MUSCLE ATROPHY AND HYPERTROPHY SIGNALLING IN
advertisement

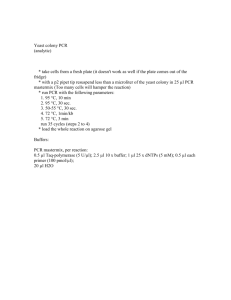
ONLINE ONLY MATERIAL Title: Atrophy and hypertrophy signalling of the quadriceps and diaphragm in chronic obstructive pulmonary disease Authors: Mariève Doucet1, Annie Dubé1, Denis R. Joanisse1,2, Richard Debigaré1, Annie Michaud1, Marie-Ève Paré1, Rosaire Vaillancourt1, Éric Fréchette1, François Maltais1. From: 1 Centre de recherche, Institut universitaire de cardiologie et de pneumologie de Québec, Université Laval, Québec, Canada, 2Division de Kinésiologie, Université Laval, Québec, Canada. Correspondence to: Dr François Maltais Centre de Pneumologie Institut Universitaire de cardiologie et de pneumologie de Québec 2725 Chemin Ste-Foy Québec, QC G1V 4G5 Tel: 418-656-4747 Fax: 418-656-4762 E-mail:francois.maltais@med.ulaval.ca Subjects The diagnosis of COPD was based on a current or past smoking history (> 10 packyear) and pulmonary function testing showing irreversible airflow obstruction (postbronchodilator forced expiratory volume in 1 s [FEV1] < 80% of predicted value and FEV1/forced vital capacity [FVC] < 70%). Patients with comorbid conditions that could be associated with muscle wasting such as active inflammatory illnesses, heart failure, diabetes, systemic corticosteroids, unstable nutritional status and treatment with chemotherapy or radiotherapy were excluded. Skeletal Muscle and Data Analysis Quantitative PCR All protocols consisted of one denaturing cycle at 90C for 10 minutes, followed by 40 cycles of denaturing at 90C for 30 seconds, annealing at 60C for 60 seconds and elongation at 72C for 60 seconds followed by final elongation at 72C for 5 minutes. At the end of the PCR amplifications the samples were subjected to a melting curve analysis. To control for any variations due to efficiencies of reverse transcription and PCR, acidic ribosomal phosphoprotein PO (RPLPO or 36B4) was used as an internal control. The comparative threshold cycles (Ct) values for Atrogin-1, MuRF1 and FoxO-1 study were normalized for RPLPO reference genes and analyzed using the 2-∆∆Ct method.[1] All qPCR runs were performed in triplicate to ensure quantitative accuracy. PCR primer sequences are provided in table 1. Protein extraction and Western blotting Cytoplasmic protein extraction was performed with 30 mg of muscle using a commercial kit according to the manufacturer protocol (NE-PER; Pierce Biotechnology, Rockford, USA). Muscle samples were homogenised using a Polytron PowerGen 125 (Omni International, Marietta, GA, USA). Protease inhibitor cocktails for mammalian cell 2 and tissue extracts (Sigma, Oakville, ON, Canada) and phosphatase inhibitor cocktails I and II (Sigma, Oakville, ON, Canada) was added to the extraction buffer. Protein content was determined by a DC protein essay (BioRad, Mississauga, ON, Canada) based on a modified Lowry method (Lowry and al., 1972). Electrophoresis was performed using 10-15 % SDS PAGE gels in buffer containing 25 mM Tris pH 8.8, 200 mM glycine and 1 % SDS. After a 3-hour protein transfer in cold (4C) buffer containing 15 mM Tris pH 8.8, 120 mM glycine and 10 % methanol, nitrocellulose membranes were blocked for 1 hour or overnight with 5% non-fat dry milk in TBS containing 0.1 % Tween-20. The membranes were then incubated either 1 hour at room temperature or overnight at 4C using the primary antibody. The membranes were then washed 3 x 20 minutes with TBS containing 0.1 % Tween-20 and incubated for 1 hour at room temperature with the secondary antibody and again washed as above. Secondary antibodies used were donkey anti-rabbit IgG (GE Healthcare, Little Chalfont, Buckinghamshire, UK) and sheep anti-mouse IgG (GE Healthcare, Little Chalfont, Buckinghamshire, UK) conjugated to horseradish peroxidase. Finally, the membranes were treated for 1 minute (ECL) or 5 minutes (ECL plus) with chemiluminescence substrates (GE Healthcare, Little Chalfont, Buckinghamshire, UK) and an X-ray film (Clonex Corporation, Markham, ON, Canada) was exposed over the nitrocellulose membranes. Antibodies and the phosphorylation site recognized along with their dilutions are shown in table 2. The antibodies against phosphorylated-p70S6K, total AKT, phosphorylated-AKT, phosphorylated-GSK3β, phosphorylated-4E-BP1 (Cell Signalling technology Inc., Danvers, MA, USA), were used as previously described.[2] The antibodies against Atrogin-1 was developed in our centre as previously reported.[2] Protein content were normalized to α-tubulin (Sigma, Oakville, ON Canada) as previously described by our team.[2] 3 REFERENCES 1. Livak KJ, Schmittgen TD. Analysis of relative gene expression data using real-time quantitative pcr and the 2(-Delta Delta C(T)) method. Methods 2001;25:402-408. 2. Doucet M, Russell AP, Léger B, et al. Muscle atrophy and hypertrophy signaling in patients with chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2007;176:261-269. 4 TABLE E1. PRIMER SEQUENCES USED FOR PCR ANALYSES Atrogin-1 Forward Reverse GCA GCT GAA CAA CAT TCA GAT CAC CAG CCT CTG CAT GAT GTT CAG T MuRF1 Forward Reverse CCT GAG AGC CAT TGA CTT TGG CTT CCC TTC TGT GGA CTC TTC CT FoxO-1 Forward Reverse AAG AGC GTG CCC TAC TTC AA CTG TTG TTG TCC ATG GAT GC RPLPO Forward Reverse TCT ACA ACC CTG AAG TGC TTG ATA TC GCA GAC AGA CAC TGG CAA CAT T Definition of abbreviations : MuRF1 = Muscle ring finger-1, FoxO-1 = Forkhead transcription factor-1, RPLPO = acidic ribosomal phosphoprotein PO. 5 TABLE 2. ANTIBODIES AND THEIR DILUTIONS Cytoplasmic proteins Atrogin-1 Total AKT p-AKT p-p70S6K p-GSK3β p-4E-BP1 Site of phosphorylation Ser 473 Thr 389 Ser 21/9 Thr 37/46 Dilution 1:2000 1:5000 1:1000 1:2000 1:1000 1:1000 Control for protein content α-tubulin 1:20000 Definition of abbreviations : p-AKT = phosphorylated-AKT, p-p70S6K = phospholylated-70kDa ribosomal S6 Kinase, p-GSK3β = phospholylatedglycogen synthase kinase 3β, p-4E-BP1 = phospholylated-eukaryotic translation initiation factor 4E binding protein-1. 6