The Neurobiology of Stroke Rehabilitation
advertisement

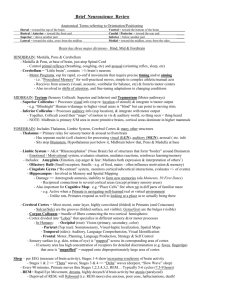
WHAT CAN NEUROBIOLOGY TELL US ABOUT THE REHABILITATION OF GOLFERS WITH CENTRAL NERVOUS SYSTEM DISEASE? Steven L. Small, M.D., Ph.D. The University of Chicago Chicago, IL Ana Solodkin, Ph.D. The University of Chicago Chicago, IL Introduction With diseases of the central nervous system (CNS), particularly cerebrovascular diseases, playing a paramount role in mortality and morbidity, the clinical and basic scientific study of acute care of CNS disease has blossomed. Concomitant advances in acute management have led both to increased survival and to increasing numbers of people with disabilities. Neurobiological study of the chronic form of these diseases has lagged behind investigation of the acute syndromes. Although the focus of this article will be on stroke, since this is the most prevalent of these diseases, the main thrust of the article equally applies to traumatic brain injury and infectious diseases, as well as to the chronic degenerative diseases, such as Parkinson’s Disease and Alzheimer’s Disease. People with expert motor skills, such as musicians and athletes, are equally affected by these diseases as are others, but the neurobiological underpinnings of the expert skill may include some additional circuits that might be an additional focus of rehabilitative efforts. Rehabilitative measures for CNS diseases are generally based on empirical concepts of functional outcome rather than on basic neurological principles. While there is significant knowledge about neuropharmacological and neuroanatomical changes that take place immediately after stroke and brain injury, and some knowledge of the neurobiology of the more chronic recovery phase, clinical neurorehabilitation does not generally use this information. The practice of rehabilitation remains rooted in empirical concepts leading to functional outcome, without any attempt to delve into the underlying biology. Whereas such information could be helpful for general motor (or sensory or cognitive) rehabilitation, it could be particularly useful in the recovery of specialized motor skills such as musical performance or sports. In the case of golfing, motor performance requires a complex interaction between brain systems for both motor planning and execution. Of the component processes involved in taking a golf shot, several involve general (non-motor) skills that have been specialized for golf, and others involve primarily motor areas of the brain. Experts and novices probably differ in the exact stages of this task, -1- with experts having highly practiced and overlearned behaviors and significant commonality among individuals, but with novices having less practiced skills that require more spontaneous motor planning and execution and are more likely to manifest large individual differences. These differences in performance suggest differences in neurobiological substrate. Expert skill at golf may resemble the overlearned simple activities of more mundane motor tasks, whereas novice performance may resemble other motor tasks that are novel and unpracticed. One plausible inference from this analogy is that the relearning of simple tasks may be akin to novel skill acquisition. Some of the attempts to alter the course of neurobiological recovery in animal models (Feeney, Gonzalez, & Law, 1982) and humans (Crisostomo, Duncan, Propst, Dawson, & Davis, 1988; McNeil, Doyle, Spencer, Goda, Flores, & Small, 1997; Small, 1994) have shown promise, but have not yet demonstrated the potential to have a major impact. In this review, we discuss several lines of research that are leading toward a neurobiological basis for rehabilitation of central nervous system injury. These efforts encompass both animal models and human studies, and focus on the chemical and/or anatomical changes occurring in the brain after stroke. This review pays special attention to those neurobiological data that might be exploited in developing a clinical neurorehabilitation that is grounded in basic scientific principles and in data that are particularly relevant to the recovery of highly skilled motor activities. Our survey begins with some general features of cerebral cortical anatomy relevant to motor recovery, considers some issues related to expert motor skill, and then discusses interventional strategies that have made use of this information as well as functional neuroimaging approaches to monitoring recovery and therapy. Aspects of Human Cortical Anatomy Prior to the most recent studies of cortical organization using functional imaging methods, most knowledge of the functional anatomy of the human cerebral cortex was derived from two sources, lesion analysis (Damasio & Damasio, 1989) of patients with focal cerebral injury and cortical electrical stimulation or recording in patients undergoing neurosurgical procedures (Ojemann, Ojemann, Lettich, & Berger, 1989). A lesion to the primary motor cortex (M1) in man (precentral gyrus; Brodmann area = BA 4) causes motor weakness in the contralateral face and limbs (Brodal, 1981). Lesions in the inferior aspects of the precentral gyrus cause weakness to the muscles of the mouth and face. More superiorly, lesions lead to weakness in the hand and arm. Lesions in the paracentral lobule cause weakness to the leg and foot. Although motor cortical lesions characteristically cause contralateral deficits, they can also produce some ipsilateral impairments, particularly when the lesion occurs on the side of the dominant hand (Kim, Ashe, Hendrich, Ellermann, Merkle, Ugurbil, & Georgopoulos, 1993). The presence of ipsilateral impairment might not be surprising, given that about 10% of fibers do not cross at the medullary decussation and are found in the lateral corticospinal tract on the same side (Brodal, 1981; Nyberg-Hanson & Rinvik, 1963). Since these ipsilateral efferent fibers innvervate proximal muscles, the ipsilateral motor deficits may reflect disruption in the complex interactions between M1 and the association motor cortices (which in fact tend to be bilateral). Hemispheric asymmetry for motor function has not received as much attention as other asymmetries, and certainly we are in the early stages of research into the complex interactions among different motor cortices(Solodkin, Hlustik, -2- Noll, & Small, 2001). Both the bilateral hemispheric innervation of the peripheral motor system and its asymmetry have important implications for neuroanatomical recovery from stroke. Direct cortical stimulation has provided the most specific details about the fine somatotopic structure of the cerebral cortex. Following the demonstration in 1870 of this method (Fritsch & Hitzig, 1870), Ferrier (1876) demonstrated a correlation between site of stimulation near the central sulcus and motor response in a macaque monkey. This technique was applied to mapping in awake patients, demonstrating somatotopy for the motor system (Penfield & Rasmussen, 1950). Interestingly, even though Penfield showed some degree of overlapping representations in his somatotopic maps, his reading audience over the years (including the authors of textbooks) has overgeneralized the concept. Using functional imaging, we have recently re-examined the extent of this somatotopy, and have described a graded overlapping topography in this region (Hlustik, Solodkin, Gullapalli, Noll, & Small, 2001a). Functional neuroimaging has confirmed the basic anatomy of the motor cortex, thus demonstrating in a reliable functional system the significant role that imaging can play in anatomical studies in human subjects. These methods have also begun to play a role in tracking recovery from (or progression of) neurological disease. Neuroimaging studies of the motor system, particularly involving finger Cognitive (Non-Motor) Assessment movements, have revealed features of Assess the functional cortical anatomy. Both distance View Choose club PET and fMRI studies demonstrate Terrain activation sites in the contralateral Assess wind primary motor cortex with finger movements (Colebatch, 1991; Grafton, Woods, Mazziotta, & E., 1991; Roland, Meyer, Shibasaki, Yamamoto, "Pre-Shot Routine" ? PM, S MA, CM A, M1 & Thompson, 1982). Some fMRI Novice: Plan studies have also demonstrated motor sequence Integrate enviipsilateral activation with these ronmental movements (Boecker, Kleinschmidt, variables Expert: Instantiate Requardt, Hanicke, Merboldt, & ? Pre-frontal motor pla n Frahm, 1994; Kim, et al., 1993). Other ? PM, CMA, BG studies have implicated the supplementary motor cortex (SMA) in complex but not simple finger Motor Execution movements (Boecker, et al., 1994; Rao, Binder, Bandettini, Hammeke, Initiate Execute Follow Yetkin, Jesmanowicz, Wong, motor motor through Estkowski, Goldstein, Haughton, & sequence sequence ?limbic Hyde, 1993). ?PM, M1 ?SMA One study that we have conducted demonstrates significant differences Figure 1: Tentative Framework for Taking a Golf Shot between brain activation patterns in left handers and right handers, and between simple and complex movements (Solodkin, et al., 2001). -3- These results have significant bearing on the understanding of advanced motor skill, including sporting and musical performance. In golf, for example, taking any form of shot, from driving the ball from the tee to putting from a short distance away, involves a complicated set of motor plans and executions. Since such performance is even more complex than the sequential movements described by Solodkin et al (2001), it would be expected that making a golf shot might require not only contralateral M1, but the other cortical motor areas as well, including ipsilateral M1 and bilateral premotor areas, both medial (cingulate motor area (CMA) and supplementary motor area (SMA)) and lateral premotor area (PM). We have recently begun an fMRI study of motor planning and execution in golfers imagining a shot, and have some unpublished pilot data suggesting that such activity may indeed involve premotor structures. Published electroencephalographic data suggest that an expert taking a golf shot requires specialized motor planning and attentional mechanisms (Crews & Landers, 1993), and based on studies of apraxia (Heilman, Maher, Greenwald, & Rothi, 1997) and imaging (Hlustik, Solodkin, Gullapalli, Noll, & Small, 1998; Hlustik, Solodkin, Noll, & Small, 2001b), we would suggest that the left lateral premotor cortex plays a special role in this pre-execution behavior. Studies of expert performance (including golfing) using electrographic methods have suggested a hemispheric difference, with left hemisphere activity diminishing just prior to execution of a complex motor skill, whether one conducted with solely the right hand (such as shooting) or those conducted with both hands (such as archery or putting). Based on a large literature in motor performance, but only limited data on expert performance, we suggest that the execution of a golf shot incorporates many subcomponents subserved by a complex interactive circuit including numerous brain regions. At the risk of over-speculation, our conception of planning and executing a golf shot appears in Figure 1. An expert golfer assesses the environment carefully prior to doing any overt motor planning or execution, and this is indicated in the Figure without comment. The motor activity related to taking a golf shot differs between experts and novices, and this is also indicated in the Figure. Overall, the expert is likely to perform a different type of planning, not only because he can maintain more selective attention than novices, but also because he likely makes access to a number of over-trained circuits related to the execution of particular golf shots. In contrast, the novice, needs more planning, since he cannot maintain the same degree of selective attention as the expert, and does not yet have these over-trained circuits that underly the experts’ representations. Under these two conditions (experts and novices), the interaction among motor areas is likely to differ significantly, since the circuits involved will subserve different actions. Acute Brain Injuries and Cerebral Cortical Plasticity Functional representations in the cerebral cortex are dynamic, with constant reshaping, remolding, and rearrangement. The most persuasive examples are the recent studies showing remarkable changes in cortical anatomy with repeated sensory (Wang, Merzenich, Sameshima, & Jenkins, 1995) or motor stimulation (Hlustik, Solodkin, Noll, & Small, 2000; Karni, Meyer, Jezzard, Adams, Turner, & Ungerleider, 1995). The ubiquity of representational changes as part of the normal functioning of the cerebral cortex should facilitate the processes of functional recovery from stroke. The overall extent and permanency of possible anatomical changes is controversial due in part to the relationship between plasticity and age. In this section, we consider several types of plasticity thought to be possible in adults, including growth of neurons themselves, axonal sprouting with new synapse -4- formation, or modification of existing synapses. Functional anatomical codes in the cerebral cortex are not static structures, but are constantly changing and reshaping with environmental influences. Changes that occur relatively fast (i.e., hours or days) include the sizes of cortical topographic regions devoted to the sensory or motor function of the digits (Gilbert, 1992; Jacobs & Donoghue, 1991). Slower alterations (i.e., months or years) occur in the process of learning new skills (e.g., complex sensorimotor skills) (Gilbert, 1992). In the case of stroke recovery, anatomical reorganization probably occurs in several phases. Evidence suggests that within the faster time frame are processes of "unmasking" existing circuits that follow pre-existing anatomical connections. On the longer time frame, axonal sprouting and synaptogenesis may mediate more substantial anatomical changes and concomitant improvements in recovery. The unmasking of existing viable circuits has been postulated to explain fast (hours to days) reorganization in motor, sensory, and visual systems after acute CNS injury (Das & Gilbert, 1995; Jacobs & Donoghue, 1991; Kaas, Krubitzer, Chino, Langston, Polley, & Blair, 1990; Keller, Weintraub, & Miyashita, 1996). In young and adult rat somatosensory cortex, for example, cortical movement representations change over a short time scale with alterations in input (tactile experience via whiskers) (Keller, et al., 1996). This was true for groups of both young and old animals. Shortterm changes in spatio-temporal reasoning have recently been demonstrated following complex musical experience (Rauscher, Shaw, & Ky, 1995). Evidence from both the visual (Das & Gilbert, 1995; Gilbert, 1992) and motor systems (Huntley, 1997) suggests that unmasking in the cerebral cortex may be mediated by the intra-cortical connection patterns present prior to a stroke. In particular, the pattern of horizontal connections between damaged and undamaged brain areas may determine the precise nature of the short-term anatomical changes that occur. The functional maps seem to shift to those areas linked to the damaged regions by these horizontal connections, and where these are absent, the maps may be incapable of shifting (Huntley, 1997; Jacobs & Donoghue, 1991). Although certain animals generate new neurons in adaptation to environmental changes (Barnea & Nottebohm, 1994), this is unlikely to be a relevant mechanism in adult stroke recovery. On the other hand, there is growing evidence that changes in behavior can lead existing neurons to change their patterns of synaptic connectivity. This has led to new receptive fields for cortical sensory neurons. Such changes have been observed in the somatosensory system with both peripheral nerve stimulation (Jenkins, Merzenich, Ochs, Allard, & Guic-Robles, 1990) and behavioral alterations (Recanzone, Allard, Jenkins, & Merzenich, 1990). In the visual system, axonal sprouting has been reported in the reorganizing adult cat striate cortex for several months following a retinal lesion (Darian-Smith & Gilbert, 1994). Dendritic proliferation may be possible in adults of all ages, including old age (Coleman & Flood, 1986). In experimental lesions of the somatosensory cortex, animals were subsequently trained on behavioral tasks to attempt to influence reorganization of cortical anatomy. Soon after the lesions, the animals used the affected hands in a limited manner, avoiding tasks requiring the type of precise somatosensory information as required for fine motor control. In this first few weeks, electrophysiological study revealed little change in the somatosensory cortical maps for the hand. However, after several months, electrophysiological recording revealed that skin areas previously encoded by the damaged region of cortex became encoded by adjacent spared cortical regions -5- (Jenkins & Merzenich, 1987). In the motor cortex, the same technique alters the cortical representations of movement (Nudo, Jenkins, & Merzenich, 1990). In cat, long-term stimulation of the ventroposterolateral nucleus of the thalamus has led to significantly increased synaptic density and synaptic active zones in M1 (Keller, Arissian, & Asanuma, 1992). These studies provide important data for neurobiological approaches to rehabilitation. It has been recognized that the behavior of a patient with a focal brain lesion, e.g., from a vascular insult, reflects less on the function the damaged region than on the function of the entire brain when it is missing that region. Many therapists believe that performance actually reflects the adaptive behavior of the entire organism (and especially the brain) in the presence of damage. The behavioral implications change from restoration of lost function to improving the functional adaptation to damage. Although this article is concerned mostly with acute CNS injuries, it is nonetheless useful to note that a strictly temporal property of vascular occlusions and traumatic injuries, i.e., their sudden onset, contributes to morbidity. By way of contrast, slow growing tumors can become quite large before affecting function at all. We recently studied patients with vascular malformations, none of whom had noticeable functional deficits, including one with a lesion affecting the inferior frontal gyrus who had a very mild dysnomia. In these patients, functional activation occurred near the region that would be expected to be involved in the target task (Witt, Konziolka, Baumann, Noll, Small, & Lunsford, 1996). This suggests that in slowly developing brain lesions, where the damage occurs in small increments over a long time period, local circuits can reorganize incrementally and successfully. In the case of larger and/or more rapidly developing lesions, such adaptation does not occur as readily. Brain regions encode functional information in a dynamic manner. In animal models, it has been possible to perform electrophysiological mapping of areas of the primary sensory and motor cortex before, during, and after altered behavior aimed at augmenting or reducing the functional responsibility of parts of these cortical regions. With practiced motor activity of certain fingers, the volume of motor cortical tissue dedicated to those fingers increased (Nudo, et al., 1990). Repetitive peripheral nerve stimulation led to reorganization of the primary sensory cortex (SI) dedicated to the stimulated area (Jenkins, et al., 1990). When two fingers were tied together and used as a single digit, the functional organization of SI changed to encode the new structure as a single digit, losing the previous cortical encoding of the inner surfaces of the two fingers (Allard, Clark, Jenkins, & Merzenich, 1991). Amputation of a finger led to reorganization of SI, with loss of the cortical encoding of the missing finger, and increase in size of the areas responsible for the adjacent fingers (Merzenich, Nelson, Stryker, Cynader, Schoppmann, & Zook, 1984). Important evidence is emerging that this cortical reshaping depends on the nature of practice, rather than simply on its presence. In an experiment with adult squirrel monkeys, goal directed motor training led to better outcomes in both performance and neuroanatomical reorganization than no training or simple motor repetition (Nudo, Wise, SiFuentes, & Milliken, 1996). Some human patients seem to exhibit "learned non-use" of a hemiparetic extremity, a maladaptive behavior pattern that can be altered by specific types of physical practice of the impaired limb while the normal limb is restrained (Taub, Miller, Novack, Cook, Fleming, Nepomuceno, Connell, & Crago, 1993). This might be important for motor rehabilitation of the skilled athlete or musician. There are a several pieces of relevant information. First is that skilled motor activities involve some of the same -6- and some different cortical structures than unskilled activities. Second is the general premise that recovery of motor function relates to reorganization of neural structures and/or employment of accessory neural structures. Third is that compensatory skill acquisition can impede remediation. Taken together, it might be the case that rehabilitation of expert golf skill requires some different (additional) approaches than rehabilitation of more mundane motor activities. This would likely depend on the precise nature of the brain lesion and the concomitant circuit disruption caused by the injury. Further, this would depend on just how much of the "expert" network was necessary to relearn the (previously) mundane motor skills, since existing evidence suggests that motor rehabilitation of even simple motor activity involves re-integrating motor plans and skills into more automatic networks, just the sort of thing requires to achieve expert proficiency at higher order motor skills. On the other hand, the expert also requires tremendous planning and attentional activity prior to task execution, something that may or may not be involved in more mundane tasks. Recovery from Brain Injuries Brain imaging has been of major importance in helping to understand brain metabolic changes that occur following acute brain injuries such as stroke. In such studies, PET scans are performed 18 during rest after the administration of [ F] fluoro-deoxyglucose (FDG), an isotope that is transported into cells with glucose, is phosphorylated as glucose, but then simply accumulates in the cell. Such scans provide data about regional brain metabolism. In patients with aphasia, it has been noted using structural imaging methods that the location of a lesion does not correlate well with symptomatology (Alexander, Naeser, & Palumbo, 1990) or with degree of recovery (Mezger & Busch, 1988). Studies of metabolism using FDG-PET have improved upon this situation to a degree, demonstrating that infarcted brain areas are not the only ones affected metabolically (Meyer, Obara, & Muramatsu, 1993). In particular, when FDG-PET hypometabolism is taken into account in defining a lesion causing aphasia, the correlation with symptomatology is better (Metter, Wasterlain, Kuhl, Hanson, & Phelps, 1981). In motor system stroke, resting metabolic PET studies have shown that recovery correlates with increased cortical metabolism in motor areas of the affected hemisphere (Di Piero, Chollet, MacCarthy, Lenzi, & Frakowiak, 1992). In contrast, patients with striatocapsular stroke (Weiller, Chollet, Friston, Wise, & Frackowiak, 1992) showed lower regional cerebral blood flow (rCBF) in the basal ganglia, thalamus, sensorimotor, insular, and dorsolateral prefrontal cortices, and in the brainstem contralateral to the side of the recovered hand and in the ipsilateral cerebellum. Increased rCBF was found in the contralateral posterior cingulate and premotor cortices, and in the caudate nucleus ipsilateral to the recovered hand. In a set of pioneering neuroimaging studies of neurological recovery using PET, the functional anatomy of the motor system was examined in groups of patients following motor system stroke (Chollet, DiPiero, Wise, Brooks, Dolan, & Frackowiak, 1991; Weiller, et al., 1992; Weiller, Ramsey, Wise, Friston, & Frackowiak, 1993). In a group of patients with different types of strokes (Chollet, et al., 1991), movement of the normal fingers led to increased rCBF in contralateral primary sensorimotor cortex and in the ipsilateral cerebellar hemisphere, whereas movement of the recovered hand showed increased rCBF in sensorimotor cortex and cerebellum bilaterally. Insula, inferior parietal, and premotor cortex were also bilaterally activated with movement of the recovered hand. Movements of the recovered hand in patients with striatocapsular infarction (Weiller, et al., 1992) activated the contralateral cortical motor areas and ipsilateral cerebellum to the same extent as did -7- normal subjects, but showed increased activation in both insulae, inferior parietal (area 40), prefrontal, and anterior cingulate cortices, ipsilateral premotor cortex and basal ganglia, and contralateral cerebellum. A follow-up to these studies (Weiller, et al., 1993) examined individual variability in this reorganizing anatomy. In comparing individual patients with the averaged results from normal subjects, it was found that most recovering stroke patients had increased activation of the ipsilateral premotor cortex and about half in the contralateral primary motor cortex. Increased activation levels occurred in other patients in combinations of ipsilateral and bilateral regions of the insula, parietal cortex, prefrontal cortex, cerebellum, and anterior cingulate. Biological Approaches to Treatment of Chronic Neurological Injury During the initial phases of acute CNS injury, a wide variety of homeostatic mechanisms supervene. The nature of these changes and their significance to the overall degree of brain injury and development of morbidity is of great current interest (Coull, 1996). Additional biological changes occur during the subsequent subacute and chronic stages of recovery, some of which might be influenced to improve recovery. A small effort in the pharmacology of neurorehabilitation has led to some interesting results. Studies of catecholamine systems in animal models of stroke have attracted the most interest, with the acute decreases in catecholamine concentration in the cortex and brainstem of the rat persisting chronically, including a decrease in the concentration of norepinephrine (NE) in the ipsilateral cortex and brainstem, and a decrease in the concentration of dopamine (DA) in the ipsilateral brainstem but not cortex (Robinson, Shoemaker, Schlumpf, Valk, & Bloom, 1975). Bilateral reduction of glucose utilization in the cortex and locus coeruleus (LC) and in the ipsilateral red nucleus are also present (Feeney, Sutton, Boyeson, Hovda, & Dail, 1985). Intravenous interventions with dextro-amphetamine, haloperidol, and phenoxybenzamine have suggested that both dopamine and norepinephrine (via 1 receptors) might play a role in mediating recovery. In general, the beneficial effects of catecholamines are only seen when drug intervention is accompanied by experience (Small, 1994). Dextro-amphetamine has been used in several human studies of motor and language recovery, all suggesting some degree of benefit (Small, 2001). As in the case of experimental animals, the beneficial effects of dextro-amphetamine seem to supervene only in the context of concomitant behavioral or physical therapy. Whether or not such pharmacological adjuncts could play a role in recovery of expert skill remains open. Summary and Conclusions Neurobiology can and must contribute to the study of central nervous system rehabilitation: although recovery of human performance following brain injuries undoubtedly depends on both acute and chronic recovery processes in the brain, clinical neurology only plays a role in the acute setting. With a neurobiological approach to rehabilitation, this situation will change. Furthermore, as discussed here, it will be possible to use specialized neurobiological insights regarding the specific skill set of an individual to tailor therapy toward the critical neural circuits and/or reorganizational -8- mechanisms. In the case of expert motor skill, the relevant networks include bilateral premotor areas, both medial and lateral, as well as frontal and parietal areas that focus on memory and attention. It is only by further study of these mechanisms in skilled performers will the full array of possibilities become clear. At no point do we expect to uncover a phrenological "golf" area of the brain. Nor do we expect to uncover circuits that are specific to golf at the exclusion of other skills. On the other hand, we do expect that expert golfers make use of highly overtrained neural networks, and that by adapting rehabilitative training to these networks, whether by golfing or through other types of activities (e.g., selective attentional tasks, related motor planning tasks), individualized therapeutic gains might be possible. Four main points should be summarized. First, the anatomical organizations of functional brain systems are less topographically precise as commonly believed and are highly variable across individuals. Second, that cortical plasticity exists in adults and takes a number of forms, including unmasking of existing circuits, growth of new synapses via axonal sprouting or dendritic proliferation, and development of compensatory processes. Third, that is it possible to manipulate this plasticity with behavioral and pharmacological interventions, and that such manipulation can have a beneficial effect on recovery. Fourth, that by understanding the neural circuits underlying unusual skills, these interventions might be tailored to rehabilitative gains in specialized areas. Finally, it is our belief that functional neuroimaging, particularly the non-invasive method of fMRI, can be used to study in vivo cerebral plasticity in normal skill acquisition as well as in recovery from CNS injury. In addition, this method can play a role in assessing the mechanisms and efficacy of interventions aiming to influence recovery by affecting this plasticity. Acknowledgments The support of the National Institutes of Health under grant NS-1-R01-37195 is gratefully acknowledged. -9- References Alexander, M. P., Naeser, M. A., & Palumbo, C. (1990). Broca's Area Aphasias: Aphasia after Lesions including the Frontal Operculum. Neurology, 40(2), 353-62. Allard, T., Clark, S. A., Jenkins, W. M., & Merzenich, M. M. (1991). Reorganization of Somatosensory Area 3b Representations in Adult Owl Monkeys after Digit Syndactyly. Journal of Neurophysiology, 66(3), 1048-1058. Barnea, A., & Nottebohm, F. (1994). Seasonal Recruitment of Hippocampal Neurons in Adult FreeRanging Black-Capped Chickadees. Proceedings of the National Academy of Sciences of the United States of America, 91, 11217-11221. Boecker, H., Kleinschmidt, A., Requardt, M., Hanicke, W., Merboldt, K. D., & Frahm, J. (1994). Functional cooperativity of human cortical motor areas during self- paced simple finger movements. A high-resolution MRI study. Brain, 117(Pt 6), 1231-9. Brodal, A. (1981). Neurological Anatomy in Relation to Clinical Medicine (Third ed.). New York: Oxford University Press. Chollet, F., DiPiero, V., Wise, R. J. S., Brooks, D. J., Dolan, R. J., & Frackowiak, R. S. J. (1991). The Functional Anatomy of Motor Recovery after Stroke in Humans: A Study with Positron Emission Tomography. Annals of Neurology, 29, 63-71. Colebatch, J. G. (1991). Regional Cerebral Blood Flow during Voluntary Arm and Hand Movements in Human Subjects. Journal of Neurophysiology, 65, 1392-1401. Coleman, P. D., & Flood, D. G. (1986). Dendritic Proliferation in the Aging Brain as a Compensatory Repair Mechanism. Progress in Brain Research, 70:, 227-237. Coull, B. M. (1996). The Many Windows of Therapeutic Opportunities in Stroke. Current Opinion in Neurology, 9(1), 43-45. Crews, D. J., & Landers, D. M. (1993). Electroencephalographic Measures of Attentional Patterns Prior to the Golf Putt. Medicine and Science in Sports and Exercise, 25(1), 116-126. - 10 - Crisostomo, E. A., Duncan, P. W., Propst, M., Dawson, D. V., & Davis, J. N. (1988). Evidence that Amphetamine with Physical Therapy Promotes Recovery of Motor Function in Stroke Patients. Annals of Neurology, 23, 94-97. Damasio, H., & Damasio, A. R. (1989). Lesion Analysis in Neuropsychology. New York: Oxford University Press. Darian-Smith, C., & Gilbert, C. D. (1994). Axonal Sprouting Accompanies Functional Reorganization in Adult Cat Striate Cortex. Nature, 368, 737-40. Das, A., & Gilbert, C. D. (1995). Long-Range Horizontal Connections and their Role in Cortical Reorganization Revealed by Optical Recording of Cat Primary Visual Cortex. Nature, 375, 7804. Di Piero, V., Chollet, F. M., MacCarthy, P., Lenzi, G. L., & Frakowiak, R. S. J. (1992). Motor Recovery after Acute Ischaemic Stroke: A Metabolic Study. Journal of Neurology, Neurosurgery, and Psychiatry, 55, 990-996. Feeney, D. M., Gonzalez, A., & Law, W. A. (1982). Amphetamine, Haloperidol, and Experience Interact to Affect Rate of Recovery After Motor Cortex Injury. Science, 217, 855-857. Feeney, D. M., Sutton, R. L., Boyeson, M. G., Hovda, D. A., & Dail, W. G. (1985). The Locus Coeruleus and Cerebral Metabolism: Recovery of Function after Cortical Injury. Physiological Psychology, 13(3), 197-203. Ferrier, D. (1876). Functions of the Brain. London: Smith, Elder. Fritsch, G., & Hitzig, E. (1870). Ueber die Elektrische Erregbarkeit des Grosshirns. Arch Anat Physiol Wiss Med, 37, 300-332. Gilbert, C. D. (1992). Horizontal Integration and Cortical Dynamics. Neuron, 9, 1-13. Grafton, S. T., Woods, R. P., Mazziotta, J. C., & E., P. M. (1991). Somatotopic Mapping of the Primary Motor Cortex in Humans: Activation Studies with Cerebral Blood Flow with Positron Emission Tomography. Journal of Neurophysiology, 66, 735-743. Heilman, K. M., Maher, L. M., Greenwald, M. L., & Rothi, L. J. (1997). Conceptual apraxia from lateralized lesions. Neurology, 49(2), 457-64. - 11 - Hlustik, P., Solodkin, A., Gullapalli, R. P., Noll, D. C., & Small, S. L. (1998). Simple and Complex Finger Movements of Either Hand Activate the Left Lateral Premotor Cortex (abstract). Neurology, 50(4), A177. Hlustik, P., Solodkin, A., Gullapalli, R. P., Noll, D. C., & Small, S. L. (2001a). Somatotopy in human primary motor and somatosensory hand areas revisited. Cerebral Cortex, (in press). Hlustik, P., Solodkin, A., Noll, D. C., & Small, S. L. (2000). Complex Motor Hand Learning Generalizes Behaviorally and Anatomically. In 2000 Meeting of the Society for Human Brain Mapping. San Antonio, Texas. Hlustik, P., Solodkin, A., Noll, D. C., & Small, S. L. (2001b). Simple and Complex Finger Movements of Either Hand Activate the Left Lateral Premotor Cortex (abstract). Brain and Cognition, (submitted). Huntley, G. W. (1997). Correlation between Patterns of Horizontal Connectivity and the Extent of Short-Term Representational Plasticity in Rat Motor Cortex. Cerebral Cortex, 7, 143-156. Jacobs, K. M., & Donoghue, J. P. (1991). Reshaping the Cortical Motor Map by Unmasking Latent Intracortical Connections. Science, 251, 944-947. Jenkins, W. M., & Merzenich, M. M. (1987). Reorganization of neocortical representations after brain injury: A neurophysiological model of the bases of recovery from stroke. Progress in Brain Research, 71, 241-266. Jenkins, W. M., Merzenich, M. M., Ochs, M. T., Allard, T., & Gu'ic-Robles, E. (1990). ReceptiveField Changes Induced by Peripheral Nerve Stimulation in SI of Adult Cats. Journal of Neurophysiology, 63, 82-104. Kaas, J. H., Krubitzer, L. A., Chino, Y. M., Langston, A. L., Polley, E. H., & Blair, N. (1990). Reorganization of Retinotopic Cortical Maps in Adult Mammals After Lesions of the Retina. Science, 248, 229-231. Karni, A., Meyer, G., Jezzard, P., Adams, M. M., Turner, R., & Ungerleider, L. G. (1995). Functional MRI Evidence for Adult Motor Cortex Plasticity during Motor Skill Learning. Nature, 377, 155-158. - 12 - Keller, A., Arissian, K., & Asanuma, H. (1992). Synaptic Proliferation in the Motor Cortex of Adult Cats after Long-Term Thalamic Stimulation. Journal of Neurophysiology, 68(1), 295-308. Keller, A., Weintraub, N. D., & Miyashita, E. (1996). Tactile Experience Determines the Organization of Movement Representations in Rat Motor Cortex. NeuroReport, 7(14), 23722378. Kim, S.-G., Ashe, J., Hendrich, K., Ellermann, J. M., Merkle, H., Ugurbil, K., & Georgopoulos, A. P. (1993). Functional Magnetic Resonance Imaging of Motor Cortex: Hemispheric Asymmetry and Handedness. Science, 261, 615-617. McNeil, M. R., Doyle, P. J., Spencer, K. A., Goda, A. J., Flores, D., & Small, S. L. (1997). A DoubleBlind, Placebo-Controlled Study of Pharmacological and Behavioural Treatment of LexicalSemantic Deficits in Aphasia. Aphasiology, 11(4/5), 385-400. Merzenich, M. M., Nelson, R. J., Stryker, M. P., Cynader, M. S., Schoppmann, A., & Zook, J. M. (1984). Somatosensory Cortical Map Changes Following Digit Amputation in Adult Monkeys. Journal of Comparative Anatomy, 224, 591-605. Metter, E. J., Wasterlain, C. G., Kuhl, D. E., Hanson, W. R., & Phelps, M. E. (1981). 18FDG Positron Emission Computed Tomography in a Study of Aphasia. Annals of Neurology, 10, 173-183. Meyer, J. S., Obara, K., & Muramatsu, K. (1993). Diaschesis. Neurological Research, 15, 362-366. Mezger, G., & Busch, G. (1988). Rehabilitation Prognosis Of Aphasias Of Various Etiologies With Reference To Clinical, Neurolinguistic And Computerized Tomography Findings. Rehabilitation, 27(2), 80-84. Nudo, R. J., Jenkins, W. M., & Merzenich, M. M. (1990). Repetitive Microstimulation Alters the Cortical Representation of Movements in Adult Rats. Somatosensory and Motor Research, 7, 463-483. Nudo, R. J., Wise, B. M., SiFuentes, F., & Milliken, G. W. (1996). Neural substrates for the effects of rehabilitative training on motor recovery after ischemic infarct. Science, 272(5269), 1791-1794. Nyberg-Hanson, R., & Rinvik, E. (1963). Some Comments on the Pyrimidal Tract with Special Reference to its Individual Variation in Man. Acta Neurologica Scandinavica, 39, 1-30. - 13 - Ojemann, G., Ojemann, J., Lettich, E., & Berger, M. (1989). Cortical Language Localization in Left, Dominant Hemisphere: An Electrical Stimulation Mapping Investigation in 117 Patients. Journal of Neurosurgery, 71, 316-326. Penfield, W., & Rasmussen, T. (1950). The Cerebral Cortex of Man. New York: MacMillan. Rao, S. M., Binder, J. R., Bandettini, P. A., Hammeke, T. A., Yetkin, F. Z., Jesmanowicz, A., Wong, E. C., Estkowski, L. D., Goldstein, M. D., Haughton, V. M., & Hyde, J. S. (1993). Functional Magnetic Resonance Imaging of Complex Human Movements. Neurology, 43, 2311-2318. Rauscher, F. H., Shaw, G. L., & Ky, K. N. (1995). Listening to Mozart Enhances Spatial-Temporal Reasoning: Towards a Neurophysiological Basis. Neuroscience Letters, 185(1), 44-7. Recanzone, G. H., Allard, T. T., Jenkins, W. M., & Merzenich, M. M. (1990). Receptive-Field Changes Induced by Peripheral Nerve Stimulation in SI of Adult Cats. Journal of Neurophysiology, 63, 1213-1225. Robinson, R. G., Shoemaker, W. J., Schlumpf, M., Valk, T., & Bloom, F. E. (1975). Effect of Experimental Cerebral Infarction in Rat Brain on Catecholamines and Behavior. Nature, 255, 332-334. Roland, P. E., Meyer, E., Shibasaki, T., Yamamoto, Y. L., & Thompson, C. J. (1982). Regional Cerebral Blood Flow Changes in Cortex and Basal Ganglia during Voluntary Movements in Normal Human Volunteers. Journal of Neurophysiology, 48, 467-480. Small, S. L. (1994). Pharmacotherapy of Aphasia: A Critical Review. Stroke, 25(6), 1282-1289. Small, S. L. (2001). Biological Approaches to the Treatment of Aphasia. In A. Hillis (Eds.), Handbook on Adult Language Disorders: Integrating Cognitive Neuropsychology, Neurology, and Rehabilitation (pp. (in press)). Philadelphia, Pennsylvania: Psychology Press. Solodkin, A., Hlustik, P., Noll, D. C., & Small, S. L. (2001). Lateralization of Motor Circuits during Simple and Complex Finger Movements. European Journal of Neurology, (in press). Taub, E., Miller, N. E., Novack, T. A., Cook, E. W., 3d, Fleming, W. C., Nepomuceno, C. S., Connell, J. S., & Crago, J. E. (1993). Technique to Improve Chronic Motor Deficit after Stroke. Archives of Physical Medicine and Rehabilitation, 74(4), 347-354. - 14 - Wang, X., Merzenich, M. M., Sameshima, K., & Jenkins, W. M. (1995). Remodelling of Hand Representation in Adult Cortex Determined by Timing of Tactile Stimulation. Nature, 378, 7175. Weiller, C., Chollet, F., Friston, K., Wise, R. J. S., & Frackowiak, R. S. J. (1992). Functional reorganization of the brain in recovery from striatocapsular infarction in man. Annals of Neurology, 31, 463-472. Weiller, C., Ramsey, S. C., Wise, R. J. S., Friston, K., & Frackowiak, R. S. J. (1993). Individual Patterns of Functional Reorganization of the Human Cerebral Cortex after Capsular Infarction. Annals of Neurology, 33, 181-189. Witt, T. C., Konziolka, D., Baumann, S., Noll, D. C., Small, S. L., & Lunsford, L. D. (1996). PreOperative Cortical Localization with Functional MRI for Use in Stereotactic Radiosurgery. Stereotactic and Functional Neurosurgery, 66, 24-29. - 15 -