ULForumANSWERS
advertisement

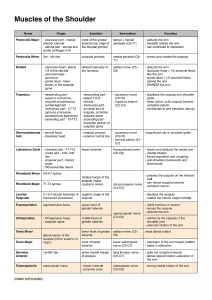
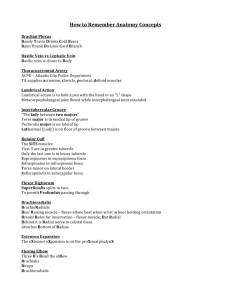
UPPER LIMB FORUM –Group Answers MOI=mechanism of injury w Study Questions 1. Define the difference between shoulder separation and shoulder dislocation. Sep. involves injury to the coracoclavicular joint & AC joint. Dislocation involves hum. Head displaced out of GF. Shoulder separation-MOI-fall or impact, shoulder appears “depressed” A mild shoulder separation involves a sprain of the AC ligament that does not move the collarbone and looks normal on X-rays. A more serious injury tears the AC ligament and sprains or slightly tears the coracoclavicular (CC) ligament, putting the collarbone out of alignment to some extent. The most severe shoulder separation completely tears both the AC and CC ligaments and puts the shoulder joint noticeably out of position. Shoulder dislocation-MOI-sudden impact applied to the humerus when the joint is fully abduct, (ant -inf dislocation- tilts humeral head downward onto inf weak part of capsule which tears; the humeral head is displaced out of the glenoid fossa; acronium acts as a fulcrum) ant and inf (usually), greater and lesser tuberosity may be sheared , axillary N (paralysis of deltoid M) or radial N may also be damaged. 2. What is the clinical significance of the radial groove? Contains radial N and profunda brachial A, if frac occurs in mid 1/3 rd of radiusN damage may result 3. List the rotator cuff muscles, their nerve supplies, origins, insertions, and functions. SITS-Provide the stability of the shoulder joint. Supraspinatus M-insert greater tubercle of humerus Infraspanatus M-lateral to the greater tubercle of humerus? Teres min- inferior facet of greater tubercle of the humerus Subscap M- LESSER tubercle of humerus Muscle Origin on scapula Attachment on humerus Function Innervation Supraspinatus muscle supraspinous fossa greater tubercle abducts the arm Suprascapular nerve (C5, C6) Infraspinatus muscle infraspinous fossa greater tubercle laterally rotates the arm Suprascapular nerve (C5-C6) Teres minor muscle lateral border greater tubercle laterally rotates the arm Axillary nerve (C5) Subscapularis muscle subscapular fossa lesser tubercle medially rotates the humerus Subscapular nerve (C5-C6) 4. What is the segmental innervation of the following muscles, and the cord of the brachial plexus involved? a. b. c. d. e. f. Supraspinatus-suprascapular n. (C5,C6), upper trunk Infraspinatus- suprascapular n. (C5,C6), upper trunk Teres minor-Axillary n. (C5,C6), posterior cord Subscapularis-Upper and Lower subscapular n. (C5,C6)-posterior cord Deltoid-Axillary n. (C5, C6)-posterior cord Levator scapulae-Dorsal Scapular Nerve (C5 root)-upper trunk 5. On the figures below, label all muscles that either originate or insert on the scapula. Study Questions 1. Define the muscular walls of the axilla. (See COA Fig. 6.23(B) and GD pg. 437 SEE CLASS NOTE SLIDE REGARDING WALLS OF AXILLA…. Pect major, subclavious, pect min, serratous ant, teres minor, lats dorsi, teres major 2. Define the distribution of the clavipectoral fascia. ….Surround subclavius/pect m -costocoracoid membrane(includes subclav and pect min)- upper segment (named for med/lat attachments)peirced by 3 structures—cephalic v, thoracoacromial a, lateral pectoral n (pect maj n) -suspensory ligament of axilla- lower segment-fuses with axillary F at axially floor (attached above to the clavicle, below, it encloses pectoralis minor and continues down as the suspensory ligament of the axilla and joins the fascial floor of the axilla. ) 3. Into what large vessel does the cephalic vein drain? Axillary Vein 4. What is the principal function and innervation of the pectoral muscles? Ribs move up if you fix scapula and flex pects. lateral pectoral nerve and medial pectoral nerve Clavicular head: C5 and C6 Sternocostal head: C7, C8 and T1 Action: Clavicular head: flexes the humerus Sternocostal head: extends the humerus As a whole, adducts and medially rotates the humerus. It also draws the scapula anteriorly and inferiorly. Medial pectoral nerves (C8, T1) Action: 5. It stabilizes the scapula by drawing it inferiorly and anteriorly against the thoracic wall. What structure occupies the bicipital groove=intertubercular groove? Medial-teres major, floor-latissimus dorsi, lateral-pectoralis major (“a Lt. btwn. 2 Majors”) 6. What happens to the scapula following complete section of the long thoracic n.? Winging of the scapula may occur if you fixate your hands on a wall. Injury: Any blow to the ribs…scapula is superficial to the muscle. 7. Explain the anatomical location of each of the three cords of the brachial plexus. First part - the part of the artery medial to pectoralis minor Second part - the part of the artery that lies behind pectoralis minor Third part - the part of the artery lateral to pectoralis minor 8. Outline the anatomical location of each of the three parts of the axillary artery, and identify the branches of each. 1-supreme thoracic A,2-thoracoacromial A, lateral thoracic A, S-supreme thoracic A. T-Thoracoacromial A. (branches into ACPD: acromion, clavicular, pectoral, deltoid) L-Lateral Thoracic A. A-Anterior Circumflex Humeral A. P-Posterior Circumflex Humeral A. S-Subscapular A. 9. 10. Draw and label a complete brachial plexus . Study Questions 1. What is the significance of collateral blood supply/circulation? Anastamoses , multiple blood sources…to compensate for collapse or blood loss, trauma, etc. 2. The medial, lateral, and posterior cords of the brachial plexus are named due to their position relative to what structure? THE SECOND PART OF THE AXILLARY ARTERY. 3. List at least one motor deficit that would follow section of each of these nerves at the indicated places: a. median nerve, proximal to the elbow – Hand of Benediction-can’t flex digits 2 &3. Flexor carpi ulnaris…a flexor on the forearm (flexes wrist) , so can’t flex wrist Loss of pronation, denervation of PQ & Lumbricals gone? Recurrent branch of median nerve…innervates the thenar muscles. (FIND IN CADAVER!!!) b. ulnar nerve, proximal to the elbow : FDP tendons to digits 4 & 5. Abductor 4 & 5. Everything but 2 LOAF. Hypothenars gone. Abductors gone. Lumbricals 4 & 5 lose add of thumb, add flex opposition of little finger (little finger can only extend) c. axillary, at the shoulder deltoids and teres min hurt-lose abd up to 90: Teres minor and deltoid, would result in probs w/lat. Rotation, & d. radial, proximal to the origin of the tricepsext of the forearm (best acronym anconeus helps triceps extend) Wrist drop-can’t extend wrist, biceps brachii would work, lose sensory to dorsum behind thumb & snuffbox, could not extend forearm due to triceps knocked out…problem is proximal to the origin of the triceps muscle. e. lower subscapular, near its origin- medial rotation (inner- teres maj and subscapularis-medially rotates & stabilizes shoulder joint)[suprascap N does infraspinatous and infraspinatous]: Teres major responsible for medial rotation and ADDuction…would lose these b/c teres major innervated by lower Subscapular n. f. musculocutaneous nerve, in the axilla-biceps, brachialis, brachioradialislose flexion of forearm: biceps would be flexion-deficient, brachialis would not be able to flex, loss of sensation in lateral forearm. 4. Draw upper limb with dermatome level map. C6 thumb and index C8 fingers 4 & 5 C7 middle finger 5. Describe the boundaries of the cubital fossa. Lat border –brachioradialis Protonator teres forms medial border 6. List in order, the mediolateral relationships of the biceps Tendon, median Nerve, and brachial Artery in the cubital fossa. TAN ( Lateralmedial) Biceps Tendon, brachial Artery, median Nerve 7. In the figure below, which is a section through the arm at the humeral mid-shaft, label the structures indicated. a-biceps brachii b-brachialis c-cephalic V d-musculocutaneuos N e-medial cutaneous N f-brachial A g-basilic V h-ulnar N I-long head of triceps j-medial head of triceps M k-lateral head of triceps l-radial N m-profunda brachii A Study Questions: 1. List the muscles associated with the common flexor tendon of the forearm. The common flexor tendon is a tendon shared by a number of superficial flexor muscles in the forearm. It attaches to the medial epicondyle of the humerus. It serves as the origin (in part) for a number of muscles (the superficial muscles of the anterior compartment of the forearm) 2. Pronator teres 3. Flexor carpi radialis 4. Palmaris longus 5. Flexor digitorum superficialis 6. Flexor carpi ulnaris 7. Describe the course of the median nerve in relation to the pronator teres and flexor digitorum superficialis. Superior to fds 8. In the figure below, which is a cross-section of the wrist through the distal carpal row, identify the tendons, nerves, arteries, and bones. A trapesium Btrapezoid C capitate D hamate E palmar cutaneous branch of median nerve F ulner artery G ulner nerve H median nerve I flexor digitorum superficialis J flexor digitorum profundus K flexor pollicis longus L flexor carpi radialis M extensor carpi ulnaris N extensor digiti minimi O extensor digitorum and extensor indicis P exgtensor carpi radialis longus and brevis Q extensor pollicis brevis R absuctor pollics longus S radial artery T extensor pollicis longus 4. What is carpal tunnel syndrome? What are the physical symptoms of a patient with it? Pressure on the median n. in the carpal tunnel. Carpal tunnel is the concave anterior surface of the carpal bones and closed by the flexor retinaculum (packed with long flexor tendons of the fingers and their surrounding synovial sheaths and the median nerve). Carpal tunnel syndrome is produced by compression of the median nerve w/in the tunnel, and is sometimes caused by thickening of the synovial sheaths of the flexor tendons or arthritic changes in the carpal bones. Physical symptoms are burning pain along the distribution of the median nerve to the lateral 3.5 fingers and weakness of the thenar muscles. 5. If a patient suffers a fracture at the medial epicondyle of the humerus, what nerve is most likely to be injured? Ulnar nerve-what motor deficits do they have? What sensory deficits do they have???? 6. What is a Colles' fracture? Besides an x-ray, what is an obvious indication that a patient has a Colles' fracture? PG. 480 Dinner-fork deformity of the wrist. The bump would be on the posterior (dorsal) surface of the wrist due to the displaced bone fragment. Usually the two styloid processes are at the same level (side-by-side) in the X-ray. Colles fracture is fx of the distal end of the radius resulting from a fall w/ outstretched hand. (Occurs in old people). The force drives the distal fragment posteriorly and superiorly, and the distal articular surface is inclined posterior Study Questions 1. What are the principal digital movements mediated by the: a) palmar interossei; b) dorsal interossei? Abduction and ADDuction. Extend the IP’s while flexing the MP joints with the Lumbricals. 2. What is the extensor expansion and what muscles insert into it? Pg 590 Fibrous sheaths serve as attachment for interossei and lumbricals. It is an extension of the extensor tendon. 3. Define the boundaries of the "anatomical snuff box" and list its key contents. Hold hand in anatomical position w/palm forward….contents are radial artery-responsible for the radial pulse, bone on floor of snuffbox is the Scaphoid. Running at the floor: radial artery (9) giving the dorsal carpal branch (10) Running at the roof: branches of the superficial branch of radial nerve Borders: Tendon of abductor pollicis longus (16) and extensor pollicis brevis (15) Tendon of extensor pollicis longus (14) 4. What are the osseous attachments of the extensor retinaculum? Pisiform and hamate 5. Know this!!! Know which fingers are C6, C7, C8…know what nerves are at that level….In the following diagram identify the cutaneous distribution of the median, ulnar and radial nerves. 6. The muscles of the hand receive motor input from the median and ulnar nerves. List the motor deficits that will result from nerve injury at the indicated locations: 7. Median nerve, proximal to flexor retinaculum (as in wrist slashing):2LOAF 8. Ulnar nerve, at the wrist (ulnar nerve entrapment):