NAME: AGE: DATE: - Inglewood Family Health
advertisement

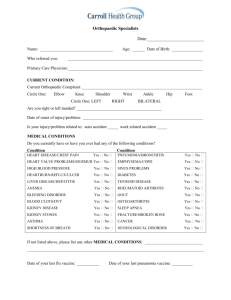
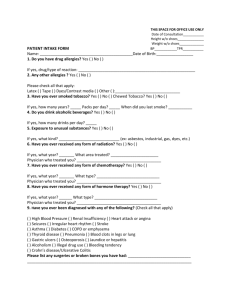
NAME: D.O.B: OCCUPATION: HT: WORK PHONE: WT: DATE: HOME PHONE: BP: TPR: What is your main reason for seeing the Doctor? Do you have any of the following? Do any blood relatives have any of the following? Diabetes: Diabetes: Thyroid: Thyroid: Cancer: Cancer: Heart Disease: Heart Disease: Lung Disease: Lung Disease: Stomach Disease: Stomach Disease: Bladder Disease: Bladder Disease: Other: Other: ALLERGIES to medications: HOSPITALIZATIONS/SURGERIES Hives? ___Yes ___ No Swelling? __Yes __ No HABITS Do you use cigarettes? ___Yes ___No How many per day? Alcohol: Blood transfusion? ___Yes ___No EYES Date: HEART & CIRCULATION LUNGS/BREATHING ___Normal ___Normal ___Cough ___Contacts/glasses ___Chest Pain ___Shortness of Breath ___Cataracts/glaucoma ___Ankle Swelling ___Pain Last exam date: ___Palpitations/rapid beats ___Sputum ___Fainting ___Wheezing ___Normal ___Dizziness ___Normal ___Pain ___Other: EARS ___Ringing ___Hearing Loss NOSE ___Normal ___Congestion/stuffy ___Bleeding ___Injury THROAT ___Pain ___Normal STOMACH/BOWELS ___Change in habits ___Nausea URINATION ___Difficulty start or stop ___Painful to urinate ___Vomiting ___Rectal Bleeding ___Pain ___Diarrhea ___Constipation ___Normal ___Flank pain ___Frequency ___Blood in urine ___Up at night ___Normal MUSCLE/BONES ___Pain ___Fracture/breaks NERVOUS SYSTEM ___Headache ___Head injury/knocked out? MENTAL STATE ___Feel blue ___Nervous ___Injury ___Other ___Normal ___Seizure ___Tingling/numbness ___Weakness ___Incoordination/unsteady ___Normal ___Memory Loss ___Confused ___Anger ___Hard to Sleep ___Normal SKIN ___Normal ___Rashes List medications you use regularly: Doctor’s Notes: REPRODUCTIVE/PERIODS