Dupuytren`s Disease Edits
advertisement

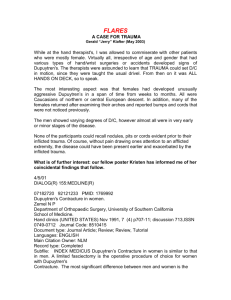
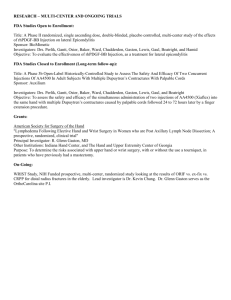
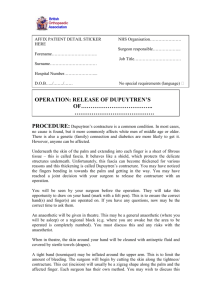
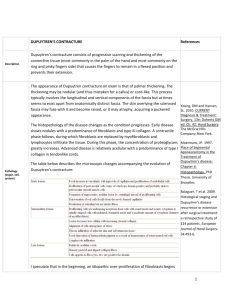
Date: 02-Apr-2014 09:47 Version: 15 Author: Joseph Bernstein Musculoskeletal Medicine for Medical Students Dupuytren Disease Table of Contents 1 Description 3 2 Structure and function 4 3 Clinical manifestations 6 4 Diagnosis 7 5 Epidemiology 8 6 Differential diagnosis 9 7 Treatment options and outcomes 10 8 Risk factors and prevention 12 9 Miscellany 13 10 Key terms 14 11 Skills and competencies 15Dupuytren Disease Version 15 3 1 Description Dupuytren Disease is a progressive disorder characterized by fibrosis of the palmar fascia (also known as the palmar aponeurosis) and is associated with the formation of palpable nodules and cords in the palm and fingers. In its later stages it causes fixed digital flexion contractures. Although the disease process spares the tendons deep to the fascia, because the contractures place the finger in flexion (as shown in the figure) the tendons cannot function normally. Dupuytren Disease typically involves the 4th finger but may include others (5th next-most likely; thumb least likely). The disease interferes with grasp primarily; it is not a painful condition.Dupuytren Disease Version 15 4 2 Structure and function Dupuytren’s disease is due to abnormal thickening and contracture of the palmar fascia (also known as the palmar aponeurosis). The palmar fascia complex is a fibrous structure that lies below the dermis and above the flexor tendons and muscles of the hand. It anchors the palmar skin and protects deeper neurovascular structures. It extends from the wrist across the palm (where it is continuous with the transverse carpal ligament); the tendon of the palmaris longus, if present, attaches to it. Distally, it courses into the fingers to become the digital fascia. The fibers of the fascia are architecturally complex, with transverse, longitudinal, or vertical orientations. source: WIKIPEDIADupuytren Disease Version 15 5 In Dupuytren disease, these fibers contract to form nodules and then cords. The fascia becomes focally adherent to the overlying skin, causing pitting, and the cords contract, causing fixed flexion deformities of the digits. The abnormal proliferation of myofibroblasts (specialized fibroblast-like cells that are vital for wound healing) is critical to the pathogenesis of Dupuytren disease. Myofibroblasts, unlike regular fibroblasts, are capable of contracting, and they are responsible for the fascial contraction that is seen in Dupuytren Disease. The fascia in Dupuytren is characterized by increased numbers of myofibroblasts and inflammatory cells and disorderly collagen deposition. There is increased expression of growth factors within the fascia and an increase in the ratio of type III to type I collagen. The underlying cause of Dupuytren remains obscure, but ischemic, autoimmune, and inflammatory mechanisms have all been suggested. The cause of Dupuytren disease remains elusive. It is likely multifactorial. Certain environmental factors are thought to play a role, including smoking, alcohol use, and diabetes. However, these do not account for all cases of Dupuytren’s. In fact, patients with diabetes tend to have milder disease. Some authors have also proposed that the use of anti-epileptic medication may be causative, but this is controversial. Another controversial suggestion is that in some cases the use of vibrating machinery may lead to Dupuytren’s. Rheumatoid arthritis, on the other hand, seems to be protective, perhaps because of the use of anti-inflammatory medications. In addition to environmental factors, there seems to be a genetic basis to at least some cases of Dupuytren’s. This is supported by the large number of patients with a family history of the disorder and by the high prevalence of Dupuytren’s in patients of Northern European descent. An autosomal dominant mode of inheritance with incomplete penetrance has been postulated, but a single gene responsible for the disease has yet to be identified. Patient presentationDupuytren Disease Version 15 6 3 Clinical Manifestations The initial manifestations of Dupuytren Disease includes thickening of the skin of the hand, and loss of normal skin mobility. The skin changes are followed by the development of palpable nodules and cords in the palm and fingers. The nodules may or may not be painful and are usually located near the distal palmar crease, near the base of the finger, or adjacent to the PIP joint. As the disease progresses, often over a period of several years, flexion contractures of the MCP and PIP joints can develop, most commonly affecting the ring and small fingers. The “tabletop test” can determine if the patient has a flexion contracture. As shown, the patient here is attempting to lay the hand palm-side down, flat on a surface. This test is more sensitive than specific; that is, patients who can lay their hands down do not have a contracture, whereas an inability to do so may have other causes In most cases, both hands are involved, although one is often more advanced than the other. Patients may also experience ectopic manifestations, such as fibrosis on the dorsum of the PIP joints (Garrod’s knuckle pads), plantar fibromatosis (Ledderhose disease), penile fibromatosis (Peyronie’s disease), and frozen shoulder. Dupuytren Disease Version 15 7 4 Diagnosis In general, Dupuytren’s disease is a clinical diagnosis. Hand x-rays will demonstrate flexion contractures and can be used to rule out other causes of deformity. Nodules and cords will not be seen, as they are radiolucent. While hand x-rays should be obtained at the time of initial evaluation, there is no role for routinely obtaining any other imaging or laboratory studies.Dupuytren Disease Version 15 8 5 Epidemiology Typical patients are of Northern European descent, with fair skin and blonde hair. Dark skinned people are not usually affected. It has been suggested that the disease is of Viking origin, although this has not been substantiated. Onset is usually in middle to late life. Dupuytren’s disease is much more common in men than women; and when it is found in women, the onset is later and the disease is less severe. The prevalence of Dupuytren’s Disease varies dramatically by region. It is highest in northern Scotland, Ireland, Norway, and Australia, where as many as 40% of elderly men may be affected. In the United States the prevalence is less than 5%. Regardless, the implications of the disease can be severe, and patients with advanced disease have difficulty with everyday activities like washing their hands or putting their hands in their pockets.Dupuytren Disease Version 15 9 6 Differential diagnosis While Dupuytren disease causes flexion contractures of the digits, a number of other disorders can present in a similar fashion, including stenosing tenosynovitis (or “trigger finger”), ulnar nerve palsy, and camptodactyly. The thickened skin, nodules, and cords may be confused with scars, calluses, tophi, ganglion cysts, prolapsed flexor tendons (as can be seen in rheumatoid arthritis), or soft tissue tumors such as giant cell tumors or even (rarely) epithelioid sarcomas. Plantar fibromatosis (Ledderhose disease) and penile fibromatosis (Peyronie’s disease) are sometimes seen in conjunction with Dupuytren disease, making thorough history-taking important. Red flags for Dupuytren’s Although the signs of early Dupuytren’s can be subtle, pitting of the palmar skin can be one of the first findings and is a relatively specific marker of the disease. Males with early onset, a family history of Dupuytren’s, ectopic involvement, and bilateral disease have the worst prognosis. Aggressive intervention should be considered when there is a MCP joint contracture of thirty degrees or more or for any degree of PIP joint contracture.Dupuytren Disease Version 15 10 7 Treatment options and outcomes Patients with limited functional impairment and no evidence of disease progression can be educated regarding the diagnosis and observed over time. When the disease progresses and symptoms become more severe, however, intervention is warranted. There is no cure for Dupuytren’s disease, but many options for mitigating its effects exist. Radiotherapy is used in the early stages of disease and is best able to prevent progression. Indications for more aggressive treatment include metacarpophalangeal flexion contractures of more than thirty degrees or any proximal interphalangeal flexion contracture. Once this degree of contracture is present, treatment involves removing or breaking apart the cords that pull the fingers into flexion. One method for removing or breaking apart the cords that pull the fingers into flexion is to cut them with a scalpel or percutaneously with a needle. This latter technique is called “needle aponeurotomy” or “needling”. The scalpel or needle disrupts or “breaks” the cord of tissue that is contracting the finger. The advantages of this technique are that there is a small or no incision, it can be performed on multiple fingers at the same setting, and usually requires little therapy after the procedure. The primary risk is accidental injury to nerves or tendons. PHOTO how to inject Dupuytren’s disease Another treatment option for breaking apart the cords is the injection of collagenase clostridium histolyticum, an enzyme that weakens the Dupuytren’s cord. This injection is performed in the office and then the day following the injection, the physician will manipulate the contracted finger in an attempt to break the cord and straighten the finger. Currently, the collagenase injection can be used only on one joint in one finger at a time and additional injections must be spaced at least one month apart. Otherwise, the risks and benefits are similar to those for needling. Limited fasciectomy, in which the involved fascia is excised, may be performed, and is often considered for more advanced cases. The principle advantage to fasciectomy is a more complete and reliable joint release than that with the needle or enzyme techniques. Disadvantages include the need for hand therapy postoperatively and longer recovery time. For the most severe and for recurrent cases, the overlying skin must be excised as well and the area skin grafted (a so-called dermo-fasciectomy). Patients are often especially stiff after dermo-fasciectomy. To assist in regaining range of motion, patients are prescribed hand therapy and often thermoplast splints. For more severe stiffness, temporary placement of skeletal traction devices, surgical release of joint contractures, or even joint fusions can be utilized.Dupuytren Disease Version 15 11 About 10% of patients regress without treatment. However, patients with progressive or debilitating disease require intervention, and, following surgery, recurrence rates are high, ranging from 2% to 60% (average 33%) . Recurrence may be due to local recurrence of disease or extension of disease to areas outside the surgical site. Small finger involvement and involvement of more than one digit are both associated with higher recurrence rates. Potential complications of surgery include skin necrosis, infection, nerve or vascular injury, reflex sympathetic dystrophy, loss of the involved digit, and stiffness. The outcomes of collagenase injections have been less well studied. They seem to be effective in the short term and appear relatively safe, although some cases of iatrogenic tendon ruptures have been observed and long-term follow-up is not yet available . “Dupuytren’s diathesis” is used to describe a constellation of factors associated with a poor prognosis: Young age, male sex, a family history of the disease, bilateral disease, and the presence of ectopic manifestations. Interestingly, diabetics tend to have a more favorable prognosis.Dupuytren Disease Version 15 12 8 Risk factors and prevention Risk factors include a family history, male sex, smoking, alcohol intake, and diabetes. Epilepsy, anticonvulsant use, hand trauma, and the use of vibrating machinery may also put patients at higher risk, although this is controversial.Dupuytren Disease Version 15 13 9 Miscellany Among bagpipe players, Dupuytren’s Disease is known as the “Curse of the MacCrimmons”, after a family of preeminent bagpipe players in 16 century Scotland. When affected by the Curse, a player’s small finger becomes bent, making bagpipe playing impossible. Famous sufferers of Dupuytren’s disease include Ronald Reagan, Bob Dole, and Samuel Beckett. The increased numbers of myofibroblasts, disorderly collagen deposition and increased expression of growth factors seen in Dupuytren disease are found in penile fibromatosis, suggesting a common underlying condition. According to Stigler’s (tongue in cheek) Law of Eponymy, "No scientific discovery is named after its original discoverer" (a phenomenon first described by Merton, Stigler points out). Dupuytren’s Disease is no exception: Baron Guillaume Dupuytren's 1831 lecture associated his name with a condition Henry Cline characterized in 1808.Dupuytren Disease Version 15 14 10 Key terms Dupuytren’s disease, palmar fascia, Dupuytren’s diathesisDupuytren Disease Version 15 15 11 Skills and competencies Recognize the presenting features of Dupuytren’s disease; Understand the underlying pathophysiology; Identify risk factors for the development of Dupuytren’s disease; Describe the various treatment options and prognosis.