.Pharmacy e-Health Information Technology
Collaborative. The Roadmap for Pharmacy Health
Information Technology Integration in U.S. Health
Care. http://www.pharmacyhit.org/pdfs/11-392_
RoadMapFinal_singlepages.pdf. Accesssed March
20, 2012.
19.Spiro RF, Gagnon JP, Knutson AR. Role of health
information technology in optimizing pharmacists’
patient care services. J Am Pharm Assoc (2003).
2010;50(1):4–8.
20.Surescripts. The National Progress Report on
E-Prescribing and Interoperable Healthcare 2010.
http://www.surescripts.com/pdfs/national-progressreport.pdf. Accessed March 20, 2012.
21.Surescripts. Surescripts announces that majority
of doctors in U.S. now use e-prescribing. http://
www.surescripts.com/news-and-events/pressreleases/2011/november/0911_safer x.aspx.
Accessed March 20, 2012.
22.Rupp MT, Warholak TL. Evaluation of e-prescribing
in chain community pharmacy: Best-practice
recommendations. J Am Pharm Assoc (2003).
2008;48(3):364–370.
23.Enderle L. The pitfalls of e-prescribing. Pharmacy Times.
November 29, 2011. http://www.pharmacytimes.com/
web-exclusives/The-Pitfalls-of-E-Prescribing. Accessed
March 20, 2012.
24.U.S. Department of Justice. Drug Enforcement
Administration. Office of Diversion Control. Electronic
prescriptions for controlled substances clarification.
http://www.deadiversion.usdoj.gov/fed_regs/
notices/2011/fr1019.htm. Accessed March 20, 2012.
25.Bluml BM. Definition of medication therapy
management: Development of professionwide
c o n s e n s u s . J A m P ha r m A s s o c (20 0 3).
2005;45(5):566–572.
26.National Transitions of Care Coalition. Transitions
of Care Measures, Paper by the NTOCC Measures
Work Group, 2008. http://www.ntocc.org/Portals/0/
TransitionsOfCare_Measures.pdf. Accessed March
20, 2012.
27.Surescripts. Walgreens and Surescripts improve
coordination of care by electronically delivering
immunization and patient summary records to
primary care providers. March 12, 2012. http://
www.surescripts.com/news-and-events/pressreleases/2012/march/312_walgreens.aspx. Accessed
March 20, 2012.
28.Millonig MK. Mapping the route to medication
therapy management documentation and billing
standardization and interoperabilility within the health
care system: meeting proceedings. J Am Pharm Assoc
(2003). 2009;49(3):372–382.
29.The Joint Commission. Safely implementing health
information and converging technologies. Sentinel
Event Alert, Issue 42, December 11, 2008. http://www.
jointcommission.org/sentinel_event_alert_issue_42_
safely_implementing_health_information_and_
converging_technologies/. Accessed March 20, 2012.
30.USP U.S. Pharmacopeial Convention. MEDMARX
2006 data report. www.usp.org/products/medMarx.
Accessed March 20, 2012.
31.Isaac T, Weissman JS, Davis RB, et al. Overrides of
medication alerts in ambulatory care. Arch Intern Med.
2009;169(3):305–311.
32.Wolfstadt JI, Gurwitz JH, Field TS, et al. The effect of
computerized physician order entry with clinical decision
support on the rates of adverse drug events: A systematic
review. J Gen Intern Med. 2008;23(4):451–458.
33.Bobb A, Gleason K, Husch M, Feinglass J, Yarnold PR,
Noskin GA. The epidemiology of prescribing errors:
The potential impact of computerized prescriber order
entry. Arch Intern Med. 2004;164(7):785–792.
DrugTopics .c om
test questions
1.
Results from a study evaluating prescribing errors
during 1 week in 2002 at a 700-bed academic
medical center showed that:
a. Most prescribing errors occurred at
discharge from the hospital.
b. Of all verified prescribing errors, 64.4% were
likely to be prevented with a computerized
provider order entry (CPOE) system.
c. Prescribing errors are uncommon in a large
academic setting.
d. The errors rated clinically significant were
most frequently related to antihypertensive
medication.
2.The goals of “The Roadmap for Pharmacy Health
Information Technology Integration in U.S. Health
Care” include:
a. Ensure federal incentives for pharmacists
b. Ensure medication standards for hospital
formularies
c. Achieve unique pharmacy coding for
pharmacy-provided immunizations
d. Achieve recognition of pharmacists as
meaningful users of electronic health record
(EHR) quality measures
3.The 15 professional core objectives required for
Medicare and Medicaid incentives include:
a. Record smoking status for adults (aged 20
years or older) only
b. Record vital signs and chart changes for
children from newborn to 20 years
c. Use a CPOE system
d. Provide patients with paper and electronic
copies of their health information
4.According to Surescripts, what percentage
of community pharmacists in the United
States are connected for routing prescriptions
electronically?
a. 73%
b. 76%
c. 82%
d. 91%
5.Because of recent changes in Drug Enforcement
Agency regulations, which of the following is no
longer a barrier to electronic prescribing?
a. Short-cut features that automatically
complete information fields
b. Pharmacists’ investment in electronic
software
c. Manual prescription information entry
d. Prohibition against electronic prescribing for
controlled substances
6.The results of a review of the medical literature
to evaluate the effects of CPOE on adverse drug
events showed that:
a. CPOE with clinical decision support
contributed a statistically significant
decrease in adverse drug events (ADEs) in
50% of the studies.
b. Three studies reported a nonstatistically
significant reduction in ADE rates.
c. Four studies demonstrated no change in
ADE rates.
d. No study met the inclusion criteria of
computer system, drug categories, types of
ADEs, and clinical outcomes.
7.The American Recovery and Reinvestment Act,
which was signed into law in 2009, authorizes:
a. $10 billion designated to implement health
information technology (HIT) regional health
information exchange networks
b. As much as $6,750 over 6 years for eligible
pharmacists
c. $27 billion over 10 years designated in
Medicare and Medicaid incentive payments
for eligible providers who use EHRs and
demonstrate “meaningful use” of HIT
d. As much as $144,000 for eligible
physicians over a 5-year period through
Medicare
8.In February 2012, federal officials released the
stage 2 guidelines for meaningful use including:
a. Requiring physicians and hospitals to
significantly increase their use of electronic
health information
b. Meaningful usage requiring that at
least 80% of patients must have their
medications and laboratory tests ordered
electronically
c. Requirements for stage 2 meaningful use to
be in place immediately
d. Pharmacy HIT systems become
interoperable by 2014
9.The nation’s goal for EHRs is to reduce costs
through less paperwork, improved safety,
and reduced duplication of testing, and to
improve health by gathering a patient’s entire
health information in a single location. EHRs
accomplish this by:
a.Being “an electronic record of health-related
information on an individual that is created,
gathered, managed, and consulted by
authorized healthcare clinicians and staff.”
b.Being “an electronic record of individually
identifiable health information on an
individual that can be drawn from multiple
sources and that is managed, shared, and
controlled by and for the individual.”
c. Restricting data from certain defined sources
and health and medical entities.
d. Being generated by physicians, patients,
hospitals, pharmacies, and other sources
but initiated and managed by the patient.
10.In more than 100 interviews with physician
practices and pharmacies nationwide this past
year, researchers at the Center for Studying
Health System Change noted flaws and
inconsistencies concentrated in 3 critical areas
in e-prescriptions. These include:
a. New prescriptions
b. Volume of electronic prescriptions
c. Connectivity between physician offices and
mail-order pharmacies
d. Computerized entry of prescription
information by pharmacists
April 2012
Drug topics
53
caSe StudieS
Continuing Education
case a
A primary care physician (PCP) electronically prescribes 5 medications for a Medicare Part D patient post yearly physician visit.
Four of the medications were continued from the previous visit.
This patient qualifies for a yearly comprehensive medication review (CMR) as defined by the Part D plan’s medication therapy
management (MTM) program.
The pharmacist receives the electronic prescriptions, and the
pharmacy management system (PMS) alerts the pharmacist that
the patient’s prescription drug plan will authorize a CMR using the
National Council for Prescription Drug Programs (NCPDP) standardized transaction (an electronic transaction for a payer to request
MTM services from a provider). Mail and fax are other ways to
receive a CMR request. Under the Part D plan’s business agreement, the clinical pharmacist in charge of the pharmacy’s MTM
service programs messages the patient and the PCP that a CMR
is needed. The PMS adopted a pharmacist electronic health record
(EHR) functionality, and the PMS is certified for the meaningful use
of the EHR criteria.
Using the pharmacy’s e-prescribing network, the PMS queries the PCP’s EHR, the patient’s personal health record (PHR),
and the state health information exchange (HIE) for the patient’s
continuity-of-care documents (CCD), which contain allergies, chief
complaints, active medications list, diagnosis, family history, immunizations, functional status, social history, vital signs, laboratory
data, etc. The patient schedules a CMR with the clinical pharmacist. The result of the CMR is electronically exchanged with the
PCP’s EHR and the medication action plan is electronically sent
to the patient’s PHR.
1.
Which of the following statements is correct?
a. Only e-prescribing networks can electronically connect with PMS.
b. PMS can connect with e-prescribing networks and HIEs.
c. Pharmacists are not allowed to access patient information through an
HIE.
d. Only physicians can access patient information through an HIE.
2.
How is a request for a CMR transmitted?
a.
b.
c.
d.
3.
Electronically using an NCPDP standardized transaction
Fax
Mail
All of the above
electronic prescription for a Schedule C-II controlled substance
was transmitted to the patient’s local pharmacy using an eprescribing network. Using the pharmacist EHR, which does
not have to be confined to the four walls of a pharmacy, the
clinical pharmacist electronically queried the patient’s hospital
discharge summary and electronically coordinated a pain medication action plan with the PCP and the home healthcare nurse.
1.
a. Controlled substance prescriptions cannot be sent via e-prescribing.
b. Only Schedule C-II medications can be sent via e-prescribing.
c. Pharmacies can receive electronic prescriptions for controlled substances from a hospital.
d. All of the above.
2. . In which of the following situations can a pharmacist query a hospital’s
EHR?
a.
b.
c.
d.
3.
c. All of the above
d. None of the above
54
Drug topics
April 2012
The medication action plan should be discussed with which of the following
individuals:
b. Patient
c. Nurse
d. All of the above
case c
An elderly patient asks her local chain pharmacy about getting
her flu shot. The pharmacist is not familiar with this patient and
notices that the patient displays symptoms of mild confusion.
Using the PMS’s EHR, the pharmacist queries the PCP’s EHR
and the public health department for the patient’s immunization
history, allergy information, and other pertinent information in
the form of a CCD. The query indicates that the patient has no
known allergies, received a flu vaccine last year, and a pneumococcal immunization the previous year. The pharmacist administers the flu vaccines and electronically transmits the new flu
vaccine information to the PCP and the public health department.
1.
If a pharmacist is unfamiliar with a patient’s vaccination history, the
following may be conducted:
a.
b.
c.
d.
2.
Patient should be asked about their vaccination history.
Using a CCD, a pharmacist can query a PCP’s EHR.
Allergy information is available in a CCD.
All of the above
Which of the following information can be found in the CCD?
a. Immunization history
b. Allergy information
case B
A patient in a car accident and post hospital surgery was
discharged home with a broken arm and leg. The patient’s
discharge summary in the form of a CCD, which contains allergies, chief complaints, active medications list, diagnosis,
family history, immunizations, functional status, social history,
vital signs, laboratory data including electronic x-ray images,
was electronically transmitted to the PCP and home healthcare agency coordinating the patient’s rehabilitation therapy. An
Pharmacist working in a community pharmacy
Pharmacist working in a chain pharmacy
Pharmacist not working within the four walls of a pharmacy
All of the above
a. PCP
A PMS can query which of the following:
a. PCP’s EHR
b. Personal health records
Which of the following statements is correct?
3.
c. Active medications list
d. All of the above
Which of the following statements is correct?
a. Pharmacists providing immunizations should only electronically transmit
flu vaccine information to the PCP.
b. The public health department should not be notified of patient immunization updates.
c. Pharmacists providing immunizations should provide vaccine information to the patient’s PCP and the public health department.
d. None of the above
DrugTopics .c om