ECG Tips
advertisement

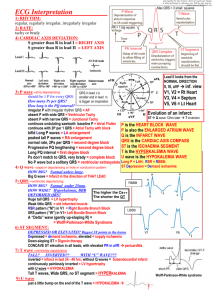
ECG Tips 21/2/11 FANZCA Notes Life in the Fast Lane Crit-IQ PY Mindmaps Stuart Lane Tutorial – Nepean Written Course (2011) The 12 Lead ECG - 10 physical leads - 12 electrical leads CALIBRATION - normal = 25mm/s calibration = 5mm wide, 10mm high = 1mV 1 small square = 1mm = 0.04s = 40ms 1 large square = 5mm = 0.2s = 200ms RATE - QRS complexes on rhythm strip x 6 = rate/min - number of large squares between R waves: 300-150-100-75-60-50 Tachycardia - narrow complex vs wide complex? - narrow: Jeremy Fernando (2011) -> AV node independent (ST, unifocal, mutlifocal, AF, Aflu) -> AV node dependent (AVN re-entry, AV re-entry, junctional) - wide: -> -> -> -> VF supra-ventricular tachycardia with BBB VT accelerated idioventricular rhythm - regular or irregular? - irregular: -> multiple ventricular ectopics -> AF with aberrancy -> AF with BBB -> AF with pre-excitation pathway - regular: -> sinus -> junctional Bradycardia - sinus: -> -> -> -> -> arrest pauses inappropriate bradycardia (vagal overactivity, myxoedema) physical fitness beta blockade - AV node dysfunction: -> 1st degree – prolongation of PR interval (>0.2s) -> 2nd degree (Mobitz type I) – progressive lengthening of PR interval with eventual dropped ventricular conduction -> 2nd degree (Mobitz type II) – intermittent dropping of ventricular conduction -> 2nd degree (2:1 type) – alternate p-wave not conducted to ventricles -> 3rd degree – complete dissociation between atria and ventricular RHYTHM - SR or not? AXIS - QRS positive in I and aVL = normal I positive and aVF negative = LAD I negative and aVF positive = RAD I and aVF negative = extreme RAD or LAD RAD Jeremy Fernando (2011) - RVH Left posterior hemiblock Lateral myocardial infarction Acute right heart strain (PE) Normal in infants and children LAD - AS Dilated cardiomyopathy AMI IHD HT -> aortic root dilation -> AR Left anterior hemiblock Extreme Axis Deviation - situs inversus - limb lead on backwards - VT P WAVE = atrial depolarisation - look for in V1 and II (best seen) must be negative in aVR (otherwise leads misplaced) normal duration: 0.12s normal eight: < 2mm - dual: heart transplant bifid: LA enlargement (mitral stenosis) peaked: RA enlargement (pulmonary hypertension) or LA enlargement inversion: atrial ectopic, junctional rhythms, dextrocardia variable morphology: multifocal atrial rhythms PR INTERVAL AND PR SEGMENT - normal duration 0.12-0.2s (3 to 5mm) long: 1st, 2nd (type I and II) and 3rd degree HB short: WPW, LGL depression: pericarditis, atrial ischaemia Q WAVES - normal: < 25% of R wave in I, aVL, aVF, V4,5,6. - pathological: if long (>0.04s) and deep (>2mm) QRS COMPLEX - normal duration < 0.12s (3 small squares) - normal transition point of R wave: V3-V4 Jeremy Fernando (2011) - amplitude: normal, large, low voltage, alternans - morphology: notched, RBBB, LBBB Positive QRS in V1 - RVH - posterior infarction - WPW type 1 - RBBB - Duchenne’s muscular dystrophy - dextrocardia - incorrect lead placement - rare causes: LV ectopics, acute right heart strain, hypertrophic cardiomyopathy, normal variant, Brugada syndrome J WAVE = positive deflection @ QRS and ST junction (J point) 1. Hypothermia (increases with severity) 2. Severe hypercalcaemia ST SEGMENT ST Elevation 1. 2. 3. 4. 5. 6. 7. AMI Pericarditis (with PR interval depression) Tako-tsuba cardiomyopathy LBBB Brugada syndrome Benign early repolarisation (isn’t so benign -> higher risk of cardiac death) LV aneurysm Contour - horizontal - upsloping - downsloping T WAVE - normal amplitude: < 2/3rds R wave peaked inverted alternans U WAVE = small positive deflection following T wave 1. Hypokalaemic Periodic Paralysis Jeremy Fernando (2011) 2. Bradycardia 3. Hypothermia 4. Drug OD – digoxin, phenothiazines, anti-arrhythmics (sotalol, amiodarone, quinidine, procainamide) 5. Hypomagnaesaemia 6. Hypocalcaemia 7. Increased ICP QT INTERVAL - rate dependent should be less than 50% of R-R interval measure in II or V5-6 (include large u wave that is fused with T wave) QTc > 440ms (11 small squares) in men or > 460ms in women (11.5 small squares) Causes of Prolonged QT - drugs: anti-arrhythmics, anti-histamines, macrolide, anti-depressants, methadone…) electrolytes: hypokalaemia, hypoMg2+, hypocalcaemia stroke: SAH ACS bradyarrhythmia congenital -> complication = Torsade de Ponte OTHER CONDUCTION DISTURBANCES RBBB - activation of the right ventricle is delayed QRS > 120ms RSR in V1 (‘M’), and ‘W’ in V6 (MARROW) broad S wave in LV leads (I and V6) normal axis 1. 2. 3. 4. 5. Can be normal Massive PE RVH IHD Congenital heart disease LBBB - septal depolarisation reversed (right to left) -> change in initial direction of QRS QRS > 120ms Q waves seen in left ventricular leads WILLIAM (W in V1, M in V6) normal axis always pathological 1. IHD 2. Cardiomyopathy 3. LVH Jeremy Fernando (2011) Left anterior hemiblock – LAD, Q waves in I and aVL, small R in III (and absence of LVH) Left posterior hemiblock – RAD, small R in I, small Q in III (and absence of RVH) Bifascicular block - RBBB + block of either left anterior or posterior fascicle. - RBBB + left anterior fascicle block -> LAD - RBBB + left posterior fascicle block -> RAD Trifascicular block – 8 types: (1) (2) (3) (4) (5) (6) (7) (8) Prolonged PR interval + LAD + RBBB LBBB + RAD AF + LAD + RBBB Junctional rhythm + RAD + RBBB Alternating BBB RBBB + alternating fascicular block BBB + second degree HB type II Any bifascicular block + 1st or 2nd degree AV block TRICKS AND TRAPS Artifacts – tremor Dextrocardia - RAD - P in I - QRS complexes decrease in amplitude across the chest leads HypoMg2+ - wide QRS peak T waves R prolongation TWI U waves VT -> Torsades Lown-Ganong-Levine - short PR interval < 0.12s - no delta wave - may have normal QRS (unless IVCD present) Overdose -> Na+ channel blockade 1. Positive QRS in II 2. Dominant R wave in aVR 3. QRS duration > 100ms Packing Spikes – failure to sense/capture/output Jeremy Fernando (2011) WPW - PR interval < 0.12s - QRS duration > 0.12s - Delta wave Cardiac Arrest in a Young Person - ARVD: RV strain and epsilom wave Long QT: TW after 50% of R-R distance Brugada: V1 and V2 have funny ST elevation HOCM: LVH WPW: see above V5R – most sensitive lead for RV infarction (ST segment will be elevated) Pericardial tamponade - electrical alternans -> heart swinging in massive pericardial effusion (c/o change in impedance) ELECTROLYTE ECG CHANGES Hyperkalaemia - tall T waves flat P waves prolonged PR wide QRS Hypokalaemia - ST depression T wave flattening U waves SVT VT Torsades de Pointes Hypermagnasaemia - bradyarrhythmias - cardiac arrest Hypomagnasaemia - prolonged PR wide QRS ventricular arrhythmias Torsades Jeremy Fernando (2011) Hypercalcaemia - shortened QTc - Osborn or J wave Hypocalcaemia - prolongation of ST segment and QT interval - VT Jeremy Fernando (2011)