Adult ENT Health Questionnaire
advertisement

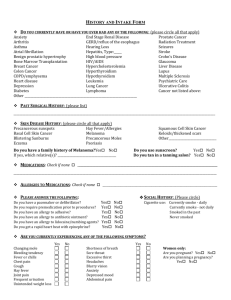
ADULT ENT HEALTH QUESTIONNAIRE Referring or family physician’s name:____________________________________________________________________ Why are you seeing the doctor today?__________________________________________________________________ Please list any medications you are currently taking (Including over the counter or herbal) _________________________________________________________________________________________________ Are you allergic to any medications? NO____ YES_____ List:_______________________________________________ Have you ever had surgery? NO___ YES___ List:________________________________________________________ Any problems with Anesthesia? NO___ YES___ List______________________________________________________ Any hospitalizations? No___ YES___ List_______________________________________________________________ Occupation:___________________ Any pets indoors? NO___ YES___ List___________________________________ Do you smoke or use chewing tobacco? (circle which one) Do you drink alcohol? No____or quit____when quit?_____________________ Yes___Packs/day?___________for____________years NO___ YES____ List number of drinks/ day_________________________________________ Family History: (Circle if your family has had any of the following problems) Allergy Diabetes Asthma Hearing Loss Problems with Anesthesia Ear Tubes Head/Neck Cancer Thyroid Problems High Blood Pressure Heart Disease Bleeding Problems Personal History: (Please circle if you have had or currently have any of the following problems). Constitutional: fevers, sweats, malaise, weight loss, change in appetite Eyes: new vision problems, double vision, cataracts ENT: ears, nose, throat Cardiovascular: murmur, congenital heart disease, heart attack, chest pain. Respiratory: cough, asthma, tuberculosis, shortness of breath, wheezing Gastrointestinal: trouble eating, nausea, vomiting, diarrhea, abdominal pain, acid reflux, indigestion Genitourinary: recent infections, difficulty urinating, frequent urination Musculoskeletal: arthritis, joint pain, mobility problems Integumentary: skin infections, rashes, skin changes Neurological: seizures, headaches, vertigo, weakness, stroke, developmental delay Psychiatric: ADHD, anxiety, depression, drug dependence Endocrine: diabetes, thyroid problems Hematologic/ Lymphatic: bleeding disorders, easy bruising Allergic/ Immunologic: immune problems, food allergy, environmental allergy, eczema, psoriasis Patient Label