Betz N, et al. 2010. Radiotherapy in early-stage
advertisement

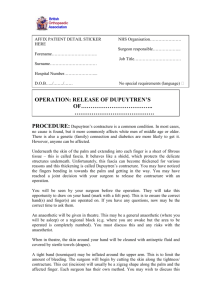
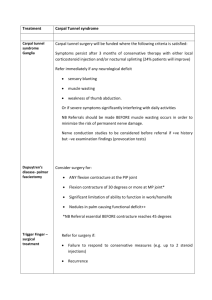
DUPUYTREN’S CONTRACTURE Description References Dupuytren’s contracture consists of progressive scarring and thickening of the connective tissue (most commonly in the palm of the hand and most commonly on the ring and pinky fingers side) that causes the fingers to remain in a flexed position and prevents their extension. The appearance of Dupuytren contracture on exam is that of palmar thickening. The thickening may be nodular (and thus mistaken for a callus) or cord-like. This process typically involves the longitudinal and vertical components of the fascia but at times seems to exist apart from anatomically distinct fascia. The skin overlying the sclerosed fascia may fuse with it and become raised, or it may atrophy, acquiring a puckered appearance. Young, DM and Hansen, SL. 2010. CURRENT Diagnosis & Treatment: Surgery, 13e; Doherty GM ed. Ch. 42: Hand Surgery. The McGrw Hills Company; New York. The histopathology of the disease changes as the condition progresses. Early disease shows nodules with a predominance of fibroblasts and type III collagen. A contractile phase follows, during which fibroblasts are replaced by myofibroblasts and lymphocytes infiltrate the tissue. During this phase, the concentration of proteoglycans Moermans, JP. 1997. greatly increases. Advanced disease is relatively acellular with a predominance of type I Place of Segmental Aponeurectomy in the collagen in tendonlike cords. Pathology (organ, cell, system) The table below describes the microscopic changes accompanying the evolution of Dupuytren’s contracture: Treatment of Dupuytren's disease; Chapter 6: Histopathology. PhD Thesis. University of Bruxelles Balaguer, T et al. 2009. Histological staging and Dupuytren's disease recurrence or extension after surgical treatment: a retrospective study of 124 patients. European Journal of Hand Surgery. 34:493-6. I speculate that in the beginning, an idiopathic over-proliferation of fibroblasts begins 1 the process of scarring and contraction. The hand, exposed to unusual forces and non physiological traction of the phalanges, likely develops reactive inflammation (hence the lymphocytic infiltration of the intermediate-stage lesions) and consequently contributes to the activation of scar tissue deposition, acting synergistically with the initial idiopathic disease process Of note, histological staging is a reliable method for predicting recurrence. Pathophysiology Like all fascia, the palmar fascia contains a population of resident fibroblasts that allow for connective tissue renewal. The pathophysiological process underlying Dupuytren contracture is fibroblast proliferation and collagen deposition. Though it is not known why this uncontrolled proliferation of palmar fascia occurs, it is thought to be related increased expression of growth factors, including basic fibroblast growth factor, platelet-derived growth factor, and transforming growth factor-beta within the diseased fascia. Differential Diagnosis The differential for Dupuytren disease includes several other conditions that affect the hand, including trigger finger, palmar tendinitis, stenosing tenosynovitis, a ganglion cyst, or a soft-tissue mass. Unlike Dupuytren contracture, trigger finger typically involves pain with flexion followed by the inability to extend the affected digit. Stenosing tenosynovitis, unlike Dupuytren disease, is also characterized by pain (as well as a history of overuse or trauma). A small, movable nodule that is tender to palpation at the metacarpophalangeal (MCP) joint is likely a ganglion cyst (unlike a more fixed fibrous nodule of Dupuytren’s) A soft-tissue mass must also be excluded from the diagnosis, especially if the patient is significantly younger than the typical patient with Dupuytren disease: patient younger than age 40 years without involvement of the dorsal hand, foot, or penis is unlikely to have Dupuytren disease, and the concerning possibility of a sarcoma must be ruled out—although the pathologic findings of a biopsy will most likely reveal a benign etiology (eg, lipoma, inclusion cyst). A firm scar may also be a simple overuse callus – though the history would likely point to it. The more advanced phase may be confused with a “hand of benediction” (neuropathic claw hand conditions caused by median or ulnar nerve injuries). Median claw hand will show hyper-extension of the MCP and flexion at the IP joints of the 2nd and 3rd digits (index and middle). Ulnar claw hand will show hyper-extension of the (MCP) and flexion at the distal and proximal (IP) joints of the 4th and 5th digits (ring and little finger). In both, clawing will become most obvious during finger extension. Unlike median and ulnar claw hads, in Dupuytren’s the MCP joints are also flexed; also, the muscles have normal strength but are limited by the scarring, unlike in the neuropathies aforementioned, in which the issue is weakness (and only over time may develop some degree of stiffness due to atrophy). Revis, DR, Dupuytren’s Contracture. E-Medicine Rheumatology: http://emedicine.medsca pe.com/article/329414overview, accessed 9/22/2010 Revis, DR, Dupuytren’s Contracture. E-Medicine Rheumatology: http://emedicine.medsca pe.com/article/329414overview, accessed 9/22/2010 Lee, S Baytion, M, Reinke, DL, Bogdan, Y. Dupuytren Contracture. E-Medicine Orthopaedics: http://emedicine.medsca pe.com/article/1238712overview, accessed 9/23/2010 2 Epidemiology The prevalence of Dupuytren’s contracture varies according to the ethic makeup of a given country, as Northern European descent confers a predisposition to developing the disease. Dupuytren contracture is very common in northern Europe and the United Kingdom and in countries inhabited by immigrants from these areas (eg, Australia, Canada, United States). In the United Statesm, A 10-year retrospective study using the Department of Veterans Affairs computer system was conducted to determine the racial distribution of this disorder: approximately 5-15% of males older than 50 years are affected. Dupuytren contracture is less common in blacks and Asians (incidence = 3%); Dupuytren contracture is least common (incidence <1%) among Indians, Native Americans, and individuals of Hispanic descent. While the characteristics of the disease in blacks are similar to those in whites (late onset, predominantly affecting the ulnar digits, associated with alcoholism, smoking, liver failure, epilepsy, trauma and diabetes), an important difference hinting to a genetic component to the pathogenesis of the disease is that the disease is rarely bilateral in blacks. Approximately 80% of affected individuals are male in all races studied. Disease onset is earlier in males than in females, and the course of disease is more rapid and severe. The mean age of disease onset in males is 49 years; in females, the mean age is 54 years. The mean age among men who seek surgery to treat this condition is also earlier, at 58 years; the mean age among females is 62 years. Revis, DR, Dupuytren’s Contracture. E-Medicine Rheumatology: http://emedicine.medsca pe.com/article/329414overview, accessed 9/22/2010 Saboeiro, AP et al. 2000. Racial Distribution of Dupuytren's Disease in Department of Veterans Affairs Patients. Plastic & Reconstructive Surgery. 106 : 71-75 The exact cause of Dupuytren contracture is noty known. The disproportionate prevalence of Dupuytren contracture in Northern Europeans suggests a genetic component: studies suggest an autosomal dominant pattern of inheritance with variable penetrance. HLA-B7 and HLA-DR3 have been identified in a number of patients, suggesting a possible immunologic influence as well. Young, DM and Hansen, SL. 2010. CURRENT Diagnosis & Treatment: Surgery, 13e; Doherty GM ed. Ch. 42: Hand Surgery. Some researchers suggest that Dupuytren contracture may result from an error in The McGrw Hills growth and regulation of the fibroblast, resulting from chromosomal changes similar to Company; New York Etiology those seen in cells undergoing neoplastic change. Trisomy 8 has been identified in the fibroblasts excised from some patients. In support of this theory, ealry nodules display features of a benign neoplasm. Because the changes occurring in the palmar fascia approximate the normal stages of wound repair and remodeling, but to an excessive and detrimental extent, another theory holds that this disease is a response to trauma. Repeated exposure to compression, stress, and other mechanical forces may trigger a reparative process in the palmar fascia. The reason for the progression to severe joint contractures remains unknown. Revis, DR, Dupuytren’s Contracture. E-Medicine Rheumatology: http://emedicine.medsca pe.com/article/329414overview, accessed 9/22/2010 In my opinion, these theories are not mutually exclusive; I tend to believe that the contracture is a symptom associated with diverse disease processes, and that the 3 palmar fascia is particularly sensitive to these disease processes and it is thus disproportionately affected. I think it is analogous to a cough in the sense that it is a symptom, but just like a cough can be due to cancer, infection, heart failure etc, a Dupuytren’s contracture is due to any processes that cause dysregulation of connective tissue remodelling. Its association with cancer favors a neoplastic-like process, while its association with trauma supports the aberrant wound healing theory. Furthermore, I think that metabolic imbalances (such as those created by DM and liver failure) may dysregulate the exceedingly complex tissue remodeling signaling cascades, leading to fibroblast over-proliferation and subsequent scarring. The inflammatory state established by those diseases further favors scarring. Dupuytren contracture manifests itself most commonly in the palm by nodular or cordlike thickening. As aforementioned, the skin may fuse with the underlying fascia and become raised and hard, or it may shrink, sometimes drawn into a deeply puckered crevasse. The disorder invades the palm at the expense of fat but is never adherent to vessels, nerves, or musculotendinous structures (though it may be adherent to flexor tendon sheaths). It has an unpredictable rate of progression, but the Young, DM and Hansen, earlier it starts in life, the more destructive and recurrent it is apt to be. SL. 2010. CURRENT Clinical manifestations Dupuytren fasciitis may involve any digit or web space, but it affects predominantly the ring and small fingers. Over time the cord contracts resulting in digital flexion contracture and reduced hand function. In longstanding cases, the fingers may be drawn tightly into the palm, resulting in secondary contracture of joint capsule and ligaments, flexor sheaths, and atrophic muscles. The condition is not usually associated with pain. Diagnosis & Treatment: Surgery, 13e; Doherty GM ed. Ch. 42: Hand Surgery. The McGrw Hills Company; New York There is a paucity of studies on the specificity/ sensitivity of the clinical findings, as Dupuytren’s contracture is a diagnosis based on surface anatomy findings and associated functional impairment. The findings are consistent with a progressive scarring process. Late presentation, complications As aforementioned, Dupuytren’s Disease has early, intermediate, and late phases. While loss of normal architecture and formation of skin pits mark the early phase and nodules and cords characterize the intermediate phase, contractures mark the late phase. The late phase tends to go through four stages of contracture, 1. contracture of the MCP joint of the ring finger in stage I; 2. contractures of the MCP and PIP joints of the ring finger and the MCP joint of the small finger in stage II; Rayan, GM. 2007. Dupuytren Disease: Anatomy, Pathology, Presentation, and Treatment. The Journal of Bone and Joint Surgery (American). 89:189-198. 3. contractures of the MCP and PIP joints of the ring finger, the MCP and PIP 4 joints of the small finger, and the MCP joint of the long finger in stage III; 4. and stage-III contractures as well as DIP joint hyperextension of the ring or small finger in stage IV. This progression is not universal, and in fact palmar fascial disease or contracture remains confined to the palm and does not progress enough to cause digital flexion deformity. Palmar involvement usually precedes extension of the disease into the digits; however, the disease may also begin and remain in the digits. A palpable interdigital soft-tissue mass is an indication that the neurovascular bundle is involved, but it is not a reliable indicator. An early intervention to slow the progression of Dupuytren’s is radiotherapy. A study showed that regardless of the individual stages, radiotherapy led to stabilization of the disease in about 50% of patients (with an even greater percentage for earlier stages) and 10 % improved. Complication of late stage of the disease have to do with QOL factors (see below) Nutritional factors Radiographic evidence Nutrition affects the disease insofar as diabetes and alcoholism both affect the likelihood of developing the disease. Some studies reported that taking 200–2,000 IU of vitamin E per day for several months was helpful in the treatment of Dupuytren’s, suggesting a role for antioxidants in slowing the progression of the fibrosing process; other studies on the effect of vitamin E, however, did not obtain the same promising results. Since Dupuytren’s disease is a surface disease, imaging is not typically obtained. Research on imaging has shown, however, that MRI is accurate for detecting Dupuytren's contracture, defining its palmar involvement, and depicting its extent. The cords of intermediate and late disease have a uniformly low signal intensity similar to that of tendons on both T1- and T2-weighted images Nodules have an intermediate signal intensity similar to that of muscle on both T1- and T2-weighted images, with focal areas of lower signal intensity. The signal characteristics of the lesions correlate with the degree of cellularity of the lesions as seen histologically. The prognostic Anonymous author. Dupuytren’s Contracture. The Institute for Optimum Nutrition, http://www.ion.ac.uk/he althnotes.php?org=ion&C ontentID=1205001 accessed 9/23/2010 Thomson GR. Treatment of Dupuytren’s contracture with vitamin E. BMJ 1949;Dec 17:1382–3. Yacoe ME, BergmanAG, Ladd AL and Hellman, BH.1993. Dupuytren's contracture: MR imaging findings and correlation between MR signal intensity and cellularity of lesions. American Journal 5 significance is that highly cellular lesions tend to have higher rates of recurrence after surgery than do hypocellular lesions. of Roentgenology, 160: 813-817. Laboratory evidence Revis, DR, Dupuytren’s Contracture. E-Medicine There are no laboratory studies that are commonly done to detect or stage the disease. Rheumatology: However, testing for associated conditions (CAGE screening and LFTs for alcoholism http://emedicine.medsca and liver failure, fasting blood glucose or glucose leading test plus HbA1C for diabetes) pe.com/article/329414may be useful in addressing the patient’s overall health. overview, accessed 9/22/2010 Psychosocial impact of disease A variety of activities can be affected. If it occurs in younger patients who are still working, their work can be greatly affected. While the ability to write is not as affected if only the fourth and fifth fingers are contracted, the disease can change one’s handwriting. It can affect one’s ability to paint, cook, play golf or any other sport that uses the hands. Aesthetically, it can be disfiguring and can greatly affect the patient, especially women. Risk factors As mentioned in the epidemiology section, being of Northern European descent is a risk factor in the development of the disease. Medical conditions that increase the risk of developing the disease include alcoholism, smoking, liver failure, epilepsy, trauma, and diabetes. Being male and being older than 50 y/o are also risk factors for developing the disease. Prevention There are no proven strategies to prevent Dupuytren’s, though the role of antioxidant vitamins (such as vitamin E) has been proposed. In light of the existence of early treatments to slow or halt the progression of the disease, awareness in predisposed groups and early diagnosis/treatment may be the best “preventative” options. Saboeiro, AP et al. 2000. Racial Distribution of Dupuytren's Disease in Department of Veterans Affairs Patients. Plastic & Reconstructive Surgery. 106 : 71-75 In early-stage Dupuytren's contracture, radiotherapy is applied to prevent disease progression. Radiation therapy acts in a similar way as it does when applied to the treatment of sarcomas and other tumors. Treatment options Messina A, Messina J. 1993. The Continouos Elongation Treatment by TEC Device for Severe A number of non surgical techniques have been attempted to treat Dupuytren’s Dupuytren's Contracture contracture, including splinting and stretching devices, ultrasonic therapy, and steroids. of the Fingers. Journal of None of these methods has been proven to benefit patients on a long-term basis. Plastic and Reconstructive Enzymatic fasciotomy using collagenase clostridium histolyticum significantly reduces Surgery; 92:84-90 contractures and improves the range of motion in joints affected by advanced Dupuytren's disease. Bird B, Ball C, Balasuntharam P. 6 Surgery is indicated when the disorder has progressed sufficiently (more than 30 degrees of flexion at the MCP joint or any flexion contracture of the PIP joint). Fasciectomy is the surgical procedure that gives the best long-term results, although in selected cases where only the longitudinal pretendinous fascial band is involved and the skin moves freely over it, subcutaneous fasciotomy done through a small longitudinal incision may release a contracture and decrease post-op disability time due to the less invasive nature of the procedure. The degree of atrophy of the skin overlying the contracture determines whether a skin graft is required for wound closure after fasciectomy. A skin graft may have the added benefit of substituting the diseased overlying dermis, which has been implicated as an inductive mechanism in this process, thus lowering the recurrence rate in severe cases. Unfortunately, the degree of contracture of the fifth digit may be so severe to require amputation. Motion should be started within 3–5 days after surgery. Dynamic splints and postoperative injection of corticosteroids into joints and the operated areas may increase patient’s adherence to the physical therapy plan. In the occasional case with acute and rapid onset of a tender nodule, local triamcinolone may be used for symptomatic relief. DMSO (Dimethyl sulfoxide) applied to the affected area may reduce pain by inhibiting transmission of pain messages, and may also soften the abnormal connective tissue; its effectiveness and safety, however, remain unproven. Rehabilitation after surgery for Dupuytren's Contracture (Protocol). Cochrane Database of Systematic Reviews 2007, Issue 2. Art. No.: CD006508. DOI: 10.1002/14651858.CD00 6508. Hurst,LC, et al.2009. Injectable Collagenase Clostridium Histolyticum for Dupuytren's Contracture. NEJM, 361:968-979 Betz N, et al. 2010. Radiotherapy in earlystage Dupuytren's contracture. Long-term results after 13 years. Strahlenther Onkol; 186:82-90. Lee, S Baytion, M, Reinke, DL, Bogdan, Y. Dupuytren Contracture. E-Medicine Orthopaedics: http://emedicine.medsca pe.com/article/1238712overview, accessed 9/23/2010 Young, DM and Hansen, SL. 2010. CURRENT Diagnosis & Treatment: Surgery, 13e; Doherty GM ed. Ch. 42: Hand Surgery. The McGrw Hills Company; New York Outcomes of treatment In terms of early treatment, a study of long term outcomes (13 years) of radiotherapy showed it is effective in prevention of disease progression and improves patients' symptoms in early-stage Dupuytren's contracture. In case of disease progression after radiotherapy, a "salvage" fasciotomy is still feasible with good outcomes despite the Betz N, et al. 2010. Radiotherapy in earlystage Dupuytren's contracture. Long-term 7 tissue changes associated with radiation therapy. A retrospective study of the outcome of carpal tunnel release was evaluated retrospectively patients followed for a median of 10 months. Outcome was considered good in 27% (pain, weakness, and numbness were essentially resolved); fair in 42% (most of the symptoms improved); and poor in 32% (symptoms persisted or worsened). Patients whose pre-operative work activity was considered physically strenuous were associated with a slightly but significantly poorer outcome (60% good or fair) compared to those in light work or with no employment (89% good or fair). Proportionately fewer patients returned to their original work when they previously engaged in strenuous activity, ranging from 27% for those using air guns to 80% in light work. The highest chance of a poor outcome from carpal tunnel release occurs in patients who have either associated symptoms of thoracic outlet syndrome or physically strenuous work activities. Another study of postoperative management of Dupuytren’s patients with prevention of applied mechanical tension in the early phases of wound healing showed that this intervention decreases complications after fasciectomy and that no digital motion is lost to this protective intervention. results after 13 years. Strahlenther Onkol; 186:82-90. Zyu, G, Firrelll, JG, Tsai, TM. 1992. Pre-Operative Factors and Treatment Outcome Following Carpal Tunnel Release. Hand Surg Eur Vol 17: 646-650 Evans RB, Dell PC, Fiolkowski P. 2002. A clinical report of the effect of mechanical stress on functional results after fasciectomy for Dupuytren's contracture. J Hand Ther. 15:331-9 Bird B, Ball C, Balasuntharam P. Rehabilitation after surgery for Dupuytren's Contracture (Protocol). Cochrane Database of Systematic Reviews 2007, Issue 2. Art. No.: CD006508. DOI: 10.1002/14651858.CD00 6508. Bird B, Ball C, Balasuntharam P. hematoma, fibrosis and stiffness, digital nerve injury, recurrence of contractures and Rehabilitation after digital ischemia secondary to digital artery injury. Reflex sympathetic dystrophy, a surgery for Dupuytren's painful, debilitating neurologic disorder of the hand, can occur after surgery and must Contracture (Protocol). be treated aggressively. In general, the functional reward for the patient is great at Cochrane Database of any age. Systematic Reviews 2007, Issue 2. Art. No.: A Cochrane review showed that although surgery can successfully correct deformity it CD006508. DOI: does not cure Dupuytren's disease and recurrence is common after surgery, and that 10.1002/14651858.CD00 reports of recurrence rates following surgery within the first few years range from 6508. The potential complications of surgery are wound breakdown (loss of skin flaps), Potential Complications of treatment 27% to 34%. After five years it has been reported between 41% and 71%. The effectiveness of surgery when the contracture involves the metacarpophalangeal Lee, S Baytion, M, Reinke, 8 (MCP) joint of only one finger is high. However, when two or more joints are involved DL, Bogdan, Y. Dupuytren complete correction is less likely. At the proximal interphalangeal joint (PIP) the improvement rate is reduced. PIP contractures in isolated cords improved by 50% after surgery but is often lost during the healing phase. Other post operative complications of Dupuytren's contracture include sympathetic flare, hypertrophic scarring, pain, joint stiffness, loss of digital extension and reduction of function. Contracture. E-Medicine Orthopaedics: http://emedicine.medsca pe.com/article/1238712overview, accessed 9/23/2010 9