06_234The Importance of Induced Pluripotent Stem Cell Research
advertisement

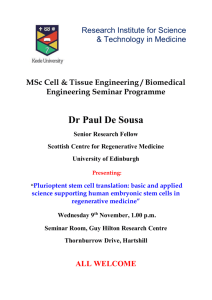
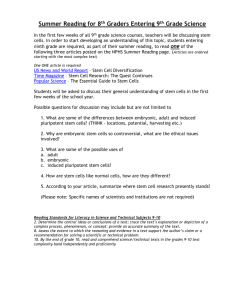
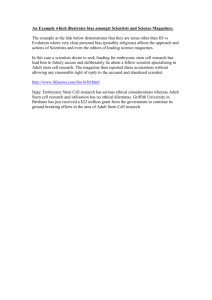
TINJAUAN PUSTAKA The Importance of Induced Pluripotent Stem Cell Research in Medical Science Agustina Kadaristiana MD, Research Assistant, PT. Admiral Jaya Medika, Jakarta, Indonesia ABSTRACT The degenerative diseases that are currently incurable, such as heart disease, stroke, and diabetes, became the global leading causes of death in 2010 and 2011. This fact urges scientists to find alternative treatment for those conditions. In 2006, Takahashi and Yamanaka succeeded in generating an alternative source of stem cells called induced pluripotent stem cell (iPSC). This groundbreaking work holds the promise of new ways to repair cell damage and improve treatment of currently untreatable conditions without raising ethical debates. Many scientists still question whether iPSC is completely interchangeable with ESC in terms of pluripotency and cell mortality. Indeed, iPSC clones and ESC clones have overlapping degrees of variation. It can be concluded that different cell lines will be best suited for different applications. This essay will describe the development stem cell research, comparison between IPSC and ESC, the promise of IPSC technology and current challenges in the applications of iPSCs. Keywords: Induced pluripotent stem cell, medical science, stem cell, untreatable disease ABSTRAK Penyakit degeneratif yang saat ini belum dapat disembuhkan, seperti penyakit jantung, stroke, dan diabetes, menjadi penyebab kematian utama di dunia pada tahun 2010 dan 2011. Fakta ini mendorong peneliti untuk mencari terapi yang bersifat kuratif. Tahun 2006, Takahashi dan Yamanaka berhasil menemukan sumber alternatif sel punca bernama sel punca pluripoten yang diinduksi/Induced Pluripotent Stem Cell (iPSC). Penemuan besar ini memberi harapan dalam memperbaiki sel rusak dan meningkatkan kualitas terapi penyakit yang belum bisa disembuhkan tanpa menimbulkan perdebatan etika. Masih dipertanyakan apakah pluripoten dan kematian sel klon sel iPS sama dengan sel punca embrionik (Embrionic Stem Cells/ESC). Ternyata, terdapat variasi tumpang tindih antara klon iPSC dan ESC. Dapat disimpulkan bahwa sel yang berasal dari alur berbeda, cocok untuk penggunaan yang berbeda. Makalah ini bertujuan untuk memaparkan perkembangan penelitian sel punca, perbandingan antara sel iPSC dan ESC, keunggulan teknologi iPSC sekaligus tantangan dalam aplikasinya. Agustina Kadaristiana. Manfaat Penelitian Induced Pluripotent Stem Cell Research untuk Dunia Kedokteran. Kata kunci: Dunia kedokteran, induced pluripotent stem cell, penyakit yang tidak dapat diobati, sel punca Introduction World Health Organization indicates that non-communicable diseases, such as heart disease, stroke, and diabetes, became the global leading causes of death in 2010 and 2011. However, until recently, those conditions are still incurable. The use of stem cells, hold the promise of new ways to repair cell damage and improve treatments.1 Stem cells are defined as the cells that have the capacity to self-renew (i.e. generate perfect copies of themselves upon division) and undergo lineage differentiation (i.e. specialized cell types that perform specific function in the body).2,3 Depending on the capacity to generate specialized cells, stem Alamat korespondensi cells are classified into tissue (or adult) stem cells and pluripotent stem cells. Tissue (or adult) stem cells are in the body to maintain the organ or tissue in which they reside. Under normal conditions, each type of this kind of cell only generates the organ or tissue systems to which it belongs (unipotency), except for the mesenchymal stem cell, which can generate bone, cartilage, and muscle (multipotency).4 In contrast, pluripotent stem cells have the potential to generate any type of cell found in the body. Pluripotent stem cells are generated in the laboratory and have not been identified in the adult body. There are three types of pluripotent stem cell, namely embryonic stem (ES) cells, epiblast stem cells, and induced pluripotent stem cells (iPSCs). Embryonic stem (ES) cells are derived from early-stage, pre-implantation embryos, and were the first type of pluripotent stem cells to be discovered.5 Epiblast stem cells are a type of pluripotent mouse stem cell derived from a slightly later stage of embryonic development than mouse ES cells; they more closely resemble the human embryonic stem.6,7 Induced pluripotent stem (iPSCs) are the stem cells that generated from adult cell by using a reprogramming technique. This groundbreaking work was awarded the Nobel Prize in Physiology or Medicine in email: kadaristiana@gmail.com CDK-234/ vol. 42 no. 11, th. 2015 811 TINJAUAN PUSTAKA 2012. Following this invention, researchers are rapidly adopting iPS cells for study, although there is ongoing discussion in the field about whether they are identical with ES cells.5,8 The Benefit of Stem Cell Research There are many ways in which human stem cells can be used both in research and clinically.5 In terms of research, studies of human embryonic stem cells could yield information about the complex events that occur during human development. Stem cell study may also provide knowledge about the biology of cell and therefore has the potential to improve and accelerate drug screening, drug discovery, and pre-clinical toxicological assessment of new drugs.9 As far as medical benefits are concerned, human stem cells have a high potential to be applied to cell-based therapy. The purpose of cell-based therapy is to replace missing or damaged cells and (in the future) to generate artificial organs for transplantation. Therefore, stem cell therapy is also known as regenerative therapy.10 Stem cells, directed to differentiate into specific cell types, offer the possibility of a renewable source of replacement cells and tissues to treat previously incurable conditions, including Alzheimer’s disease, spinal cord injury, stroke, burns, heart disease, diabetes, osteoarthritis and rheumatoid arthritis.9 The subsequent Figure 1. Stem cells and their types5 812 advances, including the derivation of hES cell lines, the human iPS cell technology, and progress in making specific specialized cells from stem cells in the laboratory, have suggested that stem cell therapies may be more broadly applied to aid a wide range of disorders.10 Development of Stem Cell Research Tissue stem cells have been used therapeutically for many years in the context of Haematopoietic Stem Cell Transplantation (HSCT), in order to treat many types of blood cancer. In addition, stem cell-based skin grafting11,12 and treatment for corneal damage13 have also been conducted. In HSCT, stem cells are harvested from patient or donor and are transplanted back into the patient to restore damaged cells. However, the need for transplantable tissues and organs far outweighs the available supply.5 In 1998, Dr. James Thomson was able to derive the first human embryonic stem cells. This invention is expected to solve the limited supply of donated organs and tissues. Moreover, studying ES cells seems to offer limitless possibilities because its property makes ESC able to generate every human cell type.14 Narsinh, et al, (2011) argue that the opportunity to model disease, discover disease mechanisms and, ultimately, use cell therapy for previously untreatable conditions is particularly alluring.15 On the contrary, the derivation of human ES cells has sparked controversy because their derivation involved the destruction of a human embryo. There were heated debates regarding the moral status of the embryo.16 Some countries take a tight but permissive approach to research involving the use of human embryos to generate ES cell lines.5 Others have placed some restrictions on research in this area, either through direct legislation, patentability or by limiting the uses of research.5,17 Another obstacle in hESCs research is logistic problem. The limited supply of donor human embryos makes this research application somewhat challenging.15 In particular, Narsinh, et al, (2011) also argue the products derived from hESCs for transplantation purposes would face rejection by the transplant recipient’s immune system or necessitate lifelong therapy with toxic immunosuppressive medication.15 All of these reasons explain the relatively low compound annual growth rate (CAGR) of hESCs global publications (Table 1 & Figure 2).5 Despite the hindrances to the study of human ES cells over the past decade, great strides were being made in understanding the pathway that regulate the maintenance and pluripotency of ES cells. In 2006, Takahashi and Yamanaka announced the successful alternative sources of personalized patient-specific stem cells called induced pluripotent stem cells (IPSCs).8 The iPS cells are derived from adult mouse fibroblast through the reprogramming of only four genes: OCT4 (also known as POU5F1), SOX2, Kruppel-like factor 4(KLF4), and c-MYC.8 In 2007, this finding was replicated in human cells.18,19 This groundbreaking work was awarded the Nobel Prize in Physiology or Medicine in 2012. On the same day, James Thomson’s group also reported the generation of human iPSC using a different combination of factors.19 The process of making IPSC does not require the destruction of human embryos, thereby circumventing the ethical debate surrounding hESC derivation. In addition, this technology allows the creation of patient-specific IPSC, which is theoretically secure against immune system.9 To date, researchers have rapidly adopted the iPS cells for study. As a consequence, the CDK-234/ vol. 42 no. 11, th. 2015 TINJAUAN PUSTAKA Table 1. CAGR for stem cells overall, ES cells (all organisms), hES cells, and iPS cells (all organism) from 2008 to 2012. Source: Scopus Table 2. Number of ESC and iPSC clones analyzed in published studies.20 Conclusion about the Relationship between ESCs and iPSCs It is difficult to distinguish between them There are notable differences growth rate of iPSC publication soared up to level off at 77,0% in only four years (Table 1). On the top of that, the total global studies of iPSCs exceeded hESCs study, in 2011-20125 (Figure 2). Comparison between ESCs and iPSCs Despite this heady progress, there are heated debates between scientists regarding the similarity between iPSCs and ESCs. Researchers still question whether iPS cells are different from ESCs, and if so, whether any differences that do exist are functionally relevant. Moreover, they also raise questions about the capability of iPS as a suitable alternative for research and therapy.15,20 According to Yamanaka (2012), during the first few years of his studies IPSC was remarkably similar to ESC.20 Narsinh, et al, (2011) have expressed a similar view that the iPSCs maintain the key feature of ESCs, including the morphology, the ability to propagate in culture indefinitely and the Clone Numbers First Author Year ESC iPSC 68 A.M. Newman 2010 23 M.G. Guenther 2010 36 54 C. Bock 2011 20 12 M.Chin 2009 3 5 C.M. Marchetto 2009 2 2 J. Deng 2009 3 4 Z. Ghosh 2010 6 4 A. Doi 2011 3 9 Y. Ohi 2011 3 9 K. Kim 2011 6 12 R. Lister 2011 2 5 capacity to generate cells.15 Starting in 2009, however, scientists started reporting differences between iPS and ESCs. For instance, a reduced and more variable yield of neural and cardiovascular progeny has been observed in iPSCs. In addition, iPSC derived early blood progenitor and endothelial cells appear to undergo premature senescence. Some researchers have concluded that iPSCs have an intrinsically lower differentiation capacity than ESCs, whereas other research groups believe that the cell of origin might have a specific effect on the differentiation capacity of the derived iPSCs.15, 20 (generally fewer than 10) for each group, whereas those that found the similarity of iPSCs to ESCs analyzed many more clones from multiple laboratories.20 These studies showed that iPSC clones and ESC clones have overlapping degrees of variation (Figure 3).20 It should be noted that variations among ESC clones have been well documented.21,22 Although it is possible that iPSCs clones show greater variation, and that some clones differ from ESCs in their gene expression, DNA methylation; of differentiation ability, it appears that at least some iPSC clones are indistinguishable from ESC clones.23 In light of such variability, To answer these questions, Yamanaka (2012) compared iPSCs and ESCs clones and has observed a clear tendency. He found that studies which report differences between those cells are comparatively small in number Figure 3. Overlapping Variations Present in iPSC and ESC Clones Measurement of a range of properties of iPSCs and ESCs, including gene expression, DNA methylation propensity, and (for mouse cells) complementation activity in embryos has led to the realization that the properties of both ESC and iPSC lines vary. However, as analysis of significant numbers of clones from multiple laboratories has accumulated, it has become clear that there is considerable overlap in terms of the properties of ESC and iPSC lines and, at a general level, Figure 2. Global publication count in stem cell research from 1996-20125 CDK-234/ vol. 42 no. 11, th. 2015 these two cell types are difficult to distin-guish. 813 TINJAUAN PUSTAKA Table 3. Disease modeled with iPS cells9 it seems likely that different cell lines will be best suited for different applications.20 The Promise of Induced Pluripotent Stem Cells (iPSCs) in Research and Therapy Since human iPSC technology as the alternative resources for generating stem cells was first introduced in 2007, this 814 invention has been a major breakthrough in biomedical science. The iPSC technology is highly promising because it allows scientists to generate an unlimited population of stem cells that can be differentiated into the desired cell types for studying disease mechanisms, screening, and developing drugs or for developing regenerative therapy in an ethical acceptable way. Patient-derived iPSCs have been shown to be useful for modeling diseases (Table 3) and screening drug candidate libraries starting with the seminal studies by the groups led by George Daley24 and Kevin Eggan.25 In 2009, Lee and colleagues harnessed iPS cells to demonstrate disease modeling and drug screening for familial dysautonomia, a rare genetic disorder of the peripheral nervous CDK-234/ vol. 42 no. 11, th. 2015 TINJAUAN PUSTAKA system. This initial report demonstrated how iPS cells can facilitate the discovery of therapeutic compounds and described how these cells provided a platform for modeling different severity of familial dysautonomia and for generating a predictive test to determine differences in the clinical manifestations of the disorder.26 Up until now, there have been more than 100 reports of modeling diseases that have been published using patient-derived iPSCs with specific disease.20 treatment of Parkinson’s disease,29 platelet deficiency,30 spinal cord injury,31,32 and macular degeneration.33 To date, researchers from RIKEN have been conducting the first clinical trial of iPSCs in human since 2013. This study, led by Masayo Takahashi, is aiming to treat age-related macular degeneration, the most common cause of visual impairment in the elderly, using the reprogrammed stem cells.34 In the future, it might become possible to apply this strategy to treat a broader range of diseases.20 The iPSC technology is contributing to the study of regenerative medicine (i.e. cell-based therapies to replace missing or damaged cells, and generate artificial organs for transplantation). The iPSCs are favorable because it is possible to use self-cell donor which suppress the risks of rejection and infection.9 One of the most striking applications of iPSCs was reported by Nakauchi and colleagues, who was able to generate a rat pancreas in a mouse using iPSCs.27 In another landmark study from Jaenisch’s research group, Werning and colleagues derived dopaminergic neurons from iPS cells that when implanted into the brain became functionally integrated and improved the condition of a rat model of Parkinson’s disease. The successful implantation and functional recovery in this model is evidence of the therapeutic value of pluripotent stem cells for cell-replacement therapy in the brain – one of the most promising areas for the future of iPS cells application. After the seminal work in mice by Rudolf Jaenisch’s laboratory,28 scientists are now making progress toward using iPSCs in regenerative medicine, for example for the Challenges in iPSCs Application Induced pluripotent stem cells technology may bring hope in curing currently untreatable diseases. In the future, this technology will contribute to personalized, predictive, preemptive,35,36 and precision medicine.37 However, there are several challenges for the field to actualize its potential. Firstly, scientists are still struggling to understand the proper production of the iPSCs population and ensure that the populations do not contain other potentially harmful cell types. For cells generated from human pluripotent stem cells, contamination of the transplant with even a small number of cells can promote tumor formation. Therefore, it is essential to determine the safest protocol regarding iPSCs transplantation before it is proposed as clinical treatment.5 In terms of accessibility, Inoue (2014) argues that the use of autologous iPSCs from every individual would likely result in high medical costs.38 In addition, it was found that the process of generating iPSCs using current methods also takes a long time (more than three months).39,40 These reasons, therefore, will limit the accessibility of iPSCs technology particularly for patients who need prompt treatment. As a consequence, iPSCs banking will probably have to be considered in order to ensure the patients receive the cells with a good immunological match, thus minimizing the use of immunosuppressant drugs.41 Conclusion This essay has examined the prospect of using induced pluripotent stem cell as an alternative source in stem cell supply. The importance of IPSC technology and its comparison with embryonic stem cells has also been discussed. Although the routine application of iPSCs is still far from being achieved, the IPSCs technology is promising for medical sciences. The iPSC technology provides the opportunity for generating an unlimited population of stem cells that can be differentiated into the desired cell type for studying disease mechanisms, for screening and developing drugs or for celltransplantation based medicine. However, understanding the proper iPS-specialized cells production still remains a hurdle and the limitations to access iPSCs technology due to financial and logistical problems have to be considered by scientists. Therefore, it is important to encourage researchers to determine the safest as well as the most effective and efficient procedure to bring iPSCs technology to medical application. To achieve this goal, it is necessary to improve research collaboration and government support. The invention of IPSCs is likely to provide solutions in regenerative medicine and enrich the knowledge of medical science. DAFTAR PUSTAKA 1. WHO. The top 10 causes of death [Internet]. 2014. Available from: http://www.who.int/mediacentre/factsheets/fs310/en/. 2. Weissman IL, Anderson DJ, Gage F. Stem and progenitor cells: Origins, phenotypes, lineage commitments, and transdifferentiations. Ann Rev Cell Development Biol. 2001; 17: 387-403. 3. Smith AG. Embryo-derived stem cells: of mice and men. Ann Rev Cell Development Biol. 2001; 17: 435-62. 4. Bianco P, Cao X, Frenette PS, Mao JJ, Robey PG, Simmons PJ, et al. The meaning, the sense and the significance: Translating the science of mesenchymal stem cells into medicine. Nature 5. Barfoot DJ, Kemp E, Doherty K, Blackburn PC, Sengoku DS, Servellen Av, et al. Stem cell research: Trends and perspectives on the evolving international landscape. World Stem Cell Summit. 6. Tesar PJ, Chenoweth JG, Brook FA, Davies TJ, Evans EP, Mack DL, et al. New cell lines from mouse epiblast share defining features with human embryonic stem cells. Nature 2007; 448(7150): 7. Brons IG, Smithers LE, Trotter MW, Rugg-Gunn P, Sun B, Chuva de Sousa Lopes SM, et al. Derivation of pluripotent epiblast stem cells from mammalian embryos. Nature 2007; 448(7150): 8. Takahashi K, Yamanaka S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006; 126(4): 663-76. 9. Robinton DA, Daley GQ. The promise of induced pluripotent stem cells in research and therapy. Nature 2012; 481: 295-303. Med. 2013; 19(1): 35-42. San Diego: SciVal; 2013. 196-9. 191-5. 10. Gearhart J, Hogan B, Melton D, Pedersen R, Thomas ED, Thomspn J, et al. Essentials of stem cells biology. 2nd ed. United Kingdom: Elsevier; 2009. CDK-234/ vol. 42 no. 11, th. 2015 815 TINJAUAN PUSTAKA 11. Green H. Regeneration of the skin after grafting of epidermal cultures. Laboratory Investigat. 1989; 60(5): 583-4. 12. Green H, Kehinde O, Thomas J. Growth of cultured human epidermal cells into multiple epithelia suitable for grafting. Proc Nat Acad Sci. US A. 1979; 76(11): 5665-8. 13. Rama P, Matuska S, Paganoni G, Spinelli A, De Luca M, Pellegrini G. Limbal stem-cell therapy and long-term corneal regeneration. N Engl J Med. 2010; 363(2): 147-55. 14. Thomson JA, Itskovitz-Eldor J, Shapiro SS, Waknitz MA, Swiergiel JJ, Marshall VS, et al. Embryonic stem cell lines derived from human blastocysts. Science 1998; 282(5391): 1145-7. 15. Narsinh KH, Plews J, Wu JC. Comparison of human induced pluripotent and embryonic stem cells: Fraternal or identical twins. Molecular Therapy 2011; 19: 635-6. 16. EuroStemCell. Embryonic stem cell research: an ethical dilemma [Internet]. 2011. Available from: http://www.eurostemcell.org/factsheet/embyronic-stem-cell-research-ethical-dilemma. 17. TheHinxtonGroup. Stem cell research patent landscape (briefing note) [Internet]. 2013. Available from: http://hinxtongroup.wordpress.com/background-2/ip-landscape/. 18. Takahashi K, Tanabe K, Ohnuki M, Narita M, Ichisaka T, Tomoda K, et al. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 2007; 131(5): 861-72. 19. Yu J, Vodyanik MA, Smuga-Otto K, Antosiewicz-Bourget J, Frane JL, Tian S, et al. Induced pluripotent stem cell lines derived from human somatic cells. Science 2007; 318(5858): 1917-20. 20. Yamanaka S. Induced pluripotent stem cells: Past, present, and future. Cell 2012: 678-84. 21. Osafune K, Caron L, Borowiak M, Martinez RJ, Fitz-Gerald CS, Sato Y, et al. Marked differences in differentiation propensity among human embryonic stem cell lines. Nature biotechnology 2008; 26(3): 313-5. 22. Ward CM, Barrow KM, Stern PL. Significant variations in differentiation properties between independent mouse ES cell lines cultured under defined conditions. Experimental Cell Res. 2004; 293(2): 229-38. 23. Miura K, Okada Y, Aoi T, Okada A, Takahashi K, Okita K, et al. Variation in the safety of induced pluripotent stem cell lines. Nature Biotechnol. 2009; 27(8): 743-5. 24. Park IH, Zhao R, West JA, Yabuuchi A, Huo H, Ince TA, et al. Reprogramming of human somatic cells to pluripotency with defined factors. Nature 2008; 451(7175): 141-6. 25. Dimos JT, Rodolfa KT, Niakan KK, Weisenthal LM, Mitsumoto H, Chung W, et al. Induced pluripotent stem cells generated from patients with ALS can be differentiated into motor neurons. Science 2008; 321(5893): 1218-21. 26. Lee G, Papapetrou EP, Kim H, Chambers SM, Tomishima MJ, Fasano CA, et al. Modelling pathogenesis and treatment of familial dysautonomia using patient-specific iPSCs. Nature 2009; 461(7262): 402-6. 27. Kobayashi T, Yamaguchi T, Hamanaka S, Kato-Itoh M, Yamazaki Y, Ibata M, et al. Generation of rat pancreas in mouse by interspecific blastocyst injection of pluripotent stem cells. Cell 2010; 142(5): 787-99. 28. Hanna J, Saha K, Pando B, van Zon J, Lengner CJ, Creyghton MP, et al. Direct cell reprogramming is a stochastic process amenable to acceleration. Nature 2009; 462(7273): 595-601. 29. Kriks S, Shim JW, Piao J, Ganat YM, Wakeman DR, Xie Z, et al. Dopamine neurons derived from human ES cells efficiently engraft in animal models of Parkinson’s disease. Nature 2011; 480(7378): 547-51. 30. Takayama N, Nishimura S, Nakamura S, Shimizu T, Ohnishi R, Endo H, et al. Transient activation of c-MYC expression is critical for efficient platelet generation from human induced pluripotent stem cells. J. Experimental Med. 2010; 207(13): 2817-30. 31. Nori S, Okada Y, Yasuda A, Tsuji O, Takahashi Y, Kobayashi Y, et al. Grafted human-induced pluripotent stem-cell–derived neurospheres promote motor functional recovery after spinal cord injury in mice. Proc Nat Acad Sci. 2011; 108(40): 16825-30. 32. Tsuji O, Miura K, Okada Y, Fujiyoshi K, Mukaino M, Nagoshi N, et al. Therapeutic potential of appropriately evaluated safe-induced pluripotent stem cells for spinal cord injury. Proc Nat Acad Sci. 2010; 107(28): 12704-9. 33. Okamoto S, Takahashi M. Induction of retinal pigment epithelial cells from monkey iPS cells. Investigative Ophthalmol Visual Sci. 2011; 52(12): 8785-90. 34. Cyranoski D. Stem cells cruise to clinic. Nature 2013; 494(7438): 413. doi: 10.1038/494413a 35. Zerhouni EA. US biomedical research: Basic, translational, and clinical sciences. JAMA. 2005; 294(11): 1352-8. 36. Auffray C, Chen Z, Hood L. Systems medicine: The future of medical genomics and healthcare. Genome Med. 2009; 1(1): 2. 37. Mirnezami R, Nicholson J, Darzi A. Preparing for precision medicine. N Engl J Med. 2012; 366(6): 489-91. 38. Inoue H, Nagata N, Kurokawa H, Yamanaka S. iPS cells: A game changer for future medicine. The EMBO J. 2014; 33(5): 409-17. 39. Nakamura M, Okano H. Cell transplantation therapies for spinal cord injury focusing on induced pluripotent stem cells. Cell Res. 2013; 23(1): 70-80. 40. Takahashi K, Yamanaka S. Induced pluripotent stem cells in medicine and biology. Development 2013; 140(12): 2457-61. 41. Turner M, Leslie S, Martin NG, Peschanski M, Rao M, Taylor CJ, et al. Toward the development of a global induced pluripotent stem cell library. Cell stem cell 2013; 13(4): 382-4. 816 CDK-234/ vol. 42 no. 11, th. 2015