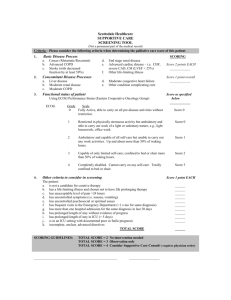
View/Open - Hasanuddin University
advertisement

1 CHAPTER I THE PROBLEM INTRODUCTION In Indonesia, in 2010 there will be around 23, 9 million older persons (9.77%) with the life expectancy 67.4 years old. It is predicted that in 2020, there will be 28, 8 million older persons people (11, 34%), with life expectancy 71.1 years old (Indonesian Statistical Bureau, 2005). In Gowa, one of the municipality in South Sulawesi, Indonesia, 5.7 % from its citizens or around 3388 is people with 65 years old and above with the life expectancy 66.2 years old (Health Profile of Gower Municipality, 2007). The data above congruent with the world trend where the number of older person population is increasing from time to time. In addition, considering the percentage of older person population in Indonesia which is more than 7%, Indonesia can be categorized as aged structure population. Increased life expectancy has resulted in increasing numbers of older persons living in the community (Sahar, 2006). To promote and maintain health among older persons, since 2009, Gowa municipality is implementing a community older persons program. Majority health workers who handle the program are nurses since the number of nurses in Gowa is 50, 37% from the total 802 health workers (Health Profile of Gowa Municipality, 2007). The nurses conduct monthly health post integration service for the older persons called Posyandu, the abbreviation of Pos Pelayanan Terpadu. Based on the observation during Posyandu implementation in Gowa municipalities, the main duties of nurses is more on medication action, they are taking the blood measurement, asking for the older 2 persons’ complaint, giving health education which mostly done individually and also giving medication. Unfortunately, instead of the number of older person’s population in Gowa municipality, though the nurses held Posyandu regularly, no data found regarding characteristic of older persons, including the most common diseases or health complaint suffered by the older persons in this municipality. The data itself is important in helping the older persons performing self-care. Since in older person’s population, they not only have high prevalence of chronic illness but also personal self-care deficiencies (Heui & Kim, 2004). Based on the self-care theory of Dorothea Orem, self-care is the practice activities that individuals initiate and performs on their own behalf in maintaining life, health and well-being. The humans are capable and willing to perform self-care. Whenever the maintenance of continuous self-care requires the use of special techniques and scientific knowledge, then nursing is required in providing the care or in designing it (Martin, 2005). Therefore, the information regarding older persons including their characteristic and common symptoms experiences is crucial to design the appropriate self-care intervention for them. Too often, nurses seek interventions to meet the needs of older persons that come from external sources rather than empowering the older persons for self-care by using their inner resources. Older persons then become passive recipients of care rather than active participants. Nurses must recognize the strengths and capabilities of older persons so that they can be responsible and active participants in rather than recipients of care. Tapping the resources of elders in their own care promotes normalcy, independence, and individuality; it also aids in reducing risks of secondary problems related to the reactions 3 of older persons to an unnecessarily imposed dependent role; and it honors their wisdom, experience, and capabilities. However, limitations to do self-care will exist if the knowledge, attitude or skills required for a self-care action are inadequate or nonexistent (Eliopoulos, 2001). Consideration of the important baseline data on characteristic of older persons as well as how the older persons do self-care, this research will address the experiences of older persons on self-care in terms of knowledge, attitude and practice in Kanjilo village, Gowa municipality. 4 STATEMENT OF THE PROBLEM To achieve the purpose and the objectives of this study, the following research question is developed: What are the nursing needs of older persons in Kanjilo Village? OBJECTIVES OF THE STUDY The purposes of this research study are to: 1. To describe the characteristics of the older persons in Gowa municipality, in terms of : a. Socio demographic characteristics b. Common symptom experiences c. Reasons for hospital consultation d. Frequency of medical/nursing consultation e. Kinds of health facility used 2. To determine the knowledge, attitude, and practices on self-care of older persons. 3. To determine the association of socio demographic factors and common symptoms experience to knowledge, attitude and practices on self-care of older persons 4. To determine the nursing needs of older persons SIGNIFICANCE OF THE STUDY The study contributes to evidence based nursing knowledge on the various components of self-care in older persons. This study is one of the first research evidence which serves as data on characteristics of older persons in Gowa municipality, since there is dearth of data about characteristics of older persons in Gowa Municipality. For nurses, 5 the result of the study is essential as the assessment data and the description of self-care practices of older persons in Kanjilo Village, Gowa municipality. In addition, this research will result the nursing need of older persons to perform maximum self-care. As for the Department of Health (DOH) of Gowa municipality, the baseline data can be used in maximizing and supporting the community older persons program which they promoting. For further research can be used as the basic for generating some hypothesis. SCOPE AND LIMITATION The study will be done in Kanjilo village, Gowa, South Sulawesi, Indonesia. The study will use 165 participants. The data from the older persons will be gathered through questionnaire to describe the characteristic of older persons as well as experiences of older persons on self-care in terms of knowledge, attitude and practice. Considering the location of studies, the findings are not a universal situation in Indonesia and therefore cannot be generalized because they do not report the thoughts of older persons in Indonesia communities with differing service accessibility. OPERATIONAL DEFINITION OF TERMS Older persons refer to individual 60 years of age and above Knowledge on self-care refers to what the older persons know regarding self-care. It will be measured by questionnaire developed by the researcher by using Orem’s theory component. The questionnaire consists of 10 statements which have 3 options: correct, incorrect and do not know options. Correct answer is given score 2, incorrect answer is 6 given 1 and do not know options is given score 0. The lowest score is 0 and the highest 20. The sum score from 0-10 classified as deficit and 11 above considered as having fair knowledge on self-care. Attitude on self-care refers to how the older perceived self-care. It will be measured by questionnaire developed by the researcher by using Orem’s theory component. The questionnaire consists of 10 statements which have 4 options: strongly agree, agree, disagree and strongly disagree options. The most positive answer are strongly agree and given score 4 and the most negative answer are strongly disagree and given score 1. The lowest score is 10 and the highest 40. The sum score from 10-25 classified as negative and 26 above considered as having positive attitude on self-care. Practice on self-care refers to set of activities done by older persons which can be categorized as self-care. It will be measured by questionnaire which is partly adopted from the Health Promoting Lifestyle Profile (HPLP) II and Orem’s theory component and by Focus Group Discussion. The questionnaire consists of 16 statements which have 3 options: never, seldom and always options. The score range from 1 for never until 3 for always option. The lowest score is 16 and the highest 48. The sum score from 16-32 classified as low and 33 above considered as high practice on self-care. Socio demographic characteristics refer to a number of older persons’ characteristic, in terms of age, gender, job, education, marital status and living arrangement. This element will be measured by sociodemographic questionnaire developed by researcher. o Age : in years o Sex : male or female o Marital status : married, single, widow/er 7 o Education : not completed elementary school, completed elementary school, not completed junior high school, completed junior high school, higher than junior high school o Job : working or not working o Living arrangement : with family or alone Common symptoms experience refers to list of health complaint suffered by the older persons in the last 6 months. Reasons for hospital consultation refer to the symptoms older persons coming to the hospital, for confinement or for consultation Frequency of medical/nursing consultation refers number of visit older persons seek medical/nursing consultation in the last 1 year, ≤ 3 times or > 3 times Kinds of health facility used refer to where the older persons go to encounter the common symptoms experience, hospital, public health center, posyandu, dukun. Nursing needs of older persons refers what nursing care the older persons need to maintain healthy and to encounter common symptoms experience. The information will be gathered through questionnaire and Focus Group Discussion. 8 CHAPTER II THEORETICAL BACKGROUND REVIEW OF LITERATURE OLDER PERSONS Aging can be defined as the sum total of all changes that occur in a person with the passing of time. Influences on how one ages come from several domains that includes the physiological processes, as well as psychological, sociological, and spiritual processes (Stanhope & Lancaster, 2002). Aging process is an unavoidable process, because it is a natural process in human life cycle. Based on biological science, a man can be categorized as the older persons after 65 years old. The basic of this classification is anatomical changes in cellular level, mainly in neuron cell. The changes cause functional decrease in cell production which is needed to affect another body process and neurological system (Sutiaputri, 1998). There are 4 distinct cohort groups among the older persons. They are: the young old (ages 65-74), the middle-old (ages 75-84), the old-old (more than 85) and the elite-old (more than 100 years old) (Meiner & Lueckenotte, 2007). According to Department of Health Indonesia (2003), older person is man or woman who is 60 years old and above. More than one-quarter of the world's population will be over the age of 60 by the year 2010. In Indonesia, in 2000, the number of older persons is 15,1 million or 7,2% of the total population with the life expectancy 64,05 years old (Indonesian Statistical Bureau, 2000). In 2010 there will be around 23,9 million older persons (9,77%) with the 9 life expectancy 67,4 years old. It is predicted that in 2020, there will be 28,8 million older persons people (11,34%), with life expectancy 71,1 years old (Indonesian Statistical Bureau, 2005). In 2007, 5,7 % of 594423 citizens of Gowa, South Sulawesi, is people with 65 years old and above and the life expectancy is 66,2 in 2002 (Health Profile of Gowa Regency, 2007). These data show that older person’s population in Indonesia increase consistently from time to time. On a study done in Korea, it was found that as they get older, the older persons usually undergo deterioration in health. The older person’s population has a high prevalence of chronic illness and personal self-care deficiencies. Arthritis, hypertension, and diabetes were frequently recognized chronic diseases among the older persons, and the most prevalent one was musculoskeletal disorder (Ahn & Kim, 2004). Indonesian older persons are suffering from a similar tendency. In Central Java, Indonesia, in 1991, the top five most frequent health complaints suffered by older persons were arthritis (49,1 %), hypertension (14,2 %), dyspnea (7,4 %), diabetes mellitus (3,3 %) and falls (2,5 %) (Sakti, 1995). Chronic disease and disability can impair physical and emotional health, self – care ability, and independence (Meiner & Lueckenotte, 2007). As chronic disease continue to affect older persons health status, self-care becomes significant in this age group (Wang, Shieh & Wang, 2004). OREM’S SELF-CARE THEORY One of the most well-developed nursing concepts has been self-care. Self-care has been described as a strategy for coping with life events and stressors, and for enhancing quality of life during the aging process, thereby promoting independence and healthy 10 aging ( Wang, Shieh & Wang, 2004). As Kart and Engler (1994) stated that self-health care is including all the actions and the decisions that an individual takes to prevent, diagnose, and treat personal ill health; all individual behaviors calculated to maintain and improve health; and decisions to access and use both informal support systems and formal medical services. In addition, Wilkinson and Whitehead (2009) viewed self-care as situation and culture specific; involves the capacity to act and make choices; is influenced by knowledge, skills, values, motivation, locus of control and efficacy as well as taking action to prevent illness and accidents, the appropriate use of medicines and treatment of minor ailments. Dorothea Orem’s self-care deficit theory, a general theory of nursing, is one of the most widely used models in nursing today. Orem presented a conceptual framework in 1959. Since then her work has continued to evolve. Orem’s general theory of nursing was formulated and expressed in 1979-1980. Orem (2001) states her general theory as the condition that validates the existence of a requirement for nursing in an adult is the health-associated absence of the ability to maintain continuously that amount and quality of self-care that is therapeutic in sustaining life and health, in recovering from disease of injury, or in coping with their effects. Figure 1 describes best the Orem’s self-care theory as cited in Tomey and Alligood (2002). 11 R=relationship, <= deficit relationship, current or projected Orem’s purpose for developing the Self-Care Framework was two-fold: she was trying to find the meaning of nursing and to develop a body of nursing knowledge based on research. According to McLaughlin-Renpenning and Taylor (2002), Orem states that “my work in theory development has focused on the beginning development of scientific knowledge in the field of nursing.” Orem’s Self-Care Deficit Theory of Nursing is a conceptual model, which is comprised of three related theories: (1) the theory of self-care, (2) the theory of self-care deficit, and (3) the theory of nursing systems. Included within these three theories are six central concepts and one peripheral concept. These central concepts of self-care and dependent care, self-care agency and dependent care agency, therapeutic self-care demand, self-care deficit, nursing agency, and nursing systems should be understood in 12 addition to the peripheral concept of basic conditioning factor, to understanding her theory (George 2002). Orem’s self-care theory included 3 constructs; that were self-care, therapeutic self-care demand and self-care agency (Rieg, 2000). Self-care is the practice activities that individuals initiate and perform on their own behalf in maintaining life, health, and well-being. Orem (2001) defined therapeutic self-care demand as a time specific calculation of the sets of actions judged to have validity and reliability in controlling factors that affect human functioning. Furthermore, she referred self-care agency as the complex acquired ability to meet ones continuing requirement of care. The theory of self-care deficit is the core of Orem’s general theory of nursing because it explains when nursing is needed. It is referred to the relationship between therapeutic self-care demand and self-care agency in which self-care agency is not adequate to meet the known therapeutic self-care demand. Therapeutic self-care demand included all actions required to maintain health and promote health, development and well-being. When therapeutic self-care demands exceed self-care capability (self-care agency) deficits occurred and nursing intervention legitimized (Rieg, 2000). Nursing is required when an adult (or in the case of dependent, the parent or guardian) is incapable or limited in the provision of continuous effective self-care. The nursing system, designed by the nurse, is based on the self-care needs and abilities of the patient to perform self-care activities (Martin, 2005). In this theory, Orem states how the patient’s self-care needs will be met by the nurse, the patient, or both. Orem identified three classifications of nursing system to meet the self-care requisites of the patient. These systems are: the wholly compensatory 13 system, the partly compensatory system and the supportive educative system (George, 2002). In the wholly compensatory system a nurse provides complete universal and health care functions for the patient. This phase is when the patient is most vulnerable and totally dependent upon the nurse to meet their self-care requisites (Martin, 2005). When the patient is able to assist and perform some self-care needs, but must rely on someone else to meet all self-care requisites in the partly compensatory system. Within the supportive/educative system, the patient is able to perform their self-care requirements and the nurse simply acts as a resource for guidance and support (Martin, 2005). A number of factors called basic conditioning factors were identified by Orem (2001) as those that influenced or modified self-care agency, therapeutic self-care requisites, and self-care. These factors included age, gender, years of education, health state, sociocultural orientation, healthcare system factors (e.g., treatment modalities), health state, family system factors, pattern of living (including activities regularly performed), environmental factors, and resource availability and adequacy. Orem’s theory is based on explicit and implicit assumptions. Meleis (1997) summarizes the explicit assumptions as: 1. Nursing is a deliberate, purposeful helping service performed by nurses for the sake of others over a period of time. This behaviour included a self-initiated, self-directed, results producing activity. 2. Persons (human agency) are capable and willing to perform self-care for self or for dependent members of the family, 14 3. Self-care is part of life that is necessary for health, human development, and wellbeing, 4. Education and culture influence individuals, 5. Self-care is learned through human interaction and communication, 6. Self-care includes deliberate and systematic actions performed to meet known needs for care, 7. Human agency is exercised in discovering, developing and transmitting to others ways and means to identify needs for and make inputs to self and others. In brief, Meleis states the implicit assumptions as: 1. People should be self-reliant and responsible for their own care needs as well as for others in the family who are not able to care for themselves, 2. People are individuals with entities that are distinct from others and from their environment. The metaparadigm is the most abstract component of the structural hierarchy of nursing knowledge. Nursing’s metaparadigm consist of concepts and propositions that are global with phenomena which is limited to the discipline of nursing with no specific perspective. The metaparadigm of nursing is composed of four concepts, which are person, environment, health and nursing. These four concepts are reflected in Orem’s theory Self-Care Framework (Fawcett, 2000). Orem defines person as human beings who are “distinguished from other living things by their capacity: 1. To reflect upon themselves and their environment, 2. To symbolize what they experience, and 15 3. To use symbolic creations (ideas, words) in thinking, in communicating, and in guiding efforts to do and to make things that are beneficial for themselves or others” (Orem, 2001). The functions of human beings are integrated to include physical, psychological, interpersonal, and social aspects. A person’s self-care needs are met by a learned behaviour. Factors which may affect an individual learning include age, mental capacity, culture, society and emotional state. When learning of self-care measures does not occur, others must learn the care and provide it (George, 2002). Orem defined health as a state of wholeness or integrity of the individual human being, his parts and his modes of functioning. She also viewed health as the responsibility of a total society and all its members. A healthy person is likely to have sufficient selfcare abilities to meet his/her universal self-care needs (Marriner-Tomey, 1994). Orem (2001) speaks to nursing as a specific type of human service based on selfhelp and help to others. Adults are expected to be self-reliant and responsible for themselves and for the well-being of their dependents. Whenever the maintenance of continuous self-care requires the use of special techniques and the application of scientific knowledge then nursing is required in providing the care or in designing it. Orem (2001) further defines nursing as a human service. Nursing is distinguished from other human services by its focus on persons with inabilities to maintain the continuous provision of health care. Nursing is needed when the adult is unable “to maintain continuously that amount and quality of [health-associated] self-care that is therapeutic in sustaining life and health”. 16 Environment as defined in the metaparadigm of nursing, refers to the person’s significant others and physical surroundings, as well as the setting in which nursing occurs, which ranges from the person’s home to clinical agencies, to society as a whole (Fawcett, 2000). According to Orem, environment is tri-dimensional, encompassing the physical, socioeconomic, and community features. The physical features involve maintaining the human structure, functioning, and well being. Socioeconomic features focus on the family, including composition by roles and ages, cultural prescriptions of authority, responsibilities and rights for the family unit. Community features are inclusive of the population and its composition by family units, by other function, collaborating social units, and by governmental voices (Fawcett, 2000). The metaparadigm concept nursing is represented in the Self-Care Framework by the concept Nursing Agency. Nursing Agency is the action of nurses in determining the needs for, design of, and production of nursing for persons with a range of types of selfcare deficits. Nursing Agency includes three dimensions which are the social system, interpersonal system and professional-technologic system. The social system includes the relationship between the nurse and the patient forming an agreement for the purpose of obtaining nursing care when an actual or potential self-care of dependent-care deficit has evolved. The interpersonal system involves the contact, association, and communication between the nurse and the patient. The professional technological system is the system of action productive of nursing. The existence of the professional-technological system is dependent on the existence of the interpersonal system, which in turn, is dependent on the existence of the social system (Fawcett, 2000). Please refer to figure-1. 17 SELF-CARE MODEL AND OLDER PERSONS According to Eliopoulos (2001), Orem’s self-care theory provides a useful framework on which a dynamic gerontological nursing practice can be built. Older individuals share similar universal life demands with all other human beings. These are basic requirements for the optimum and integrated functioning of the total individual. Age, illness, and disability may interfere with the ability to meet any of these demands and subsequently lead to the need for assistance, perhaps in the form of nursing services. It is the nurse’s responsibility to minimize or reduce limitations imposed by physical, mental, and socioeconomic restrictions (Eliopoulos 2001). An individual with a wealth of social skills is capable of a normal, active life that includes friendships and other social interaction. People who have knowledge of the hazards cigarette smoking will be more capable of protecting themselves from health problems associated with this habit. On the other hand, an older man who is widowed may not be able to cook and provide an adequate diet for himself, having always depended on his wife for meal preparation. The person who has diabetes and cannot selfinject the necessary insulin may not be able to meet the therapeutic demand for insulin administration (Eliopoulos 2001). Furthermore, Eliopoulos (2001) stated that the value a person sees in performing the action, as well as the person’s knowledge, attitudes, beliefs, and degree of motivation, influences the desire and decision for action. Limitations result if a person lacks desire or decides against action. If an individual is not interested in preparing and eating meals because of social isolation and loneliness, a dietary deficiency may develop. A hypertensive individual’s may lack of desire and decision to forfeit potato chips and meat 18 products in the diet because a belief that it is not worth the effort that may create a real health threat. The person who is not informed of the importance of physical activity may not realize the need to arise from bed during an illness and consequently may develop complications. Dying individuals, viewing death as a natural process, may decide against medical intervention to sustain life and may not comply with prescribed therapies. Values, attitudes, and beliefs are deeply established and not easily altered. Although the nurse should respect the right of individuals to make decisions affecting their lives, if limitations restrict their ability to meet self-care demands, the nurse can help by explaining the benefit of a particular action, providing by information, and motivating. In some circumstances, as with an emotionally ill or mentally incompetent person, desires and decisions may have to be superseded by professional judgments (Eliopoulos 2001). Self-care ability can be considered as a necessary condition for the realization of self-care activities and presupposes them in time. Some older persons become recipients of health care when their self-care ability is less than required in daily living (Soderhamn, Lindencrona, & Ek ,2000) On the other hand, if the individual is successful in fulfilling life demands, there is no need for nursing intervention except to reinforce the capability for self-care (Eliopoulos,2001) The inability to meet demands independently creates a need for nursing intervention. Nursing actions are directed toward strengthening self-care capacities, eliminating or minimizing self-care limitations, and providing direct care services by acting for, doing for, or assisting the individual when demands cannot be independently fulfilled. 19 Consideration must be given to assessing the impact of the illness on the individual’s self-care capacity and identifying appropriate nursing interventions to ensure that both the universal life demands and the demands imposed by illness are adequately meet. Self-care is important to well-being and nursing intervention should focus on initiating and facilitating self-care in older persons to enhance their well-being (Wang, Shieh & Wang, 2004). Nurses need to be facilitators and partners for health education not teachers or gatekeepers. Ethically nurses should practice with beneficence through provision of adequate training so a patient or individual can safely self-manage if they choose. Selfcare program should show strengthening or changing psychological attributes are more effective than teaching self-care skills but that basic education for disease management is also important. Underlying all these points is a conceptual shift from “feeling responsible for patients to feeling responsible to patients” (Wilkinson&Whitehead, 2009). On a study done by Mulford (2004), it was found that the supportive-educative role enabled the participants of the study to integrate new self-care measures enhancing his/her self-care health promotion with the use of arch supports to improve balance and/or discomfort of feet, ankle, knee, hip and back pain. Ward-Griffin and Bramwell conducted a descriptive, correlational study to explore the relationship between nurse and older persons perceptions of their self-care agency. Orem’s self-care model was used as a framework for this study because the model focused on an individual’s responsibility for health. According to Orem, self careagency is the human ability to look after oneself. Agency refers to taking action and the action that is taken by the individual is the self-care agent. Orem’s theory of Nursing 20 Systems proposes that an individual and nurse collaborate to determine and achieve selfcare goals. The study included 40 older persons participants and registered nurses’ (n = 40) selected from two different community settings. The major finding of this study was that older person and nurses perceived the older person health status differently (as cited in Mulford, 2004, p: 9-10). SOCIO DEMOGRAPHIC FACTORS AND EXPERIENCES ON SELF-CARE OF OLDER PERSONS For older persons, limitations in performing self-care exist when the experiences, in terms of knowledge, attitude or skills required for a given self-care action are inadequate or nonexistent. There are some predisposising factors which may affect the experiences (knowledge, attitude, practice) on self-care of older person. First, sociodemographic factors. A central proposition of Orem’s theory of selfcare is that capacity for meeting self-care needs may be modified by age, among other factors, such that old-old individuals have more self-care deficits than do the young-old (Kart & Engler, 1994). Furthermore, in Orem’s theory, self-care learning experience is affected by age (Martin, 2005). Similar to that, Eliopoulos (2001) also told that age interfere the self-care capacity. Increasing age also resulted in personal self-care deficiencies (Heui & Kim, 2004). Soderhamn et al. (2000), added that a decline in selfcare ability mainly takes place among the younger older persons around 75 years of age and that persons who have an age of 85+ years have reached a more stable level of selfcare ability. In their oldest years they may have adapted themselves to their actual life situation and level of health. Age had an inverse direct effect on self-care and an inverse 21 indirect effect on well-being through self-care in rural but not urban older person’s women. Compared to urban women, aging rural women lack appropriate support systems and health care resources because of geographic limitations. Understanding older persons living in different geographic locations could help community nurses design specific and effective self-care interventions (Wang, Shieh & Wang, 2004). For education and occupation as part of sociodemographic factors, it was assumed that education is a requisite personal resource for self-care agency and suggestive of the capacity for carrying out certain self-health care behaviors. Added by explicit assumption of Orem’s theory, education influences individual on self-care As for occupation, retirees have more time and perhaps more energy to engage in self-health care (Martin, 2005). The above findings was negated by the study done by Kart and Angel (1994) which investigated effect of several sociodemographic variables on self-care of older persons, it was found that education and retirement status had no statistically significant effects on the self-care measures. Whether education and/or being retired are positively related to health-promotion and illness-prevention behaviors, indicators of self-health care not included in the study, remains an empirical question. In Takalar, a municipality close to Gowa, Indonesia, 68.8% of 80 older persons respondents, had low education level (Widyastuti, 2007). Another finding, Aswar (2006), found that the highest education level of older persons in Pare-Pare, Indonesia was elementary school (51.75%) and the rest of respondents did not finish elementary school. The other sociodemographic factors are gender and marital status. The importance of marital status variable is diminished in the presence of more detailed measures of social support. Another finding, in the current study, gender evidenced significant direct 22 effects on self-health care measures. Women employed more actual self-care in response to their illness symptoms, and had more positive assessments of their capacities to provide self-care. This may reflect gender differentials in role obligations (Kart & Engler, 1994). As would be expected, the frequency of self-care practice and receipt of help from others increases with age and is more frequently reported by women than men (Norburn et.al, 1995). Nicholas (1993) found that 72 older persons aged 55 to 92 years old who lived with a spouse or others practiced more health promotion activities of nutrition, stress management, interpersonal support, exercise and self-actualization. On his study, Jemmy (2007), found that 56.6% of older persons in Makassar, Indonesia, were married. From 30 older persons who became respondents and live in Tegal alur, West Jakarta, Indonesia, it was revealed that there were more female than male older persons, and 66.7 % of older persons were deceased and there rest were married. Other findings, 100% were still live with the family members, consisting mostly of children and grandchildren. This shown that there is a genuine concern for the older persons to live with the family (Sabdono, 2007). Family networks are widely assumed to be a key source of support for older persons in Indonesia and Southeast Asia more generally, although empirical study of their composition and functioning is in its infancy (Kreager and Butterfill, 2007). Callaghan (2006) on her study regarding influences of basic conditioning factors on adolescents self-care found that from several basic conditioning factors, only support system, adequate income, adequate living condition, gender, routine practice of religion 23 and reported medical problem / disabilities which were had significant relationships to self-care in adolescents. Instead of sociodemographic variables, another predisposising factor is reasons for visiting health facility and medical/nursing consultation. According to Kart and Engler (1994), older persons are high users of medical consultation time and health facilities. Rates of chronic illness are highest among older persons, yet most illness symptoms do not lead to a medical consultation regardless of the severity of the symptoms. Many who do have contact with health care providers have treated their disorder themselves before seeking medical care. Even those who seek professional medical care and follow a prescribed treatment regimen often supplement this regimen with self-prescribed remedies, including over the counter medications and substances. This findings was also pointed on the survey done in US, it was revealed that many illness symptoms do not lead to a professional medical consultation. More than five of six (86.3%) respondents 55 years of age or older in the survey experienced at least one illness symptom within the past 6 months for which they report employing self-care only. In addition, when presented with a list of 11 illness symptoms from 5 to 35 percent of these older respondents believed that self-health care only was an appropriate response. The 10 medical conditions including osteoporosis, broken hip, hardening of the arteries, hypertension, rheumatic fever, heart diseases (including angina or heart attack), stroke, cancer, arthritis, diabetes, or blood clot (including aneurysm or varicose veins). (Kart & Engler, 1994). 24 In Indonesia, the health problems for which the older persons visited community health center most frequently included hypertension, gastritis, rheumatoid arthritis and vision problems (Sakti, 1995). On Jemmy study (2007), the percentage of older persons in Makassar, Indonesia, who visit the health facility regularly and follow the treatment advised were 89.5% (38 respondents). The next factor is health common symptoms experience suffered by the older persons. Experience with chronic illness showed direct positive effects on actual self-care. Certainly, older person who have experienced health problems in the past may be predisposed to make continued demands on the formal health care system. However, it is also the case that many chronic illnesses require self-health care efforts for rehabilitation or to maintain health status. To the extent such efforts are successful; they may provide a sense of control over health that affects how individuals respond to other illness symptoms and promotes self-care (Kart & Engler, 1994). On a study done in community-dwelling elders in Taiwan, knees were the most commonly described pain site, but the most painful site was the spinal cord area. The mean pain intensity was 3.1 (SD ¼ 1.8) and pain interference was 2.8 (SD ¼ 2.1). Most participants took prescribed medications to deal with pain; doctors were the main information source for this self-care strategy. Although participants reported using various self-care pain management strategies, most still reported moderate-to-severe worst pain. Moreover, the participants identified far fewer self-care strategies than U.S. elders with chronic pain. The three most highly effective self-care strategies for managing pain were had acupuncture, changing diet, and meditation, excluding having an 25 injection and operation. These findings suggest that community-dwelling elders in Taiwan know little about managing pain symptoms or ascribe a different meaning to pain than their U.S. counterparts (Tsai, Liu & Chung, 2010). In Aceh, Indonesia, from a study which was conducted in four communities, from 4 focus group discussions (48 older men and 81 older women) and 63 individual interviews (26 older men and 37 older women), it was found that 34 % of older persons respondents reported systemic hypertension and 55% reported diminished vision (Tyagi, 2006). There is evidence that well-being is influenced by self-care in both ill and healthy individuals. For example, Anderson showed that self-care was significantly correlated with well-being in homeless adults. Likewise, Zausniewski found that self-care and wellbeing were significantly related in 120 healthy older persons and Dungan et al showed that the well-being of older persons adults could be improved with an intervention consisting of health maintenance self-care behaviors (Wang, Shieh & Wang, 2004). Specific self-care or health promotion activities are exercising regularly, refraining from smoking, moderating alcohol consumption, sleeping 7 to 8 hours nightly, maintaining a desirable body weight, observing safety practices, seeking annual medical and dental examinations, performing monthly self-breast examination, and practicing stress management techniques (Pender, 1996). On the study done to American older person, it was found that they practice some form of self-care. When the older persons do, the most frequent type of self-care practice (75.4%) involves modification in patterns of behavior. This is not surprising, because changes in one’s built environment or in the use of special equipment or devices often 26 require substantial expenditures and complex logistical arrangements. The most common behavior changes were doing things less often and more slowly (49.1%), avoiding lifting heavy objects (47.7%), and stocking up when going to the store (25.3%). Less than half (43.2%) use various forms of equipment or adaptive devices in dealing with limitations. About one-third (31.1%) make adaptations in their living environments. A high proportion (69.4%) of older person see/receive help from others in coping with functional limitations (Norburn et.al, 1995). In Indonesia itself, there is no study that describes the self-care form or experiences. Several studies on self-care practices in various places of the world shown that culture can interfere the form of self-care. As Orem (2001), identified that one of the basic conditioning factors which may affect self-care is culture. NURSING NEEDS OF OLDER PERSON The nursing needs of older persons are varied and connected to their health problems, the manner in which they experience their illnesses and their needs when healthy, age, gender and culture (Natan, 2008). It is critical for the nurses to aware the significant nursing need for older persons. In nursing home, Israel, there was discrepancy between residents’ needs as identified by the staff, the family and the residents themselves. The nurses attributed greater significance to values and personal outlook of the residents, provision of proficient physical care, skilled mental support, social life and institutional requirements. Families ranked the most significance to the provision of information and family 27 involvement, whereas according to the residents, the most important area was skilled mental/emotional support (Natan, 2008). In the primary care setting, Walters et al (2000), claimed that older persons three most frequently identified unmet needs were with ‘eyesight/hearing’, psychological distress’ and ‘incontinence’. For the community setting, Huber M.T et al (2007) proved that 3 of 18 older persons people who become the participants explicitly wished to be visited by nurses and prefer services that focus on tertiary prevention. They didn’t regard home care as the service they thought they required. Therefore, there should be one service provider from a health background to provide all the care that might be needed ( King & Farmer, 2009). On the study done in Aceh, Indonesia, after Tsunami disaster, it was found that data and information on the health status and needs of older persons is inadequate, which is crucial for planning appropriate age-friendly health programmes ( Tyagi, 2006). COMMUNITY OLDER PERSONS PROGRAM As a group, older persons have complex needs, requiring a range of primary, community and acute hospital services (London Department of Health, 2001). The aim of the older persons’ health care is to help them to pass their old age in wellness, happy, productive and independent status. Without good planned, continuous and comprehensive health care, there will be many serious health and social problems that would occurred on the older persons. 28 According to Tabloski (2001), there are several criteria that help define the characteristics of effective community health service delivery system for the older persons. Four, in particular, deserve attention. First, for a delivery system of a community health service to be effective, it should be comprehensive. Many communities provide some programs, such as limited screening or selected activities but do not offer a full range of services to more adequately meet the needs of their senior citizens. Gaps and duplication in programs most often result from poor or nonexistent communitywide planning. Furthermore, such planning should be based on thorough assessment of older persons’ needs in that community. A comprehensive set of services should provide the following: Adequate financial support Adult day care programs Health care services (prevention, early diagnosis and treatment, rehabilitation) Health education (including preparation for retirement) In-home services Recreation and activity programs Specialized transportation services A second criterion for a community service delivery system is coordination. Often older persons go from one agency to the next. After visiting one place for food stamps, they may go to another for answers to Medicaid questions, another for congregate dining, and still another for health screening. Such a potpourri of services reflects a system organized for the convenience of providers rather than consumers. It encourages misuse and discourages use. Instead, there should be coordinated, communitywide assessment 29 and planning. Communities must consider alternatives, such as multiservice agencies, that can meet many needs in one location. A coordinated information and referral system provides another link. Most communities need this type of information network that contains a directory of all resources and services for the older persons and includes the name and telephone number of a contact person with each listing. Such network is available in some communities and should be developed. A third criterion is accessibility. Too often, services for the older persons are not conveniently located or are prohibitively expensive. Some communities are considering multiservice community centers to bring programs and services for the older persons closer to home. More convenient and perhaps specialized transportation services and more in-home services, such as home health aides, homemakers, and meals on wheels, may further solve accessibility problems for many older person ( Spradley & Allender, 2001). Similar with on Policy Unit, Age Concern England (2006), Older persons should be able to retain independence and control over their lives, even when they come to need support or healthcare. Service for them should be accessible and put the needs and wants of the individual at the centre. The fourth criterion is quality programs. This means service that truly addresses the needs and concerns of a community’s senior citizens. Evaluation of the quality of a community’s services for the older persons is closely tied to their assessed needs ( Spradley & Allender, 2001). Tyagi (2006) added that another key strategy to ensure improved health quality for older persons and healthy ageing is to make primary health care facilities and services at 30 the community level age-friendly or old-age-specific. Age-friendly means that health care is accessible and appropriate to persons of all ages but in relation to their specific needs at a specific age. According to Tsao (2006), age friendly primary health care services should be available, accessible (physically, socially and financially), appropriate (facilities and staff, appropriate knowledge, skills and attitudes), affordable (equitably financed) and integrated with other health and social service providers. Thus, primary health care workers need to be sensitised and informed about the various specific needs of older persons when providing care in the communities. Based on the study done in Aceh, Indonesia, it was revealed that at the community level, there is a visible lack of age-friendly or age-sensitive health facilities and staff. Community-based health centre staff and community health volunteers have limited awareness and knowledge of older people’s health needs and of appropriate ways to treat these illnesses or conditions either, directly or through referrals (Tyagi, 2006). In Indonesia, increased life expectancy has resulted in increasing numbers of older persons living in the community (Sahar, 2006). Several trials to care for the older persons have been introduced in Indonesia. A nationwide public geriatric examination system called ‘poswindu’, which joins ‘posyandu’, introduced 20 years before as a health check system for mothers and children, was started in 2002 in Indonesia (Wada et.al, 2005). Posyandu is the abbreviation of Pos Pelayanan Terpadu, which is translated as health post integration service. 31 According Department of Health, Indonesia (2003), the aim of Posyandu for older persons is: a. To increase the older persons welfare through independent Posyandu in the community. b. To increase the easy access for the older persons to get basic health service and referral. c. To increase coverage and quality of health service for the older persons, especially the promotion and prevention aspect without disregard curative and rehabilitative aspect. d. To develop the active group of older persons which conduct continuous and better quality activities. The activities of Posyandu are: a. Activity of daily living examination b. Mental health status examination c. Nutritional status examination d. Blood pressure measurement e. Glucose blood measurement f. Protein urine measurement g. Referral to the public health center h. Patient education i. Home visit 32 The mechanism of Posyandu activities based on 5 steps system (5 tables). They are: a. First step: older person’s registration. b. Second step: writing down the activity daily living of older persons, taking body weight and height. c. Third step: taking blood pressure measurement, physical and mental health examination d. Fourth step: urine and blood examination (simple laboratorium) e. Fifth step: counselling and patient education The activities and mechanism of Posyandu can be adjusted with the place and other mechanism instead of the steps above can be used. In South Sulawesi province, Indonesia, there are some municipalities implementing a community older persons program. One of them is Gowa municipality which starts to run community older persons service since 2009. The aim of the program is to increase degree and quality of older persons’ life so the happy and meaningful old age can be reached. The activities they planned to do are training the community member to become volunteer of older persons program, health counseling for the older persons, home care, and many more (South Sulawesi DOH, 2007). In Takalar municipality, Indonesia, 80% of its older persons actively visited Posyandu. (Widyastuti, 2007). 33 NURSES ROLE IN COMMUNITY OLDER PERSONS PROGRAM Nurses play an important role in caring for older patients by preventing, recognizing, and treating common problems and illnesses that are major causes of morbidity and mortality in the older persons ( Tabloski P.A, 2006). Cestari and Currier argued that gerontological nurse practitioners (NPs) have been providing primary care to older persons at home setting since 1970 (as cited in Dick & Frazier, 2006, p. 325). According to Dick and Frazier “a growing body of evidence suggests that in-home comprehensive geriatrics assessments performed by gerontological NPs, in collaboration with geriatriticians, provide outcomes such as detecting major and potentially reversible medical problems, delaying disability, improving functional status, and reducing institutionalization” (p. 325). Coronary heart disease, stroke, cancer and mental health problems are target areas for health improvement for older persons (Runciman et al, 2006). In Indonesia, there is no gerontological NPs yet. The front line of health service in the community is Public Health Center (PHC). In every PHC, there is one health worker who is assigned to be responsible for older persons heath care program. Majority of health workers who are responsible for the older persons health care program are nurses considering that the biggest proportion of health worker in Indonesia is nurses. On the data from Indonesian Nurses Association, there are 500,000 nurses or 60% from total health workers in Indonesia (Kompas.com, June 2009). While the number of nurses in Gowa is 50,37% from the total 802 health workers ( Health Profile of Gowa Regency, 2007). 34 SYNTHESIS Functional competence and ability for self-care are of importance for an independent life, both for individuals living in their own homes and those in institutional care. Knowledge of self-care among older persons is of importance in order to identify individuals at risk and to plan care for this group. (Soderhamn, Lindencrona & Ek, 2000). As the nurse, the information related to self-care of older persons is valuable in determining the nursing needs of older persons as well nursing education program for them. The Self-Care framework has been accepted by the nursing community to guide research and practice throughout the U.S. and other countries. A literature review of the Self-Care Framework revealed that it guided a wide range of research design, from psychometric studies of framework-based instruments to experimental studies. There are studies done on self-care of older persons. One of it is these, is study done by Soderhamn, Lindencrona and Ek (2000), which they found that in Sweden, self-care ability and selfcare agency decreased for respondents 75+ years of age. Another study done by Tsai, Liu, and Chung (2010) revealed that in Taiwan, the community-dwelling older persons use three most highly effective self-care strategies for managing pain. They are namely acupuncture, changing diet, and meditation. Unfortunately majority of the studies only investigate some part of self-care theory. Whether it is only the ability to perform self-care, the deficit on self-care, or the nursing system of self-care in nurse’s view. Less common study was done on the description of Knowledge, Attitude, and Practice (KAP) of older persons on self-care, more over in Indonesia where the older persons care is not as optimal as in other 35 countries. Based on this fact, researcher is willing to assess the KAP of older persons in Indonesia. CONCEPTUAL FRAMEWORK Knowledge, Attitude & Practice on self-care of Older Persons Nursing needs Socio demographic data Common symptoms experiences Figure -2. Conceptual Framework According to Orem (2001), self-care is the part of life and the independent practice of activities for maintaining life, health and well-being. A person is capable and willing to perform self-care. Level of knowledge, attitude and practices on self-care will affect the ability to perform self-care, which is, in Orem’s theory called as self-care agency. The level of knowledge, attitude and practices on self-care will be reflected on self-care agency. Orem identified 10 basic conditioning factors in the conceptualization of selfcare agency, including age, gender, marital status, education, living arrangement, common symptoms experiences, reasons for hospital consultation, frequency of medical/nursing consultation, and kinds of health facility used. 36 Since age can interfere the experience on self-care, there might be time when the older persons cannot perform self-care independently and become the recipients of care. Related with the self-care deficit theory of Orem, when the older person cannot meet their self-care demands, that is the time when nursing is needed. But, in the nursing system where the nurse exist, the care should be design based on the self-care needs and abilities of the older persons to perform. By understanding the nursing needs of older persons, the effective nursing care in fulfilling the self-care practice of older persons will be met. The basic data on characteristic of older persons as well as older person’s experiences on self-care and maintaining health will be used to determine nursing needs of older persons for health promotion and self-care. HYPOTHESES 1. There is association of sociodemographic characteristic to knowledge, attitude and practices on self-care of older persons. 2. There is association of common symptom experiences to knowledge, attitude and practices on self-care of older persons 37 CHAPTER III METHODOLOGY RESEARCH DESIGN This study is a mix of quantitative and qualitative study. The first data will be gathered through questionnaire while to check the result of questionnaire, Focus Group Discussion will be done once. The design will be used in this study is descriptive correlation. The researcher wants to determine the association of socio demographic factors and common symptoms experience to knowledge, attitude and practices on self-care of older persons. A correlational design examines the relationship between two or more variables within one group without aiming to determine cause and effect. It does not have an independent variable that can be manipulated by the researcher, that is, there is no intervention by the researcher, only observation (Taylor, Kermode & Roberts, 2007). Similar to that, Polit and Beck (2008), suggested that the aim of descriptive correlational research is to describe relationships among variables rather than to infer cause-and-effect relationships. In addition, by using this design, it will facilitate the identification of many interrelationships in a situation in a short period of time (Burns & Grove, 1995). SAMPLE AND POPULATION The target population is older persons who live in Kanjilo Village, Gowa municipality. Gowa is one of the municipalities in South Sulawesi, Indonesia. It is two hours distance by car from Makassar, the capital city of South Sulawesi. Ninety five 38 percents of its population is Makassarese, one the major tribes in South Sulawesi. South Sulawesi has 4 major tribes. Makassarese, Buginese, Mandarese and Torajanese. Based on the researcher observation, the characteristics of older persons who are Makassarese are majority of them still live with the big family and still working actively. The sample is half of older persons who live in Kanjilo village that will be chosen in this study. Based on the data from Kanjilo Public Health Centre Area, there are 287 older persons who live in the village in 2008. Participant selection will be carried out by purposive sampling, which is chosen by specific consideration and purpose. The study will use 165 participants. In determining the sample size, the researcher uses the Krejcie and Nomogram Harry King. Krejcie in estimating sample size is based on 5% error level. So the sample has 95% confidence level to the population (Sugiyono, 2005). So if there are 287 older persons, with the confidence level of population is 95%, the sample size is around 165. Please refer to appendices. The participants in this study are the older persons who live in Kanjilo village with the inclusion criteria: People aged 60 years old and above Including men and women Have a good hearing, sight and mental condition (older persons with dementia are excluded from the study) Can communicate in Bahasa Makassarese tribe No disability 39 STUDY FLOW CHART Population: older persons in Kanjilo village Purposive sampling: 165 older persons Data collection Purposive sampling: 6 older persons Data collection Data analysis Reporting Documentation Figure-2. Study flow chart 40 RESEARCH SETTING The study will be done in Kanjilo village, Gowa, South Sulawesi, Indonesia. The reason for choosing this area are: 1) Gowa municipality is easily reached from Makassar, the capital city of South Sulawesi, 2) There are 22 Public Health Centers in Gowa municipality which is conducting monthly Posyandu for older persons, 3) Gowa municipality commonly used as the practice area for Community Health Nursing of School of Nursing, Hasanuddin University, 4) Kanjilo village easily reached from Gowa municipality town, 5) Kanjilo village held twice regular Posyandu monthly in 2 different spots, and it was done by the nurse and cadres, 6) The average number of older persons who visit Posyandu Lansia at one spot in Kanjilo village is 20 people. RESEARCH METHODS AND TOOLS The study will use 3 instruments. They are, sociodemographic questionnaire, Knowledge, Attitude and Practices (KAP) on self-care questionnaire, and Focus Group Discussion questions. Questionnaires tend to be used in descriptive studies designed to gather a broad spectrum of information from the respondents and can be distributed to the large sample. It is also presented in consistent manner and has less opportunity for bias (Burns & Grove, 1995). Questionnaire is the most commonly used instrument for obtaining information. Through the questionnaire, the researcher can seek such demographic details as age, gender, or income. The answers on questionnaire may also e used to explore relationships between variables. Questionnaires are used frequently in correlational designs (Taylor, Kermode & Roberts, 2007). 41 The sociodemographic questionnaire includes the characteristic information of older persons. The KAP on self-care questionnaire is made from modification of self-care instrument. Numerous research studies on self-care used questionnaire. Through extensive literature review, no valid and reliable instrument on self-care found which can measure the Knowledge, Attitude and Practice (KAP) on self-care of older persons simultaneously. Most of the self-care tool was developed for children, adolescent and adult. Moreover, several of the instruments, only measure some part of Orem’s theory, whether it is self-care agency, self-care perception or self-care performance. The researcher develops KAP on self-care questionnaire based on the component of Orem’s theory as well as the result of researcher’s observation in research setting. The components of Orem’s theory included in this questionnaire are; basic conditioning factors, self-care, self-care agency, therapeutic self-care demand, explicit assumptions, self-care deficit, nursing system, and dependent care agent. In addition, special for practice on self-care questionnaire, the statements are adopted from some statements in Health Promoting Lifestyle Profile (HPLP) II. The HPLPII is a 52-item 4-point Likerttype scale that consists of six subscales: health responsibility, physical activity, nutrition, interpersonal relations, spiritual growth, and stress management. Adequate Cronbach’s alpha coefficients of internal consistency reliability were reported in a study of 379 adults with coefficients ranging from .75 to 93 (Callaghan, 2006). The KAP questionnaire consisted of 36 statements, ten statements each for knowledge and attitude on self-care and 16 statements for practice on self-care. For knowledge on self-care, the responses are correct and incorrect and do not know options. The statements are made positively, unless for number 7,9,10, they are made as negative 42 statements and scored reverse. Correct answer is given score 2, incorrect answer is given 1 and do not know options is given score 0. The lowest score is 0 and the highest 20. The sum score from 0-10 classified as deficit and 11 above considered as having fair knowledge on self-care. The items included on Orem’s theory component as follows: self-care (no. 1 and 7), basic conditioning factors (no. 2 and 3), explicit assumptions (no. 4 and 10), therapeutic self-care demand (no. 6 and 9), nursing systems (no.8), and dependent care agent (no.5). For attitude on self-care, the responses are strongly agree, agree, disagree and strongly disagree options. The statements are made positively, unless for number 2,5,6,7 they are made as negative statements and scored reverse. The most positive answer are strongly agree and given score 4 and the most negative answer are strongly disagree and given score 1. The lowest score is 10 and the highest 40. The sum score from 10-25 classified as negative and 26 above considered as having positive attitude on self-care. The items included on Orem’s theory component as follows: self-care (no. 1), self-care deficit (no. 2), basic conditioning factors (no. 5 and 6), therapeutic self-care demand (no. 3 and 9), self-care agency (no. 4), and nursing systems (no.7 and 8). For practice on self-care, the responses are never, seldom and always options. The more frequent the older persons on self-care the higher the score. The score range from 1 for never until 3 for always option. The lowest score is 16 and the highest 48. The sum score from 16-32 classified as low and 33 above considered as high practice on self-care. Some statements are adopted from HPLP instrument, and they are included on subscales in the instrument. They are: health responsibility (no. 1,3,4,9), stress management (no. 2 and 10), interpersonal relations (no. 7 and 13), nutrition (11,14,15,16), physical activity 43 (no. 12). While for the Orem’s theory component are as follows: self-care deficit (no. 8), basic conditioning factors (no. 6), and therapeutic self-care demand (no. 5). The instrument will be translated into Bahasa and will be tested its validity and reliability. The instrument will be tried to 10 respondents with the same inclusion criteria and will be tested its reliability by Cronbach Alpha. For the second part of data gathering, Focus Group Discussion (FGD) will be done by using probing questions as guidelines and observation sheet. In Focus Group Discussion, new ideas can be created, unique thoughts collected, need, expectations and issued can be identified. In addition, the participants can better understand ‘individuals’ language, knowledge and experience in an intersubjective exchange (Taylor, Kermode & Roberts, 2007). A study of older people’s livelihoods in Ethiopia used FGD to gather data. FGD participants were questioned on their understanding of the role, added value and sustainability of the older person specific livelihoods initiatives being carried out by partner agencies. (Help Age International, 2011). Another study regarding fire and life safety education for older persons in Milwaukee also used FGD as the data collection way (Smerz et al., 2003;). RESEARCH PROCESS After Ethic Research Committee of Faculty of Medicine, Hasanuddin University approved the study, the researcher visit nurse who responsible for community older persons program in Kanjilo PHC. The first process is doing participant selection by explaning the aim of the research to the nurse and asks her to select the participant candidate based on the inclusion criteria. After getting the a list of participant candidate 44 from the nurse, the researcher will visit the house of participant candidates and explain the research as well as give them informed consent sheet. In the introduction to the questionnaire, it will be clearly stated that its purpose is to improve the care of the older persons and the confidentiality of the data will be ensured. If the candidate agree to be the participant in this research and signed the informed consent sheet, the researcher will make an appointment for gathering data. The researcher will read the items of the instruments and the other questions aloud for the patients and marked the answers when the patients reported. The next procedure is to conduct a Focus Group Discussion (FGD). There will be 6 older persons who become the participants. The researcher and the nurse will select purposively the participant candidates who become key informant in the FGD. Again the candidates will be explain regarding FGD as well as asked their agreement to become the participants. DATA PROCESSING AND ANALYSIS Descriptive analysis will be done to sociodemographic characteristic, common symptoms experience, reasons for hospital consultation, frequency of using health facilities , kinds of health facility used and knowledge, attitude and practices on self-care For hypothesis testing, Pearson chi-square will be used to determine the association of socio demographic factors and common symptoms experience to knowledge, attitude and practices on self-care of older persons. The significance level is 0.05. 45 For the data gathered from Focus Group Discussion, transcript will be made. Next, making margin/list on the transcript & initial code, data horizontalization, keywords, categories, and lastly establish ing sub-theme & theme 46 Ghant Chart Activities Proposal writing Proposal Defense Proposal Revision Testing instrument Data Gathering Data analysis Design PE program Chapter IV&V writing Thesis Defense Thesis paper revision Thesis paper submission February March April May June August September