Perception of Faces and Bodies
Similar or Different?
Virginia Slaughter,1 Valerie E. Stone,2 and Catherine Reed3
1Early Cognitive Development Unit and 2Cognitive Neuroscience, School of
Psychology, University of Queensland,
Brisbane, Australia, and 3Developmental Cognitive Neuroscience Program,
Psychology Department, University of Denver
ABSTRACT—Human faces and bodies are both complex and
interesting perceptual objects, and both convey important
social information. Given these similarities between faces
and bodies, we can ask how similar are the visual
processing mechanisms used to recognize them. It has long
been argued that faces are subject to dedicated and unique
perceptual processes, but until recently, relatively little
research has focused on how we perceive the human body.
Some recent paradigms indicate that faces and bodies are
processed differently; others show similarities in face and
body perception. These similarities and differences depend
on the type of perceptual task and the level of
processing involved. Future research should take these
issues into account.
KEYWORDS—object recognition; face perception; body
schema; social information processing
1
Probably the most important and complex objects we perceive
are other humans. From the time we are born, other humans
capture our attention and elicit complex behaviors from us. We
can identify other humans as humans because they possess both
a human face and a human body. Further, we identify specific
individuals not only on the basis of their unique faces and body
shapes, but also on the basis of their characteristic expressions,
postures, and movements. Given these functional similarities
between faces and bodies, how similar are the visual processing
mechanisms used to recognize them?
FACES AS SPECIAL OBJECTS
It has long been argued that the visual system uses special
perceptual processing for faces that is different from the
processing used for other objects. The rationale is that faces are
such significant social stimuli that natural selection acted to
create dedicated face-processing mechanisms in the brain. There
is evidence consistent with the idea that faces are special: From
early in development, infants are biased to look at faces more
than other complex objects (Johnson & Morton, 1991). Also,
adult perception of faces reveals unique effects, including the
inversion effect (upside-down faces are more difficult to recognize
than other complex inverted stimuli) and the caricature
effect (a face with its distinctive features exaggerated is easier to
2
recognize than the original face). Event-related potential studies,
which measure the timing of the brain’s electrical responses to
stimuli, show that the brain responds differently to faces than to
other objects within 170 ms after they are presented. Functional
magnetic resonance imaging (fMRI) research, showing activity in
the brain while participants are actively performing perceptual
or cognitive tasks, further suggests that distinct brain areas respond
to faces compared with other objects.
However, not all researchers agree that these apparently facespecific
phenomena genuinely reflect unique processing of faces.
Some authors suggest that responses to faces are driven by the
abstract perceptual features of faces, such as symmetry or high
contrast, rather than their face-ness per se (Turati, Simion, Milani,
& Umilta, 2002). Others argue that the apparently special
processing faces receive simply reflects the ubiquity and importance
of faces, and that the perceptual effects adults exhibit
when viewing faces will be evident for any objects that they are
highly practiced at perceiving (e.g., cars for car enthusiasts or
dogs for dog breeders; Tanaka & Gauthier, 1997). These authors
propose that visual expertise changes the way that objects are
processed: Within a given domain, novices recognize objects by
focusing on their distinctive parts, but experts rely on configural
processing, focusing on the spatial relationships between parts.
3
The argument is that configural processing in general can explain
perceptual effects that appear to distinguish faces.
BODIES ARE SPECIAL, TOO
Another class of objects that may be subject to special
processing is human bodies. Although there has been relatively
little research on perception of the human body compared with
Address correspondence to Virginia Slaughter, School of Psychology,
University of Queensland, Brisbane, 4072 Australia; e-mail: vps@
psy.uq.edu.au.
CURRENT DIRECTIONS IN PSYCHOLOGICAL SCIENCE
Volume 13—Number 6 Copyright r 2004 American Psychological Society 219
that of faces, several similarities between faces and bodies
suggest that they may be processed similarly. First, bodies and
faces share a number of abstract configural properties that may
make the perceptual system treat them similarly. All faces
share the same set of parts (eyes, nose, mouth, etc.), as do all
bodies (arms, legs, torso, etc.). As a result, for both faces
and bodies, perceptual distinctions depend on the exact shape
and position of component parts. Also, from the front, both
faces and bodies are symmetrical along the vertical axis. Further,
the spatial relationships between parts of faces and between
parts of bodies are relatively fixed. Across individuals,
the configural arrangement of the eyes, nose, and mouth of the
4
face is relatively unchanging, as is the arrangement of the head,
torso, and limbs.
Second, faces and bodies are both salient conveyors of social
information. Both provide information about other individuals’
attentional and emotional states, and inform basic social categorizations,
including attributions of age, gender, and attractiveness.
Faces and bodies are both used for communication.
Finally, our embodied internal experience of both faces and
bodies could distinguish them as special object classes. Our
ability to move and functionally use our faces and bodies could
influence the visual recognition of other faces and bodies. Recent
neurophysiological studies with monkeys have revealed a
class of mirror neurons, so called because the same neurons are
active whether a given motor action is performed or observed.
There is some indirect evidence that similar motor-mirroring
structures exist in humans (see Gallese & Goldman, 1998, for
a review), suggesting that visual and motor representations interact.
The ability both to see faces and bodies and to move our
own faces and bodies may make them similarly unique compared
with other perceptual objects.
Despite these arguments for special perceptual processing of
bodies, there are also reasons to suppose that faces and bodies
may be treated differently by the visual system. The nature of
5
the information conveyed by faces and bodies is arguably different.
Faces, although often moving, are perceptually informative
even while still. We can make judgments about another
person’s gender, identity, emotion, attractiveness, and direction
of attention (conveyed most saliently in eye gaze) from a still
photograph of the face. Bodies, in contrast, are typically moving,
and much of the information that bodies convey is in dynamic
movement. We can identify another person’s gender,
emotion, and direction of attention from that person’s body most
easily if it is in motion.
Thus, it remains an open question whether the visual system
applies similar or different perceptual processes to faces and
bodies. Insight into this question may be gained by considering
two factors. First, the various ways that scientists measure face
and body perception may place more or less difficult demands
on the visual system. Second, patterns in the development of
face perception and of body perception may give insight into
how and when faces are treated similarly by the visual system.
LEVELS OF PERCEPTUAL PROCESSING OF FACES
AND BODIES
Perception of faces or bodies is a multistage process. The extent
to which faces and bodies are treated similarly by the perceptual
system depends on the stage of processing, and thus the
6
type of perceptual task participants are asked to perform. It may
be useful to distinguish two stages of perceptual processing and
two types of perceptual tasks: detection versus recognition.
Face or body detection refers to the ability to determine whether
a particular stimulus is a face or a body rather than something
else, and is an early stage of visual processing. Paradigms that
compare participants’ responses to faces or bodies with their
responses to other types of objects are measuring detection.
Face or body recognition is a later stage of visual processing
and involves making distinctions between individuals within a
category. Recognition is often tested by asking participants to
distinguish individual faces or bodies. Recognition processes
are invoked not only for identifying individual persons, but also
for identifying specific body postures (e.g., sitting vs. running)
and specific facial expressions (e.g., happy vs. angry).
Detection of Faces and Bodies
Recent work has shown that the developmental time courses for
detecting human faces and bodies are different. When young
infants are presented with a typical human face image and a
scrambled human face image in which the eyes, nose, and
mouth are moved to noncanonical locations, they prefer to look
at the typical face (Johnson & Morton, 1991). Thus, in this task,
infants detect the presence of a face (as opposed to a scrambled
7
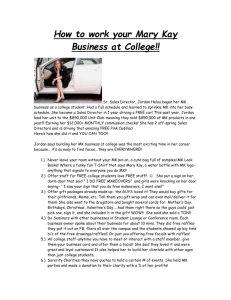
nonface). A recent study used a similar experimental procedure
to investigate development of human body perception
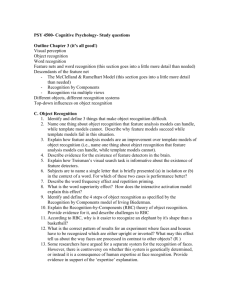
(Slaughter, Heron, & Sim, 2002). Infants between the ages of 12
and 18 months were shown typical and scrambled images of
human bodies (see Fig. 1) as well as facelike stimuli, and their
looking preferences were measured. The data indicated differences
in the way infants responded to faces and bodies. Infants
younger than 18 months of age did not show a preference for
typical or scrambled body pictures, suggesting that they did not
notice the differences between them, yet these young infants
clearly preferred the typical face to the scrambled face. By 18
months of age, infants looked longer at the scrambled than at the
typical body pictures, presumably because they found the
scrambled images novel or surprising. These developmental
data indicate that infants’ perceptual expectations about typical
human faces develop much earlier than their expectations about
human bodies.
Adults also show a dissociation between face and body detection.
In recent fMRI studies, distinct brain regions were
activated when participants viewed pictures of faces, bodies, or
body parts. Detection of faces consistently correlated with activation
in the fusiform face area, located in the ventral temporal
220 Volume 13—Number 6
8
Face and Body Perception
lobe (the underneath surface of the brain toward the back;
Kanwisher, McDermott, & Chun, 1997). In contrast, the extrastriate
body area, located in the lateral occipitotemporal cortex
(the lower left or right outside surface of the brain toward the
back), was active only when participants were shown images of
the human body or body parts (Downing, Jiang, Shuman, &
Kanwisher, 2001). The extrastriate body area does not respond
to images of faces.
Thus, both in infancy and in adulthood, there are demonstrated
differences in basic perceptual detection of human faces
and bodies.
Recognition of Faces and Bodies
In contrast to the data on detection, data on face and body
recognition reveal some similarity in how adults process faces
and bodies. Without explicit training, people should be experts
at recognizing both individual faces and individual body postures,
because of their ubiquity in everyday life. If perceptual
expertise means that visual recognition relies on configural
processing, then one would expect that both faces and bodies
would be most easily recognized by the spatial arrangement of
their component parts. The inversion effect, in which recognition
of objects is disrupted by turning them upside down, is
9
traditionally considered an indicator of configural processing
because inverting a familiar object makes it more difficult to
recognize relations between the parts. The inversion effect has
been demonstrated for faces and also for other objects when
viewed by experts (e.g., dog breeders, car experts). A recent
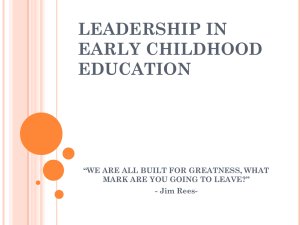
study (Reed, Stone, Bozova, & Tanaka, 2003) demonstrated that
adults show similar inversion effects for faces and body postures:
Both faces and bodies are more difficult to recognize when
presented upside down than when presented right side up, but
the same is not true of other complex stimuli, such as houses
(see Fig. 2). It appears that both face and body-posture recognition
depend on mentally representing the spatial configuration
of stimulus parts.
Despite this similarity in the recognition of faces and bodies,
there are suggestions of differences in recognition processes as
well. Evidence from neuropsychological patients indicates a
dissociation between face and body recognition. In prosopagnosia,
patients are unable to recognize individual faces—a
recognition problem that can be independent from difficulties
with recognition of other objects. This pattern of visual recognition
problems suggests that these patients have damage to a
specialized face-processing area in the brain. The disorder
autotopagnosia (or somatotopagnosia) affects patients’ ability to
10
recognize, point to, or name specific body parts within the
context of a whole body, although these patients have no difficulty
naming parts of other complex objects (e.g., Ogden, 1985).
Though each of these disorders is distinct from general object
recognition problems, prosopagnosia and autotopagnosia do not
typically occur together. The existence of these two distinct
neuropsychological disorders, one affecting face recognition
and the other body-part recognition, suggests that recognition of
faces and recognition of bodies involve some distinct processes.
CONCLUSIONS
The studies reviewed here provide evidence for both similarities
and differences in the way we perceive faces and bodies. Detection
tasks have demonstrated mostly differences: developmental
differences in responses to typical and scrambled faces
versus bodies, and activation of different brain areas for face
versus body processing in adults. Recognition tasks have shown
similarity between perception of faces and perception of bodies,
in the effects of expertise and inversion. But there are also some
differences in face and body recognition: Prosopagnosia and
autotopagnosia reveal independent deficits for recognition of
faces and bodies and do not co-occur.
0
500
11
1000
1500
2000
2500
3000
3500
4000
4500
LOOKING TIMES LOOKING TIMES
12-month-olds 15-month-olds 18-month- olds
0
1000
2000
3000
4000
5000
6000
12-month-olds 15-month-olds 18-month-olds
Fig. 1. Mean looking times (in milliseconds) to images of human bodies
(top) and facelike stimuli (bottom) with typical (white bars) and scrambled
(black bars) arrangements of parts. Results are presented separately for
12-, 15-, and 18-month-olds. From Slaughter, Heron, and Sim (2002).
Volume 13—Number 6 221
12
Virginia Slaughter, Valerie E. Stone, and Catherine Reed
This complex pattern may be explained in terms of the levels
of processing involved. Detection tasks appear to tap into relatively
basic visual categorization processes, possibly processes
depending on simple spatial properties. Thus, the evidence
from such tasks suggests the initial identification of faces and
bodies as such occurs in distinct areas of the brain. Recognition
tasks, in contrast, may recruit several different complex processes
that analyze configural properties, identify individuals,
and assign meaning. Some processing, such as the configural
processing affected by expertise, may operate similarly for faces
and bodies. Other recognition processing (e.g., how parts are
represented relative to the whole or how the motion of parts is
represented) may operate differently for faces and bodies.
DIRECTIONS FOR FUTURE RESEARCH
Understanding the extent to which faces and bodies are treated
similarly in visual processing will require more work that explicitly
contrasts responses to faces, bodies, and other complex
objects. Furthermore, it will be important for such work to define
carefully the level of processing being tested. Detection paradigms
involve differentiating faces and bodies from other objects
or scrambled stimuli. The developmental work to date has focused
on body detection, but can be expanded to explore the
13
development of body recognition. At what stage of development
would infants recognize individual, meaningful body postures?
Recognition encompasses a variety of processes, depending
on what about the face or body is being represented in the mind.
Inversion and discrimination studies, for example, test whether
participants are sensitive to relatively small changes in configuration,
and performance in these studies thus may not depend
on representing the whole object. Paradigms that test how
well parts are recognized within the whole or individually (e.g.,
tests used with autotopagnosics) may tap into a different level of
processing, at which the structure of the whole object and the
relationship of parts to that whole are represented. Processing of
bodies and processing of faces may therefore be similar in some
recognition tasks, but different in others, depending on the level
of processing involved. Detailed work testing recognition at
Fig. 2. Examples of stimuli and results from a study on ability to recognize upright
and inverted stimuli. On each trial, two stimuli, which could be
either the same or different, were presented in either upright or inverted orientation.
The task was to indicate whether the stimuli were identical.
The graphs show the percentage of trials on which participants responded
incorrectly. From Reed, Stone, Bozova, and Tanaka (2003).
222 Volume 13—Number 6
Face and Body Perception
14
different levels of processing can help clarify the levels at which
bodies and faces share processing and mental representations
and the levels at which they do not.
Finally, further work on this topic should consider the importance
of motion. The studies reviewed here all involved
detection or recognition of static human faces and bodies.
However, static and dynamic information are arguably weighted
differently in face and body processing; as noted, static information
is more meaningful in faces, whereas dynamic information
is more crucial to body perception. For example, static
images easily afford recognition of individual faces, but recognition
of individual bodies probably has less to do with body
shape than with characteristic motion patterns. Prosopagnosics
report using motion patterns to recognize familiar people. Recent
evidence suggests that facial information is processed by
two distinct cognitive streams: a ventral stream (through the
lower parts of the temporal lobes, corresponding to brain areas
below the ears) that recognizes individuals by static features
and a dorsal stream (through the upper parts of the parietal
lobes, corresponding to brain areas above the ears) that processes
dynamic information (O’Toole, Roark, & Abdi, 2002).
Different brain areas are activated by static versus dynamic
displays of facial expressions. The brain also responds differently
15
to displays of the biomechanical motion of human bodies
than to static human bodies, but this may not be a dorsal-ventral
differentiation (Vaina, Solomon, Chowdhury, Sinha, & Belliveau,
2001). Thus, perhaps one of the most important future
directions for research in this area is the exploration of how
visual processes involved in the perception of faces and bodies
depend on dynamic information.
Recommended Reading
Bentin, S., Allison, T., Puce, A., Perez, E., & McCarthy, G. (1996).
Electrophysiological studies of face perception in humans.
Journal of Cognitive Neuroscience, 8, 551–565.
Downing, P., Jiang, Y., Shuman, M., & Kanwisher, N. (2001). (See
References)
Kanwisher, N., & Moscovitch, M. (2000). The cognitive neuroscience
of face processing: An introduction. Cognitive Neuropsychology,
17, 1–11.
Reed, C.L., Stone, V.E., Bozova, S., & Tanaka, J. (2003). (See References)
Slaughter, V., Heron, M., & Sim, S. (2002). (See References)
Acknowledgments—We thank Derek Moore for his insightful
comments on an early version of this article.
REFERENCES
Downing, P., Jiang, Y., Shuman, M., & Kanwisher, N. (2001). A cortical
area selective for visual processing of the human body. Science,
16
293, 23–26.
Gallese, V., & Goldman, A. (1998). Mirror neurons and the simulation
theory of mind-reading. Trends in Cognitive Sciences, 2,
493–501.
Johnson, M.H., & Morton, J. (1991). Biology and cognitive development:
The case of face recognition. Oxford, England: Basil Blackwell.
Kanwisher, N., McDermott, J., & Chun, M. (1997). The fusiform face
area: A module in human extrastriate cortex specialized for face
perception. The Journal of Neuroscience, 17, 4302–4311.
Ogden, J. (1985). Autotopagnosia: Occurrence in a patient with nominal
aphasia and with an intact ability to point to parts of animals
and objects. Brain, 108, 1009–1022.
O’Toole, A., Roark, D., & Abdi, H. (2002). Recognizing moving faces:
A psychological and neural synthesis. Trends in Cognitive Sciences,
6, 261–266.
Reed, C.L., Stone, V.E., Bozova, S., & Tanaka, J. (2003). The bodyinversion
effect. Psychological Science, 14, 302–308.
Slaughter, V., Heron, M., & Sim, S. (2002). Development of preferences
for the human body shape in infancy. Cognition, 85(3), B71–B81.
Tanaka, J., & Gauthier, I. (1997). Expertise in object and face
recognition. In R. Goldstone, P. Schyns, & D. Medin (Eds.),
Psychology of learning and motivation: Vol. 36. Perceptual
mechanisms of learning (pp. 83–125). San Diego, CA: Academic
17
Press.
Turati, C., Simion, F., Milani, I., & Umilta, C. (2002). Newborns’
preference for faces: What is crucial? Developmental Psychology,
38, 875–882.
Vaina, L., Solomon, J., Chowdhury, S., Sinha, P., & Belliveau, W.
(2001). Functional neuroanatomy of biological motion perception
in humans. Proceedings of the National Academy of Sciences, USA,
98, 11656–11661.
Volume 13—Number 6 223
Virginia Slaughter, Valerie E. Stone, and Catherine Reed
560 TINS Vol. 20, No. 12, 1997 Copyright © 1997, Elsevier Science Ltd. All rights
reserved. 0166 - 2236/97/$17.00 PII: S0166-2236(97)01136-3
REVIEW
THE CAPABILITY OF OUR BRAIN to represent the
body and to entertain a model of human anatomy
has probably a quite precocious if not downright
innate origin. Hours or even minutes after delivery,
neonates can imitate orofacial and head movements
performed by adults in front of them1. To the extent
that they identify a movement of a specific bodily part
of the adult model, and then produce a similar movement
in the corresponding part of their own anatomy,
18
babies must in some sense be cognisant of the general
body structure. A neural basis for this deceptively
simple visuomotor performance is probably constituted
by neurones that become active either during
the observation of a specific movement made by
another individual, or during the performance of the
same movement2. It is conceivable that primates are
born equipped with this mechanism for the imitation
of elementary actions, and that during maturation the
mechanism undergoes a gradual refinement as a consequence
of systematic interactions between tactile,
proprioceptive and vestibular inputs, as well as
between such inputs and the visual perception of the
structure and movements of one’s own and other
people’s bodies. The final result, a mental construct
that comprises the sense impressions, perceptions and
ideas about the dynamic organization of one’s own
body and its relations to that of other bodies, is variously
termed body schema, body image and corporeal
awareness3. Somatosensory inputs to the brain, especially
from proprioceptors, are no doubt essential for
bodily awareness, as attested by enduring changes
caused in it by short-lasting muscle vibration and
19
other somatic manipulations4; however, the importance
of vision is attested by the anatomical distortions
evident in the misshapen attempts of congenitally
blind subjects at drawing or sculpting their own and
other people’s bodies3. The finding that normally
sighted adults are facilitated in the visual discrimination
of postural changes in another person’s arms
during movements of their own arms but not legs,
and vice versa5, argues for the existence of at least
partly common, mutually reinforcing mechanisms for
the representation of corresponding parts of one’s
own and other people’s bodies.
Brain lesions affect the representation of the body
Brain lesions can induce profound changes in the
way the body is perceived and represented. In some
cases such changes can be ascribed to a disorder of a
specific cognitive domain, such as language or spatial
attention. Disturbances of body awareness that are
caused by lesions of the left posterior parietal lobe,
such as autotopagnosia, finger agnosia and left–right
disorientation, seem to depend on an altered conceptual,
mainly linguistic representation of body parts6.
Similarly, neglect of the left hemisoma that follows
20
right posterior parietal lesions usually occurs within
the context of a general neglect of the left hemispace,
and appears to depend on an impairment of spatial
attention or space representation rather than on selective
disruption of the body schema. Some disturbances,
however, might reflect a specific alteration of
the body schema or parts of it, as, for example, in
those stroke patients who are anosognosic for their
motor and sensory defects so as to deny that they are
impaired at all7,8. When it occurs in the absence of
extrapersonal neglect, personal neglect in the form of
hemisomatoagnosia suggests a specific alteration in
the body schema9. Feelings of non-belonging, denial
of ownership of a body part and misoplegia (hatred of
hemiparetic limbs) can occur following right brain
damage10,11. The neglected or disowned body parts are
expunged from the mental body representation, and
the material existence of these parts is justified with
confabulatory explanations12,13. Although anosognosia
for hemiplegia and somatoparaphrenia have
occasionally been observed after large left-hemisphere
lesions14, they occur mostly following right-hemisphere
The body in the brain: neural bases of
21
corporeal awareness
Giovanni Berlucchi and Salvatore Aglioti
Recent studies have begun to unravel the brain mechanisms that underlie the mental
representation of the body. Imitation of movements by neonates suggests an
implicit knowledge
of the body structure that antedates the adult body schema.This can include
inanimate objects
that bear systematic relations to the body, as shown by the elimination from self
awareness of a
body part and its associated paraphernalia after selective brain lesions. Dynamic
aspects of the
body schema are revealed by spontaneous sensations from a lost body part as well
as by orderly
phantom sensations elicited by stimulation of body areas away from the amputation
line and even
by visual stimulation. The mechanisms of the body schema exhibit stability, since
some brain
regions seem permanently committed to representing the corresponding body parts
in conscious
awareness, and plasticity, since brain regions deprived of their natural inputs from a
body part
become reactive to inputs from other body parts.
Trends Neurosci. (1997) 20, 560–564
22
Giovanni Berlucchi
and Salvatore
Aglioti are at the
Dipartimento
di Scienze
Neurologiche e
della VisioneSezione Fisiologia
Umana, Strada
Le Grazie, 8,
Università di
� 78 �
Tokai J Exp Clin Med., Vol. 31, No. 2, pp. 78-82, 2006
INTRODUCTION
Balint’s syndrome is clinically designated in a category
containing three major signs: inability to scan
the visual field in spite of normal eye-movement (fixed
gaze or psychic paralysis), impaired simultaneous perception
of more than one or a few objects (simultagnosia),
and defection of visual guided reach (optic ataxia
or misreaching). A defective estimation of distance is
considered to be another major symptom [1]. The majority
of patients with Balint’s syndrome do not show
23
all three of these major signs.
Balint’s syndrome can be seen in a variety of clinical
conditions, like Alzheimer’s disease, multiple strokes,
traumatic brain injuries, tumors, HIV infections, etc.
It is, however, rarely seen in a patient with a nondementing
neurological disease [3].
Balint’s syndrome is commonly accompanied by
various neuropsychological problems such as amnesia,
apraxia, unilateral spatial neglect, aphasia, etc. [2].
They vary in degree depending on the lesions and
frequently aggravate the patient’s handicap in their social
life. The rehabilitative intervention for such cases,
however, has not been fully discussed in literature.
This case report represents the more than four-year
clinical course of a patient with Balint’s syndrome and
aphasia, but with well preserved attentional, intellectual
and memory function. The authors discuss the effects
and limitations of rehabilitative intervention on the
impairment and disability, and also comment on the
problems with the social and legal system in relation to
the social participation of such a patient.
Minoru TOYOKURA, Department of Rehabilitation Medicine, Tokai Universtiy
Oiso Hospital, 21-1 Gakkyo, Oisomachi, Nakagun, Kanagawa 259-0198,
24
Japan�Tel: +81-463-72-3211�Fax: +81-463-72-2256�E-mail:
toyokura@juno.dti.ne.jp
A CASE REPORT
A 43-year-old salesman in a company dealing in
office equipment, with a history of cerebral infarction
at the age of 9 was admitted to a hospital emergency
room due to sudden unconsciousness on April 28,
2001. Although detailed information on the old apoplexy
from his childhood was not obtainable, no clinical
aftereffects remained and he had living a normal
life without any difficulties. Neuroradiological examination
revealed a fresh cerebral hemorrhage at the left
temporal subcortical area. After surgical treatment, he
was transferred to the authors� hospital for rehabilitative
intervention on May 22, 2001.
On admission he was alert and fully oriented, but
showed a little difficulty with communication due to
mild aphasia. The major signs and symptoms of his
speech were frequent letter paraphasia, difficulty in
word-finding, and disturbed repetition of letters as well
as words and short sentences. Grammar and verbal
comprehension were relatively preserved. The clinical
diagnosis of the language disturbance was considered
25
to be conduction aphasia.
A neurological examination also clarified that he
showed no abnormality in the cranial nerves except
the right hemianopsia. Gross motor palsy was not
found. Superficial and deep sensation were mildly
disturbed on the right side of his body. Tendon reflex
was slightly increased on the right upper and lower
extremities.
Memory, intelligence, and attention were well
preserved. Color identification and recognition of the
faces of famous people were not impaired. There was
no finding of apraxia, finger agnosia, autotopagnosia,
Rehabilitative Intervention and Social Participation of a Case
with Balint’s syndrome and aphasia
Minoru TOYOKURA, Tomoharu KOIKE�
Department of Rehabilitation Medicine,
Tokai University Oiso Hospital and � Ohta-Atami General Hpospital
(Received April 10, 2006; Accepted April 25, 2006)
Balint’s syndrome is characterized by three major disorders of spatial analysis:
fixed gaze or psychic paralysis,
simultagnosia, and optic ataxia or misreaching. Most patients with Balint’s
syndrome generally do not
26
show all three of these signs. The authors herein reported the more than four-year
clinical course of a case (a
43-year-old man) with Balint’s syndrome presenting these three disorders. The
patient also had a mild type
of conduction aphasia, but his attentional, intellectual and memory functions were
well preserved. SPECT
showed cerebral hypoperfusion in the bilateral parieto-occipital areas. Whereas
rehabilitative intervention
with process specific approach for the impaired visual cognition seemed to be
significantly ineffective, a
functional adaptation approach successfully promoted the patient’s social
participation. However, the present
patient could not help having to resign from his job. Additionally, double
impairment of visual (including
optic ataxia) and language functions made it impossible for him to obtain a new
work. Like the present case,
those who have a higher brain dysfunction, but retain good physical ability can
hardly receive the benefit of
the social welfare system in Japan. Legislation addressing this problem is a matter
of great urgency.
Key words: Balint’s syndrome, aphasia, rehabilitation, participation
M. TOYOKURA et al. /A case with Balint’s syndrome and aphasia
� 79 �
27
The copying of objects was defective. He was able
to draw simple figures but could not close the lines in
the figure. He could not locate a point in the center of
a circle. His reading ability was moderately disturbed.
One reason for this dyslexia may be aphasia, but the
main reason was his inability to properly trace the next
line or paragraph, which lead to skipping whole lines
due to impaired visual cognition.
The abnormal findings above were thought to be
compatible with a typical form of Balint’s syndrome
with three major spatial disorders of misreaching, ocular
apraxia, and simultagnosia.
Because of his visual and language dysfunctions, he
could not undergo standard neuropsychological tests
such as WAIS-R and WMS-R.
Laboratory data showed no abnormalities except
for mild hyperlipidemia (total cholesterol, 230 mg/dl).
Antinuclear antibodies were negative.
The T2-weighted MR images showed subcortical
high-signal-areas in the right parieto-occipital and left
temporo-parietal regions. The left one was considered
a new lesion (Fig. 1). Bilateral hypo-perfusion of the
parieto-occipital areas together with the left temporal
28
lobe was detected in SPECT (Fig. 2).
right-left agnosia, or unilateral spatial neglect.
He, however, was unable to reach target objects with
either hand. Although the ADL (activities of daily living)
was almost independent, he showed some difficulties
in visually-guided performances (such as picking
up small foods, inserting coins into vending machines,
dialing the telephone, etc.) because of this misreaching.
He could not scan moving objects. Saccades and
pursuit eye movements under verbal command were
also impaired.
The patient often reported a great deal of difficulty
in visually perceiving more than one object at a time
and said that objects in the visual field disappeared
when he put his visual attention toward other things.
He showed difficulties in fixing on a target object that
was not placed within his central vision. These were
considered to be typical signs and symptoms of simultagnosia.
He was not able to count dots, nor compare
the size and length of two or more objects. Perspective
was lost, as well. Thus he walked like a blind man
with his hands stretched out in front. He showed great
difficulties with walking in the darkness, walking on a
29
road covered with snow, and climbing and descending
stairs.
Fig. 1 MR images (6/2001).
There are subcortical high-signal-areas in the right parieto-occipital and left
temporo-parietal areas.
Fig. 2 SPECT (6/2001).
Bilateral hypo-perfusion of
the parieto-occipital and left
temporal regions is found.
M. TOYOKURA et al. /A case with Balint’s syndrome and aphasia
� 80 �
The rehabilitative intervention and clinical course
The patient was treated with rehabilitation programs
using visuoperceptual retraining and a functional adaptation
program in divisions of occupational therapy
and of clinical neuropsychology. For visuoperceptual
retraining, the patient was required to find target
objects in a scene painting or photograph in order to
improve visual scanning. For treating simultagnosia,
we developed a program in which the patient should
compare attributes (i.e. size, shape, length, etc.) among
two or more objects. A dot-counting task was also administered.
Visually guided hand performance (picking
30
up small things, inserting a stick into a hole, etc.) was
trained to lessen misreaching.
In contrast to the visuoperceptual retraining above,
which aim to restore the basic functions of visual cognition,
the purpose of the functional adaptation program
is to facilitate restoration of functional behaviors in the
patient’s real world. He was instructed to repeatedly
practice several social and housekeeping activities in a
safe way and place. The tasks included going for frequent
strolls (around his neighborhood at first), commuting
to the hospital alone using the hospital’s shuttle
bus (he was not able to use public transportation),
washing dishes, cleaning the house, mopping the floor,
etc.A fter his leaving the hospital and returning home
on September 30, 2001, we continued these programs
in the outpatient clinic twice a week. During and after
an 18-month training period, his visual cognition and
hand performance under visual guidance were reevaluated
using the Visual Perception Test for Agnosia
(VPTA) (Shinko Igaku Shuppann, Co., 1997) and
Simple Test for Evaluating Hand Function (STEF)
(Sakai Iryo, Co., 1985), respectively. The VPTA has
been established by the Japan Society for Higher Brain
31
Dysfunction as a Japanese standard test for examining
the impairment of visual cognition. The STEF is a standardized
test for upper-extremity functions, in which
time required for completing a manual task is measured
(Fig. 3). Table 1 shows the changes in the subtests
of the VPTA and total score of the STEF. Although
his hand performance seemed to slightly improve, his
visual cognitive function was almost unchanged. The
Fig. 3 A subtest of STEF.
The subject is required, as fast as possible, to pick
up balls one by one from a right side storage space
with the right hand and put them in a space on
the left side (five balls in all). The completion time
is measured. Both hands are evaluated separately.
STEF consists of ten subtests using ten objects of
different size and shape. The completion time of
each subtest is rated on a scale from 1 (the slowest)
to 10 (the quickest). The sum of each score (ranging
from 10, the poorest to 100, the best) indicates the
functional ability of the hand.
period for the rehabilitative intervention
Month / year
VPTA & STEF 7/01 3/02 8/02 1/03 7/03 1/04
32
VPTA
discrimination (length) 0 0 0 0 0 0
discrimination (shape) 17 50 67 50 67 50
counting dots 0 0 0 0 0 0
naming object 100 100 100 100 100 100
recognizing photos of
famous people’s faces
100 100 100 100 100 100
naming colors 100 100 100 100 100 100
copying figures 0 0 0 0 33 0
STEF
(rt./lt. hands) (/100) 38/49 33/51 54/72 69/70
Visually cognitive function evaluated by VPTA is shown to be almost unchanged
throughout the time
course. In STEF, hand function slightly improved although the best performance is
still far below a
normally functional level.
�1, The cut-off score for the patient’s age is 96.
Table 1 Changes in the performance of VPTA and STEF
VPTA: corrrect answer (%), STEF: total score of ten subtests�1
M. TOYOKURA et al. /A case with Balint’s syndrome and aphasia
� 81 �
paraphasia, word-finding difficulty, and dyslexia were
33
still present, which resulted in only a minor improvement
in the communication ability.
Table 2 shows the change in his functional behaviors
and community independence between two occasions,
at discharge (September, 2001) and at the present time,
December, 2005. His repertoire of functional behaviors
were expanded and he was able to do housekeeping
work more quickly and precisely. Thus, social participation
and QOL significantly improved.
The patient, however, was ultimately forced to resign
from his job, and was unable to obtain new work
because of the double impairments of visual (including
optic ataxia) and language functions. Thus, his financial
problems resulting from his loss of income, should
be addressed using the economical support establishment
of the social welfare system. Because of his preserved
motor function, however, he could not obtain a
physically disabled persons� certificate or pension. The
authors, therefore, applied those reserved for mentally
disabled persons. The medical certificate application
was initially rejected, but after repeatedly insisting on
the legitimacy of the application to the local health center,
he was finally able to obtain the mentally disabled
34
persons� pension and reduce his financial burden.
DISCUSSION
The present case shows Balint’s syndrome in a
relatively pure form. Aside from the aphasia, no neuropsychological
problems accompanied it. His intellectual
and memory functions were well preserved.
The brain damage to the parieto-occipital area has
been pointed out as the critical locus of the lesion for
Balint’s syndrome [1]. Diffuse lesions in both hemispheres
due to cerebral anoxia, encephalitis, trauma,
and degenerative diseases may also cause this syndrome
[3]. In the present case, the recurrence of cerebrovascular
accidents produced Balint’s syndrome and aphasia.
Although the lesions detected in MR imaging were
located in subcortical areas, SPECT showed decreased
cortical blood flow in bilateral parieto-occipital regions.
No effective and specific intervention of cognitive
rehabilitation for Balint’s syndrome has yet been
established [3]. Sohlberg [6] described three forms of
cognitive rehabilitation: the functional adaptation approach
(FAA), general stimulating approach (GSA),
and process specific approach (PSA). FAA promotes
functional performance in a certain living or work
35
environment. This includes the development of environmental
manipulation or a compensatory strategy. In
this form of approach, neurological impairment itself
is not expected to improve. GSA generally uses nonspecific,
intellectual tasks such as games or puzzles. It
can be easily conducted in any treatment environment.
The basic underlying theoretical orientation, however, is
not clear. In addition, functional ability to practice realworldbehaviors sometimes fails to improve. In contrast,
the purpose of PSA is to restore particular function
in one particular cognitive area. Although the positive
impact of the treatment is limited to that specific cognitive
area, one can expect a secondary improvement of
functional performance that has been impaired by the
cognitive dysfunction (i.e., little generalizations). For
example, improvement of an attentional deficit (specific
cognitive dysfunction) can also produce better performance
in cooking that had been difficult because of
the attention disturbance.
For the present case, the authors practiced both FAA
and PSA (visuoperceptual retraining). Even after the 18
months of treatment, visual cognition did not significantly
improve. However, through repetitive practice in
36
the community he has been expanding his repertoire
of functional behaviours in his social life. During the
treatment he increased his self-confidence, self-esteem
and ability to cope with his disability. These effects
seemed to have considerably improved his QOL. Well
preserved intellectual and memory functions may have
a positive effect on the learning process.
Perez et al. [4] have reported three cases of Balint’s
syndrome and the individualized rehabilitation approaches
of multicontext treatment with intensive verbal
cuing and organizational strategies. These patients,
however, initially identified objects correctly only 20 to
75% of the time. This finding suggests a coexistence
month / year
9/01 12/05
�coming to the hospital alone�1 impossible possible
�housework�2 possible but taking time more quickly
�using a push-button phone impossible somehow possible
�walking around the neighborhood slowly and carefully much faster
�area for daytime walking only neighborhood expanded area
�walking at night with difficulty with difficulty
�riding a bicycle impossible impossible
�driving a car impossible impossible
37
�shopping impossible possible
�work suspended retired
�mentally disabled person’s certificate not received received
�disabled person’s pension not received received
�1, using the hospital’s shuttle bus
�2, washing dishes, cleaning the house, sweeping and mopping the floor, etc.
Table 2 Changes in functional behaviors and community indepedence
M. TOYOKURA et al. /A case with Balint’s syndrome and aphasia
� 82 �
of visual agnosia that is sometimes accompanied by
Balint’s syndrome. Although the response accuracy rose
to 80 to 95% after 6 to 12 months of rehabilitation,
the change possibly resulted from the improvement of
visual agnosia rather than impaired visual cognition
by Balint’s syndrome. Thus, if the patients had not
had visual agnosia like our patient, the rehabilitation
program could not have produced a significant
improvement. In this sense it seems acceptable that
rehabilitation produced little effect on visual function
in our patient.
Rosselli et al. [5] also reported the effects of a neuropsychological
treatment on a patient with a fat embolism
following a serious traffic accident. The patient
38
showed Balint’s syndrome in addition to alexia without
agraphia, visual agnosia, prosopagnosia, or memory
impairment. Rehabilitative intervention commenced
one year after the onset. The treatment protocol was
based on PSA and attempted to specifically retrain
the impaired visual spatial function. FAA was also
developed to improve the adaptive skills of ADL in
everyday life. One year after the treatments, he showed
an improvement in community independence and was
finally able to return to his former job. A significant
improvement was also shown in several neuropsychological
tests that were sensitive to visual scanning
deficits and simultagnosia. Although this may indicate
functional recovery of visual impairment, the test-retest
learning effects of the tasks cannot be denied because
the tasks were also used for the rehabilitation.
The report suggests that a productive life can be
attained by a rehabilitative approach even after the
period in which the majority of spontaneous recovery
is likely to occur. The accumulation of newly learned
functional behaviors in a patient’s social life with FAA
can persist for quite a long period. In this sense FAA is
very valuable for improving QOL.
39
FAA, however, has some disadvantages or limitations.
Depending on the behaviors, it takes a long time
to establish community independence. Focusing on the
practical adaptation of specific behaviors, FAA shows a
restricted generalizability.
The present patient could not avoid resigning from
his job. In April this year the law for employment
promotion of persons with disabilities is revised. The
new law gives a wider opportunity for disabled people
who have a mentally disabled persons� certificate to
get a job. The authors consider that the revision is appropriate
and expect the good results in the Japanese
welfare situation for the disabled. Unfortunately the
double impairment of visual (including optic ataxia)
and language was so severe that he could not receive
the benefit from the revised law. From the view-point
of rehabilitation medicine, social participation is the
most important of concerns. In this sense, this patient,
despite loosing his job, could acquire various social
skills by rehabilitative intervention.
Loss of income is a critical financial problem that
should be worked out. For those without psychiatric
disease, and with good motor function, official
40
compensation for their financial problems had been
hardly obtainable in Japan even if they had great
difficulties in their social life because of the higher
brain dysfunction, like our patient. Recently, however,
the law concerning mental health and welfare for the
mentally disabled has been revised and these patients
mentioned above have become to be able to apply for a
mentally disabled persons� certificate and pension. The
present patient finally acquired the qualification for
the pension. Although the situation has been somewhat
improved, it seems still strange that a patient without
any lunacy has a mentally disabled certificate. Legal
welfare system specialized for such patient that suffers
higher brain dysfunction but no physical and mental
disabilities has not yet been established in Japan.
Legislation against this problem is a political matter of
great urgency.
REFERENCES
1) De Renzi E: Disorders of spatial orientation. In: Handbook of
Clinical Neurology. vol. 1 (45) (ed, Frederiks JAM), Elsevier
Science Publishers, Amsterdam, 1985: 405-422.
2) Hecan H, De Ajuriaguerra J: Balint’s syndrome (psychic paralysis
of visual fixation and its minor forms). Brain 1954; 77: 373-400.
41
3) Kerkhoff G: Neurovisual rehabilitation: recent developments
and future directions. J Neurol Neurosurg Psychiatry 2000; 68:
691-706.
4) Perez FM, Tunkel RS, Lachmann E A, Nagler W: Balint’s
syndrome arising from bilateral posterior cortical atrophy or
infarction: rehabilitation strategies and their limitaion. Disability
Rehabil 1996; 18: 300-6.
5) Rosselli M, Ardila A, Beltran C: Rehabilitation of Balint� s syndrome:
A single case report. Appl Neuropsychol 2001; 8: 242-7.
6) Sohlberg MM, Matter CA: Attention Process Training. Association
for Neuropsychological Research and Development, Washington
DC, 1986.
42