Classification of Genetic Diseases
•
•
•
•
•
Single gene mendelian medical disorders
Chromosomal disorders
Multifactorial inheritance
Mitochondria inheritance
Somatic mutation
Single gene mendelian medical disorders
OMIM http://www.ncbi.nlm.nih.gov/omim
•
•
•
•
Autosomal dominant 3,802 reports
Autosomal recessive 3,771 reports
X-linked 1,848 reports
Y-linked 266 reports
• Over-all about 0.5-1% of live birth
Genetic terminology
• Genotype vs Phenotype
• Allele vs Locus (Loci)
A a
B B
A and B are loci.
A or a is an allele of locus A.
Locus A is heterozygous but
locus B is homozygous.
Achondroplasia
The achondroplasia patient 15 years from now
P
What is the risk of his child?
How to know the risk
P
What is the risk of his child?
Your role
• Understand mode of
inheritance
• Risk calculation
• Counseling
Mode of Inheritances
- Classification of genetic diseases
-Understand how genotypes are inherited.
-Understand how genotypes lead to phenotypes.
Risk calculation
How to know classification of
genetic diseases of the patient?
(How to know inheritance
of this patient?)
The achondroplasia patient 15 years from now
P
What is the risk of his child?
Punnett’s Square
The achondroplasia patient 15 years from now
P
What is the risk of his child?
50%
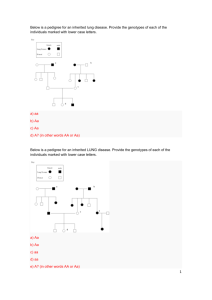
Please self describe characteristic of classical autosomal dominant pedigree
The achondroplasia patient pedigree
P
Why is his parent normal?
What is the
risk of this
child?
The achondroplasia patient pedigree
New Mutation
P
Why is his parent normal?
Fitness vs Denovo Mutation
Familial
Hypercholesterolemia
Severe Osteogenesis Imperfecta
Who was most likely new mutation?
Mosaicism
Gonadal Mosaicism
Recurrence risk of AD new mutation family is not zero.
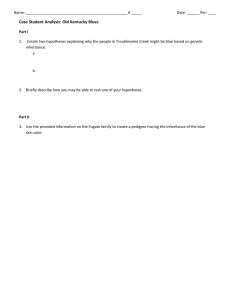
Genetic concept:
Advanced parental age
MATERNAL
PATERNAL
Chromosomal
disorders
(nondisjunction)
Single gene defects:
Autosomal dominant
(point mutation)
The achondroplasia patient 15 years from now
P
What is the risk of his child?
Why is his parent normal?
Retinoblastoma
Example of Retinoblastoma pedigree
I
1
How II2 is ill?
2
II
How III1 is not ill?
Risk of III4, IV2, IV3?
1
2
III
P
1
IV
2
P
1
3
P
2
3
4
Example of Retinoblastoma pedigree
I
1
How II2 is ill?
AD inheritance
2
II
1
2
III
P
1
IV
2
P
1
3
P
2
3
4
Example of Retinoblastoma pedigree
I
1
How II2 is ill?
AD inheritance
How III1 is not ill?
Non-penetrance
20%
2
II
1
2
III
P
1
IV
2
P
1
3
P
2
3
4
Example of Retinoblastoma pedigree
I
1
How II2 is ill?
AD inheritance
How III1 is not ill?
Non-penetrance
20%
Risk of III4 = 40%
2
II
1
2
III
P
1
IV
2
P
1
3
P
2
3
4
Example of Retinoblastoma pedigree
I
1
How II2 is ill?
AD inheritance
How III1 is not ill?
Non-penetrance
20%
Risk of III4 = 40%
IV2 = 40%
2
II
1
2
III
P
1
IV
2
P
1
3
P
2
3
4
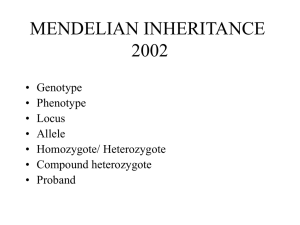
Example of Retinoblastoma pedigree
I
1
How II2 is ill?
AD inheritance
How III1 is not ill?
Non-penetrance
20%
Risk of III4 = 40%
IV2 = 40%
IV3 = 1/15
2
II
1
2
III
P
1
IV
2
P
1
3
P
2
3
4
I
?
II
1
II1 is 3 yr old.
II2 is 1 yr old. Diagnosis?
2
I
?
II
1
Two year later.
II2 is 3 yr old. Diagnosis?
2
I
?
II
1
2
1
2
I
Three year later
II2 is retinoblastoma.
Why?
II
I
?
II
1
2
1
2
I
II1 was ill at 3 yrs but
II2 is ill at 4 yrs.
Why?
Variation in expression
(age of onset)
II
Neurofibromatosis I
Example of
Variation in
Expression:
Severity of
Phenotype
AD Inheritance- Exceptions
•
•
•
•
New mutation
Reduced penetrance
Variable expressivity
Germline mosaicism
Examples of AD Disorders
•
Skeletal dysplasia
– Achondroplasia
– Osteogenesis imperfecta
•
Connective tissue disorders
– Marfan syndrome
– Ehlers Danlos syndrome
•
Craniosynostosis
– Crouzon syndrome
– Apert syndrome
•
Neurocutaneous syndrome
– Neurofibromatosis
– Tuberous sclerosis
•
Adult-onset genetic disorders
– Familial hypercholesterolemia
– Huntington disease
– AD polycystic kidney disease
Please do self
study to
understand these
diseases’
phenotypes. No
need to remember
all detail at this
point.
Achondroplasia
Osteogenesis imperfecta
Marfan syndrome
•
•
•
tall stature
Ectopia lentis
Dilated arotic root
Ehlers-Danlos syndrome
Crouzon syndrome
Apert syndrome
Neurofibromatosis type I
Tuberous sclerosis
Angiofibroma
Ashleaf
Shagreen
Summarized AD pedigree
Example of Autosomal
Recessive in Thailand
Alpha Thalassemia Hydropfetalis
Beta Thalassemia
Autosomal recessive medical disorders in general are rare.
1:20,000 to 1:100,000
Nevertheless,
some are more common in particular populations.
Cystic fibrosis
1:2,000 to 1:4,000 in Caucasian.
Phenylketonuria
1:10,000 in Caucasian.
Sickle cell anemia
1:500 in African.
Thalassemia (alpha & beta)
Why?
1:100 in South-East Asia &
Mediterranean
Autosomal recessive medical disorders in general are rare.
1:20,000 to 1:100,000
Nevertheless,
some are more common in particular populations.
Why?
-Selective advantage (of carrier)
-Common ancestor
-Mating within small population because of racial,
geographic and ethnic differences.
-Genetic drift
Founder Effect
A high frequency of a specific gene mutation in
a population founded by a small ancestral
group
Original
population
Marked population
decrease,
migration, or
isolation
Generations
later
Autosomal Recessive Inheritance
Absolute risk of birth defect between couple
First degree relative
Unrelated person
First cousins
P
30-50%
2-3%
4-5%
Risk of birth defect from AR
¼ x pC x pC (pC = probability of being carrier)
In this case II1 = ?
P
Risk of birth defect from AR
¼ x pC x pC (pC = probability of being carrier)
In this case II2 = ?
P
The probability of being carrier in AR pedigree
Consider
II1 & II2
I1 & I2 & II3
III2
III3
(General Population)
Risk of birth defect from AR
¼ x pC x pC (pC = probability of being carrier)
In this case = ¼ x 2/3 x ¼ = 1/24
P
Carrier frequency is approximately equal to
Disease frequency1/2 x 2
For example if incidence of alpha thal is 1/100,
the carrier frequency in this population is
1/1001/2 x 2 = 1/5
General frequency 1 = N2 + 2ND + D2
N is close to 1 and we know D2 = disease frequency.
2ND = Disease frequency1/2 x 2
Summary of AR pedigree
Autosomal Recessive Inheritance
•
•
•
•
Hemoglobinopathies, thalassemias
Cystic fibrosis
Most of inborn errors of metabolism
Spinal muscular atrophy
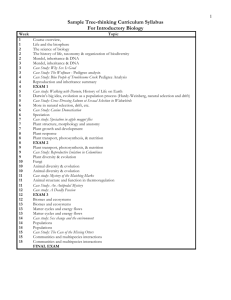
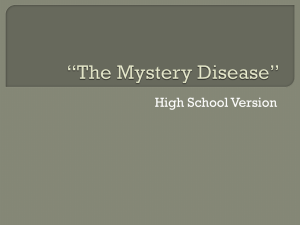
X-linked Recessive Inheritance
Summarized X-linked pedigree
Who are oligate carriers in this pedigree?
2/3
Carrier?
Does X-linked
Female show
Phenotype?
How?
Carrier detection?
X-linked Recessive Inheritance
•
•
•
•
Hemophilia A
Hemophilia B
Duchenne muscular dystrophy
Wiskott-Aldrich syndrome (X-linked
immunodeficiency)
• X-linked agammaglobulinemia
• X-linked adrenoleukodystrophy
X-linked adrenoleukodystrophy
X-linked Dominant Inheritance
X-linked Dominant Inheritance
• Affected heterozygous females are seen.
• Affected males with normal mates have
no affected sons and no normal
daughters.
• Both male and female offspring of female
carriers have a 50% risk of inheriting the
phenotype.
• The phenotype is about twice as common
in females as in males.
X-linked Dominant Inheritance
• Affected heterozygous females are seen.
• Affected males with normal mates have
no affected sons and no normal
daughters.
• Both male and female offspring of female
carriers have a 50% risk of inheriting the
phenotype.
• The phenotype is about twice as common
in females as in males.
Clues
• Pedigree similar to AD,
but no male-to-male
transmission,
with F:M = 2:1
X-linked dominant,
lethal in male
• Only female
survives
X-linked Dominant Inheritance
• X-linked hypophosphatemic
rickets
• Incontinentia pigmenti
• Rett syndrome
Y-linked Inheritance
• Only males affected
• Male to male transmission
• Examples:
– SHOXY (Leri-weil, Langer mesomelic
dysplasia)
– Testes specific protein
– Sex determining region Y
– Zinc finger protein Y
– Azoospermia factor 2
– Azoospermia factor 1
Summary
Mendelian medical disorders
• The family is suffering from a single
gene disorder?
• Mode of inheritance
• New mutation & germline mosaicism
• Penetrance
• Variation in expression
• Risk calculation
• Carrier identification
 0
0