Suppl. Material
advertisement

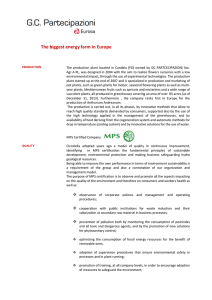
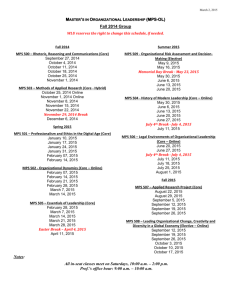
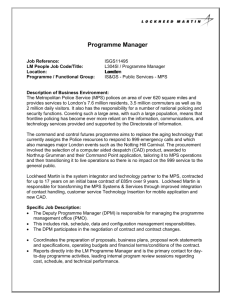
Materials & Methods Study Population. Ten patients (6 men and 4 women) with ACS (comprising unstable angina pectoris (UAP), ST-segment elevation myocardial infarction (STEMI) and non-STEMI (NSTEMI)) 1 who had a percutaneous coronary intervention (PCI), but no evidence of previous myocardial infarction, were recruited. All patients were admitted to the coronary care unit (CCU) of The First Affiliated Hospital Xi'an Jiaotong University. All patients experienced ongoing pain despite pharmacotherapy, including aspirin, intravenous heparin and nitroglycerin, and orally administered prophylactic anti-anginal agents as indicated in Table 1. In view of these symptoms, all patients underwent coronary angiography (CAG), and the degree of coronary artery stenosis was recorded for subsequent correlation with the MP levels. All patients with disorders, such as severe trauma, multiple sclerosis, hypertension, lupus anticoagulant, infectious diseases, renal failure, and the acute phase of rheumatic diseases, were excluded given that these conditions are independent causes of elevated MPs. Ten age- and sex-matched healthy subjects were enrolled as a control group. This study was approved by The First Affiliated Hospital Xi'an Jiaotong University Ethics Review Board. Informed consent was obtained from all patients and controls. Blood sampling and MPs concentration. Fasting blood samples were obtained on the day of hospitalization before any medications were administered. Blood samples were centrifuged (11,000 g, 2 minutes, 4ºC) to obtain platelet-poor plasma. Then, MPs were obtained by centrifugation at 13,000 g for 45 minutes (4ºC) 2. After aspirating the supernatant carefully, the precipitated MPs were resuspended in 100 µl of RPMI1640. The final MP concentration was determined by a bicinchoninic acid protein assay (Merck). The MPs were stored at -80°C until further analysis. Our studies included observations on vasodilation, Western blotting, nitric oxide (NO) and superoxide (O2˙−) production that collectively required significant numbers of MPs. Given the limited availability of blood from ACS patients, we pooled MPs from several patients to create a batch of ‘mixed MPs’ to complete our experimental protocols. To reduce inter-batch differences, each mixture included samples from patients with STEMI, NSTEMI, and both high and low degrees of stenosis. Final microparticles concentrations we used corresponded to their circulating plasma2, as show in Fig 1A. We suppose 3mg/ml as physiological concentrations(Fig 1A: control group:2.7±0.4 mg/ml), and 5mg/ml as pathologic concentrations(Fig 1A: ACS day 0: 4.52±0.7 mg/ml; ACS day 2: 4.47±1.1 mg/ml). For the lacking of enough MPs, we only test the vasodilatation with 5mg/ml concentration. Flow cytometry analysis. Blood samples were centrifuged (11,000 g, 2 minutes, 4°C), and 50 µl of the supernatant platelet-poor plasma was incubated with both 5 µl of anti-CD31-PE and 5 µl of anti-CD41-FITC or CD14-FITC (their corresponding isotypes were used as controls, Beckman Coulter) at room temperature for 30 min3. Before the samples were analyzed, 50 µl of flow count calibrator beads (Beckman Coulter) was added into the antibody-labeled tubes. Histograms were gated at <1 µm, the estimated size of an EMP. CD31(+)/CD41(-) microparticles were identified as endothelial-derived MPs (EMP), whereas CD31(+)/CD41(+) microparticles were identified as platelet-derived MPs (PMP). Vasodilatation detection. All animal experiments were approved by The First Affiliated Hospital Xi'an Jiaotong University Animal Ethics Committee. The rats were purchased from the Animal Experimental Center of Xi’an Jiaotong University. After decapitation, the thoracic aortas were dissected and placed in ice-cold Krebs solution with the following composition (in mmol/L, Sigma- Aldrich, St. Louis, MO): NaCl 119.0, NaHCO3 25.0, glucose 11.1, CaCl2 1.6, KCl 4.7, KH2PO4 1.2, and MgSO4 1.2 (37°C, pH 7.4). After removing tissue surrounding the aortas carefully, four or five 2 to 3 mm-wide aortic rings were obtained from each rat and connected to an isometric force transducer (EMKA Technologies, Paris, France) as previously described4. The aortic rings, with a pre-tension of 1 g, were suspended in organ chambers filled with Krebs solution and aerated continuously with 95% O2 and 5% CO2. After 60 min of equilibration, rings were exposed to 60 mmol/l KCl at least thrice to assess their stability, and only preparations with a maximum tension value that remained unchanged during these trials were used for the experiments. The rings were subsequently treated with MPs from controls at 3 mg/ml or ACS patients at 5 mg/ml for 30 min before pre-constriction with 10−6 mol/l phenylephrine (PE, Sigma-Aldrich, St. Louis, MO). Endothelium-dependent relaxation to acetylcholine (Ach: 10−8–10−4 mol/l; Sigma-Aldrich, St. Louis, MO) was recorded with or without pre-incubation with 1 mmol/l NG-nitro- L-arginine methyl ester (L-NAME; an inhibitor of eNOS, Sigma-Aldrich, St. Louis, MO) for 30 min. The vascular relaxation curves were produced by Graph-Pad Prism, version 5 (Graph-Pad Software, San Diego, CA, USA). Measurement of superoxide production. Lucigenin-enhanced chemiluminescence was measured as previously described5. Briefly, the aorta was cut into rings and incubated in Krebs solution for 30 min for equilibration. Then, L-NAME (1 mmol/l) was added to certain samples for an additional 30 min. After 30 min of pre-incubation, vessels were treated with or without MPs (3 mg/ml) from controls or patients with ACS. After incubation with the MPs, the rings were placed into 96-well plates with Krebs containing 5 μmol/l lucigenin (Sigma- Aldrich, St. Louis, MO). The rings were allowed to adapt in the dark for 10 min at 37°C before O2˙− production was measured using a SpectraMax M5/M5e multi-detection reader (Molecular Devices). After measurement, the aortic samples were dried and weighed, and O2˙− generation was reported as relative light units (RLU)/second/mg protein. Measurement of nitric oxide (NO) generation. Briefly, aortas were cut into rings and equilibrated for 30 min in Krebs solution in 12-well plates. The tissues were maintained in this solution for an additional 30 min with or without L-NAME (1 mmol/l) and then treated with or without MPs (3 mg/ml) from controls or ACS patients. After incubation with the MPs, the supernatant was assessed for NO generation using a specific detection kit (Nanjing Jiancheng Bioengineering Institute, Nanjing, China). The aortic samples were dried and weighed, and NO generation was reported as nmol/mg protein3. Western blot analysis. Whole rat thoracic aortas were treated with or without MPs (3 mg/ml) from controls or ACS patients for 1 h and then washed thrice with Hanks’ balanced salt solution (HBSS). The aortic proteins were then harvested, and immunoblots were performed as previously described3. Antibodies to Akt (Cell Signaling Technology, Beverly, MA, USA), phosphorylated Akt (Cell Signaling Technology, Beverly, MA, USA ), endothelial nitric oxide synthase (eNOS; Santa Cruz Biotechnology, Santa Cruz, CA, USA), phosphorylated at Ser1177 eNOS (Cell Signaling Technology, Beverly, MA, USA ), and β-actin (Cell Signaling Technology, Beverly, MA, USA ) were used for Western blot analyses. Immunoprecipitation. Aortas were treated with or without MPs (3 mg/ml) from controls or ACS patients for 1 h and then washed three times with HBSS before the aortic proteins were harvested. The aortic protein lysates were incubated for 24 h with an anti-eNOS antibody (Santa Cruz Biotechnology, Santa Cruz, CA, USA) to immunoprecipitate eNOS. The eNOS immunocomplex was mixed with Laemmle buffer, heated (95°C, 5 min), mixed, and stored on ice until fractionation. The separated proteins were immunoblotted for eNOS and heat shock protein 90 (Hsp90, Santa Cruz Biotechnology, Santa Cruz, CA, USA) as previously described3. Statistical analysis. Data are presented as the means±SD, and analyzed using GraphPad Prism, version 5.0 (GraphPad Software, San Diego, CA, USA). Normally distributed continuous variables were compared using an independent-samples t-test. Non-normally distributed continuous variables were evaluated with a Mann-Whitney U-test. An independent-samples t-test was used for two-group comparisons, and a one-way analysis of variance was used for multigroup comparison. Dichotomous data are presented as absolute numbers. Correlations between selected variables were estimated by Spearman’s rank correlation coefficient. Differences were considered significant when P < 0.05. Results Plasma MPs. Plasma MPs concentrations were elevated in patients with ACS (day 0: 4.52±0.7; day 2: 4.47±1.1, n = 10) compared with the control group (2.7±0.4, n = 10; Fig. 1A). Much more EMP (43.5%±1.5%, Fig. 1B,C) were detected in day2 MPs compared with day0 MPs (PMP, 32.3%±2.3%, Fig. 1B,C). EMP in day0 contained 38.5%±1.5%, and PMP occupied 35.3%±2.3%. Effects of MPs on endothelium-dependent vasodilatation. Endothelium-dependent relaxations in response to Ach were impaired after incubation with MPs (3mg/ml) from both day0 and day2 ACS patients, but there were no significant difference between day0 and day2 (Fig. 2A). And this effect was enhanced at the concentration of 5mg/ml, and there weren’t statistical difference between day0 and day2 either (Fig. 2B). Effects of MPs on NO and O2˙− generation. NO and O2˙− generation were measured to detect whether MPs from patients with ACS of day0 and day2 have difference on increasing oxidative stress. There were no statistical difference between day0 and day2 on decreasing NO (Fig. 3A) or production of O2˙− (Fig. 3B). Effects of MPs on the Akt/eNOS pathway. Western blotting was used to investigate the different effects on phosphorylation of Akt and eNOS between day0 and day2 MPs from ACS patients. We found that MPs from day2 ACS patients can reduce eNOS phosphorylation at the Ser1177 site (Fig. 4A) and Akt phosphorylation (Fig. 4B) much more, but the difference weren’t significant compared with day0 MPs. Effects of MPs on eNOS and Hsp90 association. The immunoprecipitation experiment revealed that both day0 and day2 MPs would decrease the association of eNOS and Hsp90. And there were no statistical difference between day0 and day2 on the effects of eNOS associated with Hsp90 (Fig. 5). * * 4 2 AC S( da y 0) AC S( co nt da y ro 2) 0 l Concentration of MPs (mg/ml) 6 B 50 40 # * 30 20 10 rs ot he PM EM P 0 P Mean percentage of MPs(%) A C Fig. 1. Origins of day2 MPs from ACS patients. Wen-Qi Han a: MPs were increased in patients with ACS (day 0: 4.52±0.7; day 2: 4.47±1.1, n = 10) compared with control group(2.7±0.4, n=10). Data are means ± SD, * vs. control, P<0.05. b/c: Origins of MPs from day 2 ACS patients. Endothelial-derived MPs (EMP, CD31(+)/CD41(-), blue area, b) occupied the most (43.5%±1.5%,c); then platelet-derived MPs (PMP, CD31(+)/ CD41(+), green area, b; 32.3%±2.3%, c ); MPs that we didn’t test their origins held 24.1%±2.3% (other, c ). * vs. EMP and PMP, # vs. EMP P<0.05, n=10. control ACS day0 (3mg/ml) ACS day2 (3mg/ml) 80 100 * 60 40 control ACS day0 (5mg/ml) ACS day2 (5mg/ml) 80 Relaxation (%) Relaxation (%) 100 * 60 40 20 20 0 0 8 7 6 5 Acetylcholine (-log M) A 4 8 7 6 5 4 Acetylcholine (-log M) B Fig. 2. Effects of MPs from day0 and day2 ACS patients on endothelium-dependent dilatation. Wen-Qi Han MPs from day0 and day2 ACS patients both at 3mg/ml (a) and 5mg/ml (b) could significantly impair endothelium-dependent dilatation stimulated by acetylcholine (Ach).But there were no significantly difference between day0 and day2 at the same concentration of MPs stimulation. Data are means ± SD, * vs. control p<0.05, n=5. 4 # 3 2 1 2 * A o c n la b y2 C S da y0 A C S da ro A co nt an bl l k + 0 L b la 0 n -N k n tr co AM o nt A l+ r E C o l S A Ld CS NA a M y 0 da E A + C y S A L- 0 d CS NA a M y 2 da E + y L -N 2 A M E * RL U/s e c o n d /mg * 4 k nitrite+nitrate(mol/g protein) 6 B Fig. 3. Effects of MPs on nitric oxide (NO) and superoxide anion (O2 ˙-) generation. Wen-Qi Han a: a significant decreasing in NO production was evident with MPs from day0 ACS patient in cultured aorta. The future descending of NO in day2 wasn’t significant compared with day0. *P <0.05 vs. blank and control. b: O2˙- generation was increased in both day0 and day2 ACS groups. Although O2˙- production was higher in day2 group, there was no statistical difference compared with day0. The increased O2˙generation in both groups can be inhibited by NG-nitro- L-arginine methyl ester (L-NAME). * vs. ACS day0 and ACS day2 ; # vs. ACS day0+ L-NAME and ACS day2+ L-NAME, P < 0.05, n = 5. B C D0 IB eNOS IB AKT IB S1177 IB P-AKT IB β-actin IB β-actin D2 B C D0 p-AKT/AKT p-eNOS/eNOS 0.25 0.6 0.4 * * 0.2 Relative Density 0.0 0.20 0.15 0.10 * 0.05 * eNOS/-actin y2 AC S da AC S da y0 l ro co nt bl an k da y2 AC S S da y0 l ro AC co nt bl an k 0.00 AKT/-actin 0.8 Relative Density 1.0 0.8 0.6 0.4 0.2 0.4 0.2 y2 AC S da S AC da y0 l ro k an bl y2 AC S da y0 S da ro AC co nt an bl l 0.0 k 0.0 0.6 co nt Relative Density 0.8 Relative Density D2 Fig. 4. MPs of day0 and day2 from patients with ACS had no significant difference on decreasing endothelial nitric oxide synthase (eNOS) and phosphorylation of Akt (p-Akt) in rat thoracic aorta. Wen-Qi Han Representative immunoblot (IB) showing that MPs of day0 and day2 from patients with ACS decreased eNOS phosphorylation at the Ser1177 site (p-eNOS) and p-AKT with the same degree in rat thoracic aorta. * vs. blank and control P <0.05, n= 5. IP eNOS IB eNOS IB Hsp90 B C D0 D2 Hsp90/eNOS Relative Density 0.8 0.6 0.4 * * 0.2 y2 AC S da S AC da y0 l ro co nt bl an k 0.0 Fig. 5. Effects of MPs from day0 and day2 ACS patients on the association of eNOS with heat shock protein 90 (Hsp90) in rat thoracic aortas. Wen-Qi Han MPs of day0 and day2 from patients with ACS significantly decrease the association between eNOS and Hsp90, but there were no statistical difference between them. * vs. blank and control P < 0.05, n =5. References 1. Y. H. Chen, J.M. Liu, R. J. Hsu, S.C.Hu, H.J. Harn, S.P. Chen, J.R. Jenp, C.L. Wu, J.Y. Ho, C.P.Yu; Angiotensin converting enzyme DD genotype is associated with acute coronary syndrome severity and sudden cardiac death in Taiwan: a case control emergency room study, BMC Cardiovascular Disorders 2012;12:6. 2. Boulanger CM, Scoazec A, Ebrahimian T, Henry P, Mathieu E, Tedgui A, Mallat Z; Circulating Microparticles From Patients With Myocardial Infarction Cause Endothelial Dysfunction. Circulation 2001;104:2649-2652. 3. Ci HB, Ou ZJ, Chang FJ, Liu DH, He GW, Xu Z, Yuan HY, Wang ZP, Zhang X, Ou JS; Endothelial microparticles increase in mitral valve disease and impair mitral valve endothelial function. Am J Physiol Endocrinol Metab 2013;304: 695–702. 4. Ketonen J. Mervaala EMA; Effects of dietary sodium on ROS formation and endothelial dysfunction in LDL receptor deficient mice on high fat diet. Heart Vessels 2008;23:420–429. 5. Ketonen J, Merasto S, Paakkari I, Mervaala EM; High sodium intake increases vascular superoxide formation and promotes atherosclerosis in apolipoprotein E-deficient mice. Blood Press 2005;14:373–382.