gene202-10-13-2015-1..
advertisement

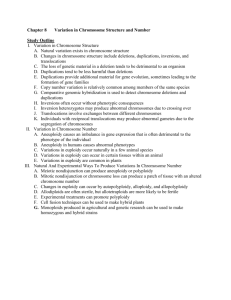
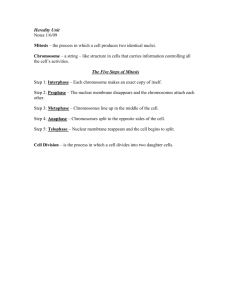
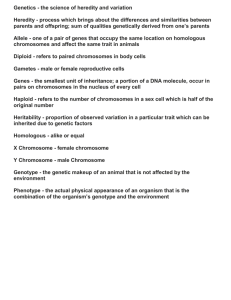
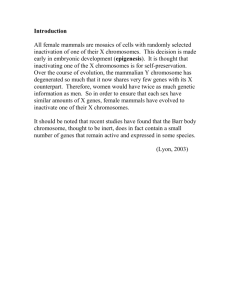
Genetics Mid-Quarter Review Session October 13, 2015 TAs: Ryan, Kayla, Paige, Paula, and Grace Notes 1. Review materials a. The slides from this session and review tables are posted on coursework b. Short videos posted on coursework c. This session will be videotaped 2. TA office hours a. Wednesdays in LK Cafe- see weekly email for exact times b. We are always happy to meet: please email us if the scheduled times do not work for you 3. Dr. Bernstein office hours a. Check coursework for dates/times b. Next one is tomorrow (Wed) at 2pm in LK Cafe Review Handouts Available on Coursework Agenda for Review Session 1. Mendelian Inheritance (Kayla) 2. Cytogenetic Abnormalities (Grace) 3. Cytogenetic and Molecular Testing (Ryan) 4. Non-Mendelian Inheritance (Paula) 5. Hardy-Weinberg, Bayes, and Consanguinity (Paige) Mendelian Inheritance Patterns ● Autosomal Dominant ○ ○ ○ ○ Penetrance Variable expression New mutations Anticipation ● Autosomal Recessive ○ Consanguinity ○ Founder effect ● X-linked Recessive ● X-linked Dominant *Optional Video Available on Coursework: Modes of Inheritance and Pedigrees What inheritance pattern is this? Autosomal Dominant Conditions 1. 2. 3. 4. Seen in multiple, successive generations Males and females equally affected Male-to-male transmission 50% risk to offspring of affected individuals in case of complete penetrance Autosomal Dominant Considerations 1. Penetrance: a. Not everyone with the mutation will develop the disease b. Think all or none 2. Variable expression: a. Different disease phenotypes arising from the same mutation b. Think spectrum 3. Anticipation: a. Symptoms appear to become more severe and/or arise earlier as generations pass b. Think trinucleotide repeat expansion 4. Other considerations: a. De novo (occurrence increases with paternal age) b. Germline mosaicism c. Nonpaternity What inheritance pattern is this? Autosomal Recessive Conditions 1. 2. 3. 4. Usually seen in a single generation Males and females are equally affected Recurrence risk for two carrier parents is 25% Unaffected sibling of an affected individual has a 67% risk of being a carrier 5. All offspring of an affected individual are obligate carriers; may be affected if other parent is a carrier or affected 6. Consanguinity increases likelihood Autosomal Recessive Considerations 1. Consanguinity: a. Matings between close relatives b. Increases likelihood of autosomal recessive condition 2. Founder Effect: a. High frequency of a specific gene mutation in a specific population due to the presence of that mutation in a single ancestor or a small number of ancestors ex. Ashkenazi Jews and Tay Sachs Disease What inheritance pattern is this? X-linked Recessive Conditions 1. 2. 3. 4. Affected males always related via females Male-to-male transmission does not occur All daughters of affected males are obligate carriers Sons of female carriers have 50% chance of being affected 5. Daughters of female carriers have a 50% chance of being a carrier What inheritance pattern is this? X-linked Dominant Conditions 1. Transmission from affected female is like autosomal dominant: all children (male and female) have a 50% chance of being affected 2. Transmission from affected male is like X-linked recessive: all females and no males will be affected 3. Rule out X-linked dominant: If a son of an affected male is affected or a daughter of an affected male is NOT affected Cytogenetic Abnormalities ● Disorders of Chromosome Number ● ● Euploidy Aneuploidy ● Isochromosomes ● Deletions/Duplications ● Ring Chromosomes ● Translocations- videos ● ● Reciprocal Robertsonian ● Inversions- video ● ● Paracentric Pericentric Cytogenetic Abnormalities ● Disorders of Chromosome Number ● ● Euploidy Aneuploidy ● Isochromosomes ● Deletions/Duplications ● Ring Chromosomes ● Translocations- videos ● Reciprocal ● Robertsonian ● Inversions- video ● ● Paracentric Pericentric http://www.larasig.com/sites/larasig.com/files/images/trisomy21_0. jpg Euploidy v. Aneuploidy ● Euploidy = chromosome # is an exact multiple of the haploid number (n)* --> Instead of (2n), zygote is (3n), (4n), (5n), ... Remember, n = 23 in humans ● Aneuploidy = chromosome # is NOT an exact multiple of the haploid number (n)* Monosomy: one fewer chromosome Turner Syndrome (45, XO) Trisomy: one extra chromosome Klinefelter Syndrome (47, XXY), Down Syndrome (47, XX/XY, +21) Aneuploidy ● Abnormal chromosome # that is NOT an exact multiple of the haploid number - Missing/extra chromosomes can be autosomes or sex chromosomes ● Due to: nondisjunction ■ Anaphase I of meiosis: homologous chromosomes fail to separate ■ Anaphase II of meiosis: sister chromatids fail to separate parent 1 gametes: parent 2 gametes: zygote: + n = 2n + 1 ➔ trisomy ONE EXTRA + n = 2n - 1 ➔ monosomy ONE FEWER http://www.biology.iupui.edu/biocourses/N100/2k2humancsomaldisorders.html Cytogenetic Abnormalities ● Disorders of Chromosome Number ● ● Euploidy Aneuploidy ● Isochromosomes ● Deletions/Duplications ● Ring Chromosomes ● Translocations- videos ● Reciprocal ● Robertsonian ● Inversions- video ● ● Paracentric Pericentric Isochromosomes Definition: Chromosomes with identical arms with each pair of loci equidistant from the center Result from: transverse rather than longitudinal division at the centromere (http://www.wikilectures.eu/images/2/29/Isochromosomes.jpg) Cytogenetic Abnormalities ● Disorders of Chromosome Number ● ● Euploidy Aneuploidy ● Isochromosomes ● Deletions/Duplications ● Ring Chromosomes ● Translocations- videos ● Reciprocal ● Robertsonian ● Inversions- video ● ● Paracentric Pericentric (http://upload.wikimedia.org/wikipedia/commons/5/5f/Deletion. gif) Deletions & Duplications ● Can be large or small (micro) ○ Larger deletions/duplications tend to have greater effects ● Location ○ Terminal - at the end of a chromosome ○ Interstitial - NOT at the end of a chromosome Deletions: generally more harmful ○ Ex: DiGeorge Syndrome (22q11.2 deletion) Duplications: generally less harmful Cytogenetic Abnormalities ● Disorders of Chromosome Number ● ● Euploidy Aneuploidy ● Isochromosomes ● Deletions/Duplications ● Ring Chromosomes ● Translocations- videos ● Reciprocal ● Robertsonian ● Inversions- video ● ● Paracentric Pericentric ring chromosome in Turner Syndrome Ring Chromosomes ● Double strand breaks at ends of a chromosome --> fusion of opposite arms to form a ring ● Usually associated with terminal deletions ● Can be inherited ring chromosome in Turner Syndrome Cytogenetic Abnormalities ● Disorders of Chromosome Number ● ● Euploidy Aneuploidy ● Isochromosomes ● Deletions/Duplications ● Ring Chromosomes ● Translocations- videos ● ● Reciprocal Robertsonian ● Inversions- video ● ● Paracentric Pericentric Translocations ● Definition: movement (“trans-location”) of a fragment of a chromosome to another, non-homologous chromosome ● Types: ○ Balanced v. Unbalanced ■ Balanced – no loss or gain of genetic information ■ Unbalanced – loss or gain of genetic information ○ Reciprocal and Robertsonian Reciprocal Translocations ● Non-homologous chromosomes swap chromosome segments ● ● ● Any pair of non-homologous chromosomes Breaks at any point along the chromosomes Can be balanced (more common) or unbalanced Possible Gametes - Reciprocal Chromosomal Rearrangements Robertsonian Translocations ● Non-homologous chromosomes swap chromosome segments ● ● ONLY acrocentric non-homologous chromosomes (13, 14, 15, 21, 22) Breaks ONLY at the centromeres ● This produces… ● ● Metacentric fusion of p arms → lost in subsequent divisions, contain redundant material Metacentric fusion of q arms → propagated in offspring p p q q q p p q Possible Gametes - Robertsonian balanced carrier trisomy/monosomy trisomy/monosomy Chromosomal Arrangements Cytogenetic Abnormalities ● Disorders of Chromosome Number ● ● Euploidy Aneuploidy ● Isochromosomes ● Deletions/Duplications ● Ring Chromosomes ● Translocations- videos ● Reciprocal ● Robertsonian ● Inversions- video ● ● Paracentric Pericentric Inversions ● Definition: a segment of a chromosome is inverted (reversed, end to end) and inserted back into the same position ● Types: 1) Paracentric – the inverted segment DOES NOT include the centromere → Produces gametes with acentric and dicentric chromosomes; these offspring are non-viable 2) Pericentric – the inverted segment DOES include the centromere * I = INCLUDES the centromere! Your Favorite Diagram! Pericentric Inversions Normal TAKE-HOME POINTS: Inverted * 4 possible meiotic products * If you suspect two family members have the same condition but their phenotypes differ... * If you see a duplication & deletion on the same chromosome... THINK PERICENTRIC INVERSION Helpful OPTIONAL video on Coursework! Cytogenetic and Molecular Techniques ● Cytogenetic techniques: ○ Karyotype - video ○ FISH - video ○ array CGH - video ● Molecular Techniques: ○ Sanger sequencing - video ○ Next generation sequencing - video ○ SNP genotyping - videos ○ MLPA - video ○ Methylation studies - video Helpful OPTIONAL videos on Coursework! Karyotype ● What is it? ○ A cytogenetic method of surveying the entire genome for numerical or structural chromosome abnormalities ● How is it done? ● What types of tissue sources are used? ○ ○ ○ ○ T lymphocytes from blood (easily induced to divide in cell culture) Fibroblasts from skin biopsy Amniotic fluid and chorionic villi (prenatal) Bone marrow, solid tumors (cancer) All living cells! Karyotype: Final Result chromosomes are placed in order from the images Karyotype resolution Karyotype ● Typically used for: ○ Numerical chromosomal abnormalities ○ Balanced translocations ○ Inversions (peri- and para-) ● Limitations: ○ Do not detect submicroscopic deletions and duplications Fluorescence in situ hybridization (FISH) ● What is it? ○ A method to look for presence or absence, copy number, or chromosomal location of a particular DNA sequence in the context of a chromosome ● How is it done? ○ ○ ○ ○ ○ ○ Produce an interphase cell nucleus or metaphase chromosome preparation; attach cells/chromosomes to glass slide Construct a cloned DNA sequence (aka ‘probe’) Tag with fluorescent dye Denature cell DNA in place (in situ) to expose single strands; denature probe Allow probe to hybridize to the chromosomal DNA The hybridized probe will fluoresce when viewed with wavelength of light that excites the fluorescent dye View under microscope Fluorescence in situ hybridization (FISH) Metaphase versus Interphase FISH ● Metaphase FISH ○ ○ ● Chromosomes look like those in a karyotype Provides better information on the position of a probe target sequences Interphase FISH ○ ○ Can aid in identifying closely spaced duplications of genetic material as the chromosomes are less condensed Can be done more quickly since the cells do not have to be in any specific stage of the cell cycle. Fluorescence in situ hybridization (FISH) ● Typically used for: ○ Testing for specific microduplication or microdeletion ○ Confirming array CGH results/confirming the location ● Limitations: ○ Each FISH probe tests for deletion or duplication at one locus ● Alternatives: ○ MLPA Array Comparative Genomic Hybridization (CGH) ● What is it? ○ Method to quantitatively test for presence or absence of many specific DNA sequences simultaneously (can test the entire genome at once) ● How is it done? Sample aCGH data-deletion chromosome 22 duplication chromosome 16 * More dots (DNA elements on array) = higher resolution * Smallest detectable anomalies: ~50 kb Array Comparative Genomic Hybridization (CGH) ● Typically used for: ○ Simultaneous testing for microduplications and microdeletions across the genome ○ Can detect changes too small to be seen under microscope ○ Does not require prior knowledge of chromosomal location of any variant ● Limitations: ○ Does not detect balanced rearrangements ○ Resolution depends on the number of elements on array ○ Does not provide information on position of Sanger Sequencing ● What is it? ○ ○ ● Most commonly used method for assessment of DNA sequence in clinical practice Most clinical sequencing focused on exons and exon boundary sites How is it done? Sanger Sequencing ● Typically used for: ○ Identification of single base pair change ○ Small insertions and deletions ● Limitations: ○ Does not reliably detect large deletions / duplications ○ Not quantitative ○ Allele drop-out (one of two alleles is not detected in the assay because presence of deletion prevents primer binding) ○ Does not distinguish whether two sequences are present in cis versus trans configuration Next Generation Sequencing Next Generation Sequencing ● ● ● ● ● ● ● DNA is fragmented Linker is ligated, DNA is conjugated to flow cell Bridge amplification of DNA First round of amplification with reversible terminator Laser excite and image Repeat cycles Image and reconstruct data Next Generation Sequencing ● ● ● ● ● Typically used for screening of multiple genes In combination with capture approaches can be used to sequence a specific panel of genes Higher error rate than Sanger sequencing (this is improving) High chance of incidental findings Relatively expensive Multiplex Ligation-Dependent Probe Amplification Assay (MLPA) ● What is it? ○ A method to detect medium to large deletions/duplications (kilobase to megabase) ● How is it done? ○ Combination of DNA hybridization and PCR amplification Multiplex Ligation-Dependent Probe Amplification Assay (MLPA) MLPA sample result: deletion in dystrophin gene Multiplex Ligation-Dependent Probe Amplification Assay (MLPA) ● Typically used for: ○ Assessment for a specific set of microdeletions / microduplications ● Limitations: ○ Does not provide information on large-scale architecture ○ Does not indicate presence or absence of cytogenetic abnormalities ○ Does not provide position information ● Alternatives: ○ high resolution CGH Methylation studies ● Typically used for: ○ Assessment of methylation status ○ Why? DNA sequencing methods and the PCR reaction do not distinguish methylated from unmethylated DNA ● Methylation in DNA is present on cytosine Methylation studies: bisulfite treatment methylation-sensitive PCR, MLPA Methylation studies Method 2: Restriction enzymes Sample with Sample with No methylation site HpaII HpaII These techniques are used in combination ● aCGH + FISH ● NGS + Sanger sequencing ● Karyotype + FISH Non-Mendelian Inheritance ● Epigenetic ● Imprinting ○ Methylation testing ● Mitochondrial ○ Heteroplasmy ● Multifactorial ○ Threshold Model ○ Empirical Risk Studies ○ GWAS Imprinting What is imprinting? A. DNA methylation at locations rich in CG dinucleotides (CG motifs), associated with gene silencing (blocks transcription factors, recruit repressors) Genomic imprinting: A. Sex of the parent can cause distinguishable methylation during meiosis Example of Imprinting Disorders Prader-Willi Syndrome (PWS) Angelman Syndrome (AS) ● Both due to defects in the same area of chr15 (15q1113) (Pagon et al., 2013) Angelman vs. Prader-Willi 1. Angelman Syndrome: a. Due to deletion/inactivation of information on maternal chromosome b. UBE3A gene dysregulated c. Phenotype: hypotonia, poor feeding, microcephaly, seizures, poor speech, ataxia, happy demeanor 2. Prader-Willi Syndrome: a. Deletion/inactivation of information on chromosome b. A snoRNA cluster of genes affected c. Phenotype: hypotonia, initial poor feeding, later excessive feeding, motor and language delay, hypogonadism paterna Causes of Angelman Syndrome (Adams 2008) Causes of Prader-Willi Syndrome (Cassidy & Driscoll 2009) Detecting DNA Methylation Mitochondrial Inheritance (Lemire 2005) Mitochondrial Inheritance = Heteroplasmy Mitochondrial (Lemire 2005) Multifactorial Inheritance Liability Environmental Factors Empirical Risk Model Concordance: presence of the same trait in both twins Heritability: portion of a trait attributable to genetic variance (Smoller & Finn 2003) Hardy-Weinberg p2+2pq+q2=1 ● Assumptions: random mating, no migration, no new mutations, no selection ● 3 possible genotypes: AA, Aa, aA, aa ● Allele frequencies ○ p= frequency of dominant allele, A ○ q=frequency of recessive allele, a ● Genotype frequencies ○ p2 =chance of being AA ○ q2 =chance of being aa ○ 2pq=carrier frequency ● 2pq≈2 x 1 √(incidence of the condition) Population and Quantitative Genetics ● Autosomal recessive ● Incidence is 1/4900 ● P (Mother is Carrier) ? ● P (Father is Carrier) ? ● P (Child would be affected) ? Bayes Theorem ● Update a risk estimate based on new info ○ Family history ○ Test results ○ Age dependent penetrance ● P (Child would be affected) ? *Optional Videos Available on Coursework: Probability and Bayes Theorem Consanguinity ● 2nd cousins or closer ● Risk of recessive disease ● Identity by descent ○ When both copies of an allele are identical because they were inherited from a common ancestor ● Coefficient of inbreeding ○ Fraction of a person’s genes that are identical by descent ○ Probability that a person is identical by descent at a particular locus Consanguinity ● P (Mother is Carrier) ? ● P (Father is Carrier) ? ● P (Child is affected) ? ● Increased risk for AR conditions Thanks! Please feel free to email the TAs if you have any questions. Ryan: rmgallag@stanford.edu Kayla: kaylah@stanford.edu Paige: pqin@stanford.edu Paula: ptrepman@stanford.edu Grace: gxiong@stanford.edu