Health Care Financing over the Life-Cycle, Universal
advertisement

Health Care Financing over the Life-Cycle,
Universal Medical Vouchers and Welfare
Juergen Jung
Towson University, Maryland
Chung Tran
University of New South Wales
Baltimore - May 2010
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
1 / 39
Introduction
Main problems of the U.S. health insurance system
1
Health insurance coverage is low
47 million are uninsured in 2006 (15%)
2
Health expenditure is high
16% of GDP in 2006
close to 20% by 2015
3
Questionable health outcomes?
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
2 / 39
Introduction
Analyzing comprehensive health care reform
Medicare Prescription Drug, Improvement, and Modernization Act
(2003)
Health Savings Accounts
Medicare Part D (2006) for prescription drugs
Stop imports of generic drugs
Restrict Medicare's ability to negotiate drug prices
Patient Protection and Aordable Care Act (2010)
Health insurance exchanges plus mandate
Restrictions on insurance companies
Expansion of Medicaid
Cuts in Medicare
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
3 / 39
Introduction
Health insurance and expenditure proles (2004/05)
911
71
51
31
01
101
61
51
41
31
21
01
91
101
#$
21
#
21
31
41
51
61
!"
31
41
71
81
51
61
71
81
%&
'()
*+,-./01223412256
78*(9)
76
*
:;<9)
&
=76
*>*
7?
6
>&
@:
()
7@A
*7@B>*7?
6
>:
9*
@B&
@'7:9*
)
A
;<>;
(:
*
>;?
B&
@A
;
C*
;=*)6
>*?
&
<
*D
A
EA?
*
F
Jung
and
Tran
(TU
and
UNSW)
Life Cycle Health
2010
4 / 39
Introduction
Objectives and main contributions
1
Develop a modelling framework to analyze comprehensive health care
reform:
Stochastic dynamic general equilibrium life-cycle
1
2
endogenous health expenditures and
insurance choice to
model
with
account for the life-cycle patterns of
1
2
2
health expenditures and
insurance take-up rates observed in the data
Demonstrate the usefulness of the model by
quantifying the short-run and long-run eects of a comprehensive
reform with universal medical vouchers
incl. transitions and welfare analysis
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
5 / 39
Introduction
Related literature
1
2
3
4
5
Health expenditure over the life cycle
Grossman (1972a,1972b), Grossman (2000)
Consumption over the life cycle
Deaton (1992), Gourinchas and Parker (2002)
Fernandez-Villaverde and Krueger(2006,2009)
Health expenditure shocks, health insurance and precautionary savings
Kotliko (1986), Hubbard, Skinner and Zeldes (1995)
Palumbo (1999) and DeNardi, French and Jones (2006)
Quantitative macromodels with exogeneous health expenditure shocks
Attanasio, Kitao and Violante (2008), Jeske and Kitao (2009)
Macromodels with endogenous health expenditures and insurance
Suen (2006), Jung and Tran (2008) and Feng (2009)
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
6 / 39
Introduction
Outline
1
Model
2
Calibration
3
Policy experiments
4
Conclusion
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
7 / 39
The Model
MODEL
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
8 / 39
The Model
The Model: Key Features
1
An overlapping generations model with heterogenous agents
Sectors: household, rm and government
Markets: consumption, labor and capital
Agents live for multiple-periods as workers and retirees, and face period
mortality shocks and labor productivity shocks
Incomplete nancial markets
2
New features from the Grossman literature
Health as a durable good: consumption and investment
Health depreciation and health shocks
Endogenous demand for health care and health insurance
Mix of private and public health insurance
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
9 / 39
The Model
Preferences and technology
Preferences:
u (cj , sj )
Health capital:
service ow from health capital
health production
health shocks
sj = s ( h j )
(1)
hj = h (mj , hj −1 , εj )
(2)
pj (εj , εj −1 )
=
Pr (εj |εj −1 , j )
Human capital:
accumulation
ej = e (hj −1 , j )
for j = {1, ..., J1 }
productivity shocks
πj (j , j −1 )
Jung and Tran (TU and UNSW)
= Pr (j |j −1 , j )
Life Cycle Health
2010
10 / 39
The Model
Health insurance arrangements
A private health insurance market for workers
Two insurance plans: individual and group
Group insurance oers provided by employers with a probability
ωGI (iGI ,j , iGI ,j −1 )
=
Pr (iGI ,j |iGI ,j −1 , income )
Health insurance choice: endogenous
inj = 0 : no insurance
inj = 1 : individual based insurance
inj = 2 : group based insurance (if oered via employer)
A public insurance program for retirees (Medicare): no insurance
choice
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
11 / 39
The Model
Health expenditures and nancing
The total health expenditure: pm m
Worker's out of pocket health expenditures:
o W (mj ) =
pm,noIns m
min [pm,Ins mj , γ + ρ (pm,Ins mj − γ)]
if inj = 0,
if inj = 1, 2
Retiree's out of pocket health expenditures:
o R (mj ) = min pm,Med mj , γ Med + ρMed pm,Med mj − γ Med
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
12 / 39
The Model
Households
Household problem: Timing of events
ũ
ũнϭ
+ a’: asset
+ h’: health capital
+ in’: insurance
+ a: asset
+ h: health capital
+ in: insurance
Shocks:
+ : health
+ : productivity
+ : group insurance
x(j) = {a, h, in , , ,
}
Choices:
+ c: consumption
+ m: medical services
+ a’: savings
+ in’: insurance
choice = {c, m, a’, in’}
x(j+1) = {a’, h’, in’, ’, ’,
’}
Jung and Tran (TU and UNSW)
Shocks:
+ ’: health
+ ’: productivity
+ ’: group insurance
Life Cycle Health
2010
13 / 39
The Model
Households
Worker's dynamic optimization problem
V j ( xj ) =
max
n
{cj ,mj , aj +1 ,inj +1 }
o
u (cj , sj ) + βπj Eεj +1 ,j +1 ,iGI ,j +1 |εj ,j ,iGI ,j [V (xj +1 )]
s.t.
(1), (2) , 0 ≤ aj +1 , and
1 + τ C cj + (1 + g ) aj +1 + o W (mj ) + 1{inj +1 =1} p (j , h) + 1{inj +1 =2} p
=
we (hj −1 , j ) + R aj + T Beq + Insprot1 + Insprot2 − Taxj + TjSI
where
Taxj
ỹjW
=
=
τ̃ ỹjW + τ Soc + τ Med
we hj −1 , j − 1{in
j +1 =2}
=
we hj −1 , j + raj + rT Beq + Insprot1 + Insprot2
− τ Soc + τ Med we hj −1 , j − 1
{in
j +1 =2}
TjSI
p
p − 1{inj +1 =2} p
max 0, c + Taxj − we hj −1 , j − R aj + T Beq − InsP1 − InsP2
h
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
i
14 / 39
The Model
Households
Retiree's dynamic optimization problem
V j ( xj ) =
max
{cj ,mj , aj +1 }
n
o
u (cj , sj ) + βπj Eεj +1 |εj [Vj +1 (xj +1 )]
s.t.
(1), (2) , 0 ≤ aj +1 , and
cj + (1 + g ) aj +1 + o R (mj ) + pjMed
Jung and Tran (TU and UNSW)
=
R aj + T Beq + TjSoc + TjSI − Taxj
Life Cycle Health
2010
15 / 39
The Model
Firms and Insurance
Firms and insurance companies
Firms:
max {F (K , L) − qK − wL} , given (q , w )
{K ,L}
Insurance companies:
(1 + ωins )
=
J1
X
µ
Z h
i
1{inj (xj )=1,2} (1 − ρ) max (0, pm,Ins mj (xj ) − γ) d Λ (xj )
j =2 j
Z J1
X
(1 + r )
µ
1{inj (xj )=1,2} p (j , h) d Λ (xj )
j =1 j
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
16 / 39
The Model
Government
Government I
Bequests:
XJ
j =1
Z
µj
TjBeq (x ) d Λj
(x ) =
XJ
j =1
Z
µ̃j
aj (x ) d Λj (x )
Social Security:
XJ
Z
TjSoc (x ) d Λj (x )
j =J1 +1
Z
XJ 1
=
µj τ Soc we (j , hj , ) − 1{inj +1 =2} p d Λj (x )
j =1
Jung and Tran (TU and UNSW)
µj
Life Cycle Health
2010
17 / 39
The Model
Government
Government II
Medicare:
XJ
µj
Z
1 − ρMed max 0, mj (x ) − γ Med d Λj (x )
j =J1 +1
Z
XJ 1
=
µj τ Med we (j , hj , ) − 1{inj +1 =2} p d Λj (x )
j =1
Z
XJ
+
µ
pjMed d Λj (x )
j =J1 +1 j
General government budget:
G+
=
J
X
j =1
XJ
j =1
Z
µj
Z
µj
Jung and Tran (TU and UNSW)
TjSI (xj ) d Λ (xj )
Taxj (xj ) d Λ (xj ) +
Life Cycle Health
XJ
j =1
Z
µj
τ C c (xj ) d Λ (xj ) .
2010
18 / 39
The Model
Government
A competitive equilibrium
Given the transition probability matrices and the exogeneous government
policies, a competitive equilibrium is a collection of sequences of
distributions of household decisions, aggregate capital stocks of physical
and human capital, and market prices such that
Agents solve the consumer problem
The F.O.Cs of rms hold
The budget constraints of insurances companies hold
All markets clear
All the government programs and the general budget clear
The distribution is stationary
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
19 / 39
Calibration
CALIBRATION
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
20 / 39
Calibration
Calibration
Preferences:
u (cj , sj ) =
Health services:
cjη sj1−η
1−σ
1−σ
sj = hj
Health production:
hj = φmjξ + 1 − δh,j hj −1 + εj
Human capital:
ej = e (j )χ (hjθ−1 )1−χ for j = {1, ..., J1 }
Markov switching probabilities of the productivity shocks and group
insurance oer states are estimated from MEPS 2004-2005 data.
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
21 / 39
Calibration
Calibration
Baseline Parameters
Demographics:
J1 = 9
J2 = 5
n = 1.2%
Health Production:
φ=1
ξ = 0.32
Preferences:
σ = 2.5
Health Productivity:
θ = 0 , χ = 0.9
Insurance:
γ = 1.7% of median income
ρ = 34%
γ Med = 6% of elderly's aver health spending
ρMed = 30%
Exogenous premium growth
depending on age and health
β =?
Technology:
α = 0.36
δ = 15%
g = 1.5%
Depreciation rates of health capital δh,j =?
Magnitudes and transition probabilities of health shocks εj =?
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
22 / 39
Calibration
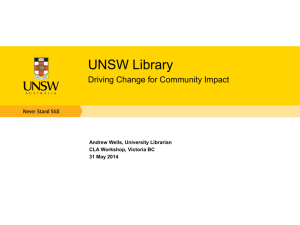
The model and the data
[1] Insurance Coverage in %
100
50
Model
Data
0
20
30
40
50
60
Age
[2] Medical Spending in % of Income
70
80
90
40
50
60
Age
[3] Average Assets
70
80
90
80
60
Model
Data
40
20
0
20
30
1
0.5
Model
Data
0
20
30
40
50
60
70
80
90
Age
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
23 / 39
Policy Experiments
POLICY EXPERIMENTS
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
24 / 39
Policy Experiments
A counterfactual health care reform: Universal Medical
Vouchers
Motivated by Kotliko (2007) and Emanuel and Fuchs (2007)
1
Government
issues medical vouchers to all individuals
Vouchers are calculated individually based on the amount of the
expected health expenditures for next year (experience rating system)
Vouchers are nanced by a consumption, payroll, or lump sum tax
2
3
Individuals purchase private health insurance contracts from insurance
companies using the voucher
Participating insurance companies have to accept vouchers and oer
basic insurance contracts
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
25 / 39
Policy Experiments
Steady State Resutls
Aggregate eects of the voucher program fnanced by a
payroll tax
Capital: K
Human capital: L
Output: Y
Med spending: pm ∗ M
Consumption: C
Consumption tax: τC
Payroll voucher tax: τV
Interest rate: R in %
Wages: w
Voucher Payments % of GDP
Benchmark
100.00
100.00
100.00
100.00
100.00
5.155
0.000
3.981
100.000
0.0
Regime 1 - Payroll tax
89.823
100.000
96.210
101.538
97.602
5.676
8.227
4.704
96.210
5.208
Table: Steady state result with health as consumption good only θ = 0.
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
26 / 39
Policy Experiments
Steady State Resutls
Negative eciency eects driven by:
1
Savings eect
2
Moral hazard eect
3
Tax eect
4
General equilibrium eect
1 + τ C cj + (1 + g ) aj +1 + o W (mj ) + p (xj )
1 − τ V we (hj −1 , j ) + R aj + T Beq − Taxj + TjSI + vj − τ LS
=
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
27 / 39
Policy Experiments
Steady State Resutls
Aggregate eciency eects: four key channels
Benchmark
100.00
Regime 1 - Payroll tax
89.823
2. Med spending: pm ∗ M
(The moral hazard eect)
100.00
101.538
3. Payroll voucher tax: τV
(The tax eect)
0.000
8.227
3.981
100.000
4.704
96.210
1. Capital: K
(The saving eect)
4a. Interest rate: R in %
4b. Wages: w
(The general equilibrium price eect)
Table: Steady state result with health as consumption good only θ = 0.
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
28 / 39
Policy Experiments
Steady State Resutls
Aggregate eects with consumption tax
Benchmark
100.00
Regime 2 - Cons Tax
98.293
2. Med spending: pm ∗ M
(The moral hazard eect)
100.00
107.858
3a. Consumption tax: τC
(The tax eect)
5.155
18.049
3b. Payroll voucher tax: τV
0.000
0.000
3.981
100.000
3.988
99.382
1. Capital: K
(The savings eect)
4a. Interest rate: R in %
4b. Wages: w
(The general equilibrium price eect)
Table: Steady state results with health as consumption good only θ = 0.
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
29 / 39
Policy Experiments
Steady State Resutls
Health as Consumption and Investment Goods
Additional channel: the human capital eect
Similar results as in the case without human capital eect
Higher health spending produces higher health
Higher health capital alleviates some of the negative tax distortions
Negative savings eect is now smaller
Price (G.E.) eects are smaller
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
30 / 39
Policy Experiments
Steady State Resutls
Health as consumption and investment good
1. Capital: K
(The saving eect)
2. Med spending: pm ∗ M
(The moral hazard eect)
3. Payroll voucher tax: τV
(The tax eect)
4a. Interest rate: R in %
4b. Wages: w
(The G.E price eect)
5. Human capital L
(The human capital eect)
Benchmark
θ=0
100.00
Payroll tax
θ=0
89.823
Benchmark
θ=1
100.00
Payroll tax
θ=1
90.902
100.00
101.538
100.00
101.077
0.000
8.227
0.000
8.224
3.981
100.000
4.704
96.210
4.251
100.000
4.919
96.555
100.000
100.000
100.000
100.199
Table: Steady state results with health productivity θ = 1.
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
31 / 39
Policy Experiments
Steady State Resutls
Health as consumption and investment good
Previous 4 channels
Additional channel: the human capital eect
Benchmark
100.000
Payroll tax
90.902
Consumption tax
100.078
Human capital: L
100.000
100.199
100.382
Output: Y
Medical spending: pm ∗ M
Consumption: C
Interest rate: R in %
Wages: w
Voucher Payments in % of GDP
100.000
100.000
100.000
4.251
100.000
0.000
96.747
101.077
98.346
4.919
96.555
5.227
100.273
107.454
96.548
4.121
99.891
5.673
Capital: K
Table: Steady state results with health productivity θ = 1.
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
32 / 39
Policy Experiments
Steady State Resutls
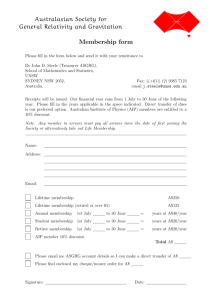
Transitions from benchmark to regime 1: payroll tax
Output
Capital
100
θ=0
θ=1
98
96
100
0
10
20
Time
Consumption
30
90
40
80
105
110
100
105
95
0
10
20
30
Time
Medical Expenditure
40
120
100
0
10
20
30
Time
Health Capital
40
0
10
20
30
Time
Human Capital
40
0
10
20
Time
Wages
30
40
0
10
20
Time
30
40
100.5
100
%
80
0
10
20
Time
Interest
30
40
100
5
100
4
98
3
0
10
Jung and Tran
20
30
Time
Consumption
Tax
(TU
and UNSW)
40
96
Life Cycle Health
2010
33 / 39
Policy Experiments
Welfare Analysis
Welfare eects: Payroll vs. consumption tax
Negative eciency eects
Capital drops
Output drops
Household income drops (w decrease)
Consumption of C drops
Positive insurance eects
More insured, improved risk sharing
Increases in medical spending
Increases in health capital H
If H is productive, it has a positive eect on output
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
34 / 39
Policy Experiments
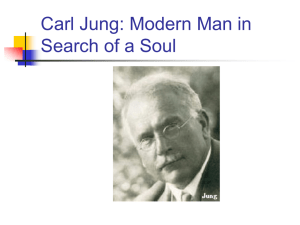
Welfare Analysis
Welfare eects: Payroll vs. consumption tax
Regime 1 (τ ): Compensating Consumption per GDP (in %)
L
6
4
Losses
%
2
0
Gains
−2
θ=0
θ=1
−4
−6
0
5
10
15
Time
20
25
30
Regime 1 (τ ): Compensating Consumption per GDP (in %)
C
6
4
Losses
%
2
0
Gains
−2
θ=0
θ=1
−4
−6
0
5
Jung and Tran (TU and UNSW)
10
15
Time
Life Cycle Health
20
25
30
2010
35 / 39
Policy Experiments
Welfare Analysis
Aggregate eects: Payroll vs. consumption tax
Benchmark
Capital: K
Human capital: L
Output: Y
Med spending: pm ∗ M
Consumption:
C
Consumption tax: τC
Payroll voucher tax: τV
Interest rate: R in %
Wages: w
Voucher Payments % of GDP
100.00
100.00
100.00
100.00
Regime 1
Payroll tax
89.823
100.000
96.210
101.538
Regime 2
Consumption Tax
98.293
100.000
99.382
107.858
100.000
97.602
96.227
5.155
0.000
3.981
100.000
0.0
5.676
8.227
4.704
96.210
5.208
18.049
0.000
3.988
99.382
5.583
Table: Steady state result with health as consumption good only θ = 0.
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
36 / 39
Policy Experiments
Welfare Analysis
Key Lessons
General equilibrium channels
Tax nancing instruments: Payroll vs. consumption tax
Role of health: Productive vs. non-productive health
Policy outcomes: Aggregate vs. welfare eects
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
37 / 39
Conclusion
Conclusion
1
2
3
Construct a heterogeneous agents macro-model with health as a
durable good
Account for life-cycle patterns of health expenditures and private
insurance take up rates
Assess the macroeconomic eects of introducing a universal health
insurance system
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
38 / 39
Conclusion
Future work on macro-health economics
1
Model:
Elastic labor and Medicaid
The life cycle proles with a pure age eect
A structural estimation of the health production function
2
Research Questions:
Life cycle consumption puzzle
The tax deductible policy and health insurance markets
The macroeconomic eects of Obama's health care reform 2010
Optimal public health insurance policy
Financing health costs in an aging economy
Jung and Tran (TU and UNSW)
Life Cycle Health
2010
39 / 39