Recurrent shoulder dislocations secondary to coracoid process
advertisement

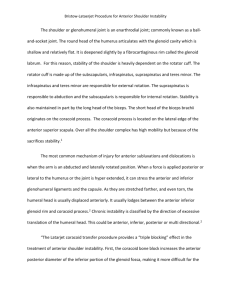
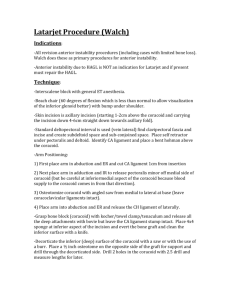
Journal of Orthopaedic Surgery 2012;20(1):121-5 Recurrent shoulder dislocations secondary to coracoid process fracture: a case report Hitesh Lal,1 Pankaj Bansal,2 Vinod Kumar Sabharwal,1 Lalrin Mawia,1 Deepak Mittal1 Department of orthopaedics, Postgraduate Institute of Medical Education & Research, Dr. Ram Manohar Lohia Hospital, New Delhi, India 2 BL Kapur Hospital, New Delhi, India 1 INTRODUCTION ABSTRACT Coracoid process fracture is easily missed in recurrent anterior shoulder dislocation. We report one such case in a 48-year-old man. Radiology revealed the Bankart lesion and the Hill-Sachs lesion only; the coracoid process fracture was discovered intra-operatively. The anatomy of the shoulder was restored by fixing the fragment to its scapular remnant with a 4-mm cannulated cancellous screw. The tip and the proximal fragment were reamed before inserting the screw. This fragment was routed with attached short head of biceps and coracobrachialis through the lower one third of the subscapularis, before homing it and fixing it to the proximal coracoid fragment. This extraarticular repair resulted in less stiffness than any intra-articular procedure. At the 2-year follow-up, the patient had had no further shoulder dislocation. Key words: bone screws; fracture fixation; shoulder dislocation Coracoid process fracture is uncommon. It can be due to direct trauma or associated with dislocations of acromioclavicular and shoulder joints.1,2 It can also occur during treatment for acromioclavicular dislocations,3 as avulsion-fractures by muscle pull of the biceps and coracobracobrachialis4 and as stress fractures in trapshooter shoulders.5 Coracoid process fractures and non-unions are easily missed on radiographs,6 as they rarely cause disturbing symptoms. Only 9 cases of coracoid process fracture with shoulder instability have been reported.1,6–11 CASE REPORT In January 2009, a 48-year-old right-handed man presented with recurrent right shoulder dislocation. Eight years earlier, he had sustained injury to his shoulder when a heavy load slipped and fell behind his back. The shoulder was hyper-abducted and -extended, as he was throwing the load in an overhead position. The load slipped behind his back Address correspondence and reprint requests to: Dr Pankaj Bansal, C-11 (first floor), Vikram Nagar, Kotla, Delhi, 02, India. E-mail: bansalpankajj@gmail.com Journal of Orthopaedic Surgery 122 H Lal et al. and added an element of external rotation, which led to anterior dislocation of the shoulder. He felt pain immediately and could not move his shoulder. He underwent closed reduction and immobilisation elsewhere and had an uneventful recovery. Two years later, he sustained another dislocation while holding an overhead bar in a bus when the bus suddenly braked. The arm was hyper-abducted, -extended, and externally rotated. He again underwent closed reduction and immobilisation. Since then, more episodes of dislocation occurred in the past 6 years (about 3 per year); the last one was 1.5 months earlier. On examination, there was slight wasting of the anterior deltoid muscles, as the smooth rounded contour of the shoulder was lost. Bony contours of the coracoid, clavicle, acromion, scapular spine, and lateral humeral head prominence were normal. The Dugas and Hamilton ruler tests for shoulder dislocation were negative, but apprehension, anterior draw, relocation, and fulcrum tests for anterior shoulder instability were positive. Abduction and external rotation of the shoulder were restricted owing to the patient’s apprehension. There was no neurovascular deficit; axillary and suprascapular motor and sensory nerve tests were normal. The patient had no ligamentous laxity or other signs suggestive of collagen disorders. Radiographs revealed no obvious bony lesion on the scapular side, but a Hill-Sachs lesion of the humeral head was evident in full internal rotation (Fig. 1). Magnetic resonance imaging revealed anterior capsule-labral tear (Bankart lesion) with a wedge-shaped impaction along the posterolateral aspect of the humeral head (Hill-Sachs depression), but no tear was noted in the rotator cuff (Fig. 2). The patient was prepared for open Bankart repair for the Hill-Sachs lesion. The deltopectoral approach was used. After the clavipectoral fascia was incised, a small bony fragment was noted at the lower border of the subscapularis. Based on its tendon and muscle fibre direction, the fragment appeared to be a fractured coracoid process. The subscapularis underneath the retracted coracoid process was normally attached to the lesser tuberosity of the humerus. So it was decided to restore the anatomy of the shoulder by fixing the fragment to its scapular remnant with a 4-mm cannulated cancellous screw. The tip and the proximal fragment were reamed before inserting the screw. This fragment was routed with the attached short head of biceps and coracobrachialis through the lower one third of the subscapularis, before homing it and fixing it to the proximal coracoid fragment (Fig. 3). This extra-articular repair resulted in less stiffness than any intra-articular procedure. Figure 1 Preoperative radiographs showing no obvious bony lesion on the scapular side, but there is a Hill-Sachs lesion of the humeral head (arrow) in full internal rotation. At the 2-year follow-up, the patient had had no further shoulder dislocation. DISCUSSION There are 2 types of coracoid process fractures according to their relationship with the coracoclavicular ligaments.6,14,15 Type-I fractures occur behind the site of attachment of coracoclavicular ligaments (between the scapular body and the coracoclavicular ligaments) and may destroy the scapuloclavicular connection. These fractures are typically associated with additional shoulder injuries (such as acromioclavicular dislocation, fractures of the scapular spine, acromion, and/or lateral clavicle), which further destabilise both the coracoid process fracture and the scapuloclavicular connection, and disrupt the superior shoulder suspensory complex. Type-II fractures occur anteriorly/distally to the attachment of these ligaments. They are usually caused by impaction by the humeral head or avulsion by the conjoined tendon, and do not disturb the scapuloclavicular connection. Our patient probably had the type-II fracture, as it was related to avulsion but not acromioclavicular joint injury. When lifting a load, the elbow was flexed and the biceps and its concomitant short head contracted. When the weight fell over his head, the biceps stretched and the coracoid process and short biceps head avulsed and fractured. The mechanism of fracture during shoulder dislocation involves 2 aspects: (1) strong traction exerted by the attached muscles leading to avulsion and fracture, and (2) direct impact of the dislocated humeral head leading to fracture.1,16 Vol. 20 No. 1, April 2012 Recurrent shoulder dislocations secondary to coracoid process fracture 123 Figure 2 Magnetic resonance images showing an anterior capsule-labral tear (Bankart lesion) with a wedge-shaped impaction (arrow) along the posterolateral aspect of the humeral head (Hill-Sachs depression), but no tear in the rotator cuff. Figure 3 Postoperative scapular Y and Stryker notch radiographs and a computed tomographic transverse section showing fixation of the coracoid process with a screw. Coracoid process fractures are easily missed, as the symptoms are non-specific and shoulder dislocation tends to dominate the picture.13 Diagnosing such a fracture requires good clinicoradiological acumen and the use of a scapular Y view, a Stryker notch view, or an anterior oblique or axillary view of the shoulder. We missed it because: (1) The patient presented late with no previous records and radiographs. (2) Radiographs were unremarkable except for the Hill-Sachs lesion. In retrospect, a narrow tip coracoid probably indicated an associated chip fracture of the coracoid tip. The 124 H Lal et al. axillary radiograph was a lateral and not oblique view, which shows up the coracoid process fracture better.1 (3) Magnetic resonance imaging showed the Bankart and Hill-Sachs lesions only, likely owing to inadequate sections perpendicular to the fracture plane. Thus, magnetic resonance imaging appears inferior to computed tomography in diagnosing these fractures. Recurrent anterior shoulder instability was likely due to both the coracoid process non-union and the Bankart and Hill-Sachs lesions. The avulsed coracoid process fragment with its conjoined tendon was widely displaced inferiorly to the lower border of the subscapularis. This led to deficiency of the dynamic protective anterior apron (against anterior instability of the shoulder). From deep to superficial, the anterior apron of the shoulder is formed by the anterior capsule, subscapularis, and the conjoined tendons of short head of biceps and coracobrachialis.17 The conjoined tendons of short head of the biceps and coracobrachialis form the superficial and foremost layer. During hyperabduction, they also exert a dynamic protective horizontal adduction, which is a stabilising force on the shoulder. As the fragment was widely displaced, the subscapularis may have jumped/subluxated over the coracoid in an overhead abduction position. The Latarjet procedure and modified Boytchev procedures keep the subscapularis inferior to the equator of the humeral head in overhead abduction, as they are routed through it, and thus protect the shoulder from dislocation.18,19 Fixation of the coracoid process with its attached tendons (after routing through the subscapularis to reinforce the anterior wall) was effective in stabilising the shoulder. Restoration of corocoid anatomy should be sufficient to stabilise the shoulder, because of the stabilising role of the coracoid-conjoint tendon complex. Open Bankart repair for recurrent avulsed anterior inferior glenohumeral ligaments and the labrum complex is the treatment of choice. We adopted the Journal of Orthopaedic Surgery middle path of the Boytchev procedure to restore the anatomy of the coracoid process. The coracoid process was transferred through the subscapularis to its parent fragment. This extra-articular repair results in less stiffness than any intra-articular procedure like the Bankart repair. The Bankart lesion may be the primary cause or may have developed secondarily to recurrent dislocation. Open approaches achieve a low recurrent instability rate (5%),20 although the complication of subscapularis rupture may ensue.21,22 Arthroscopic repair has a lower risk of subscapularis failure and enables smaller incisions, better range of movement, and earlier return to work. Compared to the open operations, patients treated arthroscopically achieve higher functional scores postoperatively, but have a significantly increased risk of recurrent instability and dislocation (12–16%).20,23 Other studies report comparable outcomes following the extra-articular, non-anatomic Bristow-Latarjet procedure with open techniques.19 Thus, the modified extra-articular Boytchev procedure was used to fix the fractured coracoid tip to its parent by rerouting it through the subscapularis. This kept the subscapularis and conjoint tendon approximated to the anteroinferior aspect of glenohumeral joint, and thus acted as a static anterior shoulder stabilising apron. Moreover, it avoided the disadvantage of the original Boytchev procedure, wherein the coracoid is routed behind the subscapularis, thus lifting it away from the glenohumeral joint and increasing the risk of recurrent dislocation.24,25 As the coracoid fragment with its attached conjoint tendon was passed through the lower third of the subscapularis, which was kept inferior to the equator of the humeral head in overhead abduction.18,19 The pressure between the humeral head and the subscapularis tendon was increased. This enhanced proprioceptive stimuli in the subscapularis tendon and thus accelerated the protective reflex needed to prevent shoulder dislocation.26 REFERENCES 1. Garcia-Elias M, Salo JM. Non-union of a fractured coracoid process after dislocation of the shoulder. A case report. J Bone Joint Surg Br 1985;67:722–3. 2. Bernard TN Jr, Brunet ME, Haddad RJ Jr. Fractured coracoid process in acromioclavicular dislocations. Report of four cases and review of the literature. Clin Orthop Relat Res 1983;175:227–32. 3. Moneim MS, Balduini FC. Coracoid fractures as a complication of surgical treatment by coracoclavicular tape traction. A case report. Clin Orthop Relat Res 1982;168:133–5. 4. Rounds RC. Isolated fracture of the coracoid process. J Bone Joint Surg Am 1949;31:662. 5. Boyer DW Jr. Trapshooter’s shoulder: stress fracture of the coracoid process. Case report. J Bone Joint Surg Am 1975;57:862. 6. Cottias P, le Bellec Y, Jeanrot C, Imbert P, Huten D, Masmejean EH. Fractured coracoid with anterior shoulder dislocation and greater tuberosity fracture—report of a bilateral case. Acta Orthop Scand 2000;71:95–7. Vol. 20 No. 1, April 2012 Recurrent shoulder dislocations secondary to coracoid process fracture 125 7. Saragaglia D, Picard F, Gerard P, Tourne Y, Leroy JM. Anterior instability of the shoulder associated with fracture of the coracoid process. Apropos of 3 cases [in French]. Rev Chir Orthop Reparatrice Appar Mot 1994;80:651–5. 8. Subramanian AS, Khalik MA, Shah MM. Isolated fracture of the coracoid process associated with unstable shoulder. ANZ J Surg 2007;77:188–9. 9. Kalicke T, Andereya S, Gekle J, Muller EJ, Muhr G. Coracoid pseudarthrosis caused by anterior shoulder dislocation with concomitant coracoid fracture [in German]. Unfallchirurg 2002;105:843–4. 10. Goodier D, Maffulli N, Good CJ. Coracoid process and greater tuberosity fracture in unreduced shoulder dislocation. Injury 1994;25:113–6. 11. Wong-Chung J, Quinlan W. Fractured coracoid process preventing closed reduction of anterior dislocation of the shoulder. Injury 1989;20:296–7. 12. Benton J, Nelson C. Avulsion of the coracoid process in an athlete. Report of a case. J Bone Joint Surg Am 1971;53:356–8. 13. Zilberman Z, Rejovitzky R. Fracture of the coracoid process of the scapula. Injury 1981;13:203–6. 14. Ogawa K, Yoshida A, Takahashi M, Ui M. Fractures of the coracoid process. J Bone Joint Surg Br 1997;79:17–9. 15. Thomas K, Ng VY, Bishop J. Nonoperative management of a sagittal coracoid fracture with a concomitant acromioclavicular joint separation. Int J Shoulder Surg 2010;4:44–7. 16. Benchetrit E, Friedman B. Fracture of the coracoid process associated with subglenoid dislocation of the shoulder. A case report. J Bone Joint Surg Am 1979;61:295–6. 17. Jiang LS, Cui YM, Zhou ZD, Dai LY. Stabilizing effect of the transferred conjoined tendon on shoulder stability. Knee Surg Sports Traumatol Arthrosc 2007;15:800–5. 18. Dalsgaard HL, Gothgen CB, Hoogmartens MJ. The Boytchev procedure for recurrent anterior dislocation of the shoulder. A controversial technique. Acta Orthop Belg 2000;66:248–50. 19. Matthes G, Horvath V, Seifert J, Ptok H, Stengel D, Schmucker U, et al. Oldie but goldie: Bristow-Latarjet procedure for anterior shoulder instability. J Orthop Surg (Hong Kong) 2007;15:4–8. 20. Eyres KS, Brooks A, Stanley D. Fractures of the coracoid process. J Bone Joint Surg Br 1995;77:425–8. 20. Lenters TR, Franta AK, Wolf FM, Leopold SS, Matsen FA 3rd. Arthroscopic compared with open repairs for recurrent anterior shoulder instability. A systematic review and meta-analysis of the literature. J Bone Joint Surg Am 2007;89:244–54. 21. Bottoni CR, Smith EL, Berkowitz MJ, Towle RB, Moore JH. Arthroscopic versus open shoulder stabilization for recurrent anterior instability: a prospective randomized clinical trial. Am J Sports Med 2006;34:1730–7. 22. Scheibel M, Tsynman A, Magosch P, Schroeder RJ, Habermeyer P. Postoperative subscapularis muscle insufficiency after primary and revision open shoulder stabilization. Am J Sports Med 2006;34:1586–93. 23. Cooney A, Sinha S, Craig Campbell A. Twelve years’ experience of the mini-Bankart repair for recurrent anterior dislocation of the shoulder. Int J Shoulder Surg 2009;3:46–8. 24. Ha’Eri GB. Boytchev procedure for the treatment of anterior shoulder instability. Clin Orthop Relat Res 1986;206:196–201. 25. Chatterjee ND, Nath C, Pal AK, Baksi DP. Modified Boytchev procedure for the treatment of recurrent anterior dislocation of the shoulder. Int Orthop 2002;26:7–9. 26. Shibata Y, Honjo N, Shinoda T, Kumano T, Naito M. Pressure between the humeral head and the subscapularis tendon after the modified Boytchev procedure. J Shoulder Elbow Surg 2004;13:170–3.