Lecture8&9
advertisement

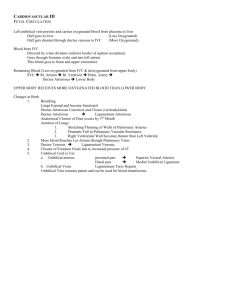
Lecture #8 Study Guide – Diagnosis & Length of Pregnancy and the Development of Germ Layers 1. What are some presumptive signs of pregnancy? 2. What are some probable signs of pregnancy? 3. What are the positive signs of pregnancy? And at what stage are these possible? 4. What is the normal length of pregnancy and how is this calculated? 5. When is an infant considered “premature” (duration of gestation or birth weight)? 6. When is an infant considered “small for date?” 7. When is an infant considered “post-mature?” 8. What do the inner cells divide into and what these different layers develop into? 9. What are the main functions of circulation? 10. Name the major components of the circulatory system and their functions. 11. Trace the path of blood through the (adult) types of blood vessels as it leaves the heart and returns (in general terms). _______________________________________________________________ Lecture #8 Study Guide Answers 1. amenorrhea, nausea & vomiting (morning sickness), engorgement of breasts, frequent urination, constipation, fatigue, skin pigmentation, softening of lower uterine segment, hormonal tests 2. all of the above signs, uterine enlargement, uterine contraction, detection by ultrasound 3. Auscultation of fetal heartbeats (17-18 weeks), Palpation of fetal outline (24 weeks), imaging (sonogram, MRI – variable) 4. a. 280 days (40 weeks or 10 lunar months) from beginning of last menstrual period b. 266 days (280 days minus 14 days) 5. < 37 weeks gestation or <5.5 lbs. 6. born after 38 weeks but < 5.5 lbs 7. born 2+ weeks after expected due delivery date, weight > 9 LBS 8. a. Ectoderm: epidermins, nervous system, chromaffin organs (adrenal gland), eye structure, neuroepithelium, some GI epithelium and teeth enamel b. Endoderm: epithelial lining in the GI (ESP pancreas and liver), epithelium of inner ear, epithelium of larynx, trachea & smaller passages, epithelium of urinary tracts, bladder, urethra and prostate c. Mesoderm: all connective tissue, teeth, entire body musculature (smooth and striated), blood and lymphatic vessels, adrenal cortex, lining of pericardium, pleura and peritoneum 9. a. b. c. d. supply O2 to tissues transport nutrients from GI tract to tissues transport CO2 to lungs transport metabolic and other wastes to kidneys and GI for excretion e. regulation of body temperature f. distribution of hormones and other agents regulating cell function through the body 10. a. Heart – pumps blood through blood vessels to cells b. Blood & Blood vessels: carry gases, metabolic products, hormones from all tissue to heart and back c. Brain and Peripheral Nervous centers: control of vasodilation and vasoconstriction substances, regulation of cardiovascular function 11. Left atria of heart -> large arteries (AORTA) -> arteries -> arterioles > capillaries (site of nutrient/oxygen/waste/etc transfer between blood and other cells) -> venules -> veins -> large veins (INFERIOR AND SUPERIOR VENA CAVA) -> right atria of heart Lecture #9 Development of Fetal Circulation 1. What does the umbilical vein do? 2. What do the two umbilical veins do? 3. Trace the pathway of fetal circulation from the umbilical vein to the umbilical artery. 4. Where is the actual anatomical site of nutrient and gas exchange within the placenta? 5. What are the three mechanisms by which the fetus avoidance a Mount Everest situation (a state of low oxygenation leading to hypoxia)? 6. Why is the liver considered the most important organ in blood distribution? 7. Why is the brain, which is first in priorities in the adult, relegated to the three spot? 8. What is the function of the ductus venosus? 9. What is the function of the foramen ovale? 10. What is the ductus arteriosus? 11. What do the maternal corkscrew arteries? 12. Describe the major differences between the adult and fetal heart. 13. What is the tubular heart? 14. At what point in development (what week) does the heart start beating? 15. At 16-18 weeks, what is the normal heart rate of the fetus? 16. When do the atria and ventricles of the embryonic heart take shape? 17. By what point will the heart have an adult EKG pattern? 18. Name three congenital defects that can occur during development. Answers to Lecture #9 1. carries highly oxygenated and nutrient rich blood from placenta to fetus 2. carry poorly oxygenated blood and high concentrations of metabolic waste blood from fetus to placenta 3. Please See Diagram Below and UNDERSTAND!! Step 1: Richly oxygenated blood enters umbilical vein from the placenta and travels to the liver. Step 2: Via the ductus venosus, most of the oxygenated blood is shunted away from the liver (but still giving it first dibs on the most richly oxygenated blood) to the inferior vena cava Step 3: Partially oxygenated blood enters the right atria, some of this still pretty well oxygenated blood travels through the foramen ovale to the left atria while the rest goes through to the right ventricle. Step 4a: From right ventricle, blood feeds the collapsed lungs through the pulmonary trunk. However, most of the blood is shunted via the ductus arteriosus back to the aorta. Step 4b: Partially oxygenated blood from the left atria, travels to left ventricle and into the aorta. Step 5: Partially deoxygenated blood in the aorta splits into the brachiocephalic trunk, which feeds the brain, and the rest of the body. Step 6: Partially deoxygenated blood will travel around the rest of the body and eventually make its way back to the placenta via the umbilical arteries. Sites of deoxygenated blood: 1. After the blood has left the brain, 2. after the blood has left the lungs 3. as the blood is traveling up the IVC before it meets the ductus venosus. 4. Uterine sinus – embryo/fetus discharges CO2 via umbilical arteries and picks up nutrients and O2 via umbilical veins 5. A. Establishment of a preferential hierarchy for tissues (Liver, Heart, Brain, Everything Else) B. Establishment of specific structures in maternal and placental unit C. Fetal Hemoglobin which has a higher affinity for oxygen than HgB A (Adult Hemoglobin) and releases it more easily 6. responsible for making all new proteins without which development CANNOT occur 7. Because it is not as active as in adult stage, the brain does not require as much blood. For example, there is no need for thermoregulation because that is done by the mother. 8. The shunt between the umbilical vein and the inferior vena cava in order to provide “best” fetal circulation. 9. It is the shunt between the right from the left atria and it provides the “second best” fetal circulation to the rest of the body. 10. It is the shunt between the pulmonary artery and aorta that assures the “third best” circulation. 11. They are the arteries on the maternal side of the placenta that “spray” blood into the uterine sinuses where the chorion will absorb nutrients and gas, etc. 12. a. In the adult heart, there is a septa between the left and right side of the heart. In the fetal heart, there is communication between the right and left atria through the foramen ovale. There is also communication between the right ventricle and the aorta through the ductus arteriosus. b. The pressure in the adult is higher on left side of the heart (because there is more pressure pumping to the systemic circulation). The pressure in the fetus is higher on the right side of the heart (because there is more pressure pumping to the collapsed lungs). c. In the adult, deoxygenated blood and oxygenated blood are kept separate. In the fetus, oxygenated blood from the umbilical veins is mixed with the deoxygenated blood from the vena cava. 13. It is the primitive heart that is formed between 2-4 week by the development of “cell clusters.” The ventral mesoderm and endoderm form two parallel lines that fuse to form a single tube. At week 3-4, the tubular heart forms three layers: the pericardium, the endocardium and myocardium. 14. 4th week of development 15. 120-140 beats per minute 16. 6th week of development 17. 16-18th week of development 18. Abnormal position of the heart, abnormalities of large blood vessels entering the heart, abnormalities of the ductus arteriosus, defect of cardiac septa, failure of the foramen ovale to close upon birth (not really developmental but important to know about) Step 4b: Deoxygenated Deoxygenated Pretty Well Oxygenated but mixed with IVC Well Oxygenated Partially Deoxygenated Well Oxygenated Please check out this website for a VERY good interactive display of the fetal circulation: http://www.indiana.edu/~anat550/cvanim/fetcirc/fetcirc.html