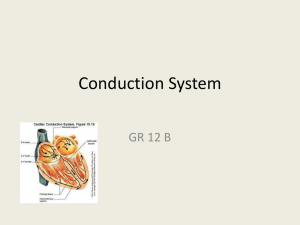
The heart: • cells that generate impulses = pacemaker system • cells
advertisement

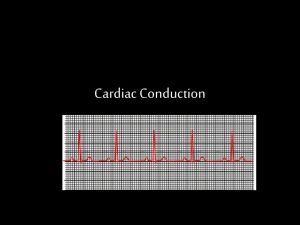
The heart: • cells that generate impulses = pacemaker system • cells that conduct impulses = conduction system • cells that respond to electrical impulses = working myocardium rhythmicity: the frequency and regularity of pacemaking activity are intrinsic to the heart all-or-none response: an impulse arising at any part of the heart→ copmlete contraction of both ventricle and atria or to none • • • a pacemaker potential- no constant resting potential = the cell potential in sinoatrial node→ slow depolarization immediately after each repolarization MDP = maximum diastolic potential- the most negative diastolic cell potential (-70 mV) PP = prepotential = the slow diastolic depolarization→ threshold potential (TP)→ triggering of action potential (AP) AP → voltage-gated Ca channels (associated with dihydropiridine receptors) in the sarcolemma of myocardial cells opened → Ca influx from extracellular fluid → local increase in cytosolic Ca triggers ligand-gated ryanodine-sensitive Ca channels in the sarcoplasmic reticulum →↑ Ca in cytosol → electromechanical coupling → myocardial contraction → active Ca transport back 1. into Ca stores by Ca-ATPase (SERCA), 2. to extracellular fluid by Ca-ATPase and 3Na/Ca exchange carrier driven by electrochemical Na gradient established by Na-K-ATP-ase rate of impulse generation in SA node (pacemaker)→ heart rate (sinus rhythm at rest: 60-100 beat per min) • the intrinsic rhythms of other pacemakers- slower than sinus rhythm (slope of their PPs- flatter) Working myocardium: voltage-gated fast Na channels • chronotropism- rate of impulse genration by the pacemaker (firing frequency of SA node)→ heart rate • dromotropism (velocity of impulse conduction; AV node!!!) • inotropism (heart contractily = force of working muscle contr.) pathological changes in impulse generation or conduction (visible in ECG) disturbances in impulse generation (normal- nomotopic impulses generated): 1. sinus tachycardia (> 100/min) 2. sinus bradycardia (< 60/min) (1,2: the rate is regular) 3. sinus arrhythmias (the rate varies) ectopic pacemakers: focus in atrium, AV node, ventricles→ abnormal ectopic (heterotopic) impulses generated (+/- nomotopic –sinus impulses genrated): 1. atrial tachycardia→ ventricular response rate > 200/min (only second/third stimulus transmitted to the ventricles (Purkinje= frequency fibers) 2. atrial flutter >350/min→ totally irregular ventricular stimulation 3. extrasystoles in ventricles→ ventricular tachycardia→ inadequate ventricular filling → ↓ stroke volume 4. ventricular fibrillation (uncoordinated contr.) AV conductance disturbed→ AV block: 1. first-degree: prolonged, normal impulse conduction in AV node (PQ interval > 0,2 sec) 2. second-degree: every second/third impulse conducted (2:1, 3:1) 3. third-degree: no impulses conducted→ ventricular atopic pacemakers take over (ventricular bradycardia with normal atrial excitation rate)→ heart rate 40-55/min (AV node is pacemaker) or 25-40/min (ventricular pacemaker)→ sudden cardiac arrest (AdamesStock attack; syncope) Bundle- branch block arrhythmia→ abnormality in • impulse generation • impulse conduction • both because of ◊ ischemia of heart muscle (infarction, ↑oxygen demand, anemia) ◊ endocrinological disturbances (hypothyroidism) ◊ electrolyte imbalance ◊ excess of catecholamines/ACh/↑ sensitivity to transmitters ◊ autonomic nervous system influence ◊ heart muscle infarction→ scar formation ◊ drugs (TCA, thyroid hormones prep., antiarrhythmics) ◊ toxins ◊ alcohol ◊ stimulants: caffeine, nicotine Antidysrhythmic drugs Class I: drugs that block voltage-sensitive sodium channels (fast current) They are subdivided: Ia, Ib, Ic Class II: beta-adrenoceptor antagonists Class III: drugs that substantially prolong the cardiac action potential (↑repolarization phase) Class IV: calcium channel antagonists Effects of antidysrhythmic drugs on the different phases of the cardiac action potentials Pacemarker potential Phase 4 Class II Rapid depolarisation Phase 0 Class I Plateau Phase 2 Class IV Class II Repolarisation Phase 3 Class III (and Ia) Vaughan Williams’s classification of antidysrhythmic drugs Ia Dysopyramide: sodium channel block intermediate dissociation Ib Lidokaine: sodium channel block fast dissociation Ic Flecainide: sodium channel block slow dissociation II Propranolol: beta-adrenoceptor antagonism III Amiodarone Sotalol: potassium channel block IV Verapamil: calcium channel block Antidysrhythmic drugs unclassified in the Vaughan William’s system Atropine used in sinus bradycardia Adrenaline (epinephrine) used in cardiac arrest Isoprenaline used in heart block Digoxin used in rapid atrial fibrillation Adenosine used in supraventricular tachycardia Calcium chloride used in ventricular tachycardia Magnesium chloride used in ventricular fibrillation and in case of digoxin toxicity