Nutrition Profile - Daniella Wolf, RD
advertisement

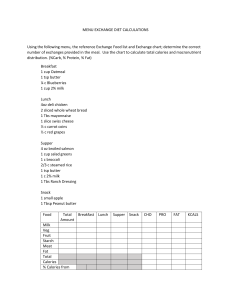
Daniella Wolf, BASc. RD Pink sections are For Office Use only. Consulting Dietitian and Nutritionist NUTRITION PROFILE . Patient History Name: _______________________________________ Date of Consultation: ________________________________ Address: _____________________________________ Family Doctor: ____________________________________ street ______________________________________ city province Letter to Doctor: postal code Phone: (H) ________________ (W) _______________ Address: __________________________________________ Birthdate: ____________________________________ Phone: ___________________________________________ Occupation: __________________________________ Referred by: _______________________________________ Reason For Referral: ___________________________ Medical Conditions: ________________________________ Additional Information: _________________________ Date of last physical exam: ___________________________ Lab Data: ____________________________________ Medications: ______________________________________ Height: ____cm (____in.) Weight: ____kg (____lb.) BMI: ____WC*: ____ Goal: Weight: ____kg (___lb.) BMI:_____ Weight Change History: _______________________________________________________________________________ Physical Activity: ____________________________________________________________________________________ Food Allergies/Intolerances/Dislikes: ____________________________________________________________________ Vitamin/Mineral Supplements: __________________________________________________________________________ Factors Affecting Food Intake: ___________________ Recent Changes In Food Habits: _______________________ Meal Preparation: _____________________________ Meals Eaten Out: Lunch ______ Dinner______ Food Frequency: Milk Products: skim 1% 2% soy cheese ______________ yogurt ______________ frozen yogurt ________ ice cream ___________ Grains: cereal __________________ bread __________________ rice ___________________ potatoes ________________ pasta __________________ Meat/Alternatives: chicken ________________ fish ___________________ beef ___________________ pork __________________ legumes _______________ eggs __________________ lamb __________________ cottage cheese __________ tofu __________________ nuts __________________ Fruit: juice _______________ fresh _______________ Vegetables: salads __________________ cooked _________________ Fats: butter _________________ margarine ______________ peanut butter ____________ oil ____________________ salad dressing ___________ mayonnaise ____________ Liquids: coffee/tea ___________ soft drinks ______________ wine/beer/alcohol _____________ water _______________________ Sweets/Snacks: _________________________________________________ One-Day Food Recall: Breakfast: _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ Lunch: _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ Dinner: ____________________________ ____________________________ ____________________________ ____________________________ ____________________________ Snack: Snack: Snack: _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ _____________________________ ____________________________ ____________________________ ____________________________ ____________________________ ____________________________ Initial Suggestions: Food Recall Analysis 1.__________________________ 4. __________________________ Calories __________ Fibre _______________ 2.__________________________ 5. __________________________ Carbs ____________ Unsaturated Fat ______ 3.__________________________ 6. __________________________ Saturated Fat ______ Calcium ____________ Protein ___________ Nutritional Diagnostic Statements: 1. _______________________________________ 4. _______________________________________ 2. _______________________________________ 5. _______________________________________ 3. _______________________________________ 6. _______________________________________ Diet Provided:______________________________________________________________________________ Educational Materials: WCFG HLP GHEG Sample Food Plan Other______________________ Food Plan: Calories: ______________________ Protein:__________ g _________ % Food Group Svgs Fat: ______ g ______% Carbohydrates:______ g _______% Date Meat & Alt Grains Milk Products Fruit Vegetables Fats Dietitian's Signature: ________________________ Completion Date: __________________________ *WC waist circumference M<102cm/40in F<88cm/35in