Health care reform impacting
Tourism, Hospitality, and
Leisure at a glance
Contents
2
Your five basic questions, answered.
1
1. Why is health care reform a big deal to THL companies specifically?
2
2. What does employer health care in THL companies look like today?
3
3. How will employer health care change through 2015?
4
4. Which provisions of reform will have the greatest impact,
and when do they take effect?
5
5. How can you prepare for health care reform?
7
More questions? Just ask.
8
Your five basic questions, answered.
Are you ready to step up to health care reform with
redesigned benefits plans?
The tourism, hospitality, and leisure (THL) industry — with
labor costs comprising 45% of operating costs and 33%
of revenues1 — is particularly challenged to imagine new
business models that will accommodate health care reform
without breaking the bank.
The Patient Protection and Affordable Care Act (PPACA)
represents a substantial shift in the way health care and
health insurance will work in the United States. Given
the labor-intensive nature of THL businesses, the possible
financial risks are real. The costs of compliance — and
the fines for noncompliance — could require a THL
enterprise to increase prices (a risky strategy in a struggling
economy), reduce or restructure staffing models, and/or
reduce benefits.
Businesses that understand the potential impacts of
health care reform may achieve a significant advantage in
managing both costs and employee expectations.
You need the facts. That is why we are asking — and
answering — these five fundamental questions.
Health care reform impacting Tourism, Hospitality, and Leisure at a glance
1
1. Why is health care reform a big deal
to THL companies specifically?
In the past, companies in the THL industry have exercised
a lot of latitude in deciding whether to offer health care
benefits to employees (and what benefits to offer). Two
atypical variables — a relatively large number of part-time
employees and particularly high rate of first-year turnover
— have typically put a premium on that flexibility.
ōIn 2010, the average employee in a THL company
worked 24.8 hours per week, whereas the average
employee in all private nonfarm industries worked
33.4 hours per week2.
ōThe January 2011 average monthly separations rate for
THL companies was 5%, which is more than 30% higher
than the rate for all private nonfarm industries3.
ōIn service industries in 2010, 72% of companies offered
health benefits to their employees4.
At the same time, THL companies often have diverse and
global employee populations. In 2009, the minority labor
participation rate in the THL industry was slightly more
than 47%, compared to only 34% for all other industries5.
All these factors — together — mean that THL companies
face unique challenges in complying with health care
reform and in communicating any changes in their plans
to employees.
2
2. What does employer health care in
THL companies look like today?
Some hotel and restaurant management companies
delegate the decision of whether to offer employee
health benefits to individual franchisees. As a result,
smaller franchisees (those with relatively fewer
employees) have to pay more to offer benefits at
employer group rates.
In 2010, citing reason for not offering benefits, 54%
of THL companies said high costs and 12% said small
group size6. Furthermore, only 61% of companies with
5,000 or more employees offered health benefits to
part-time workers.
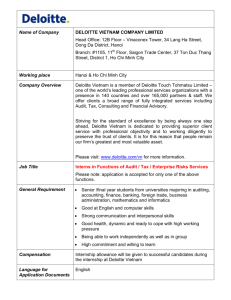
More and more organizations, regardless of the size are
beginning to offer a variety of health benefits to their
employees (Chart 1). Yet, companies are also trying to
mitigate rising employer health care costs. In 2010, 34%
of companies with more than 1,000 employees offered
a high-deductible plan option. Other companies have
implemented wellness or disease management programs
in hopes to mitigate rising costs7.
Chart 1
Among firms offering health benefits, percentage offering a particular wellness program to their employees, by firm size, region, and industry, 2010
Gym membership
discounts or on-site
exercise facilities
Smoking cessasion
program
Web-based resources
for healthy living
Wellness newsletter
Personal health
coaching
Firm size
3–24 workers
27%
19%*
49%
42%
8%*
25–199 workers
35
35*
52
46
20*
200–999 workers
59*
57*
78*
59*
40*
1,000–4,999 workers
71*
66*
84*
58*
44*
5,000 or more workers
77*
76*
92*
64*
56*
All small firms (3–199 workers)
29%*
23%*
49%*
43%*
11%*
All large firms (200 or more workers)
63%*
60%*
80%*
60%*
42%*
Industry
Agriculture/mining/construction
5%*
8%*
37%
28%
6%
Manufacturing
30
34
59
38
20
Transportation/communications/utilities
33
30
73
29
23
Wholesale
38
29
43
47
18
Retail
5*
10*
17*
12*
6
Finance
27
24
49
71*
28
Service
39
24
52
46
10
State/local government
14
12
86*
81*
7
Health care
39
45
70
65
7
30%
24%
51%
44%
12%
All firms
Source: Kaiser/HRET Survey of Employer-Sponsored Health Benefits 2010.
Note: Asterisk indicates an estimate is statistically different within type of wellness program from estimate for all other firms not in the indicated size, region, or industry category (p<.05).
Health care reform impacting Tourism, Hospitality, and Leisure at a glance
3
3. How will employer health care change
through 2015?
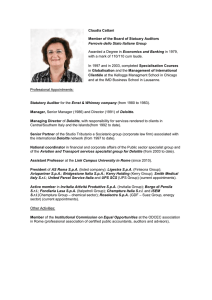
90% of chief financial officers (CFOs) participating in a
recent Deloitte8 survey said that health care reform will
increase the cost per employee of providing health benefits
(Chart 2). But even though the CFOs agree that health
care reform will likely increase costs, more than 60% of
those surveyed intend to continue offering health benefits
to employees. In fact, fewer than 4% indicated that their
companies plan to drop employee health benefits and
pay the mandated penalties (Chart 3). Those planning to
continue offering health benefits would probably do well
to seek professional advice to ensure both compliance with
the new regulations and the identification of innovative
ways to minimize benefit costs.
For THL companies, health care reform could change
decisions about whether to offer health benefits to
employees, which employees are eligible for benefits, how
to cope with additional health care costs, and how to
involve employees in their own health care choices.
For example, the legislation requires that by 2014,
employers with more than 50 full-time employees provide
health benefits or pay penalties equivalent to $2000 per
year for each full-time employee (FTE) in excess of 30
employees. This penalty will increase in subsequent years,
as the costs of health care increase.
Chart 2: Health Reform—Impact on company
Level of impact health care reform is expeted to have on companies*
Number of people offered benefits
Quality or breadth of benefits offered
Number of domestic staff
Proportion of full-time workers
Ability to compete with domestic competitiors for talent
Ability to compete with foreign competitors for talent
Benefits cost per employee
0%
Decline markedly
Decline
No change
25%
Rise
50%
75%
100%
Rise markedly
Chart 3: Health reform legislation—Company responses
Percent of respondents who are considering each alternative*
Continue current enrollment levels and
work to control health care cost inflation
Maintain current scope and level of benefits
for employees, early retirees, and actives
We have not yet begun to consider our options
Limit employer-sponsored coverage to the
minimum permissible under the legislation
For actives, consider converting to a defined contribution
and encouraging enrollment in an exchange
For full-time employees, drop employer-sponsored
coverage and pay the penalities
For early retirees, consider converting to a defined
contribution and encouraging entrollment in an exchange
This topic does not apply to my company
0
4
10
20
30
40
50
60
70
80
4. Which provisions of reform will
have the greatest impact, and when do
they take effect?
Because of their labor-intensive profiles, THL companies
need to pay special attention to those provisions of health
care reform related to part-time workers, waiting periods,
the grandfathering of self-funded plans, and employer
mandates. Additionally, because all employees are diverse
and geographically dispersed, communicating health plan
changes could be a significant challenge.
Part-time employee eligibility for employer health
plans—Effective January 1, 2014
In the past, the eligibility of part-time workers depended
on criteria specified by the employer. Beginning in
2014, health care reform says that (1) employees
working more than 30 hours per week are eligible
for employer-sponsored plans and (2) new part-time
employees working more than 30 hours must be
automatically enrolled in employer plans. THL companies
may find themselves forced to expand dramatically the
number of employees who receive health care coverage.
One solution might be to reduce the number of part-time
and temporary workers by converting them into full-time
staff or reduce the number of hours their part-time
employees work to avoid the 30-hour threshold.
Elimination of waiting periods beyond 90 days—
Effective January 1, 2014
Industries employing lower-skilled workers often use
relatively longer waiting periods for health insurance
eligibility as a way to cope with high first-year turnover.
Health care reform shortens these waiting periods to
a maximum of 90 days for all new employees; for a
THL company that could raise costs overall, especially
if first-year turnover rates continue to be higher
than average.
Grandfathering self-funded employer health plans—
Plans existing before March 23, 2010
Until now, companies have had considerable
freedom to choose what they want to offer in their
employer-sponsored health plans. For example, they
could decide not to cover experimental drugs, chiropractic
services, and a variety of other services and providers.
Grandfathering allows companies with self-funded plans
to continue offering their existing menu of coverage
with a few modifications to comply with new mandates.
If grandfathered status is lost, employers may have to
include a number of treatment options mandated by the
government — options that could increase the costs of the
self-funded plans. In another unintended consequence,
fully insured plans for senior executives could be affected.
Because many health plans for THL companies are selffunded, it is important that management be aware
of actions that could result in the premature loss of
grandfathered status.
Employer mandates for organizations of more than
50 employees—Effective January 1, 2014
Beginning in 2014, companies that employ more than
50 FTEs (full-time defined as 30 hours per week) will be
required to provide health benefits for employees or pay
penalties. The method of calculating these penalties is
somewhat complex, but depends on the total number of
employees. A company with more than 50 FTEs that offers
no health benefit coverage could be penalized $2,000
per year for every employee above 30 FTEs. Further, even
companies offering health benefits could be susceptible
to penalties if any employee seeks coverage through
state-based insurance exchanges.
Employee communication requirements
Above and beyond new W-2 reporting requirements taking
effect in 2011, health care reform mandates employee
communication. In 2012, employers will be required to
issue uniform explanations of cost sharing, exceptions, and
limits on coverage. In 2013, employers will be required to
notify employees of coverage options available through
health exchanges in 2014. For THL companies, with their
diverse employee populations speaking multiple languages,
these new communications requirements could be costly
and time consuming.
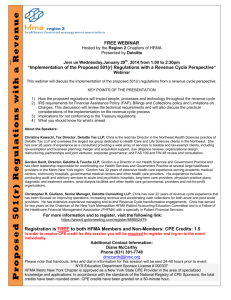
Chart 4 details other relevant aspects of PPACA that will
take effect in the next five years.
Health care reform impacting Tourism, Hospitality, and Leisure at a glance
5
Chart 4: Plan design provisions
Provisions
Effective dates
Employer implications
Elimination of lifetime dollar limits on essential health benefits
September 23, 2010
ō Benefit strategy and design decisions
ō Compliance process assessment and modifications
ō Plan documentation, benefit administrations, and employee communication
assessment and modifications
ō Fully-insured executive benefit plan assessment and modifications
Elimination of health saving account (HSA), flexible spending account
(FSA), or health reimbursement account (HRA) reimbursement for
over-the-counter drugs
January 1, 2011
ō Plan documentation and modifications
ō Reimbursement procedure assessment and modificaitions
Annual FSA contributions limited to $2,500
January 1, 2013
Elimination of annual dollar limits on essential health benefits
January 1, 2014
Extension of coverage to dependent children up to age 26, regardless of
dependent marital or student status
Elimination of preexisting condition exclusions for children under the
age of 19
Restriction of annual dollar limits on essential health benefits
Elimination of cost-sharing requirements for certain preventive health
services
Elimination of coverage rescission abilities
Application of nondiscrimination eligibility rules to fully-insured plans
Elimination of waiting periods in excess of 90 days
Elimination of preexisting condition exclusions for adults
“Employer mandate” and potential penalities
ō Plan documentation, benefit administration, and employee communication
assessment and modifications
ō Potential for increased enrollment in employer-sponsored plans
ō Potential for increased plan costs
ō Potential for financial penalities
Automatic enrollment for new full-time employees (30+ hours per week)
Employers may offer financial incentives (limited to 30% of the cost of
coverage) to wellness program participants
Communication, reporting, and filing provisions
Provisions
Effective dates
Employer implications
Effective internal and external appeals process
September 23, 2010
ō Plan documentation, benefit administration, and employee communication
assessment and modifications
W-2 reporting
January 1, 2011
ō Calculation and disclosure of health benefit aggregate cost for each
covered employee
Uniform explanations of coverage
January 1, 2012
ō Employee communication assessment and modification
Employee notification regarding health exchange availability (in 2014)
and coverage options
January 1, 2013
ō Employee communication and modifications
ō Working knowledge of health exchange
Annual reporting (for the government and plan participants)
January 1, 2014
ō Plan documentation, benefit administration, and regulatory communication
assessment and modifications
Subsidy, credit, penalty, and tax provisions
Provisions
Effective dates
Employer implications
Establishment of a temporary $5 billion reinsurance pool for retirees
under age 65
June 23, 2010
ō Potential financial benefit for employers offering medical benefits to early retirees
ō Validation, preparation, and assembly of all claims information to be submitted
when applying for this program
Nonhealth HSA distributions taxed at 20%
January 1, 2011
ō Compliance and plan documentation assessment and modifications
ō Reimbursements procedure assessment and modifications
Medicare Part A tax increased to 2.35% for earnings over $200,000
(individual return) or $250,000 (joint return)
January 1, 2013
ō Increase in retiree medical costs
January 1, 2014
ō Health plan cost assessment and tax planning
Elimination of employer tax deduction for Medicare Part D retiree
drug subsidy
40% tax on high-value plans (over $10,000 for individuals or $27,500
for families)
6
5. How can you prepare for health
care reform?
Considering the many financial implications of health
care reform, what is the outlook for large THL employers?
Deloitte’s Employer Health care Reform Diagnostic helps
answer that question by providing valuable insights
to employers on two strategic fronts: plan design
modifications and workforce planning.
Plan design modifications
The financial impact of health care reform depends on
your current plan’s provisions and employee cost-sharing
philosophy. Using your company’s data, the diagnostic
tool provides usable information that exposes potential
problems and suggests appropriate mitigation strategies.
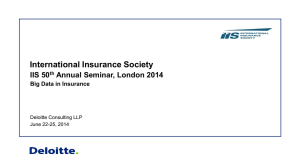
With the diagnostic results, you can balance the health
benefit coverage you want to provide with the new health
care reform legislation requirements (Chart 5).
you could require new strategies for workforce structure,
mix, and talent management.
In addition, you should review your company’s underlying
health benefit participation rules; a comprehensive
workforce planning reevaluation might be required. For
example, new rules for waiting periods and new definitions
of “full time” status for benefits eligibility might create a
new workforce composition; the optimal mix of full-time
and part-time workers could change dramatically.
Using the Deloitte diagnostic, you can identify potential
future costs associated with the new rules and begin to
develop organizational strategies that match the new
realities under health care reform.
Workforce planning
Health care policy changes, together with the possible
“opening up” of the small-group insurance market, may
impact important workforce planning variables, including
employee retention, choices about the workforce
composition, and incentives given to certain workforce
segments.
If these impacts affect labor supply and demand, your
company could face challenges and higher costs in
recruiting, hiring, and retaining the “right” people. Overall,
Employer Health care Reform Diagnostic
Deloitte’s diagnostic addresses more than 25 separate
health care reform provisions that could significantly
impact THL employers. Specifically, the diagnostic:
ōSummarizes each provision
ōDescribes each one’s impact based on analysis of your
company’s plan and financial information
ōProvides specific financial impact projections based on
historical employer data and actuarial and workforce
planning assumptions
ōProvides preliminary thoughts on cost mitigation Chart 5
Finding the right balance between costs and value
Benefit cost
Penalties
Continue health
converge at health levels
Continue health
converge, but reduce
health levels to "safe
harbors"
Discontinue health
converge, but fund HRAs for
EEs (defined contribution)
Discontinue health
converge, but partially
gross up salaries
Discontinue health
converge
Typically $8,000–$10,000
PEPY
Lower, e.g., $6,000 PEPY
Depends on HRA contribution
None
None
None
Minimal
$2,000 PEPY
$2,000 PEPY
$2,000 PEPY
Payroll cost
No change
No change
No change
Increased
No change
Tax savings
Benefit costs fully
deductible
Benefit costs fully
deductible
HRA contribution fully
deductible
Additional salaries
deductible by employer
None
Exposure to future cost
increases and fluctuations
High
High
Low
Low
None
Administrative and
compliance cost
High
High
Moderate
Low
None
Talent cost impact
Lowest–EEs fully "taken
care of"
Moderate–low
Moderate–low
High–additional salary
is taxed
Highest–full burden on EE
Health care reform impacting Tourism, Hospitality, and Leisure at a glance
7
More questions? Just ask.
The practitioners in Deloitte’s tourism, hospitality, and leisure practice are mobilized around providing solutions to the
challenges facing the food service, restaurants, and franchising industry. Our 6,000 consumer products, retail, and
services professionals work with clients to develop appropriate strategies and apply new perspectives that maximize
profitability and operations for greater efficiency. If you would like to initiate or discuss your health care strategies or
plans, we welcome the conversation.
For more information
Visit us at www.deloitte.com/us/thl
Contact
Adam Weissenberg
Vice Chairman, US Tourism,
Hospitality & Leisure Leader
Deloitte & Touche LLP
Tel: +1 973 602 6789
aweissenberg@deloitte.com
Contributing contacts
Scott Rosenberger
Principal, Tourism, Hospitality & Leisure
Consulting Leader
Deloitte Consulting LLP
Tel: +1 404 942 6535
srosenberger@deloitte.com
Alex Kyriakidis
Global Managing Partner
Tourism, Hospitality & Leisure
Deloitte & Touche LLP
Tel: +44 20 7007 0865
Alt Tel: +9714 3322 487
akyriakidis@deloitte.co.uk
Shaz Khan
Principal
Deloitte Consulting LLP
Tel: +1 313 396 3307
shazkhan@deloitte.com
8
Joe Krolczyk
Director
Deloitte Consulting LLP
Tel: +1 412 338 7618
jkrolczyk@deloitte.com
Researchers, writers, and contributors
Michael Carnovali, Deloitte Consulting LLP
Chandni Chopra, Deloitte Consulting LLP
Aaron Gutnick, Deloitte Consulting LLP
Grace Huang, Deloitte Services LLP
Heather Levy, Deloitte Consulting LLP
Dinah Koehler, Deloitte Services LLP
Budd Shaffer, Deloitte Consulting LLP
Josh Taylor, Deloitte Consulting LLP
Naila Stephens, Deloitte Consulting LLP
Endnotes
1
Hospitality Trends, “Health Care Legislation – Which Hotels Might Get Sick?” (November 2009)
2
U.S. Bureau of Labor Statistics, “2010 Current Employment Statistics Survey: B-2. Average hours and earnings of production and nonsupervisory
employees on private nonfarm payrolls by major industry sector, 1964 to 2010” ftp://ftp.bls.gov/pub/suppl/empsit.ceseeb2.txt
3
U.S. Bureau of Labor Statistics,” Job Openings and Labor Turnover” (January 2011) http://www.bls.gov/news.release/pdf/jolts.pdf
4
The Kaiser Family Foundation & Health Research and Educational Trust, “Employer Health Benefits 2010 Annual Survey, 2011”
5
U.S. Equal Employment Opportunity Commission, “2009 Job Patterns For Minorities And Women In Private Industry,” (2010)
http://www1.eeoc.gov/eeoc/statistics/employment/jobpat-eeo1/2009/index.cfm#select_label>
6
U.S. Bureau of Labor Statistics, “2010 Current Employment Statistics Survey: B-2. Average hours and earnings of production and nonsupervisory
employees on private nonfarm payrolls by major industry sector, 1964 to 2010
7
The Kaiser Family Foundation & Health Research and Educational Trust, “Employer Health Benefits 2010 Annual Survey, 2011”
8
As used in this document, “Deloitte” means Deloitte Consulting LLP, a subsidiary of Deloitte LLP. Please see www.deloitte.com/us/about for a
detailed description of the legal structure of Deloitte LLP and its subsidiaries.
Health care reform impacting Tourism, Hospitality, and Leisure at a glance
9
This publication contains general information only and is based on the experiences and research of Deloitte
practitioners. Deloitte is not, by means of this publication, rendering business, financial, investment, or other
professional advice or services. This publicaiton is not a substitute for such professional advice or services,
nor should it be used as a basis for any decision or action that may affect your business. Before making
any decision or taking any action that may affect your business, you should consult a qualified professional
advisor. Deloitte, its affiliates, and related entities shall not be responsible for any loss sustained by any person
who relies on this publication.
Copyright © 2011 Deloitte Development LLC. All rights reserved.
Member of Deloitte Touche Tohmatsu Limited