הודעה על החמרה ( מידע בטיחות)
advertisement
")
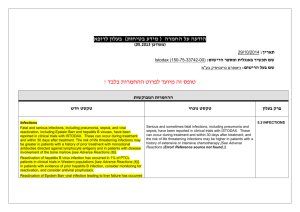
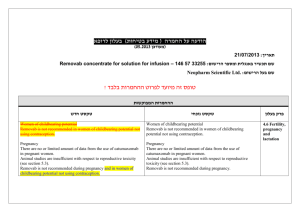
בטיחות) מידע בטיחות) החמרה (( מידע על החמרה הודעה על הודעה תאריך _________ 9ספטמבר_______2009 , שם תכשיר באנגלית_DILANTIN מספר רישום ___ 123 70 24017 שם בעל הרישום __PFIZER PHARMACEUTICALS ISRAEL LTD השינויים המבוקשים על רקע צהוב לצרכן בעלון לצרכן בעלון פרטים על השינוי/ים המבוקש/ים טקסט נוכחי פרק בעלון אין להשתמש אם ידועה לך רגישות לאחד ממרכיבי התרופה מתי אין להשתמש בתרופה? אין להשתמש בתרופה מבלי להיוועץ ברופא לפני התחלת הטיפול: אזהרות: תגובות בין תרופתיות תופעות לוואי המחייבות התייחסות מיוחדת: טקסט חדש אין להשתמש אם ידועה לך רגישות לאחד ממרכיבי התרופה או לתרופות ממשפחת ההידנטואין. אם הינך סובל/ת או סבלת בעבר מליקוי בתפקוד :מערכת החיסון ,סכרת ,חווית בעבר תופעות של רגישות יתר לתרופות נוגדות פרכוסים Anticonvulsant Hypersensitivity )Syndrome (AHS בטיפול ממושך בתרופה יש לערוך בדיקת צפיפות עצם ורמות ויטמין Dבאופן תקופתי. טניפוזיד ,חומצה פולית תנועות לא רצוניות של העיניים ,הפרעה בחוש הטעם ,שיעור יתר ,מחלת פיירוני, שוק אנפילקטי ,קשיי נשימה עד אובדן הכרה )דווח במתן בהזרקה או במינון יתר) :הפסק את הטיפול ופנה לרופא מיד רופא בעלון ללרופא בעלון פרטים על השינוי/ים המבוקש/ים פרק בעלון CONTRAINDICATIONS Special warnings and precautions טקסט נוכחי Dilantin is contraindicated in those patients with a history of hypersensitivity to phenytoin or other hydantoins. טקסט חדש Dilantin is contraindicated in those patients with a history of hypersensitivity to phenytoin or other hydantoins, or the inactive ingredients of this preparation. Anticonvulsant Hypersensitivity Syndrome (AHS) is a rare drug induced, multiorgan syndrome which is potentially fatal and occurs in some patients taking anticonvulsant medication. It is 53268 characterized by fever, rash, lymphadenopathy, and other multiorgan pathologies, often hepatic. The mechanism is unknown. The interval between first drug exposure and symptoms is usually 24 weeks but has been reported in individuals receiving anticonvulsants for 3 or more months. for use Patients at higher risk for developing AHS include black patients, patients who have a family history of or who have experienced this syndrome in the past, and immuno-suppressed patients. The syndrome is more severe in previously sensitized individuals. If a patient is diagnosed with AHS, discontinue the phenytoin and provide appropriate supportive measures. Toxic hepatitis and liver damage have been reported and may, in rare cases, be fatal. Cases of acute hepatotoxicity, including infrequent cases of acute hepatic failure, have been reported with phenytoin. These incidents have been associated with a hypersensitivity syndrome characterized by fever, skin eruptions, and lymphadenopathy, and usually occur within the first 2 months of treatment. Other common manifestations include arthralgias, rash, jaundice, hepatomegaly, elevated serum transaminase levels, leukocytosis, and eosinophilia. The clinical course of acute phenytoin hepatotoxicity ranges from prompt recovery to fatal outcomes. In these patients with acute hepatotoxicity, phenytoin should be immediately discontinued and not re-administered. Integumentary Effect - Published literature has suggested that there may be an increased, although still rare, risk of hypersensitivity reactions, including skin rash, SJS, TEN, hepatotoxicity, and Anticonvulsant Hypersensitivity Syndrome in black patients. Studies in patients of Chinese ancestry have found a strong association between the risk of developing SJS/TEN and the presence of HLA-B*1502, an inherited allelic variant of the HLA B gene, in patients using another carbamazepine. Limited evidence suggests that HLA-B*1502 may be a risk factor for the development of SJS/TEN in patients of Asian ancestry taking drugs associated with SJS/TEN, including phenytoin. Consideration should be given to avoiding use of drugs associated with SJS/TEN, including phenytoin, in HLA-B*1502 positive patients when alternative therapies are otherwise equally available. Literature reports suggest that the combination of phenytoin, cranial irradiation and the gradual reduction of corticosteroids may be associated with the development of erythema multiforme, and/or Stevens-Johnson syndrome, and/or toxic epidermal necrolysis. Musculoskeletal Effect Phenytoin and other anticonvulsants that have been shown to induce the CYP450 enzyme are thought to affect bone mineral metabolism indirectly by increasing the metabolism of Vitamin D3. This may lead to Vitamin D deficiency and heightened risk of osteomalacia, bone fractures, osteoporosis, hypocalcemia, and hypophosphatemia in chronically treated epileptic patients. Drug classes which may potentially increase phenytoin serum levels: Analgesic / Anti-inflammatory agents: azapropazone 53268 Interaction Antibacterial agents: erythromycin Anticonvulsants: felbamate Antifungal agents: amphotericin B , fluconazole , ketoconazole, miconazole , itraconazole Benzodiazepines /Psychotropic agents: viloxazine Calcium channel blockers / Cardiovascular agents: diltiazem, nifedipine Proton pump inhibitors: omeprazole Serotonin re-uptake inhibitors: fluvoxamine, sertraline with other medicinal products and other forms of interaction Drugs which may decrease phenytoin plasma levels: Anticonvulsants: vigabatrin Bronchodilators: theophylline Hyperglycemic agents: diazoxide Drugs whose blood levels and/or effects may be altered by phenytoin: Antibacterial agents: praziquantel Anticonvulsants: lamotrigine Antifungal agents: azoles Antineoplastic agents: teniposide Calcium channel blockers / Cardiovascular agents: nicardipine, nimodipine, verapamil Neuromuscular blocking agents: alcuronium, pancuronium vecuronium Opioid analgesics: methadone Oral hypoglycemic agents: chlorpropamide, glyburide Psychotropic agents / Antidepressants: clozapine, Sertraline Patients should be advised not to drive a car or operate potentially dangerous machinery until it is known that this medication does not affect their ability to engage in these activities. Effects on ability to drive and use machines Body as a Whole: Anaphylactoid reaction and anaphylaxis. Special Senses: Taste perversion. Post-marketing Experience: Musculoskeletal System: Bone fractures and osteomalacia have been associated with long-term (10 years) use of phenytoin by patients with chronic epilepsy. Osteoporosis and other disorders of bone metabolism such as hypocalcemia, hypophophatemia and decreased levels of Vitamin D metabolites have also been reported. 53268 Undesirable effects