anteroposterior radiographs of the osteoarthritic knee
advertisement

ANTEROPOSTERIOR
RADIOGRAPHS
OSTEOARTHRITIC
SAM
S.
MESSIEH,
From
PETER
THE
KNEE
J. FOWLER,
the University
OF
TOM
Hospital,
MUNRO
Ontario
Destruction
of the articular
cartilage
is the first change
seen on gross examination
of the knee in
osteoarthritis.
Weight-bearing
radiographs
are conventionally
taken
with the knee
in full extension.
Biomechanical
studies have shown, however,
that the major contact sfresses in the femorotibial
articulation
occur when the knee is flexed about 28g. Arthroscopy
has confirmed
that cartilage
loss occurs
in a more
posterior
portion
of the femoral
condyles
than is revealed
by radiographs
taken in full extension.
The
‘standing
tunnel
view’ is a weight-bearing
postero-anterior
radiograph
taken with the knee in 30’ of flexion.
The radiographs
of 64 patients
have been used to compare
the conventional
with the standing
tunnel view. In
10 knees in which the conventional
view suggested
normal cartilage
the standing
tunnel view revealed
severe
degeneration.
Destruction
of the
seen on gross
Non-weight-bearing
the degree
assessing
views
articular
have
of
been
advocated
with the patient’s
and Siber 1970).
knees
the width
ofthe
space often
have
severe
have
is the
change
\
-
in
loss : weight-bearing
are
conventionally
(Leach,
done
Gregg
Fig.l
weight-bearing
views
record
space more accurately,
the joint
to be normal
in patients
cartilage
loss.
is there this discrepancy,
observed,
first
in osteoarthritis.
limited
value
in full extension
Although
cartilage
appears
knee
have
cartilage
but
Why
to obtain a more reliable
We
cartilage
examination
of the
radiographs
and
estimate
who,
what
of cartilage
at arthroscopy,
that
can
Fig.
in fact,
we do
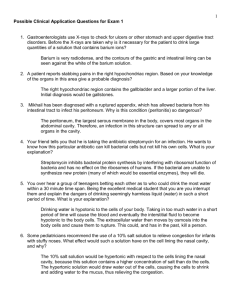
Anteroposterior
extension.
Figure
weight-bearing
2 - In 30#{176}
flexion
radiographs.
the ‘standing
view.
major
caudally
occur
This
graphs
were subsequently
measured
at the mid-point
with
compartment.
with
stresses
the
knee
studies
in about
suggested
that standing
the
slightly
knee
conventional
have
shown
in the tibiofemoral
28#{176}
flexion
flexed
views
would
taken
that
the
articulation
(Maquet
anteroposterior
be
1976).
radiographs
of more
value
tion
a three-month
for osteoarthritis
standing
undergoing
evaluahad a conventional
(Fig.
1) and
a ‘standing
S. S. Messieh,
MD, FRCS
C
P. J. Fowler,
MD, FRCS
C, Associate
Professor,
Orthopaedic
Surgery
T. Munro,
MD, FRCP
C, Associate
Professor,
Radiology
University
of Western
Ontario,
London,
Ontario,
Canada
N6A 5A5.
©
1990 British
Editorial
Society
ofBone
030l-620X/90/41
19 $2.00
J Bone Joint Surg [Br]
1990; 72-B :639-40.
VOL.
72-B, No. 4, JULY
1990
the
2). We examined
S. S. Messieh
and
radiograph
X-ray
tube
taken
angled
64 patients
;
reviewed
of the
We measured
198 tibiofemoral
knees there was a normal
joint
views
views
with
22#{176}
the radio-
and the joint
spaces
affected
tibiofemoral
Joint
at 2559
Surgery
Caroline
space
compartments.
In
on the conventional
but marked
narrowing
on the standing
(average
difference,
3.2 mm).
This
was
both medial (Fig.
In 32 compartments
joint
to Dr
43209.
full
RESULTS
period,
patients
of the knee
Correspondence
should
be sent
Avenue,
Columbus,
Ohio,
USA
(Fig.
in extension.
in extension
radiograph
In
-
than
METHOD
Over
1
view’.
of
tunnel
view’,
a postero-anterior
the knee in 30#{176}
of flexion
and
Biomechanical
Figure
tunnel
thickness?
destruction
the cartilage
occurs
in a more posterior
site on the femoral
condyles
than
is shown
by the conventional
standing
contact
2
space
the space
3) and lateral
between
wider
compartments
tunnel
seen
in
(Fig.
there
was over 2 mm difference
the two views.
In only four cases
on the tunnel
10
4).
in
was
view.
DISCUSSION
Marklund
have
and
already
taken
in slight
space
most
Myrnets
reported
flexion
accurately.
(1974) and Railhac
et al (1981)
that weight-bearing
radiographs
reflect
the width of the cartilage
The
biomechanical
studies of
639
S. S. MESSIEH,
640
Fig.
P. J. FOWLER,
T. MUNRO
3a
Fig.
Conventional
Fig.
views
and
standing
tunnel
views
of the same
3b
patient.
4a
Fig.
Conventional
views
and
standing
tunnel
views
of the same
4b
patient.
that cartilage
loss occurs in a more posterior
part of the
the major
contact
stresses
in
condyles
than
shown
by the
conventional
when the knee is in 24#{176}
to 28#{176} femoral
standing
view.
Figure
5 illustrates
the classical
location
stance
phase
of gait the joint
Maquet
(1976)
suggest
that
the tibiofemoraljoint
occur
of flexion.
During
pressure
may vary
of the weight-bearing
and
20 cm2,
the
greatest
surfaces
become
the
between
flexion.
During
move backwards
progressively
We have
3 and 19 kg/cm2
surfaces
may
smaller
surface
observed,
flexion
these
on the
smaller.
and
the area
vary between
17 cm2
areas
occurring
in
tibial
by arthrotomy
weight-bearing
plateaux
and
as they
arthroscopy,
erosions
on a femoral condyle at a site
which makes contact with the tibia near 30#{176}
of flexion.
If
such a knee is extended and conventional
weight-bearing
views obtained,
the cartilage
space would
appear
normal
since most anterior cartilage
is well maintained.
of osteoarthritic
No benefits
commercial
in any
party
form have been
related
directly
received
or will be received
or indirectly
to the subject
from a
of this
article.
REFERENCES
Leach
RE,
Gregg
T,
osteoarthritis
ofthe
Siber
knee.
Maquet
PGJ. Biomechanicsoftheknee
and the surgica/
treatment
Verlag,
1976.
Marklund
height
Fig.
Classical
location
of erosions
Railhac
5
on a femoral
condyle.
T, Myrnets
R.
in the kneejoint.
FJ.
Weight-bearing
radiography
Radio/ogy
1970; 97:265-8.
in
withapplication
to the pathogenesis
of osteoarthritis.
Berlin,
etc : SpringerRadiographic
Acta Orthop
determination
Scand
1974;
of
45:752-5.
cartilage
JJ,
Fournie
A, Gay R, Mansat
M, Putois
J. Exploration
radiologique
du genou
de face en l#{233}g#{232}re
flexion
et en charge
: son
inter#{234}tdans
le diagnostic
de l’arthrose
f#{233}moro-tibiale.
J Radial
1981 ; 62:157-66.
(Eng.
abstr.)
THE
JOURNAL
OF BONE
AND
JOINT
SURGERY