Bowling 1
Jake Bowling
BIOL 303
10/27/2011
Proteus Syndrome: An Overview
Background
Proteus syndrome (PS) (also Wiedemann’s syndrome) was first described as an
unknown hamartomatous disorder in a clinical publication on birth defects in 1979
(Cohen & Hayden, 1979) and was given its name four years later after the Greek sea-god
Proteus, who in mythology was said to take on multiple forms (Wiedemann, et al. 1983).
PS is characterized by segmental overgrowth and hyperplasia of multiple tissues along
with high susceptibility to tumor development. Despite the syndrome’s rare incidence (<1
in 1 million population), it gained somewhat widespread notice with the release of the
1980 film The Elephant Man, a film about the life of 19th century Englishman and
proteus sufferer Joseph Merrick. PS is a mosaic disorder, meaning some cells in the
patient’s body are affected while others are not (Lindhurst, et al. 2011). Because literature
on this syndrome only started appearing in the 1980’s, much is still being learned about
the characterization, management, and cause of PS. The intent of this paper is to both
provide an overview of what is currently known about the Proteus syndrome and also
discuss recent research being done on the genetics of PS.
Mosaicism
For some time after its first clinical description in 1979, the pathology of PS was
unknown due to it having several unusual characteristics for a congenital disorder. PS
was never reported to recur in a family, yet had been reported in discordant “identical”
twins (Lindhurst, et al. 2011). PS patients also presented with the same overall signs and
symptoms yet had wide variety in the amount of tissue seemingly affected by the
Bowling 2
disorder. These observations led to the currently accepted pathological model of
mosaicism, first published by Happle in 1987. Happle studied several other diseases with
similar unusual characteristics to PS, and proposed that the cause was a lethal mutation in
a gene surviving with mosaicism. He proposed that the mutation causing PS was lethal if
present in the zygote, and that cells with the mutation could only survive in close
proximity to normal cells. This meant the mutation was somatic, yet had to occur early
enough in embryonic development for the eventual child to have enough cells affected to
show noticeable symptoms (Happle 1987). Though at the time and for some time after
this proposition had limited experimental evidence (Biesecker 2006), it has been accepted
as correct because it explains both the nonexistent pattern of inheritance and the wide
variety of severities seen in PS.
Characterization and Diagnosis
Because the mutation causing Proteus occurs early in development, virtually any
body tissue can be affected by the disorder (with the exception of blood cells, which
cannot survive with the mutation) (Lindhurst, et al. 2011). Affected tissues progressively
overgrow, most rapidly at the age of 6-18 months. Bone, connective tissue, and fat seem
to be the most commonly affected tissues. Overgrowth in PS is accompanied by
distortion and calcification, and often the bone under the affected tissue distorts into a
nonfunctional shape. Other common characteristics of PS include vascular
malformations, local overgrowth of fat tissue, and a distinctive skin malformation called
a cerebriform connective tissue nevus (CCTN). A CCTN (Figure 1B, Figure 2B)
typically grows through adolescence on the feet soles or hands, and is called
Bowling 3
“cerebriform” because it resembles the branching meningial grooves of the cerebrum
(Biesecker 2006).
The incredibly wide variety of manifestations of PS makes for a challenging
diagnosis. Though obvious overgrowth is easily suggestive of a hamartomatous
condition, PS is often misdiagnosed as several similar syndromes most commonly
including neurofibromatosis type 1, hemihyperplasia, and multiple lipomatosis syndrome.
Most early descriptions of PS, such as Wiedemann’s 1983 study, did not include defined
diagnostic criteria and actually included many patients with other disorders (Biesecker
2006). In fact, a 2004 study applied today’s diagnostic criteria (Biesecker, et al. 1999) to
previous literature on PS and found that more patients in these studies did not have PS
than truly did (Turner, et al. 2004). Though far from perfect, the most successful
diagnostic criteria to date were established in 1999 (Biesecker, et al. 1999). These criteria
include both a general component that must be met for consideration (mosaic
distribution, sporadic, and progressive manifestations) and a specific component to refine
the diagnosis (Biesecker 2006). A correct diagnosis of PS is important not only to
counsel the patient and their family on the management of the disease but also to exclude
non-PS patients from research studies to ensure valid data.
Bowling 4
QuickTime™ and a
decompressor
are needed to see this picture.
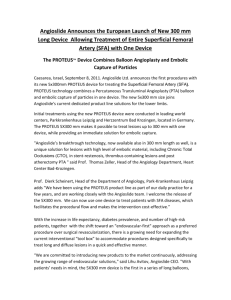
Figure 1: Panels A, B, and C are Proteus patients. CCTN is shown in panel C. Panels D
and E show hemihyperplasia patients exhibiting a different type of “ballooning”
overgrowth. (Biesecker 2006)
Figure 2: A 12 year old boy with PS. Note
the severe bone curvatures and overgrowth
present on hands and feet. (Lindhurst, et al.
2011)
Management
Because the severe overgrowth in Proteus syndrome patients causes both cosmetic
and functional issues, much of the therapy in these patients is aimed at controlling the
overgrowth. This typically involves multiple orthopedic procedures across the
individual’s lifespan (Biesecker 2005). The typical lifespan of a PS patient is tough to
estimate because of the wide variety of severities, but of an estimated 300 published
Bowling 5
cases to date approximately 1/10 reported premature deaths (<30 years of age). A main
cause of death for PS patients has been identified to be deep vein thrombosis and
pulmonary embolism (Cohen 2001). Unfortunately, chronic anticoagulation is not a
recommended option for PS patients because of their widespread presence of vascular
malformations. Finally, though PS patients seem to have a high susceptibility to tumor
development, the data available do not suggest that early detection of these tumors
improves a PS patient’s prognosis (Biesecker 2006). Overall, management of PS
involves regular checkups with physicians and orthopedic surgeries to control the
overgrowth. Though PS patients typically live longer than one would expect given the
huge amount of abnormalities, management of the disorder is challenging both because
of the varying characteristics of the syndrome and because data is scarce due to the small
number of cases. Despite all this, recent research on the genetic basis of PS provides
hope for improved therapies in the near future.
A Genetic Breakthrough
Though the accepted pathogenic model for PS (a somatic mutation which could
only survive in a mosaic state) was published in 1987 (Happle 1987), until recently no
specific mutations were identified as the cause of PS. However, a recent study done by
Lindhurst, et al. (2011) has demonstrated that a mutation in oncogene AKT1 (c.49 G>A,
causing a substitution of lysine for glutamine at amino acid 17) is the definitive cause of
the Proteus syndrome. The study sequenced the entire exome of multiple affected tissues
in PS patients and simply looked for common variants from a human reference sequence,
an approach that was too expensive to consider only a few years ago (Optiz & Jorde
2011).
Across the exomes of 11 tissue samples from 6 different PS patients, 265,821
Bowling 6
total variants from the reference sequence were identified. However, upon software
analysis with several filters, only one of these variants was determined to be significant:
the described point mutation in AKT1 (Lindhurst et al., 2011). AKT1 codes for a protein
kinase in the PTEN-PI3K-AKT pathway, a crucial signaling pathway involved in
apoptosis and cancer cells. The causal mutation identified was found to upregulate the
AKT pathway causing the various symptoms of PS. Mouse studies have showed
supporting evidence - that artificial activation of AKT1 cause calcification and skin
hyperplasia, two of the defining symptoms of PS (Fukai, et al 2010).
On a large scale, the study described represents a significant advancement in
identifying causative mutations. The hypothesis is simple; a mutation shown to recur in
affected patients and not in unaffected people can be said to be causative (if the
functionality of the change is consistent). Even so, the current ability to rapidly and
inexpensively sequence the entire exomes of patients is exciting and will undoubtedly
lead to many more identifications of causal mutations. Aside from these widespread
implications, the identification of the mutation causing PS means an increase in correct
diagnoses and therefore effective management. Though challenges of PS will remain for
the foreseeable future, it is reasonable to say that medical care for Proteus patients will
improve considerably within the decade.
Bowling 7
Glossary
Anticoagulation
Discordant Twins
Hamartoma
Hyperplasia
Mosaic
Oncogene
Protein kinase
Application of a substance that prevents blood from clotting.
Monozygotic twins with a birthweight difference >20%.
Localized overgrowth of a single or combination of tissues
causing little pain.
Increased proliferation of cells.
The presence of two populations of cells with different
genotypes in an individual.
A gene known to, when activated, contribute to cancer cell
development.
An enzyme that phosphorylates other proteins.
Bowling 8
Works Cited
Biesecker LG, Happle R, Mulliken JB et al: Proteus syndrome: diagnostic criteria,
differential diagnosis, and patient evaluation. Am J Med Genet 1999; 84: 389–
395. <http://www.ncbi.nlm.nih.gov.pallas2.tcl.sc.edu/pubmed/10360391>
Biesecker LG: Proteus syndrome; in Cassidy SB, Allanson J (eds): Management of
Genetic Syndromes. Hoboken: John Wiley and Sons, Inc., 2005, vol 1, pp 449–
456.
Biesecker, Leslie. "The Challenges of Proteus Syndrome: diagnosis and management."
European Journal of Human Genetics 14 (2006): 1151-1157.
<http://www.nature.com/ejhg/journal/v14/n11/full/5201638a.html>
Cohen Jr MM, Hayden PW: A newly recognized hamartomatous syndrome. Birth Defects
Orig Artic Ser 1979; 15: 291–296.
Cohen Jr MM: Causes of premature death in Proteus syndrome. Am J Med Genet 2001;
101: 1–3. <http://www.ncbi.nlm.nih.gov.pallas2.tcl.sc.edu/pubmed/11343327>
Fukai A, Kawamura N, Saito T, et al. Akt1 in murine chondrocytes controls cartilage
calcification during endochondral ossification under physiologic and pathologic
conditions. Arthritis Rheum 2010;62:826-836
<http://www.ncbi.nlm.nih.gov.pallas2.tcl.sc.edu/pubmed/20187155>
Happle, R. "Lethal Genes Surviving by Mosaicism: a possible explanation for sporadic
birth defects involving the skin." Journal of the American Academy of
Dermatology 16.4 (1987): 899-906.
Bowling 9
Lindhurst, Marjorie J., et al. "A Mosaic Activating Mutation in AKT1 Associated with
the Proteus Syndrome." The New England Journal of Medicine 365 (2011): 611619. <http://www.nejm.org/doi/full/10.1056/NEJMoa1104017>
Opitz, John M., Jorde, Lynn B., . (2011) Hamartoma Syndromes, Exome Sequencing,
and a Protean Puzzle. New England Journal of Medicine 365:7, 661-663
<http://www.nejm.org/doi/full/10.1056/NEJMe1107384>
Turner JT, Cohen Jr MM, Biesecker LG: Reassessment of the Proteus syndrome
literature: application of diagnostic criteria to published cases. Am J Med Genet
2004; 130A: 111–122.
<http://onlinelibrary.wiley.com.pallas2.tcl.sc.edu/doi/10.1002/ajmg.a.30327/full>
Wiedemann HR, Burgio GR, Aldenhoff P, Kunze J, Kaufmann HJ, Schirg E: The proteus
syndrome. Partial gigantism of the hands and/or feet, nevi, hemihypertrophy,
subcutaneous tumors, macrocephaly or other skull anomalies and possible
accelerated growth and visceral affections. Eur J Pediatr 1983; 140: 5–12.
 0
0