fractures of the coracoid process
advertisement

FRACTURES
K. S. EYRES.
Fivin
the
OF
A. BROOKS,
Northern
THE
0.
CORACOID
STAN1.EY
General
Sheffield,
Hospital,
England
We have reviewed
12 fractures
of the coracoid
In two of these
patients
the fracture
extended
body
of the scapula
and
PROCESS
resulted
process.
into the
in displacement
of the
(Wolf
reported
The
upper
et al 1976:
glenoid
Ishizuki
fossa
et al 1981).
and
the
upper
scapular
border
acromioclavicular
and
glenohumeral
dislocations
or
fractures
of the clavicle
and the acromion.
Two patients
required
internal
fixation
to restore
congruence
of the
develop
from the same epiphysis,
which
is separate
from
the main body
of the scapula.
A force
directed
into the
upper
glenoid
may therefore
cause
a transverse
fracture
which
extends
through
the physeal
scar to involve
the
superior
border
of the scapula,
the type-Ill
fractures
of the
glenoid;
glenoid
fossa
coracoid
glenoid,
process
and the
and force sufficient
glenoid.
In
the
some
cases,
others
there
were
were
treated
associated
conservatively
with
success.
We
which
J Bone
present
a new
helps in their
Joint
Received
Surg
16 Ma
classification
management.
fBr]
1995:77-B:425-8.
/994:
Accepted
of coracoid
fractures
may
13 Septeniher
also
of
cause
Goss
stress
the
potential
trauma
(Boyer
1975; Sandrock
1975; Froimson
1978) or by
avulsion,
either
by the coraco-clavicular
ligaments
during
an acromioclavicular
dislocation
(Benton
and Nelson
1971;
Protass,
Stanipfli
and Osmer
1975; Smith
1975; Wolf, Shoji
and Chuinard
1976;
Montgomery
and Loyd
1977: Lasda
and Murray
1978; Ishizuki
et al 1981) or by violent
contraction
of the attached
cases have been reported
muscles
(Rounds
I 949).
of fracture
of the coracoid
during
dislocation
of the shoulder
(Benchetrit
man 1979; Wong-Pack,
Bobechko
and Becker
may
impede
joint
reduction
(Wong-Chung
1989)
and be associated
with
(MartIn-Herrero,
RodrIguez-Merchan
nez 1990; Baccarani,
Porcellini
Isolated
process
and Fried1980). This
and Quinlan
a fracture
of the clavicle
and Munuera-MartIand Brunetti
1993).
Fractures
are most common
at the base of the coracoid,
but injuries
have been described
to the distal half (Benton
and Nelson
197 1) and through
the coracoid
epiphysis
(Montgomery
and Loyd 1977). Avulsion
injuries
extending
into the superior
body
of the scapula
have
also been
fracture
experience
severity
extend
into the scapula
pose a new classification
Fractures
of the coracoid
are uncommon,
occurring
in
about 2% to 5% of all scapular
fractures
(Wilber
and Evans
1977; Ada and Miller
1991).
They
are caused
by direct
PATIENTS
AND
of
Correspondence
should
be sent
©1995
British
Editorial
Society
0301 -620X195/3972
$2.(X)
VOL.
77-B,
No. 3. MAY
1995
to Mr
D. Stanley.
of Bone
and
Joint
Surgery
the
coracoid
and displace
of fractures
(MartIn-
fractures
and
of its base
which
the glenoid.
We proinvolving
the coracoid
METHODS
From
1989 to 1993, 12 patients
were treated
with fractures
of the coracoid
process.
There were eight men of mean age
3 1 years (23 to 46) and four women
of mean age 4 1 years
(27 to 85). The injuries
were
caused
front or side of the shoulder
and a road-traffic
accident
included
dislocation
patients,
fracture
patient
of the acromioclavicular
bone scan for unexplained
Nine patients
(75%)
sling,
them
by direct
trauma
in two patients,
a fall
in three.
Associated
joint
to the
in seven
injuries
in three
and in one patient
each glenohumeral
dislocation,
of the acromion
and fracture
of the clavicle.
In one
(case 5), the diagnosis
was made from an isotope
analgesia
regained
pain.
were managed
with
a broad
arm
and early
shoulder
mobilisation;
eight of
normal
shoulder
function,
but the other was
an elderly
patient
who had abduction
restricted
to 900. One
patient
required
open
reduction
of a dislocated
shoulder
because
the fractured
base of the coracoid
impeded
closed
reduction
and required
screw fixation.
The management
of
patients
anterolateral
A discrete
Road.
both
of the glenoid
of fractures
is described
below.
Case 1. A 27-year-old
woman
her left shoulder
during
an
Henries
displaces
articular
surface
of the
to fracture
the coracoid
process.
three
K. S. Eyres,
FRCS
Orth, FRCS,
Senior
Registrar
A. Brookes,
MB ChB, Senior
House
Officer
D. Stanley,
FRCS.
Consultant
Orthopaedic
Surgeon
Department
of Orthopaedics,
Northern
General
Hospital.
Sheffield
55 7AU,
UK.
This
superior
enough
a displaced
Herrero
et al I 990).
We describe
our
1994
(1992).
der,
her
pain
tender
in a grossly
mass was
acromioclavicular
sustained
repeated
blows on
assault
and presented
with
swollen
palpable
joint
was
and bruised
shoulder.
anterior
to the shouldislocated
but
reduci-
ble and she had hypoaesthesia
in the distribution
of the
axillary
nerve.
Anteroposterior
and scapular
radiographs
showed
a displaced
fracture
at the base of the coracoid
which
extended
into the glenoid
fossa. There
was also an
425
426
K. S. EYRES.
A. BRoOKS.
D. STANI.EY
Fig. I
Fig. 2
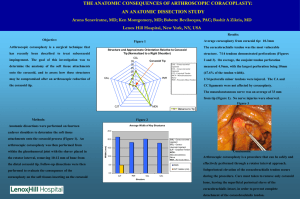
Figure
1 - An anteroposterior
view shows
a coracoid
fracture.
which
was more
I ). Extension
into the glenoid
is seen clearly. An acroniioclavicular
separation
(arrow).
Figure
2 - CT confirms
the intra-anticular
extension
of the fracture.
undisplaced
views
and
fracture
fracture
of the acromion
CT showed
the displacement
more
distinctly
reconstructions
did
not
2),
(Fig.
show
the
(Fig.
and
but
1 ). Coracoid
extent
of the
three-dimensional
fracture
lines
clearly.
Figure
(case
3
-
A fracture
4
2). Figure
of the
-
CT
coracoid
process
confirms
involvement
otis
has
hceii
the X-ray
re(luced.
and
when
but after accurate
had been achieved
35
IflIfl
Gentle
The coracoid
fracture
was exposed
through
an anterior
deltopectoral
approach.
The coracoacromial
and coracoclavicular
ligaments
were intact.
A small
transverse
mcision in subscapularis
allowed
inspection
of a transverse
fracture
line across
the glenoid
between
its upper
and
middle
thirds.
Traction
on the arm displaced
the fracture,
Fig.
oh
AO
heant
there
sva
tilted
45
is an undisplaced
reduction
of the intra-articular
the coracoid
fracture
was
small-fragment
passive
cancellous
and active
shoulder
after three weeks.
The axillary
there was no evidence
of injury
Full shoulder
movements
were
component
fixed
by
two
screws.
exercises
were
started
Case
2. A 23-year-old
male
pedestrian
was
rendered
unconscious
by a direct
blow
to the head
and
the
left
shoulder
after colliding
with a bus. On admission
he was
Fig.
body
direction
(case
of the acromion
nerve palsy recovered
and
to the stlprascapular
nerve.
restored
within
six weeks.
3
extends
into the superior
of the glenoid
fossa.
in a cephalic
fracture
of the scapula
and
the glenoid.
There
Till
JOLRNAI.
is
an asoci:itcd
(II
ItONt
4
fracture
.\Nt)
of the
JOINT
clavicle
SURGERY
FRACTURES
OF THE
CORACOID
PROCESS
of the scapula
The clavicle
ments
full
427
taking care not to penetrate
the glenoid
was fixed with a six-hole
plate. Active
started
range
after
of
three
weeks
shoulder
of passive
movement
was
fossa.
move-
exercises
and
regained
by
a
nine
weeks.
Case
3. A 17-year-old
when
it overturned
man
falling
was driving
on top of him
right arm. Among
his other injuries
was
the base of his right coracoid
process,
scapular
view (Fig.
a broad-arm
sling,
shoulder
as comfort
and
or absence
Fractures
of the coracoid
into the five types
shown
in
as A or B according
to the
respectively
of associated
the acromioclavicular
joint which
affect
On our classification,
type-I,
type-Il
tures
are probably
caused
by traction
attached
severe.
when
..,
tendons
or ligaments.
They
probably
result
the scapula
is forced
anterior
and
lateral
injuries
to
scapular
stability.
and type-Ill
fracforces
from
the
Types
IV and V are more
from shearing
forces
either
inwards
by a lateral
humeral
head or when
the clavicle
makes
with the coracoid,
as is sometimes
indicated
on the
using
the
permitted.
mechanisms.
can usefully
be subdivided
Figure
6 with subgrouping
presence
a fracture
through
well shown
on a
5). It was treated
conservatively,
and he was allowed
to mobilise
actively
Classification
a fork-lift
truck
and trapping
his
aspects
blow
on the
direct
contact
by contusions
of the shoulder.
Fig. 5
A scapular
view clearly
of the coracoid
process
conscious
obvious
with
fracture
shows
a fracture
(case 3).
a Glasgow
of the
coma
middle
neurovascular
injury.
Radiographs
clavicular
fracture
and a fracture
through
the
DISCUSSION
base
scale of 15 and
of the clavicle,
had
but
an
no
showed
the displaced
of the coracoid
extending
into the superior
border
of the scapula
and the glenoid
(Fig.
3). CT of the shoulder
confirmed
the intra-articular
extension of the coracoid
fracture
(Fig. 4), but three-dimensional
reconstruction
The
approach
articular
fixed
screw
was
fracture
again
was
unhelpful.
exposed
and the glenohumeral
fracture
was reduced
using
placed
through
a
joint inspected.
and the coracoid
deltopectoral
The intrafracture
was
a single
large-fragment
35 mm
cancellous
through
the base of the coracoid
into the body
Most
reports
cases,
and
of coracoid
we
believe
fractures
that
we
have
have
been
collected
of
one
isolated
of the
largest
series to be published
in English.
Coracoid
fractures
are included
in various
classifications
of scapular
fractures,
such as the type-IC
fractures
of Ada and Miller
( 199 1 ). We
propose
a more
precise
classification
to help to identify
patterns
and
assist
rational
management.
Only
conservative
treatment
is needed
for
although
internal
fixation
is often recommended
when
there is an associated
acromioclavicular
Pseudorupture
the
muscles
1956)
and
impede
fractures
of the
may
damage
rotator
produce
to the
cuff
due
temporary
suprascapular
cuff function
and affect
make
a full functional
most cases
especially
separation.
to haemorrhage
paralysis
nerve
diagnosis.
recovery,
into
(Neviaser
may also
Most
scapular
but when
the
TPe,)JEI”7
TYPel7
Fig. 6
Classification
of coracoid
fractures:
type I, tip or epiphyseal
involved;
type 5. extension
into the glenoid
fossa.
The suffix
ligamentous
connections
to the scapula.
VOL.
77-B.
No.
3. MAY
1995
fracture;
type 2, mid-process;
A or B can be used to record
type 3, basal
the presence
fracture:
or absence
type 4, superior
body of scapula
of damage
to the clavicle
or its
428
K. S. EYRES.
glenoid,
may
acromion
be poor
Evans
We
or coracoid
results
1977).
suggest
fractures
that
of types
process
in up to 90%
I, II and
is involved,
of patients
undisplaced
there
(Wilber
fractures
III can
A. BROOKS,
and
and
displaced
be successfully
treated
D. STANLEY
infrascapular
show
bone
the extent
our cases
presumably
although
because
cuts
3 mm
with
(Wilber
and
Evans
of the intra-articular
1977).
three-dimensional
of the thickness
table
movement)
and
of the
been
use
of screws
described
to stabilise
(Wong-Chung
would
identified
patient.
have
an
fracture
has
1989).
We
a coracoid
and
of
the orientation
and Broughton
Haydar
1991).
The
to
in two
failed,
(4 mm
fracture
lines
to the scanner.
Finer
slices
enhanced
the image.
An isotope
bone scan
unsuspected
coracoid
fracture
in one elderly
and
for
helped
reconstruction
of the slices
conservatively
as agreed
by others
(Urist
1946;
Rounds
1949;
Boyer
1975; Protass
et al 1975; Montgomery
and
Loyd
1977; Froimson
1978; Lasda
and Murray
1978; Carr
1989; MartIn-Herrero
et al 1990; Gill
We recommend
surgical
stabilisation
CT
involvement
Quinlan
type-IV
and type-V
fractures
which involve
the base of the
coracoid,
and either the body of the scapula
or the glenoid
fossa.
Other indications
for surgery
are dissociation
of the
found that a single
large-fragment
cancellous
screw,
inserted through
the mid-part
of the coracoid
process,
was useful
in aiding reduction
before
fixation,
and helped
to avoid risk
scapula
and clavicle,
caused
by acromioclavicular
dislocation or clavicular
fracture
(Barentsz
and Driessen
1989) and
obstruction
to the shoulder
reduction
due to the coracoid
to the suprascapular
verse incision
in the
isation
of the glenoid
fragment
Careful
intra-articular
(Wong-Chung
preoperative
any intra-articular
cated fracture.
The
and Quinlan
assessment
extension
coracoid
of
view
1989).
is essential
neurovascular
subscapularis
to ensure
component
bundle.
A small
transwill allow good visualadequate
reduction
of the
of the
fracture.
to identify
an apparently
uncomplidirected
45#{176}
in a cephalic
direction
gives
clearer
views
than
plain
posteroanterior
radiographs
(Froimson
1978).
Fractures
of the coracoid
must be distinguished
from anatomical
variations
such as
the persistence
of the ossification
centre
known
as the
The authors
wish to thank the Departments
of Radiology
in Sheffield
and
Cambridge,
Mr Cam (Oxford),
the consultants
at the Northern
General
Hospital
and Royal
Hallamshire
Hospital.
Sheffield
and the Medical
Illustration
Departments
of the Royal
Hallamshire
Hospital
for their
contributions.
No benefits
in any form have been received
or will be received
from a
commercial
party
related
directly
or indirectly
to the subject
of this
article.
REFERENCES
Ada
JR,
Orthop
Miller
ME.
Scapular
fractures:
analysis
of
1 1 3 cases.
C/in
1991:269:174-80.
Baccarani
G, Porcellini
G, Brunetti
E. Fracture
of the coracoid
process
associated
with fracture
of the clavicle:
description
of a rare case. Chir
Organi
Mov 1993:78:49-51.
Barentsz
ill,
Driessen
APPM.
Fracture
of the coracoid
scapula
with acromioclavicular
separation:
case report
the literature.
Acta Orthop
Be/g
1989;55:499-503.
process
of the
and review
of
of
i, Nelson
a case.
Boyer
DW
process:
Carr
AJ,
fracture
Froimson
Gill
C. Avulsion
J Bone
Jr.
Surg
Trapshooter’s
case
report.
Broughton
of the
Al.
of the coracoid
Joint
TP
Fractures
1992;74-A:299-305.
process.
of the
J.shizuki
the
NA, Murray
associated
with
a case
report
1978; 134:222-4.
of
report
coracoid
associated
with
l989;29:l25-6.
process
of the
of the coracoid
cavity.
the
1975:57-A:862.
dislocation
J Trauma
coracoid
glenoid
in an athlete:
fracture
[Am]
J
Smith
DM. Coracoid
tion: a case report.
Joint
report.
Surg
[Am]
I, Isobe Y, et aL Avulsion
scapula:
report
of five cases.
DG
Fracture
acromioclavicular
and
review
separation
dislocation:
of
the
fracture
of the superior
J Bone
Joint Surg [Am]
of
the coracoid
process
conservative
treatment:
literature.
C/in
Orthop
of degenerative
Osmer
separation.
JC.
Coracoid
Radio/ogv
of
the
shoulder
lesions.
process
fracture
1975:116:61-4.
of the coracoid
Sandrock
AR. Stress
fracture
Radio/ogv
1975:117:274.
J Bone
a case
FV,
Rounds
RC. Isolated
fracture
[Am]
l949:31-A:662-3.
Urist
scapula.
process:
Bone
ii, Stampfli
in acromioclavicular
C, Munuera-MartInez
presentation
of seven
cases
1990:30:1597-9.
process.
coracoid
diagnosis
J Bone
process
of
Bu//
Joint
the
fracture
associated
with acromioclavicular
Cliii Orthop
1975:108:165-7.
Wilber
MC, Evans
EB. Fractures
of the
cases
and
review
of the
literature.
1977;59-A:358-62.
AW, Shoji
H, Chuinard
process:
a case report
and
lAin]
1976;58-A:423-4.
Wong-Chung
i, Quinlan
closed
reduction
of
1989;20:296-7.
WK,
shoulder
RG.
review
W.
anterior
Bobechko
dislocation.
THE
PE,
scapula:
J Bone
Surg
scapula.
disloca-
MR.
Complete
dislocations
of the acromioclavicular
joint:
nature
of the traumatic
lesion
and effective
methods
of treatment
an analysis
of forty-one
cases.
J Bone Joint Surg 1946:28:813-37.
Wong-Pack
anterior
L
and
RD. Avulsion
fracture
of the coracoid
epiphysis
separation:
report
of two cases in adolescents
literature.
J Bone
Joint
Surg
[Am]
1977:59-A:
JS. Pathological
review
Joint Dis l956;17:297-304.
Protass
Wolf
M, Yamaura
border
of the
1981 ;63-A:820.
Lasda
of
Surg
Joint
Joint Surg lAin]
1978:60-A:710-1.
JF, Haydar
A. Isolated
injury
J Trauma
199l;31:l696-7.
Goss
stress
Acromioclavicular
coracoid
Fracture
process
associated
Surg [A,n]
197 l;53-A:356-8.
shoulder:
J Bone
NS
[Am]
Montgomery
SP, Loyd
with acromioclavicular
and review
of the
963-5.
Neviaser
Hosp
Benchetrit
E, Friedman
B. Fracture
of the coracoid
process
with subglenoid
dislocation
of the shoulder.
J Bone Joint
1979;61-A:295-6.
Benton
MartIn-Herrero
T, RodrIguez-Merchan
Fractures
of the coracoid
process:
review
of the literature.
J Trauma
the
with
an analysis
of forty
Joint
Surg
[Am]
Unusual
fractures
of the coracoid
of the literature.
J Bone Joint Surg
Fractured
coracoid
dislocation
of
the
process
preventing
shoulder.
Injury
Becker
EJ. Fractured
coracoid
J Can Assoc
Radio!
I 980:31:278-9.
JOURNAL
OF BONE
AND
JOINT
with
SURGERY