The prevalence of visual impairment in the UK A review of the literature Rosemary Tate, Liam Smeeth, Jennifer Evans, Astrid Fletcher Dept of Epidemiology & Population Health London School of Hygiene & Tropical Medicine Chris Owen St George’s Hospital Medical School Alicja Rudnicka Wolfson Institute of Preventive Medicine Report commissioned by the Royal National Institute for the Blind Acknowledgements Funding for the review was provided by the Royal National Institute for the Blind Advisory Committee Liz Bates (Director Corporate Policy, Ashton, Leigh & Wigan Primary Care Trust) Prof Ian Bruce (VOLPROF, City University) Prof Alistair Fielder (Professor of Ophthalmology, Imperial College London and Western Eye Hospital) Dr Carol Lupton (Policy Research Programme, Department of Health Dr Angela McCullagh (Research Director, The Pocklington Trust) RNIB Lesley-Anne Alexander (Chief Executive) Nigel Charles (Research Development Manager) Fazilet Hadi (Director of Policy) Dr Adam Ockelford (Assistant Director, Education and Employment) Many thanks also to Sue Keil at RNIB who provided extra information for Chapter 5. Special thanks to Nigel Charles for commissioning this project and for invaluable support and advice. Authors’ details Rosemary Tate PhD, research fellow, London School of Hygiene & Tropical Medicine (now at Institute of Child Health) Liam Smeeth MRCP, Senior clinical lecturer in epidemiology, London School of Hygiene & Tropical Medicine Jennifer Evans PhD, lecturer in epidemiology, London School of Hygiene & Tropical Medicine Astrid Fletcher PhD, Professor of epidemiology, London School of Hygiene & Tropical Medicine Chris Owen PhD, Senior Research Fellow in Epidemiology, St George's Hospital Medical School Alicja Rudnicka PhD, Lecturer in Epidemiology & Medical Statistics, Wolfson Institute of Preventive Medicine Contribution of authors Rosemary Tate undertook the literature review and preparation of main tables. Liam Smeeth reviewed and updated Chapter 5 on Children. Jenny Evans contributed the section on blindness registrations and provided critical comments on the review. Chris Owen and Alicja Rudnicka carried out the analyses and wrote the material for Chapter 6. Astrid Fletcher took overall responsibility for the project and wrote the Summary, Chapter 1 and Chapter 7. Authors’ potential conflict of interest Data on self reported visual difficulties and visual acuity measures reviewed in this report comes from the MRC funded Trial of assessment and management of older people in the community (Principal Investigator Astrid Fletcher), the associated causes of vision impairment study funded by the The Pocklington Trust (with Jenny Evans and Richard Wormald) and the nested MRC funded trial of screening for vision impairment within the main MRC Trial (with Liam Smeeth). 1 Summary We identified three approaches to describing visual problems in the population. 1. Visual difficulties - based on self-report of difficulties with vision related functions ranging from single item questions to disability scales. Most studies have used questions on difficulty in “reading newsprint” as minimum criteria for difficulties with seeing. 2. Clinical measures, predominantly visual acuity. Distance visual acuity is the basis for categorising vision impairment in the WHO International Classification of Diseases (ICD). Most studies have measured distance acuity using an illuminated Snellen chart. Visual acuity can be measured with usual aids if worn i.e. contact lenses or glasses (“presenting vision”) or after full refraction for refractive error (“best corrected visual acuity”). In surveys full refraction may not be available and studies may use pinhole correction to try to remove some of the refractive error (pinhole corrected visual acuity). Results may be presented as binocular vision or as vision in the better eye. The WHO ICD classifications use best corrected visual acuity ie vision in the better eye after full correction. Vision impairment is defined as a Snellen acuity <6/18 and blindness is defined as visual acuity <3/60. Visual acuity <6/12 is not used internationally to define impairment but is reported by some studies as it represents a reduction in visual acuity sufficient to affect lifestyle e.g. it corresponds to the requirements for sight for the UK driving licence. A recent report from the WHO Prevention of Blindness group recommends that binocular presenting vision should also be reported in population based surveys as this represents the actual impairment experienced by the individual in their everyday life (whether due to underlying disease such as cataract or due to uncorrected refractive error). Information on the causes of poor acuity provides important information for policy and service provision. Among children, a commonly used criteria is visual loss sufficiently bad to mean a child is identified as being in need of special educational or social services. 3. Vision related “quality of life” describing the impact of vision problems on everyday functioning and well-being using specially developed scales. This is a relatively new area and to date there has been little experience in the use of such scales in population based studies in the UK. A review of the literature was undertaken for all UK population based studies and reports which had included information on at least one of the above. Vision- related quality of life data were available for one study only (from the authors of this report) and are presented in Chapter 6. Findings Visual difficulties The estimates of visual difficulties (described as visual disability in some studies) derive predominantly from large government surveys and are reviewed in Chapter 2. The results show, when using similar survey methods and criteria for visual disability, (as in the OPCS surveys of 1985 and 1996/7) some consistency in the results in the older population: 22% of the over 75s in private households reported difficulties with reading newsprint or worse and 26% when people in communal establishments were included. There was less consistency in the results for the younger age groups where the two surveys differed over 2 fold in their estimates for the 2 population aged 16-64 from 0.8% to 2.0 % mainly due to a difference in the selection criteria into the survey. If the proportion of the younger population with visual difficulties is over estimated this will substantially inflate the numbers with sight difficulties in the population since the numbers of people in the population aged 16-64 is much greater than in the older age groups. Thus the estimated numbers with sight difficulties in private households in England and Wales based on the 1996/7 survey was estimated at nearly 2 million compared to 1.4 million from the 1985 survey. There are doubts concerning the reliability of all estimates based on the criteria of “difficulties with reading newsprint” or worse. The lack of reliability is based on findings from the OPCS/RNIB 1998/1999 survey. The sample for this study included a re- survey of respondents who had reported sight difficulties in the 1996/7 survey. A substantial proportion of respondents who initially self reported with a sight problem denied on re-survey they had had a sight problem. The main change in response was to the questions: “Difficulty in seeing a friend across the road” and “Difficulty reading ordinary newsprint”. With more severe task difficulties the level of misclassification was minimal. The estimates of visual disability in the OPCS/RNIB 1998/1999 study took account of this misreporting and were considerably lower than either of the two previous surveys with a prevalence for difficulties with reading newsprint or worse of 14% for the over 75s and 1.1% for the 16-59 age group. However, estimates from the OPCS/RNIB 1998/1999 study may be too low because they exclude some people who initially had a problem and had subsequently received treatment. Confidence in the results on is further limited by the lack of detailed information on response rates in the government surveys. These surveys used a “sift” approach to screen out people with no apparent disability with successive reductions in response with successive sifting. Although the final response rates in the sample from which the estimates are derived are not clearly presented they are of the order of 50% or less in most government surveys. The representativeness of the surveyed population is therefore difficult to assess. Visual acuity The studies which have measured visual acuity in the population are reviewed in Chapter 3. The overwhelming majority of studies have been in the older population. Because of differences between studies in reporting results and criteria for defining visual impairment it was not possible to pool the results to obtain a single estimate. The prevalence of vision impairment varied according to the definitions for defining visual impairment and whether refractive error was included in the estimates. Prevalence of visual impairment Studies using visual acuity measurements have used various criteria for definitions and cut points of visual impairment. The results from two studies: National Diet and Nutrition Study (NDNS), and MRC Assessment Trial that were nationally representative of the older population and use uncorrected presenting VA and similar cut points are given in the table below (unpublished data 3 from NDNS provided by Dr van der Pols and unpublished data on VA <6/12 for MRC Assessment Trial using same LogMar criteria as NDNS). 65-74 NDNS community sample1 VA <6/18 VA<6/12 MRC Assessment Trial2 VA <6/18 VA<6/12 475 5.6 15.8 Age group not included 95% CI 75-84 95%CI 429 13.3 28.3 3.5, 7.6 12.6, 19.1 11500 8.5 18.7 85+ 95% CI 10.1, 16.5 24.1, 32.6 222 31.7 54.0 25.5, 37.8 47.4, 60.6 7.1, 9.8 16.5, 20.9 3100 26.8 45.8 23.9, 29.7 42.2, 49.5 1 Best score (Glasgow Acuity Cards) of two eyes without pinhole correction 2 Binocular acuity without pinhole correction These results show that the point prevalence estimates of vision impairment (VA <6/18) are : 6% NDNS only) at ages 65-74, 8% to 13% at ages 75-84 and 27% to 32% at ages 85+. Estimates of the prevalence of minor visual loss (visual acuity <6/12) are 16% (NDNS only) at ages 65-74, between 19% to 28% at ages 75-84 and 46% to 54% at ages 85+. Considering the upper and low bounds of the 95% confidence intervals the results show that the estimates of vision impairment (VA <6/18) range from 4% to 8 % (NDNS only) at ages 65-74, 7% to 16% at ages 75-84 and 24% to 38% at ages 85+. Similarly the range of estimates of the prevalence of minor visual loss (visual acuity <6/12) are from 13% to 19% (NDNS only) at ages 65-74, between 16% to 33% at ages 75-84 and 42% to 61% at ages 85+. Estimates for the nursing home population from NDNS show high levels of pinhole corrected vision impairment (VA <6/18): 12.1% at ages 65-74 (95% CI 9.7%, 23.2%), 30.0% of those aged 75-84 (95% CI 20.5%, 39.5%) and 46.9% of those aged 85+ (95% CI 37.7%, 56.1%). However as these are the only recent estimates available for the nursing home population we recommend that they are viewed with some caution. Two studies provided estimates of blindness using international criteria of VA < 3/60. In the MRC assessment trial the estimates for blindness for the 75+ age group were 2.1 (95% CI 1.8, 2.4) and in a small study in London the estimates for blindness were very similar (1.9%) although the confidence intervals were very wide (0.2, 6.6) In Chapter 4 we reviewed the few UK studies which have provided some information on the causes of vision impairment. Untreated refractive error and cataracts are the major remediable causes of vision impairment in older people ranging from 50% to 70% as a proportion of visual impairment. With increasing age the proportion of treatable vision impairment declines as age related macular degeneration becomes more prevalent. In Chapter 3 we reviewed an earlier report from the RNIB that raised concerns that a large proportion of the visually impaired population were not on the Blind/partial Sight register. As the 4 results for visual impairment from that report were based on sight tests alone without excluding possible remediable conditions (such as refractive error and cataracts) the registerable component is likely to have been considerably overestimated (around two fold). We showed that, based on other studies which have collected data on the causes of vision impairment, the numbers likely to be registered because of permanent vision loss and the actual numbers registered from Department of Health statistics were of a similar magnitude (and differed by about 10%, possible range 0% to 20%). We conclude that, although registration rates may show some under ascertainment in the older age groups, the evidence does not support substantial under-reporting. Chapter 5 summarises the literature relating to the prevalence of visual impairment and visual disability in children in the UK. Most of the available data about visual loss in children comes from registers or from surveys of providers of health care, social care or educational services to children with visual loss. There are marked variations in the criteria used to define visual disability and visual impairment in different areas of the UK and in the various surveys performed. Caution is required in interpretation of any single estimate of the prevalence of visual impairment or blindness among children in the UK. However, using a broad and pragmatic definition of visual loss sufficiently poor as to mean a child is identified as being in need of special educational or social services, the existing data suggest a prevalence of visual impairment in the region of 10-20/10,000 children. For severe visual loss, the best estimate available suggests a cumulative incidence of blindness or severe visual impairment by the age of 16 years of 5.9/10,000 children. Notably, around half the children receiving support from visual impairment services may have additional disabilities, and this proportion may be even higher for children with severe visual loss. Only one UK population based study reported vision related quality of life. Using the NEI-VFQ 25, 69% reported their vision was excellent or good and 31% reported their vision as fair or poor. Around a half reported problems with near or distance activities. Visual acuity levels were strongly associated with all sub-scales except ocular pain. The most important scales related to visual acuity were general vision, near activities, and social functioning and, to a lesser extent, dependency and colour vision. However visual acuity only explained about a fifth of the variation between people in their reporting on these scales. Most studies have been done in the older population and there is a scarcity of data in younger adult age groups in the UK. A review of epidemiological studies performed in Western Europe, North America and Australia covering the age group 20 to 59 years found the prevalence of blindness was 0.08 and of visual acuity 6/24 to 6/48 was 0.07%. These figures agree well with the prevalence of registrations in a similar age range and we conclude that registration data provide reasonably accurate estimates of the prevalence of serious vision impairment in the younger adult age groups. Information is lacking on less severe levels of visual acuity. Conclusions and Recommendations Policy Estimates of the numbers of people in the population with sight problems are critically dependent on the validity of the methods, definitions used and the quality of the studies (such as response rates and representativeness of the population). 5 Estimates based on self report from government surveys are less reliable than estimates based on visual acuity because of concerns about the validity of the questions and the poorer response rates. In addition, these estimates are likely to be a substantial overestimate of the numbers since they include people with minimal problems. Estimates based on visual acuity measurements from the representative studies of the older population are sufficiently consistent for general purposes of planning and estimation of the proportion and numbers of people in the UK with vision impairment. However we caution that these estimates are seen as approximations and not as “tablets of stone” as prevalence estimates will vary from place to place and over time and because all estimates carry a range of uncertainty as shown by the 95% confidence intervals. Estimating the prevalence of vision impairment for future older populations requires assumptions about temporal trends in the underlying conditions, and future levels of service provision and uptake. No data are available on temporal trends in the incidence of refractive error, cataracts or age related macular degeneration and such data would be prohibitively expensive to obtain. The estimated increase in the proportion of people with age related macular degeneration eligible for registration has been calculated to increase by 11% over a 11 year period to from 2000 to 2020 assuming no change in the prevalence of this condition or improved treatments Studies in the older population have consistently shown that about 50% of visual impairment is due to treatable conditions i.e. cataract and refractive error. Appropriate action e.g. media campaigns and advocacy is required to ensure that eye care providers are aware of the current unacceptably high levels of untreated conditions. Campaigns should also target older people and their carers to raise awareness of poor vision in later life and the potential for improving visual impairment through spectacle correction and cataract surgery. For children, agreed criteria to define visual disability, visual impairment and the need for specialist support are needed. The needs of children with visual disability who also have other disabilities should also be a priority. Recommendations for adoption of standards for measurement and reporting We have shown the considerable variation in definitions and cut points used in the UK based studies. We strongly recommend the adoption of standards for measurement and reporting which have been recommended by international organisations (WHO and the International Council of Ophthalmology) and are described in Chapter 7. Vision related quality of life scales are a useful adjunct to clinical measurements, but should not be used as a substitute for visual acuity. We recommend the use of validated questionnaires or scales for measuring self reported vision problems or vision related quality of life. We emphasize the need to thoroughly test all questions before use in surveys. We encountered difficulties in understanding the methods and basis for calculations in some of the reports we reviewed due to a lack of clarity and transparency in the reporting of data. We recommend that reports which present novel research findings (but are not submitted for publication in academic journals) should conform to the same standards of reporting as the 6 formal peer review process of academic journals (for example as published by the International Council of Medical Editors). Further details are given in Chapter 7. Recommendations for further research Most studies have been done in the older population and there is a scarcity of data in younger adult age groups in the UK. A review of epidemiological studies performed in Western Europe, North America and Australia covering the age group 20 to 59 years found the prevalence of blindness was 0.08 and of visual acuity 6/24 to 6/48 was 0.07%. These figures agree well with the prevalence of registrations in a similar age range and we conclude that registration data provide reasonably accurate estimates of the prevalence of serious vision impairment in the younger adult age groups. Information is lacking on less severe levels of visual impairment. Due to the lack of data on the prevalence of visual problems, visual impairment or specific types of eye disease in ethnic groups in the UK population, studies in ethnic groups are required. The reasons for higher levels of vision impairment in women and in more deprived social groups requires further understanding, in particular the extent, if any, to which this reflects under utilisation of services. The reasons for high levels of treatable conditions in the older population require further investigation. In particular information is required on public awareness of signs and symptoms of treatable conditions, and barriers to service utilisation and access. New strategies to identify the most cost effective way of screening the older population for vision impairment are urgently needed. 7 Chapter 1 Introduction 8 Valid and reliable estimates of the levels of vision impairment in a population are important to a number of agencies and professional groups, which include national policy makers, health and social service providers, health professionals, public health departments and academic institutions including epidemiologists and voluntary sector organizations. We emphasize validity and reliability as key data requirements. Users of data on visual problems need to be reassured that the measures are valid i.e. measuring vision problems relevant to the use to which the data will be put. In this context we define reliable to mean that the estimates are obtained from well conducted studies, measured without bias and with a high level of precision. Although user perspectives may vary in emphasis and focus the critical information required relates to the classic epidemiological questions: How much, Who, Where, When, and Why? All these questions require a clear definition of What is the problem. We will discuss the What? question at the end of this section although of course it normally would be the starting point in any study. How much of a disease/condition is there in a population? In quantifying how much of a condition there is in a population, different measures are used. Prevalence is a measure of the number of people with a disease/ condition at a particular time point in relation to the total number of people in the population. This is typically expressed in terms of a proportion (usually %) and sometimes described as a prevalence rate. A prevalence measure requires a time reference which relates to the point at which the estimates are made, e.g. over a few days or months or annually. Often however the period is not clearly described. For most surveys the prevalence is point prevalence. Incidence is a measure that describes the number of new cases of the disease/condition that occur over a specified time period in people who were disease/condition free at the start of the period. Numbers of people in a population with the disease/condition at a particular time point are estimated by applying prevalence rates, which are usually obtained from surveys, to national population estimates. These measures are all useful because they each provide a different perspective. Prevalence rates describe the relative importance of a disease/condition in terms of how common it is. This aids in prioritizing the diseases/conditions which makes the largest contributions to a population’s ill health. Epidemiologists use prevalence data from a number of international populations for comparative purposes as a first step in understanding the aetiology or risk factors related to a disease/condition. Crucial to interpretation of these data are age standardisations to ensure that the population data being compared are adjusted for any age differences as for most diseases age is the major prognostic factor of morbidity. Incidence data provide information on the natural history of a disease/condition; identifying people and the associated risk factors which best predict the development of the disease/condition. The gap between prevalence and incidence is also a measure of whether a disease/condition is chronic or curative. The actual numbers in a population are vital for planning services and to voluntary sector organizations for understanding the size of the client group on whose behalf they are campaigning. 95% confidence intervals. Although prevalence or incidence rates are a single number, the estimates should be presented with their 95% confidence intervals. 95% confidence intervals give the range i.e. an upper and lower boundary within which the true but unknown estimate will lie. The 95% is a measure of our certainty about this range i.e. we are 95% certain. Who has the disease/condition? 9 Prevalence measures are usually described by the major demographic characteristics of age group and sex, because these data are easy to collect and because most disease/conditions vary considerably across age groups. Sex differences may also be important suggesting either difference in aetiology or in access to services. Other factors of relevance at the population level may be socio-economic status and ethnic group both to identify whether there are different sub populations for needs assessment, and access to services and to suggest possible factors in aetiology. There is an important distinction between the numbers in a population with a disease/ condition and those sub groups in a population who have the highest proportion of a disease/condition. The classic example is where the highest prevalence occurs in the older age groups but the actual numbers in the population with the condition may be mainly contributed from younger age groups with lower prevalence. This simply reflects the much lower proportions of the older age groups in the population. Where do people with the disease/condition live? Geographical information such as regional, urban/rural and, for some conditions, living circumstances (in the community or in communal establishments such as nursing and residential homes) may help to estimate requirements for local service provision and, in the case of living circumstances, where the main target population may be identified. As described above at an international level these data are useful for suggesting possible true differences between populations in the prevalence of risk factors When? Temporal data describe changes in the prevalence or incidence of a condition/disease usually over a fairly extended time period for chronic conditions. Temporal data may be provided from routinely collected national statistics (e.g. mortality, cancer incidence) or by comparing cross sectional information such as from surveys collected at different years. There are a number of methodological pitfalls in interpreting temporal data: definitions of disease/conditions may have changed, the reported number of cases may have apparently increased as a result of greater awareness or improved diagnostic procedures, better treatment may lead to reduced prevalence but not incidence. Temporal changes in numbers only and not in rates are especially misleading as there is no indication of the underlying population. Increases or decreases in numbers may simply reflect changes in the population structure. Interpretation of Blindness and Partial Sight registrations is such an example. Why? Understanding why some people in a population get a disease/condition compared to others who do not is the main area for epidemiological research and outside the prime focus of this report. What is the problem? A number of terms are used to describe visual problems and we will discuss these in greater detail. As an introduction to this area we note that the choice of terminology and of measurement instruments is influenced by the purpose for which the information is required. We need to distinguish between measures which relate to understanding of the underlying clinical condition/disease and those which describe the impact of the condition/disease on the person’s function and everyday life. The objective of clinical measures of vision is to describe the level of visual loss and the reasons for this. Since at the population level in the UK most vision problems 10 are due to refractive error, untreated cataracts, age-related macular degeneration, diabetic retinopathy and glaucoma, a service provider perspective would include the need for specific data that assists in planning for services and treatments that include: optometry, cataract surgery and other clinical treatments, low vision aids, and for some conditions, frequent hospital visits for monitoring. Most importantly, estimates of the prevalence of visual impairment in a population will vary over time and between populations according to the proportion of untreated but remediable vision problems. Thus, measures of vision loss alone are a first step to describing the population burden but are not informative unless we understand what the problem is due to. Although we would expect a high correlation between functional difficulties described by a person and a clinical measure, a person’s functional problems will be also influenced by a number of both personal and situational factors. Clinicians will also use patients’ perspectives as an adjunct to both understanding at an individual level of the impact of the problem on a person, and at a group level to evaluate the effectives of clinical treatments and services. Measurement of Vision and Visual Problems A recent report to the International Council of Ophthalmology [1] (www.icoph.org/pdf/visualstandards.pdf ) provides an excellent summary of different approaches to measure and categorise vision and vision problems. From the perspective of this report and the available literature we will concentrate on the following measures since they have been used the most frequently in UK based population studies. 1. Vision difficulties - based on self-report of difficulties with vision related functions ranging from single item questions to disability scales 2. Clinical measures, predominantly visual acuity. 3. Vision related “quality of life” describing the impact of vision problems on everyday functioning and well-being (few studies at present). 1. Vision difficulties 1.1 OPCS disability questions In most of the UK national surveys carried out by the government survey services (Office of National Statistics, previously Office of Population Census and Surveys OPCS) which are described in this report a number of questions related to difficulties with seeing were used (Table 1.1.). All the questions on “seeing” included the adjunct “wearing glasses or contact lenses “so that disability was based on usual vision with corrective aids (though not usually magnifying or other low vision aids). These questions on seeing were part of a set of scales from four linked surveys that were carried out to establish the prevalence and type of disability in the UK. The concept of disability was heavily influenced by the WHO classification of International Classification of Impairments, Disabilities and Handicaps (ICIDH) [2]which drew distinctions between impairments (“ loss or abnormality of psychological, physiological or anatomical structure or function”), disability (“ restriction or lack of ability (resulting from an impairment) to perform an activity in the manner or within the range considered normal for a human being”) and handicap (“ a disadvantage for a given individual, resulting from an impairment or disability that limits or prevents the fulfilment of a role depending on age, sex and social and cultural factors for that individual). The ICIDH classification of disability was adopted for the OPCS surveys; separate scales were developed for 10 disability areas (later expanded to 13 areas) including seeing. Within each of the areas of disability the severity of specific difficulties 11 was ranked on a 10 point scale using panels drawn from OPCS staff, professional experts in disability and disabled people and their carers. Further work involved the use of a common 15 point disability scale to which the individual disability specific items were mapped. Finally an overall disability score was produced based on the three highest severity scores from the separate areas. None of the disability scales underwent the process known as validation that would nowadays be expected as part of the process of development of questionnaires. In particular the sensitivity and specificity of the questions and overall seeing scale against other measures of visual problems (such as visual acuity) were not established. This was largely because the concept of disability was considered as independent of external “gold standards”. However a potential problem in the lack of validation could arise when some of the questions were used as a preliminary screen for people with disabilities, known as “the sift questionnaire”. In several of the OPCS studies a selfcompleted questionnaire was used as a quick and easy method of identifying people with disabilities for a further more detailed assessment (Table 1.1). Two specific vision questions from the full seeing scale were included in the sift questionnaire (S9: “difficulty reading ordinary newspaper print” and S10 “difficulty recognising a friend across the road”). However a decision was made that people who responded only to S10 and not to any other question were treated as the non-disabled. People answering positively only to S9 or worse were included. Since the prevalence estimates in some surveys are derived from people who have been “sifted in”, it is important that the sift questions have high sensitivity (i.e. people with vision problems are not missed). Specificity is also critical because estimates may be biased by false positives. Sift questions can also be used to measure prevalence based only on the two sift questions asked. Many of the estimates presented in the report are based on the combined prevalence of S9 and/or S8. In later surveys, different questions from the Seeing difficulty scale were used e.g. in the Health Survey for England [3, 4] prevalence was based on a positive answer to S8 “Cannot see well enough to recognise a friend across a road” with S4 “Cannot see well enough to recognise a friend who is an arms length away” being asked for a positive response to S8. 1.2 Other questions used in surveys. The English Longitudinal Study on Ageing (ELSA) [5] moves away from the “difficulty” or “cannot” style of questions in the OPCS surveys to asking people to rate their vision, overall and for two specific examples. Participants were asked to rate their eyesight, using glasses or corrective lenses, as excellent, very good, good, fair or poor. They were also asked to rate how good their eyesight was for seeing things at a distance and for seeing things close up. 2. Clinical measures A number of clinical measures exist of which the most commonly used and internationally accepted is visual acuity. Other clinical measures include visual fields, colour vision, contrast sensitivity, light/dark adaptation and motion perception. Visual acuity and, to a lesser extent, visual fields are measures that are practical to use in population based studies. Other clinical measures described above are used mainly in the clinical setting for diagnosis and for clinical research. The current consensus is that these other clinical measures are not yet suitable for use in the population[6]. Further work is required to refine the use of such measures and demonstrate their added value, over that of visual acuity, in characterisation of visual loss at the population level. Visual acuity 12 Visual acuity is the basis for categorising vision impairment in the WHO International Classification of Diseases (ICD10) [7] (Table 1.2) but the definitions used may not necessarily fit with the goals of a particular survey. Alternative definitions have been proposed by the International Council of Ophthalmology[1] which include minor categories of visual loss. Distance visual acuity is the most usual measurement but additionally some surveys have also included near acuity i.e. close up vision. Measurement of distance visual acuity. A detailed explanation of the letter charts and scoring methods used in population surveys is given in the report to the ICO [1]. The most commonly used measure has been the Snellen chart, preferably illuminated, tested at a distance of six metres. Most people will be familiar with this method of testing as it is routinely used in high street optometrists. The Snellen chart has been in use for over a hundred years [8]. Snellen designed a chart for screening and for use with refraction based on special characters called “optotypes”. He defined the reference standard as the ability to recognize letters that are 5 min of arc high. However the chart is not fine enough at lower levels of visual acuity and, for this reason, a chart with a logarithmic progression of letter sizes was first proposed by Bailey and Lovie [9]and adopted in the ETDRS[10] (Early Treatment Diabetic Retinopathy Study). The EDTRS chart and others similar [11] which provide equal steps at all levels have come to be preferred in clinical use and are also increasingly recommended as the preferred method in population surveys [1, 6]. These charts are commonly known as LogMAR (Log of the Minimum Angle of Resolution) charts. Near acuity is commonly measured by the distance at which newsprint can be read, usually 40 cm. Although some surveys use cards with text (to simulate news or book print) another method is to use LogMAR or Snellen cards. From the point of view of classification there are a number of important features related to the measurements of distance acuity. 1. Visual acuity can be measured either unaided or with glasses /contact lenses if worn. This latter measurement is usually described as “presenting “or “walk about” vision and is regarded as the measurement that best reflects the everyday vision of the person. 2. Vision can be measured in both eyes (separately) or together (binocular). Binocular vision is also regarded as better reflecting the everyday vision than the uniocular vision. For many definitions, including the WHO definitions and the legal requirements for registration, the vision in the better eye is the criterion by which the person’s visual acuity is categorized. 3. “Best” corrected visual acuity is the visual acuity after using the best available methods for correction for refractive error. In population surveys full refraction may not be available and a simple (though imperfect) method to try to correct for refractive error is to use a pinhole and remeasure visual acuity with the person looking through the pinhole. In the WHO categories the visual acuity definitions are based on best correction in the better eye (Table 1.2) Vision impairment is defined as a Snellen acuity <6/18 and blindness is defined as visual acuity <3/60. Visual acuity <6/12 is not used internationally to define impairment but is reported by some studies as it represents a reduction in visual acuity sufficient to affect lifestyle e.g. it corresponds to the requirements for sight for driving licence in the UK and in other countries. Obtaining high quality measurements of visual acuity in population based surveys requires a written protocol on how to administer the tests, attention to adequate lighting and necessary distances between the patient and the charts, standard instructions on amount of prompting and encouragement to be given to ensure that participants have the best chance to attempt the letters. 13 Training and quality control of fieldworkers in population based surveys is absolutely essential to ensure reliable results. Visual fields Visual field loss is more complex to characterise than visual acuity. However visual field loss can occur independently of visual acuity. A recent report on standards for characterization of vision less and visual functioning concluded that more work needed to be done to develop good methods for testing visual fields in population surveys[6]. Automated perimetery is the recommended method for field surveys but requires more expertise and care than measurement of visual acuity. The ICO report [1]notes that the most appropriate visual fields depends on the question: central fields are the most important for identification of the underlying cause of vision loss, such as glaucoma while peripheral fields are a more relevant measure of the consequences of the underlying condition. A Visual Field score has been developed which provides a single summary score based on assigning points for every point seen on a visual field grid. This score has been correlated with orientation and mobility performance scores. There are to date no data on the use of the Visual Field scores in the UK population. Such data that are available on visual fields are in the context of estimating the prevalence of glaucoma and include other criteria such as cup: disc ratio, and intra-ocular pressure. Blindness and partial Sight Registration in the UK The number of blind people in Britain has been recorded since 1851. Initially, this consisted of a declaration of blindness on Census returns. These were discontinued after 1911. In 1920, the Blind Persons Act created statutory benefits to the blind and its implementation led to a register of blind persons. Initially, all that was required for registration was a certificate from any medical practitioner that the patient was blind. From the mid-1930’s, certificates were only accepted on designated forms (BD8) signed by ophthalmologists. The National Assistance Act in 1948 set up the current system of registration, with local authorities required to establish registers of people with disabilities, including those blind or partially sighted, and to administer the statutory services to which the visually disabled are entitled. Any person seeking registration as blind or partially sighted is required to see an ophthalmologist who certifies that the person is eligible for registration. A person is certified as blind if they are “so blind that they cannot do any work for which eyesight is essential”. This is recommended to be a best binocular acuity of less than 3/60 Snellen, or a much contracted field of vision. A person can be certified as partially sighted if they are “substantially and permanently handicapped by defective vision cause or by congenital defect or illness or injury”. It is suggested that this corresponds to an acuity of 6/60 or less or gross field defects (or 6/24 or less in certain cases). Since November 2003, the system has changed in England only. This change was initiated by concerns, probably unfounded, that only a minority of people eligible for registration were taking up registration. The BD8 form has been superseded by a “certificate of vision impairment (CVI)”. There are now two categories of vision impairment: “sight impaired or partially sighted” and “severely sight impaired or blind”. Mechanisms have also been put into place to ensure that visually impaired people are referred promptly from the high street optician and hospital eye service for support. Data on number of people on the registers and new registrations These data are collected separately in England, Wales, Scotland and Northern Ireland. Local Authority Social Services departments complete forms SSDA 902 in England and Wales and 14 SWB in Scotland and return these to relevant government agencies (Department of Health, Scottish Executive and Welsh assembly) whose job it is to analyse and publish these data. Data from Scotland is most easily available being online and up to date (published to year end March 2003 (http://www.scotland.gov.uk, accessed September 14th 2004). Data for England are available from the Department of Health publications office [12]. Cause of visual loss Data on the cause of visual loss has been analysed periodically[13-16]. Since 1990, part 5 of the BD8 form has been sent to the Office of National Statistics (ONS) and coded according to ICD9. The last time period for which national data were analysed for England and Wales was 1990/91 [13]. At that time the main cause of blindness was “degeneration of the macula and posterior pole” (48.5%) followed by glaucoma (11.7%), diabetic retinopathy (3.4%), optic atrophy (3.4%), cataract (3.3%) and other conditions (20.0%). For partial sight the main causes of visual loss were similar. Some authors have reported cause of visual loss at local area level [17-19]. Current arrangements for the analysis of cause of visual loss at the national level have not been publicised. Strengths of the Registration System Data on number of people on the blind and partially sighted registers and number of new registrations is national, routinely collected data reflecting the prevalence and incidence of severe vision loss in the population. It is available over long periods of time and, in theory, could be used for monitoring temporal trends in causes of severe visual loss that are not amenable to treatment [20]. The registers potentially provide the opportunity for monitoring the incidence of important causes of preventable or “avoidable” visual loss, such as diabetic retinopathy[21] . However, that would depend on having regular analyses of data on cause of visual loss at the regional level. Weaknesses Registration is voluntary and the legal definitions are vague. This means that there is uncertainty as to the coverage of registration. One small study at the population level indicated that the blind register was probably fairly complete, the partial sight register less so [22]. Other studies at the hospital level have indicated that a proportion of visually impaired people attending the hospital eye service are not registered[23, 24]. There might also be considerable time delay between onset of severe vision loss and registration. Chapter Summary In this chapter we have reviewed the importance of obtaining information on the levels of visual problems in a population, different approaches to the methods of measuring visual problems including self reported, visual acuity measurements and blindness and partial sight registrations. In the following chapters we will review the available literature using different methods for categorising vision: Chapter 2: Vision difficulties in adults Chapter 3: Visual acuity estimates in adults Chapter 4: Causes of vision impairment in adults 15 Chapter 5: Vision impairment in children Chapter 6: Vision related quality of life Chapter 7: Conclusions and Recommendations The literature was ascertained (i) from a PubMed search using the key words ``prevalence" ``visual" and ``blindness" (ii) by asking the advisory group members for relevant publications and (iii) searching the bibliography of those most recently published. 16 Table 1.1 Seeing Severity Scales and categories as described in Martin et al 1988 [25] Scale Description Score S1 Cannot tell by the light where the windows are 12 S2 Cannot see the shapes of the furniture in the room 11 S3 Cannot see well enough to recognise a friend if close to his face 10 S4 Cannot see well enough to recognise a friend who is an arm’s length away 8 S5 Cannot see well enough to read a newspaper headline 5.5 S6 Cannot see well enough to read a large print book 5 S7 Cannot see well enough to recognise a friend across a room 4.5 S8 Cannot see well enough to recognise a friend across a road 1.5 S9 Has difficulty reading ordinary newspaper print 0.5 S10* Has difficulty recognising a friend across the road *Not included as a criteria for sift but in the original scale 17 Table 1.2 Visual acuity scoring systems, WHO ICD classifications of blindness and low vision (ICD10) [7]and ICO recommendations for categorisation of visual loss[1] WHO ICD 10 Based on VA in better eye after best correction for refractive error International Council of Ophthalmology Ranges of vision loss2 defined by decimal notation Normal vision >= 0.8 Not defined by WHO Mild vision loss < 0.8 and >= 0.3 2 Moderate vision Moderate vision loss < 0.3 and >= 0.125 Low vision impairment < 6/18 – 6/60 2 Severe vision loss < 0.125 and >= 0.05 Severe vision impairment <6-60Profound vision loss < 0.05 and >= 0.02 3/60 Blindness < 3/60 Near-total vision loss (near blindness) < 0.02 and >= NLP Total vision loss (total blindness NLP Decimal notation Snellen (UK notation) Snellen (USA notation) 1.0 0.8 0.5 0.32 0.25 0.16 6/6 6/7.5 6/121 6/18 6/24 6/36 20/20 20/25 20/40 20/63 20/80 20/125 LogMAR ETDRS or Bailey Lovie 0 0.1 0.3 0.5 0.6 0.8 0.125 6/48 20/160 0.9 0.1 6/60 20/200 1.0 3/60 20/400 1.3 <0.02 1/60 or less less 1.8-1.9 0.0 NLP3 NLP 2.0 0.05 1 <6/12 approximates to driving licence threshold 2 These definitions of have been proposed as alternatives to the terminology of Low Vision which may be confused with people eligible for Low Vision services 3 No Light Perception Chapter 2 Vision Difficulties in Adults Included in this section are all studies which have used self reported responses to questions on problems with vision related tasks (vision difficulties) or to self assessment of vision (as described in the previous chapter) (Table 2.1). Some reports use the term “visual disability” to describe the prevalence of “seeing difficulties”. The Prevalence of Disability among Adults (Martin et al.1988) [25] Summary The OPCS disability survey of adults in private household and communal establishments in Great Britain was carried out in 1985. Questionnaires were sent to 100,000 private households. 28,415 adults, aged 16 and over, were identified as disabled of whom 18,000 were selected for interview and 14,308 (79%) were interviewed. 3,775 people in communal establishments were interviewed, either personally or by proxy. The criteria for “visual disability” were “has difficulty reading ordinary newspaper print” and/or “cannot see well enough to recognise a friend across the road”. The prevalence of visual disability for adults aged 16 and over in private households was estimated to be 3.2% increasing to 3.8% when residents of communal establishments were included. Methods Private Households A screening (“sift”) questionnaire was sent out to a random sample of 100,000 households identified from the Postcode Address File (PAF). The PAF divides Great Britain into about 8,500 postal sections. The OPCS frame combined these into some 800 areas each containing a minimum of 500 addresses. The first stage was to sample 500 of these areas with probability proportional to size. The sectors were stratified by region, by a metropolitan/non metropolitan split and then systematically ordered by the proportion of people above retirement age. The second stage was to select 200 addresses from each of the selected areas producing a total of 100,000 addresses. In 400 of the areas (covering 80,000 addresses) the screening was carried out by post. In the remaining 100 (urban) areas (and also addresses that had been identified as having multiple households) interviewers delivered the screening questionnaire personally. The questionnaire contained detailed questions on health problems and disabilities. Those related to seeing were “difficulty recognising a friend across the road even if glasses or contact lenses are worn” and “difficulty reading ordinary newspaper print even if glasses or contact lenses are worn”. People with disabilities were then followed up and interviewed. The response rate to the screening questionnaire was 80%. There were 28,415 adults who answered “yes” to at least one question relating to long-term health problem or disability. 50% of those over 65 and all those aged under 65 were selected for interview (n = 18,000). Of these, 14,308 (79%) were interviewed. Of these 11,035 were identified as disabled from the interviews. 2534 of these were categorised as visually disabled because they answered ``yes" to the question “has difficulty reading ordinary newspaper print” or “cannot see well enough to recognise a friend across the road”. In the derivation of the estimates of the number of disabled adults in the total population the numbers are weighted to account for under-sampling of 60+ and also non-response. 2 Communal Establishments A list of institutions held by the Vital Statistics Branch of the Population Statistics division of the OPCS (approximately 20,000 entries) and an equivalent list from the General Registrar's Office for Scotland was used as the sampling frame. Hospitals, homes and hostels were included. Educational establishments, places of detention and military establishments were excluded. 1,408 institutions were contacted. 892 (63% of institutions) were found to be eligible, i.e. that they had four or more permanent residents and were willing to co-operate. One third of the 892 institutions were randomly rejected leaving a sample of 595 institutions. One in four residents were selected for interview in institutions where the number of permanent residents was 80 or less, and one in twelve where the number was 81 or more. Selection was made by the interviewer or institution administrator. Interviews were obtained from 3775 permanent residents from 595 institutions. In some cases interviews were split between a member of staff and the resident and in other cases the administrator was interviewed on behalf of all the subjects, even if they were competent to answer. It was assumed that all permanent residents in establishment had some degree of disability. Weights were used to produce national estimates, to allow for those who could not be interviewed, the institutions that did not reply, the sampling within the selected establishments and for sampling and non-response of establishments. Results Figures 2.1 and 2.2 show the stages in the sampling and selection process that led to the estimates for visually disabled adults in private households and communal establishments respectively. Table 2.2 shows the estimated prevalence rates for visually disabled adults aged 16 and over, by age and gender. Of the 10,561 interviewed, 2534 were classified as visually disabled. The overall prevalence rate of adults, aged 16+ in private households in GB with visual disabilities, was estimated to be 3.2% and the estimated number of visually disabled adults in private households in GB to be 1,384,000. Prevalence estimates for those in communal establishments were not reported, only those for the total population i.e. private plus communal. The estimates were based on the assumption that there are no disabled people in the excluded types of establishment. The prevalence rate when residential homes were included increased to 3.8%. The estimated percentage prevalence by age group for adults in all establishments was 0.8 for the 16-59 age group, 5.6 for 60-74 and 26.2 for those ages 75 and over. 3 Figure 2.1: Flow chart showing the numbers of participants at each stage of the OPCS 1985 survey of adults in private households 4 Figure 2.2: Flow chart showing the numbers of participants at each stage of the OPCS 1985 communal establishments’ survey . Comment The survey was a large random sample of the total population of Great Britain. A specially devised questionnaire to measure disability based on successive “sifting” was used which allowed in-depth interviews to be carried out on those screened into the survey as positives. This approach is cost effective because large numbers of people with no disability do not need to be interviewed in depth. The disability scales and sift questions are described in detail in the report. The selection process of the 1 in 4 or 1 in 12 residents in communal establishments was not random. Some residents were interviewed personally whereas in some homes the administrator provided all the answers, even if the residents were capable of answering. No figures were given for the number found to be disabled in communal establishments, and thus it was not possible to calculate the number of visually disabled in the sample. Although the estimates are based on large numbers, 95% confidence intervals were not provided. 5 Disability in Great Britain: Results From the Office for National Statistics (ONS) 1996/97 Disability Follow-Up to the Family Resources Survey (Grundy et al.1999)[26] Summary This report is based on interviews obtained from a subset of those interviewed in the 1996/7 Family Resources Survey. It provided estimates of adults (16+) with seeing disabilities in private homes. It used the same criteria for disability as in the 1985 survey, but the questions on the ``sift" questionnaire for overall disability were different and included questions on long standing illness or disability. Overall 23% of the 5589 disabled adults included in the survey were classified as having a “seeing” disability. The estimated weighted prevalence of visual disability in adults aged 16+ in private households in Great Britain was 4.5%. The total number of visually disabled adults in Great Britain was estimated to be 1,973,860. Methods The sample for this survey was a sub-sample of people interviewed for the Family Resources Survey (FRS) between July 1986 and March 1997. The FRS includes questions on limiting long standing illness, on health problems limiting ability to work and on benefit receipt. FRS is conducted on a continuous basis with some 25,000 households. 47,000 adults are interviewed each year using computer assisted personal interviews. Those included in the disability follow-up survey fulfilled at least one of the following criteria: 75 years of age or older long-standing illness or disability Restricted in type or amount of work receipt of War Disablement Pension, Disability Working Allowance, Severe Disablement Allowance, Attendance Allowance, Mobility or Care component of Disability Living Allowance, Incapacity Benefit or Industrial Injury Disablement Benefit Awaiting a claim for Disability Living Allowance, Incapacity Benefit or Industrial Injury Disablement Award Receiving certain types of pensions with increments. The criteria for being classified as visually disabled was the same as in the OPCS disability study described previously[25] i.e. at least S9 in Table 1.1. Base figures from the original FRS survey were used to produce the prevalence estimates. Figure 2.3 shows an outline of the sampling procedure. Weighting procedures were used to allow for the probability of being selected for the FRS, response to the FRS and response to the Disability survey among FRS respondents. It is not clear how, or if, weighting was carried out to allow for the over-sampling of people aged over 75. 6 Figure 2.3: Flow chart showing the sampling procedures and numbers included at each stage of the OPCS 1996/7 FRS follow-up private household survey Results The number of participants at each stage is shown in Figure 2.3. The response rate at the first stage was 80% and to the second stage was 85% giving an overall response rate of 68%. Prevalence estimates by age and sex are shown in Table 2.2. The total estimated number of disabled adults aged 16+ in GB was 8,582,000. Of these 1,973,860 were estimated to be visually disabled. The estimated prevalence of visual disability in adults 16+ in private households in GB was 4.5% and for age 75+ was 22.6%. Comment This was a large survey, for which the sample was drawn from the GB population. Because of the way in which the sample were selected ie as a sub-sample of those assessed as disabled (or aged 75+) it is not easy to find the exact numbers of people interviewed at each stage, as they appear to differ between tables and text. The report is somewhat opaque and base figures are not provided in the tables that give data on visual disability. 95% confidence intervals were not provided. The report is concerned with all types of disability and contains very little information about people with sight problems. 7 Health Survey for England. Disability among older people (DOH 2000 and 2001) [3, 4] Summary The 2000 report from the Health Survey for England focused on the health of older people aged 65+ and included a sample from care homes in the UK. The prevalence of S8 (cannot recognize a friend across the road) in 2,493 people in care homes (75% response) was 27%. Data on those in private households was combined with data from the 2001 survey of those aged 16 and over resulting in 1,677 adults aged 65 and over (response 75%) from the 2000 survey and 15,647 (67% response). The prevalence of S8 in the 16+ population was 2.6% and 9.8% in the over 75 population. Methods The Health Survey for England is a series of annual surveys about the health of people in England. The Health Survey was first proposed by the Department of Health in 1990 to improve information on morbidity in the population. The survey was carried out in 1991-1993 by the Office for Population Censuses and Surveys (OPCS), now the Office for National Statistics (ONS). From 1994 onwards the survey has been carried out by the Joint Survey Unit of the National Centre of Social Research and the Department of Epidemiology and Public Health at University College London. The main focus of the 2000 survey was on the health of older people aged 65 and over living in private households and care homes. The questions relating to sight disability were: “can you see well enough to recognise a friend at a distance of four metres (across the road)” (S8) and, “if no, can you see well enough to recognise a friend at a distance of one metre (at arms length)?” (S4) Care Homes In the 2000 survey a stratified random sample was selected from a large database of all care homes in the UK. In homes with six or fewer residents aged 65 and over all residents were interviewed. If there were seven or more such residents six were randomly selected for interview. Interviews were carried out with 2,493 residents comprising 75% of those selected in these homes. Of these 1,273 were carried out via proxy information. Private Households A stratified random sample was selected from the PAF. Interviews were obtained with 1,677 adults aged 65 and over. Interviews were carried out at 75% of the private households at the selected addresses and interviews were obtained with 95% of adults aged 65 and over living in these households. For the 2001 survey a stratified random sample was selected from the PAF, giving a total selected sample of 13,680 addresses aged 16 and over. Interviews were obtained with 15,647 adults aged 16 and over. The response rate to interview was 67% (71% among women and 63% among men). The 2001 sample was combined with the equivalent sample of the population resident in private households in Health Survey for England 2000 to improve the precision of estimates. The same questions were asked as in the 2000 survey. Results Care Homes The estimated prevalence of sight disability in care homes (as defined by answering a positive response to S8 by age and gender) is shown in Table 2.2. The prevalence rates were 20% for 8 males aged 65-79 and 27% for those over 80 and for females 17% for those aged 65-79 and 31% for those aged over 80. The report also showed the reported causes of disability but only a very small percentage ( 3%) of those visually impaired gave the cause. Results for private Households The estimated prevalence for all ages 16+ was 2.6%. The estimated prevalence by age and gender were males 16-64, 1.2%, 65-74, 3%, 75-84 6%, females 16-64, 1.6%, 65-74 5%, 75+ 11% with an estimated prevalence of 9.8% for both sexes age 75+. Comment The results were based on two large surveys of the population and a separate component for care homes. No 95% confidence intervals were provided. 1998/99 Survey of the Needs and Lifestyles of Visually Impaired Adults. (RNIB/ONS 2000)[27] Summary This survey was commissioned by RNIB to provide a picture of the needs and lifestyles of visually impaired people in Great Britain and Northern Ireland. The random component of the sample was obtained from the FRS/disability follow-up survey, three Omnibus surveys and several other smaller surveys. 1076 people aged 16 and over were interviewed (response less than 30%).The prevalence in those aged 16+ of at least S9 (difficulty reading ordinary newsprint) was 2.8% and 14.4% in those aged 75+. Methods The survey estimated prevalence based on (i) the sift questions (ii) results of sight tests. In this chapter we consider only the results for the sift questions and present the results for the sight tests in Chapter 3. The Great Britain sample of visually impaired adults was drawn from a number of sources: three surveys which included questions to identify respondents with sight problems: the Disability follow-up survey to the 1996 Family Resources Survey (FRS), the 1997-98 Labour Force Survey (LFS), and the ONS Omnibus surveys for April, June and July 1998. Local Authority registers of blind or partially sighted people and a “boost” of ethnic minority respondents from a focused enumeration within 50 districts found at the 1991 Census to contain an ethnic minority population density of 40 % or higher. Questions were added to the Omnibus to identify respondents with sight problems. Interviews were sought from people answering “yes” to S9 or worse in the FRS/disability follow-up survey (n=1166) and the OMNIBUS surveys of April June and July 1998 (n=817). The Omnibus surveys were used due to a low response and ineligibility rate for the FRS sample (see below). The interview covered a wide variety of topics including: causes of visual impairment; daily living skills; communication (use of Braille, tapes, computers); mobility; shopping; use and awareness of Social Services. Weighting procedures were used to allow for non-response and to adjust for the non-random sampling in the calculation of prevalence estimates. 9 Results Interviews were achieved with only 640 (32.3%) of the 1,983 subjects originally classified as visually impaired in the FRS/disability follow-up survey and the three omnibus surveys. Figure 2.5 shows a breakdown of the response rates at each stage for these two components of the sample. The main reason for low response was ineligibility of many participants who had originally been classified as visually disabled on first sift, but when the (same) questions were repeated for the RNIB, participants claimed they had never had a seeing problem or their sight had improved (see table 2.3). Approximately 30% from the FRS survey fell into this category and 55% of those from the OMNIBUS surveys. Of the 117 people from the FRS who said their sight had improved the main reasons were cataract removed (36%), new/better glasses (36%). 7.3% of those in the FRS study who said they had never had a problem who would have been classified as Blind (S1 to S5), and 47.9% as Partially Sighted (S6 to S8) based on their original responses. Similar information was not provided for the Omnibus Survey. The authors of the report were unable to establish the reason for the poor reliability of the vision questions and concluded that (i) the sift questions may be imprecise because they use the words “have difficulty” which is open to wide interpretation by respondents and (ii) the misreporting error seemed to have been greatest in the Omnibus survey when people were asked questions on vision and other disabilities as part of a general purpose questionnaire. Table 2.3 People at least S9 on previous FRS ONS survey Omnibus survey Both sources survey N=1166 N=926 N= 2092 Refusals/non contact 170 (14.6%) 112 (12.1%) 282 (13.5%) Sight improved 117* (10.0%) 23 (2.5%) 140 (6.7%) Never had a problem 234 ** (20.1%) 487 (52.6%) 721 (34.5%) Other 93 (8.0%) 7 (0.8%) 100 (4.8%) Prevalence rates by age group were estimated for the sift questions (Table 2.2). On the sift questions, people were categorised as partially sighted for S6-S8, Blind at least S1-S5, and PS+ (sight problem but better than partially sighted) for S10. The prevalence estimates included people who were sift positive at the re survey plus those whose sight problems had improved. Comment The poor response rate is a cause for concern. This was the first report to suggest poor reliability of the S9 question. 10 Figure 2.5: Flow chart showing the numbers of participants at each stage of the sampling of the random components of the RNIB 1998/99 survey of adults in private households 11 MRC Trial of Assessment and management of older people in the community (Smeeth et al 2002 and unpublished data provided by AF) [28] Methods The MRC Trial of the Assessment and Management of Older People in the Community is a cluster randomised trial comparing different methods of multidimensional screening in people aged 75 years and over [29]. One hundred and six general practices from the UK Medical Research Council General Practice Research Framework were recruited to the trial. The practices were recruited from England, Wales and Scotland and were stratified to provide a representative sample of the mortality experience (Standardised Mortality Ratio) and deprivation (Jarman Score) of general practices within Britain. In each practice all patients aged 75 years and over were invited to take part excluding those in long term care or with a terminal disease. The trial consisted of two arms. In the “universal” arm, all participants received a brief health questionnaire followed by a more detailed assessment by a practice nurse. In the “targeted” arm, all participants received a brief questionnaire but only those who “triggered” on predefined responses received a detailed assessment. Practices were also randomised to one of three methods of administering the brief questionnaire: postal, lay interviewer, practice nurse. The brief questionnaire included a single question on sight. : Do you have difficulty in seeing newsprint, even if you are wearing glasses? Participants were given a choice of three responses: No difficulty, A little difficulty and a lot of difficulty. The visual acuity tests in the detailed nurse assessment are described in Chapter 3. Results Of 42,278 eligible patients, 32,990 people responded to the brief questionnaire, an overall response rate of 78.0%. Men were more likely to respond than women (80.5% versus 76.7%, P<0.001) and the sex difference persisted after controlling for age. Responders were slightly younger than non-responders (median age of responders 80.3 years, non-responders 81.0 years, P<0.001). Response rates were slightly higher with the postal questionnaire (84%) compared to Lay (74%) or Nurse (76%). The proportions with missing responses to the vision question were very low: Postal (2%), Lay (0.7%), Nurse (0.9%) The percentages in each response category are shown according to the method of administration (Figure 2.6) with relatively small differences other than a slightly higher response for postal administration for “a lot of difficulty”. Overall 67.6% reported “no difficulty”, 22.8% reported “a little difficulty” and 9.6% reported “a lot of difficulty”. The proportions reporting a lot of difficulty were higher in women (11.2%) than in men (7.5%) and rose steeply with age 9.8% in those aged 75-84 compared with 19.5% in the over 85 age group (Table 2.2). For any difficulty (“a little” combined with “a lot” the proportions overall are 32% and again higher in women than in men and rising with age. 12 Comment The data provide good estimates of the prevalence of the response to S9 in the older population being derived from a large study with high response rates and drawn to be representative of patients in general practice in Britain. An advantage over other surveys which have used the S9 question was the use of a categorical rather than binary response scale to distinguish those with minor difficulties (“a little”) from those with major difficulties (“a lot”). 95% confidence intervals are provided. The limitations of the study are that it does not include people in nursing home care although people in residential or sheltered housing are included. Figure 2.6 100% 8 80% 24 10 11 19 24 60% 40% 68 71 65 A lot of difficulty A little difficulty No difficulty 20% 0% Nurse = 10,358 Lay = 9,757 Postal = 12,857 13 English Longitudinal Study of Ageing (ELSA) [5] The ELSA sample was drawn from households previously responding to the Health Survey for England (HSE) during 1998, 1999 and 2001. Individuals aged over 50 were eligible for interview. 12,000 people took part (response rate of 67%). The true response rate is lower than this (at around 45%) since the HSE response rates were about 70%. The topic areas covered by the ELSA questionnaire included: individual and household characteristics; physical, cognitive, mental and psychological health; social participation and social support; housing, work, pensions, income and assets; and expectations for the future. The vision questions used were “How good is your eyesight for seeing things at a distance, like recognising a friend across the street”; “How good is your eyesight for seeing things close up, like reading ordinary newspaper print”. The choice of response scales was: excellent, very good, good, fair or, poor. The questions included (using glasses or corrective lens as usual) The first results from the 2002 data collection were reported in December 2003. Results were provided only for the responses to “reporting fair or poor eyesight” (Table 2.2). The results show 16% of the over 50 age group reporting fair or poor eyesight with a steep increase with age. The proportions are higher in women than men across the age range. Comment ELSA is a nationally representative sample of people in private households with the opportunity to obtain longitudinal data. Overall response rates to successive sampling are less than 50%. It is difficult to understand what is being measured by the question on rating eye sight. Unlike the questions used in the other surveys, which are task oriented, the question is general and may be influenced by the person’s expectations of their eyesight and other personal characteristics. 14 Chapter summary The estimates of the prevalence of visual difficulties in the different studies are summarised in Tables 2.2 and 2.4. As S8“cannot recognise a friend across the road” is a worst severity than the question S9 “difficulty reading newspaper”, the estimates from the surveys that have used at least S9 are considered together. The figures show some consistency for the older age groups with most studies showing a prevalence in the over 75s of around 25% to 30% for reading difficulties or worse. The exception is the second RNIB/ONS 2000 survey which reports a lower prevalence for the over 75s age group. The overall prevalence in the adult population aged 16+ varies from 2.6 to 4.8%. For more serious difficulties (as in the MRC assessment trial or the Health Survey for England) the prevalence in the over 75s is around 10%. The difference between the first and second OPCS disability surveys (i.e. 1985, and 1996/7) are more difficult to explain. The second survey produced a much higher predicted number of people with overall disability in the community than the first one (5,600,000 vs. 8,582,200). The authors of the second study state that it is difficult to explain the apparent increase but suggest it is due to different sift criteria for overall disability. The prevalence of visual disability in the overall adult population (16+ age group) is also higher (3.2% vs. 4.5%). However, the differences are primarily in the younger age groups; the prevalence at ages 16-64 in males is 0.8% in the first survey and 2.2% in the second survey while for women at ages 16-59 the prevalences are 0.9% in the first survey and 2.0% in the second. In the oldest age groups the prevalences were 22.5 and 22.6 respectively in the two surveys. Another factor could be that the reliability of the responses in the second survey was poor. As described earlier in the chapter, information from the second RNIB survey showed that 30% of the original FRS/disability follow-up participants who had originally said that they had a seeing problem, subsequently stated that they had never had a problem, despite being asked the same questions on both occasions. No information is available on the reliability of the questions in the first ONS survey. Estimates of the proportion or numbers in the population with self reported visual difficulties are based on the criteria of difficulties reading newsprint or worse. They do not give information on the severity of the problem and use a criterion which includes minor visual problems. Only one study (the MRC trial of assessment in the elderly) used a categorical scale for severity of reading newsprint. 32% of the over 75s age group reported any problem with reading newsprint but only 9.8% reported a lot of difficulty. The large Health Survey for England used the question “could not recognise a friend at 40 metres” to categorise sight difficulties with 9.8% of the over 75s reporting positively to this question. Confidence in the results is further limited by the lack of detailed information on response rates especially in the government surveys. Response rates are difficult to estimate for many of the studies that have used different samples and successive sifting. For example the second RNIB/ONS 2000 Needs survey includes people from previous surveys (FRS and Omnibus) plus top up samples from a number of other sources including non random groups from local authority registers. The response rate from the FRS sample was 86% but the FRS sample itself had a response rate of 68% (cumulative response rate was less than 60%). Most studies have not provided the final response rates in the sample from whom the estimates are derived. 15 Table 2.1 Summary of studies considered in this Chapter Survey Age Number surveyed Response ONS Disability survey 1988 16+ 189,479 64% ONS/FRS Disability survey 1999 16+ 33,897 68% ONS /RNIB 2nd Needs Survey 2000 16+ 11,673 59% Health Survey for England 2001 16+ 17,324 67% MRC Assessment trial 2002 75+ 33,326 77% English Longitudinal Study of Ageing 2003 50+ 11,384 50% 16 Table 2.2: Prevalence of reported visual difficulties among adults in Great Britain. Survey Population OPCS 1985 Disability Survey (Martin et al.1988) [25] Private Household Original Sample Size 185,688 Criteria for prevalence estimates Difficulty reading newsprint and/or cannot recognise friend across road Sex Age Prevalence % M1 16-64 65-74 75+ 16-59 60-74 75+ 16+ 16-59 60-74 75+ 16-59 60-74 75+ 16+ 16-64 65-74 75+ All 16+ 16-59 60-74 75+ All 16+ 16+ 75+ 16-59 0.8 5.7 19.4 0.9 5.2 25.4 3.2 0.8 5.2 22.5 0.9 5.6 26.2 3.8 2.2 6.4 17 3.5 60-74 4.00 75+ 16+ 14.4 2.82 65-79 80+ 65-79 80+ 65+ 16-64 65-74 75+ 16-64 65-74 75+ 16+ 75+ 20 27 17 31 27 1.2 3 8 1.6 5 11 2.6 9.8 75-84 85+ 5.8 (5.1, 6.6) 15.4 (13.7, 17.2) F All All 1996/7 Disability Survey: FRS follow-up (Grundy 1999) [26] Private households and communal establishments Private households 189,479 Difficulty reading newsprint and/or cannot recognise friend across road 33,897 All M Difficulty reading newsprint and/or cannot recognise friend across road F All RNIB/ONS 2000 [27] DOH Health Survey for England 2000 [3] Private households and communal establishments Care Homes All 11,673 2,493 17,324 DOH Health Survey for England 2000/ & 2001 [3, 4] At least S9 on sift questions on re-survey Cannot recognise friend at 4 metres (across the road) Cannot recognise friend at 4 metres (across the road) M F All M F All MRC trial of assessment of older 1 106 general practices 33,000 people Reporting “ a lot of M Figures for men and women for the 1985 OPCS survey are obtained from [Grundy et al.1999] 17 2.0 6.7 26.3 5.3 4.5 22.6 1.14 people [28] (additional results provided by AF) representative of mortality and deprivation in the UK aged 75+ excluding those in nursing homes difficulty” in reading newsprint F All Reporting “any difficulty in reading newsprint” M F All English Longitudinal Study of Ageing [5] Random sample from 3 separate years of HSE 11,384 aged 50+ Reporting fair or poor eyesight in response to question How good is your eyesight? M F All Table 2.4 Prevalence of self reported visual difficulties in different studies 16+ Difficulty reading newsprint OPCS 1985 Disability Survey[25] FRS follow-up survey 1999[26] RNIB/ONS 2000 [27] MRC assessment trial [28] Any difficulty A lot of difficulty Cannot recognise friend across road DOH HSE 200 and 2001 [3, 4] 75+ 3.2 4.5 2.8 22.5 22.6 14.4 32.4 9.6 2.6 Fair /Poor eyesight ELSA 2003 [5] 9.8 27.9 18 75-84 85+ 75-84 85+ 75+ 75-84 85+ 75-84 85+ 75-84 85+ 75+ 50-64 65-74 75+ 50-64 65-74 75+ 50-64 65-74 75+ 8.0 (7.2, 8.7) 21.2 (19.3, 23.0) 7.1 (6.5, 7.8) 19.5 (17.9, 21.0) 9.8 (9.0, 10.6) 23.4 (21.5, 25.3) 43.2 (40.5, 45.9) 29.9 (28.1. 31.7) 50.9 (48.5, 53.3) 27.4 (25.6, 29.2) 48.6 (46.5, 50.7) 32.0 (30.2, 33.7 ) 11.2 13.2 24.0 12.6 16.4 30.3 11.9 14.7 27.9 Chapter 3 Population-based surveys using visual acuity measurements 19 The methods employed for each survey are shown in Table 3.1 and the key results are presented in Table 3.2. Since most of the relevant material is presented in these tables, only a short summary of each survey is provided in the following text. The exception to this is the 1991 report by Bruce et al which is a sub-survey of the OPCS 1988 disability survey ([25]). A full description of the study methods and results is presented in the text. Vision and visual-acuity in an elderly population (Lavery et al.1988) [30] Summary Visual acuity data were obtained from 529 people (response rate 78%) from a large general practice in Melton Mowbray. 18% of men and 30.2 % of women aged 76 and over were found to have a best corrected visual acuity in the better eye of 6/18 or worse. Methods The data were obtained from an earlier eye disease study carried out in 1982 [31]. All those registered in a general practice in Melton Mowbray (the only general practice in the town) who were 75 and over on December 31 1980 and alive on April 1st 1982 were included in the sample. 529 (out of the 677 eligible) subjects were examined (78.1%), 55 at home or in hospital, the rest were examined in a hospital outpatients department. Acuity was measured using a standard 6 metre illuminated Snellen chart, both with and without spectacles with full refraction by an optometrist. The prevalence estimates given are for best corrected acuity in the better eye. Results 2.6% of the men and 4.4% of the women were found to have visual acuity (best corrected) of less than 6/36 (3.8% both sexes). 15.4% of the men and 25.8% of the women had visual acuity between 6/18 and 6/36 (22.4%, both). 18% of men and 30.2 % of women aged 76 and over were found to have a best corrected visual acuity in the better eye of 6/18 or worse. 88.9% of males and 88.6% of females had near vision of N8 of better and 94.9% males and 94.0% females had N10 or better. Comment The measures of visual acuity were carried out by an optometrist and likely therefore to be accurate. Near acuity was measured. The response rate was high. The main limitations are: the results are based on a small sample size; 95% CIs were not provided; the population surveyed was from a small market town and it is difficult to extrapolate to other urban or rural areas. Visual problems in the elderly population and implications for services (Wormald et al.1992) [32] Summary 207 subjects aged 65+ (response 72%) from an inner London general practice were examined. The prevalence of blindness was found to be 1% by WHO criteria (VA <3/60) and 3.9% by the US criteria (VA < 6/60). The prevalence of vision impairment (VA <6/18) was 7.7%. 75% of visual impairment was due to cataract. 20 Methods The study was a random sample from an inner London general practice. 207 subjects aged 65+ (response rate of 72%) were examined in a day centre for the elderly. Subjects underwent a full eye exam by an ophthalmologist. Binocular distance visual acuity was measured using Snellen charts and best monocular 3 m Sonksen Silver acuity in each eye, with spectacles if normally worn. Near vision was recorded as being able to able to read N6 with normal reading correction. Confidence intervals were calculated by exact methods for small proportions and normal approximation to binomial distribution for larger ones. Results The prevalence of blindness was 1% by WHO criteria (<3/60 in better eye) and 3.9% by US criteria (better eye < 6/60). The prevalence of low vision by WHO criteria (best acuity <6/18) was 7.7%. The tests for binocular near vision showed that that 88.9% of males and 88.6% of females had near vision of N8 or better and 94.9 males and 94.0 females had near vision of N10 or better. The proportion of acuity problems due to eye diseases was recorded (see Chapter 4). Comment The measures of visual acuity were carried out by an ophthalmologist. Near acuity was measured. The response rate was reasonable. The main limitations are: small sample size and hence lack of precision; the participants were from a single inner city general practice. Prevalence of serious eye disease and visual impairment in a north London population: population based, cross sectional study (Reidy et al.1998) [33] Summary 1547 participants (84% response) were recruited from 17 randomly sampled general practices from north west London. 30% had presenting visual acuity of <6/12 in both eyes and a further 23.6% in one eye only. Methods Cross sectional survey using two stage cluster random sampling. The sample frame was 17 GP practices (1840 people) in 6 electoral wards in north west London. The wards were chosen after consultation with district and regional health authorities. 1,547 people, (response 84%) aged 65 and over, were examined and visual acuity measured using a LogMAR chart. Glasses were used if worn. Each eye was tested with and without a pinhole. Full refraction was also carried out. . Visual impairment was defined as a visual acuity of less than 6/12. Calculation of the population prevalence estimates and their 95% confidence intervals took into account the two stage cluster random sampling design. Results 30.2 % (448) of the sample aged 65 or older were found to be visually impaired (<6/12) in both eyes. Of these, the visual acuity in the worst affected eye was <6/12 to 6/18 in 19%, <6/18 to 6/60 in 61%, and <6/60 in the remaining 21%. 21 Comment The study had high response rates and a moderate sample size. Confidence intervals were presented. The eye examination was conducted by ophthalmologists. The report was mainly concerned with the prevalence of eye conditions and there is very little information by levels of visual acuity or by age and gender specific rates. No data are presented on visual acuity levels in the better eye for comparative purposes with other data. Visual acuity measurements in a national sample of British elderly people (van der Pols et al.2000) [34] Summary 1,362 people aged 65 and older from private homes and nursing homes (response rate 75% in the private homes and 94% in nursing homes) participating in the National Diet and Nutrition Survey (NDNS) were measured by a nurse for visual acuity. 14.3% (9.3% from private homes and 35.6% in nursing homes) had pinhole corrected visual acuity <6/18. Methods A random cross-sectional survey of people aged 65+ was carried out for the National Diet and Nutrition Survey. Participants were given eye tests using Glasgow Acuity Cards (LogMAR) at 3 metres at their place of residence by a nurse who had been trained in this method. The tests were carried out (i) without spectacles (ii) with spectacles and (iii) spectacles and pinhole occluder. Prevalence rates are based on pinhole corrected visual acuity in the better eye. Results 14.4% of those interviewed had visual impairment (pinhole corrected<6/18). The prevalence of visual impairment increased significantly with age (65-74 years 3.1%; 75-84 years 11.6%; 85+ years 35.5%. Impaired vision was more common in subjects living in a nursing home, odds ratio adjusted for age 2.59 (95% CI 2.23 to 2.96) and in women, odds ratio adjusted for age 1.55 (95% CI 1.21 to 1.89). 132 (9.7%) subjects had previously undergone cataract surgery and another 157 (11.5%) had been told that they currently had cataract. Comment The study population was a representative sample covering the whole population of Great Britain and of a moderate sample size. This is the only survey to give figures for those in residential/nursing homes. The measurements were done by a nurse in the participant’s home and the conditions under which the test were done (e.g. poor lighting, inadequate distance) may have affected the results. The accuracy of nurses to carry out the measurements, compared to eye specialists (optometrists or ophthalmologists), is not known. 22 Prevalence of visual impairment in people aged 75 years and older in Britain: results from the MRC trial of assessment and management of older people in the community (Evans et al.2002) [35] Summary 14,600 subjects aged 75 and over (response 71%) from 53 general practices across Britain were examined for visual acuity. 12.4% overall (95% CI 10.8 to 13.9) were visually impaired (binocular VA < 6/18); 10.3% (95% CI 8.7 to 11.8) were categorised as having low vision (binocular acuity <6/18 to 3/60) and 2.1% (95% CI 1.8 to 2.4) were blind (binocular acuity <3/60). Methods The design of the MRC Trial was described in Chapter 2. The data used in this Chapter relate to the results of the visual acuity testing reported for the universal assessment arm of the trial which took place in 53 practices. Visual acuity was measured at 3 metres with a Glasgow Acuity Chart. Binocular vision was measured first, followed by vision in the right and left eyes. All vision measurements were conducted with usual spectacle correction. People with visual acuity of 0.5 or more in either eye (equivalent to less than 6/18 Snellen acuity) were retested with a pinhole occluder. Prevalence rates are presented for four levels of visual acuity also visual acuity of less than 6/12 and less than 6/18, along with 95% confidence intervals adjusted for cluster design. Results Out of 21,241 eligible people, 15,126 (71%) had a detailed assessment. Of these 699 did not have a vision test: 173 were registered blind/partially sighted and in 526 (3.5%) there was no information on vision (these people were older, more likely to be women and more likely to require a proxy for the interview). People who were registered blind or partially sighted and who did not have a visual acuity test were included in the estimates for visual impairment. Using the criterion of binocular presenting vision, 12.4% overall (1803) were visually impaired: 1501 (10.3%) were categorised as having low vision (<6/18- 3/60) and 302 (2.1%) were blind (<3/60). The prevalence was higher in women than men and rose steeply with age. At ages 7579, 6.2% of the cohort was visually impaired with 36.9% at age 90+. At ages 75-79, 0.6% of the study population were blind, with 6.9% at age 90+. After pinhole correction, the prevalence of VA < 6/18 in the better eye was 10.3%. However there were problems with the use of the pinhole in the study: only 62% of those with VA 6/18 in either eye completed the pinhole test satisfactorily and therefore the pinhole corrected estimates are likely to be an overestimate since some correctable refractive error was not removed. If visual impairment had been defined as visual acuity of less than 6/12 the age-specific prevalence estimates would have increased by 60% with 19.9% of study participants with a binocular acuity of less than 6/12. Comment Results are based on a large sample size covering many areas of Britain and the participants are from general practices which were recruited to be representative of the mortality and deprivation of the UK. The response rate is moderately high. The large sample size allowed for presentation of data in the oldest age groups i.e. 80-84, 85-89 and 90+. Measurements were carried out by nurses and the reliability of nurses compared to eye specialists (optometrists or ophthalmologists) is not known. Full refraction was not possible and difficulty with the pinhole 23 means that a proportion of people with refractive errors may have been underestimated. The study sample excluded those in long stay hospital or nursing homes. What is the prevalence of visual impairment in the general and diabetic populations: are there ethnic and gender differences? (Hayward et al.2002) [36] Summary This was a population-based cross-sectional observational study investigating the prevalence of visual impairment and ethnic and gender differences in the general and diabetic population in Leicestershire of all ages (0+). Using capture mark recapture methods, the prevalence of blindness and partial sight in the general and diabetic populations was estimated to be 0.52% and 1.49% respectively. Methods Subjects were classified as blind or partially sighted if (i) already registered (ii) visual acuity in appropriate criteria and/or registration was reported by hospital staff (iii) participants were unregistered but answered “yes” to questions S9 or S8 (as described in table 1.3). Visual acuity tests for category (iii) are mentioned, but not described. Capture Mark recapture (CMR) methods were used to estimate prevalence. Data on visual impairment in the population to be studied was obtained from the Royal Leicestershire Rutland and Wycliffe Society for the Blind (RLRWSB). Secondary recapture, used to correct for under-ascertainment of those eligible for registrations, was from four sources: (i) Mass media inviting people who had, or knew others, with poor vision to volunteer information (ii) information on patients known to be blind or partially sighted provided by consultants and nurses on hospital wards (iii) hospital admissions data on anyone with ICD10 code for blindness or low vision and (iv) information from general practitioners. A census day was set (November 5th 1997) with computer cross-linkage to Leicestershire Health authority data ensured patients were alive and resident in Leicestershire at that date. Estimates of diabetes, ethnicity and gender prevalence were calculated using the 1991 census. Results According to the register and 1990 census figures, 0.52% (4,477) of the population of Leicestershire was registered as blind or partially sighted (all ages). The prevalence of blindness and partial sight in the diabetic population was 1.49% .Data was also presented for Asians compared to Whites. In the white population there were significantly more females with visual loss than males, but the reverse was true in the Indo-Asian population. The estimated prevalence for Asian males was more than double that for Asian women. Approximately 30% of those eligible for registration were not registered as blind or partially sighted (based on sift criteria). Comment This was the only survey to use CMR and registration figures. The method for classifying unregistered subjects as blind or partially sighted for mass media recapture group was unclear. There are very few (41) Asians included in the study and the prevalence estimates for Asians will therefore be unreliable. No age-related estimates of blindness and partial sight were provided. Using the sift questions as an estimate of registerable blindness and partial sight is inappropriate as the estimates may include those with treatable conditions. 24 Blind and partially sighted adults in Britain: The RNIB survey (Bruce et al 1991) [37] Summary This report was an investigation of blind and partially sighted people and their needs by the RNIB. The survey was based on interviews with 595 people, two thirds of whom were respondents to the 1985 OPCS survey[25] and one third whose names were obtained from the local authority partial or blind sight registers. Prevalence estimates were calculated based on 338 people aged 25 + with sight tests and who were interviewed. These results were applied to the adult population 16+ and expressed as those eligible to be registered as blind or partially sighted. These figures were 0.03% aged 16-59, 2.3% aged 60 to 74, 15% aged 75 and over. Overall response rates were probably lower than 50% as people were lost at successive stages. Methods The sampling procedure used to select the interviewees is depicted in Figure 3.1 along with the response rates (where given). The initial sample was 2,359 respondents aged 16+ from the 1985 OPCS disability survey that had responded positively to the questions “has difficulty to read ordinary newspaper print” and/or “cannot see well enough to recognise a friend across the road” Of these, all aged under 60 and 50% of those aged over 60 were offered a home sight test . The response rates to the sight test were not given. The sight test was measured using a standard Snellen chart (scaled down for use at 10 feet). Spectacles, if worn, were used. For near vision the test type used was the standard ‘N’ form. The criterion for inclusion in the RNIB survey was visual acuity no better than 6/24 or no better than N14 for near vision in the better eye. People aged 16-24 were not eligible for the sight test as this age group was being used by OPCS for another study. 1,248 people aged 25 + fulfilled these criteria. Further selection of the sample took place to identify for invitation (i) all those who said that they were registered, (ii) all those reporting they were not registered but with “lower residual vision levels “(not defined but assumed to be <6/36) (iii) all aged under 60 and half of those aged 60 and over who had visual acuity equal or better than 6/36. OPCS initially approached those selected for an “in principle” agreement to take part (the numbers refused are not given but there is a statement that “a handful refused). 524 people were invited for the needs survey of whom 338 took part (response rate of 65%). Because of concern over low numbers, especially in the under 60s age group, a “top up sample” was recruited. 67 people from the OPCS group “at registerable vision levels” were included; 69% of these participated. In addition nine local authorities were approached and asked to provide names of people on their registers. No information provided on how this was done and whether the numbers represented 100% of those on the registers or whether this was a selected sample. 312 “agreed to be interviewed” of whom 211 participated (68% response rate) This mixed sample i.e. 384 from the OPCS survey plus 211 from the local authority registers formed the 595 people. Estimating prevalence and numbers The population prevalence for private households by age groups were calculated by using, as the denominator, the actual numbers in these age groups in the full OPCS sample applying the relevant weighting to the >60 group who were successively under sampled. The numerator was the 384 people (described above) above who had a sight test in the OPCS sample and who 25 fulfilled the visual acuity distance or near vision criterion described above. These people were distributed by age group: 25-59 (133); 60-74 (84); 75+ (167). These prevalence estimates were then applied to the population of Great Britain to provide estimated numbers of people in private households with registerable visual impairment. Since the age group 16-25 were not given sight tests and hence not in the needs survey, the estimated prevalence rates for the age group 16-59 were based on the assumption that people aged 16-25 have the same prevalence of visual impairment as those 25-59. The estimated number of those in residential institutions was calculated by analysing the responses to the OPCS questionnaires by residence in communal establishments and assuming that all those in severity stage 3-10 for seeing difficulties were visually disabled, i.e. S6 and worse which is those that cannot read large print and/or cannot see well enough to recognise a friend across a room. It was unclear as to why people in the communal sample of the OPCS survey were not offered sight tests. Results The report estimated there were 757,000 visually “impaired” adults in private households aged 16+ in Great Britain eligible for registration. The estimate for all adults 16+ (including those in residential institutions) was 959,000. The age-related prevalence estimates, for people in private households classified as eligible for registration as blind or partially sighted, were: 0.3% for ages 16-59, 2.3% for ages 60-64 and 15.2% for 75+. These estimates are based on those who have a binocular visual acuity of no better than 6/24 and/or near vision of no better than N14. Gender related figures are not provided in this report. The estimates for those aged 16-59 are based on the sample of those aged 25-59, based on the assumption that the prevalence for 16-25 is the same as that of 25-59. They also found that the responses to the sift questions were related to the Snellen scores but that there was considerable deviation to a one-to-one relationship. Another interesting finding was that not all of those reporting that they were registered blind had acuity levels of 3/60. Some had acuity measurements of better than 6/60. Conversely, some of those reporting that they were registered as partially sighted had acuity of 3/60 or worse. At interview additional information was collected on a number of aspects of services, mobility, activities of daily living leisure and employment and self report of cause of sight problem. The main cause of sight problems reported by a third of respondents was cataract (15% ages 25-59, 35% 60-74, and 35% aged 75+); 8% overall (30% of 25-59, 12% aged 60-74 and 3% of 75+) reported vision problem from birth while the respective figures for accident were 8%, 7% and 3%. 26 Figure 3.1 Sampling procedures 100,000 households selected Response rate 81% 185,688 on sift forms 28,415 aged 16+ with disability 18,000 selected for interview Response rate 79% 14,308 interviewed 2,534 with seeing difficulties All < 60 + 50% 60+ Invited for home sight test of near and distance vision 1,248 aged 25+ with VA <=6/24 or <=N14 Response rate ? Not given Selected 1. All who reported they were registered 2. All reported they were unregistered with VA <6/36 3. 50% of those aged 60+ with VA >= 6/36 Numbers not given OPCS wrote to those selected asking if they would agree to be approached for re-interview Response rate ? Not given “handful refused” 524 people invited; 338 interviewed Ages 25-59 110 60-74 75 75+ 153 TOP UP SAMPLE 67 aged 25+ from OPCS sample with “registerable” vision levels (all ages) of whom 46 interviewed plus Non random selection of nine local authorities (LAs) LAs wrote to people registered as blind or partially sighted (number not given) aged 16+ 312 agreed to be interviewed Response rate 65% Ages 25-59 69% 60-74 66% 75+ 61% Response rate 69% of original OPCS sample plus 68% of LA sample 211 actually interviewed Combined number in OPCS and LA sample interviewed = 595 27 Comment The RNIB OPCS sample was derived from sight test results of people who were a sample of those who reported a seeing disability. As Figure 2.3 shows the identification of these people assumes that the sift process and seeing disability questions have high sensitivity so that people with visual impairment were not missed at the successive stages. Additionally, one third of the interviews were obtained from a non-randomly sampled population and since these people were aggregated with the OPCS sample for almost all analyses, it is not possible to examine the results separately for the national sample. However the estimates of prevalence and numbers were carried out separately. Although at each stage of sample selection the response rates are reasonable (varying from 65% for the needs survey to 81% for the first step in the OPCS disability study), the cumulative response rate is much lower (at least less than 41.5%). It is likely to be lower than this since, at various stages, response rates are not provided e.g. the proportions that refused a sight test. There is little information on the results of the sight tests in the full sample that underwent these. 1998/99 Survey of the Needs and Lifestyles of Visually Impaired Adults. (RNIB/ONS 2000) [27] The methods for this survey were described in detail in the previous chapter. Interviewers also administered a sight test (using a Snellen light box scaled down for use at 10 feet) in their homes. For near vision the standard ‘N’ form was used. Glasses, if used, were worn. The report does not present details of the results of the sight test. A variable was derived which defined visual impairment according to the following: registered as blind or partially sighted, or not registered but with vision < 6/24, or with VA in the range 6/24 – 6/12, or better than 6/12 with field loss or failed reading test. The reading test was defined as failed if one word or more was wrong on the smallest (6pt) line of the grey card. In the calculations of prevalence we excluded those with vision better than 6/12 but with field loss as it was not clear how this information on field loss was obtained. The results show lower prevalences than obtained on other studies. 28 Chapter summary This chapter includes data from six studies and two OPCS/RNIB reports. Only two studies (the MRC Assessment trial [35]and the NDNS study [34]) and the two OPCS/RNIB reports [27, 37] were based on samples covering the whole of Britain. The others are from selected regions, two in London [32, 33]and two in Leicestershire[30, 36] . The MRC Assessment Trial is much the largest with 14,600 people aged 75 and over examined. The North London Study [33]and the NDNS [34] examined 1547 and 1362 people respectively (aged 65+). Lavery et al [30] examined 529 people (aged 75+), and Wormald et al [32]examined 207 (aged 75+). The number included in the secondary recapture in the survey by Hayward et al [36]was 499 although it appears that only 26 of these were given visual acuity measurements. The survey by Hayward was the only survey to include people of all ages, and the only one to include people aged under 65. Unfortunately they do not give a breakdown of the estimates by age or sex. In order to compare the rates in the different studies, a summary of the age-specific prevalence rates for each survey is shown in Table 3.3 together with the 95% confidence intervals. If confidence intervals were not provided, these were calculated using the binomial method with no adjustment for clustering (since the clustering information was not available). For the two RNIB surveys it was not possible to calculate confidence intervals since the base population was not given. Caution must be used in comparing results from different studies as it is not possible to age standardise across the studies and the relative proportions of the very elderly (with the highest levels of impairment) may be very different across the studies. Carrying out a formal pooling of the studies in the UK was attempted but was not possible because the age specific data (numbers examined and numbers with different acuity levels) could only be provided by two studies. Table 3.3 shows that there appears to be reasonable agreement for the over 75 age group between three of the studies that presented estimates for <6/18, i.e. NDNS (15.2%), MRC Assessment Trial (12.4%) and Wormald et al (14.2%) but that of Lavery et al is much higher at 26.2%. However the measurements are all of different parameters: NDNS reported pinhole corrected, the MRC Assessment Trial binocular presenting and Wormald et al and Lavery et al are best corrected. The MRC Trial estimate is lower than in the other studies and even lower when pinhole corrected acuity is considered. On the other hand, the 95% confidence interval shows that the estimates from the trial are the most precise and the upper bound of 13.9 excludes the point estimates of both Wormald et al and for the NDNS. The confidence interval for the Wormald et al study is very wide. The Lavery et al estimate may reflect a genuine difference due to the population in Melton Mowbray or it may reflect a higher level of vision impairment in an elderly population measured nearly 20 years before the more recent surveys, for example if there were more untreated cataracts 20 years ago the prevalence of vision impairment would be higher. Age differences will also play a part. For example, of those aged 75+, proportionately more were aged over 85 years in the NDNS study (34%) compared to the MRC Trial (21%) and Lavery et al (21%). The age specific rates for 75-84 and aged 85+ which we have calculated from Table 3.2 are very similar for the MRC Trial (8.6 %) and the NDNS (7.7%) (pinhole corrected) and 26.5 and 29.7 respectively in the 85+ group. 29 The North London Study estimates are also very high which again may again be peculiar to the North London population. The prevalence estimates for the two ONS/RNIB studies are very similar for the age groups 16-59 (0.3 vs. 0.31) and 60-74 (2.3 vs. 2.05) but are completely different for those aged over 75 (15.2 vs. 5.4). As discussed above, the lower prevalence in the 2000 RNIB survey may reflect the exclusion of those identified on the sift questions whose sight problems had been resolved (mainly cataract and new glasses). It is therefore (as we will discuss in the next chapter) closer to the criterion for registerable impairment. If the 1990 ONS/RNIB estimates are taken as binocular presenting vision (without any criteria for registration) they are close to the estimates for the over 75s age group reported by the MRC Trial and NDNS. 30 Table 3.1 Population based surveys using visual acuity measurements - methods Name North London Study Locatio n and date of survey North London 1995-6 Reidy et al. 1998 [33] NDNS Van Der Pols et al. 2000 [34] Great Britain 1994 1995 Aims Inclusion /Exclusion Criteria Design and methods Visual measurement Sample size Response rates Number examined Demographi c To estimate prevalence of main serious eye disorders Age 65+ Cross sectional survey using two stage cluster random sampling. Sample frame 17 GP practices in 6 electoral wards. Wards chosen after consultation with district and regional health authorities. Accounted for clustering effect in estimation of standard errors. Cross-sectional survey. 80 postcode sectors selected with probability according to size. Individuals randomly selected with probabilities required to produce suitable numbers for statistical comparisons in each sex and age group. LogMAR at 6 metres by ophthalmic nurse. Glasses if worn were not removed. 1,840 from 7 GP practices 84% 1547 from 7 GP practices Age and sex distribution similar to that of sample population. 94.3% white 2,060 75% of those in private household s and 94% in nursing homes 1362 Mean Age 78.2 (sd 8.0) To measure visual acuity in elderly Registered at GP practices Age 65+ Private households and nursing homes (no geriatric hospitals) Not mentally impaired One person per household 3 per nursing home Pinhole test Glasgow acuity Cards (LogMAR) at 3 metres at their home by a nurse who had been trained in this method. 1.without spectacles. 2. with spectacles 3. spectacles and pinhole occluder Prevalence figures are based on best visual acuity score from 1,2, or 3 22.6% of those measured live in institutions 99.2% white 49.2 female MRC Assessment Trial Evans et al. 2002 [35] Great Britain 1994 1999 To estimate Prevalence of visual impairment Age 75+ . Not in long stay hospitals or nursing homes or terminally ill Cluster randomised cross sectional survey (using data from MRC cluster randomised trial). Sample frame 106 GP practices stratified by SMR and Jarman score. Glasgow acuity Cards (logMAR) at 3 metres by trained practice nurse. Glasses if worn were not removed. 21,241 from 53 GP practices 71% 4477 on blind and PS registers. 499 of the 720 from secondary sources deemed eligible (of whom 340 were already registered) 14,600 from 53 GP practices 75+. Median age 80.3 Pinhole test. Accounted for clustering effect in estimation of standard errors. Hayward et al. 2002 Leicest ershire 1997 [36] Wormald et al. 1992 [32] Inner London (date not To estimate prevalence of visual impairment in general and diabetic population. Investigatio n of ethnic and gender differences To estimate prevalence of visual disability All ages (including children) Included if 1.already registered or certified as B or Ps. 2. visual status and registration reported by hospital staff 3. unregistered but answered “yes” to RNIB questions. Age 65+ Population-based crosssectional observational study. Population derived from 1991 census. 229 counted as visually impaired on basis of selfreported registration. Unclear. Mention Snellen charts and `E’ charts for the mass media source, but do not explain how performed. Capture Mark Recapture methods used to estimates of prevalence. Cross-sectional random sample survey. Confidence intervals Complete ocular examination. Binocular visual acuity – Snellen, 32 720 from secondary recapture sources 288 from one practice 72% Details on age distribution shown in table 3.1 207 51% aged 75+ given) Lavery et al 1988 [30] Melton Mowbr ay 1982 and common eye disease among elderly people on inner London To present visual acuity data for the Eye study. Aged 75 and over on December 31 1980 and surviving on April 1st 1982 calculated by exact methods for small proportions and normal approximation to binomial distribution for larger ones. and Uniocular 3 m Sonksen Silver visual acuity with spectacles normally worn. Near Vision. Cross-sectional study of all those registered in the single general practice in Melton Mowbray. Full refraction by an optometrist Acuity measurements with and without spectacles. 33 677 78.1% 529 Age/sex distribution shown in a chart. Table 3.2 Population based surveys using visual acuity measurements - results. Study Key Results Presenting visual acuity <6/12 North London Study [33] Aged 65+ Number of cases One eye Binocular 367 448 MRC Assessment Trial [35] %Prevalence (95% CI) 23.6 30.2 20.9 to 26.3 24.8 to 35.5 All ages 75+ Total Number 14 600 All visual impairment. Presenting Binocular acuity <6/18 % 95% CI Prevalence 12.4 10.8 to 13.9 Men 5620 9.1 Women 8980 Men and women 75-79 Low vision. Presenting Binocular acuity <6/18 to 3/60 Blindness. Presenting Binocular acuity < 3/60 % 95% Prevalence CI 2.1 1.8 to 2.4 1.7 1.3 to 2.0 2.3 1.9 to 2.8 Presenting Binocular Acuity <6/12 % Prevalence 95% CI 10.3 8.7 to 11.8 7.9 to 10.4 7.5 6.2 to 8.7 14.4 12.6 to 16.2 12.1 10.2 to 13.9 6898 6.2 5.1 to 7.3 5.6 4.5 to 6.6 0.6 80-84 4602 11.9 9.9 to 13.8 9.6 7.6 to 11.5 2.3 85-89 2319 23.4 20.5 to 26.4 19.2 16.2 to 22.1 4.3 90+ 781 36.9 32.5 to 41.3 30 25.8 to 34.1 6.9 Men 34 0.4 to 0.8 1.8 to 2.8 3.4 to 5.2 4.8 to 9.0 % Prevalence 95% CI 19.9 17.8 to 22.0 15.2 13.5 to 16.9 22.8 20.3 to 25.3 10.8 9.1 to 12.6 20.0 17.6 to 22.4 35.3 31.7 to 38.8 53.1 48.3 to 57.9 75-79 2961 4.8 3.6 to 5.9 4.2 3.1 to 5.2 0.6 80-84 1695 10 8.4 to 11.7 7.7 6.0 to 9.4 2.3 85-89 782 19.2 15.5 to 22.9 16 12.4 to 19.6 3.2 90+ 182 28.6 21.6 to 35.5 22 15.6 to 28.4 6.6 75-79 3937 7.2 6.0 to 8.5 6.6 5.4 to 7.8 0.6 80-84 2907 12.9 10.4 to 15.5 10.6 8.1 to 13.1 2.3 85-89 1537 25.6 22.3 to 28.9 20.8 17.5 to 24.0 4.8 90+ 599 39.4 34.5 to 44.3 32.4 27.3 to 37.4 7.0 0.3 to 0.9 1.5 to 3.1 2.0 to 4.4 3.1 to 10.1 8.9 7.1 to 10.7 16.3 14.3 to 18.4 30.2 25.9 to 34.5 42.3 34.5 to 50.1 0.3 to 1.0 1.6 to 3.0 3.6 to 6.0 4.7 to 9.3 12.3 10.4 to 14.2 22.1 19.0 to 25.2 37.9 33.9 to 41.8 56.4 51.0 to 61.9 Women NDNS [34] Pinhole-corrected visual acuity <6/18 Age in years All 65-74 75-84 85+ All subjects Community Institution All subjects Community Institution All subjects Community Institution All subjects Community Institution No measured 1362 1126 236 508 475 33 519 429 90 335 222 113 No. of cases 195 111 84 16 12 4 60 33 27 119 66 53 % Prevalence 14.3 9.9 35.6 3.1 2.5 12.1 11.6 7.7 30.0 35.5 29.7 46.9 Gender M Number measured 690 No. cases 72 10.4 Age in years All 35 65-74 75-84 85+ F M F M F M F Age All (65+) Hayward et al. [36] All subjects Community Institution 65-74 All subjects Community Institution 75-84 All subjects Community Institution 85+ All subjects Community Institution Population group age range 0 + White Asian White Female White Male Asian Female Asian Male Wormald et al. [32] 672 272 236 283 236 135 200 123 5 11 28 32 39 80 Pinhole corrected visual acuity <6/12 18.3 1.8 4.7 9.9 13.6 28.9 40.0 Number measured Number of cases Estimated % prevalence 1362 386 28.3 1126 252 22.4 236 134 56.8 508 50 9.8 475 41 8.6 33 9 27.3 519 134 25.8 429 87 20.3 90 47 52.2 335 202 60.3 222 124 55.9 113 78 69.0 Age standardised prevalence % 95% CI Blindness and partial sight (registerable) 0.49 0.48 to 0.503 1.21 1.10 to 1.32 0.51 0.49, to 0.52 0.46 0.44 to 0.48 0.77 0.67 to 0.89 1.88 1.64 to 2.12 Best corrected VA <3/60 Age Gender Number measured 36 % Prevalence 95% CI 65-74 75+ All (65+) Both Men Women Both Men Women Both Men Women 101 38 63 106 28 78 207 66 141 0 0 0 1.9 0 2.6 1.0 0 1.41 Gender Number measured % Prevalence 95% CI Both 101 0.99 0.03 to 5.4 Men 38 0 Women 63 1.59 0.04 to 8.5 Both Men 106 28 6.6 3.57 2.7 to 13.1 0.09 to 18.4 Women Both Men Women 78 207 66 141 7.7 3.9 1.5 5.0 2.9 to 16 1.7 to 7.5 4.3 to 8.2 2.0 to 10.0 0.2 to 6.6 0.3 to 8.9 0.15 to 3.4 0.2 to 5.0 Best corrected VA <6/36 Age 65-74 Age 75+ All (65+) Best corrected VA <6/18 Age Gender Number measured % Prevalence 95% CI 65-74 Both 101 0.99 0.03 to 5.4 37 75+ All (65+) Men Women Both Men Women Both Men Women 38 63 106 28 78 207 66 141 0 1.59 14.2 10.7 15.4 7.7 4.5 9.2 0.04 to 8.5 7.5 to 20.8 2.3 to 28.2 8.2 25.3 4.5 to 12.2 0.95 to 12.7 5.0 to 15.3 Visual acuity <6/12 and > 6/60 Age Gender Number measured % Prevalence 65-74 Both Men Women Both Men Women Both Men Women 101 38 63 106 28 78 207 66 141 0.99 0.03 to 5.4 0 1.59 0.04 to 8.5 19.8 12.2 to 27.4 21.4 8.3 to 40.9 19.2 11.2 29.7 10.6 6.4 to 14.8 9.1 3.4 to 18.7 11.3 6.1 to 16.6 Best corrected visual acuity in better eye 6/18 to 6/36 <6/36 % prevalence % prevalence 10.3 2.9 18.2 0.0 18.2 3.0 25.9 4.2 22.7 0.0 35.5 10.5 75+ All (65+) Lavery et al [30] Age 76-79 80-84 85+ Gender Men Women Men Women Men Women Number measured 68 99 66 143 22 76 38 95% CI 76+ RNIB 1991 [37] Private Household RNIB/ONS 2000 [27] Private Household Men Women All 185,688 156 318 474 VA 6/24 or <N14 and eligible for registration <6/12 Blind registered or visual acuity <6/60 Blind or partially sighted registered or visual acuity < 6/24 2 15.4 25.8 22.4 16+ 16-59 60-74 75+ 16-59 60-74 75+ 16+ 16-59 60-74 75+ 16+ 16-59 60-74 75+ 2.6 4.4 3.8 1.72 0.3 2.3 15.2 0.55 2.10 10.52 1.7 0.12 0.49 2.0 0.35 0.31 1.10 5.4 16+ 0.90 Since overall figure not given in Bruce et al 37. Bruce I, M.A., Walker E., Blind and partially sighted adults in Britain: the RNIB survey. 1991, Royal National Institute for the Blind: London.. this was calculated as 757/1384 = 0.546 of OPCS prevalence estimate 39 Table 3.3 Prevalence % of visual impairment and blindness in different studies1 Visual acuity levels <3/60 <6/36 <6/60 Wormald Wormald Age 65+ (95% confidence interval) 1.0 (0.15, 3.4) Best corrected, better eye 3.9 (1.7, 7.5) Best corrected better eye Age 75+ (95% confidence interval) Wormald 1.9 (0.2, 6.6) Better eye MRC Assessment Trial 2.1 (1. 8, 2.4) Binocular presenting Lavery (76+) Wormald 3.8 (2.3, 5.9) 2 Best corrected 6.6 (2.7,13.1) Best corrected VA 6/24 or <N14 RNIB 1990 15.2 Binocular presenting Blind or partially sighted registered or visual acuity < 6/24 RNIB 2000 5.4 Binocular presenting Wormald 7.7 (4.5, 12.2) Best corrected better eye NDNS 9.9 (8.2, 11.6) Pinhole corrected Wormald 14.2 (7.5, 20.8) Best corrected <6/18 NDNS MRC Assessment Trial 15.2 (12.4, 18.0) 4 Pinhole corrected 12.4 (10.8, 13.9) Binocular presenting 10..3 Pinhole corrected Lavery Wormald NDNS MRC Assessment Trial RNIB 2000 26.2 (22.2, 30.2) 4 Best corrected 21.8 (14.4, 31.0) Best corrected 32.4 (28.8, 36.0) 3 Pinhole corrected 19.9 (17.8, 22.0) Binocular presenting 10.5 Binocular presenting <6/12 North London 30.2 (24.8, 35.5) Both eyes 53.8 (48.4, 59.2) Either eye NDNS 22.4 (20.0, 24.8) 4 Pinhole corrected 1 Unless otherwise stated results are for people living in the community including registered and those who failed reading test and/or had field loss 3 Minimum estimate (calculated by adding estimate for VA<6/12 > 6/60 and VA <3/60) 4 No adjustment made for clustering when calculating the confidence interval 2 . 40 Chapter 4 Causes of Visual Impairment 41 Introduction This chapter reports the results from five UK population-based prevalence studies that have investigated the causes of visual impairment. The methods employed by each survey are shown in Table 4.1 and the results are presented in Table 4.2. A study of the prevalence of eye disease in the elderly in an English community (Gibson et al 1985) [31] Summary 484 subjects living in Melton Mowbray aged 76+ were examined by an ophthalmologist and an ophthalmic optician. The prevalence of eye diseases associated with a visual acuity of less than 6/9 was 46.1%, for senile macular degeneration 41.5% and for open angle glaucoma 6.6%. Methods A randomly selected age-stratified sample from all those registered in the single general practice in Melton Mowbray who were 75 and over on December 31 1980 and still living there on April 1st 1982. The data were obtained from the same survey that was discussed in Lavery et al.1988 in Chapter 3. 529 (out of the 677 eligible) subjects were examined, 55 at home or in hospital, the rest were examined in a hospital outpatients department. Eye diseases were defined as follows: 1. Age-related cataract were defined as best corrected visual acuity of 6/9 or worse in the affected eye attributable to lens opacities. Subjects with aphakia were included in this group, but cataracts that could be ascribed to congenital or secondary causes were excluded. 2. Senile macular degeneration was diagnosed in those with best corrected visual acuity of 6/9 or worse and the presence of degenerative changes. Degenerative changes were divided into dry and exudative type. A history of secondary or congenital causes of macular disease excluded the diagnosis of senile macular degeneration. 3. Open angle glaucoma a) Glaucomatous cupping of the optic disc, defined as a cup-disc ratio of > 0.5 or the presence of notching of the neural rim or asymmetry of the optic discs. b) Intraocular pressure by applantation tonometry about 21 mmHg. c) An open anterior chamber angle as judged by the method of Herick and Shaffer. d) If the above criteria were met the subject was asked to attend an eye clinic where a repeat ophthalmic examination included Goldman perimetry was performed. Glaucomatous field defects were considered as enlargement of the blind spot, arcuate scotoma, paracentral scotoma, nasal step and advanced field loss. A diagnosis of low-tension glaucoma was made if a, c, d but not b were present. Results The prevalence rates of senile cataract, senile macular degeneration and open angle glaucoma by age and sex in the sample are shown in Table 4.2. The overall prevalence of senile cataract was 46.1 % which increased with age. The odds of having senile cataract in the 85+ age group as opposed to the 76-84 group was 2.6 (1.6,4.3). There was no significant difference between the sexes. The overall prevalence of senile macular degeneration was 41.5%. There was no significant difference between the sexes but the odds of having this disease in the older age group was 1.8 (1.1, 2.9). The overall prevalence open angle glaucoma was 6.6% with no significant difference between the sexes or age groups. 42 Comment The results were based on rigorous clinical examination and clearly defined criteria. The definitions were based on very minimal levels of visual acuity (<6/9) and, for macular degeneration, degenerative changes which included very early maculopathy. Visual problems in the elderly population and implications for services (Wormald et al.1992) [32] Summary 207 people age 65 and over, from an inner London health centre, were examined in order to determine the prevalence of common eye problems. The majority of those with best corrected visual impairment had cataract. Methods Sampling methods are described in Chapter 3. The central visual field was tested with the Henson CFS2000.Intraocular pressure was tested with the Perkins mark 2 tonometer with the slit lamp. After dilation with tropicamide 1%, the optic disc vertical cup to disc ratio was recorded. Subjects were assessed clinically by one of two ophthalmologists. When indicated the retinal periphery was examined with a binocular indirect opthalmoscope and 28 dioptre aspheric lens. Results The results are shown in table 4.2. Cataract was the main cause of vision impairment in 12/16 with best corrected visual acuity < 6/18.Ageing maculopathy was the cause of vision impairment in 3/16. This disease was found only in the 75+ age group (2.8%). Glaucoma caused blindness in one person and was prevalent in 4.4% of those aged over 65. More than 72% of the bilateral visual impairment was potentially remediable by surgery or glasses, nearly one in three had visually impairing cataract and 88% of these were not in touch with the eye services. Eye problems were more prevalent in people living in relatively underprivileged areas. 56 subjects (27%) would probably have benefited from refraction. Comment Clinical examination carried out by an ophthalmologist but results are based on very small numbers. The prevalence of eye disease in Leicester - a comparison of adults of Asian and European descent (Das et a 1994) [38] Summary A random sample from two neighbouring inner Leicester general practices of approximately the same size, one predominately European, the other predominately Asian was used in this survey. Cataract prevalence was significantly related to age and differed markedly between the racial groups. Asians had a significantly higher prevalence of age-related cataract. Age was significant for age-related macular degeneration but sex and racial group were not. 43 Methods The samples were stratified by age (40-59 and 60+). 369 subjects were measured at a specialist eye clinic for visual acuity, near and distance vision , full refraction and split lamp biomicroscopy. Perkins applanation tonometry and fundus examination with direct and binocular indirect ophthalmoscopy after pupillary dilation. Examination for cataract was carried out by direct ophthalmoscopy after mydriasis and direct and retroillumination with the slit lamp. Age related cataract was said to be present when the best-corrected visual acuity was 6/9 or worse in the affected eye and this was attributable to lens opacity. Age related macular degeneration was defined by the presence of degenerative changes together with a best-corrected visual acuity of 6/9 or worse. People with a history of secondary of congenital cause of macular disease were excluded from the age-related macular degeneration category. The criteria for the diagnosis of diabetic retinopathy were a history of diabetes and the presence of microaneurysms, dot haemorrhages, hard exudates, microvascular abnormalities or neovascularization. The diagnosis of open-angle glaucoma was made if there was glaucomatous cupping of the optic disc and an intra-ocular pressure above 21 mmHg and an open anterior chamber angle and glaucomatous field defects. Results Of the 377 that attended for examination 165 were Asian. The pattern of response varied between the two ethnic groups with the chance of response increased if the subject had a previous contact with the local hospital service, especially if they had had a previous appointment at the eye clinic. This effect was stronger in the Asian community than in the European. The prevalence of age-related cataract, aphakia, pseudophakia and age-related macular degeneration are shown in table 4.2. Cataract prevalence was significantly related to age (p<0.001). After adjustment for age, the prevalence did not differ significantly with sex (p=0.94) but did differ markedly between the racial groups (p<0.001). Asians had a significantly higher prevalence of age-related cataract: 30% compared to 3% for those aged under 60 and 78% vs. 54% in those age 60 and over, Age was significant (p<0.001) for age-related macular degeneration but sex and racial group were not. Comment This was the only study to investigate eye disease in the Asian community. However the study population was a small sample from a selected region which may not be representative of the general ethnic population in Britain. There was a low response rate (42%). Prevalence of serious eye disease and visual impairment in a north London population: population based, cross sectional study (Reidy et al 1998) [33] Summary 1,547 people aged 65+ sampled from populations in North London underwent an eye examination conducted by ophthalmologists. The prevalence of VA <6/12 due to eye diseases was : cataract 30%, refractive error 9%, age related macular degeneration 8%, glaucoma 3%, and suspected glaucoma 7%. 44 Methods The sampling methods were described in Chapter 3. Visual acuity, autorefraction, and field examinations were carried out by a trained ophthalmic nurse. The remainder of the examination was by ophthalmologists. Refractive status was ascertained by using the Humphrey 580 autorefractor. Visual fields were assessed in all subjects by the 76 point visual fields of the Humphrey 730 screener, with reading correction. Anterior segment examination was carried out using a slit lamp. Lens, vitreous, and retinal examinations were done after pupil dilatation. Comparison with LOCS II standard photographs was used to record cataract type and density. People were classified as having cataract causing visual impairment when the visual acuity in one or both eyes was poorer than 6/12 and the impairment was attributable to a lens opacity. Those with age related macular changes causing visual impairment (visual acuity <6/12) in one or both eyes were classified as having age related macular disease causing visual impairment. These two classes were not exclusive. So that the prevalence of either class would not be underestimated, patients in whom both conditions contributed to the poor vision were included in both classes. Refractive error causing visual impairment was defined as reduced visual acuity of <6/12 in any eye due only to refractive error. People were classified as “definite glaucoma cases” when there was an absolute field defect and either a cup:disc ratio of 0.7 or larger or substantial asymmetry of the cups (a difference in cup:disc ratio of 0.3 or larger) between the two eyes. “Glaucoma suspect cases” were those who had an absolute field defect and either a cup:disc ratio of 0.5 but <0.7 or asymmetry of 0.2 but <0.3. Results The results are shown in table 4.2. The prevalence of visual acuity <6/12 due to unoperated cataract was 30%, due to age related macular degeneration was 8%, and due to refractive error was 9%. The prevalence of definite chronic open angle glaucoma was 3%, and a further 7% of subjects were suspected of having glaucoma. Impaired vision in one or both eyes was present in more than half of the sample (53.8%) (815/1547). The proportion of VA < 6/12 in one or both eyes due to cataracts was 55% and due to refractive error was 16.7 %; taking both causes into account the authors report that the proportion of VA< 6/12 that was potentially remediable was 72 %.when both eyes were impaired and 69% when either eye was impaired. Comment This was a well conducted survey with high response rates and a detailed clinical examination. Data on the causes of visual impairment were reported only for visual acuity <6/12. Causes of visual impairment in people aged 75 years and older in Britain: an add-on study to the MRC Trial of assessment and management of older people in the community. (Evans et al. 2004) [39] Summary Causes of vision impairment were ascertained for 1,742 people who had been identified with vision impairment (binocular VA<6/18) in the MRC Trial of Assessment [35](see chapter 3). The main causes were refractive error (31.6%), age-related macular degeneration (32.6%); 45 cataract (20.4%), glaucoma (6.4%), myopic degeneration (2.6%) and diabetic eye disease (2.1%). Methods The results on causes of vision impairment came from an add-on study to the main MRC Trial The methods for ascertaining visual impairment have been described in detail in the previous chapter [35]. 49 of the 53 practices who took part in the MRC trial took part in the cause of visual impairment study. For those with VI <6/18 not corrected by pinhole, data regarding the cause of vision loss were extracted from the general practice medical notes and additional follow-up questionnaires were also sent to the hospital ophthalmologist to confirm the cause of vision loss. This questionnaire was in the form of a checklist by eye that covered: age-related macular degeneration (exudative, geographic atrophy), cataract (age-related, congenital, and other), and glaucoma (primary open-angle, primary closed-angle, other), diabetes (diabetic retinopathy, other), myopic degeneration, other (specify). The ophthalmologist was asked to rank, if possible, any conditions ticked in order of their contribution to cause of visual loss. Results There were 1,742 (12.5%) people visually impaired in the 49 participating practices. Of these, 450 (26%) had a pinhole acuity 6/18 or better. Of the remaining 1292, the cause sought from GP notes was obtained in 976 (76%) cause obtained and in 316 (24%) the cause was not known. The causes of vision impairment are shown in Figure 4.1 and were: 31.6% due to refractive error; 32.6% due to age related macular degeneration, 20.4% due to cataract, 6.4% due to glaucoma, 2.1% due to diabetic eye disease, 2.6% due to myopic degeneration in 2.6% and due to other rarer causes aggregated together in 3.8%. Figure 4.1 31.6 Refractive error AMD Cataract 32.6 Glaucoma 3.8 Diabetic eye disease 2.6 Myopic deg 2.1 6.4 Other 20.4 Thus in the over 75s age group, a half of visual impairment can be attributed to remediable causes: refractive error and cataract. Comment The results were based on a very large sample from the 75 and over population in Britain. Difficulties with the pinhole in 40% of those with VA< 6/18 suggest that refractive error may have been underestimated. Causes of vision impairment were extracted from GP notes or 46 hospital records and no direct eye exam was available. In around a quarter the cause was unknown. The nursing home population was not included. Chapter summary This chapter summarises five surveys that provide population prevalence rates of (mainly agerelated) eye diseases. One study [39] is based on a sample covering the whole of Great Britain, the others are from selected regions, two in London [32, 33]and two in Leicestershire [31, 38]. All except one study [38] are concerned with the elderly. It is difficult to compare directly the results from the studies as they all use different definitions of disease, and cut points for the group being investigated e.g. <6/18 in the MRC Trial and VA< 6/12 in the North London Study. It is clear that cataract, refractive error and age related macular degeneration are the major causes of vision impairment in the elderly with the contribution from age related macular degeneration increasing with increasing age. The data from the MRC Assessment Trial also show that the relative contribution of different causes varies by level of impairment with cataracts being most important for low vision, and age related macular degeneration for blindness. Glaucoma and diabetic retinopathy make minor contributions to vision impairment. However not all studies have included additional tests such as fields, or funduscopic examination so it is possible that the contribution of glaucoma and diabetic retinopathy to visual impairment may have been underestimated. In the North London study which did include a detailed assessment for glaucoma, definite glaucoma was the reason for VA <6/12 in either eye in 3% and possible glaucoma in 7%. In contrast the prevalence of cataract associated with VA < 6/12 in one or both eyes was 30% and refractive error was 9%. In terms of the proportion of visual acuity <6/12 in at least one eye which is due to remediable causes, cataracts and refractive error account for 69%. Based on the proportions with cataract and refractive error on the studies we have estimated the prevalence of visual impairment due to non remediable causes (Table 4.3). This has the biggest proportional reduction in the studies by Wormald et al and in the North London (over 65 age group) where up to 75% of visual impairment was reported as due to these two causes. The effect is smaller in the MRC Trial (52%) since age related macular degeneration is a more important cause of vision impairment in the older age group. In order to place these revised prevalence figures for visual impairment into context with the registration figures, estimates of the prevalence rates for registered blind people in England were calculated using the published figures for blind and partially sighted registration [12] and 2000 census (http://www.statistics.gov.uk/census2001/pop2001/england.asp). The estimates are shown in Table 4.4. Overall 0.624% (306,500) of the population were registered rising to 5.7% of the over 75s (211,070). We next examined how these estimates agreed with the results from the studies reported in Table 4.3 and the impact on the numbers of the variation in prevalence. The MRC Trial estimates and those from the ONS/RNIB 2000 are closest to the actual registration figures (237,116 and 200,067) respectively. The estimates by Wormald (131, 526) are very low but the numbers of over 75s in that study were small and the estimates show wide confidence intervals. Finally the 1990 RNIB first Needs Survey [37] gave estimated numbers (563,152) which are considerable higher than the actual registrations. The RNIB report gives the number of people eligible for registration as blind or partially sighted. However, people are not usually registered if their sight loss is remediable. If the visual acuity tests on which the estimates were 47 based were not corrected for refractive error, or included people with operable cataract, for example, then these will be over-estimates of the number of people requiring registration. Since 35% of the over 75s in the RNIB study self reported the main cause of the vision problem as due to cataracts it is likely that the high figures reported by RNIB are because cataracts and probably also refractive error have been included. As no ophthalmological exam was conducted in the RNIB sample this cannot be confirmed. 48 Table 4.1 Studies on causes of visual impairment – Methods Name Location Aims Gibson et al. 1985 [31] Melton Mowbray Das et al 1994 [38] Leicester. To estimate prevalence of eye disease To estimate prevalence of eye disease in Leicester. Comparison of adults of Asian and European descent Prevalence of main serious eye disorders North London Study Reidy et al. 1998 [33] North London Age 40+ Sample size Response rates Number Included Age/sex etc 677 71.5% 484 896 42% 369 Mean age 83 (SD 4.3) 147 males, 337 females 165 Asian, 204 European Excluded 8 people of West-Indian origin 209 subjects aged 60+ Age 65+ Registered at GP practices 1840 from 7 GP practices 84% 1547 from 7 GP practices 65+ 94.3% white Great Britain To ascertain causes of visual impairment Age 75+ . Not in long stay hospitals or nursing homes or terminally ill 49 GP practices 69% 1,742 visually impaired (12.5%) from 49 GP practices 75+. mean age 81.3 percentage male 39% Inner London To determine prevalence of common eye disease Age 65+ 288 from one practice 72% 207 51% aged 75+ MRC Assessment Trial Evans et al. 2004 [13] Wormald et al. 1992 [32] Inclusion /Exclusion Criteria 49 Table 4.2 Studies on causes of visual impairment – Results Name of study Gibson et al. [31] Estimated prevalence of visual impairment Not given Causes (not necessarily mutually exclusive). Senile cataract Best corrected VA <6/9 Age 76-84 Total number examined = 484 85+ Senile macular degeneration 76+ 76-84 85+ Open angle glaucoma 76+ 76-84 85+ 76+ 50 Sex Men Women All Men Women All All Men Women All Men Women All All Men Women All N examined 132 260 392 15 77 92 484 132 260 392 15 77 92 484 132 260 392 % prevalence 37.1 43.8 41.6 60.0 66.2 65.2 46.1 40.9 37.7 38.8 40.0 55.8 53.3 41.5 9.8 5.8 7.1 Men Women All All 15 77 92 484 4.2 2.6 2.9 6.6 Wormald et al 1992 [32] Percentage in population. Age 65+ n=207 Blindness <6/36 3.9% N. with condition Ageing maculopathy Glaucoma Cataract Ageing maculopathy Optic atrophy Cataract VA < 6/18 7.7% All aged 65 and over Cataract Aphakic Glaucoma Diabetic retinopathy Ageing maculopathy Name of study North London Study [33] 1 1 6 2 2 12 Age 65+ 65-74 75+ 65+ 65+ 65+ 65+ 65-74 75+ % of visually impaired with condition 12.5 12.5 75 13 13 75 Population prevalence % 5.8 1.0 10.4 5.8 4.4 1.0 1.4% 0 2.8 Estimated prevalence of visual impairment Causes (not necessarily mutually exclusive). Number of cases Estimated prevalence % 95% CI 53.8 % age 65+. Criterion VA < 6/12 in either eye 1. Cataract 451 30 25.1 to 35.3 2. Had cataract surgery (one or both eyes) 162 10 5.5 to 10.8 8 5.8 to 10.8 3. Age related macular disease 133 3 2.3 to 3.6 4. Glaucoma (chronic open angle) 47 7 5.4 to 8.4 5. Suspected glaucoma 109 9 7.0 to 11.4 6. Refractive error causing visual impairment (one or both eyes) Age-related cataract, aphakia or pseudophakia 136 1547 examined Das et al. 1994 [38] 95% CI 3.0 to 9.9 0.03 to 5.8 4.6 to 16.2 3.0 to 9.9 2.0 to 8.0 0.1 to 3.4 0.3 to 4.2 0.5 to 8.0 Not given Total number examined =369 Asian Age Number examined Prevalence % Std. error 40-49 50-59 60-69 17 49 69 17 49 69 5.2 8.2 6.7 51 European 70+ 40-49 50-59 60-69 70+ 93 39 32 69 64 93 0 6 30 64 4.9 4.3 5.5 6.0 Asian 60-69 20 0 - 70+ 60-69 70+ 13 28 15 23 0 7 11.7 6.4 60-69 32 3 3.1 70+ 60-69 70+ 39 37 25 28 3 16 7.2 2.7 7.3 Age-related macular degeneration Women Men European Women Men MRC Trial [39] Estimate of prevalence of visual impairment for 75+ 12.5% Criterion binocular visual impairment (VA < 6/18 ) N=1426 8.55% Binocular VA < 6/18 excluding those with refractive error. N=976 Cause N. with condition % of with condition 95% confidence interval Refractive error 450 31.6 28.3 to 34.8 AMD 516 36.2 32.9 to 39.5 Cataract 350 24.5 21.8 to 27.4 Glaucoma 113 7.9 6.2 to 9.6 Diabetic eye disease 33 2.3 1.5 to 3.1 Vascular occlusions 9 0.6 0.1 to 1.1 Myopic degeneration 41 2.9 1.9 to 3.8 Other Cause 67 N. with condition 4.7 % of visually impaired with condition 3.7 to 5.7 95% confidence interval Refractive error AMD Cataract Glaucoma Diabetic eye disease Vascular occlusions Myopic degeneration - - 516 52.9 49.2 to 56.5 350 35.9 31.7 to 40.1 113 11.6 9.1 to 14.0 33 3.4 2.2 to 4.6 9 0.9 0.2 to 1.6 41 4.2 2.8 to 5.6 - 52 Other Cause All aged 75 and over N=14,403 Refractive error AMD Cataract Glaucoma Diabetic eye disease Vascular occlusions Myopic degeneration Other 67 N. with condition 6.9 Population prevalence with va <6/18 5.5 to 8.2 95% conf. Int. 450 3.2 2.6 to 3.8 516 3.7 3.1 to 4.1 350 2.5 2.0 to 3.0 113 0.8 0.6 to 1.0 33 0.2 0.15 to 0.32 9 0.06 0.01 to 0.11 41 0.3 0.2 to 0.4 67 0.5 0.4 to 0.6 53 Table 4.3 Prevalence of visual acuity before and after exclusion of cataracts and refractive error (RE) using data reported from individual studies on the causes of visual impairment as reviewed in the chapter %Prevalence % of visual impairment1 due to RE & Cataract 65+ 30.2 72 8.5 <6/12 either eye 65+ 53.8 69 16.7 <6/18 best corrected 65+ 7.7 752 1.9 <6/18 presenting binocular 75+ 12.4 52 6.4 75+ 15.2 Not known3 Not Known 75+ 5.4 Not known Not known Study Visual impairment criterion North London [33] < 6/12 both eyes Wormald [32] MRC Assessment Trial [39] RNIB 1990 [37] RNIB 2000 [27] 1 Age Group %Prevalence after excluding cataract & RE VA 6/24 or <N14 Blind or partially sighted registered or visual acuity < 6/24 Visual impairment defined in column 2 2 Cataract was the reason for visual impairment in 75% of people aged 65+ with best corrected VA < 6/18. The proportions with refractive error could not be estimated as best corrected acuity “removes” those with refractive error 3 The main cause reported by 35% of those aged 75+ was cataracts but an ophthalmological examination was not conducted and therefore the figures are not included in the above table. No information is available on the proportion with refractive error. 54 Table 4.4 Estimated prevalence of registered blind and partially sighted in England in 2001 (calculated by the authors)4. Number of people on 2000 blind register [12] Number registered Partially Sighted Number registered Blind and PS Population of England from 2001 census Prevalence of blindness registration 2000/2001 Prevalence of Blindness and Partial Sight registration 2000/2001 All ages 157,820 1 0-4 710 5-17 3,150 18-49 16,450 50-64 13,360 65-74 15,780 75+ 108,360 148,6801 620 3,650 14,030 11,500 16,160 102,710 306,500 1,330 6,800 30,480 24,860 31,940 211,070 49,138,831 2,926,46 0 8,214,680 21,630,529 8,559,561 4,102,656 3,704,945 0.032% 0.024% 0.038% 0.076% 0.16% 0.39% 2.92 % 0.624% 0.045% 0.083% 0.141% 0.29% 0.78% 5.70% 1 Numbers in age groups do not add to total because of rounding (stated in report of the register) [12] 4 Prevalence estimates calculated using the 2001 census data and the blind and partially sighted register of 2000 55 Table 4.5 Actual registration figures for 2000 for people aged 75 and over in England [12] and expected numbers in England eligible for registration from other studies/surveys DOH registration figures Study 5.70% 211,070 Numbers (95% CI) likely to be eligible for registration RNIB 19902 Prev (95% CI) of those likely to be eligible for registration 6.4 % 95% CI 5.6,7.2 3.6% 95% CI (1.9, 5.2) Not known RNIB 20002 Not known 200,067 MRC Trial 1 Wormald 19921 237,116 207,477, 266,756 131, 526 69, 468 to 192, 657 563,152 based on estimates of prevalence adjusted for “treatable causes of vision impairment” 1 2 based on estimates of prevalence but without adjustment for treatable causes of vision impairment 56 Chapter 5 Prevalence of visual disability and visual impairment in children in the United Kingdom 57 Introduction This chapter summarises the literature relating to the prevalence of visual impairment in children in the UK. The first section concentrates on nationwide surveys, a number of which RNIB played a leading role in. Data from the larger local (rather than national) surveys are then summarised. The methods for each national survey are summarised in table 5.5 and the results in table 5.6. The surveys from geographically defined areas are summarised in table 5.7. There are no agreed definitions of visual impairment among children, an issue discussed in detail elsewhere. [40] Terms such as visual impairment and visual disability have been used to mean different things in different studies and contexts. As far as possible, we have therefore defined what the outcomes were in the various studies. The prevalence of disability among children, OPCS surveys of disability in Great Britain (Bone et al 1989) [41] Summary This is the report of the 1985 OPCS disability surveys of children aged 15 and under in private household and communal establishments in Great Britain. The sampling procedure was the same as in Martin et al.1988 [25](see chapter 2). Questionnaires were sent to 100,000 private households in 1985. Interviews were obtained with or on behalf of 2,025 of the 2,403 children, identified as disabled from the sift forms. Interviews were obtained on behalf of 1,019 children in communal establishments. The main questionnaires covered the same areas of disability as the adult interviews and had the same basic structure, but were adapted for children. The estimated prevalence rate of visual disability for children aged 15 and under both in private households and resident in communal establishments was 0.2%. The estimated number of disabled children aged 15 and under in Great Britain was 22,000. Visual disability refers to not seeing well enough to recognise things in a picture book or cannot see well enough to follow a TV programme sitting at a normal distance to the TV set or cannot see well enough to recognise someone across a road Methods Private Households The sample was the same as that for the adult disability survey [25]see chapter 2 for details of the sampling procedure). A screening questionnaire was sent out to a random sample of households. The design is shown in figure 5.1. The questionnaire contained detailed questions of health problems and disabilities. There was a separate box for questions relating to children asking if there were any children under 16 (including babies and toddlers) in the household and, if the answer was yes, the following was asked: “Is there any child in your household: a) who is unable to do things which most children of the same age can do because of a health development or behaviour problem? b) who needs more help than usual for children of the same age with feeding, dressing, toileting walking going up and down stairs or other daily activities? 58 c) who attends a special school or special or remedial unit of an ordinary school because of health or behaviour problem , disabilities or learning difficulties? d) who attends an ordinary school but is limited in taking part in school activities because of health or behaviour problems or disabilities? e) whose health , behaviour of development causes worry that he or she may have a longterm health problem, physical or mental disability or handicap?" All households with the answer “yes” to one or more of these (sift) questions were included in the sample for interview. The questions and severity scores are shown in table 5.1 for children aged 6 and over and in table 5.2 for children younger than 6. Interviews were carried out with, or in the presence of, one of the child’s parents, usually the mother. Children were categorised as visually disabled if the answer was ``yes" to any of the questions shown in table 5.1 or table 5.2 depending on their age. 59 Figure 5.1: Flow chart showing the numbers of participants at each stage of the OPCS 1985 survey of children in private households 60 Scale S1 S2 S3 S4 S5 S6 S7 S8 S9 S10 S11 S12 S13 Table 5.1: Seeing Severity scores for children aged 6-15 [Bone and Meltzer1989] Description Score Cannot tell by the light where the windows are 12 Cannot see well enough to recognise someone he knows if close to his face 10.3 Cannot see well enough to walk around an unfamiliar room without bumping into things 9.7 Is aged at least 8 and cannot see will enough to read a large print book even if held close to his face. 9.2 Cannot see well enough to reach for and pass things at meal times 8.3 Cannot see well enough to enjoy a book of pictures unless held close to his face 8.0 Cannot see well enough to follow a TV programme even if sitting up close to the TV set 7.6 Is aged at least 8 and can only see well enough to read a large print book if held up close to his face. 6.8 Cannot see what was written on the blackboard if sitting at the front of the classroom 6.8 Cannot see well enough to recognise someone he knows across a room 6.3 Cannot see well enough to follow a TV programme sitting at a normal distance to the TV set 4.7 Is aged at least 8 and cannot see well enough to read ordinary newspaper print. 4.3 Cannot see well enough to recognise someone he knows across a road 2.3 61 Scale S1 S2 S3 S4 S5 S6 S7 S8 S9 Table 5.2: Seeing Severity Scores for children aged 5 and under [Bone and Meltzer1989][41] Description Score Is aged 5 and cannot tell by the light where the windows are 11.8 Is aged 5 and cannot see well enough to recognise someone he knows if close to his face 9.5 Is aged 6 months to 1 year and cannot see well enough to follow a moving object with his eyes 9.5 Is aged 5 and cannot see well enough to walk around an unfamiliar room without bumping into things 8.1 Is aged 5 and cannot see well enough to see things in a picture book held very close to his face. 7.9 Is aged 5 and cannot see well enough to follow a TV programme even if sitting up close up to the TV 5.7 Is aged 5 and cannot see well enough to recognise someone he knows across a room 4.8 Is aged 5 and cannot see well enough to recognise things in a picture book held at a normal distance to 4.7 his face. Is aged 5 and cannot see well enough to follow a TV programme sitting at a normal distance to the TV 1.5 set 62 Communal establishments A list of institutions providing residential care for children was obtained from various government departments. This list was then sent to the general managers of health authorities, directors of social services, directors at the administrative headquarters of voluntary and charitable organisations, and chief education officers asking the recipients to amend and update it. The design is shown in figure 5.2. 3,421 establishments were found in this way. In order to identify those establishments that contained children who were eligible a “census form” was sent to each of these establishments asking for the name and age of each child and indicates whether they were disabled. The form stated that: “A child should be regarded as disabled if he/she has difficulties with everyday activities because of a long-term health problem. This includes physical, mental and behavioural problems which are chronic in nature.” The same interview questions were asked as in the private households’ children's survey. Interviews were obtained for a maximum of 4 children in each establishment. For the communal establishments a weight was applied to compensate for inclusion of different proportions of institutions according to the number of residents. In both surveys weights were applied to allow for non-response and to bring the sample estimates up to the population estimates. 63 Figure 5.2: Flow chart showing the numbers of participants at each stage of the OPCS 1985 survey of children in communal establishments 64 Results 3,421 establishments were sent the census forms. 79% responded. The highest response rates were from establishments administered by health authorities (85%) and the lowest from establishments run by voluntary and charitable organisations (76%). The analysis of data in the census forms indicated that 687 (25%) of institutions were eligible to be included in the survey. The majority of the remaining 75% were short-term homes. All establishments with more than 11 eligible children were included in the sample and there was selective sub-sampling of those with a smaller number than this. 332 institutions were selected for interviews. Of these 44 were found subsequently to be ineligible (mainly because the children went home at weekends and would therefore have been eligible for the private households’ survey. 1,019 Children from 288 co-operating institutions were interviewed. Prevalence estimates are not provided for institutions on their own. The estimated prevalence rates for visually disabled children aged 15 and under living in private homes and institutions was 0.2% for all age groups. The estimated number of visually disabled children in communal establishments in Great Britain in 1985 was estimated to be 1,000. The number of disabled children in the total population was estimated to be 22,000. Comment This survey included a random sample of the total population of Great Britain, a large sample size and used its own questionnaire. The report includes the “sift” questionnaire and details the disability scales. Although detailed questions were asked on levels of seeing disability (see tables 5.1 and 5.2), data on levels of sight disability are not provided in this report. Prevalence estimates are provided only for those deemed to have some sight disability. A specific weakness of this report is that it does not detail how children aged between 6 months and 5 were identified as visually disabled. No figures were given for the number found to be disabled in communal establishments, and thus it was not possible to calculate the number of visually disabled in the sample. Blind and partially sighted children in Britain: The RNIB survey (Walker et al 1992) [42] Summary This report is concerned with blind and partially sighted children and their needs. The survey was based on interviews carried out in April and May 1988 with parents or guardians of 285 visually impaired children (aged 3 to 19) randomly selected from 33 local education authorities (LEAs) in England, Scotland and Wales. The education authorities were selected to provide a representative sample of LEAs in Great Britain. The estimated number of children in Great Britain categorised as visually disabled (for educational purposes) by the local authorities was 10,000 (0.1%). The prevalence of visual disability was greater in boys than in girls (64% versus 36%), with a greater disparity among those aged 12 years and over (70% versus 30%). Methods A random sample of 37 LEA's were selected after splitting Great Britain into 8 geographic regions and stratifying the LEA's within each region by metropolitan or county area, educational policy and population density. Selection of the LEA's was made independently within each 65 region with a probability according to the total number of school children in the area. 33 out of the 37 selected LEA's co-operated in the survey. The prevalence estimates were based on the number of school children (aged between 3 and 19 years) who had been identified as having a visual disability by selected LEAs. A form was sent to each LEA contact person (appointed by the LEA) asking for: “Details on every child or young person for whom you have records or identified as having a visual handicap, whether “educationally blind” or “partially sighted”, including those with multiple handicaps. We are trying to assess the total population of visually handicapped children (defined below), so include those children whom you may not have formally assessed, but you acknowledge as meeting the criteria, providing as much information as you have available. “Educationally blind” means a child or young person requiring education by means not involving the use of sight (i.e. dependent wholly or partly on non-printed materials). “Partially sighted” denotes someone who, although not blind, requires specialised help or attention, but who can benefit from sighted methods of education.” The prevalence figure was calculated by dividing the number of children aged 3-19 identified as visually handicapped by the LEA's by the total number in the 33 LEA's. The ratio so obtained was then applied to the total population of 110 LEA's to provide an estimate for the whole of GB. Children not living in private households were excluded from this survey. Results The 33 LEA's identified 4,390 children as having some form of visual disability. Dividing this by the total number of school children in the LEA's (4,265,300) gave a prevalence rate of 10.3/10,000 children. Applying this ratio to all the 9,516,000 children in the 110 LEA's gave an estimate of 9,795. There was a large variation between LEA's in the prevalence rates. The highest reporting authority had a prevalence rate of 2.6 per 1,000, which was more than fourteen times that of the lowest at 0.18 per 1,000. There were more visually disabled girls than boys, 64% boys and 36% girls. Comment The prevalence estimates are based on information provided by 30% of the LEA's in the UK. The fact that the rates vary widely between LEA's implies that different criteria are used. No attempt was made out to identify the differences. The estimate of visually disabled children in Great Britain was less than half that estimated to have a 'seeing disability' in the OPCS report [41]. The authors conclude that the disparity was due to large-scale under-identification by the LEAs. Their estimate was also half the estimate of the survey carried out by the RNIB in 1995 (also based on LEA records) only 7 years later (see the following report). Where have all The Children Gone? An Analysis of New Statistical Data on Visual Impairment Amongst Children in England, Scotland and Wales (Clunies-Ross 1997) [43] Summary This article reports findings from a study (carried out by the RNIB) of the numbers of visually impaired (as defined by heads of visual impairment services) children aged 0-16 in England, 66 Scotland and Wales. There were over 19,000 visually impaired children in Great Britain known to the local authorities in 1995. Methods Questionnaires, each with a covering letter, were sent to Heads of all LEA visual impairment Services and also subsequently to Heads of special schools for children with visual impairment during 1995. They were asked how many children with visual impairment were known to them and to list the criteria they used to identify visually impaired children (table 5.3). The number of children with visual impairment in Great Britain was estimated by extrapolation. Table 5.3 Criteria used by Heads of visual impairment Services to identify children as visually impaired (from Clunies-Ross 1997). Criteria Percentage Visual acuity: 6/18 or less in best corrected eye 16.2 6/18 or less and significant field loss 3.9 significant visual field loss 11.9 other visual acuity criteria e.g. 3/60, 6/24, 6/60 7.9 Impaired functional vision 6.3 Vision not corrected by glasses 1.6 Named eye condition e.g. nystagmus 6.0 Degenerative eye condition e.g. RP 5.5 Temporary eye condition e.g. squint 1.2 Registered/registerable 3.5 Statement/record of need 0.8 Ophthalmological referral 1.6 Medical referral 4.7 Difficulty in accessing National Curriculum 17.8 Large print required 2.0 Mobility needs 1.6 Reference to other disabilities (not MDVI) 1.6 67 Results Information was obtained from LEAs representing 76% of the population aged less than 16 years. Table 5.3 shows the criteria that were used by the Heads of visual impairment services to identify children as visually impaired. Visual acuity and visual field were the key criteria. A few services used WHO criteria as a basis for recording children with visual impairment. The number of children aged 0-16 in GB was estimated to be 19,379.The estimated prevalence of visual impairment was 2.1 children per 1,000. The highest rate recorded by an authority was 5.06 visually impaired children per 1,000 and the lowest 0.67 per 1,000. The percentage of multidisabled children aged 0-16 was 34.5% of all children with visual impairment known to the LEA's. Comment This was a large study incorporating the whole of Great Britain. The study investigated the criteria used by the LEA's to identify children with visual impairment. However, there was no breakdown by age or sex. In addition, no attempt was made to standardise for the different criteria for visual impairment used by different authorities. Survey of educational provision for blind and partially sighted children in England, Scotland and Wales in 2002 (Keil 2003)[44] Summary A postal questionnaire of local education authorities (LEAs) carried out by RNIB in 2002. A prevalence estimate of 2.4/1000 children aged 0-16 years who received specialist educational support to enable them to access the curriculum in Great Britain was obtained. Method Postal questionnaire to LEA visual impairment advisory services in England, Scotland and Wales. The questionnaire asked about numbers of children, a detailed age breakdown and presence of other disabilities. Results The response rate was 65%. A prevalence estimate of 2.4/1000 children aged 0-16 years who received specialist educational support to enable them to access the curriculum in Great Britain was obtained, giving a population estimate of 24,000. 50% of children receiving visual impairment services had additional disabilities. Comment The marked variation in services provided and thresholds used was noted (see discussion at end of chapter below). The prevalence and nature of ascertained handicap in the National Child Development Study (1958 cohort) (Peckham and Pearson 1976) [45] 68 Summary The prevalence and causes of partial sight and blindness were investigated in 15,275 11-year-old children from the 1958 birth cohort. The prevalence of blindness was estimated to be 0.13/1000 and of partial sight 0.46/1000. Classification as blind or partially sighted was based on the descriptions used in educational and medical records. Methods 16,000 children born in a single week in 1958 were included in the National Child Development Study. By the age of 11 years, medical and/or educational data were available for 15,275. Ascertained handicaps were based on a definition of: “…any condition severe enough for the child to require formal ascertainment by the local education authority.” Children identified were thus those whose visual disability was severe enough for the child to require formal ascertainment by the local education authority. Classification as blind or partially sighted was based on the descriptions used in educational and medical records. Results The prevalence of blindness was estimated to be 1.3/10,000 and of partial sight 4.6/10,000, but these estimates were based on a total of 9 children with a notified visual handicap. Comment A large proportion (of children born in one week in 1970 were included, thus producing a representative sample of all children of that age in Great Britain. However, some underascertainment was likely to have occurred, the extent of which is difficult to quantify. Some indication of under-ascertainment can be gained by considering the following report of a birth cohort in which visual acuity was measured. Partial sight and blindness in children of the 1970-birth cohort at 10 years of age (StewartBrown and Haslum 1988)[46] Summary The prevalence of partial sight and blindness were investigated in 14,907 10-year-old children from the 1970 birth cohort. The prevalence of blindness was estimated to be between 3.4 and 4.0/10,000 and of partial sight between 5.4 and 8.7/10,000. The definitions were based on visual acuity measurements: Blindness visual acuity <6/60 and partial sight visual acuity <6/24>=6/60. Methods An estimated 97% of all children born in the week of 5th-11th April 1970 were included. Of these, 93% of the survivors were assessed in 1980. Corrected and uncorrected distance visual acuities were measured by a clinical medical officer. Detailed instructions were given to the medical officer and in most cases a Snellen chart was used. The medical officers were asked to record the presence of any abnormal condition affecting the children's eyes. Causes were ascertained by the medical officer from their own examination and a detailed examination of the child's school medical records. 69 Results Five children had best corrected visual acuity of less than 6/60. All were registered blind. One additional child who had never been ophthalmologically assessed was also included (in the upper estimate for prevalence) who was thought to be blind following measles encephalitis and 6 month of age and who attended a school for educationally severely abnormal. Eight children had best corrected visual acuity of between 6/24 and 6/60 inclusive. Only three had been registered as partially sighted and none as blind. A further three children had presenting VA <6/24 that improved to VA 6/24 after correction. Two children were reported as having refractive errors, no diagnosis was determined for the other child. These three children were included in the upper prevalence estimate of partial sight. Comment The study included a large proportion (over 90%) of children born in one week in 1970, thus producing a representative sample of all children of that age in Great Britain. Children had their vision measured. Severe visual impairment and blindness in children in the UK (Rahi et al, 2003)[47] Summary National active surveillance schemes were used to identify children newly diagnosed with severe visual impairment or blindness during 2000. The annual incidence was highest in the first year of life, being 4.0 (95% CI 3.6-4.5) per 10 000, with a cumulative incidence by 16 years of age of 5.9 (5.3-6.5) per 10 000. The study was restricted to those children with a severe visual impairment or blindness (described below) Methods In the UK, children aged younger than 16 years newly diagnosed with severe visual impairment or blindness (SVI/BL, WHO criteria) during 2000 were identified through national active surveillance schemes in ophthalmology and paediatrics. Eligible children were identified through both the British Ophthalmological and the British Paediatric Surveillance Units, whose reporting bases consist of all consultant ophthalmologists and paediatricians, respectively, participating in national active surveillance schemes. Every month clinicians reported all children younger than 16 years who were newly diagnosed as severely visually impaired or blind (SVI/BL) as a result of any disorder. Such a definition included: children with corrected distance visual acuity of worse than 6/60 in the better eye (SVI/BL by WHO international taxonomy); those eligible for notification to the national registers of blindness; those with clinical features consistent with SVI/BL (e.g. cannot fix or follow a light) but whose acuity could not be measured formally. From these data, yearly age-group specific incidence and cumulative incidence rates were calculated. Only children with permanent SVI/BL at 1 year of follow-up were included: children whose vision exceeded this level after treatment or spontaneously were not included. Children with unilateral visual loss and those born outside the UK were not included. 70 Results Of 439 newly diagnosed children, 336 (77%) had additional non-ophthalmic disorders or impairments (SVI/BL plus). Total yearly incidence was highest in the first year of life, being 4·0 (95% CI 3·6-4·5) per 10 000, with a cumulative incidence by 16 years of age of 5·9 (5·3-6·5) per 10 000. 10% (44) of all children died within 1 year of diagnosis of blindness. The main results are shown in table 5.4. Age-specific incidence Age (years) <1 1-4 5-15 0-15 Cumulative incidence Age (years) 1 5 16 Incidence per 10 000 (95% CI) 4·04 (3·56-4·52) 0·32 (0·28-0·38) 0·06 (0·04-0·08) 0·35 (0·31-0·38) 4·04 (3·56-4·52) 5·30 (4·76-5·84) 5·90 (5·33-6·47) Table 5.4 Annual age-specific incidence and cumulative incidence of SVI/BL Comment The study was a rigorously designed and executed national survey. The case definition was intended to include all children with impairment of vision sufficient to interfere significantly with development, or have major educational implications, or both, and the study thus concentrated on the severe end of the clinical spectrum. The definition was used in the absence of an existing standard definition of SVI/BL that was applicable to all children, including those too young, or who cannot participate in formal visual function tests for other reasons, such as developmental delay. The study depended on children being known to the relevant health services and on clinicians reporting newly diagnosed children. A small degree of under-ascertainment was therefore likely. Annual Schools Census (DfES 2004)[48] Summary The Department for Education and Science now collects data on every pupil in maintained schools in England. At January 2004, from a population of 7.7 million pupils in England in maintained primary, secondary and special schools, there were 7200 children with visual impairment as their primary special educational need. This gives a prevalence of 9.35/10,000 children. 71 Method Analysis of routinely collected data. Based upon survey returns from over 99% of primary, secondary and special schools in England (around 22,300). Children identified are those who have a special education need status of School Action Plus or who have a statement of special educational need. Results At January 2004, from a population of 7.7 million pupils in England in maintained primary, secondary and special schools, there were 7200 children with visual impairment as their primary special educational need. This gives a prevalence of 9.35/10,000 children. However, an additional 900 children had multi-sensory impairment, giving a prevalence of visual disability of 10.5/10,000 children. Children with visual impairment or multi-sensory impairment as their primary type of need comprised 1.3% of children with special educational need status. Comment Only data on primary type of need are so far available. Given the frequency with which visual disability occurs with other needs, it is likely that a substantial number of children with other primary special needs also have a visual disability. Data on secondary needs will be published in late 204 or early 2005. Summary tables Tables 5.5 and 5.6 below summarise the national surveys of visual impairment and visual disability among children in Great Britain 72 Table 5.5 Methods used in the national surveys of visual impairment in children Name Location Inclusion Design and Visual and /Exclusion methods measurement date of Criteria survey Great Age 15 and Cross sectional None OPCS Disability Britain under survey Survey 1985 (Bone et al.1989) [41] RNIB survey Great Aged Questionnaires sent None (Walker et al. Britain between 3-19 to random sample of 1985) [42] 1988 years. LEA’s , stratified by Excluded region and size. those not living in private households. Clunies-Ross Great Children Questionnaires sent None 1997 [43] Britain aged up to 16 to a heads of all 1995 LEA visual impairment services in England, Scotland and Wales. Keil 2003 Great Children Questionnaires sent None [44] Britain aged up to 16 to a heads of all 2002 LEA visual impairment services in England, Scotland and Wales. 73 Sample size Response rates Number Included 100,000 households 81% 2,025 children identified as disabled 37 LEA’s 33/37 LEA’s 4,390 children identified as having some form of visual disablement Not applicable “Reliable data” obtained from 76% of the LEA’s Not applicable Response rate of 65% Name Location and date of survey Great Britain 1969 Inclusion /Exclusion Criteria StewartBrown 1988 [46] Great Britain 1980 Rahi 2003[47] Great Britain 2000 England Peckam 1976[45] DfES 2004[48] Design and methods Visual measurement Sample size Response rates Number Included Birth cohort study none 95% (approx) 15,275 Children born in week one week in April 1970. Birth cohort study All notified cases Active surveillance system Corrected and uncorrected monocular distance Snellen visual acuities not applicable approx 16,000 children aged 11 years 14,907 children surveyed aged 10 years not applicable not applicable not applicable Children at maintained schools Routine data collection 7.7 million children data from over 99% of schools not applicable none 74 93% (health data), 13,871 health 85% (visual data, 12,853 acuity) visual acuity measured Table 5.6 Prevalence estimates obtained from the surveys of visual impairment in children Survey What the prevalence estimate refers to OPCS Disability Survey (Bone et al.1989) [41] RNIB survey (Walker et al. 1985) [42] Clunies-Ross 1997 [43] Keil 2003 [44] Peckam 1976[45] Stewart-Brown 1988 [46] Cannot see well enough to recognise things in a picture book or cannot see well enough to follow a TV programme sitting at a normal distance to the TV set or cannot see well enough to recognise someone across a road. Identified by LEA as having a visual handicap, i.e. “educationally blind” or “partially sighted” Criteria as used by heads of services for visually impaired children to identify visually impaired children Criteria as used by heads of services for visually impaired children to identify visually impaired children Visual handicap severe enough for the child to require formal ascertainment by the local education authority. Classification as blind or partially sighted based on the descriptions used in educational and medical records Blindness: visual acuity <6/60 Age 0-15 years Prevalence estimate /10,000 20 3-19 years 10.3 0-16 years 21 0-16 years 24 11 years 1.3 (blindness) 4.6 (partial sight) 10 years Partial sight: visual acuity <6/24>=6/60 Rahi 2003[47] DfES 2004[48] Corrected distance visual acuity of worse than 6/60 in the better eye; those eligible for notification to the national registers of blindness; and those with clinical features consistent with severe visual impairment or blindness Children with visual impairment or multi-sensory impairment as their primary special educational need 75 3.4 (blindness) 5.4 (partial sight) Cumulative incidence by age 16 years 5.9 All school ages 10.5 Locally based surveys There have been a number of estimates of visual impairment in geographically defined populations in the United Kingdom. The main characteristics and findings of the larger and more rigorous studies are presented in table 5.7. The Flanagan study is notable because it comes from Northern Ireland: the national surveys presented above were all restricted to Great Britain. These studies have used a range of methods, sources, and definitions, outcome measures, limiting the scope to generate a summary estimate. However, the findings are broadly similar to the national surveys of visual impairment, with prevalence estimates around 10-20/10,000 children. While taking these caveats into account, the estimate from Northern Ireland (Flanagan) appears similar to estimates from the rest of the United Kingdom. 76 Table 5.7. Characteristics and findings of surveys in geographically defined populations Study and Setting Method Main findings year Crofts 1998 Berkshire, Bucks, Children identified as Visual acuity 6/18 or poor [49] Oxfordshire and visually impaired from the behavioural responses, born Northamptonshire Oxford Register of Early 1984-1987 and diagnosed by Childhood Impairment age 5 years, 10.3/10,000 Rogers Liverpool Children identified as Corrected vision sufficiently 1996[50] visually impaired from the abnormal to interfere with Liverpool vision development or to have assessment team database ongoing education implications in children aged 0-16 years, 18.1/10,000. Flanagan Belfast Children identified as Best-corrected visual acuity 2003 [51] having visual impairment 6/18 in the better eye or from multiple sources significant decrease in visual including paediatricians, field size, ages 0-18 years, teachers, social workers 16.1/10,000 and statutory registers, visual acuity and fields measured Visual Scotland Information sent to all Rates not presented and Impairment heads of special education cannot be calculated as no Scotland services in each local denominators given. 2003 [52] authority plus to community paediatricians 333 children met criteria for asking them to identify “significant visual possible children and impairment” (see text for disseminate information on details). the project to families. Notification was by parents. Welsh Wales Audit of LEA visual Among people aged 0-19 Assembly impairment services years, 20/10,000 people Government received specialist support 2004 [53] from visual impairment services 77 Overall comments Definitions used A key issue is the variation in definitions used for visual impairment and in the criteria used by local education authorities to identify children in need of services. One survey asked visual impairment services how they identified visually impaired children and multi-disabled visually impaired children. The criteria are described in tables 5.8 and 5.9 below. Table 5.8: criteria used by visual impairment services to identify a visually impaired child from a sample of 152 providers (Clunies-Ross 1997)[43] A child who is ‘educationally significantly visually impaired’. Generally this means children with a visual acuity of 6/18 or less in the best correct eye. 6% Visual acuity of 6/18 or less and/or restricted visual fields. 4% A child who experiences difficulties in gaining access to the National Curriculum due to impaired vision. This includes children with visual acuity of 6/18 or less in the best corrected eye, also significant field loss. Combination of factors, including named eye condition, prognosis, visual acuity and field of vision. Criteria are as much decided by functional vision as by clinical assessment of vision. 14% 74% Other 2% 100% Table 5.9: criteria used by visual impairment services to identify a multi-disabled visually impaired child from a sample of 152 providers (Clunies-Ross 1997)[43] Any child who has significant visual impairment with additional or multiple difficulties. Children with visual impairment who have additional handicaps which combine to cause severe learning difficulties, including profound and multiple difficulties. Children with multiple disabilities including visual impairment who are not able to benefit from education in mainstream. Pupils with a visual impairment who have a major additional physical/medical/emotional/behavioural/learning difficulty, normally falling into the SLD or PMLD range. Other 28% 20% 13% 38% 1% 100% 78 The variation in definitions and policies was highlighted in the recent report from Wales (summarised in table 5. 7 above) carried out by the Welsh Assembly Government in 2003. This report noted that “…there are considerable differences in policies for referrals across the 22 Welsh LEAs.” and that “In some areas the service for visually impaired children and young people has included children and young people with a slight reduction in visual acuity who may only be seen by them twice-yearly or annually. In other areas, these children/young people would not meet the descriptors for intervention.” [53]. The Visual Impairment Scotland project [52]used a modified version of a visual impairment classification system first developed in Scandinavia, called the NORDSYN system [54]. The target population was “children with significant visual impairment” under the age of 16 years who had any of: best corrected binocular acuity equal to or worse than 6/18 any form of visual field loss an eye movement disorder which affects visual function any form of cognitive visual dysfunction due to disorders of the vision parts of the brain. These definitions were chosen because they were felt to represent thresholds of relevance to the educational and developmental needs of children. Multiple disability A consistent finding has been that a substantial proportion of children with visual impairment have additional disabilities/needs. The 2002 RNIB survey of LEA visual impairment services [44] found that around half of children with visual impairment had additional disabilities. In the Visual Impairment Scotland project, 57.1% of children identified as having “significant visual impairment” were found to have another disability in addition to a visual problem [52]. The Thirty per cent were classified as having severe or profound and multiple learning difficulties in addition to a visual impairment, while the remaining 20% had additional disabilities excluding severe or profound learning difficulties. In the study by Rahi et al[47] ; 77% of children newly diagnosed with severe visual impairment or blindness had additional non-ophthalmic disorders or impairments. A re-analysis of the 1989 OPCS child disability survey used cluster analysis to group together the children into different groups or clusters according to shared characteristics, with the aim of taking into account and “make(ing) more visible the type, severity and combination of all the disabilities experienced by a child” [55]. The study showed that children were likely to either have a mild to moderate visual impairment with few other disabilities, or to have visual impairments of a more severe nature, along with several other disabilities also of a severe or profound nature. Summary This chapter summarises the literature relating to the prevalence of visual impairment and visual disability in children in the UK. Most of the available data about visual loss in children comes from registers or from surveys of providers of health care, social care or educational services to children with visual loss. Thus the available estimates rely on children with visual loss being known to the relevant services. This may be a reasonable assumption for children, because substantial visual loss is very likely to be detected, particularly at school. 79 Because of the variation in definitions and service provisions, great caution is required in interpretation of any single estimate of the prevalence of visual impairment or blindness among children in the UK. However, using a broad and pragmatic definition of visual loss sufficiently bad as to mean a child is identified as being in need of special educational or social services, the existing data suggest a prevalence of visual impairment in the region of 10-20/10,000 children. For severe visual loss, the estimates from the study by Rahi et al are likely to be much the most reliable. In this study, the cumulative incidence of blindness or severe visual impairment by the age of 16 years was estimated to be 5.9/10,000 children. The term “cumulative incidence” is correctly used because the data were not derived from a true prevalence survey, but can be interpreted as similar to prevalence at the age of 16 years. Around half the children receiving support from visual impairment services may have additional disabilities, and this proportion may be even higher for children with severe visual loss. 80 Chapter 6 Visual acuity and vision related quality of life 81 Introduction Visual acuity is a good indication of the degree of vision loss, but may not reflect an individual’s own perception of how vision affects their everyday life, from the ability to perform every day tasks or the psychological and social consequences of reduced vision. A number of questionnaires have been developed, primarily in the US, to measure visual function / vision related quality of life [56]. Only two scales- the National Eye Institute Visual Function Questionnaire (NEI-VFQ) [57] and the Indian Vision Function Questionnaire (IND-VFQ) [58] were developed from patient elicited problem statements collected from focus groups, in contrast to other scales developed from clinical judgement. The need for a specific measure of visual function led to the development of A 51-item questionnaire was originally devised in the US from focus groups of people with major causes of eye disease The NEI 51-item original questionnaire was later shortened to 25 items, based predominantly on the responses from those with eye disease and visual impairment, and also from a minority group without eye disease [59]. The NEI-VFQ 25 has been used in used to show that those with age-related macular disease [60], glaucoma [61], optic neuritis [62], diabetes mellitus [63], central retinal vein occlusion [64], subfoveal choroidal neovascularisation and accompanying visual impairment [65] have lower scores compared to a reference group without ocular disease or visual impairment. This questionnaire has also been used to show the longitudinal benefit of vision rehabilitation amongst a group without correctable visual impairment.[66, 67] Despite some concerns about the range of measurement obtained with the NEI-VFQ [68], it has also been used in adult populations (aged 40 years or more) to show that those with visual impairment have lower scores compared to those without reduced visual acuity [69, 70]. Use of the NEI VFQ in non US populations is more limited especially among the older population who are likely to experience higher levels of visual difficulties than younger age groups. To our knowledge there are no published vision function data from a population based UK sample. A nested trial within the MRC Elderly Trial permitted the possibility of collecting these data. Full details of the nested trial design and results have been published elsewhere [71] . Methods Surviving participants in 20 randomly selected general practices from each arm of the main trial were invited to have an assessment of their vision and complete the 25-item NEI-VFQ. Research nurses measured presenting monocular and binocular visual acuity (defined as using their habitual distance correction) on the LogMAR scale using Glasgow acuity charts [11]. NEI-VFQ questions are grouped in 12 sub-scales ( general health, general vision, ocular pain, near activities, distance activities, social functioning, mental health, role difficulties, dependency, driving, colour vision and peripheral vision), as well as a combined total score (Table 6.1). We followed the NEI VFQ scoring method. Each sub-scale was assigned a score from 0 to 100, where 0 is the worst and 100 represent no disability related to vision (that is, ratings of excellent or no difficulty). 2589 people were invited of whom 1807 participated (69.8%), 670 refused (25.9%) and 112 (4.3%) were too ill. The mean age of participants was 83 years (ranging from 77 to 101 years); and the majority were female (64%). Complete data, including a measure of visual acuity and a completed NEI-VFQ, were available for 1745 participants. The prevalence of presenting visual acuity less than 6/12 in the better eye was 31% (n=545/1745), and 12% (n=203/1745) for visual 82 impairment (acuity less than 6/18 in the better eye). The cause of visual impairment was only available for a minority, and hence is not considered further. With the exception of general health, few respondents reported at the extreme ends of the scales in the NEI-VFQ subscales. For this reason responses were categorised into “no problems” or “any problems” for all scales except for General Health and the Total score. The proportions are shown in the second column of Table 6.2. For General Health only 8% reported no problems and 30% reported having poor health. In contrast, for general vision 68% reported having good to excellent eyesight. The percentage reporting problems for the other scales (ranked by highest proportion of reporting problems was: 53% for near activities, 51% with distance activities, 45% for driving, 45% for ocular pain, 46% mental health, 41% difficulties in carrying out roles, 25% peripheral vision, 22% reported some level of dependency, 20% had some problems in social functions, and 10% with colour vision. For the overall VFQ score, only 25% scored 100 i.e. no problem on any of the sub-scales; and at the top end 25% had high scores. The third column of Table 6.2 shows the proportion with visual acuity <6/12 in each problem category for each of the sub-scales and overall scale and the fifth columns gives the proportion for VA <618. For example in the General Vision scale 59% of those reporting problems had a VA <6/12 compared with 20% with VA<6/12 in those who reported no general vision problems. For VA <6/18 the differences are greater, i.e. 33% of those reporting problems on the General Vision scale have VA <6/18 compared with only 4% in those who report no problems in general vision. Columns 4 and 6 present the comparisons between the proportions with poor visual acuity according to whether they have problems or not on the sub-scales. The analyses are given as odds ratios (ORs) and in all the comparisons the effects of age and gender were taken into account. The OR for General Vision is 5.75 for VA <6/12 and 11 for VA <6/18 i.e. there is a five fold chance of having VA <6/12 for people who reported problems on the General Vision sub-scale and an eleven fold chance of having VA <6/18. The P-value shows that this result is highly statistically significant (unlikely to have occurred by chance). Significantly increased ORs were seen for all sub-scales except ocular pain. Another way of reporting the results is shown in the last two columns of the table. The mean LogMAR score and the equivalent level of Snellen chart acuity is presented according to the reporting of problems. Because sub-scales are correlated with each other i.e. a person who reports problems on one subscale is likely also to report problems on another scale, further analyses investigating which of the sub-scales was the most important in terms of vision impairment was carried out. The results showed that difficulties with general vision, near activities, and social functioning remained strongly associated with visual impairment. Difficulties with dependency and colour vision were of borderline significance. A combined score was derived from the average of these sub-scales. Although visual acuity is clearly strongly associated with vision function we investigated how much of the combined score was accounted for by visual acuity. If there was a perfect correlation for visual acuity with vision function, the variation in the score accounted for by visual acuity would be 100%. Our results showed that 20% of the combined score was explained by visual acuity, and only an additional 4% by age and gender and area of residence. Measures of deprivation were not related to the scores. We do not know what other factors contribute to the variation in the score. It is likely that psychological attributes such as coping strategies, or being a pessimistic or optimistic type of person may influence the way in which people with the same levels of visual acuity report their general vision function. For example, of 242 people with VA <6/18, 50 (21%) reported no problems with their General Vision. For specific problems such as Near Activities the proportion was much lower, with only 27 (11%) of those with VA 83 <6/18 reporting no problems. We used visual acuity alone as a “clinical” measure. Although useful in population vision testing, visual acuity is a relatively limited measure of vision performance and it is possible that inclusion of a broader spectrum of tests, such as contrast sensitivity, colour vision and assessment of the visual field would provide a more comprehensive picture. Chapter Summary In a general population sample of elderly people (mean age 83), the prevalence of presenting visual acuity less than 6/12 in the better eye was 33% and 14% (n=243/1785) had acuity less than 6/18 in the better eye). Using the NEI-VFQ 25, 68% reported their vision was excellent or good and only 32% reported their vision as fair or poor. Around half of the reported problems were with near or distance activities. Visual acuity levels were strongly associated with all subscales except ocular pain. The most important scales related to visual acuity were general vision, near activities, and social functioning and, to a lesser extent, dependency and colour vision. However visual acuity only explained about a fifth of the variation between people in their reporting on these scales. Of concern were the 21% of visually impaired people reporting no problems with vision although this proportion was lower when considering specific activities. We conclude that NEI-VFQ scores should be considered as an additional measure of visual disability and not as a substitute for visual acuity. 84 Table 6.1 NEI VFQ 25 Questions and sub-scale scores NEI-VFQ sub-scale Number of questions used to derive sub-scale score 1 1 2 3 NEI-VFQ question numbers used Distance activities 3 8,9,14 Vision specific: Social functioning Mental health 2 4 11,13 3,21,22,25 2 3 3 1 1 17,18 20,23,24 15c,16 12 10 All General health General vision Ocular pain Near activities Role difficulties Dependency Driving Colour vision Peripheral vision Total VFQ score 1 2 4,19 5,6,7 Questions asked Perception of overall health (5 levels) Perception of eyesight (6 levels) Pain and discomfort in and around the eyes and the degree of ocular pain Difficulty reading ordinary print in newspapers, performing work or hobbies requiring near vision, and finding something on a crowded shelf Difficulty reading street signs or names of shops, going down steps, stairs or kerbs in poor light and visiting people in unfamiliar surroundings Difficulty seeing how people react and visiting people in unfamiliar surroundings Worries and frustration about eyesight, embarrassment and loss of control caused by eyesight Lack of accomplishment and limitations caused by eyesight Need to stay at home, reliance on others, and need of help Difficulty driving during the daytime and at night Difficulty picking out and matching clothes Difficulty noticing objects off to the side whilst walking A total score averaged for the subscale scores listed above 85 Table 6.2 NEI-VFQ 25 scores and association with visual acuity NEI VFQ subscales Responses by Number (%) with OR VA<6/12 (95% Number (%) with OR VA<6/18 (95% category VA<6/12 in each CI) VA<6/18 in each CI) N (%) category of NEI- category of NEI- VFQ subscale VFQ subscale Mean logMAR Snellen equivalent General health No problems 142 (8) 41 (29) 1.00 16 (11) 1.00 0.22 (0.18, 0.26) 6/10 Few problems 493 (28) 129 (26) 0.78 (0.50, 1.22) 44 (9) 0.68 (0.36, 1.29) 0.20 (0.18, 0.22) 6/10 Moderate health 614 (34) 198 (32) 1.03 (0.67, 1.59) 91 (15) 1.16 (0.64, 2.11) 0.23 (0.21, 0.25) 6/10 Poor health 534 (30) 216 (40) 1.43 (0.93, 2.22) 91 (17) 1.25 (0.68, 2.28) 0.26 (0.24, 0.28) 6/11 Total 1783 584 (33) P-value † 242 (14) <0.001 1744 0.018 0.001 General vision No problems 1206 (68) 244 (20) 1.00 50 (4) 1.00 0.16 (0.15, 0.17) 6/9 Problems 577 (32) 339 (59) 5.75 (4.53, 7.31) 192 (33) 11.0 (7.72, 15.5) 0.37 (0.35, 0.39) 6/14 Total 1783 583 (33) P-value 242 (14) <0.001 1744 <0.001 <0.001 Ocular pain No problems 982 (55) 316 (32) 1.00 120 (12) 1.00 0.23 (0.21, 0.24) 6/10 Problems 801 (45) 267 (33) 1.04 (0.83, 1.29) 122 (15) 1.22 (0.91, 1.64) 0.23 (0.21, 0.24) 6/10 Total 1783 583 (33) P-value 242 (14) 0.751 1744 0.176 0.891 Near activities No problems 838 (47) 156 (19) 1.00 27 (3) 1.00 0.16 (0.14, 0.17) 6/9 Problems 940 (53) 422 (45) 3.48 (2.75, 4.40) 213 (23) 8.35 (5.44, 12.8) 0.29 (0.28, 0.31) 6/12 86 Total 1778 540 (31) P-value 240 (14) <0.001 1740 <0.001 <0.001 Distance activities No problems 839 (50) 185 (22) 1.00 40 (5) 1.00 0.18 (0.16, 0.19) 6/9 Problems 856 (51) 339 (40) 2.11 (1.67, 2.66) 178 (21) 4.91 (3.37, 7.14) 0.26 (0.25, 0.28) 6/11 Total 1695 524 (31) P-value 218 (13) <0.001 1658 <0.001 <0.001 Social function No problems 1420 (80) 357 (28) 1.00 95 (7) 1.00 0.19 (0.18, 0.20) 6/9 Problems 355 (20) 219 (62) 4.71 (3.60, 6.16) 145 (41) 9.38 (6.81, 12.9) 0.39 (0.37, 0.42) 6/15 Total 1775 576 (32) P-value 240 (14) <0.001 1736 <0.001 <0.001 Mental health No problems 954 (54) 218 (23) 1.00 56 (6) 1.00 0.18 (0.17, 0.19) 6/9 Problems 829 (46) 365 (44) 2.54 (2.03, 3.17) 186 (22) 4.46 (3.20, 6.23) 0.29 (0.27, 0.30) 6/12 Total 1783 583 (33) P-value 242 (14) <0.001 1744 <0.001 <0.001 Role difficulties No problems 1058 (60) 246 (23) 1.00 52 (5) 1.00 0.18 (0.16, 0.19) 6/9 Problems 721 (41) 33 (46) 2.79 (2.23, 3.49) 188 (26) 6.77 (4.81, 9.55) 0.30 (0.29, 0.32) 6/12 Total 1779 579 (33) P-value 240 (13) <0.001 1740 <0.001 <0.001 Dependency No problems 1381 (78) 335 (24) 1.00 91 (7) 1.00 0.19 (0.17, 0.20) 6/9 Problems 400 (22) 246 (64) 4.80 (3.70, 6.24) 150 (38) 7.45 (5.44, 10.2) 0.38 (0.36, 0.40) 6/14 Total 1781 581 (33) 241 (14) 87 1742 P-value <0.001 <0.001 <0.001 Driving * No problems 299 (55) 29 (10) 1.00 3 (1) 1.00 0.11 (0.08, 0.13) 6/8 Problems 246 (45) 79 (32) 4.63 (2.81, 7.62) 38 (15) 24.5 (6.57, 91.1) 0.21 (0.18, 0.23) 6/10 Total 545 108 (20) P-value 41 (8) <0.001 534 <0.001 <0.001 Colour vision No problems 1578 (90) 445 (28) 1.00 146 (9) 1.00 0.20 (0.19, 0.21) 6/10 Problems 178 (10) 121 (68) 5.39 (3.74, 7.78) 89 (38) 9.86 (6.77, 14.3) 0.45 (0.41, 0.49) 6/17 Total 1756 566 (32) P-value 235 (13) <0.001 1718 <0.001 <0.001 Peripheral vision No problems 1300 (75) 326 (25) 1.00 94 (7) 1.00 0.19 (0.18, 0.20) 6/9 Problems 440 (25) 227 (52) 3.02 (2.37, 3.87) 95 (24) 5.03 (3.68, 6.87) 0.32 (0.30, 0.34) 6/13 Total 1740 553 (32) P-value 189 (11) <0.001 1703 <0.001 <0.001 Total VFQ score No problems 442 (25) 75 (17) 1.00 12 (3) 1.00 0.16 (0.13, 0.18) 6/9 Few problems 447 (26) 103 (23) 1.45 (1.02, 2.07) 21 (5) 1.72 (0.82, 3.58) 0.18 (0.16, 0.20) 6/9 Moderate vision 456 (26) 136 (30) 2.01 (1.43, 2.83) 41 (9) 3.37 (1.72, 6.60) 0.21 (0.19, 0.23) 6/10 Poor vision 438 (25) 269 (61) 6.93 (4.93, 9.75) 168 (38) 19.5 (10.5, 36.5) 0.39 (0.37, 0.41) 6/15 Total 1783 583 (33) P-value 242 (14) <0.001 1744 <0.001 <0.001 1.00 0.16 (0.13, 0.18) Total VFQ score No problems 442 (25) 75 (17) 1.00 12 (3) 88 6/9 Few 447 (26) 103 (23) 1.47 (1.03, 2.09) 21 (5) 1.78 (0.85, 3.71) 0.18 (0.16, 0.20) 6/9 Moderate 456 (26) 136 (30) 2.02 (1.43, 2.85) 41 (9) 3.42 (1.74, 6.72) 0.21 (0.19, 0.23) 6/10 Lots 399 (23) 230 (58) 5.93 (4.20, 8.38) 129 (32) 15.1 (8.04, 28.5) 0.39 (0.37, 0.41) 6/15 Total 1744 544 (31) <0.001 <0.001 P-value † 203 (12) <0.001 89 Chapter 7 Conclusions and recommendations In this chapter we summarise the evidence relating to prevalence estimates, discuss how the estimates relate to registration data and identify gaps in the knowledge base where further research is required. As described in Chapter 1 the methods of measuring visual problems use two different approaches: self reported visual difficulties (reviewed in Chapter 2) and clinical measures of visual acuity (reviewed in Chapter 3). Prevalence of visual difficulties The estimates of visual difficulties (described as visual disability in some studies) derive predominantly from large government surveys and show, when using similar survey methods and criteria for visual disability, (as in the OPCS surveys of 1985 [25]and 1996/7 [26]) some consistency in the results in the older population: 22% of the over 75s in private households reported difficulties with reading newsprint or worse and 26% when people in communal establishments were included. There was less consistency in the results for the younger age groups where the two surveys differed over 2 fold in their estimates for the population aged 1664 from 0.8% to 2.0 %. If the proportion of the younger population with visual difficulties is over estimated this will substantially inflate the numbers with sight difficulties in the population since the numbers of people in the population aged 16-64 is much greater than in the older age groups. Thus the estimated numbers with sight difficulties in private households in England and Wales based on the 1996/7 [26] survey can be estimated at nearly 2 million compared to 1.4 million from the 1985 survey[25]. There are doubts concerning the reliability of all estimates based on the criteria of “difficulties with reading newsprint” or worse. The lack of reliability is based on findings from the OPCS/RNIB 1998/1999 survey [27] . The sample for this study came from a re- survey of respondents who had reported sight difficulties in the 1996/7 survey quoted above and in the Omnibus survey. A substantial proportion of respondents who initially self reported with a sight problem on re-survey denied they had had a sight problem. The main change in response was to the questions: “Difficulty in seeing a friend across the road” and “Difficulty reading ordinary newsprint”. With more severe task difficulties the level of misclassification was minimal. The estimates of visual disability adjusted for misreporting in the OPCS/RNIB 1998/1999 study. were considerably lower than either of the two previous surveys with a prevalence for difficulties with reading newsprint or worse of 14% for the over 75s and 1.1% for the 16-59 age group. Estimates from OPCS/RNIB 1998/1999 study may also be too low because some people who initially had a problem had subsequently received treatment. Confidence in the results is further limited by the lack of detailed information on response rates especially in the government surveys. The government surveys on disability used a “sift” approach to screen out people with no apparent disability with successive reductions in response with successive sifting. Although the final response rates in the sample from whom the estimates 90 are derived are not clearly presented they are of the order of 50% or less in most government surveys. The representativeness of the surveyed population is therefore difficult to assess. We advise against the use of data on self reported sight problems to estimate the levels of visual impairment in the population. Prevalence of visual impairment Studies using visual acuity measurements have used various criteria for definitions and cut points of visual impairment. The results from two studies: National Diet and Nutrition Study (NDNS), and MRC Assessment Trial that were nationally representative of the older population and use uncorrected presenting VA and similar cut points are given in the table below (unpublished data from NDNS provided by Dr van der Pols and unpublished data on VA <6/12 for MRC Assessment Trial using same LogMar criteria as NDNS). 65-74 NDNS community sample1 VA <6/18 VA<6/12 MRC Assessment Trial2 VA <6/18 VA<6/12 475 5.6 15.8 Age group not included 95% CI 75-84 95%CI 429 13.3 28.3 3.5, 7.6 12.6, 19.1 11500 8.5 18.7 85+ 95% CI 10.1, 16.5 24.1, 32.6 222 31.7 54.0 25.5, 37.8 47.4, 60.6 7.1, 9.8 16.5, 20.9 3100 26.8 45.8 23.9, 29.7 42.2, 49.5 1 Best score (Glasgow Acuity Cards) of two eyes without pinhole correction 2 Binocular acuity without pinhole correction These results show that the point prevalence estimates of vision impairment (VA <6/18) are : 6% NDNS only) at ages 65-74, 8% to 13% at ages 75-84 and 27% to 32% at ages 85+. Estimates of the prevalence of minor visual loss (visual acuity <6/12) are 16% (NDNS only) at ages 65-74, between 19% to 28% at ages 75-84 and 46% to 54% at ages 85+. Considering the upper and low bounds of the 95% confidence intervals the results show that the estimates of vision impairment (VA <6/18) range from 4 to 8 % (NDNS only) at ages 65-74, 7% to 16% at ages 75-84 and 24% to 38% at ages 85+. Similarly the range of estimates of the prevalence of minor visual loss (visual acuity <6/12) are from 13% to 19% (NDNS only) at ages 65-74, between 16% to 33% at ages 75-84 and 42% to 61% at ages 85+. Estimates for the nursing home population from NDNS show high levels of vision impairment (VA <6/18): 12.1% at ages 65-74 (95% CI 9.7%, 23.2%), 30.0% of those aged 75-84 (95% CI 20.5%, 39.5%) and 46.9% of those aged 85+ (95% CI 37.7%, 56.1%). However as these are the only recent estimates available for the nursing home population we recommend that they are viewed with some caution. 91 Two studies provided estimates of blindness using international criteria of VA < 3/60. In the MRC assessment trial the estimates for the 75+ age group were 2.1 (95% CI 1.8, 2.4) and in a small study in London the estimates for blindness were very similar (1.9%) although the confidence intervals were very wide (0.2, 6.6) Information on visual impairment alone is only partially useful and is enhanced by knowledge of the causes of vision impairment. Similarly if the focus of interest is in identifying people who could benefit from services and treatments, measures of vision impairment alone are inadequate. In Chapter 4 we reviewed the few UK studies which have provided some information on the causes of vision impairment. Prevalence estimates of different eye diseases/conditions differed between studies because of differences in the visual acuity cut points in the studies e.g. <6/12 in North London Study[33], <6/18 in the MRC Assessment Trial [39] and differ also in the age range, 65+ in the North London Study and 75+ in the MRC Trial. All studies highlighted untreated refractive error and cataracts as major remediable causes of vision impairment in older people ranging from 70% to 50% as a proportion of visual impairment. With increasing age the proportion of treatable vision impairment declines as age related macular degeneration becomes more prevalent. In the UK studies, consistently higher estimates of poor visual acuity were reported for women compared to men. This reflected higher prevalence rates for untreated cataracts[13, 33]and for age related macular degeneration[39]. The seven country EUREYE study reported higher rates of vision impairment and for age related macular degeneration in women compared with men [72]. A pooled analysis of studies conducted mainly in the US found that women were 30% more likely to have VA < 6/12 compared with men of the same age [73]. Gender differences in the prevalence of vision impairment in the UK may reflect lower access to services and aetiological factors for age related macular degeneration. In the North London Study, a higher prevalence of refractive errors and cataracts in people was found for those living in the more deprived areas. What proportion of the visually impaired population eligible for registration are unregistered? The RNIB/ONS 1990 report [37] raised concerns that a large proportion of the visually impaired population were not accessing services and support via the registration system. As the results for visual impairment from that report were based on sight tests alone without excluding possible remediable conditions (such as refractive error and cataracts) the registerable component is likely to be overestimated by around two fold. We showed that, based on other studies which have collected data on the causes of vision impairment the numbers likely to be registered because of permanent vision loss, and those registered were of a similar magnitude (Table 4.5). Even if we consider that some of the prevalence estimates of vision impairment may be biased towards the low side, and therefore there is some under reporting, it is extremely unlikely that it is of the order of magnitude suggested by the RNIB/ONS 1990 estimates. For example using data from the MRC Assessment trial we estimate that around 237000 aged over 75 were likely to have visual impairment eligible for registration. Comparing this with the actual figures from the DOH of 211000 registered suggest that approximately 10% of the over 75s may not be registered. If we take the lower figure from the 95% confidence interval of 207,000 then the registration numbers are slightly higher than those we estimate and if we take the upper confidence interval the extent of under registration is 20%. 92 International data also provide some reassurance that the prevalence of registerable vision in the UK is similar to that expected from the population studies. In a recent pooling of studies predominantly from the USA [73] the prevalence of blindness based on best corrected VA <3/60 was very similar to the percent prevalence for registration figures for England in the comparable age groups (as shown in Table 4.4). Estimates of registerable visual impairment due to age related macular degeneration in the UK also suggest good agreement between predictions and observations [74, 75]. Owen at al [74] pooled the data from international studies to provide age specific prevalence rates for visually impairing age related macular degeneration and applied these rates to the UK population to obtain expected numbers of those eligible for registration. The estimated numbers were 214,000 (95% CI 151,000 to 310,000) with visual impairment caused by AMD (visual acuity 6/18 or worse). Evans et al using prevalence rates for AMD from the MRC Assessment Trial[75] estimated the numbers as slightly lower at 192,000, 95% CI 144,000 to 239,000). There was a small difference in the definition of visual impairment (<=6/18 in Owen and <6/18 in Evans). We conclude that, although registration rates may show some under ascertainment in the older age groups, the evidence does not support substantial under-reporting. Gaps in evidence Most studies have been done in the older population and there is a scarcity of data in younger adult age groups in the UK. A review by Nissen et al[76] of epidemiological studies performed in Western Europe, North America and Australia covering the age group 20 to 59 years found the prevalence of blindness was 0.08 and of visual acuity 6/24 to 6/48 was 0.07%. These figures agree well with the prevalence of registrations in a similar age range and we conclude that registration data provide reasonably accurate estimates of the prevalence of serious vision impairment in the younger adult age groups. Information is lacking on less severe levels of visual impairment. For children, agreed criteria to define visual disability, visual impairment and the need for specialist support are needed. The needs of children with visual disability who also have other disabilities should also be a priority. There are very little data on vision impairment in different ethnic groups in the UK population. Two small studies attempted to examine ethnic differences (Asian) in the prevalence of registerable blindness/partial sight [36] or cataracts [38]. These studies suggested that rates might be higher in Asian groups. The OPCS/RNIB 2000 [27]report also examined prevalence rates by responses to the sift questions on seeing difficulty for a variety of ethnic groups and found that the highest levels were in Black Caribbean populations with low rates for Asians. At present the data are too sparse and unreliable to comment on the prevalence of visual impairment or specific types of eye disease in different ethnic groups. The reasons for higher levels of vision impairment in women requires further understanding, in particular the extent to which this reflects under utilisation of services. The reasons for high levels of treatable conditions in the older population requires further investigation. Some indications of possible barriers was provided by our randomised trial of 93 screening visual acuity by a practice nurse [71]. Although visual impairment was common, few people benefited from subsequent intervention, and screening did not reduce levels of visual impairment. Key explanations for the lack of effect identified were under-detection of uncorrected refractive error and that only around half the recommendations for referral to an ophthalmologist resulted in referral by the general practitioners. In addition participants themselves reported an unwillingness to self-refer to optometry services for further assessment, citing fear of costs and lack of perceived need. Recommendations Policy The estimates provided from the studies of visual acuity for the older population are sufficiently consistent for general purposes of planning and estimating the numbers of people in the UK with vision impairment. However we caution that these estimates are seen as approximations and not as “tablets of stone” as prevalence estimates will vary from place to place and over time and because all estimates carry a range of uncertainty (as expressed by the 95% confidence interval). Studies in the older population have also consistently shown that about 50% of visual impairment is due to treatable conditions i.e. cataract and refractive error. This proportion diminishes with increasing age due to the higher prevalence of age related macular degeneration as a cause of vision impairment. Increased awareness of these facts is important for agencies dealing with visually impaired people. Appropriate action e.g. media campaigns and advocacy is required to ensure that both eye care providers and older people themselves are aware of these conditions and of the current unacceptably high levels of untreated conditions. Strategies to identify the most cost effective way of targeting the older population, including novel approaches to screening older people, are urgently needed Standards for Reporting and Measurement We have shown the considerable variation in definitions and cut points used in the UK based studies. This applies even more at the international level especially when comparing data with the US where very different definitions on blindness and low vision are used. A recent WHO Informal Consultation Working Group [6] has made recommendations for measuring acuity and it is hoped that this will go some way to improving the consistency of reporting across studies. The Working Group recommended that vision assessment in population-based studies should include a measurement of visual acuity using LogMAR charts at distance and near under standardized conditions. Information collected should record: (i) monocular and binocular distance presenting visual acuity, whether a method of vision correction is used (e.g. spectacles) and, if so, the type and power of vision correction device; (ii) monocular and binocular near presenting visual acuity at 40 cm, whether a method of vision correction is used (e.g. spectacles) and, if so, the type and power of vision correction device; (iii) monocular and binocular bestcorrected visual acuity at distance and near, following refraction using an age-appropriate addition for near acuity. Few UK studies have used best corrected visual acuity largely because of the extra resources required to collect these data. Presenting binocular vision impairment 94 probably represents the measurement of vision most closely related to vision experienced by the individual. However, an additional measurement of best corrected visual acuity would clearly identify the level of refractive error and the remaining vision loss due to eye diseases. The Working Group also suggested that revisions should be made to the categorisation of visual acuity as in ICD-10 (Table 7.1). The categories should be based on presenting (not best corrected vision as currently applies). We recommend the use of validated questionnaires or scales for measuring self reported vision problems or vision related quality of life. We emphasize the need to thoroughly test all questions before use in surveys. There was a substantial lack of clarity and detail in some of the reports that we reviewed. We recommend that reports which present novel research findings (but are not submitted for publication in academic journals) should conform to the same standards of reporting as the formal peer review process of academic journals; for example the guidelines of the International Committee of Medical Journal Editors [77] (www.icmje.org). 95 Table 7.1 Recommendations for categorisation of visual acuity [6] Category Presenting distance visual acuity Worse than: Equal to or better than: Mild or no visual impairment 0 Moderate visual impairment 1 6/18 3/10 (0.3) 6/19 3.2/10 (0.3) 20/63 6/60 1/10 (0.1) 20/200 Severe visual impairment 2 6/60 1/10 (0.1) 20/200 3/60 1/20 (0.05) 20/400 Blindness 3 3/60 1/20 (0.05) 20/400 1/60* 1/50 (0.02) 5/300 (20/1200) Blindness 4 1/60* 1/50 (0.02) 5/300 (20/1200) Light perception Blindness 5 No light perception 96 References 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. 18. 19. 20. 21. 22. Colebrander A. Visual standards: aspects and ranges of vision loss with emphasis on population surveys. Report prepared for the International Council of Ophthalmology. in 29th International Congress of Ophthalmology. 2002. Sydney, Australia. International Classification of Impairments, Disabilities and Handicaps (ICIDH-80). 1980, World Health Organization: Geneva. Health Survey for England. Disability among older people. Technical report. 2000, Department of Health: London. Health Survey for England. Disability. Technical report. 2001 Department of Health. London English Longitudinal Study on Ageing. http://www.ifs.org.uk/elsa/report03/app7.pdf Consultation on development of standards for characterization of vision loss and visual functioning, in WHO/PBL/03.91. 4-5 September 2003, World Health Organization Prevention of Blindness & Deafness: Geneva. World Health Organization. International Statistical Classification of Diseases and Related Health Problems: Tenth Revision. 1992, Geneva. Snellen, H, Letterproeven tot Bepaling der Gezichtsscherpte. 1862, Utrecht,: Weyers. Bailey IL, Lovie J, New Design Principles for Visual Acuity Letter Charts. Am J Optom & Physiol Opt 1976; 53: 740-745. Ferris FL, Kassov A, Bresnick GH, Bailey I, New Visual Acuity Charts for Clinical Research. Am J Ophthalmol 1982.;94: 91-96. McGraw P, Winn .B, Glasgow Acuity Cards: a new test for the measurement of letter acuity in children. Ophthalmic Physiol Opt 1993; 13: 400-4. Registered blind and partially sighted people year ending 31 March 2000.England. Technical report. 2001. Department of Health. Evans, J., Causes of blindness and partial sight in England and Wales 1990-1991, in Studies on Medical and Population Subjects 57. 1995: London: HMSO. Sorsby A. The causes of blindness in England and Wales, in Medical Research Council Memorandum no 24. 1950: London: HMSO. Sorsby A. The incidence and causes of blindness in England and Wales 1948- 62 in Reports on Public Health and Medical Subjects. 1966. Sorsby, A., The incidence and causes of blindness in England and Wales 1963-8 in Reports of Public Health and Medical Subjects. 1972. Ghafour IM, Allan D, Foulds WS, Common causes of blindness and visual handicap in the west of Scotland. Br J.Ophthalmol 1983; 67: 209-13. Grey RHB, Burns C, Hughes A, Blind and partial sight registration in Avon. Br J Ophthalmol 1989; 73: 88-94. Yap M, Weatherill J, Causes of blindness and partial sight in the Bradford Metropolitan District from 1980 to 1985. Ophthal Physiol Opt 1989; 9: 289-92. Evans J, Wormald R, Is the incidence of registrable age-related macular degeneration increasing? Br JOphthalmol, 1996; 80: 9-14. Evans JR, Rooney C, Dattani N, Ashwood F, Wormald RPL Causes of blindness and partial sight in England and Wales. HlthTrends 1996; 28: 5-12. Gibson JM, Lavery JR, Rosenthal AR, Blindness and partial sight in an elderly population. Br J Ophthalmol. 1986; 70: 700-5. 97 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. Robinson R, Deutsch J, Jones HS, Youngson-Reilly S, Hamlin DM, Dhurjon L et al, Unrecognised and unregistered visual impairment. Br J Ophthalmol. 1994; 78: 733-4. Bunce C, Evans J, Fraser S, Wormald R, BD8 certification of visually impaired people. Br J Ophthalmol 1998; 82: 72-6. Martin J, Meltzer H, Elliot D, The prevalence of disability among adults. OPCS surveys of disability in Great Britain Report 1. 1988 Office of Population Censuses and Surveys: London. Grundy E, Ahlburg D, Ali M, Breeze E, Sloggett A, Disability in Great Britain: results from the 1996/97 disability survey Technical Report 94. 1999, Dept of Social Security: London,. 1998/99 RNIB Survey of the Lifestyles and Needs of the Visually Impaired Technical report. 2000., Office of National Statistics: London. Smeeth L, Fletcher AE, Stirling S, Nunes M, Breeze E, Ng ESW, Bulpitt CJ, Jones D. A randomised comparison of three methods of administering a screening questionnaire to elderly people: findings from The MRC Trial of the Assessment and Management of Elderly People in the Community. BMJ 2001; 323: 1-7. Fletcher AE, Jones D, Bulpitt CJ, Tulloch AJ, The MRC Trial of assessment and management of older people in the community: objectives, design and interventions [ISRCTN23494848]. BMC Health Services Research 2002. 2(21). Lavery JR, Gibson JM, Shaw DE, Rosenthal AR, Vision and visual-acuity in an elderly population. Ophthalmic Physiol Opt, 1988; 8: 390-393. Gibson JB, Rosenthal AR, Lavery J., A study of the prevalence of eye disease in the elderly in an English community. Trans Ophthalmol Soc UK 1985; 104: 196-202. Wormald RPL, Wright LA, Courtney P, Beaumont B, Haines AP, Visual problems in the elderly population and implications for services. BMJ 1992; 304: 1226-1229. Reidy A, Minassian DC, Vafidis G, Joseph J, Farrow S, Wu J, Desai P, Connolly A, Prevalence of serious eye disease and visual impairment in a north London population: population based, cross sectional study. BMJ 1998; 316: 1643-6. van der Pols JC, Bates C, McGraw PV, Thompson JR, Reacher M, Prentice A, Finch S, Visual acuity measurements in a national sample of British elderly people. Br J Ophthalmol 2000; 84: 165-170. Evans J, Fletcher AE, Wormald R, Ng ESW, Stirling S, Smeeth L, Nunes M, Breeze E, Bulpitt CJ, Jones D, Tulloch A., Prevalence of visual impairment in people aged 75 years and above in Britain: results from the MRC Trial of assessment and management of older people in the community. Br J Ophthalmology 2002;86: 795800. Hayward LM, Burden ML, Burden AC, Blackledge A, Raymond NT, Botha JL, Karwatowski WSS, Duke T, Chang YF, What is the prevalence of visual impairment in the general and diabetic populations: are there ethnic and gender differences? Diabetic Med 2002; 19: 27-34. Bruce I, McKennell A, Walker E., Blind and partially sighted adults in Britain: the RNIB survey. 1991, Royal National Institute for the Blind: London. Das BN, Thompson JR, Patel R, Rosenthal AR, The prevalence of eye disease in Leicester - a comparison of adults of Asian and European descent. J R Soc Med 1994; 87: 219-222. Evans JE, Fletcher AE, Wormald RPL, Causes of visual impairment in people aged 75 years and above in Britain: an add-on study to the MRC Trial of assessment and 98 40. 41. 42. 43. 44. 45. 46. 47. 48. 49. 50. 51. 52. 53. 54. 55. 56. 57. 58. management of older people in the community. Br J Ophthalmology 2004; 88: 365370. Praat A and K. S, Defining sight difficulties for education and employment research. British Journal of Visual Impairment 2003; 21: 93-97. Bone M, Meltzer H, The prevalence of disability among children, OPCS surveys of disability in great Britain Technical Report 3. 1989, Office of Population Censuses and Surveys: London HMSO. Walker E, Tobin M, McKennell A, Blind and partially sighted children in Britain: The RNIB survey. Technical report RNIB & OPCS. 1985.: London HMSO. Clunies-Ross L Where have all the children gone? An analysis of new statistical data on visual impairment amongst children in England, Scotland and Wales. British Journal of Visual Impairment 1997; 15: 48-53. Keil, S., Survey of educational provision for blind and partially sighted children in England, Scotland and Wales in 2002. British Journal of Visual Impairment 2003; 21: 93-97. Peckham CS, P.R., The prevalence and nature of ascertained handicap in the National Child Development Study (1958 cohort). Public Health, 1976; 90: 11-21. Stewart-Brown SL, Haslum MN, Partial sight and blindness in children of the 1970birth cohort at 10 years of age. J Epidemiol Community Health 1988; 42: 17-23. Rahi JS, Cable N. Severe visual impairment and blindness in children in the UK Lancet 2003; 362: 1359-65. Pupil characteristics and class sizes in maintained schools in England. 2004, Department for Education and Skills. Crofts BJ, King R, Johnson A. The contribution of Low Birth Weight to severe vision loss in a geographically defined population. Br J Opthalmol1998; 82: 9-13. Rogers M Vision impairment in Liverpool: prevalence and morbidity. Arch Dis Child 1996; 74: 299-303. Flanagan, NM, Jackson AJ, Hill AE Visual Impairment in Children: Insights from a community-based survey. Child Care, Health and Development 2003; 29: 493-499. Visual Impairment Scotland. A new system of notification of childhood visual impairment and the information it has provided on services for Scottish children. 2003, University of Edinburgh: Edinburgh. Educational services for visually impaired children and young people. Consultation document, Pupil support division. Date of issue: 28 May 2004. 2004, Welsh Assembly Government. Blohme J, Tornqvist K, Visual impairment in Swedish children III. Diagnoses. Acta Ophthalmol Scand 1997; 75: 681-7. Gordon P et al., Disabled children in Britain: a re-analysis of the OPCS disability surveys. 2000, London: The Stationery Office. Massof RW, Rubin GS, Visual function assessment questionnaires. Surv Ophthalmol 2001; 45: 531-48. Mangione CM, Berry S, Spritzer K, Janz NK, Klein R, Owsley C et al, Identifying the content area for the 51-item National Eye Institute Visual Function Questionnaire: results from focus groups with visually impaired persons. Arch Ophthalmol 1998; 116: 227-33. Murthy GVS, Gupta S, Thulasiraj RD, Viswanath K, Donoghue M, Fletcher AE., The Development of the Indian Vision Function Questionnaire (IND-VFQ): Questionnaire Content. Br J Ophthalmol 2004: in press. 99 59. 60. 61. 62. 63. 64. 65. 66. 67. 68. 69. 70. 71. 72. 73. Mangione CM, Lee P, Gutierrez PR, Spritzer K, Berry S, Hays RD, Development of the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol 2001; 119: 1050-8. Brody BL, Gamst AC, Williams RA, Smith AR, Lau PW, Dolnak D et al, Depression, visual acuity, co-morbidity, and disability associated with age-related macular degeneration. Ophthalmology 2001; 108: 1893-900. Jampel HD, Friedman DS, Quigley H, Miller R, Correlation of the binocular visual field with patient assessment of vision. Invest OphthalmolVis Sci 2002; 43: 1059-67. Cole SR, Beck RW, Moke PS, Gal RL, Long DT, The National Eye Institute Visual Function Questionnaire: experience of the ONTT. Optic Neuritis Treatment Trial. Invest Ophthalmol Vis Sci 2000; 41: 1017-21. Klein R, Moss SE, Klein BE, Gutierrez P, Mangione CM, The NEI-VFQ-25 in people with long-term type 1 diabetes mellitus: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Arch Ophthalmol 2001. 119: p. 733-40. Deramo VA, Cox TA, Syed AB, Lee PP, Fekrat S, Vision-related quality of life in people with central retinal vein occlusion using the 25-item National Eye Institute Visual Function Questionnaire. Arch Ophthalmol 2003; 121: 1297-302. Miskala PH, Hawkins BS., Mangione CM, Bass EB, Bressler NM, Dong LM et al, Responsiveness of the National Eye Institute Visual Function Questionnaire to changes in visual acuity: findings in patients with subfoveal choroidal neovascularization--SST Report No. 1. Arch Ophthalmol 2003; 121: 531-9. Scott IU, Smiddy W., Schiffman J, Feuer WJ, Pappas CJ, Quality of life of lowvision patients and the impact of low-vision services. Am J Ophthalmol 1999; 128: 54-62. Stelmack JA, Stelmack TR, Massof RW, Measuring low-vision rehabilitation outcomes with the NEI VFQ-25. Invest Ophthalmol Vis Sci 2002; 43: 2859-68. Massof RW, Fletcher DC, Evaluation of the NEI visual functioning questionnaire as an interval measure of visual ability in low vision. Vision Res 2001; 41: 397-413. Paz SH, Globe DR, Wu J, Azen SP, Varma R, Relationship between self-reported depression and self-reported visual function in Latinos. Arch Ophthalmol, 2003; 121: 1021-7. Broman AT, Munoz B, Rodriguez J, Sanchez R, Quigley HA, Klein R et al, The impact of visual impairment and eye disease on vision-related quality of life in a Mexican-American population: proyecto VER. Invest Ophthalmol Vis Sci. 2002; 43: 3393-8. Smeeth L, Fletcher .AE, Hanciles S, Evans J, Wormald R, Screening older people for impaired vision in primary care: a cluster randomised trial within the MRC trial of the assessment and management of older people in the community. BMJ 2003; 327: 1027-1031. Augood C, Fletcher AE, Chakravarthy U, De Jong PVTM. Rahu M, Seland J, Soubrane G, Tomazzoli L, Topouzis F, Vioque J, Prevalence of age-related maculopathy in the EUREYE study. Invest. Ophthalmol. Vis Sci 2004. 45: p. EAbstract 3048. Congdon N, O'Colmain CB, Klaver CC, Klein R, Munoz B, Friedman DS, Kempen J, Taylor HR, Mitchell P; Eye Diseases Prevalence Research Group, Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol 2004; 122: 477-85. 100 74. 75. 76. 77. Owen CG, Fletcher AE, Donoghue M, Rudnicka AR., How big is the burden of visual loss caused by age-related macular degeneration in the UK? Br J Ophthalmology, 2003; 87: 312-317. Evans JE, Fletcher AE, Wormald RPL Age-related macular degeneration causing visual impairment in people aged 75 years and above in Britain: an add-on study to the Medical Research Council Trial of assessment and management of older people in the community. Ophthalmology 2004;111: 513-517. Nissen KR, Sjolie AK, Jensen H, Borch-Johnsen K, Rosenberg T, The prevalence and incidence of visual impairment in people of age 20-59 years in industrialized countries: A review. Ophthalmic Epidemiol 2003; 10: 279-291. International Committee of Medical Journal Editors. Uniform Requirements for Manuscripts submitted to Biomedical Journals. Ann Intern Med 1997; 126: 36-47. 101
 0
0
advertisement
Related documents




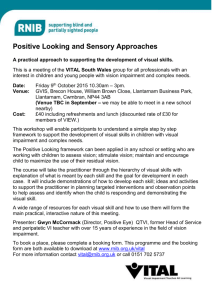

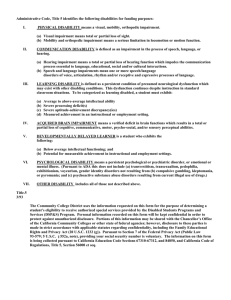
Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users