Administrative Office St. Joseph's Hospital Site, L301
advertisement

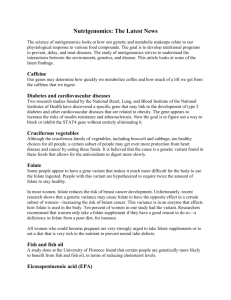
Administrative Office St. Joseph's Hospital Site, L301-10 50 Charlton Avenue East HAMILTON, Ontario, CANADA L8N 4A6 PHONE: (905) 521-6141 FAX: (905) 521-6142 http://www.fhs.mcmaster.ca/hrlmp/ Issue No. 89 QUARTERLY NEWSLETTER August 2006 Folate: A Test No Longer Routinely Warranted Background Folate, a water-soluble B vitamin, is found naturally in raw leafy vegetables, citrus fruits, dried beans and peas. Natural folate is 50% bioavailable compared to 85% in fortified foods and almost 100% when taken as a supplement. In blood 95% of folate is within erythrocytes. Folate is taken up only by the developing erythrocyte. Folate concentration in erythrocytes therefore reflects overall tissue folate concentration better than serum folate. Serum folate reflects transitory changes in folate concentration and low levels do not differentiate between reduced intake and chronic deficiency signifying depleted folate stores and functional changes. Since erythrocyte folate represents the average folate availability over the past 2-3 months it gives a better indication of tissue stores than serum folate. Fortification of foods with folate Fortification of foods with folate was fully implemented in Canada beginning January 1998. The purpose of fortification was to reduce the risk of neural tube defects (NTD). The incidence of NTDs was reduced by 47% from 1995 to 1999 in Ontario (16.2 to 8.5 per 10,000 pregnancies).1 Folate fortification in Canada 150 μg/100 g 200 μg/100 g white flour in foods uncooked pasta μg/10 g cornflour Widespread consumption of foods fortified with folate has increased the level 150-200 of folate in the population. In addition folate is consumed through nutritional supplements and from other fortified foods and drinks. (voluntary) Causes of low folate levels Low consumption of foods containing folate Undernutrition in the elderly and in persons with alcoholism Malabsorption due to inhibition of folic absorption (e.g., alcoholism, medications) and gastrointestinal diseases Decreased metabolism (e.g., elderly, medications) Increased loss (renal failure, dialysis) Increased demand including pregnancy and cancer Megaloblastic anemia Folate and vitamin B12 deficiency are both associated with a reduction in hemoglobin and production of megaloblastic cells. Although folate supplementation can reverse vitamin B12 deficiency megaloblastic anaemia, it does not treat and may even worsen the neurological disease associated with vitamin B12 deficiency Medications that may lower folate Antacids and anti-ulcer medications Folic acid antagonist drugs Anticonvulsants Phenytoin Primidone, Phenobarbital Anticancer drugs Aminopterin Methotrexate Antibiotics/antibacterials Sulfasalazine Pyrimethamine Trimethoprim Trimetrexate Sodium channel-blocking potassium sparing diuretics Oral contraceptives Nonsteroidal anti-inflammatory drugs Oral hypoglycemic agents Metformin Reference interval There is no accepted standard for folate deficiency or inadequacy based on folate concentrations. In addition, there is currently no standard for folate measurement and values can vary significantly from one laboratory to another because of method differences.2 For this reason it is important to interpret folate results from different laboratories and published studies with caution. The Institute of Medicine (IOM) publication on Dietary Reference Intakes (DRI) 1998 reviewed the literature and based on several studies suggested a value of < 317 nmol/L (140 ug/L) to be a reasonable indicator of deficiency.3 The Hamilton Regional Laboratory Medicine Program (HRLMP) uses a method, which gives higher values than methods used in the studies described in the IOM document (Quantaphase II, Bio-Rad Laboratories). Based on published comparisons, the IOM value was converted to the corresponding value for the method used by the HRLMP (E170, Roche Diagnostics).4 The converted HRLMP value for RBC folate deficiency is < 520 nmol/L. 2 - Population studies Results from our laboratory and other studies suggest that American and Canadian populations have reached unprecedented levels of folate and that folate deficiency has been essentially eliminated. The prevalence of folate deficiency has decreased by 61% in the National Health and Nutrition Examination Surveys (NHANES, 1988-1996 to 2001-2002) and 84% in the Framingham Study (1995 to 1998) after folate fortification was initiated. A survey conducted in Ontario between 1997 and 2000 showed a decrease in RBC folate deficiency of 77%.5 The 95% confidence interval for RBC folate performed by the HRLMP is 813 to 3453 nmol/L. The percentage of tests with a low level (< 520 nmol/L) is 0.3%. Frequency distribution of RBC folate tests performed within the HRLMP ( 2004 to 2006, n = 19,885) 9 Age distribution of RBC folate tests ordered: 7 < 18 y 19 – 40 y 41 – 65 y > 65 y 6 5 Deficiency < 520 nmol/L 4 3 6% 18% 33% 44% 2 1 5700 5500 5300 4100 4900 4700 4500 4300 4100 3900 3700 3500 3300 3100 2900 2700 2500 2300 2100 1900 1700 1500 1300 900 1100 700 500 300 0 100 Based on these statistics, and because 60% of the folate tests also have a vitamin B12 test ordered at the same time, routine ordering of folate (serum or RBC) is no longer warranted. The low incidence of folate deficiency indicates that vitamin B12 should be the preferential test for investigating megaloblastic anemia. Frequency (%) 8 RBC folate (nmol/L) Nonetheless, higher folate levels may be required for risk reduction of neural tube defects but the optimum level is unknown. Further research is required to decide what the implications of folate may be for cardiovascular disease, cancer, cognitive function and if there are adverse effects to high levels of folate. 6 References 1. 2. Dietary Reference Intakes Gucciardi E, Pietrusiak M-A, Reynolds DL, Rouleau J. Incidence of neural tube defects in Ontario, 1986-1999. CMAJ 2002; 167: 237-40. Gunter EW, Bowman BA, Cuadill SP, Twite DB, Adams MJ, Sampson EJ. Results of an international round robin for serum and whole-blood folate. Clin Chem 1996; 42: 1689-94. Food and Nutrition Board, Institute of Medicine, Dietary Reference Intakes: Thiamin, riboflavin, niacin, vitamin B6, folate, vitamin B12, pantothenic acid, biotin, and choline. National Academy Press, Washington, DC (1998) Owen WE, Roberts WL. Comparison of five automated serum and whole blood folate assays. Am J Clin Pathol 2003; 120: 121-6. Ray JG, Vermeulen MJ, Boss SC, Cole DEC. Declining rate of folate insufficiency among adults following increased folic acid food fortification in Canada. Can J Public Health 2002; 93: 24953. Ulrich CM, Potter JD. Folate supplementation: too much of a good thing? Cancer Epidemiol Biomarkers Prev 2006; 15: 18993. Reference Values for Folate Adapted from Health Canada’s Food and Nutrition website. Males and Females 3. μg/day (DFE) Age EAR RDA/AI UL 0 – 6 mo * ND 65 ND 7 – 12 mo * ND 80 ND 4. 1–3y 120 150 300 4–8y 160 200 400 9 – 13 y 250 300 600 5. 14 – 18 y 330 400 800 19+ y 320 400 1000 Pregnancy 520 600 1000† Lactation 450 500 1000† 6. *AI Adequate Intake DFE Dietary Folate Equivalents 1 DFE = 1 μg food folate = 0.6 μg folic acid supplements and fortified foods Websites: EAR Estimated Average Requirement Dietary Supplement Fact Sheet: Folate RDA Recommended Dietary Allowances http://dietary-supplements.info.nih.gov/factsheets/folate.asp UL Tolerable Upper Intake Level Investigation & Management of Vitamin B12 and Folate Deficiency http://www.healthservices.gov.bc.ca/msp/protoguides † 800 μg/day for < 18 y Cynthia Balion MSc, PhD, FCACB, Clinical Chemist Karina Rodriguez-Capote MD, PhD, Postdoctoral Fellow, Clinical Biochemistry Richard Cleve, MSc, MD, Resident, Medical Biochemistry Discipline of Chemistry Hamilton Regional Laboratory Medicine Program