Journal of Biomechanics 35 (2002) 665–671
Fluid dynamics of the left ventricular filling in dilated
cardiomyopathy
Bernardo Baccania, Federico Domenichinia,*, Gianni Pedrizzettib, Giovanni Tontic
Dipartimento di Ingegneria Civile, Universita" di Firenze, Via S. Marta 3, 50139 Firenze, Italy
b
Dipartimento di Ingegneria Civile, Universita" di Trieste, p.le Europa 1, 34127 Trieste Italy
c
Ospedale SS. Annunziata, Division of Cardiology, via Circonvallazione Occidentale 145, 67039 Sulmona, Italy
a
Accepted 28 December 2001
Abstract
Modifications in diastolic function occur in a broad range of cardiovascular diseases and there is an increasing evidence that
abnormalities in left ventricular function may contribute significantly to the symptomatology. The flow inside the left ventricle
during the diastole is here investigated by numerical solution of the Navier–Stokes equations under the axisymmetric assumption.
The equation are written in a body-fitted, moving prolate spheroid, system of coordinates and solved using a fractional step method.
The system is forced by a given volume time-law derived from clinical data, and varying the two-degrees-of-freedom ventricle
geometry on the basis of a simple model. The solution under healthy conditions is analysed in terms of vorticity dynamics, showing
that the flow field is characterised by the presence of a vortex wake; it is attached to the mitral valve during the accelerating phase of
the E-wave, and it detaches and translate towards the ventricle apex afterwards. The flow evolution is discussed, results are also
reported as an M-mode representation of colour-coded Doppler velocity maps. In the presence of ventricle dilatation the mitral jet
extends farther inside the ventricle, propagation velocity decreases, and the fluid stagnates longer at the apex. r 2002 Elsevier
Science Ltd. All rights reserved.
Keywords: Left ventricle; Diastole; Fluid dynamics; Vorticity dynamics; Vortices
1. Introduction
The role of the diastolic function in human health and
disease remains nowadays enigmatic, depending on the
difficulty in its assessment by physical examination or
even by direct invasive measurement. Diastolic dysfunction can be defined as the inability of the hearth to
accept adequate filling volume without an abnormal
raise of the filling pressure; it is an early, and sometimes
unique, manifestation of myocardial disease (Mandinov
et al., 2000). Unfortunately, the non-invasive diagnostic
tools currently available in the clinical setting are
affected by the large number of haemodynamic dependent or independent variables which influence the
measured parameters. For this reason, an unambiguous
interpretation in terms of correspondence between
*Corresponding author. Tel.: +39-055-4796321; fax: +39-055495333.
E-mail address: federico@ingfi1.ing.unifi.it (F. Domenichini).
definite pathological processes and typical semeiologic
signs is difficult to achieve. An intriguing aspect of the
left heart dynamics is the hypothesised occurrence of
diastolic vortices within the ventricular chamber; it has
been recognised by several investigators using simple
theoretical models and flow visualisation techniques
(Bellhouse, 1972; Reul et al., 1981; Wieting and
Stripling, 1984; van Dijk, 1984). Those studies and
other recent observations based on colour Doppler
mapping (Kim et al., 1994; Firstenberg et al., 2000;
Tonti et al., 2001) and on Magnetic Resonance Imaging
(Kim et al., 1995; Kilner et al., 2000) stimulated our
interest in clarifying the phenomenon with the objective
to obtain a quantitative description. An accurate
modelling of the flow inside the left ventricle can
contribute to build interpretative schemes of these
observations.
Recently, the problem has been investigated using
the numerical approach. From a mathematical point
of view, the problem can be represented as a
0021-9290/02/$ - see front matter r 2002 Elsevier Science Ltd. All rights reserved.
PII: S 0 0 2 1 - 9 2 9 0 ( 0 2 ) 0 0 0 0 5 - 2
666
B. Baccani et al. / Journal of Biomechanics 35 (2002) 665–671
three-dimensional flow entering into an expanding
cavity, where a dominant role is played by the fluid–
wall interaction; in order to solve such a problem several
parameters are in principle required, among these the
ventricular geometry, the mechanical properties of the
wall, and the time-laws of the entering flow and of the
pressure, at least in one point of the domain. Different
models have been developed, each of them focussed on
the analysis of particular aspects of the problem, thus
characterised by specific simplifying assumptions. A
relevant phenomenon commonly detected is the presence of diastolic vortices, which are generated by the
incoming flow through the mitral valve.
A numerical scheme based on the adaptive finite
elements method has been employed to analyse the
flow during the diastolic filling (Vierendeels et al., 2000).
The wall finite displacements are there evaluated by a
linear thin elastic membrane model with a time-varying
Young modulus, extending a one-dimensional scheme
developed previously (Vierendeels et al., 1997). This
technique, although limited to the axisymmetric approximation, requires a special effort to capture the local
details of the diastolic flow: a high resolution is
necessary to describe the thin vorticity layer shed from
the mitral valve, and to solve the complex interaction
between the incoming jet and the thin wall boundary
layers. A further difficulty is represented by the
definition of the inlet velocity profile, depending on
the scarcity of experimental data, whose characteristics
are intimately connected to the properties and the size of
the wake vortices. In (Vierendeels et al., 2000) an
ellipsoidal ventricle is assumed at end systole, the valve
is reproduced by extending the length beyond the
maximum ellipsoid radius, and an unspecified blunt
inlet profile is assumed. As a result, the mitral jet
front vortex occupies the whole chamber similarly to the
tube flow in presence of an expansion (Pedrizzetti,
1996). Notwithstanding these points the analysis of
Vierendeels et al. (2000) represents, presently and to the
authors’ knowledge, the most accurate simulation under
realistic conditions, therefore the one to compare with.
The alternative method of the immersed boundary
elements, for the coupled solution of the fluid–wall
problem, has been applied to the dynamics of the left
heart (Lemmon and Yoganathan, 2000, and references
therein). This general three-dimensional technique is
able to give an overall picture in arbitrarily complex
geometry, however it is unable to resolve accurately the
boundary layers depending on the used interpolating
procedure.
The numerical results can be compared with experimental and clinical data; in the present context it is
useful to compare them with quantities commonly
measured in the clinical practice, such as the space–time
distribution of the velocity component along a vertical
line inside of the ventricle given by a color M-mode
Doppler echocardiography (Takatsuji et al., 1997;
Garcia et al., 1998, and references therein). The
mentioned numerical results (Vierendeels et al., 2000)
give M-mode maps in qualitative agreement with clinical
observations (Stugaard et al., 1994; Garcia et al., 1998)
and with experimental findings obtained with a thin
rubber ventricle model (Steen and Steen, 1994), where
the dependency of the measured velocity on the
characteristics of the mitral valve is quantified.
On the basis of the experimental and numerical results
a physical picture of the left ventricle filling can be given,
at least in axisymmetric flow under healthy conditions.
Initially, the mitral inflow enters at once in the whole
ventricle with a velocity that decreases from the valve
value to the slowly moving apex; during this initial
phase a wake is generated and remains attached to the
valvular edge. In a second phase, usually corresponding
to the deceleration of the inlet flow (diastasis), the
attached wake is released and translates toward the
ventricle apex; the wake interacts with the ventricle wall,
generates induced boundary-layers and secondary vortices.
The present work aims to provide an insight to the
fluid mechanics in the left ventricle during the unsteady
filling period, diastole, by an accurate numerical
solution of the Navier–Stokes equations in an idealised
ventricle geometry. The flow phenomena are studied
under healthy conditions using data adapted from
clinical measurements, the results are assumed as a
reference for the subsequent investigation. This deals
with the flow modifications induced by a different
geometry of the ventricle, which in the present work is
assumed as a simplified model of dilated cardiomyopathy. The axisymmetric approximation is assumed in
this first instance. The left ventricle is modelled as a
truncated prolate spheroid, a geometry representative of
an idealised still realistic ventricle. The mitral valve, held
open, corresponds to a thin circular orifice at the inlet
where a flow with infinitesimal boundary layer is
allowed. The fluid equations are solved by finite
differences in boundary fitted moving coordinates.
The numerical scheme allows a detailed description
of the most relevant fluid phenomena, in particular
it is able to capture narrow vorticity layer, like the
boundary layer at the wall and the entering vortex
wake, and their interaction. The system is forced by a
given time law of the inflow discharge adapted from
clinical data, the wall motion is derived from this on the
basis of a simple elastic membrane model. A physically
based irrotational inlet velocity profile is assumed,
without any further specification. Results are reported
under healthy conditions and at different pathological
stages of a virtual dilated cardiomyopathy. The fluid
dynamics is analysed in combination with clinical-like
M-mode to eventually propose interpretative physical
pictures.
B. Baccani et al. / Journal of Biomechanics 35 (2002) 665–671
where Cm and CZ represent the convective terms, which
include the coordinates’ kinematics,
2. Methods
The flow dynamics inside a model left ventricle of an
incompressible fluid with density r and kinematic
viscosity n is studied. The ventricle is assumed to be
half of a prolate spheroid, with half long axis H n ðtn Þ
and diameter Dn ðtn Þ; tn is the dimensional time. The
mitral valve is modelled as an orifice of infinitesimal
thickness in the equatorial plane, with a diameter Dnv ðtn Þ;
the ratio Dnv =Dn is kept constant in time. The system is
forced by a given temporal law of the inlet discharge
Qn ðtn Þ; derived by clinical data. The relative dynamics of
the two degrees of freedom ventricle geometry is
determined on the basis of a simple elastic wall
modelling.
The fluid flow is assumed to be axisymmetric.
The problem is made dimensionless assuming
as reference time scale T the heartbeat period.
A reference inlet velocity U is the peak inlet mean
velocity at the valve orifice; the reference lengthscale is
then L ¼ UT ; and the unit mass is rL3 : Such choices
allow an easy readability of results and immediate
comparison with clinical data, being i.e. TC1 s and
UC1 m=s: In what follows dimensionless quantities are
considered.
The equations to be solved are the Navier–Stokes and
continuity equations
@v
1
þ ðv rÞv ¼ rp þ
r2 v;
@t
ReT
ð1Þ
r v ¼ 0;
ð2Þ
where v is the velocity vector, p the pressure, ReT ¼
U 2 T=n is the Reynolds number corresponding to the
chosen units. The impenetrability and no-slip conditions
at the wall give the fluid–structure interaction; the
conditions at the inlet represent a model for the
upstream atrial flow.
The equations are expressed in a moving, boundaryfitted, prolate spheroid system of coordinates fm; Zg;
whose relations with the standard cylindrical coordinates
fr; zg
are
r ¼ dðtÞ sinhðaðtÞmÞ sin Z;
z¼
dðtÞ coshðaðtÞmÞ cos Z (Baccani et al., 2002). The functions d and a are connected to the geometric properties
by d ¼ ðH 2 D2 =4Þ1=2 ; a ¼ tanh1 ðD=2HÞ: In these
coordinates, the flow domain is mA½0; 1 ZA½0; p=2;
the ventricle wall corresponds to the coordinate curve
m ¼ 1; the mitral plane is Z ¼ p=2; and the axis of
symmetry is along the two coordinate curves m ¼ 0 and
Z ¼ 0: The vector form (1) of the Navier–Stokes
equations is split in its scalar components
@vm
1
þ Cm þ Gm ðp; dÞ Dm ðvm ; vZ ; dÞ ¼ 0;
ReT
@t
@vZ
1
þ CZ þ GZ ðp; dÞ DZ ðvm ; vZ ; dÞ ¼ 0;
ReT
@t
667
ð3Þ
Cm
¼
CZ
¼
1 @vm
1 @vm
ðvm cm Þ þ
ðvZ cZ Þ
ah @m
h @Z
vZ @h
vZ @h
þ 2 ðvm cm þ mh’aÞ 2 ðvZ cZ Þ;
h @Z
ah @m
1 @vZ
1 @vZ
ðvm cm Þ þ
ðvZ cZ Þ
ah @m
h @Z
vm @h
vm @h
2 ðvm cm þ mh’aÞ þ 2 ðvZ cZ Þ;
h @Z
ah @m
the cm ; cZ are the velocity components of the moving grid
in the physical space
’ sinhðamÞ coshðamÞ þ m’ah;
cm ¼ dd
h
’ cos Z sin Z;
cZ ¼ dd
h
the dot means time derivative, and the metric coefficient
h ¼ dðcosh2 ðamÞ cos2 ZÞ1=2 : G and D are the gradient
and Laplacian operators, respectively (Morse and
Feshbach, 1953). The continuity constraint (2) is then
imposed in the numerical method by the fractional-step
technique. Eqs. (3) are completed by the symmetry and
no-slip boundary conditions. At the inlet the entering
velocity profile is automatically evaluated from the
incompressibility of the fluid under the condition of
irrotational entry flow, representing the properties of the
incoming atrial flow. The flow inside the atrium
accelerates to enter through the narrow mitral valve
into the ventricle, the boundary layer is extremely thin
because of the converging nature of the flow and of its
unsteadiness.
The flow in the ventricle is specified once the temporal
variation of the two geometric parameters DðtÞ and HðtÞ
is given. These can in principle be obtained from the
computed transmural pressure by assuming an elastic
model for the whole ventricle and by the knowledge of
the time varying elastic properties; in addition the
pressure time-law pðtÞ at the inlet must also be given.
These data are not measured in routine clinical
observations. In the present work, the coupled fluid–
wall dynamics is not analysed; the wall motion is derived
on the basis of a simple elastic model and from the
knowledge of the inlet discharge QðtÞ which is the
temporal variation of volume. For this purpose, the
following relation:
dD ð8H 2 D2 Þ dH
¼
D
4H 2
H
ð4Þ
is introduced.
Formula (4) is obtained assuming that the ratio
between deformations (not deformation itself ) can be
taken from a simplified elastic membrane model, when
the deformations are estimated from the membrane
stresses at the equatorial plane (Baccani et al., 2002).
Being the discharge Q ¼ dV =dt and V ¼ ðp=6ÞD2 H the
ventricle volume, insertion of (4) gives an ordinary
B. Baccani et al. / Journal of Biomechanics 35 (2002) 665–671
668
differential equation for the diameter
2
2
dD 6Q
8H D
¼
dt
p 20H 3 D 2HD3
ð5Þ
and, from (4), for the ventricle height HðtÞ: Based on
these, the temporal evolution of the prolate spheroid
parameters d and a can then be obtained. Relation (4)
has the correct asymptotic behaviour of a sphere, that is
dD=D ¼ dH=H; when D ¼ 2H; when HbD; a cylinder
is reproduced, giving dD=D ¼ 2 dH=H: Relation (4) has
been tested with one clinical data set showing errors that
could not be separated from the measurement uncertainty. Given the available data and the possible large
variation of real conditions, approximation (4) represents a simplest first approach to model the wall
dynamics on the basis of the only knowledge of an inlet
flow-rate and an initial condition for the ventricle
geometry.
The problem has been numerically solved in primitive
variables, with finite differences, using a fractional step
method on a face-centred staggered grid. An explicit
third-order Runge–Kutta scheme has been used for time
advancement, the spatial derivative are approximated
with a second-order finite differences scheme. In order
to obtain a better resolution close to the walls and in
correspondence of the inlet edge, where large gradients
are expected, stretched coordinates are adopted. A
complete description of the mathematical formulation
and of the numerical technique is given in Baccani et al.
(2002).
3. Results
Clinical observations show that the dilated cardiomyopathy is, in first instance, characterised by enhanced
ventricle dimensions; modifications of the inflow timelaw are also detectable, and they become increasingly
relevant when pathology grows worse (Garcia et al.,
1998; Kaji et al., 2001, and references therein). In the
present work, the inlet flow is kept constant when the
ventricle diastolic volume is increased, in order to
_4
x 10
6
E
A
3
Q 0
_3
S
_6
0
0.2
0.4
t
0.6
Fig. 1. Inlet flow rate.
0.8
1
investigate the influence of the ventricle dilatation only.
The inlet discharge is adapted from clinical data and is
reported in Fig. 1, it presents two maxima, the first
corresponding to the early filling stage, E-wave, and a
secondary, A-wave, given by the atrial contraction. The
systolic phase, S, is here reproduced numerically, only to
allow the observation after the end of diastole, simply by
allowing the flow to exit from the whole equatorial
plane.
The dependence of the ventricle size on the different
degrees of pathology has been modelled introducing the
linear relations for the geometry at the end of the
diastole
D ¼ 0:04g þ D0 ;
H ¼ H0 þ 0:02g;
ð6Þ
where D0 ¼ 0:05 and H0 ¼ 0:09 are the values for
normal conditions (healthy, non-professional athlete);
the numerical coefficient g in (6) has been adapted from
clinical data and assumes values in the range between 0
and 1 depending on the ventricle dilatation. The cases
g ¼ ½0; 0:25; 0:5; 0:75 have been studied here.
Once the inflow is given, Fig. 1, the temporal law DðtÞ;
and similarly HðtÞ; is evaluated integrating equation (5)
with different initial condition, giving therefore different
evolution of the ventricle geometry. The inlet unitary
velocity at the peak of the E-wave is kept constant,
fixing the same value of the valve diameter at this
reference instant of time.
The flow evolution in the healthy case, g ¼ 0; is first
analysed in order to describe the typical features of the
diastolic filling. The fluid is initially subjected to the Ewave strong accelerating phase; the presence of the
mitral valve induces an almost instantaneous flow
separation with the birth of an attached positive vortex
sheet that immediately rolls-up into a wake vortex. This
vortex induces an opposite sign boundary-layer vorticity
at the ventricle wall, Fig. 2a at t ¼ 3=64: At the end of
the accelerated phase, tC0:165; the boundary-layer
vorticity sharply separates from the wall, the primary
vortex is released from the valvular edge and begins to
translate toward the ventricle apex, Fig. 2b. At this time
a weaker newly formed vortex is created at the valve
when the inflow decays to small values. Afterwards, the
primary wake vortex translates inside the ventricle and
reaches, during its decay, the apex; one instant of the
vortex propagation process is reported in Fig. 2c at
tC21=64: The subsequent dynamics presents a complex
interaction between the detached vortices, and the
superposition of the secondary filling wave, A-wave,
with a weak new vortex at the mitral edge.
A common measure in clinical practice is given by the
time evolution of the axial velocity along a transmitral
line in the centre of the ventricle. This is represented as a
colour image, M-mode image, which gives an insight to
the space-temporal flow pattern. This is shown in Fig. 3
in correspondence of the present simulation with
B. Baccani et al. / Journal of Biomechanics 35 (2002) 665–671
669
0.02
0.01
0
0.01
0.02
(a)
0.02
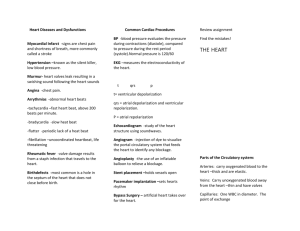
Fig. 3. Space–time map of the axial velocity, g ¼ 0: Contour levels
from 0:9 to 0:9; step 0:2; the estimation of the propagation velocity
Vp ¼ 0:23 is shown by thick dashed line.
0.01
0
0.01
0.02
(b)
0.02
0.01
0
0.01
0.02
(c)
0.08
0.06
0.04
0.02
0
Fig. 2. Instantaneous vorticity and velocity fields, g ¼ 0 (healthy case);
3
6
(a) t ¼ 64
; (b) t ¼ 64
; (c) t ¼ 21
64: Vorticity levels: from 5 to 105; step 10
(black) and symmetric negative values (grey).
contour lines superimposed. The main feature is
represented by two well recognisable velocity traces.
The first one develops during the initial accelerating
phase, it is almost vertical and corresponds to the
irrotational bulk flow entering into the ventricle during
the E-wave. It presents a higher velocity at the mitral
orifice and lower values into the wider, ventricle
chamber. The second trace is given by the higher
velocities found in correspondence of the primary
vortex, after it has detached, during its translation
toward the apex; a linear approximation of such a trace
is reported in Fig. 3, thick dashed line. The slope of this
line, therefore, represents the propagation velocity of the
vortex during its initial dynamics, while the velocity
decreases when the vortex approaches the apex, say after
tC0:4: The slope has been estimated by using a best-fit
procedure, once local extrema of the space–time map of
the axial velocity have been found, giving a value
Vp C0:24:
The appearance of a pathological behaviour can be
related to a different evolution of the primary vortex. In
Fig. 4, the instantaneous fields, immediately before the
primary vortex detachment from the valvular edge, are
reported for the three cases analysed, g ¼ 0:25; 0:5; 0:75:
The wake reduces its influence to the side wall when the
ventricle is more dilated. It follows that the still attached
primary wake vortex is able to elongate well inside the
ventricle. Wake elongation increases at increasing values
of g; it grows in size and remains attached to the mitral
valve even during the decelerating phase of the E-wave.
This pathological behaviour can be noticed from the
M-mode representations given in Fig. 5. The first phase
does not terminate at the E-wave inflow peak because
the jet flow persists until the vortex remains attached to
the valvular edge. It is well known that the dynamics of
an attached vortex is completely different from that of a
free vortex because the flux of vorticity changes its
impulse (Pullin, 1978; Saffman, 1992). The initial almost
vertical trace, which corresponds to an irrotational
synchronous entry flow, is then curved by the decelerating translation of the attached vortex. Afterwards, when
the vortex detaches, a smaller propagation velocity can
be estimated before the vortex slows down near the
apex. These effects are increasingly appreciable with
growing dilatation of the ventricle, giving values of Vp
ranging between 0:21 and 0:11; for g ¼ 0:25 and 0:75;
respectively.
4. Discussion
The flow dynamics inside the a model left ventricle
has been analysed by an accurate numerical method
under the assumptions of axisymmetric flow and fixed
mitral valve. In the case of healthy conditions the flow is
characterised by the generation of a wake vortex during
the E-wave; it detaches from the valvular edge at the end
of the accelerating phase because of the vortex induced
boundary-layer separation. Afterwards, the vortex ring
B. Baccani et al. / Journal of Biomechanics 35 (2002) 665–671
670
0.02
0
0.02
(a)
0.02
0
0.02
(b)
Fig. 5. Space–time map of the axial velocity; (a) g ¼ 0:25; (b) g ¼ 0:5;
(c) g ¼ 0:75: Contour levels from 0:9 to 0:9; step 0:2; the estimations
of the propagation velocity Vp ¼ ½0:21; 0:15; 0:11; a to c, respectively,
are shown by thick dashed lines.
0.02
0
0.02
(c)
0.1
0.08
0.06
0.04
0.02
0
Fig. 4. Instantaneous vorticity and velocity fields; (a) g ¼ 0:25 at t ¼
15
20
22
64; (b) g ¼ 0:5 at t ¼ 64; (c) g ¼ 0:75 at t ¼ 64: Vorticity levels: from 5 to
105; step 10 (black) and symmetric negative values (grey).
translates towards the apex by self-induced convection.
This behaviour is well represented in a M-mode
visualisation which shows the two traces corresponding
to the initial synchronous inflow and the following
vortex propagation. Such a dynamics is in general
agreement with the experimental results by Steen and
Steen (1994) and with the numerical outcomes of an
analogous case by Vierendeels et al. (2000) despite some
differences in the assumptions and in the modelling.
The simulated pathological conditions, dilated ventricle with the same inflow time-profile, nearly corre-
spond to a dilated cardiomyopathy, where the ventricle
stiffness is moderately increased before the appearance
of substantial modifications of the inflow pattern due to
an increased preload. The wake vortex detaches from
the valve at later times, presents increased intensity and
reduced propagation velocity, and stagnates longer near
the apex. From the physiopathologic point of view, the
fluid stagnation may be related to the occurrence of
apical thrombosis that frequently complicates dilated
cardiomyopathy, particularly when an ischaemic heart
disease causes an abnormal kinematic behaviour of the
apical walls.
A decrease of the propagation velocity has been
recently validated as a reliable index of abnormal
ventricular filling due to diastolic dysfunction of the
left ventricle (Brun et al., 1992; Stugaard et al., 1994;
Garcia et al., 1998). In the present work, the propagation velocity values are calculated in correspondence of
the vortex travelling velocity. Usually cardiologists are
not able to recognise the vortex pattern from unprocessed M-mode colour, and the flow propagation
velocity is computed as the slope of the initial early
B. Baccani et al. / Journal of Biomechanics 35 (2002) 665–671
filling trace when the vortex is still attached to the mitral
valve. For this reason, much higher values of velocity
propagation are typically reported, e.g. 0:570:1 (Garcia
et al., 1998). The present M-mode pattern shows an
initial almost vertical trace, a behaviour also observable
in the previously cited experimental and numerical
findings (Steen and Steen, 1994; Vierendeels et al.,
2000). A possible explanation can be imputable to the
assumption of a fixed mitral geometry which does not
take into account the valve opening dynamics which
surely influences the initial acceleration phase. The
reliability of this hypothesis is testified by the strict
relation between the mitral valve opening speed and the
flow propagation velocity (Laiken et al., 1979).
The axisymmetric assumption is a limitation of the
present study, which rules out the three-dimensional
vortex instability and produces a more persistent vortex
wake mainly dissipated by viscous decay only. The
results here reported represent a preliminary study to
support the physical interpretation of phenomena
observed in the clinical practice, and to complete the
physiopathology characterisation derived from the
available diagnostic instruments. A three-dimensional
numerical modelling of the flow is now in progress to
reproduce the whole heart cycle by including the lateral,
aortic, outflow.
References
Baccani, B., Domenichini, F., Pedrizzetti, G., 2002. Vortex dynamics
in a model left ventricle during filling. Submitted for publication.
Bellhouse, B.J., 1972. Fluid mechanics of a model mitral valve and left
ventricle. Cardiovasc Research 6, 199–210.
Brun, P., Tribouilloy, C., Duval, A.M., Iserin, L., Meguira, A., Pelle,
G., Dubois-Rande, J.L., 1992. Left ventricular flow propagation
during early filling is related to wall relaxation: a color M-mode
Doppler analysis. Journal of the American College of Cardiology
20, 420–432.
Firstenberg, M.S., Vandervoort, P.M., Greenberg, N.L., Smedira,
N.G., Mccarthy, P.M., Garcia, M.J., Thomas, J.D., 2000.
Noninvasive estimation of transmitral pressure drop across the
normal mitral valve in humans: importance of convective and
inertial forces during left ventricular filling. Journal of the
American College of Cardiology 36, 1942–1949.
Garcia, M.J., Thomas, J.D., Klein, A.L., 1998. New Doppler
echocardiographic applications for the study of diastolic function.
Journal of the American College of Cardiology 32, 865–875.
Kaji, S., Yang, P.C., Kerr, A.B., Tang, W.H.W., Meyer, C.H.,
Macovski, A., Pauly, J.M., Nishimura, D.G., Hu, B.S., 2001.
Rapid evaluation of left ventricular volume and mass without
breath-holding using real-time interactive cardiac magnetic resonance imaging system. Journal of the American College of
Cardiology 38, 527–533.
671
Kilner, P.J., Yang, G.Z., Wilkes, A.J., Mohiaddin, R.H., Firmin,
D.N., Yacoub, M.H., 2000. Asymmetric redirection of flow
through the heart. Nature 404, 759–761.
Kim, W.Y., Bisgaard, T., Nielsen, S.L., Poulsen, J.K., Pedersen, E.M.,
Hasenkam, J.M., Yoganathan, A.P., 1994. Two-dimensional mitral
flow velocity profiles in pig models using epicardial echo Doppler
cardiography. Journal of the American College of Cardiology 24,
532–545.
Kim, W.Y., Walker, P.G., Pedersen, E.M., Poulsen, J.K., Oyre, S.,
Houlind, K., Yoganathan, A.P., 1995. Left ventricular blood flow
patterns in normal subjects: a quantitative analysis by threedimensional magnetic resonance velocity mapping. Journal of the
American College of Cardiology 26, 224–238.
Laiken, S.L., Johnson, A.D., Bhargava, V., Rigo, P., 1979. Instantaneous transmitral blood flow and anterior mitral leaflet motion in
man. Circulation 59, 476–482.
Lemmon, J.D., Yoganathan, A.P., 2000. Three-dimensional computational model of left heart diastolic function with fluid-structure
interaction. Journal of Biomechanical Engineering 122, 109–117.
Mandinov, L., Eberli, F.R., Seiler, C., Hess, O.M., 2000. Review:
Diastolic heart failure. Cardiovascular Research 45, 813–825.
Morse, P.M., Feshbach, H., 1953. Methods of Theoretical Physics.
McGraw-Hill, New York.
Pedrizzetti, G., 1996. Unsteady tube flow over an expansion. Journal
of Fluid Mechanics 310, 89–111.
Pullin, D.I., 1978. The large-scale structure of unsteady self-similar
rolled-up vortex sheets. Journal of Fluid Mechanics 88, 401–430.
Reul, H., Talukder, N., Muller, W., 1981. Fluid mechanics of the
natural mitral valve. Journal of Biomechanics 14, 361–372.
Saffman, P.G., 1992. Vortex Dynamics. Cambridge University Press,
Cambridge.
Steen, T., Steen, S., 1994. Filling of a model left ventricle studied by
colour M mode Doppler. Cardiovascular Research 28, 1821–1827.
. C., Ihlen, H., Smiseth, O.A., 1994. Intracavitary
Stugaard, M., Risoe,
filling pattern in the failing left ventricle assessed by color M-mode
Doppler echocardiography. Journal of the American College of
Cardiology 24, 663–670.
Takatsuji, H., Mikami, T., Urasawa, K., Teranishi, J.I., Onozuka, H.,
Takagi, C., Makita, Y., Matsuo, H., Kusuoka, H., Kitabatake, A.,
1997. A new approach for evaluation of left ventricular diastolic
function: spatial and temporal analysis of ventricular filling flow
propagation by color M-Mode Doppler echocardiography. Journal
of the American College of Cardiology 27, 365–371.
Tonti, G., Pedrizzetti, G., Trambaiolo, P., Salustri, A., 2001. Space
and time dependency of inertial and convective contribution to the
transmitral pressure drop during ventricular filling. Journal of the
American College of Cardiology 38 (1), 290–291.
van Dijk, P., 1984. Direct cardiac NMR imaging of heart wall and
blood flow velocity. Journal of Computer Assisted Tomography 8,
429–436.
Vierendeels, J.A., Verdonck, P.R., Dick, E., 1997. Intraventricular
pressure gradient and the role of pressure wave propagation.
Journal of Cardiovascular Diagnosis and Procedures 14, 147–152.
Vierendeels, J.A., Riemslagh, K., Dick, E., Verdonck, P.R., 2000.
Computer simulation of intraventricular flow and pressure during
diastole. Journal of Biomechanical Engineering 122, 667–674.
Wieting, D.W., Stripling, T.E., 1984. Dynamics and fluid dynamics of
the mitral valve. In: Duran, C., Angell, W.W., Johnson, A.D.,
Oury, J.H. (Eds.), Recent Progress in Mitral Valve Disease.
Butterworths, London, pp. 13–46.