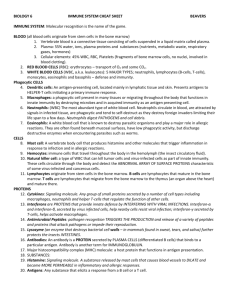
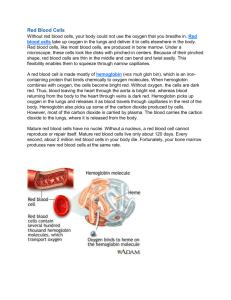
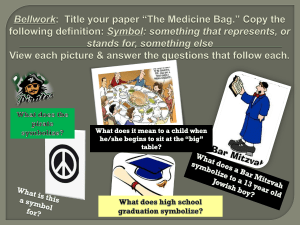
Blood physiology by prof.Israa F.Jafar Physiology of Blood Components, Characteristics, Functions of Blood Major Components of Blood 1. Formed elements - the actual cellular components of blood (special connective tissue) a.erythrocytes - red blood cells b.leukocytes - white blood cells c.platelets - cell fragments for clotting 2. Blood plasma - complex non-cellular fluid surrounding formed elements; protein & electrolytes. Separation of Components in a Centrifuge VOLUME clear/yellowish PLASMA 55% thin/whitish buffy coat <1% with LEUKOCYTES & PLATELETS reddish mass - ERYTHROCYTES 45% LAYER top middle bottom hematocrit - percentage by VOLUME of erythrocytes when blood is centrifuged (normal = 45%) Characteristics of Blood 1. bright red (oxygenated) 2. dark red/purplish (unoxygenated) 3. much more dense than pure water 4. pH range from 7.35 to 7.45 (slightly alkaline) 5. slightly warmer than body temperature 100.4 F 6. typical volume in adult male 5-6 liters 7. typical volume in adult female 4-5 liters 8. typically 8% of body weight 1 Blood physiology by prof.Israa F.Jafar Major Functions of Blood 1. Distribution & Transport a. oxygen from lungs to body cells b. carbon dioxide from body cells to lungs c. nutrients from GI tract to body cells d. nitrogenous wastes from body cells to kidneys e. hormones from glands to body cells 2. Regulation (maintenance of homeostasis) a. maintenance of normal body pH by blood proteins (albumin) & bicarbonate b. maintenance of circulatory/interstitial fluid by electrolytes that aid blood proteins (albumin) c. maintenance of temperature (blushed skin) 3. Protection a. platelets and proteins "seal" vessel damage b. protection from foreign material & infections byleukocytes, antibodies& complement proteins Plasma (the liquid part of blood) A. General Characteristics 1. plasma makes up 55% of normal blood by volume 2. water is 90% of the plasma by volume 3. many different SOLUTES in the plasma a. albumin - pH buffer & osmotic pressure b. globulins - binding proteins & antibodies c. clotting proteins - prothrombin & fibrinogen d. other proteins - enzymes, hormones, others e. nutrients - glucose, fatty acids, amino acids, cholesterol, vitamins f. electrolytes - Na+, K+, Ca++, Mg++, Cl-, phosphate, sulfate, bicarbonate, others 2 Blood physiology by prof.Israa F.Jafar BONE MARROW In the adult, red blood cells, many white blood cells, and platelets are formed in the bone marrow. In the fetus, blood cells are also formed in the liver and spleen, and in adults such extramedullary hematopoiesis may occur in diseases in which the bone marrow becomes destroyed or fibrosed. In children, blood cells are actively produced in the marrow cavities of all the bones. By age 20, the marrow in the cavities of the long bones, except for the upper humerus and femur, has become inactive . Active cellular marrow is called red marrow; inactive marrow that is infiltrated with fat is called yellow marrow. The bone marrow is actually one of the largest organs in the body, approaching the size and weight of the liver. It is also one of the most active. Normally, 75% of the cells in the marrow belong to the white blood cell-producing myeloid series and only 25% are maturing red cells, even though there are over 500 times as many red cells in the circulation as there are white cells. This difference in the marrow reflects the fact that the average life span of white cells is short, whereas that of red cells is long. The bone marrow contains multipotent uncommitted stem cells (pluripotential stem cells) that differentiate into one or another type of committed stem cells (progenitor cells). These in turn form the various differentiated types of blood cells. There are separate pools of progenitor cells for megakaryocytes, lymphocytes, erythrocytes, eosinophils, and basophils, whereas neutrophils and monocytes arise from a common precursor. The bone marrow stem cells are also the source of osteoclasts , Kupffer cells . mast cells, dendritic cells, and Langerhans cells . The pluripotential cells are few in number but are capable of completely replacing the bone marrow when injected into a host whose own bone marrow has been completely destroyed. The best current source for these hematopoietic stem cells is umbilical cord blood. The pluripotential cells are derived from uncommitted, totipotent stem cells that at least in theory can be stimulated to form any cell in the body. There are a few of these in adults, but they are more readily obtained from the blastocysts of embryos. Totipotential cells from human embryos have now been cultured, and there is immense interest in stem cell research. However, there are ethical as well as scientific issues involved, and debate on these issues will undoubtedly continue. Erythrocytes (red blood ells; RBCs) Structure 1. 7.5 micron diameter; 2.0 micron thick 2. biconcave disk shape; ideal for gas exchange;the shape is maintained by 3 Blood physiology by prof.Israa F.Jafar spectrin - elastic protein; allows shape change. 3. mature cells are anucleate (no nucleus) 4 very few organelles; mainly a hemoglobin carrier i. hemoglobin – 33% of cell mass; carries oxygen 5. no mitochondria; only anaerobic respiration 6. ratio erythrocytes:leukocytes = 800:1 7. red blood cell count: as cells per cubic millimeter i. normal male count - 5. to 5.8 million ii. normal female count - 4.3 to 5.2 million Functions (oxygen & carbon dioxide transport) Hematopoiesis and Erythropoiesis: hematopoiesis (hemopoiesis) - the maturation, development and formation of blood cells a. red bone marrow (myeloid tissue) - location of hematopoiesis; in blood sinusoids which connect with capillaries; mainly in axial skeleton and heads of femur & humerus b. hemocytoblast (stem cell) - the mitotic precursor to blood cells before differentiation i. differentiation - maturing cell becomes "committed" to being certain type blood cell Erythropoiesis - the maturation, development, and formation of Red Blood Cells hemocytoblast ->proerythroblast ->early (basophilic) erythroblast ->late (polychromatophilic) erythroblast ->(hemoglobin) normoblast -> (nucleus ejected when enough hemoglobin)reticulocyte -> (retaining some endoplasmic reticulum) ERYTHROCYTE life span: hemocytoblast -> reticulocyte reticulocyte -> ERYTHROCYTE ERYTHROCYTE lifespan (primarily destroyed by macrophages in the spleen) 3-5 DAYS 2 DAYS (in blood) 100-120 DAYS 3. Regulation of Erythropoiesis a. hormonal controls - erythropoietin is the hormone that stimulates RBC production DECREASED oxygen level in blood causes KIDNEYS to increase release of erythropoietin 1. Less RBCs from bleeding 2. Less RBCs from excess RBC destruction 3. Low oxygen levels (high altitude, illness) 4. Increased oxygen demand (exercise) 4 Blood physiology by prof.Israa F.Jafar Eythropoietin now genetically engineered and synthesized to stimulate erythropoisis Testosterone can also mildly stimulate production of RBCs in humans b. Iron - essential for hemoglobin to carry oxygen i. 65% of Fe in body is in hemoglobin ii. liver and spleen store most excess Fe bound to ferritin and hemosiderin iii. Fe in blood bound to transferrin iv. daily Fe loss: 0.9 mg men/l.7 mg women v. women also lose Fe during menstrual flow c. B-complex Vitamins - Vitamin B12 and Folic Acid essential for DNA synthesis in early mitotic divisions leading to erythrocytes 5 Blood physiology by prof.Israa F.Jafar Hemoglobin The red, oxygen-carrying pigment in the red blood cells of vertebrates is hemoglobin, a protein with a molecular weight of 64,450. Hemoglobin is a globular molecule made up of 4 subunits .Each subunit contains a heme moiety conjugated to a polypeptide. Heme is an ironcontaining porphyrin derivative . The polypeptides are referred to collectively as the globin portion of the hemoglobin molecule. There are two pairs of polypeptides in each hemoglobin molecule. 1. (hemoglobin A is α2 β2 ) the normal adult human hemoglobin ; the two types of polypeptide are called the α chains, each of which contains 141 amino acid residues, and the β chains, each of which contains 146 amino acid residues. Thus, hemoglobin A is designated α2β2. 2. hemoglobin A2 (α2δ2). this forms about 2.5% of the hemoglobin, in which β chains are replaced by δ chains (α2δ2). The δ chains also contain 146 amino acid residues, but 10 individual residues differ from those in the β chains. 3.There are small amounts of hemoglobin A derivatives closely associated with hemoglobin A that represent glycated hemoglobins. One of these, hemoglobin A1c (HbA1c), has a glucose attached to the terminal valine in each β chain and is of special interest because the quantity in the blood increases in poorly controlled diabetes mellitus . 4.Hemoglobin in the Fetus 1.The blood of the human fetus normally contains fetal hemoglobin (hemoglobin F hemoglobin F is( α2 γ2). The γ chains also contain 146 amino acid residues but have 37 that differ from those in the β chain. Fetal hemoglobin is normally replaced by adult hemoglobin soon after birth. In certain individuals, it fails to disappear and persists throughout life. In the body, its O2 content at a given PO2 is greater than that of adult hemoglobin because it binds 2,3-DPG less avidly. This facilitates movement of O2 from the maternal to the fetal circulation 2. In young embryos there are, in addition, ζ and ε chains, forming Gower 1 hemoglobin (ζ2ε2) and Gower 2 hemoglobin (α2ε2). 6 Blood physiology by prof.Israa F.Jafar Reactions of Hemoglobin 1.oxygenation:Hemoglobin binds O2 to form oxyhemoglobin, O2 attaching to the Fe2+ in the heme. The affinity of hemoglobin for O2 is affected by pH, temperature, and the concentration in the red cells of 2,3-diphosphoglycerate (2,3-DPG). 2,3-DPG and H+ compete with O2 for binding to deoxygenated hemoglobin, decreasing the affinity of hemoglobin for O2 by shifting the positions of the four peptide chains (quaternary structure). 2.oxidation: When blood is exposed to various drugs and other oxidizing agents in vitro or in vivo, the ferrous iron (Fe2+) that is normally in the molecule is converted to ferric iron (Fe3+), forming methemoglobin. Methemoglobin is dark-colored, and when it is present in large quantities in the circulation, it causes a dusky discoloration of the skin resembling cyanosis . Some oxidation of hemoglobin to methemoglobin occurs normally, but an enzyme system in the red cells, the NADH-methemoglobin reductase system, converts methemoglobin back to hemoglobin. Congenital absence of this system is one cause of hereditary methemoglobinemia. 3. Carbon monoxide reacts with hemoglobin to form carbon monoxyhemoglobin (carboxyhemoglobin). The affinity of hemoglobin for O2 is much lower than its affinity for carbon monoxide, which consequently displaces O2 on hemoglobin, reducing the oxygencarrying capacity of blood . 4. Heme is also part of the structure of myoglobin, an oxygen-binding pigment found in red (slow) muscles 5.In addition, neuroglobin, an oxygen-binding globin, is found in the brain. It appears to help supply O2 to neurons. There is heme in the respiratory chain enzyme cytochrome c . Abnormalities of Hemoglobin Production The amino acid sequences in the polypeptide chains of hemoglobin are determined by globin genes. There are two major types of inherited disorders of hemoglobin in humans: the hemoglobinopathies, in which abnormal polypeptide chains are produced, and the thalassemias and related disorders, in which the chains are normal in structure but produced in decreased amounts or absent because of defects in the regulatory portion of the globin genes. The α thalassemias are defined by decreased or absent α polypeptides. The β thal-assemias are defined by decreased or absent α and β polypeptides. abnormal hemoglobins Mutant genes that cause the production of abnormal hemoglobins are widespread, and about 1000 abnormal hemoglobins have been described in humans. They are usually identified by letter—hemoglobin C, E, I, J, S, etc. In most instances, the abnormal hemoglobins differ from normal hemoglobin A in the structure of the polypeptide chains. 7 Blood physiology by prof.Israa F.Jafar hemoglobin S, the α chains are normal but the β chains are abnormal, because among the 146 amino acid residues in each β polypeptide chain, one glutamic acid residue has been replaced by a valine residue . When an abnormal gene inherited from one parent dictates formation of an abnormal hemoglobin—ie, when the individual is heterozygous—half the circulating hemoglobin is abnormal and half is normal. When identical abnormal genes are inherited from both parents, the individual is homozygous and all of the hemoglobin is abnormal. It is theoretically possible to inherit two different abnormal hemoglobins, one from the father and one from the mother. Many of the abnormal hemoglobins are harmless. However, some have abnormal O2 equilibriums. Others cause anemia. For example, hemoglobin S polymerizes at low O2 tensions, and this causes the red cells to become sickle-shaped, hemolyze, and form aggregates that block blood vessels. The result is the severe hemolytic anemia known as sickle cell anemia. Heterozygous individuals have the sickle cell trait and rarely have severe symptoms, but homozygous individuals develop the full-blown disease. The sickle cell gene is an example of a gene that has persisted and spread in the population. It originated in the black population in Africa, and it confers resistance to one type of malaria. This is an important benefit in Africa, and in some parts of Africa 40% of the population have the sickle cell trait. In the United States black population its incidence is about 10%. Hemoglobin F has the ability to decrease the polymerization of deoxygenated hemoglobin S, and hydroxyurea causes hemoglobin F to be produced in children and adults. It has proved to be a very valuable agent for the treatment of sickle cell disease. In patients with severe sickle cell disease, bone marrow transplantation has been carried out and the patients have generally done well, though more study is needed. Synthesis of Hemoglobin The average normal hemoglobin content of blood is 16 g/dL in men and 14 g/dL in women, all of it in red cells. In the body of a 70-kg man, there are about 900 g of hemoglobin, and 0.3 g of hemoglobin is destroyed and 0.3 g synthesized every hour . The heme portion of the hemoglobin molecule is synthesized from glycine and succinyl-CoA. Catabolism of Hemoglobin When old red blood cells are destroyed in the tissue macrophage system, the globin portion of the hemoglobin molecule is split off, and the heme is converted to biliverdin. The enzyme involved is a subtype of heme oxygenase . and CO is formed in the process. CO may be an intercellular messenger, like NO . 8 Blood physiology by prof.Israa F.Jafar In humans, most of the biliverdin is converted to bilirubin and excreted in the bile . The iron from the heme is reused for hemoglobin synthesis. Exposure of the skin to white light converts bilirubin to lumirubin, which has a shorter halflife than bilirubin. Phototherapy (exposure to light) is of value in treating infants with jaundice due to hemolysis. Iron is essential for hemoglobin synthesis; if blood is lost from the body and the iron deficiency is not corrected, iron deficiency anemia results. Anemias: I.Defeciency of substrates which are necessary for RBC or Hb production like: 1. Iron deficiency anaemia(increaseloss, or decrease intake) 2.folic acid deficiency anaemia(low intake) folic a. is necessary for DNA formation and maturation of RBCs. 3 B12 defeciency anaemia. B12 is necessary for DNA formation of RBCs.defeciency due to low intake as in vegetarians or intrinsic factor deficiency (pernicious anaemia). II. membrane defects as in hereditary spherocytosis or elliptocytosis. Haemolytic anaemia eg:autoimmune Haemolytic anaemia,erythroblastosis fetalis. III.Hemoglobinopathies.Thalassaemiaand sickle cell anaemia. IV . bone morrow infiltration like aplastic anaemia and different forms of leukaemias. V. Anaemia of chronic disease.like chronic renal failure. Effect of anemia on circulation: 1. Decrease the viscosity of blood. 2. increase work load on the heart (PALPITATION & TIREDNESS) 3. In exercise there will be tissue hypoxia that leads to heart failure. Treatment toward the cause. Polycythemia: Increase production of RBCs (count 6-8 milio/mm3)its of 2 types: 1.primarypolycythemia vera(count7-8 milio/mm3) 2.Secondary due to tissue hypoxialike in high altitude or chronic smokers. Effect of polycythemia on circulation increases the viscisity of blood leads to sluggish circulation this leads to thrombosis. Blood pressure increases increase work load on the heart leads to heart failure. Tretment by venesection 9 Blood physiology by prof.Israa F.Jafar Iron In adults, the amount of iron lost from the body is relatively small. The losses are generally unregulated, and total body stores of iron are regulated by changes in the rate at which it is absorbed from the intestine. Men lose about 0.6 mg/d, largely in the stools. Women have a variable, larger loss averaging about twice this value because of the additional iron lost in the blood shed during menstruation. The average daily iron intake in the United States and Europe is about 20 mg, but the amount absorbed is equal only to the losses. Thus, the amount of iron absorbed ranges normally from about 3 to 6% of the amount ingested. Various dietary factors affect the availability of iron for absorption; for example, the phytic acid found in cereals reacts with iron to form insoluble compounds in the intestine. So do phosphates and oxalates. Most of the iron in the diet is in the ferric (Fe 3+) form, whereas it is the ferrous (Fe2+) form that is absorbed. There is Fe3+ reductase activity associated with the iron transporter in the brush borders of the enterocytes . No more than a trace of iron is absorbed in the stomach, but the gastric secretions dissolve the iron and permit it to form soluble complexes with ascorbic acid and other substances that aid its reduction to the Fe2+ form. The importance of this function in humans is indicated by the fact that iron deficiency anemia is a troublesome and relatively frequent complication of partial gastrectomy. Almost all iron absorption occurs in the duodenum. Fe2+ is Transported into the enterocytes . Some is stored in ferritin, In the plasma, Fe2+ is converted to Fe3+ and bound to the iron transport protein transferrin. This protein has two iron-binding sites. Normally, transferrin is about 35% saturated with iron, and the normal plasma iron level is about 130 ug/dL (23 umol/L) in men and 110 ug/dL (19 umol/L) in women. 70% of the iron in the body is in hemoglobin, 3% in myoglobin, and the rest in ferritin, which is present not only in enterocytes but also in many other cells. Apoferritin is a globular protein made up of 24 subunits. Iron forms a micelle of ferric hydroxyphosphate, and in ferritin, the subunits surround this micelle. The ferritin micelle can contain as many as 4500 atoms of iron. Ferritin molecules in lysosomal membranes may aggregate in deposits that contain as much as 50% iron. These deposits are called hemosiderin. 10 Blood physiology by prof.Israa F.Jafar Intestinal absorption of iron is regulated by three factors: 1. Recent dietary intake of iron. 2. The state of the iron stores in the body. 3. The state of erythropoiesis in the bone marrow. Iron overload causes hemosiderin to accumulate in the tissues, producing hemosiderosis. Large amounts of hemosiderin can damage tissues, causing hemochromatosis.This syndrome is characterized by pigmentation of the skin, pancreatic damage with diabetes ("bronze diabetes"), cirrhosis of the liver, a high incidence of hepatic carcinoma, and gonadal atrophy. 11 Blood physiology by prof.Israa F.Jafar Blood Transfusions and Blood Typing Transfusion of Blood 1. Whole blood transfusion - all cells and plasma; anticoagulants (citrate and oxalate salts) used 2. Packed red blood cells - most of the plasma has been removed prior to transfusion Human Blood Groups: 1. Agglutinogens - glycoproteins on the surface of blood cells; causes "agglutination" (clumping) 2. ABO Blood Groups - determined by presence or absence of Type A and Type B agglutinogen proteins on cell membrane TYPE type A type B type AB type O GENES A/A, A/O, O/A B/B, B/O, O/B A/B or B/A no A or B PEOPLE (30-40%) (l0-30%) (3-5%) (40-50%) Antibodies Anti-B Anti-A none Anti-A, Anti-B Receive Blood from: A, O B,O A, B, AB, O O only 3. agglutinins - antibodies against either A or B agglutinogen a. transfusion reaction - patient's antibodies attack the donor blood i. A (anti-B) receives A,O (not B) ii. B (anti-A) receives B,O (not A) iii. AB (none) receives A, B, AB, O universal recipient iv. O (anti-A,anti-B) receives O universal donor b. agglutination - when incorrect blood transfused, antibodies will "clump" new blood after clumping, RBCs may rupture(hemolysis), releasing hemoglobin this Hb is harming to the kidneys & can lead to renal shutdown . 4. Blood Typing - mixing Donors Blood with Recipient Antibodies (Anti-A, Anti-B, anti-Rh) in order to identify agglutination 5. Expanding Blood Volume to Avoid Shock by either pure plasma without antibodies or by plasma expanders - purified human serum albumin, plasminate, dextran or by isotonic saline - normal electrolyte solution isotonic to blood plasma (Ringer's Solution) 12 Blood physiology by prof.Israa F.Jafar The Rh Group The "Rh factor," named for the rhesus monkey because it was first studied using the blood of this animal, is a system composed primarily of the C, D, and E antigens, although it actually contains many more. Unlike the ABO antigens, the system has not been detected in tissues other than red cells. D is by far the most antigenic component, and the term "Rh-positive" as it is generally used means that the individual has agglutinogen D. The "Rh-negative" individual has no D antigen and forms the anti-D agglutinin when injected with D-positive cells. The Rh typing serum used in routine blood typing is anti-D serum. Eighty-five percent of Caucasians are D-positive and 15% are D-negative; over 99% of Asians are D-positive. Unlike the antibodies of the ABO system, anti-D antibodies do not develop without exposure of a D-negative individual to D-positive red cells by transfusion or entrance of fetal blood into the maternal circulation. However, D-negative individuals who have received a transfusion of D-positive blood (even years previously) can have appreciable anti-D titers and thus may develop transfusion reactions when transfused again with D-positive blood. Hemolytic Disease of the Newborn Another complication due to "Rh incompatibility" arises when an Rh-negative mother carries an Rh-positive fetus. Small amounts of fetal blood leak into the maternal circulation at the time of delivery, and some mothers develop significant titers of anti-Rh agglutinins during the postpartum period. During the next pregnancy, the mother's agglutinins cross the placenta to the fetus. In addition, there are some cases of fetal-maternal hemorrhage during pregnancy, and sensitization can occur during pregnancy. In any case, when anti-Rh agglutinins cross the placenta to an Rh-positive fetus, they can cause hemolysis and various forms of hemolytic disease of the newborn (erythroblastosis fetalis). If hemolysis in the fetus is severe, the infant may die in utero or may develop anemia, severe jaundice, and edema (hydrops fetalis). Kernicterus, a neurologic syndrome in which unconjugated bilirubin is deposited in the basal ganglia, may also develop, especially if birth is complicated by a period of hypoxia. Bilirubin rarely penetrates the brain in adults, but it does in infants with erythroblastosis, possibly in part because the blood-brain barrier is more permeable in infancy. However, the main reasons that the concentration of unconjugated bilirubin is very high in this condition are that production is increased and the bilirubin-conjugating system is not yet mature. About 50% of Rh-negative individuals are sensitized (develop an anti-Rh titer) by transfusion of Rh-positive blood. Since sensitization of Rh-negative mothers by carrying an Rh-positive fetus generally occurs at birth, the first child is usually normal. However, hemolytic disease occurs in about 17% of the Rh-positive fetuses born to Rh-negative mothers who have previously been pregnant one or more times with Rh-positive fetuses. Fortunately, it is usually possible to prevent sensitization from occurring the first time by administering a single dose of anti-Rh antibodies in the form of Rh immune globulin during the postpartum period. Such passive immunization does not harm the mother and has been demonstrated to 13 Blood physiology by prof.Israa F.Jafar prevent active antibody formation by the mother. In obstetric clinics, the institution of such treatment on a routine basis to unsensitized Rh-negative women who have delivered an Rhpositive baby has reduced the overall incidence of hemolytic disease by more than 90%. In addition, fetal Rh typing with material obtained by amniocentesis or chorionic villus sampling is now possible, and treatment with a small dose of Rh immune serum will prevent sensitization during pregnancy. Platelets (thrombocytes - "clotting") The platelets are small, granulated bodies that aggregate at sites of vascular injury. They lack nuclei and are 2-4 um in diameter . There are about 300,000/uL of circulating blood, and they normally have a half-life of about 4 days. The megakaryocytes, giant cells in the bone marrow, form platelets by pinching off bits of cytoplasm and extruding them into the circulation. Between 60% and 75% of the platelets that have been extruded from the bone marrow are in the circulating blood, and the remainder are mostly in the spleen. Splenectomy causes an increase in the platelet count (thrombocytosis). Platelets have a ring of microtubules around their periphery and an extensively invaginated membrane with an intricate canalicular system in contact with the ECF. Their membranes contain receptors for collagen, ADP, vessel wall von Willebrand factor . and fibrinogen. Their cytoplasm contains actin, myosin, glycogen, lysosomes, and two types of granules: (1) dense granules, which contain the nonprotein substances that are secreted in response to platelet activation, including serotonin, ADP and other adenine nucleotides, (2) α-granules, which contain secreted proteins other than the hydrolases in lysosomes. These proteins include clotting factors and platelet-derived growth factor (PDGF). PDGF is also produced by macrophages and endothelial cells. PDGF stimulates wound healing and is a potent mitogen for vascular smooth muscle. Platelet production is regulated by : 1. colony- stimulating factors that control the production of megakaryocytes. 2. thrombopoietin, a circulating protein factor. This factor, which facilitates megakaryocyte maturation Thrombocytopenic purpura When the platelet count is low, clot retraction is deficient and there is poor constriction of ruptured vessels. The resulting clinical syndrome (thrombocytopenic purpura) is characterized by easy bruisability and multiple subcutaneous hemorrhages. Purpura may also occur when the platelet count is normal, and in some of these cases, the circulating platelets are abnormal (thrombasthenic purpura). Individuals with thrombocytosis (increased number of platelets) are predisposed to thrombotic events 14 Blood physiology by prof.Israa F.Jafar Hemostasis (stoppage of blood flow after damage) Steps of hemostasis:1. Vascular spasms (vasoconstriction at injured site) 2. Platelet plug formation (plugging the hole) 3. Coagulation (blood clotting - complex mechanism) Vascular Spasms: first response to vascular injury - vasoconstriction is stimulated by: a. compression of vessel by escaping blood b. injury "chemicals" released by injured cells c. reflexes from adjacent pain receptors Formation of a Platelet Plug 1. damage to endothelium of vessel 2. platelets become spiky and sticky in response 3. platelets attach to damaged vessel wall to plug it 4. platelets produce thromboxane A2 - granule release 5. serotonin release enhances vascular spasm 6. ADP - attracts and stimulates platelets at site 7. prostacylin - inhibits aggregation at other sites Platelet aggregation: When a blood vessel wall is injured, platelets adhere to the exposed collagen and von Willebrand factor in the wall via the receptors on the platelet membrane. Binding produces platelet activations which release the contents of their granules. The released ADP acts on the ADP receptors in the platelet membranes to produce further accumulation of more platelets Coagulation (blood clotting) General Events in Clotting Is shown in the diagram 15 Blood physiology by prof.Israa F.Jafar 16 Blood physiology by prof.Israa F.Jafar Fibrinolysis Blue arrows = stimulation; red arrows = inhibition. tPA is released by damaged endothelium 17 Blood physiology by prof.Israa F.Jafar summary: 1. anticoagulant - chemical that inhibits clotting 2. procoagulant - chemical that promotes clotting 3. intrinsic pathway - within the damaged vessel a. more procoagulants needed (I-XIII) toward PF3 and Factor X b. allows more "scrutiny" before clotting occurs 4.extrinsic pathway - in outer tissues around vessel a tissue thromboplastin (Tissue Factor) - skips intrinsic steps straight to PF3 and Fac X b. allows rapid response to bleeding out of vessel (clot can form in 10 to 15 seconds) 5. After activation of Factor X, common pathway: Factor X, PF3 (thromboplastin), Factor V, Ca++ --> prothrombin activator -> prothrombin converted -> thrombin (active enzyme) thrombin stimulates: fibrinogen -> fibrin (meshwork) Ca++ & thrombin -> Factor XIII (fibrin stabilizer) Clot Retraction (shrinking of clot) 1.actomyosin - causes contraction of platelets 2.blood serum - plasma WITHOUT clotting Factors 3.platelet-derived growth factor (PDGF) - stimulates fibroblast migration and endothelial growth Clot Eradication (Fibrinolysis) 1.healing occurs over 2 - 10 days 2.tissue plasminogen activator (TPA) - causes the activation of plasminogen 3.plasminogen--> plasmin 4.plasmin degrades proteins within the clot Factors Limiting Growth and Formation of Clots 1. Limiting Normal Clot Growth a. blood moves too fast to allow procoagulants b. factors interfere with normal clotting i.prothrombin III - deactivates thrombin ii.protein C - inhibits clotting Factors iii.heparin - inhibits thrombin; prevents adherence of platelets to injured site 18 Blood physiology by prof.Israa F.Jafar Disorders of Hemostasis A. Thromboembolytic Disorders (undesirable clotting) 1. Thrombus - blood clot in normal blood vessel 2. Embolus -blood clot/gas bubble floating in blood a.TPA, streptokinase - can dissolve a clot b.aspirin - inhibits Thromboxane formation c.heparin - inhibits thrombin & platelet deposit d.dicumarol - anticoagulant, blocks Vitamin K B. Bleeding Disorders 1.thrombocytopenia - reduced platelet count; generally below 50,000 per cubic millimeter; can cause excessive bleeding from vascular injury 2.impaired liver function - lack of procoagulants (Clotting Factors) that are made in liver a. vitamin K - essential for liver to make Clotting Factors for coagulation 3.hemophilias - hereditary bleeding disorders that occur almost exclusively in males a. hemophilia A - defective Factor VIII (83%) b. hemophilia B - defective Factor IX (10%) c. now genetically engineered TPA and Factor VIII are produced so patients do not need transfusions as often. White Blood Cell Count (WBC) and Differential White blood cells, or leukocytes, are classified into two main groups: granulocytes and nongranulocytes (also known as agranulocytes). General Structure and Function 1. protection from microbes, parasites, toxins, cancer 2. 1% of blood volume; 4-11,000 per cubic mm blood 3 diapedesis - can "slip between" capillary wall 4. amoeboid motion - movement through the body 19 Blood physiology by prof.Israa F.Jafar 5. chemotaxis - moving in direction of a chemical 6. leukocytosis - increased "white blood cell count" in response to bacterial/viral infection The granulocytes, which include neutrophils, eosinophils, and basophils, have granules in their cell cytoplasm. Neutrophils, eosinophils, and basophils also have a multilobed nucleus. As a result they are also called polymorphonuclear leukocytes or "polys." The nuclei of neutrophils also appear to be segmented, so they may also be called segmented neutrophils or "segs." The nongranuloctye white blood cells, lymphocytes and monocytes, do not have granules and have nonlobular nuclei. They are sometimes referred to as mononuclear leukocytes. The lifespan of white blood cells ranges from 13 to 20 days, after which time they are destroyed in the lymphatic system. When immature WBCs are first released from the bone marrow into the peripheral blood, they are called "bands" or "stabs." Leukocytes fight infection through a process known as phagocytosis. During phagocytosis, the leukocytes surround and destroy foreign organisms. White blood cells also produce, transport, and distribute antibodies as part of the body's immune response. 1. Neutrophils - destroy and ingest bacteria & fungi (polymorphonuclear leuks.; "polys") a. most numerous WBC b. defensins - antibiotic-like proteins (granules) c. polymorphonuclear - many-lobed nuclei d. causes lysis of infecting bacteria/fungi e. HIGH poly count --> likely infection 2. eosinophils - lead attack against parasitic worms a. only 1-4% of all leukocytes b. two-lobed, purplish nucleus c. acidophilic (red) granules with digest enzymes d. phagocytose antigens & antigen/antibody complex e. inactivate chemicals released during allergies 3. basophils - releases Histamine which causes inflammation, vasodilation, attraction of WBCs a.RAREST of all leukocytes (0.5%) b.deep purple U or S shaped nucleus c.basophilic (blue) granules with HISTAMINE d.related to "mast cells" of connective tissue e.BOTH release Histamine with "IgE" signal f.antihistamine - blocks the action of Histamine in response to infection or allergic antigen 20 Blood physiology by prof.Israa F.Jafar Agranulocytes - WBCs without granules in cytoplasm 1. lymphocytes - two types of lymphocytes a. T lymphocytes - (thymus) respond against virus infected cells and tumor cells. b. B lymphocytes - (bone) differentiate into different "plasma cells" which each produce antibodies against different antigens c. lymphocytes primarily in lymphoid tissues d. very large basophilic (purple) nucleus e. small lymphocytes in blood (5-8 microns) f. larger lymphocytes in lymph organs (10-17 mic) 2. monocytes - differentiate to become macrophages; serious appetites for infectious microbes a. largest of all leukocytes (18 microns) b. dark purple, kidney shaped nucleus Leukopoiesis and Colony Stimulating Factors (CSFs) 1. leukopoiesis - the production, differentiation, and development of white blood cells all cells derived from hemocytoblast 2. colony stimulating factors (CSF) - hematopoietic hormones that promote leukopoiesis a. produced by Macrophages and T lymphocytes i. macrophage-monocyte CSF (M-CSF) ii. granulocyte CSF (G-CSF) iii. granulocyte-macrophage CSF (GM-CSF) iv. multi CSF (multiple lymphocyte action) v. interleukin 3 (IL-3) (general lymphocytes) Two measurements of white blood cells are commonly done in a CBC: -the total number of white blood cells in a microliter (1x10 -9 liters) of blood, reported as an absolute number of "X" thousands of white blood cells, and -The percentage of each of the five types of white blood cells. This test is known as a differential and is reported in percentages. Normal values for total WBC and differential in adult males and females are: Total WBC: 4,000 - 11,000 Bands or stabs: 3 - 5 % Granulocytes (or polymorphonuclears) 21 Blood physiology by prof.Israa F.Jafar o Neutrophils : 50 - 70% relative value (2500-7000 absolute value) o Eosinophils: 1 - 3% relative value (100-300 absolute value) o Basophils: 0.4% - 1% relative value (40-100 absolute value) Agranulocytes (or mononuclears) o Lymphocytes: 25 - 35% relative value (1700-3500 absolute value) o Moncytes: 4 - 6% relative value (200-600 absolute value) Each differential always adds up to 100%. To make an accurate assessment, consider both relative and absolute values. For example a relative value of 70% neutrophils may seem within normal limits; however, if the total WBC is 20,000, the absolute value (70% x 20,000) would be an abnormally high count of 14,000. Q (It is important to consider both the relative and absolute values of various types of white blood cells when interpreting a WBC differential. True, False) The numbers of leukocytes changes with age and during pregnancy. On the day of birth, a newborn has a high white blood cell count, ranging from 9,000 to 30,000 leukocytes. This number falls to adult levels within two weeks. The percentage of neutrophils is high for the first few weeks after birth, but then lymphocyte predominance is seen. Until about 8 years of age, lymphocytes are more predominant than neutrophils. In the elderly, the total WBC decreases slightly. Pregnancy results in a leukocytosis, primarily due to an increase in neutrophils with a slight increase in lymphocytes. Leukocytosis, a WBC above 10,000, is usually due to an increase in one of the five types of white blood cells and is given the name of the cell that shows the primary increase. Neutrophilic leukocytosis = neutrophilia Lymphocytic leukocytosis = lymphocytosis Eosinophilic leukocytosis = eosinophilia Monocytic leukocytosis = monocytosis Basophilic leukocytosis = basophilia 22 Blood physiology by prof.Israa F.Jafar In response to an acute infection, trauma, or inflammation, white blood cells release a substance called colony-stimulating factor (CSF). CSF stimulates the bone marrow to increase white blood cell production. In a person with normally functioning bone marrow, the numbers of white blood cells can double within hours if needed. An increase in the number of circulating leukocytes is rarely due to an increase in all five types of leukocytes. When this occurs, it is most often due to dehydration and hemoconcentration. In some diseases, such as measles, pertussis and sepsis, the increase in white blood cells is so dramatic that the picture resembles leukemia. Leukemoid reaction, leukocytosis of a temporary nature, must be differentiated from leukemia, where the leukocytosis is both permanent and progressive. Therapy with steroids modifies the leukocytosis response. When corticosteroids are given to healthy persons, the WBC count rises. However, when corticosteroids are given to a person with a severe infection, the infection can spread significantly without producing an expected WBC rise. An important concept to remember is that, leukocytosis as a sign of infection can be masked in a patient taking corticosteroids. Q (Corticosteroids can mask infection by suppressing the inflammatory response and the release of WBCs. True, False Leukopenia occurs when the WBC falls below 4,000. Viral infections, overwhelming bacterial infections, and bone marrow disorders can all cause leukopenia. Patients with severe leukopenia should be protected from anything that interrupts skin integrity, placing them at risk for an infection that they do not have enough white blood cells to fight. For example, leukopenic patients should not have intramuscular injections, rectal temperatures or enemas. A WBC of less than 500 places the patient at risk for a fatal infection. A WBC over 30,000 indicates massive infection or a serious disease such as leukemia. Immune System Innate Immune System I. Parts of the Immune System A. Innate or Nonspecific system 1. External body membranes like skin and mucosae i. prevents physical entry of microorganisms ii. first line of defense 2. Phagocytes, antimicrobial proteins, inflammation i. activated by chemical signals when external defenses are penetrated ii. Second line of defense B. Adaptive or Specific system 1. Main components are the B and T lymphocytes i. B-lymphocytes involved in humoral or antibody-mediated immunity 23 Blood physiology by prof.Israa F.Jafar ii. T-lymphocytes involved in cellular or cell-mediated immunity 2. Takes considerable time but is highly specific i. this is the body’s third line of defense C. Functional System 1. has organs that are involved in the immune response but involves trillions of individual immune cells 2. the immune system confers immunity which is resistance to disease II. Innate defenses A. Function 1. combat pathogens which are harmful or disease-causing microorganisms 2. in a state of readiness and responds to protect the body from ALL foreign substances starting within minutes of invasion. B. Surface Barriers 1. Skin i. heavily keratinized epithelial membrane is a physical barrier ii. resistant to most weak acids, weak bases, bacterial enzymes and toxins. iii. secretions are acidic (pH 3-5) and inhibit bacterial growth iv. sebum contains chemicals that are toxic to bacteria 2. Mucous membranes i. line all body cavities that open to the exterior including the digestive, respiratory, urinary, and reproductive tracts ii. stomach secretes HCl and protein-digesting enzymes which kill microorganisms. iii. Saliva and lacrimal fluid contains lysozyme, an enzyme that destroys bacteria. iv. Sticky mucus traps microorganism that enter the digestive and respiratory passageways. v. structure modifications such as the tiny mucus-coated hairs and ciliated mucosa of the respiratory tract which trap and sweep particles away from lower respiratory passages. 3. When surface barriers are breached by small nicks or cuts then the microorganisms invade deeper tissues and the internal innate defenses are important C. Internal Defenses 1. Nonspecific and consists of phagocytes, natural killer cells, antimicrobial proteins, fever, and the inflammatory response which includes macrophages, mast cells, and all types of white blood cells. 2. Phagocytes i. cells that engulf or “eat” pathogens 24 Blood physiology by prof.Israa F.Jafar ii. mainly macrophages a. derived from monocytes which leave the bloodstream and enter tissue and enlarge. b. can roam tissues search for cellular debris or “foreign invaders” like alveolar macrophages of the lungs or dendritic cells of the epidermis. c. can be fixed like Kupffer cells in the liver or microglia of the brain iii. neutrophils a. most abundant type of white blood cell b. may become phagocytic upon exposure to infectious material c. secrete defensins, which are antibiotic-like chemicals d. can release oxidizing and bleach-like chemicals which can destroy cells, including themselves e. prolonged activity may cause normal tissues to become cancerous iv. eosinophils a. weak phagocytes but are important against parasitic worms b. discharges destructive contents of cytoplasmic granules v. mast cells a. involved in allergies but have some phagocytic capabilities 3. Mechanism of Phagocytosis i. Ameoba-like digestion: phagocyte engulfs particle using flowing cytoplasmic extensions the particle is enclosed within a membrane-lined vacuole called a phagosome a lysosome fuses with the phagosome to form a phagolysosome pathogen killed and digested within the phagolysosome indigestible waste is removed by exocytosis ii. requires adherence of the particle to the phagocyte a. carbohydrate signatures b. pneumococcus has a capsule which makes adherence difficult c. opsonization, which is the coating of foreign particles with complement proteins and antibodies, increases adherence iii. some pathogens can survive lysosomal enzymes and can multiply within the vacuole. a. respiratory burst can be activated by adaptive immune systemchemicals that produce free radicals, like nitric oxide, which can kill cells. 4. Natural Killer Cells i. in the blood and lymph ii. can kill and lyse cancer cells and virus-infected body cells iii. belong to the group large granular lymphocytes 25 Blood physiology by prof.Israa F.Jafar iv. recognize surface sugars but are fairly nonspecific v. not phagocytic, but release cytolytic chemicals called perforins vi. secrete chemicals that enhance the inflammatory response 5. Inflammation i. triggered by body tissue injuries like physical trauma, heat, irritating chemicals, infection by viruses, fungi, and bacteria. ii. functions to: a. prevents spread of damaging agents b. disposes of cell debris and pathogens c. sets the stage for repair processes iii. signs of inflammation are redness, heat, swelling, pain, and sometimes impairment of function. iv. begins with the release of inflammatory chemicals called inflammatory mediators into the extracellular fluid a. can come from injured tissue cells, phagocytes, lymphocytes, mast cells, and blood proteins v. main inflammatory mediators are histamine, kinins, prostaglandins, complement, and cytokines a. cause vasodilation and hyperemia, which is congestion with blood, that is responsible for the redness and heat b. increase permeability of local capillaries i.fluid containing proteins like clotting factors and antibodies, called exudates, flows from the bloodstream into tissue spaces ii. local edema occurs and pain is triggered vi. edema can be beneficial a. helps to dilute harmful substances that may be present b. brings in large quantities of oxygen and nutrients needed for repair. c. allows entry of clotting proteins which forms a fibrin mesh that prevents the spread of harmful agents. vii. increases the production of -defensins, which are antibiotic-like chemicals. 6. Phagocyte mobilization i. sequence: mast cells neutrophils macrophages ii. leukocytosis is first and chemicals called leukocytosis-inducing factors are released from injured cells to promote neutrophil release from red bone marrow. iii. margination is the process of cell adhesion molecules (CAMs) of neutrophils binding to cell adhesion molecules (CAMs) called selectins of the endothelial cells of capillary walls causing the neutrophils to cling to the capillary wall. 26 Blood physiology by prof.Israa F.Jafar iv. diapedesis is the process of neutrophils emigrating through the capillary walls to the site of inflammation. v. chemotaxis is the attraction of neutrophils and other white blood cells to the site of injury due to inflammatory chemicals called chemotactic agents. vi. monocytes become macrophages about 8-12 hours after entering the tissues. Macrophages are dominant at sites of chronic inflammation. 7. Pus is a mixture of dead or dying neutrophils, broken-down tissue cells, and living and dead pathogens. 8. Abscesses are sacs of pus walled off by collagen fibers 9. Infection granulomas are tumorlike growths containing macrophages infected by pathogens “hiding” within it surrounded by uninfected macrophages and an outer fibrous capsule. 10. Antimicrobial proteins i. attack microorganisms directly or inhibit their ability to reproduce ii. interferon a. different types like , , and -interferon b. are small proteins which “interferes” with viral replication. c. not virus specific d. comes from lymphocytes e. comes from most other leukocytes f. comes from fibroblasts g. activates macrophages and mobilizes natural killer cells h. play an anticancer role i. is used to treat genital warts and can combat Hep C 11. Complement system i. group of at least 20 plasma proteins that destroy foreign substances by lysis when activated. ii. amplifies the inflammatory process iii. there is a classical pathway and an alternative pathway that both lead to the activation of C3, one of the complement proteins, which is then cleaved into two subunits which can cause inflammation and opsonization. iv. MAC is the membrane attack complex which inserts into the membrane of the target cell and inhibits the cell’s ability to eject Ca+2 and causes lysis 12. Fever i. body temperature is controlled by hypothalamic neurons and is set to about 36.2 C ii. fever occurs when pyrogens, chemicals secreted by leukocytes and macrophages exposed to foreign matter, resets the neurons higher. iii. high fevers can denature enzymes iv. fevers are helpful because it speeds up the metabolic rate of tissue cells and 27 Blood physiology by prof.Israa F.Jafar cause the liver and spleen to contain iron and zinc, which bacteria require in large amounts to multiply 28 Blood physiology by prof.Israa F.Jafar Immune System Adaptive Immune System I. Adaptive or Specific Immune System General Characteristics 1. Specific so that it can eliminate with equal precision almost any type of pathogen 2. Functional System a. can eliminate specific foreign substances as well as abnormal body cells b. can magnify the inflammatory response i. responsible for most complement activation 3. Must be primed by an initial exposure to a specific foreign substance called an antigen a. takes time important findings about the adaptive immune response a. antigen-specific b. systemic c. has “memory” Two branches of adaptive immunity 1. Humoral immunity or antibody-mediated immunity consists of antibodies circulating in the fluids of the body a. produced by lymphocytes or their offspring 2. Cellular or cell-mediated immunity – lymphocytes themselves a. Targets – virus or parasite-infected tissue cells, cancer cells, foreign graft cells b. can act directly by lysing foreign cells or indirectly by releasing chemicals that enhance the inflammatory response or activate other lymphocytes or macrophages. II. Antigens Antigens vs. Haptens:1. Antigens – substances that can mobilize the immune system and provoke an immune response a. most large, complex molecules that are NOT normally present in the body b. help distinguish “self” from “nonself” 2. Complete antigens formation of specific b. a. they have immunogenicity – the ability to stimulate lymphocytes and antibody production have reactivity – the ability to react with the lymphocytes and antibodies 29 Blood physiology by prof.Israa F.Jafar c. 3. antigens include nearly all foreign proteins, nucleic acids, lipids, and many large polysaccharides. proteins are the strongest antigens d. other antigens can be pollen grains or microorganisms e. generally small molecules like peptides, nucleotides, and many hormones are NOT immunogenic f. these small particles can link with other substances though and become immunogenic allergies Haptens – small molecules that are reactive but not immunogenic unless attached to a protein carrier Cytokines Cytokines are hormone-like molecules that actto regulate immune responses. They are secreted not only by lymphocytes and macrophages but by endothelial cells, neurons, glial cells, and other types of cells. Most of the cytokines are initially named for their actions, eg, B cell-differentiating factor, B cell-stimulating factor 2. However, there is a convention that once the amino acid sequence of a factor in humans is known, its name is changed to interleukin. Thus, for example, the name of B cell- differentiating factor was changed to interleukin-4(IL4). The effects of the principal cytokines Some of them have systemic as well as local effects. For example, IL-1, IL-6, and tumor necrosis factor α cause fever, and IL-1 increases slowwave sleep and reduces appetite. Another superfamily of cytokines is the chemokine family. Chemokines are substances that attract neutrophils and other white blood cells to areas of inflammation or immune response. The Complement System The cell-killing effects of innate and acquired immunity are mediated in part by a system of plasma enzymes originally named the complement system because they "complemented" the effects of antibodies. Nomenclature for the over 30 proteins in the system is confusing because it is a mixture of letters and numbers: examples include C1q, C3, and C3b. Three different pathways or enzyme cascades activate the system: the classic pathway, triggered by immune complexes; the mannose-binding lectin pathway, triggered when this lectin binds mannose groups in bacteria; and the alternative or properdin pathway, triggered by contact with various viruses, bacteria, fungi, and tumor cells. The proteins that are produced have three functions: They help kill invading organisms by opsonization, chemotaxis, and eventual lysis of the cells; they serve in part as a bridge from innate to acquired immunity by 30 Blood physiology by prof.Israa F.Jafar activating B cells and aiding immune memory; and they help dispose of waste products after apoptosis. Cell lysis, one of the principal ways the complement system kills cells, is brought about by inserting proteins called perforins into their cell membranes. The holes produced in this fashion permit free flow of ions, with disruption of membrane polarity. Innate Immunity The cells that mediate innate immunity include neutrophils, macrophages, and natural killer (NK) cells, large lymphocytes that are not T cells but are cytotoxic. All these cells respond to lipid and carbohydrate sequences unique to bacterial cell walls and to other substances characteristic of tumor and transplant cells. They exert their effects by way of the complement and other systems, with the cells they attack frequently dying by osmotic lysis or apoptosis. Their cytokines also activate cells of the acquired immune system. Acquired Immunity the key to acquired immunity is the ability of lymphocytes to produce antibodies that are specific for one of the many millions of foreign agents that may invade the body. The antigens stimulating antibody production are usually proteins and polypeptides, but antibodies can also be formed against nucleic acids and lipids if these are presented as nucleoproteins and lipoproteins, and antibodies to smaller molecules can be produced experimentally when the molecules are bound to protein. Acquired immunity has two components: humoral immunity and cellular immunity. Humoral immunity is mediated by circulating immunoglobulin antibodies in the γ-globulin fraction of the plasma proteins. Immunoglobulins are produced by B lymphocytes, and they activate the complement system and attack and neutralize antigens. Humoral immunity is a major defense against bacterial infections. Cellular immunity is mediated by T lymphocytes. It is responsible for delayed allergic reactions and rejection of transplants of foreign tissue. Cytotoxic T cells attack and destroy cells that have the antigen which activated them. They kill by inserting perforins (see above) and by initiating apoptosis. Cellular immunity constitutes a major defense against infections due to viruses, fungi, and a few bacteria such as the tubercle bacillus. It also helps defend against tumors. Development of the Immune System During fetal development, lymphocyte precursors come from the bone marrow. Those that populate the thymus become transformed by the environment in this organ into the lymphocytes responsible for cellular immunity (T lymphocytes). humoral immunity (B lymphocytes the transformation to B lymphocytes occurs in bursal 31 Blood physiology by prof.Israa F.Jafar equivalents, ie, the fetal liver and, after birth, the bone marrow. After residence in the thymus or liver, many of the T and B lymphocytes migrate to the lymph nodes and bone marrow. Most of the processing occurs during fetal and neonatal life. However, there is also a slow, continuous production of new lymphocytes from stem cells in adults. T and B lymphocytes are morphologically indistinguishable but can be identified by markers on their cell membranes. B cells differentiate into plasma cells and memory B cells. There are three major types of T cells: cytotoxic T cells, helper T cells, and memory T cells. There are two subtypes of helper T cells: T helper 1 (TH1) cells secrete IL-2 and γinterferon and are concerned primarily with cellular immunity; T helper 2 (TH2) cells secrete IL-4 and IL-5 and interact primarily with B cells in relation to humoral immunity. Cytotoxic T cells destroy transplanted and other foreign cells, with their development aided and directed by helper T cells. Markers on the surface of lymphocytes are assigned CD (clusters of differentiation) numbers on the basis of their reactions to a panel of monoclonal antibodies. Most cytotoxic T cells display the glycoprotein CD8, and helper T cells display the glycoprotein CD4. These proteins are closely associated with the T cell receptors and may function as coreceptors. Natural killer cells are also cytotoxic lymphocytes, though they are not T cells. Memory B Cells & T Cells After exposure to a given antigen, a small number of activated B and T cells persist as memory B and T cells. These cells are readily converted to effector cells by a later encounter with the same antigen. This ability to produce an accelerated response to a second exposure to an antigen is a key characteristic of acquired immunity. The ability persists for long periods of time, and in some instances (eg, immunity to measles) it can be lifelong. After activation in lymph nodes, lymphocytes disperse widely throughout the body and are especially plentiful in areas where invading organisms enter the body, eg, the mucosa of the respiratory and gastrointestinal tracts. This puts memory cells close to sites of reinfection and may account in part for the rapidity and strength of their response. Chemokines are involved in guiding activated lymphocytes to these locations. It had been argued that the long life of memory cells involves their repeated exposure to small amounts of antigen. However, memory cells persist when infused into mice in which the ability to process the antigen to which they are sensitive has been abolished by gene knockout. It may be that they avoid apoptosis by taking up nerve growth factor in the peripheral tissues. Antigen Recognition 32 Blood physiology by prof.Israa F.Jafar The number of different antigens recognized by lymphocytes in the body is extremely large. The recognition ability is innate and develops without exposure to the antigen. Stem cells differentiate into many million different T and B lymphocytes, each with the ability to respond to a particular antigen. When the antigen first enters the body, it can bind directly to the appropriate receptors on B cells. However, a full antibody response requires that the B cells contact helper T cells. In the case of T cells, the antigen is taken up by an antigenpresenting cell and partially digested. A peptide fragment of it is presented to the appropriate receptors on T cells. In either case, the cells are stimulated to divide, forming clones of cells that respond to this antigen (clonal selection). Antigen Presentation Antigen-presenting cells (APCs) include specialized cells called dendritic cells in the lymph nodes and spleen and the Langerhans dendritic cells in the skin. Macrophages and B cells themselves can also function as APCs. In APCs, polypeptide products of antigen digestion are coupled to protein products of the major histocompatibility complex (MHC) genes and presented on the surface of the cell. The products of the MHC genes are called human leukocyte antigens (HLA). The class I MHC proteins (MHC-I proteins) are coupled primarily to peptide fragments generated from proteins synthesized within cells. The peptides to which the host is not tolerant, eg, those from mutant or viral proteins, are recognized by T cells. The class II MHC proteins (MHC-II proteins) are concerned primarily with peptide products of extracellular antigens, such as bacteria, that enter the cell by endocytosis and are digested in the late endosomes. 33 Blood physiology by prof.Israa F.Jafar n the upper pathway; foreign protein or antigen (1) is taken up by an antigen-presenting cell (2). The antigen is processed and displayed on an MHC II molecule (3), which interacts with a T helper cell (4). In the lower pathway; whole foreign proteins are bound by membrane antibodies (5) and presented to B lymphocytes (6), which process (7) and present antigen on MHC II (8) to a previously activated T helper cell (10), spurring the production of antigen-specific antibodies (9). 34 Blood physiology by prof.Israa F.Jafar Antigen presentation stimulates T cells to become either "cytotoxic" CD8+ cells or "helper" CD4+ cells. T Cell Receptors The MHC protein-peptide complexes on the surface of the antigen-presenting cells bind to appropriate T cells. Therefore, receptors on the T cells must recognize a very wide variety of complexes. CD8 occurs on the surface of cytotoxic T cells that bind MHC-I proteins. CD4 occurs on the surface of helper T cells that bind MHC-II proteins The CD8 and CD4 proteins facilitate the binding of the MHC proteins to the T cell receptors. The activated CD8 cytotoxic T cells kill their targets directly, whereas the activated CD4 helper T cells secrete cytokines that activate other lymphocytes. B Cells B cells can bind antigens directly, but they must contact helper T cells to produce full activation and antibody formation. It is the TH2 subtype that is mainly involved. Helper T cells are pushed along the TH2 line by the cytokine IL-4 . On the other hand, IL-12 pushes helper T cells along the TH1 line. IL-2 acts in an autocrine 35 Blood physiology by prof.Israa F.Jafar fashion to cause activated T cells to proliferate. The activated B cells proliferate and transform into memory B cells (see above) and plasma cells. The plasma cells secrete large quantities of antibodies into the general circulation. The antibodies circulate in the globulin fraction of the plasma (see below) and, like antibodies elsewhere, are called immunoglobulins. The immunoglobulins are actually the secreted form of antigen-binding receptors on the B cell membrane. Immunoglobulins Circulating antibodies protect their host by binding to and neutralizing some protein toxins, by blocking the attachment of some viruses and bacteria to cells, by opsonizing bacteria and by activating complement. Five general types of immunoglobulin antibodies are produced by the lymphocyte-plasma cell system. The basic component of each is a symmetric unit containing four polypeptide chains The two long chains are called heavy chains, whereas the two short chains are called light chains. There are two types of light chains, κ and λ, and eight types of heavy chains. The chains are joined by disulfide bridges that permit mobility, and there are intrachain disulfide bridges as well. In addition, the heavy chains are flexible in a region called the hinge. Each heavy chain has a variable (V) segment in which the amino acid sequence is highly variable, a diversity (D) segment in which the amino acid segment is also highly variable, a joining (J) segment in which it is moderately variable, and a constant (C) segment in which the sequence is constant. Each light chain has a V, a J, and a C segment. The V segments form part of the antigen-binding sites (Fab portion of the molecule). The Fc portion of the molecule is the effector portion, which mediates the reactions initiated by antibodies. Two of the classes of immunoglobulins contain additional polypeptide components : IgMs, five of the basic immunoglobulin units join around a polypeptide called the J chain to form a pentamer. IgAs, the secretory immunoglobulins, the immunoglobulin units form dimers and trimers around a J chain and a polypeptide that comes from epithelial cells, the secretory component (SC). 36 Blood physiology by prof.Israa F.Jafar 37 Blood physiology by prof.Israa F.Jafar 1. IgG - Gamma heavy chains 2. IgM - Mu heavy chains 3. IgA - Alpha heavy chains 4. IgD - Delta heavy chains 5. IgE - Epsilon heavy chains Recognition of Self A key question is why T and B cells do not form antibodies against and destroy the cells and organs of the individual in which they develop. Current evidence indicates that self antigens are presented along with nonself antigens but are then eliminated during development (tolerance). Central tolerance occurs in the thymus for T cells and the bone marrow for B cells. This is supplemented by peripheral tolerance occurring in the lymph nodes and elsewhere in the body. Autoimmunity Sometimes the processes that eliminate antibodies against self antigens fail, and a variety of different autoimmune diseases are produced. These can be B cell- or T cell-mediated and can be organ-specific or systemic. They include type 1 diabetes mellitus (antibodies against pancreatic islet B cells), myasthenia gravis (antibodies against nicotinic cholinergic receptors), and multiple sclerosis (antibodies against myelin basic protein and several other components of myelin). In some instances, the antibodies are against receptors and are capable of activating receptors; for example, antibodies against TSH receptors increase thyroid activity and cause Graves' disease . Other conditions are due to the production of antibodies against invading organisms that cross-react with normal body constituents . An example is rheumatic fever following a streptococcal infection; a portion of cardiac myosin resembles a portion of the streptococcal M protein, and antibodies induced by the latter attack the former and damage the heart. Some conditions may be due to bystander effects, in which inflammation sensitizes T cells in the neighborhood, causing them to become activated when otherwise they would not respond. However, much is still uncertain about the pathogenesis of autoimmune disease. Tissue Transplantation The T lymphocyte system is responsible for the rejection of transplanted tissue. When tissues such as skin and kidneys are transplanted from a donor to a recipient of the same species, the transplants "take" and function for a while but then become necrotic and are "rejected" because the recipient develops an immune response to the transplanted tissue. This is generally true even if the donor and recipient are close relatives, and the only transplants that 38 Blood physiology by prof.Israa F.Jafar are never rejected are those from an identical twin. A number of treatments have been developed to overcome the rejection of transplanted organs in humans. The goal of treatment is to stop rejection without leaving the patient vulnerable to massive infections. One approach is to kill T lymphocytes by killing all rapidly dividing cells with drugs such as azathioprine, a purine antimetabolite, but this makes patients susceptible to infections and cancer. Another is to administer glucocorticoids, which inhibit cytotoxic T cell proliferation by inhibiting production of IL-2, but these cause osteoporosis, mental changes, and the other stigmas of Cushing's syndrome . A third is treatment with cyclosporine . Other Clinical Correlates As knowledge about the immune system has increased, over 50 immunodeficiency syndromes due to abnormalities in the function of immune cells have been described. These produce abnormalities ranging from a moderate increase in the incidence of infections to severe, usually fatal conditions. Malignant transformation can occur at various stages of lymphocyte development. Most if not all cases of chronic lymphocytic leukemia are due to uncontrolled proliferation of B lymphocytes, whereas multiple myeloma is due to malignant proliferation of clones of mature plasma cells. Some cases of acute lymphocytic leukemia are T lymphocyte cancers. Acquired immune deficiency syndrome (AIDS), a disease that is currently a major worldwide problem, is unique in that HIV (human immunodeficiency virus), the retrovirus that causes many cases of it, binds to CD4 and produces a decrease in the number of CD4 helper T cells. The loss of helper lymphocytes leads in turn to failure of proliferation of CD8 and B cells, with eventual loss of immune function and death from infections due to normally nonpathogenic bacteria or cancer. 39
 0
0
advertisement
Related documents







Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users