TOE Exemplar (1) - UCLA | School of Nursing
advertisement
 - UCLA | School of Nursing")
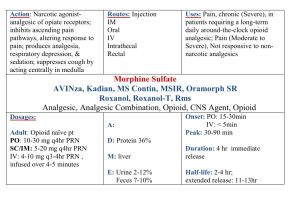
CITATION PURPOSE SAMPLE/SETTING METHODS Kelly A.M., Brumby, C., Barnes, C. (2005). Nurse-initiated, titrated IV opioid analgesia reduces time to analgesia for selected painful conditions. Can J Emerg Med, 7(3):149-54 Retrospective study to find the impact of Nurse-initiated protocol on time to first opioid dose. n= 157 visits of 126 patients to the emergency department of the Western hospital at Melbourne, Australia. with diagnosis of renal or biliary colic. Fry, R., Ryan, J., Alexander, N. (2004). A prospective study of nurse initiated panadeine forte: Expanding pain management. Accident and Emergency Nursing, 12 (3), 136-140. doi: 10.1016/j.aaen.200 Medical records of the patients were reviewed using a data collection tool by two researchers. Demographics and whether analgesia was Nurse initiated (NI) or doctor initiated were identified from August 1, 2002 January 31, 2003. Data analysis was done using Chi square and Descriptive statistics Prospective N = 202. 96% of Analogue scale exploratory patients n= 195 met was used to study to criteria and received measure pain. evaluate the the drug. n = 7 (3%) Data tool effectiveness of received Panadeine developed for the using a specific Forte without meeting study collected drug just after criteria. Conducted adherence to the triage by RN in a referral hospital's protocol. Data ED in Australia in was analyzed 2003 for 12 weeks using the SPSS package. RESULTS DISCUSSION & LIMITATIONS 37% of samples Generalizability received NI and may not be possible 63% by non NI; as study includes Inter-rater nursing staff with reliability of NI or training, Nurse non NI was patient ratios, legal measured on 82% and political issues of records with may be different in Kappa analysis hospital setting. yielding 0.92. The groups were not Median time to first randomized; dose was 37 min for treatment group the NI analgesia were identified post group and 57 min hoc by chart review. for the second Documentation group (Mannerrors and omissions Whitney U test). possible No respiratory depression were identified 202 patients received the drug with an average time of 23 min; median time was 6 min. Average pain score prior to receiving the drug was 68 mm and after the drug administration was 38 mm on the analogue visual Study cannot be conducted in ED's with inexperienced nurses. Convenience sample makes generalizability difficult. Outcome unknown regarding patients left without physician evaluation. Study had a vast 4.02.006 Muntlin, A., Carlsson, M., Safwenberg, U., Gunningberg, L. (2011) Outcomes of a nurse-initiated intravenous analgesic protocol for abdominal pain in an emergency department: A quasi-experimental study. International Journal of Nursing Studies, 48(1), 13 23. doi: 10.1016/j.ijnurstu.2 010.06.003 Quasiexperimental study to compare between standard care given in the ED as opposed to using nurseinitiated opioid analgesic ABA phase Quasiexperimental study with n = 50 for A1, n = 100 for B and n = 50 A2 at a Swedish university hospital ED. Nurses were educated to assess pain and use of pain protocol. Questionnaire for ED patients was developed to find out perceptions of pain management. Medical records reviewed to collect data on pain assessment, time to analgesic, transit time in the ED, frequency of analgesic administration. scale of 100 mm. Wilcoxon signed rank test with p < 0.001 showed statistically significant lower pain scores after the drug was given. Pain management improved along with patients perception of pain. Intervention phase showed a significant reduction in receiving analgesic. exclusion criteria. Questionnaire not filled out by all patients resulting in drop outs. Some patients refused analgesic during the intervention phase and did not complete questions. Generalizability still should be only to Emergency departments with same type setting and patients.