DOWNLOAD and VIEW research summary and an in-depth
advertisement

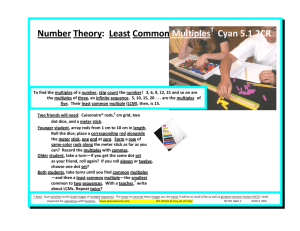
MEDICAL BREAKTHROUGHS RESEARCH SUMMARY TOPIC: REPORT: GROWING RODS FOR SCOLIOSIS MB #3985 BACKGROUND: Scoliosis is an abnormal curve or bend in the spine that affects two percent of women and 0.5 percent of men worldwide. Over 80 percent of scoliosis cases have no known cause and are commonly found in otherwise healthy patients. The condition can run in families, especially those with a history of spina bifida, muscular dystrophy and cerebral palsy. There are three types of curves: a C-shape (levoscoliosis), a reverse C-shape (dextroscoliosis), and Sshape. Children and teens with untreated scoliosis can develop a more severe bend due to their skeleton’s fast rate of growth. Usually, doctors recommend seeking treatment for scoliosis if the curvature is greater than 20 degrees. (Source: http://www.spinehealth.com/conditions/scoliosis/scoliosis-what-you-need-know, http://iscoliosis.com/causes.html) TREATMENTS: Before a treatment plan can be determined, the patient’s condition needs to be evaluated by a doctor. The patients’ skeletal age and maturity and the degree of the curvature are the most important factors in deciding on whether a brace or surgery is necessary. For patients with small curvatures, the doctor may decide that an intervention is not needed and the condition is monitored on a regular basis to measure and evaluate the growth of the child. An orthopedic surgeon will take X-rays of the spine and will monitor if the curve increases. For patients in their adolescence and a curve of over 25 degrees, they are fitted with a back brace to stop the growth of the curvature. The brace will not fix the curve or cause any changes in the shape of the spine. More severe curvatures in children or adults require surgery, and can correct the condition by about 50 percent. Orthopedic surgeons can choose to enter through the back (posterior) or through the front (anterior) of the patient. (Source: http://www.spinehealth.com/conditions/scoliosis/scoliosis-surgery, http://www.spinehealth.com/conditions/scoliosis/scoliosis-treatment) NEW TECHNOLOGY: Gregory Mencio, MD, Pediatric Orthopedic Surgeon and Professor and Chief of Pediatric Orthopedics at Monroe Carell Jr Children’s Hospital at Vanderbilt University implanted magnetic growing rods in the first patient at Vanderbilt. The procedure uses MAGEC (magnetic expansion control) rods that are able to be non-invasively lengthened using an external remote. The rods are intended for patients under the age of 10 with a curvature of 30 degrees or more. Patients in pre-adolescence are subject to more risks and surgeries with other growing rod procedures. With the MAGEC rods, the patient only has X-rays to monitor the spine and lengthening and because the rods are controlled remotely, there are fewer surgeries. (Source: Gregory Mencio, MD, http://ellipse-tech.com/wpcontent/uploads/2014/06/magecproduct.pdf) FOR MORE INFORMATION ON THIS REPORT, PLEASE CONTACT: Craig Boerner Media Director, National News Director Vanderbilt University Medical Center 615-322-4747 Craig.boerner@vanderbilt.edu If this story or any other Ivanhoe story has impacted your life or prompted you or someone you know to seek or change treatments, please let us know by contacting Marjorie Bekaert Thomas at mthomas@ivanhoe.com Gregory Mencio, M.D., Pediatric Orthopedic Surgeon at Vanderbilt University Medical Center talks about scoliosis treatment for children using growing rods. Interview conducted by Ivanhoe Broadcast News in June 2015 Let’s first talk about scoliosis in children, how many kids get this? What are some of the first signs of it and how does it affect them? Dr. Mencio: Scoliosis is very common, probably about one in 1000 to 1500 kids get it. We see a lot of kids that have small curves and we see fewer kids that have big curves that actually need to be treated. It presents usually because the parents notice a curvature, deformity or an imbalance of the spine. And the concern, of course, is that it starts as a little curve and then it can progress to a big curve and as it gets bigger, it can create some health issues. Probably the two biggest things are just the deformity issue and functional issues occasionally, like back pain, and we see it in different age groups. The most typical age group that we see it in is adolescent age children. In that group, the traditional treatments are using a brace and then, if the curves fail brace treatment and get big enough, they can be managed surgically. The problem is, in younger kids who develop scoliosis, of course we can treat them with a brace but as the curves get bigger, doing spine fusion surgery is not really a good option because their torso is short and if you correct the curve and fuse the spine you’re going to lock their torso into a relatively short height. So doing fusion surgery in young kids is really not an option. So the transition point where you can do traditional treatment for big curves in scoliosis is somewhere around 11 or 12. For kids much younger than that, we have to do other things. We have to try to preserve growth while we control the curve. Typically before growing rods, what would you do for a child who needed them? Dr. Mencio: We actually still do some of the same things, non-operative treatment is always the first line and that can be simply observation. Once the curve gets past 25 or 30 degrees, then we have to start looking at real treatment options and that would be either a brace or a cast. You’re actually going to apply and put the kids to sleep and put them in a cast that has to be changed out every three or four months. So we can do non-operative treatment in the form of either bracing or casting. Or we can do growing rods. We can actually put rods in to the spine that essentially act as an internal brace that can be lengthened as the spine and the child grows, to allow the spine to grow while still controlling the curve. Because growth is certainly one of the things that cause curves to progress, the goal is to try to control the curve, keep it from getting bigger while the kids are growing. With these growing rods, how is it beneficial for the child compared to the traditional methods? Dr. Mencio: Well, the benefit of growing rods is it allows the spine to grow until the child gets to be old enough and mature enough to have something done surgically. The benefit of the current technology that we have with these magnetically-controlled rods is that we can actually do the lengthening in the clinic rather than in the operating room. With the traditional growing rods, that is what was available up until a couple of years ago, the procedure would be to put in the growing rods at one operation and then come back six months to a year later and have another operation, all be it smaller in magnitude. But still, another operation where the child has to be put to sleep, have an incision, have the rods lengthened and the incision closed and then go home and do that again every six to nine months. So they would have the initial procedure to put the rods in and then additional individual procedures, all which require anesthesia every six to nine months to lengthen the rods until the kids got to be of an age where we could convert to a formal fusion. If you start that in a four year old, then you are targeting 10 or 11 or 12 years old as a time to do definite surgery. Twice a year, that’s probably, let’s see, my math is eight years, twice a year, that’s potentially 12 to 16 operations in that child’s lifespan. With the magnetic rods, now we have the ability to put those rods in and then, instead of going back to have a surgical procedure to lengthen the rods, we can actually do that in the office. So, the kids have their main surgery and they come to the office three or four months later, then we use an external device, a magnet, that activates the rods and elongates them and they’re done. It takes about 15 to 20 minutes. We can actually measure the length of the rods using ultrasound, so we don’t even necessarily have to do X-rays so it saves on that, but we can still do an X-ray, if need be. It’s an office visit every four months as opposed to an operative procedure every six to nine months, pretty good tradeoff. And that’s just a little less traumatizing for kids. Dr. Mencio: Sure, exactly. Are there any drawbacks to these? Dr. Mencio: Well, there are drawbacks to everything, let’s face it. But the risks of putting the rods in are the same as the risks associated with the older type of growing rods and those are just the risks associated with surgery. So you got to put the rods in and it’s got to be done appropriately. All these procedures carry a very small risk of wound healing and infection problems, that’s no different between the two techniques. The things that can go wrong with growing rods are the rods can break and the traditional rods can do that but so can the newer rods. The other thing, that’s particular to the magnetic rods, is that there is an electromagnetic device that has to function and so, in theory, that could fail, and the rods could jam. We haven’t seen that but that’s certainly a possibility. And if that were to happen, then the rods would have to be changed out or you have to revert back to the other option of growing rods. But we haven’t seen that. There have been some reports of it, so that’s the potential downside, but that’s really a manageable problem. How many of the magnet growing rods have you given to kids? Dr. Mencio: We actually just started in the last six months and, at the end of this week, we’ll have done our seventh rod. The hospital gave us permission to do a trial of five rods just to see how it went and we’ve extended it and we’re hopefully going to be able to continue offering this going forward. So what are your thoughts as a surgeon having this kind of technology? Dr. Mencio: I think it’s great. I think the clear advantage is avoiding the trips back to the ER for the kids and their families, that’s the huge benefit of this. And, as I said, it really doesn’t have a downside relative to the other technique. We’re still relatively early in our experience with it, our personal experience. But there’s international experience in some centers that were very early developers and adopters that have a little bit longer experience with it but it’s been very positive, generally speaking. In Brook’s case, can you explain what you meant about how she had a little bit of anxiety about this? Dr. Mencio: Yeah, so Brook, she’s a great kid, but she’s just like most kids. Most of them don’t like coming to the doctor’s office and she had some anxiety issues just in coming to the office, and I think certainly with her initial surgery. And, for her, having the stressors of coming in the morning, have her go through pre-op and anesthesia and have a surgery and then the post-op discomfort that goes along with any operation even if it’s a small one. But that’s a great advantage. I mean, she came back to the office to have her rods lengthened and she was terrific. You know, it was no big deal and she did great so maybe we converted her. How many more times will she have to come back to get them lengthened? Dr. Mencio: Our current protocol is about every four months. We have one day we set up so far, a rod lengthening day, and we’re going to bring the kids in on that day. So, for her, it will be every four months for the next two to three years. But just to allow her to grow and to physiologically mature to the point that we can eventually take the rods out and put new rods in. It doesn’t eliminate the need to do a definitive procedure. So when she gets to be appropriate size and age, then we’ll do that conversion. What’s the prognosis for that, if everything goes well? By the time she’s 20, is everything going to be good? Dr. Mencio: The long-term prognosis of scoliosis that’s been treated is actually very good. And it really should be no different than if she showed up as an adolescent and had her back operated on at that point. Once the curves are fused, they usually don’t progress. A small percentage of kids, who are now adults, will have some back pain related to the surgery or the rods but most do very well throughout their life and, so, long-term prognosis is good. The big thing is just bridging the time from when the kids are little until they get to be an appropriate age, that’s what we’re trying to do with this procedure. What’s the max length that they can extend? Dr. Mencio: Currently, the rods come in two lengths. There’s a 70 millimeter length and a 90 millimeter length. The longer rod will allow up to nine centimeters of lengthening and the smaller up to about seven centimeters of lengthening. That’s the carry within the magnetic portion and the size of the rod we can put in is dictated by the size of the patient and we have to have length between the end of the magnetic portion of these rods and the screws above and below. We put in the longer rod, if we can, and then that, in theory, barring any mechanical problems, will allow us up to nine centimeters of lengthening rod, which is plenty. That’s way more than we could get with the older technique, the more traditional technique of using growth rod connectors. In those, the connectors were 50, 70 and 90, so you couldn’t get quite as much length. They’d have to be changed out about every two or three times. With this, there’s potential for more lengthening with one device, barring any mechanical problems. Do these have a coating on them to prevent metal allergy? Dr. Mencio: They’re titanium and titanium is the preferred metal for spinal implants. It’s associated with a lower risk of infection. It is very rare to get metal allergies to titanium or even to stainless steel implants, but even less so to titanium implants. END OF INTERVIEW This information is intended for additional research purposes only. It is not to be used as a prescription or advice from Ivanhoe Broadcast News, Inc. or any medical professional interviewed. Ivanhoe Broadcast News, Inc. assumes no responsibility for the depth or accuracy of physician statements. Procedures or medicines apply to different people and medical factors; always consult your physician on medical matters. If you would like more information, please contact: Gregory Mencio, M.D. 1211 Medical Center Dr. Nashville, TN 37232 615-322-5000 Sign up for a free weekly e-mail on Medical Breakthroughs called First to Know by clicking here.