- The Annals of Thoracic Surgery
advertisement

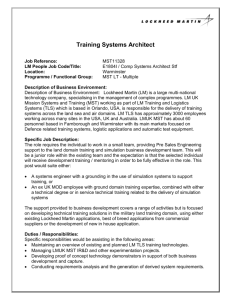
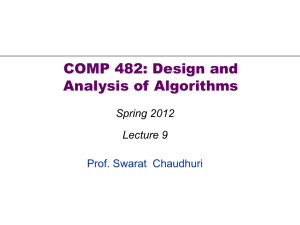
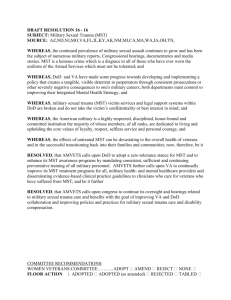
REVIEW A Meta-Analysis Comparing Muscle-Sparing and Posterolateral Thoracotomy Mohammed M. Uzzaman, MRCS, MS, J. Daniel Robb, FRCS, MRCP, Peter C. E. Mhandu, MRCS, MCChB, Habib Khan, MRCS, MBBS, Kamran Baig, FRCS, MD, Sanjay Chaubey, MRCS, and Donald C. Whitaker, FRCS, MD Department of Cardiothoracic Surgery, King’s College Hospital, London, United Kingdom We compared outcomes of posterolateral thoracotomy vs muscle-sparing thoracotomy after open thoracic operations. Twelve trials were included, comprising 571 patients in the muscle-sparing thoracotomy group and 512 patients in the posterolateral thoracotomy group. There was significantly improved shoulder internal rotation (weighted mean difference, –1.28; 95% confidence interval, –2.45 to –0.11; p [ 0.03) and pain scores on day 7 (weighted mean difference, –0.76; 95% confidence interval, –1.26 to –0.27; p [ 0.002) but higher seroma rates (odds ratio, 8.26; 95% confidence interval, 2.16 to 31.56; p [ 0.002) in the muscle-sparing thoracotomy group compared with the posterolateral thoracotomy group. We advocate using muscle-sparing thoracotomy, especially on patients dependant on quicker recovery of shoulder function. A Several trials have assessed MST compared with PLT after thoracic procedures [10–22]. A meta-analysis of these trials allows a pooled analysis, thereby minimizing any type II error. The purpose of this meta-analysis was to assess the clinical outcomes of MST compared with PLT after open thoracic procedures. Address correspondence to Dr Uzzaman, Department of Cardiothoracic Surgery, King’s College Hospital, Bessemer Rd, London SE59RS, UK; e-mail: mohsinuzzaman@yahoo.co.uk. Ó 2014 by The Society of Thoracic Surgeons Published by Elsevier Inc Material and Methods An electronic search was performed using the MEDLINE, CINAHL, DARE, ACP, LILACS, SCOPUS, Google Scholar, and EMBASE databases from 1966 to 2010. The search terms “Thoracotomy,” “Posterolateral,” “Muscle sparing,” “Minimal invasive,” “Thoracic,” “Limited,” “Standard,” “Randomised trial,” “Randomized trial,” “Trial,” “Prospective,” “Retrospective,” “Anterolateral,” “Axillary,” “Vertical,” and “Anterior,” and MeSH headings “Thoracotomy” (MeSH), “Thoracic” (MeSH) “Surgery” (MeSH) were used in combination with the Boolean operators “and” or “or.” The criteria were widened further by using the “related article” function during the search. Two authors conducted the electronic searches independently in March 2012. This search was supplemented by a hand search of published abstracts from 1980 to 2010 in meetings of the Society of Academic and Research Surgery, Surgical Research Society, Society of Cardiothoracic Surgeons (SCTS), World Congress of Cardiothoracic Surgery, The European Society of Cardiothoracic Surgeons, and The American Association of Thoracic Surgery (AATS). Finally, the Current Controlled Trials Register, The Cochrane Database Of Controlled Trials, and Science Citation Index Expanded were searched. The reference lists of all articles obtained were also examined to identify additional relevant studies. Review 0003-4975/$36.00 http://dx.doi.org/10.1016/j.athoracsur.2013.08.014 REVIEW posterolateral thoracotomy (PLT) in which muscles are divided is still the standard approach for most thoracic surgical procedures. It has the advantage of providing good access and can be easily and quickly extended if greater access becomes necessary. Although the choice of thoracotomy incision is guided primarily by the exposure required to perform a safe procedure, cosmesis and the potential for improved recovery should also be considered. PLT requires the division of the latissimus dorsi (LD) and sometimes other chest wall muscles such as trapezius, the rhomboids, and serratus anterior (SA). As a result, PLT may be associated with considerable morbidity, including postoperative pain, impaired lung function, and compromised function of the shoulder girdle [1–3]. In an attempt to decrease these shortcomings, less invasive thoracotomy procedures, such as muscle-sparing thoracotomy (MST) [4–9] and video-assisted thoracoscopic surgery (VATS), [10] have been introduced. Various types of MSTs have been proposed during the last 25 years, including vertical and transverse axillary thoracotomy [4, 5], auscultatory triangle thoracotomy [6], limited lateral thoracotomy [7], and muscle-sparing posterolateral thoracotomy [8]. By using a more limited muscle dissection than PLT, there is the potential for MST to reduce postoperative pain, allow better respiratory and lung function by preserving accessory muscles, and reduce postoperative complications. However, the difference in the postoperative outcomes between these techniques remains undetermined. (Ann Thorac Surg 2014;97:1093–102) Ó 2014 by The Society of Thoracic Surgeons 1094 REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES articles were obtained to determine other possible studies. Trials were included irrespective of the language in which they were published. We applied the guidelines for Meta-analysis of Observational Studies in Epidemiology (MOOSE) [23]. Ann Thorac Surg 2014;97:1093–102 the Cochran Q value and quantified using the I2 inconsistency test. In this study, we did not perform metaregression or sensitivity analysis because of the small number of studies included. All p values were 2-sided, and a 5% level was considered significant. Study Eligibility REVIEW Eligibility for study inclusion into the meta-analysis and study quality assessment was performed independently by 2 of the authors (M.U. and P.M.). Study data were extracted onto standard forms. Any disagreements were resolved by the third author (D.R.). Studies were included if they were trials in which direct comparisons were made between patients who had PTL vs MST during a thoracic surgical procedure. A posterolateral thoracotomy procedure must involve division of the latissimus dorsi muscle. An MST approach does not allow division of the latissimus dorsi muscle but can allow division of other muscles such as SA or trapezius. Any unclear or missing information was obtained by contacting the authors of the individual trials. For duplicate publications, the smaller data set was excluded. Any data directly comparing a VAT approach vs thoracotomy techniques were excluded from the analysis. The quality of each study was assessed by use of Newcastle-Ottawa scale, a 9-point scale that assigns points on the basis of the process of selection (0 to 4 points), comparability (0 to 2 points), and identification of the outcomes of study participants (0 to 3 points) [24]. The primary outcome measures were lung function tests measured by forced expiratory volume in 1 second (FEV1) and vital capacity (VC), range of shoulder movement (in degrees) at 30 days, and pain score on a linear visual analog scale at 1, 7, and 30 days after the operation. Secondary outcomes were duration of operation (in minutes), incision size (in cm), hospital stay (in days), and overall documented complication rates, including seroma. The duration of operation was defined as the time taken to perform the procedure starting from knifeto-skin through completion of skin closure. Only trials that reported at least one of the primary or secondary outcome measures were included in the meta-analysis. Statistical Analysis Data from the individual eligible studies were entered into a spreadsheet for further analysis. StatsDirect 2.5.7 software (StatsDirect, Altrincham, UK) was used to perform the statistical analysis. Weighted mean differences (WMD) were calculated for the effect size of continuous variables such as duration of surgery and postoperative visual analog scale pain scores. Pooled odds ratios (OR) were calculated for discrete variables such as complication and seroma rate. A positive WMD and an OR of less than 1.00 favors PLT, whereas a negative WMD or an OR of less than 1.00 favors MST. Random effects models (DerSimion Laird) were used to calculate the outcomes of binary and continuous data to control any heterogeneity among the studies. Heterogeneity among the trials was determined by means of Results The initial search identified 58 publications (Fig 1). The meta-analysis included 13 publications describing 12 trials that fulfilled the inclusion criteria [10–22]. Publication dates ranged from 1991 to 2010. There were 1,083 patients, of whom 512 had PLT and 571 had MST. There were no baseline imbalances in age, sex, or body mass index between the two groups. Trial details are reported in Table 1 and Table 2, including details of study design, sample size, intervention, and follow-up. Primary Outcome LUNG FUNCTION TESTS. Six studies reported the percentage change in FEV1 after 30 days [10, 12, 14, 16, 18, 21]. There was no statistical heterogeneity between studies (Cochran Q ¼ 3.13, p ¼ 0.68; I2 ¼ 0%, 95% confidence interval [CI], 0% to 61%). In the random effects model, there was no significant difference in the FEV1 compared with preoperative levels between the PLT and MST group (pooled WMD, 2.74; 95% CI, –0.92 to 6.41; p ¼ 0.14; Table 3). Five studies reported the percentage change in VC after 30 days [12, 14, 15, 18, 21]. There was statistical heterogeneity between studies (Cochran Q ¼ 11.39, p ¼ 0.02; I2 ¼ 64.9%, 95% CI, 0% to 84.5%). In the random effects model, there was no significant difference in the VC compared with preoperative levels between the PLT and MST group (pooled WMD, 3.10; 95% CI, –3.05 to 9.24; p ¼ 0.32; Table 3). SHOULDER MOVEMENTS. Three studies reported the range of shoulder movement after 30 days [12, 18, 21]. For shoulder abduction, there was no statistical heterogeneity between studies (Cochran Q ¼ 0.40, p ¼ 0.82; I2 ¼ 0%, 95% CI, 0% to 72.9%). In the random effects model, there was no significant difference in shoulder abduction between the PLT and MST group at 30 days (pooled WMD, 2.33; 95% CI, –0.69 to 5.35; p ¼ 0.13; Table 3). For shoulder flexion, there was statistical heterogeneity between studies (Cochran Q ¼ 11.95, p ¼ 0.002; I2 ¼ 83.3%, 95% CI, 2.8% to 92.7%). In the random effects model, there was no significant difference in shoulder flexion between the PLT and MST group at 30 days (pooled WMD, 8.18; 95% CI, –1.65 to 18.01; p ¼ 0.10; Table 3). For internal rotation, there was no statistical heterogeneity between studies (Cochran Q ¼ 2.24, p ¼ 0.32; I2 ¼ 10.9%, 95% CI, 0% to 75.7%). In the random effects model, postoperative internal rotation was significantly better at 30 days in the MST group than in the PLT group (pooled WMD, –1.28; 95% CI, –2.45 to –0.11; p ¼ 0.03; Fig 2 and Table 3). For external rotation of the shoulder, there was statistical heterogeneity between studies (Cochran Q ¼ 14.22, REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES 1095 Fig 1. Quality of reporting of meta-analyses diagram for the study. (RCT ¼ randomized controlled trial; VATS ¼ video-assisted thoracoscopic surgery.) p ¼ 0.00; I2 ¼ 85.9%, 95% CI, 34% to 93.6%). In the random effects model, there was no significant difference in postoperative external rotation between the PLT and MST group (pooled WMD, –3.01; 95% CI, –8.57 to 2.55; p ¼ 0.29; Table 3). PAIN SCORES. Six studies reported the pain scores on day 1 after the procedure [10, 14, 15, 18, 21, 22]. There was statistical heterogeneity between studies (Cochran Q ¼ 77.55, p ¼ 0.00; I2 ¼ 93.6%, 95% CI, 89.3% to 95.6%). In the random effects model, there was no significant Table 1. General Characteristics of Included Trials Study Year Nosotti [10] Endoh [11] 2010 2010 Athanassiadi [12] Ochroch [13] Akcali [14] Nomori [15] Benedetti [17] Sugi [18] Landreneau [19] Ponn [20] Hazelrigg [21] Lemmer [22] 2007 2005 2003 1999 1998 1996 1996 1991 1991 1990 NS ¼ not specified; Trial Surgeon Study Period Follow-Up Single RCT Retrospective Single surgeon Various surgeons Jul 2003–2006 Oct 2001–Mar 2007 Single-center RCT Single-center RCT Single-center RCT Prospective Prospective Single-center RCT Retrospective Prospective Single-center RCT Single-center RCT 2 surgeons 3 surgeons NS 2 surgeons NS Single surgeon Various surgeons Various surgeons NS NS Jun 2004–Dec 2004 Mar 1998–Jul 1999 1999–2000 Jan 1993–Dec 1997 NS NS NS (40 months) NS NS NS 3 years Hospital stay (minimum 7 days) 60 days 48 weeks 1 month 6 months 1 month 30 days 1 year 6.4 2.8 months 1 month 24 hours RCT ¼ randomized controlled trial. Newcastle-Ottawa Score 8 6 8 7 7 6 5 5 5 5 7 5 REVIEW Ann Thorac Surg 2014;97:1093–102 REVIEW 1096 Sample Size, No. Study Selection Criteria Inclusion Exclusion Intervention Experimental Control PLT MST Nosotti [10] 100 50 50 Stage I/II non-small cell lung cancer Pneumonectomy, chest wall extension, epidural Standard way 12-15 cm incision; auscultatory triangle; no muscle division Endoh [11] 73 26 47 Lung cancer Prolonged pulmonary leakage, unable to perform tests due to complications 15-cm incision; division of LD and rib Athanassiadi [12] 100 50 50 Primary elective lung operation LD and lower edge of SA divided Ochroch [13] 120 82 38 Segmentectomy, lobectomy, bilobectomy Akcali [14] 60 30 30 Various thoracic diseases Thoracic trauma, thoracic surgery, pneumonectomies, chest wall or brachial plexus involvement, atypical resections Pneumonectomy, chronic pain, opioid use, neurologic impairment, CCS III/IV, severe pulmonary disease, unable to have epidural Not stated 8-13 cm incision; ALT, AAT and vertical approach; division or partial resection anterior SA SA was freed to inferior aspects (anterior border 6th rib) Nomori [15, 16] 84 56 28 Lung cancer Benign operation 30-35 cm incision, Lower trapezius and entire LD and SA divided Benedetti [17] 24 13 11 Segmentectomy Previous thoracotomy Division of LD þ/– SA/ trapezius Incision width of LD; LD divided þ/– resection posterior 6th rib. SA spared. 7-cm incision anterior to LD, LD spared; insertion of SA on 4th and 5th rib dissected Division of entire LD and lower edge of SA LD and SA both freed and retracted posteriorly/ anteriorly respectively (1) 12-cm ALT incision, dividing pectoralis major and splitting SA. (2) 20- to 25-cm AAT incision, dividing SA and pectoralis major Incision along auscultatory triangle, muscle spared Post-op Analgesia/ Care Patient controlled analgesia for 72 hours, ketorolac then paracetamol and codeine as required. No drains Epidural catheter 30-mg subcutaneous opioids for 48 hours, then oral paracetamol or codeine. 2 chest drains Epidural for 3-5 days, as required ketorolac; beyond this, oral ibuprofen, codeine and acetaminophen Intercostal nerve block, IV/IM pethidine for 24 hours. 2 soft drains in the subcutaneous layer Epidural analgesia for 8 days; indomethacin suppository as required Not stated (Continued) Ann Thorac Surg 2014;97:1093–102 Total REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES Table 2. Specific Characteristics of Included Trials Sample Size, No. Study Selection Criteria Experimental Control 30 15 15 Stage 1/2 lung cancer Benign cases Division of entire LD and lower edge of SA 335 148 187 Pneumonectomy, chest wall resection Lobectomy for stage I lung cancer Division of entire LD and lower edge of SA Ponn [20] 79 62 17 Segmentectomy, lobectomy, pneumonectomy Concomitant chest wall resection, diaphragmatic, or other radical resections; initially wedge resections of small peripheral lesions LD and anterior border of SA/trapezius divided Hazelrigg [21] 50 26 24 Various thoracic disease requiring thoracotomy Previous thoracotomy, vascular procedures, thoracotomy in lower intercostal space Division of entire LD and lower edge of SA Lemmer [22] 28 13 15 ASA 1 or 2, elective wedge, lobectomy or mediastinal resection Pneumonectomy; ASA > 2 Division of trapezius, LD and SA Landreneau [19] Exclusion PLT MST Both LD and SA were freed and retracted posteriorly and anteriorly, respectively (1) Axillary approach: anterior slips of SA 3rd/4th rib divided (2) lateral approach 10- to 12-cm sparing all muscles (1) Axillary approach: SA divided in line with fibers. (2) Limited lateral; LD and SA both freed and retracted. Occasionally, serratus insertions freed from ribs LD and SA both freed and retracted posteriorly/ anteriorly respectively Both LD and SA were freed and retracted; partial division of SA if needed Post-op Analgesia/ Care Rectal diclofenac as required. 2 soft drains in the subcutaneous layer Intercostal nerve block, epidural catheter for 4 days; after, patientcontrolled analgesia and oral medications. 28F chest drain and Jackson-Pratt drain in subcutaneous flaps. Epidural catheter for 1-4 days. Jackson-Pratt drain to evacuate subcutaneous flap Single intercostal nerve block (Marcaine) above and below intercostal space. Jackson-Pratt drain for at least 4 days Morphine in 2-mg increments for 24 hours þ/– ¼ with or without; AAT ¼ anteroaxillary thoracotomy; ALT ¼ anterior limited thoracotomy; ASA ¼ American Society of Anesthesiologists; CSS ¼ Charlson Comorbidity Score; intramuscular; IV ¼ intravenous; LD ¼ latissimus dorsi; MST ¼ muscle-sparing thoracotomy; PLT ¼ posterolateral thoracotomy; SA ¼ serratus anterior. IM ¼ REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES Total Sugi [18] Inclusion Intervention Ann Thorac Surg 2014;97:1093–102 Table 2. Continued 1097 REVIEW 1098 REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES Ann Thorac Surg 2014;97:1093–102 Table 3. Summary of Results of Meta-Analysis for Individual Primary and Secondary Outcomes Variable Primary outcome FEV1 % (30 days) VC % (30 days) Abduction Flexion Internal rotation External rotation Pain day 1 Pain day 7 Pain day 30 Secondary outcomes Incision size Duration of operation Hospital stay Total complication Seroma CI ¼ confidence interval; posterolateral thoracotomy; Patients, No. Included Studies [Ref] PLT MST WMD Pooled OR (95% CI) p Value 6 5 3 3 3 3 6 4 4 194 147 89 89 89 89 162 117 126 196 177 91 91 91 91 190 147 128 þ2.74 þ3.10 þ2.33 þ8.18 –1.28 –3.01 –0.65 –0.76 –0.49 . (–0.92 to þ6.41) . (–3.05 to þ9.24) . (–0.69 to þ5.35) . (1.65 to þ18.01) . (–2.45 to –0.11) . (–8.57 to þ2.55) . (–1.51 to þ0.21) . (–1.26 to –0.27) . (–1.08 to þ0.10) 0.14 0.32 0.13 0.10 0.03 0.29 0.14 <0.01 0.10 2 9 61 460 63 470 –2.91 –3.67 . (–7.19 to þ1.36) . (–16.19 to þ8.85) 0.18 0.57 6 9 9 331 416 416 314 450 450 –1.02 . . . (–2.18 to þ0.15) þ0.94 (þ0.52 to þ1.71) þ8.26 (þ2.16 to þ31.56) 0.09 0.85 0.002 FEV1 ¼ forced expiratory volume in 1 second; MST ¼ muscle-sparing thoracotomy; WMD ¼ weighted mean difference; VC ¼ vital capacity. REVIEW difference in postoperative pain on day 1 between the PLT and MST group (pooled WMD, –0.65; 95% CI, –1.51 to 0.21; p ¼ 0.14; Table 3). Four studies reported the pain scores on day 7 after the procedure [10, 15, 18, 21]. There was statistical heterogeneity between studies (Cochran Q ¼ 9.16, p ¼ 0.03; I2 ¼ 67.3%, 95% CI, 0% to 86.6%). In the random effects model, postoperative pain scores were significantly lower on day 7 in the MST group than in the PLT group (pooled OR ¼ odds ratio; PLT ¼ WMD, –0.76; 95% CI, –1.26 to –0.27; p < 0.01; Fig 3 and Table 3). Four studies reported the pain scores on day 30 after the procedure [10, 12, 17, 18]. There was statistical heterogeneity between studies (Cochran Q ¼ 19.38, p < 0.01; I2 ¼ 84.5%, 95% CI, 48.3% to 92.2%). In the random effects model, there was no significant difference in postoperative pain scores on day 30 between the PLT and MST group (pooled WMD, –0.49; 95% CI, –1.08 to 0.10; p ¼ 0.10; Table 3). Secondary Outcome Fig 2. Forest plot for weighted mean difference for the effects on internal rotation between posterolateral thoracotomy (PLT) and muscle-sparing thoracotomy (MST) groups 30 days after the operation. The solid squares denote mean difference, the horizontal lines represent the 95% confidence intervals (CI), and the diamond denotes the weighted mean differences. (DL ¼ DerSimion Laird.) INCISION SIZE. Two trials reported the incision size [10, 17]. There was significant statistical heterogeneity between the two studies (Cochran Q ¼ 6.30, p ¼ 0.01; I2 ¼ *%, 95% CI ¼ *% to *%). In the random effect model, there was no significant difference in the incision size between PLT and MST group (WMD, –2.91, 95% CI, –7.19 to 1.36; p ¼ 0.18; Table 3). DURATION OF OPERATION. Nine trials reported on duration of the operation between the two groups [10–15, 18, 19, 22]. There was significant statistical heterogeneity between the nine studies (Cochran Q ¼ 76.91, p ¼ 0.00; I2 ¼ 89.6%, 95% CI, 82.7% to 92.9%). In the random effect model, duration of the operation did not differ significantly between the PLT and the MST group (WMD, –3.67, 95% CI, –16.19 to 8.85; p ¼ 0.57; Table 3). HOSPITAL STAY. Six trials reported the hospital duration of stay between the two groups [10, 11, 18–20, 22]. There was no significant statistical heterogeneity between the six studies (Cochran Q ¼ 9.77, p ¼ 0.08; I2 ¼ 48.8%, 95% CI, 0% to 77.9%). In the random effect model, the hospital duration of stay did not differ significantly between the Fig 3. Forest plot for weighted mean difference postoperative pain scores between posterolateral thoracotomy (PLT) and muscle-sparing thoracotomy (MST) groups on postoperative day 7. The solid squares denote mean difference, the horizontal lines represent the 95% confidence intervals (CI), and the diamond denotes the weighted mean differences. (DL ¼ DerSimion Laird.) PLT and the MST group (WMD, –1.02; 95% CI, –2.18 to 0.15; p ¼ 0.09; Table 3). TOTAL COMPLICATIONS. Nine trials reported total complications between the two groups [10, 12, 14, 15, 18–22]. These included bleeding, infection, atelectasis, arrhythmia, prolonged air leak, seroma and thromboembolic complications. There were 102 complications in the 571 patients (17.9%) in the MST group. On the other hand, there were 96 complications in the 512 patients (18.8%) in the PLT group. There was no statistical heterogeneity among the studies (Cochran Q ¼ 13.62, p ¼ 0.06; I2 ¼ 41.3%, 95% CI, 0% to 75.3%). In the random effect model, the total complications rate did not differ significantly between the PLT and the MST groups (pooled OR, 0.94; 95% CI, 0.52 to 1.71; p ¼ 0.85; Table 3). Pulmonary complications consisted of prolonged air leak in 24 patients in the PLT group vs 19 in the MST group, atelectasis in 13 patients in the PLT group vs 10 in the MST group, pneumonia in 14 patients in the PLT group vs 7 in the MST group, and finally, pneumothorax in 3 patients in the PLT group vs 1 in the MST group. SEROMA. Nine trials reported seroma between the two groups [10, 12, 14, 15, 18–22]. Seroma was diagnosed in 23 of 571 patients (4.0%) in the MST group; however, no seroma was reported in the PLT group. Four studies documented no seroma in either group. These studies appear to be excluded on the Forest plot (upper confidence limit is infinity; Fig 4). However, this was not the case because the StatsDirect software allows for a correction term by adding 0.5 to all cells that are 0 (Haldane method). There was no statistical heterogeneity between studies (Cochran Q ¼ 0.68, p ¼ 0.95; I2 ¼ 0%, 95% CI, 0% to 64.1%). In the random effect model, the risk of seroma was significantly higher in the MST group than in the PLT group (pooled OR, 8.26; 95% CI, 2.16 to 31.56; p < 0.01; Fig 4; Table 3). REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES 1099 Fig 4. Forest plot for pooled odds ratio of reported case of seroma after posterolateral thoracotomy (PLT) and muscle-sparing thoracotomy (MST). The solid squares denote odds ratios, the horizontal lines represent the 95% confidence intervals, and the diamond denotes the pooled odds ratio. (DL ¼ DerSimion Laird.) Comment A traditional PLT, which provides excellent exposure of the lung, pulmonary hilum, and mediastinum, has been the standard incision for pulmonary procedures for the past 100 years. However, disadvantages of this approach include the division of the major muscles of the chest, resulting in increased potential for blood loss, a moderate time requirement for opening and closing the incision, prolonged ipsilateral shoulder and arm dysfunction, scoliosis, compromised pulmonary function, and chronic postthoracotomy pain syndromes [1–3, 14]. As a result, there has been a search to identify the ideal incision in open thoracic operations. This search has been greatly facilitated with the advent of single-lung ventilation and the liberal use of stapling instruments that allow safe and precise resection through a less extensive thoracic opening [21, 22]. Vertical axillary thoracotomy was first reported by Browne in 1953 [4] but further developed in adult practice by Baeza and Foster [5]. Mitchell and colleagues [7] proposed a lateral MST, whereas Bethencourt and Holmes [8] were able to perform a MST with a conventional posterior thoracotomy approach. Horowitz and colleagues [6] described a technique involving an incision through the “auscultatory triangle.” Common to these incisions is preservation of the integrity of the LD and preservation of the SA or division of this muscle in line with the direction of its fibers. Of the described muscle-sparing incisions, in only the technique described by Horowitz and colleagues—through the auscultatory triangle—are no muscles divided [6]. In other described muscle-sparing incisions, when a lateral incision is used, slips of SA usually need to be elevated from the ribs, and the anterolateral and vertical axillary incisions both require splitting of the SA in line REVIEW Ann Thorac Surg 2014;97:1093–102 1100 REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES REVIEW with its fibers [4, 5, 7, 8]. More recently, there have been modifications of these techniques, including anteroaxillary and PLT with LD and SA detachment from its origin [22, 25, 26]. In general, it has been advocated that these MST approaches reduce postoperative pain, preserve pulmonary function, and lessen postoperative complications. Another potential advantage is the availability of extrathoracic musculature, such as LD and SA, for rotational flap control of postresectional space problems, empyema, or bronchopleural fistulas [14]. This meta-analysis shows that the pain scores are lower with MST than with PLT. However, the pain scores are only significantly lower on postoperative day 7. On day 1 and day 30, the reduction in pain was not deemed significant. This meta-analysis also showed that MST significantly improves internal rotation of the shoulder on day 30. However, there was no improvement in lung function (FEV1 or VC) on day 30. The secondary outcomes analysis showed an increased rate of seromas with the MST technique compared with PLT, although there was no difference in the total reported complications between the groups. There was also no significant difference between the incision sizes, duration of the operation, and hospital length of stay. Various factors contribute to postoperative pain after thoracic operations, including positioning during the procedure, crush injuries or muscle ischemia, injuries to intercostal nerves and vessels, especially during retraction, and rib fractures [27]. Pain also results from trauma to paraspinal ligaments and to the muscles and small joints of the back [28]. Furthermore, anesthesia, analgesic requirements, and patient-related factors such as age, sex, complications, or sociocultural aspects also all affect pain [29]. This meta-analysis showed that there was no significant improvement with the MST technique in reducing pain scores on day 1. One possible factor underlying our finding may be due to the contribution to postthoracotomy pain from incision of the skin and pleura and retraction of muscles and intercostal nerves. Both incisions elicit profound pain of both somatic and visceral origin. However, the difference in pain from muscle division alone, which is higher in the PLT group, may not be severe enough to impart a difference in outcome when measured against the degree of rib spreading, which is greater in MST to compensate for the diminished field of view. Furthermore, the incision made during certain MST approaches (eg, vertical and axillary) crosses at least 2 dermatomes, whereas the incision made during PLT runs along only 1 dermatome, and this may play a role in the early pain experienced by the patients [13]. Another explanation for why there appears to be no major difference in pain scores on day 1 may be that aggressive postoperative epidural analgesia, used in several of the studies, specifically targets the tissue disruption that might lead to greater pain in the PLT group [13]. Factors such as rib retraction, presence of chest drains, and epidural analgesia are less of an issue by day 7, which possibly accounts for the significant difference in pain scores observed between the groups at this stage. Ann Thorac Surg 2014;97:1093–102 Postthoracotomy pain can present for several weeks and months and represents a serious problem for some patients. Chronic pain, in particular, may have a major effect on the quality of life and is associated with significant health care costs. Neurophysiologic assessments have shown that intercostal nerve function is more commonly impaired 1 month after the operation with the PLT incision than with the MST incision [17]. However, our meta-analyses have shown no significant difference in postthoracotomy pain scores between the groups by day 30. Our failure to appreciate a small difference with respect to incision type may likely be the result of the relatively low rate of postthoracotomy pain on day 30, rendering it difficult to appreciate small differences between the groups. This meta-analysis showed no significant difference in the change in postoperative FEV1 and VC between the two groups after 30 days. PLT and MST both involve dividing the intercostal muscles within a given interspace, impaired lung compliance, and loss of volume due to lung resection. As a result, both groups will have a degree of postoperative respiratory dysfunction. However, the main difference between the two groups lies in the fate of the LD and SA muscles, both of which are weak accessory muscles of respiration. As a result, the lack of a significant difference in lung dysfunction between the groups on day 30 is not surprising. Ponn and colleagues [20] showed limited muscle sparing incisions may result in better long-term pulmonary function, but the differences were small and of no apparent clinical advantage in the average patient. Varela and colleagues [30] reported that preoperative FEV1, postoperative pain scores, and epidural analgesia were independently and reliably associated with the postoperative FEV1 ratio. By day 30, the difference in pain scores was insignificant in our meta-analysis, and this is a possible reason why there is no difference in the degree of respiratory dysfunction. There may have been a discernible difference in lung function tests between the two groups on day 7 when there was a significant difference in pain scores. However, we did not assess the FEV1 and VC status within the first postoperative week due to the limited number of studies available. This meta-analysis shows a significant improvement in internal rotation with MST compared with PLT 30 days after the procedure. This is to be expected given the sparing of the LD muscle, which has attachment to the humerus. The preservation of LD and SA allows range of movement and function of the arm to return to normal more readily. The studies that explored shoulder movement [12, 18, 21] specifically used the posterolateral MST approach. This approach does not risk damaging structures functionally involved, such as the long thoracic nerve. Although not significant, Landreneau and colleagues [19] showed that shoulder function returned to 97% of preoperative function after MST compared with 92% in the PLT group. Several studies, using a manual muscle test, have shown that MST results in better postoperative muscle strength of the shoulder girdle [14, 22]. Other studies that used a dynamometer to test isokinetic muscle strength also showed preserved strength of the shoulder girdle muscle after MST compared with PLT [28, 31, 32]. Preservation of muscle movement and strength by MST may be useful in manual workers, young adults, and athletes, particularly if the operation involves the dominant side. It is noteworthy that this is exactly the group of people in whom MST is technically more difficult and exposure more limited due to bulky musculature [6, 31]. Our evaluation of secondary outcomes showed a significantly increased incidence of seroma in the MST group. This is more commonly observed in the posterolateral MST where there is extensive mobilization of the LD leading to the creation of subcutaneous flaps [21, 22]. Five studies reported seroma in the MST groups [14, 18–21]. Four of these studies used the posterolateral approach [14, 18, 20, 21], which accounted for the higher rates of seroma seen overall in the MST approach due to the creation of flaps. The other study [19] used an anterior lateral MST approach. Various authors have tried to reduce the rates of seroma by modifying their technique such as the anteroaxillary thoracotomy technique [15, 16]. Despite the higher rates of seroma, the overall rates of complications reported, and therefore, hospital stay, were comparable between the groups. We have found that the MST does not increase the overall operative time. The increased time required to create the subcutaneous flaps and mobilize the LD and or SA are probably made up at closure, because it is not necessary to reapproximate the muscle edges. Our meta-analysis also showed no differences in the incision size between the groups. The MST provides acceptable access to the chest cavity for pulmonary resections when required. In addition, the MST allows access to the mediastinum and complete lymphadenectomy. Occasionally, its exposure may be difficult in heavily muscled individuals. In particular, axillary and auscultatory triangle thoracotomies are limited in opening width due to the lack of movable ribs and sometimes cause rib fractures at the opening site. However, if further visualization is required, it may be converted to the standard opening by simply incising the thoracic musculature. It was interesting to note that only one study in this meta-analysis reported rib fractures in both MST and PLT groups [10], whereas no cases in any study required conversion from MST to PLT [10–22]. This meta-analysis has inevitable limitations. The heterogeneity of some variables in this study is worthy of comment. The included trials varied in the inclusion criteria for the type of patients that they studied. For example, some only studied patients with lung cancers, whereas others assessed patients undergoing varied thoracic procedures. Unfortunately, the insufficient raw data were available to perform subgroup analyses. In addition, the types of MST procedures performed varied. We tried to counter these heterogeneities by using the random effects model. In addition, each individual trial had a different followup protocol and used different methods to evaluate some REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES 1101 of the outcome measures. There were also disparities in the quality of individual trials. Only three of the studies reported an intention-to-treat analysis, and this could lead to attrition bias in the other studies. None of the studies had a clear allocation concealment trail, and therefore, all were susceptible to selection bias. In addition, the trials included in our analysis spanned 20 years, a period in which surgical and anesthetic techniques changed dramatically. One thing we have learned with VATS is to compare approaches according to the rib-spreading process. One limitation of this meta-analysis is that the extent of rib spreading is not known. One study by Nosotti and colleagues [10] explored the extent of rib spreading between the groups but the results were not specified. Likewise, data on concomitant rib shearing or resection (indeed a possibility for both muscle-sparing and posterolateral techniques) are missing and may be important for pain analysis. Finally, this review has demonstrated that only a small number of trials have studied this subject. Conclusions drawn from a small number of studies must be interpreted with caution, and clearly, further research in this area is warranted. In conclusion, this meta-analysis demonstrates that the MST technique is associated with significant improvement in shoulder movement (internal rotation) and intermediate pain scores (day 7). There is negligible improvement in lung function tests on day 30. Despite the significantly higher rates of seroma, the overall complication rates are comparable between the two groups. We advocate the MST approach in most cases, particularly on the physically active patients who are dependent on a quicker recovery of shoulder function. We acknowledge the statistical analysis contribution from senior statistician, Peter Browne, from the institution of Medical Statistics, Queen Mary’s University, London, UK. References 1. Bernard A, Brondel L, Arnal E, Favre JP. Evaluation of respiratory muscle strength by randomized controlled trial comparing thoracoscopy, transaxillary thoracotomy, and posterolateral thoracotomy for lung biopsy. Eur J Cardiothorac Surg 2006;29:596–600. 2. Karmakar MK, Ho AM. Postthoracotomy pain syndrome. Thorac Surg Clin 2004;14:345–52. 3. Kucukarslan N, Kirilmaz A, Arslan Y, Sanioglu Y, Ozal E, Tatar H. Muscle sparing thoracotomy in pediatric age: a comparative study with standard posterolateral thoracotomy. Pediatr Surg Int 2006;22:779–80. 4. Singh SJ, Kapila L. Denis Browne’s thoracotomy revised. Pediatr Surg Int 2002;18:90–2. 5. Baeza OR, Foster ED. Vertical axillary thoracotomy: a functional and cosmetically appealing incision. Ann Thorac Surg 1976;22:287–8. 6. Horowitz MD, Ancalmo N, Ochsner JL. Thoracotomy through the auscultatory triangle. Ann Thorac Surg 1989;47: 782–3. 7. Mitchell R, Angell W, Wuerflein R, Dor V. Simplified lateral chest incision for most thoracotomies other than sternotomy. Ann Thorac Surg 1976;22:284–6. REVIEW Ann Thorac Surg 2014;97:1093–102 1102 REVIEW UZZAMAN ET AL META-ANALYSIS OF THORACOTOMY TECHNIQUES REVIEW 8. Bethencourt DM, Holmes EC. Muscle-sparing posterolateral thoracotomy. Ann Thorac Surg 1988;45:337–9. 9. Landreneau RJ, Mack MJ, Hazelrigg SR, et al. Videoassisted thoracic surgery: basic technical concepts and intercostal approach strategies. Ann Thorac Surg 1992;54: 800–7. 10. Nosotti M, Baisi A, Mendogni P, Palleschi A, Tosi D, Rosso L. Muscle sparing versus posterolateral thoracotomy for pulmonary lobectomy: randomised controlled trial. Interact Cardiovasc Thorac Surg 2010;11:415–9. 11. Endoh H, Tanaka S, Yajima T, Ito T, Tajima K, Mogi A, et al. Pulmonary function after pulmonary resection by posterior thoracotomy, anterior thoracotomy or video-assisted surgery. Eur J Cardiothorac Surg 2010;37:1209–14. 12. Athanassiadi K, Kakaris S, Theakos N, Skottis I. Musclesparing versus posterolateral thoracotomy: a prospective study. Eur J Cardiothorac Surg 2007;31:496–9. 13. Ochroch EA, Gottschalk A, Augoustides JG, Aukburg SJ, Kaiser LR, Shrager JB. Pain and physical function are similar following axillary, muscle-sparing vs posterolateral thoracotomy. Chest 2005;128:2664–70. 14. Akçali Y, Demir H, Tezcan B. The effect of standard posterolateral versus muscle-sparing thoracotomy on multiple parameters. Ann Thorac Surg 2003;76:1050–4. 15. Nomori H, Horio H, Suemasu K. Anterior limited thoracotomy with intrathoracic illumination for lung cancer: its advantages over anteroaxillary and posterolateral thoracotomy. Chest 1999;115:874–80. 16. Nomori H, Horio H, Fuyuno G, Kobayashi R. Non-serratussparing antero-axillary thoracotomy with disconnection of anterior rib cartilage. Improvement in postoperative pulmonary function and pain in comparison to posterolateral thoracotomy. Chest 1997;111:572–6. 17. Benedetti F, Vighetti S, Ricco C, et al. Neurophysiologic assessment of nerve impairment in posterolateral and muscle-sparing thoracotomy. J Thorac Cardiovasc Surg 1998;115:841–7. 18. Sugi K, Nawata S, Kaneda Y, Nawata K, Ueda K, Esato K. Disadvantages of muscle-sparing thoracotomy in patients with lung cancer. World J Surg 1996;20:551–5. 19. Landreneau RJ, Pigula F, Luketich JD, et al. Acute and chronic morbidity differences between muscle-sparing and standard lateral thoracotomies. J Thorac Cardiovasc Surg 1996;112:1346–50. Ann Thorac Surg 2014;97:1093–102 20. Ponn RB, Ferneini A, D’Agostino RS, Toole AL, Stern H. Comparison of late pulmonary function after posterolateral and muscle-sparing thoracotomy. Ann Thorac Surg 1992;53: 675–9. 21. Hazelrigg SR, Landreneau RJ, Boley TM, et al. The effect of muscle-sparing versus standard posterolateral thoracotomy on pulmonary function, muscle strength, and postoperative pain. J Thorac Cardiovasc Surg 1991;101:394–400. 22. Lemmer JH Jr, Gomez MN, Symreng T, Ross AF, Rossi NP. Limited lateral thoracotomy. Improved postoperative pulmonary function. Arch Surg 1990;125:873–7. 23. 2000 Guidelines of Meta-analysis Of Observational Studies In Epidemiology. Available at: www.consort-statement.org/? o¼1347. Accessed June 5, 2012. 24. The Newcastle-Ottawa Scale for assessing quality of nonrandomised studies in meta-analyses. Available at: http:// www.ohri.ca/programs/clinical_epidemiology/oxford.asp. Accessed June 5, 2012. 25. Fraund S, B€ oning A, Scheewe J, Cremer JT. Antero-axillary access for hypoplastic aortic arch repair. Ann Thorac Surg 2002;73:278–88. 26. Loscertales J, Congregado M, Moreno S, JimenezMerchan R. Posterolateral thoracotomy without muscle division: a new approach to complex procedures. Interact Cardiovasc Thorac Surg 2012;14:2–4. 27. Khelemsky Y, Noto CJ. Preventing post-thoracotomy pain syndrome. Mt Sinai J Med 2012;79:133–9. 28. Khan IH, McManus KG, McCraith A, McGuigan JA. Muscle sparing thoracotomy: a biomechanical analysis confirms preservation of muscle strength but no improvement in wound discomfort. Eur J Cardiothorac Surg 2000;18:656–61. 29. Wenk M, Schug SA. Perioperative pain management after thoracotomy. Curr Opin Anaesthesiol 2011;24:8–12. 30. Varela G, Brunelli A, Rocco G, et al. Predicted versus observed FEV1 in the immediate postoperative period after pulmonary lobectomy. Eur J Cardiothorac Surg 2006;30:644–8. 31. Kutlu CA, Akin H, Olcmen A, Biliciler U, Kayserilioglu A, Olcmen M. Shoulder-girdle strength after standard and lateral muscle-sparing thoracotomy. Thorac Cardiovasc Surg 2001;49:112–4. 32. Ziyade S, Baskent A, Tanju S, Toker A, Dilege S. Isokinetic muscle strength after thoracotomy: standard vs. musclesparing posterolateral thoracotomy. Thorac Cardiovasc Surg 2010;58:295–8.