Articular cartilage
advertisement

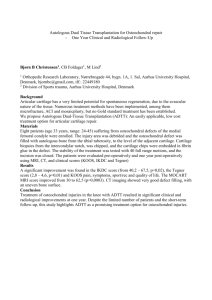
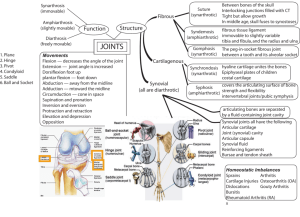
CARTILAGE Cartilage is a key body component, performing important structural and functional roles. Cartilage cells develop from mesenchymal stem cells.[1] Developing as early as the 5th week of embryonic growth, it forms 1% of total adult tissue volume and is also closely involved in the development of bone.[2] In humans, cartilage is found in many forms in various locations around the body. Its major role in adults is to provide mechanical support as well as a range of secondary functions. These functions provide; a smooth surface for articulation of bones, growth of long bones and strengthening of tendons such as at the pubic syphysis. The different forms are divided into 3 main groups (See Table 1). TABLE 1: TYPES OF CARTILAGE AND FUNCTION Type of Cartilage Key Locations Hyaline Tracheal Rings, Joint surfaces of Bone Elastic External Ear, Epiglottis Fibrocartilage Intervertebral Discs, Pubic Syphysis The different functions of cartilage require a variety of micro structures, which relate to the functional role it is undertaking. All of the different types of cartilage are made up of similar components. Through different levels of gene expression and synthesis, of these components, the structural differences of cartilage are exhibited. COMPONENTS OF CARTILAGE Cartilage is made up of 3 components; chondrocytes (cartilage cells), extracellular matrix (ECM) and interstitial fluid. Cartilage is avascular, alymphatic and has no innervation. CHONDROCYTES Chondrocytes are the sole constituent cell of cartilage. Cells average only 2% of total cartilage volume,[3] a situation almost unique within the human body. They are sparsely distributed and isolated from neighbouring cells by the ECM. The chondrocytes role is to produce and organise the ECM, which carries out the functions of cartilage. Chondrocytes are rounded or polygonal in shape, and on average have a diameter of 13µm.[2] They have an abundance of rough endoplasmic reticulum and glogi apparatus (FIGURE 1), as expected for a cell producing such large quantities of extracellular material. Chondrocytes also have relatively few mitochondria as a result of their low oxygen/avascular environment. In fact the whole cells metabolism is geared to low oxygen tensions. In the deep layers of cartilage oxygen tensions may be less than 1%.[4] FIGURE 1: AN ELECTRON MICROGRAPH OF A CHONDROCYTE From “The Chondrocyte”[4] Chondrocytes are regulated by a poorly understood combination of mechanical, electrical and physiochemical signals. These are thought to be transmitted by the ECM to the cell through membrane receptors and direct binding. The chondrocytes respond to these stimuli by regulating their metabolic activity through gene expression.[5] This area will be discussed in more detail later with regard to articular cartilage. COMPONENTS OF THE EXTRACELLULAR MATRIX (ECM) COLLAGEN Collagen acts as the organised structure or ‘endoskeleton’ of cartilage. It represents up to 50% of the dry weight of cartilage.[6] It provides the tensile strength,[7] and resistance to forces. Collagen also provides resistance to the osmotic pressure exerted on the proteoglycans which indirectly attach to the collagen framework. Collagen is composed of repeat amino acids sequences, with side chains. There are more than 20 types of collagen. They are broadly classified into fibrillar and non-fibrillar. The 4 major collagens in cartilage are outlined below (See Table 2). Collagen forms the ‘pillars’ and 4 ‘beams’ which give cartilage its inherent structure however it is the ‘filling in’ of these spaces that give cartilage its strength against compression. TABLE 2 : TYPES OF COLLAGEN AND FUNCTION Collagen Fibrillar / Non-Fibrillar Function II Fibrillar Structural/ Mechanical Fibres VI Non-Fibrillar Peri-cellular Adhesion IX Non-Fibrillar Point of attachment on fibrils for cross-linking X Non-Fibrillar Small Network to facilitate calcification Adapted from: Skeletal Tissue Mechanics.[7] Collagen is formed from chains of amino acid. These chains combine to form the collagen units (see table 2), these units are either fibrillar (fibrous) in form or not. Finally these fibrils combine along with non-fibrillar units to form larger units known as fibres. Collagen II is the key molecule that provides tensile strength. It consists of three identical α1 chains arranged in helical form. This forms the majority of the fibrils (FIGURE 2) in the ECM. In certain zones it accounts for 80-90% of the dry weight of cartilage.[8] The fibrils are strengthened further by cross linking. Collagen VI forms highly branched filaments that intertwine with collagen II.[9] It is found almost exclusively in pericellular regions and is thought to be involved in attaching the chondrocyte to the ECM. It also binds to hylauronan, a component of the proteoglycan aggregate, discussed later. Collagen IX assists in the process of cross linking fibrils.[10] It is attached to the fibrils in a perpendicular manner. This offers a point of attachment for cross links (FIGURE 2). Also by attaching to binding points on the fibrils it prevents lateral growth. Collagen IX is also prominent in the pericellular region. It represents 2% of total collagen.[10] Collagen X is found in growth plates and areas of calcified cartilage. It is produced by hypertrophic chondrocytes and is normally found in the pericellular region. It is a short chain that forms a hexagonal network, this assists in the mineralisation of the ECM.[11] It is used as a marker for mineralisation. 5 PROTEOGLYCANS Proteoglycans consist of glycosaminoglycan (GAG) chains bound to a protein core. They account for up to 12.5% of the dry weight of cartilage.[7] The most common proteoglycan in articular cartilage is aggrecan, making up 90% of the total proteoglycan mass. [8] Aggrecans comprise 10% core protein and 90% GAG.[12] The protein backbone is made up of 4 domains. The G1 domain (See Figure 2) is the proximal binding site. It can bind to hyaluronan, with the assistance of a link protein, or other less common sites. G2 domain (See Figure 2) is an area of structural importance. G3 domain (See Figure 2) is the termination of the protein back bone. The 4th region between G2 and G3 is the GAG attachment domain. The GAGs bind perpendicularly to the protein backbone. Around 150 GAG chains may be attached to a single aggrecan protein backbone, [8] to form a ‘bottle brush’ structure. FIGURE 2: MACROFIBIBILLAR COLLAGEN NETWORK & PROTEOGLYCAN AGGREGATE Key: HA - Hylauronan CS - Chondroitin sulphate KS - Keratin sulphate From “Composition and Structure of Articular Cartilage” [13] 6 GYLCOSAMINOGLYCANS (GAGS) GAGs are repeating disaccharide units of uronic acid and a sugar. They are normally sulphated which leads to the formation of a polyanion.[8] The three main GAGs in cartilage are hyaluronan, chondroitin sulphate and keratan sulphate. Hyaluronan is a repeating chain of hyaluronic acid which can reach up to 2 million repeats in size.[14] Hyaluronan intertwines with the collagen fibrils, forming a “weave” that maintains the hyaluronans position within the ECM (See Figure 2). Hyaluronan offers the most abundant source of binding sites for proteoglycans (PGs). Many PGs indirectly link to hyaluronan which forms aggregates. Hyaluronan also links the ECM to the chondrocytes via an interaction with the chondrocyte cell surface receptor CD44.[15] PROTEOGLYCANS (PGS) PGs are formed by a protein backbone which binds to GAGs covalently attach. [8] The most prolific PG in cartilage is aggrecan. [8] Aggrecan contains two different forms of GAGs; chondroitin sulphate and keratin sulphate. Both are repeating disaccharide units, chondonite sulphate is about 30 units long, while keratan sulphate is shorter. Both types of chains contain carboxyl and sulphate groups that when in contact with interstitial fluid become negatively charged and so attract cations. It is this affinity for water that carries out aggrecans function. The water attracted by the negative charge swells the aggregates, until their expansion is restricted by the collagen fibrils of the ECM. Even after maximal swelling, aggregates still has further affinity for water. This means that when cartilage is placed under compression, the compressive force is attempting to force the water out of the cartilage, against frictional and osmotic forces which are attempting to prevent water leaving. These forces are closely balanced in healthy cartilage, causing resistance to compression.[16] INTERSTITIAL FLUID The role of the interstitial fluids is to provide nutrition to the chondrocytes and remove waste products. As such it consists of; electrolytes, small molecules, glucose, metabolic wastes, 7 carbon dioxide and constituent parts of ECM all of which are suspended in water. Nutrients and wastes have to be carried to and from the chondrocytes through the ECM, which acts as a sieve. The ECM’s great affinity for water means that diffusion over any significant distance is negligible. This accounts for the low oxygen tensions at the deep layers of cartilage.[4] Articular cartilage has adaptations to these low oxygen tension which are discussed later. 8 ARTICULAR CARTILAGE Articular cartilage is a form of hyaline cartilage, with particular structural variances to assist it in its role. Articulating ends of involved joints are covered by this load bearing elastic material. It serves as resistance to compressive forces and a low friction surface. Together with the synovial fluid in the joint capsule they create an almost frictionless joint.[13] ZONES Articular cartilage is structurally divided into 4 layers that run parallel to the joint surface. These 4 layers are; the superficial, transitional, deep and calcified zones. This organisation of zones is of functional use and the composition of structural components differs between zones. SUPERFICIAL ZONE The superficial zone runs on the free surface of articular cartilage. It is the thinnest of the zones, but contains the highest cell density.[3] Cells in this layer are discoid or flattened as opposed to their usual polygonal form.[4] Water concentrations are high as there is a low proteoglycan content leaving room for the water.[17] The majority of the zone consists of densely packed layers of collagen. The thin collagen fibrils of this zone are uniformly packed and divided into 2 layers. The first layer, known as the lamina slendens, is the linear fibres that form the articular surface. It is formed by bundles of collagen running parallel to each other. This forms a smooth surface, which is comparable to man-made metalwork.[18] The subsequent layers of collagen fibrils are arranged perpendicular to the articular surface. These layers produce a filtering effect on the fluid passing through to the deeper layers of the cartilage. A molecule as small as an immunoglobulin may be prevented from entering the cartilages interstial fluid, by this filtering effect.[8] 9 TRANSITIONAL ZONE The transitional zone contains and is produced by rounded chondrocytes. Collagen of the ECM is randomly arranged and proteoglycan content is greater than that of the superficial zone.[14] DEEP ZONE The deep zone is characterised by chondrocytes arranged in columns. Chondrocytes are at their lowest concentration in this zone, which is dominated by a proteoglycan rich ECM.[17] An irregular line separates this zone from the calcified zone. Between the 2 zones bands of collagen can be seen. These bands tether the deep zone to the calcified zone, to prevent shearing forces separating the two zones. CALCIFIED ZONE Here, round hypertrophic chondrocytes remain in non-calcified area. They are surrounded by an ECM which is almost absent in proteoglycan.[8] The collagen fibres are arranged perpendicular to the surface and are anchored to the calcified matrix.[14] The line of communication between the calcified zone and underlying cortical bone is wave like in form. ARTICULAR CARTILAGE FORMATION Articular chondrocytes produce different quantities of ECM components due to variation in the stimuli each zone of cells is subjected to. During joint loading, forces on the ECM cause stimulation of the chondrocytes via CD44 and other receptors.[14] These stimuli vary in type and intensity dependent on cell location. It is this which causes the variance in gene expression leading to ECM production.[19] The second method of stimulation of the chondrocytes is through hydrodynamic pressures.[20] Articular cartilage is effectively a very stiff sponge. When joint loading occurs it forces liquid / synovial fluid out of the ECM, so causing fluid flows within the ECM. This fluid flow takes positive charges ions with it, meaning the membrane potential is depolarised. In addition the intracellular fluid composition has not changed and is now more heavily attracted to the extra-cellular negative charge causing an osmotic swelling of the cell. Both of these processes add to the stimulation of the call and can cause ECM production. 10 This fluid movement caused by loading of the joint also carries nutrients to the chondrocytes and metabolites away from them. 11 ARTICULAR CARTILAGE INJURY & TREATMENTS ARTICULAR CARTILAGE INJURY Cartilage injuries fall into two main patterns; full or partial thickness. The two are differentiated by the involvement of subchondral bone, which is the barrier between the cartilage and bone marrow. Partial thickness injuries do not repair on their own,[21] due to cell immobility in cartilage. Other factors that effect cartilages ability to heal include; the location of the injury, the age of the patient and any associated infection. Full thickness injuries do heal, due to their contact with the marrow space and its mesenchymal stem cells and blood supply. This forms a blood clot in the defect. Lesions 12mm in diameter can heal but larger lesions may not totally fill with clot,[22] leading to poor healing. The clot adheres well to the bony surface but poorly to the articular edges, which can lead to necrosis at the periphery of the neocartilage.[23] After a few days, mesenchymal cells begin to infiltrate the haematoma. These cells help produce a fibrocartilage that fills the void created by the injury. Ossified material is deposited deeper to reseal the marrow space. Fibrocartilage is mechanically inferior to articular cartilage as it gradually degenerates over time.[23] TREATMENTS OF ARTICULAR CARTILAGE INJURY Treatments for articular cartilage injury currently fall into three main categories, arthroscopy/levage, marrow stimulating techniques and implantation techniques. ARTHROSCOPY / LAVAGE This procedure is carried out in two sets of circumstances. The first is if physical and radiological assessment deems it likely a patient has a free body in the joint. A free body is typically a piece of cartilage that has broken off during the injury event and is now floating within the joint capsule. The lavage removes this free body so preventing it from damaging the articular surface in any other area. This involves placing an access port into the capsule and washing out the free body. 12 The second indication for lavage is for pain relief. If a patient has pain that is effecting their activities of daily living then lavage may be of some use.[24] Pain relief is achieved through an unknown mechanism. It is postulated that by replacing the synovial fluid, pain signalling agents are also removed. However it also gives the surgeon the opportunity to place a fibre optic camera into the joint and visually inspect the injury. This gives the surgeon a definitive assessment of the injury and allows a decision to be made if any further treatment would be beneficial. MARROW STIMULATING TECHNIQUES These techniques attempt to stimulate a healing of the injury similar to that found in full thickness injuries. This is achieved by a range of techniques from debridment to subchondral drilling. They are all base around the principle of exposing the bone marrow space to the injury site by mechanical measures. The microfracturing technique is an adaptation of the subchondral drilling technique first described by Pirdie in 1959.[25] Steadman et al.[26] created microfracturing which consists of creating holes; 4mm deep, 1mm in diameter and 3-4mm apart, across the extent of the defect. This creates a communication to the bone marrow and allows a clot to form in the defect so leading on to fibrocartilage creation. The holes are created by an arthroscopic awl which has a number of benefits over Pirdies’ drill. It is carried out by arthroscopy so causes less tissue damage, the awl does not cause the heat necrosis to surrounding tissue that a drill might and the small holes mean that less trauma is caused to the subchondral plate, which help maintains its biomechanical properties. In young people it has been reported to improve joint functionality and gives pain relief in up to 75% of patients.[27] The fibrocartilage created will however be of inferior quality to articular cartilage and it is expected that these patients will suffer problems in the future. IMPLANTATION AUTOGENOUS CHONDROCYTE IMPLANTATION The first reported use of a autogenous chondrocyte implantation was by Grande et al, in rabbits[28] This technique involved the removal of a 3mm full thickness segment from a 13 rabbits patella. The defect was then covered with a periosteal patch. The chondrocytes where then liberated from the extracted segment and cell number was expanded in vitro. The cells were then injected back into the defect under the periosteal patch. At six weeks the cells had contributed to the repair of the defect and results were considerably better than the controls. Following this Brittberg et al.,[29] published the first human study in 1994. The results of the first 100 patients were subsequently published and are very encouraging.[30] 92% of the repairs carried out, were rated good to excellent. The only major complication associated with successful grafts is periosteal patch over growth, which occurs in 10-15% of patients. These are relatively easily debrided by an arthroscopic procedure. While these early results are encouraging , the use of these techniques is highly specialised and long term results are unknown. In a canine study, cartilage produced is known to be vastly inferior to native cartilage,[31] however clinical results in human studies seem to exceed these expectations. CARTILAGE TRANSPLANTATION The main difference cartilage transplantation is the location of their donor site. Grafts are either autografts (from the same patient) or allografts (from cadaver donors). The allografts are then subdivided into fresh refrigerated grafts or frozen cryopreserved grafts. AUTOGRAFTS The advantages of autografts are the smaller risk of disease transmission and less risk of graft failure due to immuno incompatibility. However these benefits must be compared to donor site morbidity. Mosaicplasty is a technique used in the knee, which was developed by Hangody et al. in 1992.[32] Small osteochondral grafts are harvested from the supra chondylar ridges or the intra-chondylar ridges and then pressed into the pre-prepared holes in the defect. The size of the donor grafts, 2.7-4.5mm in diameter, helps to reduce morbidity associated with their harvesting.[32, 33] The bone of the graft is then pressed into the recipient hole, this heals well and the small amount of blood that escapes forms a uniform cartilage surface between 14 the grafts. The graft cartilage survives and has intervening fibrocartilage, formed from the blood, to support it.[28] Handgody et al., reports 91% of patients achieve good to excellent scores on the Hospital for Special Surgery knee scoring system at 3 years.[33] There are however limits as to the size of defect which can be treated. Ideally it should be less than 2cm in diameter and have a discrete margin. This technique can also not be used on anyone who has an active inflammatory or infective process in the knee and can not be used if there is any degenerative change to the cartilage. ALLOGRAFTS The first was carried out in 1907 by Lexer.[34] He performed a “half joint transplantation”. After his initial success he continued to perform allografts for partial and whole joint transplantations, reporting a 50% success rate.[34] This early work found that infection was the main reason for failure and as such Lexer favoured fresh donor material. It was Mankin et al. who pioneered the use of cryopreserved allografts which are logistically more practical than fresh grafts.[35] However later analysis showed that the cartilage of the frozen allografts rarely survived after 8 years.[36] It was hypothesised that the freezing process killed the chondrocytes, which were dead after thawing. Without the chondrocytes to maintain it the ECM begins to degrade with wear and tear. Today, because of the above problem, fresh allografts are almost exclusively used. They tend to be harvested 12-24hrs after the donors death. The graft is then placed in physiological solution and stored at 4ºC. Most surgeons advocate its use within 24hrs of harvest.[37, 38] Although chodrocytes remain viable up to 7 days in this environment, other parts of the graft are less well adapted to survive in low oxygen environments.[39] Most clinical trials have procured their allografts from donors below the age of 30. Garret,[38] describes probably the most widely advocated surgical technique. The defect is normally converted into a cylindrical shape with a depth of 8-10mm. Then a similarly sized plug is harvested from the corresponding place on the donor, this is then press fitted into the defect. 15 In clinical trials fresh allografts are used. The first of these trials were carried out in 1972 by Gross et al.[40] and McDermott et al.[41] A recent review with an average follow up time of 7.5years showed an 85% success rate. Success was defined as no need to re-operate and nonrecurrence of pre-operative symptoms. All patients undergo a similar regime of rehabilitation post-transplant. Non-weight bearing for the first few days, followed by protected weight bearing until the graft has incorporated. This is followed by limited exercise and finally by full weight bearing, which may take up to 2 years to achieve if the graft is slow to incorporate. 16 TISSUE ENGINEERING In recent years, in-vitro strategies for the repair of cartilage defects have reached levels of development, so as to make them plausible alternatives to in-vivo therapies. Tissue engineering strategies “focus on the delivery or in situ mobilisation of cells, capable of restoring pathologically altered architecture and function”.[42] There are 2 main focuses of research; the implantation of cells in an artificial supportive matrix and the in-vitro development of a complete transplant. The development of these two different approaches, are based on much of the same research. Developments in this area have been rapid, with the application of old and new knowledge in the search for a viable clinical therapy. The ultimate aim of a complete transplant would be to harvest cells from the patient, sort them, place them into a growth platform and produce a high quality transplant that could be used to replace damaged areas. The use of “bioreactors” holds the promise of producing high quality cartilage for use in such a transplant. There does however remain a lot of development to be under taken to scale them up to an appropriate size.[43] Cell transplantation in scaffolds uses a similar concept as Brittbergs et al. Instead of being held in place by a periosteal patch, scaffolds attempt to maintain chondrocytes in the defect by using a porous material,[44] until cells produce enough ECM to maintain their own position. This research is also being used to fix chondrocytes in position in bioreactors and as such much research is shared with cell implantation, tissue engineering. SCAFFOLDS These scaffolds must meet a number of design criteria. The material and its degradation products must be compatible with all human tissues.[44, 45] In addition the scaffold must allow nutrient diffusion to the encapsulated cells, be porous enough to allow native cells to infiltration and be able to maintain structural integrity[44] and position.[42] The porosity of the scaffold is required “both to encourage retention of implanted cells and to favour colonisation by native cells”.[46] Native cell infiltration is imperative as implants that do not bond and integrate with adjacent tissues are “destined to fail”.[47] 17 Scaffold Materials fall into two main categories; synthetic and natural materials. SYNTHETIC SCAFFOLD MATERIALS Polymeric materials are used heavily in the research of tissue engineering cartilage. Widely used are polylatic acid and polyglycolic acid. PLOYLACTIC ACID (PLA) Initial animal studies with this scaffold showed discouraging results,[48, 49] with poor subchondral bone repair and lower levels of biochemical markers than intrinsic cartilage. Since then the initial retention of cells has been improved.[50] Also work has been carried out using PLA as a carrier of exogenous transforming growth factors and its effects on mesenchymal stem cells. POLYGLYCOLIC ACID (PGA) PGA comes in the form of a foam or fibre mesh that has been used in vivo cartilage defect repair. In porcine models autologous chondrocytes implanted in defects produce good results at 24 weeks.[51] Both biochemical and tissue interface results were good. Co-polymers between PLA and PGA have been extensively investigated. The ratio between PLA, PGA and additional constituents has been used to manipulate degradation time. The addition of other constituents can, among other things, encourage bone growth into the scaffold.[52] NATURAL SCAFFOLD MATERIALS FIBRIN As the major component of a blood clot that forms at the site of full thickness injuries, fibrin seems a logical choice as a potential scaffold. It has two major problems; it exhibits no significant intrinsic mechanical strength and exogenous fibrin can cause an immune response.[53] Despite this fibrin has been shown to be an effective scaffold. With both cartilage chip[54] and mesenchymal stem cell[55] studies using it with good outcomes. Fibrin glue is also used to fixate other perichondral scaffold grafts in place.[56] 18 AGAROSE & ALIGINATE These polysaccharides form hydrogels that allow even distribution of culture cells throughout the scaffold as it is cast.[57] Agarose is used extensively in vitro but doesn’t break down well and can induce an immune response in vivo.[58] In contrast seeded alginate scaffolds shows poor biochemical markers,[59] but good histological integration with native cartilage.[60] COLLAGEN As the largest constituent of the ECM collagen it also seems a logical choice as a scaffold. There have been decades of work with collagen in vitro as well as a number of animal studies.[61, 62] It is an essential tool within tissue engineering, as it can easily be combined with proteins[62] and even gene therapy techniques[63] to provide improvements in the quality of cartilage produced. Recently collagens from bovine sources has been identified as a possible poroduct that could spread prion induced bovine spongiform encephlalopathy.[64] This may limit its use to research as in-vitro work would come with an unacceptable risk. HYALURONAN As another major component of ECM hyaluronic acid also seems an excellent potential scaffold. However it was discovered to cause chondrocyte chondrolysis, inducing almost total loss of proteoglycan rich areas.[65] Despite this rabbit studies have shown good results, with marginally thinner cartilage at graft sites being the only major problem.[66] CHITOSAN Chitosan is a polysaccharide which forms a gel when cross-linked by a second substance. Initially chondronitin sulphate was used,[67] but cellulose was later found to be a more practical cross-linker.[68] Chitosan is such an attractive scaffold due to its thermal properties. It is liquid at room temperature (21ºC) but forms a gel at body temperature (37ºC).[68] This sparked a flurry of research into the properties of chitosan and its possible use as a scaffold for cell transplantation in a variety of fields.[69] Though little attention has been focussed on 19 its possible use as a bioreactor scaffold. Its biocompatibility has been investigated and confirmed.[70] It also has the advantageous quality of adherence with bone and cartilage.[71] 20 METHODS MATERIALS Dulbecco’s Modified Eagle Medium (DMEM-F12), foetal calf serum, Fungizone™, gentamycin and Picogreen™ Dye were sourced from Invitrogen, UK. Pronase E™ was sourced from VWR Interbational, UK. Protasan UP (product: G213) was sourced from Novamatrix, Norway. Hydroxyethyl-cellulose (cellulose), β-Glycerol phosphate (βGP) and all other reagents were sourced from Sigma-Aldrich, UK. MEDIUM DIGESTION MEDIUM Digestion medium (DM) consisted of DMEM-F12 media supplemented with 50µg/mL gentamycin, 2.5ng/mL Fungizone™ and 50 µg/ml ascorbic acid-2-phosphate. COMPLETE CULTURE MEDIUM Complete culture medium (CCM) consisted of DM supplemented with foetal calf serum at 10% by volume. GEL COMPONENTS PROTASAN SOLUTION Protasan powder was weighed and sterilised under UV light for 2 hours. Then, under a lamina flow hood, it was placed in a bottled of sterile lab grade water with a magnetic stirrer that had been autoclaved. It was stirred until all the powder had dissolved. After stirring it was stored at 4˚C until required. Β-GLYCEROL PHOSPHATE SOLUTION βGP was weighed and made up to the appropriate concentration with autoclaved lab grade water and vortex mixed. It was stored at 4˚C till required. It was filter sterilised through a 22µm filter when added to the protasan solution. CELLULOSE SOLUTION Cellulose was weighed and made up to the appropriate concentration with DMEM-F12 and vortex mixed. It was filter sterilised through a 22µm filter when used. 21 EXPERIMENTAL METHODS ISOLATION OF CHONDROCYTES FROM ARTICULAR CARTILAGE Bovine joints were obtained from an abbatoir shortly after the animals slaughter. All animals were aged under 30 months. A thickness from superficial to deep zone of cartilage was dissected from the joint surface of the trochleal humerous and radial head of the thoracic limb. Disected cartilage was placed into DM to prevent drying. Finally dissected pieces were diced into 1-3mm pieces. Chondrocytes were then isolated using a published method.[72] Briefly, the diced tissue is digested with 700U pronase E™ for 1 hour at 37˚C on a rotary mixer. Then 100U/mL collagenase XI and 0.1mg/mL for Dnase I, were added and the cartilage digested for 16 hours to release the chondrocytes from the ECM.[72] Chondrocytes from the supernatant were then strained through a 70µm sieve. Then washed and pelleted three times in 10% CCM by centrifugation at 750g. Cell viability was then determined by Trypan Blue exclusion. Briefly, 10µL of the final chondrocyte suspension were mixed with buffered Trypan Blue dye and cells that excluded the dye were counted on a Neubald Hemacytometer. CHITOSAN GEL PREPERATION & CELL ENCAPSULATION. Gel formation and cell encapsulation was based upon a previously published method.[71] In brief, isolated cells were resuspended in 1 of 2 cellulose solutions and mixed with a 2% (w/v) protasan solution which is dissolved in 0.1M βGP solution. The βGP solution was added to the protasan solution on ice over a magnetic stirring plate. 700µL was then placed in the wells of 24 well plates using wide bore pipette tips. The two cellulose concentrations used were 12.5mg/ml and 25mg/ml. Cells were pelleted down then resuspended in the filter steralised cellulose solutions. 175µL of each cellulose solution was pippeted into the wells and the gels were manual mixed. Negative control gels were also cast with plain cellulose solution. Gels consisted a total of 875µL of materials, giving an approximate depth of 0.5cm in the well. Cell concentration was 250,000 cells per well. 22 Gels were placed in a 37˚C, 5% CO2 incubator to set. They were rinsed thrice with 1ml of DMEM-F12 for 20 minutes. 1ml CCM was then placed on the gels for the duration of the experiment. Gels were kept at 37˚C in a humidified atmosphere containing 95% air and 5% CO2. Positive controls with the same cell number where kept in 1ml CCM and digested with the day 0 samples. SAMPLING 5 gels were cast for each cellulose concentration (with corresponding controls), for each time point. These gels and medium were biochemically analysed separately. 2 more gels were cast for each cellulose concentration for live/dead analysis, with medium from these gels used to monitor pH. SAMPLE PREPERATION FOR BIOCHEMICAL ANALYSIS Samples were digested with 10 U/ml proteinase K in 100mM ammonium Acetate, pH 7.0 at 60˚C for 2 hours with agitation. The protinase K was then inactivated by heating to 95˚C for 10 minuites and samples were store at -20˚C for analysis. ANALYSIS LIVE/DEAD VIABILITY Viability in the gels was evaluated using a fluorescence technique. The gels designated for this purpose were washed twice with 1ml of PBS for 20 minutes, to remove residue CCM. 1µL of ethidium homodimer (red) and 2µL of calcein AM (green) dissolved in 1ml PBS, was placed in with each gel and left for 1 hour. After a further 20 minute wash in 1ml PBS to remove excess reagents, part of each gel was compressed between a microscope slides and cover. These were then visualized using a Zeiss fluorescence microscope equipped with a digital camera. Under these conditions live cells fluoresce green and dead cells red. No formal analysis was undertaken, other than a visual approximation of % viability. Images were captured by the camera for possible further software analysis. 23 GAG / DIMETHYLMETHYLENE BLUE DYE The GAG content was analysed using a standard method.[73] Sulphated GAGs were detected spectrophotometrically in the digestion by 1,9-dimethylmethylene blue (DMMB) dye method. This method detects anions, which when in complex with DMMB alters its absorbance.[74] 50µL of samples or standard, in triplicate, were mixed with 200µL of 32mg/L DMMB dye in 40 mM glycine buffer at pH3.0, in a 96 well plate. The plate was then read immediately on a spectrophometric plate reader. Absorbance values at 490nm were read against a standard curve plotted from 0, 2, 10, 50, 100, 200 µg/ml bovine tracheal chondroitin sulphate standards. DNA/ PICOGREEN™ DNA was quantified spectrophometrically using the Picogreen™ dye, which binds to double stranded DNA. When bound it forms a fluorescent complex through a proposed binding of the DNA polymer.[75] 10µL volume of each sample and control were added to 215µL of 10mM Tris-EDTA pH 7.4, in duplicate. An equal amount of Picogreen™ dye, dissolved in DMSO, was added. Fluoresence emission counts were read at 535nm against a standard curve of 0, 25, 250, 2500, 25000 pg/ml DNA. Cell number was calculated using the reported average number of 7.7pg of DNA per chondrocyte.[76] STATISTICAL ANAYLSIS All data represents the mean and standard deviation values derived from 5 replicates at each time point. An paired Student’s t test was applied where indicated using SPSS™ v14 software. A level of 5% was considered significant (p<0.05). 24 REFERENCES 1. Hall, B.K. and T. Miyake, All for one and one for all: condensations and the initiation of skeletal development. Bioessays, 2000. 22(2): p. 138-47. 2. Stockwell, R.A., The cell density of human articular and costal cartilage. J Anat, 1967. 101(Pt 4): p. 753-63. 3. Stockwell, R.A., Biology of cartilage cells. 1979: CAmbridge: Cambridge University Press. 4. Archer, C.W. and P. Francis-West, The chondrocyte. Int J Biochem Cell Biol, 2003. 35(4): p. 401-4. 5. DeLise, A.M., L. Fischer, and R.S. Tuan, Cellular interactions and signaling in cartilage development. Osteoarthritis Cartilage, 2000. 8(5): p. 309-34. 6. Mankin, H.J., et al., Articular Cartilage structure composition and function. Orthopaedic basic science: biology and biomechanics of the musculoskeletal system. 2000: Rosemont III: American Academy of Orthopaedic Surgeons. 7. Martin, R.B., D.B. Burr, and N.A. Sharkey, Skeletal Tissue Mechanics. 1998: Springer-Verlag New York. 8. Huber, M., S. Trattnig, and F. Lintner, Anatomy, biochemistry, and physiology of articular cartilage. Invest Radiol, 2000. 35(10): p. 573-80. 9. von der Mark, H., et al., Immunochemistry, genuine size and tissue localization of collagen VI. Eur J Biochem, 1984. 142(3): p. 493-502. 10. Diab, M., J.J. Wu, and D.R. Eyre, Collagen type IX from human cartilage: a structural profile of intermolecular cross-linking sites. Biochem J, 1996. 314 ( Pt 1): p. 32732. 11. Mayne, R., Structure and function of collagen types. 1987, Orlando; London: Academic Press. 25 12. Mow, V.C., W.Y. Gu, and F.H. Chen, eds. Structure and function of articular cartilage. 3 ed. Basic orthopedic biomechanics and mechanobiology, ed. M.V. C and H. R. 2005, Lipincott Williams and Wilkins: Philadelphia. 13. Poole, A.R., et al., Composition and structure of articular cartilage: a template for tissue repair. Clin Orthop Relat Res, 2001(391 Suppl): p. S26-33. 14. Poole, A.R., Cartilage in Health and Disease. 14 ed. Arthritis and Allied Conditions. A Textbook of Rheumatology. Vol. 1. 2001: Lippincott Williams And Wilkins. 15. Chow, G., et al., Antisense inhibition of chondrocyte CD44 expression leading to cartilage chondrolysis. Arthritis Rheum, 1998. 41(8): p. 1411-9. 16. Mow, V.C., et al., Biphasic creep and stress relaxation of articular cartilage in compression? Theory and experiments. J Biomech Eng, 1980. 102(1): p. 73-84. 17. Venn, M.F., Chemical composition of human femoral and head cartilage: influence of topographical position and fibrillation. Ann Rheum Dis, 1979. 38(1): p. 57-62. 18. Bloebaum, R.D. and K.M. Radley, Three-dimensional surface analysis of young adult human articular cartilage. J Anat, 1995. 187 ( Pt 2): p. 293-301. 19. Mow, V.C., C.C. Wang, and C.T. Hung, The extracellular matrix, interstitial fluid and ions as a mechanical signal transducer in articular cartilage. Osteoarthritis Cartilage, 1999. 7(1): p. 41-58. 20. Gu, W.Y., W.M. Lai, and V.C. Mow, A mixture theory for charged-hydrated soft tissues containing multi-electrolytes: passive transport and swelling behaviors. J Biomech Eng, 1998. 120(2): p. 169-80. 21. Buckwalter, J.A., Articular cartilage: injuries and potential for healing. J Orthop Sports Phys Ther, 1998. 28(4): p. 192-202. 22. Jackson, D.W., et al., Spontaneous repair of full-thickness defects of articular cartilage in a goat model. A preliminary study. J Bone Joint Surg Am, 2001. 83-A(1): p. 5364. 23. Shapiro, F., S. Koide, and M.J. Glimcher, Cell origin and differentiation in the repair of full-thickness defects of articular cartilage. J Bone Joint Surg Am, 1993. 75(4): p. 532-53. 26 24. Jackson, R.W. and C. Dieterichs, The results of arthroscopic lavage and debridement of osteoarthritic knees based on the severity of degeneration: a 4- to 6-year symptomatic follow-up. Arthroscopy, 2003. 19(1): p. 13-20. 25. Pridie, A., The method of resurfacing osteoarthritic knee joints. J bone Joint Surg, 1959. 41: p. 618. 26. Steadman, J.R., et al., [The microfracture technic in the management of complete cartilage defects in the knee joint]. Orthopade, 1999. 28(1): p. 26-32. 27. Sledge, S.L., Microfracture techniques in the treatment of osteochondral injuries. Clin Sports Med, 2001. 20(2): p. 365-77. 28. Grande, D.A., et al., The repair of experimentally produced defects in rabbit articular cartilage by autologous chondrocyte transplantation. J Orthop Res, 1989. 7(2): p. 208-18. 29. Brittberg, M., et al., Treatment of deep cartilage defects in the knee with autologous chondrocyte transplantation. N Engl J Med, 1994. 331(14): p. 889-95. 30. Minas, T. and S. Nehrer, Current concepts in the treatment of articular cartilage defects. Orthopedics, 1997. 20(6): p. 525-38. 31. Breinan, H.A., et al., Effect of cultured autologous chondrocytes on repair of chondral defects in a canine model. J Bone Joint Surg Am, 1997. 79(10): p. 1439-51. 32. Hangody, L., et al., Arthroscopic autogenous osteochondral mosaicplasty for the treatment of femoral condylar articular defects. A preliminary report. Knee Surg Sports Traumatol Arthrosc, 1997. 5(4): p. 262-7. 33. Hangody, L., et al., Mosaicplasty for the treatment of articular cartilage defects: application in clinical practice. Orthopedics, 1998. 21(7): p. 751-6. 34. Lexer, E., The classic. Joint transplantation. 1908. Clin Orthop Relat Res, 1985(197): p. 4-10. 35. Sammarco, V.J., et al., Human articular cartilage storage in cell culture medium: guidelines for storage of fresh osteochondral allografts. Orthopedics, 1997. 20(6): p. 497-500. 36. Ohlendorf, C., W.W. Tomford, and H.J. Mankin, Chondrocyte survival in cryopreserved osteochondral articular cartilage. J Orthop Res, 1996. 14(3): p. 413-6. 27 37. Ghazavi, M.T., et al., Fresh osteochondral allografts for post-traumatic osteochondral defects of the knee. J Bone Joint Surg Br, 1997. 79(6): p. 1008-13. 38. Garrett, J.C., Treatment of osteochondral defects of the distal femur with fresh osteochondral allografts: a preliminary report. Arthroscopy, 1986. 2(4): p. 222-6. 39. Kwan, M.K., et al., Histological and biomechanical assessment of articular cartilage from stored osteochondral shell allografts. J Orthop Res, 1989. 7(5): p. 637-44. 40. Gross, A.E., et al., The allotransplantation of partial joints in the treatment of osteoarthritis of the knee. Clin Orthop Relat Res, 1975(108): p. 7-14. 41. McDermott, A.G., et al., Fresh small-fragment osteochondral allografts. Long-term follow-up study on first 100 cases. Clin Orthop Relat Res, 1985(197): p. 96-102. 42. Risbud, M.V. and M. Sittinger, Tissue engineering: advances in in vitro cartilage generation. Trends Biotechnol, 2002. 20(8): p. 351-6. 43. Freed, L.E., G. Vunjak-Novakovic, and R. Langer, Cultivation of cell-polymer cartilage implants in bioreactors. J Cell Biochem, 1993. 51(3): p. 257-64. 44. Frenkel, S.R. and P.E. Di Cesare, Scaffolds for articular cartilage repair. Ann Biomed Eng, 2004. 32(1): p. 26-34. 45. Lu, L., et al., Biodegradable polymer scaffolds for cartilage tissue engineering. Clin Orthop Relat Res, 2001(391 Suppl): p. S251-70. 46. Coutts, R.D., et al., Matrices for cartilage repair. Clin Orthop Relat Res, 2001(391 Suppl): p. S271-9. 47. Hunziker, E.B., Growth-factor-induced healing of partial-thickness defects in adult articular cartilage. Osteoarthritis Cartilage, 2001. 9(1): p. 22-32. 48. Chu, C.R., et al., Osteochondral repair using perichondrial cells. A 1-year study in rabbits. Clin Orthop Relat Res, 1997(340): p. 220-9. 49. Dounchis, J.S., et al., Cartilage repair with autogenic perichondrium cell and polylactic acid grafts. Clin Orthop Relat Res, 2000(377): p. 248-64. 50. Giurea, A., et al., Adhesion of perichondrial cells to a polylactic acid scaffold. J Orthop Res, 2003. 21(4): p. 584-9. 28 51. Liu, Y., et al., Repairing large porcine full-thickness defects of articular cartilage using autologous chondrocyte-engineered cartilage. Tissue Eng, 2002. 8(4): p. 709-21. 52. Sherwood, J.K., et al., A three-dimensional osteochondral composite scaffold for articular cartilage repair. Biomaterials, 2002. 23(24): p. 4739-51. 53. Kawabe, N. and M. Yoshinao, The repair of full-thickness articular cartilage defects. Immune responses to reparative tissue formed by allogeneic growth plate chondrocyte implants. Clin Orthop Relat Res, 1991(268): p. 279-93. 54. Peretti, G.M., et al., A biomechanical analysis of an engineered cell-scaffold implant for cartilage repair. Ann Plast Surg, 2001. 46(5): p. 533-7. 55. Gelse, K., et al., Articular cartilage repair by gene therapy using growth factor- producing mesenchymal cells. Arthritis Rheum, 2003. 48(2): p. 430-41. 56. Bouwmeester, S.J., et al., Long-term results of rib perichondrial grafts for repair of cartilage defects in the human knee. Int Orthop, 1997. 21(5): p. 313-7. 57. Weisser, J., et al., Role of growth factors in rabbit articular cartilage repair by chondrocytes in agarose. Osteoarthritis Cartilage, 2001. 9 Suppl A: p. S48-54. 58. Rahfoth, B., et al., Transplantation of allograft chondrocytes embedded in agarose gel into cartilage defects of rabbits. Osteoarthritis Cartilage, 1998. 6(1): p. 50-65. 59. Dausse, Y., et al., Cartilage repair using new polysaccharidic biomaterials: macroscopic, histological and biochemical approaches in a rat model of cartilage defect. Osteoarthritis Cartilage, 2003. 11(1): p. 16-28. 60. Marijnissen, W.J., et al., Tissue-engineered cartilage using serially passaged articular chondrocytes. Chondrocytes in alginate, combined in vivo with a synthetic (E210) or biologic biodegradable carrier (DBM). Biomaterials, 2000. 21(6): p. 571-80. 61. Sams, A.E., et al., Local and remote matrix responses to chondrocyte-laden collagen scaffold implantation in extensive articular cartilage defects. Osteoarthritis Cartilage, 1995. 3(1): p. 61-70. 29 62. Sellers, R.S., et al., Repair of articular cartilage defects one year after treatment with recombinant human bone morphogenetic protein-2 (rhBMP-2). J Bone Joint Surg Am, 2000. 82(2): p. 151-60. 63. Samuel, R.E., et al., Delivery of plasmid DNA to articular chondrocytes via novel collagen-glycosaminoglycan matrices. Hum Gene Ther, 2002. 13(7): p. 791-802. 64. Carruthers, J. and A. Carruthers, Mad cows, prions, and wrinkles. Arch Dermatol, 2002. 138(5): p. 667-70. 65. Knudson, W., et al., Hyaluronan oligosaccharides perturb cartilage matrix homeostasis and induce chondrocytic chondrolysis. Arthritis Rheum, 2000. 43(5): p. 1165-74. 66. Solchaga, L.A., et al., Treatment of osteochondral defects with autologous bone marrow in a hyaluronan-based delivery vehicle. Tissue Eng, 2002. 8(2): p. 333-47. 67. Lahiji, A., et al., Chitosan supports the expression of extracellular matrix proteins in human osteoblasts and chondrocytes. J Biomed Mater Res, 2000. 51(4): p. 586-95. 68. Chenite, A., et al., Novel injectable neutral solutions of chitosan form biodegradable gels in situ. Biomaterials, 2000. 21(21): p. 2155-61. 69. Roughley, P., et al., The potential of chitosan-based gels containing intervertebral disc cells for nucleus pulposus supplementation. Biomaterials, 2006. 27(3): p. 388-96. 70. VandeVord, P.J., et al., Evaluation of the biocompatibility of a chitosan scaffold in mice. J Biomed Mater Res, 2002. 59(3): p. 585-90. 71. Hoemann, C.D., et al., Tissue engineering of cartilage using an injectable and adhesive chitosan-based cell-delivery vehicle. Osteoarthritis Cartilage, 2005. 13(4): p. 31829. 72. Lee, D.A. and M.M. Knight, Mechanical loading of chondrocytes embedded in 3D constructs: in vitro methods for assessment of morphological and metabolic response to compressive strain. Methods Mol Med, 2004. 100: p. 307-24. 73. Calabro, A., V.C. Hascall, and R.J. Midura, Adaptation of FACE methodology for microanalysis of total hyaluronan and chondroitin sulfate composition from cartilage. Glycobiology, 2000. 10(3): p. 283-93. 30 74. Farndale, R.W., C.A. Sayers, and A.J. Barrett, A direct spectrophotometric microassay for sulfated glycosaminoglycans in cartilage cultures. Connect Tissue Res, 1982. 9(4): p. 247-8. 75. Singer, V.L., et al., Characterization of PicoGreen reagent and development of a fluorescence-based solution assay for double-stranded DNA quantitation. Anal Biochem, 1997. 249(2): p. 228-38. 76. Kim, Y.J., et al., Fluorometric assay of DNA in cartilage explants using Hoechst 33258. Anal Biochem, 1988. 174(1): p. 168-76. 31 TABLE OF CONTENTS Cartilage .................................................................................................................................... 3 Components of cartilage ........................................................................................................ 3 Chondrocytes ..................................................................................................................... 3 Components of the extracellular matrix (ECM) ................................................................ 4 Interstitial fluid .................................................................................................................. 7 Articular cartilage ...................................................................................................................... 9 Zones ..................................................................................................................................... 9 Superficial zone ................................................................................................................. 9 Transitional Zone............................................................................................................. 10 Deep Zone ....................................................................................................................... 10 Calcified zone .................................................................................................................. 10 Articular cartilage formation ............................................................................................... 10 Articular cartilage injury & treatments.................................................................................... 12 Articular cartilage injury ..................................................................................................... 12 Treatments of articular cartilage injury ............................................................................... 12 Arthroscopy / lavage ........................................................................................................... 12 Marrow stimulating techniques ........................................................................................... 13 Implantation......................................................................................................................... 13 Autogenous chondrocyte implantation ........................................................................... 13 Cartilage transplantation.................................................................................................. 14 Tissue engineering ................................................................................................................... 17 Scaffolds .............................................................................................................................. 17 Synthetic scaffold materials ............................................................................................ 18 Natural scaffold materials................................................................................................ 18 Methods ................................................................................................................................... 21 Materials .............................................................................................................................. 21 32 Medium ........................................................................................................................... 21 Gel Components .............................................................................................................. 21 Experimental Methods ........................................................................................................ 22 Isolation of chondrocytes from articular cartilage ........................................................... 22 Chitosan gel preperation & cell encapsulation. ............................................................... 22 Sampling .......................................................................................................................... 23 Analysis ........................................................................................................................... 23 Statistical anaylsis ............................................................................................................... 24 References ............................................................................................................................... 25 Table of Contents .................................................................................................................... 32 33