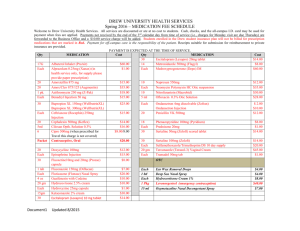
Empirical Antibiotic Management of Common Infections in Adults
advertisement

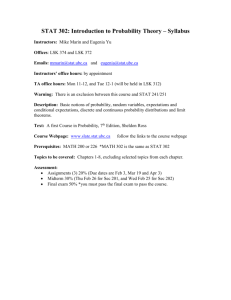
Empirical Antibiotic Management of Common Infections in Adults: Med Microbiologyx1970 (emergency blp6480). Pharmacy blp 7508. Out of hours Reg. aircall SG395, Pharm blp 6267 Infection 1 st line Antibiotics Alternative if allergic to 1 st line Oral switch Duration Community acquired pneumoni a (CAP) Record CURB-65 score and evidence of Chest X-Ray consolidation. (If clear, treat as LRTI) Confusion (new onset) ºAge >65yrs Urea>7mmol/l Respiratory rate>30/min BP<90mmHg (systolic) or <60 (diastolic) If severe send blood cultures, urine for antigen detection & sputum for v iral PCR Infecti ve Exacerbati on of COPD and LRTI No Chest X-Ray changes Send sputum Hos pital Acquired Pneumoni a (HAP) Occurring >5 days in hospital Record Chest X-ray evidence of consolidation Send sputum and BC if severe Aspiration Pneumonia Record Chest X-Ray ev idence of consolidation 48-72hrs following aspiration Send sputum and BC if severe Urinary Tract Infection Urine dipstick (send to micro for M C&S if positive) Always collect urine specimen before starting antibiotics Only treat positive CSU if features of urinary sepsis Change treatment according to microbiology results Intra-abdominal Sepsis Send BC if severe and sample of pus, where possible Cellulitis Wound swab if skin is broken Mark affected area Contact microbio logy if patient is shocked and for necrotic skin infect ions Osteomyelitis/ Septic Arthritis in nati ve joints (contact microbi olog y if prosthesis) Refer patient to OPAT if fit fo r discharge on IV ab x Clostri dium di fficile Infecti on – unknown source (no sepsis) Order chest x-ray, Urine dipstick – M C&S and BC Suspected Sepsis – site and organism unknown Clin ical symptoms of infection (sweats, chills, malaise, rigors etc) plus 2 or more o f the following: Temp >38° or <36°, HR >90bpm, RR >20/ min WCC <4 or >12 Order Chest X-ray, send blood and urine cultures Meningitis (Start antibiotics immediately) Take blood cultures plus blood in EDTA fo r mo lecular studies and a throat swab. Seek advice on need for a CT scan, timing of LP and need for dexamethasone. LOW S EVERITY (CURB-65 score 0-1) Amo xicillin PO 500mg – 1g 8-hrly Do xycycline PO 200mg STAT then 100mg OD MODERATE-S EVERE (CURB-65 score 2-5) Seek microbiology advice Amo xycillin 500mg –1g, 8-hrly Benzy l Pen icillin IV 1.2g, 4-hrly + +/- Do xycycline PO 200mg STAT Do xycycline PO 200mg STAT then 100-200mg then 100mg OD OD (use Clarithro mycin IV 500mg , 12-hrly if unable to take oral) Patients with moderate CAP (CURB=2) may be suitable for a more rapid IV to oral switch Do xycycline PO 200mg STAT then Amo xycillin PO 500mg – 1g 8-hrly OR Do xycycline PO 200mg STAT 100mg OD (or A mo xicillin IV 1g 8-h rly if severe Clarithromycin PO 500mg 12-hrly then or unable to take orally) 100mg OD Do xycycline PO 200mg STAT then 100mg OD Seek microbiology advice Do xycycline PO 200mg STAT OR (if severe or unable to take oral) then Benzy l Pen icillin IV 1.2g, 4-hrly + Gentamicin IV 100mg OD OD as per dosing guidelines Do xycycline PO 200mg STAT then Seek microbiology advice Do xycycline PO 200mg STAT 100mg OD +Metronidazole PO 400mg, 8-hrly OR then (if severe or unable to take oral) Ben zyl Penicillin 100mg OD IV 1.2g, 4-h rly + Metronidazole IV 500mg, 8-hrly +Metronidazole PO 400mg, 8-hrly Uncomplicated UTI Nitro furantoin PO 50-100mg , 6-hrly Trimethoprim PO 200mg , 12-hrly (only if CrCl>20ml/ min) Complicated UTI (structural abnormality or Ciproflo xacin PO 500mg 12h rly + Co-amo xiclav 625mg, 8-hrly OR post-urological surgery) & Pyelonephritis Gentamicin IV 5mg/kg STAT if shocked Ciproflo xacin PO 500mg 12h rly Co-amo xiclav IV 1.2g, 8-hrly + (Check results of urine M C&S) Gentamicin IV 5mg/kg STAT if shocked Catheter-associated UTI: Treat only if sympto matic (The presence of organisms in the urine does not imply infection) If sympto matic – send CSU and give a singledose of Gentamicin IV and rev iew with CSU results Amo xicillin IV 1g, 8-hrly + Gentamicin IV OD as Seek microbiology advice Co-amo xiclavPO 625mg, 8-hrly per dosing guidelines + Metronidazole IV 500mg, 8-hrly NON S EVERE Clarithromycin PO 500mg, 12-hrly Fluclo xacillin PO 500mg, 6-hrly Clindamycin IV/PO 600mg 6hrly : SEVERE Fluclo xacillin 500mg –1g, 6-h rly Clindamycin has excellent oral Fluclo xacillin IV 2g, 6-hrly OR Clindamycin 450-600mg 6bioavailability so early switch is hrly recommended Fluclo xacillin IV 2g, 6-hrly Vancomycin IV as per dosing guidelines Fluclo xacillin 500mg -1g, 6-hrly Seek microbiology advice if Penicillin allergic Refer to full gui delines Do xycycline PO 200mg STAT then Review urine culture and CXR Amo xicillin IV/PO 1g 8hrly + Gentamicin IV 100mg OD + Gentamicin IV STAT treat as per specific guidelines STAT 5 – 7 days 7-10 days in total IV + PO (review needed for doxycycline on oral switch) 5 – 7 days 5-7 days in total IV + PO 5-7days in total IV + PO Women – 3 days Men – 7 days Co mplicated UTI 7 – 10 days Pyelonephritis 10-14 days Review IV after 48 hrs 7 days Review IV after 5-7 days depending on response Usually 2 weeks IV then 4 weeks PO (seek microadvice) 3-5 days Co-amo xiclav PO 625mg or IV 1.2g, 8-hrly + Gentamicin IV 5mg/kg STAT Antibiotics should be administered within an hour Seek microbiology advice Review after 24hrs Ceftriaxone IV 4g OD + Aciclovir IV 10mg/ kg 8hrly if viral encephalitis suspected + A mo xicillin IV 2g 4hrly if immunocompro mised or >55 years to cover for listeria. Seek microbiology advice Dependent on culture results (seek micro or CIU advice)