How to Avoid CASTI - Wheat Ridge Animal Hospital
advertisement

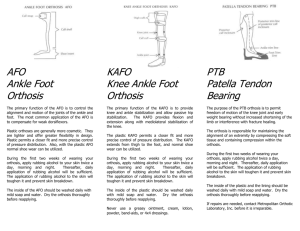
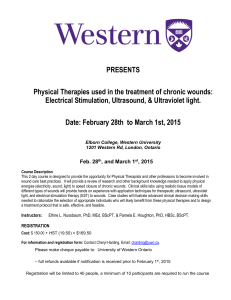
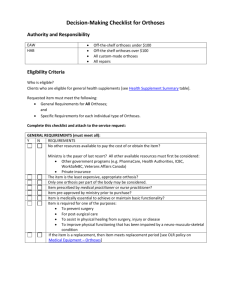
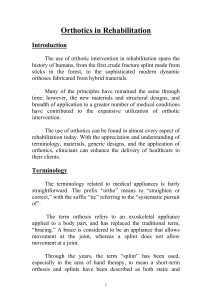
How to Avoid CASTI: Cast Associated Soft Tissue Injury Patrice M. Mich, DVM, MS, DABVP, DACVAA, DACVSMR, CCRT Types of external co-aptation External co-aptation can be generally categorized as bandage, splint, brace, and orthosis. Each of these are further divided into specific types or applications as well as different materials. It is important to understand the intended purpose in order to select the proper co-aptation. Bandage: A strip of material such as gauze used to protect, immobilize, compress, or support a wound or injured body part. Wrap (support): An elastic material used primarily for support and muscle compression; shorten a muscle’s angle of pull; reduce joint range of motion; apply compression to reduce swelling Splint: A rigid or flexible appliance for fixation of displaced or movable parts Brace: An orthopedic appliance that supports or holds a movable part of the body in correct position while allowing motion of the part. Orthosis: Any medical device attached to the body to support, align, position, prevent or correct deformity, assist weak muscles, or improve function. The term orthosis is a more correct term in that it expands the concept of bracing and more specifically defines the various clinical applications possible. Proper application can be challenging in veterinary species. Differences in patient size, coat type, injury location and severity, temperament and activity level must be considered. Attention must be paid to intended purpose and duration of use. Finally, secure attachment and alignment to the limb can be challenging; these are critical in terms of function, comfort and safety. Bandages and wraps: Advantages: variable thickness, some are reuseable, some are disposable, inexpensive, wound protection, can incorporate wound dressing materials and medications Disadvantages: must be replaced if wet; cannot support against significant increase in range of motion (e.g. carpal hyperextension); can be difficult to keep in place/properly aligned; may cause wounds or binding (pressure and friction); risk of tourniquet effect; skin irritation from repeated tape application and removal. Splints: Advantages: inexpensive; some are moldable; reuseable; provides rigid support if needed; Disadvantages: must be applied with bandage material which can become wet; not dynamizable (no articulation); distal joints unaffected by injury are immobilized (must manage iatrogenic consequences such as flexor contraction and joint capsule fibrosis); causes atrophy by virtual of fixed joint angles; can be difficult to keep in place/properly aligned; may cause pressure wounds; risk of tourniquet effect; skin irritation from repeated tape application and removal. Braces and Orthoses: Advantages: body part specific; injury specific; reuseable; provides rigid support if needed; some are dynamizable (articulated, variably articulated, or not articulated); moldable or customizable; improved retention on the limb; tape not needed (designed suspension and velcro attachment); ease of removal and re-application allows for frequent examination of injured area; can get wet; replacement parts available for some Disadvantages: more expensive; best used for longer term use (>8 weeks); can cause wounds and distal extremity swelling if not properly designed, adjusted, and monitored; no controlled clinical studies as yet available; lack of professional fabricators knowledgeable in the design, manufacture, and use of these devices for veterinary species. Use in Veterinary Rehabilitation Orthoses (braces) are a natural adjunct to rehabilitation with the ultimate goal of improved mobility, functional independence, and pain management. 1 The clinical purposes of orthosis use include 1) Maintenance or correction of body segment alignment; 2) Assistance or resistance to joint motion; 3) Axial loading of the orthosis & therefore relief of distal weight bearing force; 4) Protection against physical insult.2 A common misconception is that splints are the same as braces (orthoses) and further, that all such devices lead to disuse atrophy as a consequence of reliance on the device. This idea has lead to an incorrect and unfortunate tendency to avoid the use of mechanical appliances in both short and long term patient care. In this lecture we will explore the significant therapeutic differences and applications of splints and orthoses, and debunk the myths surrounding their use in rehabilitation. Mechanical principles of proper bandaging, splinting, and bracing The mechanical basis of splinting and bracing is the Three-Point Pressure Principle (3PPP); Properly applied the 3PPP employs a single force at the area of correction or at the area of deformity or angulation while 2 counter forces act in opposing direction, usually above and below the primary area of correction (Figure 1 and 2). Figure 1 Figure 2 The further the counter forces from the joint center the more torque and less force required to achieve alignment. Therefore, the 3PPP is also the root cause of most wounds associated with bandaging as well as splinting and bracing. The magnitude of force placed on the skeleton through soft tissue is greater the closer the contact point is to the fulcrum or corrective force (Figure 3). It is not surprising therefore that pressure wounds occur at CF1 and CF2 especially when bandages, splints or orthoses are too short. Additionally the more acute the joint angle the more force required (CRF3) to re-align the segment AND therefore since CF1 + CF2 = CRF the greater the force applied to the skin at CF1 and CF2 (Figure 4). It is not surprising then to find wounds for example at the olecranon, the accessory carpal bone/pad or the calcaneal tuberosity. Figure 3 Figure 4 Pressure must be evenly applied over the entire structure. If not wounds occur at points of increased contact. Good examples include the medial and lateral malleoli and the radial and ulnar styloids. In bandaging, splinting, or bracing accommodation must be made or these structures such that pressure above and below these points is the same as directly over these points. Several Resources are available with regard to bandaging, splinting, and bracing. 3,4,5,6 References 1 Prokop LL (2006). Upper extremity orthotics in performing artists. Phys Med Rehabil Clin N Am 17:843-852. 2 Deshales LD (2002). Upper extremity orthoses. In: CA Trombly, MV Radomski editor(s). Occupational Therapy for Physical Dysfunction. 5th ed. pp313–49. Baltimore: Lippincott, Williams & Wilkins. 3 Adamson C, Kaufmann M, Levine D, Millis DL, Marcellin-Little DJ. 2005. Assistive devices, orthotics, and prosthetics. Vet Cl N Am, 35(6): 1247-1518. 4 Swaim SF, Renberg WC, Shike KM. Small Animal Bandaging, Casting, and Splinting techniques. Wiley-Blackwell 2011. 5 Mich PM, Fair, L, Borghese I. Assistive Devices, Orthotic, Prosthetics, Bandaging in VanDyke J, Zink MC, editors: Canine Sports Medicine and Rehabilitation. Wiley Blackwell in press 6 Mich PM, Kaufmann, MW. Custom external coaptation as a pain management tool: Veterinary orthotics and prosthetics (V-OP) in Egger C, Doherty T, editors: Pain Management in Veterinary Practice. Wiley Blackwell in press