Pa#ent Safety Academy Chief Opera#ng Officer: Dr Paul Durrands Introduction to safety
culture
AHSN core purpose – health and wealth • Licensed by NHS England for 5 years to deliver four
objectives:
• Focus on the needs of patients and local populations:
support and work in partnership with commissioners and
public health bodies to identify and address unmet health and
social care needs, whilst promoting health equality and best
practice.
• Speed up adoption of innovation into practice to improve
clinical outcomes and patient experience - support the
identification and more rapid uptake and spread of research
evidence and innovation at pace and scale to improve patient
care and local population health.
• Build a culture of partnership and collaboration: promote
inclusivity, partnership and collaboration to consider and
address local, regional and national priorities.
• Create wealth through co-development, testing, evaluation
and early adoption and spread of new products and services.
Oxford AHSN Governance Structure Oxford AHSN Board
Programme Office
AHSN Partnership
Board
AHSN Partnership
Council
Oversight
Group
Oversight
Group
Oversight
Group
Oversight
Group
Oversight
Group
Oversight
Group
Best Care
Programme
(1)
Clinical
Innovation
Adoption
R&D
Programme
Wealth
Creation
Programme
Informatics
Theme
PPIEE
Theme
Clinical
Networks
Projects
Projects
Projects
Projects
Projects
(1) Best Care Programme – Clinical Networks incorporates Sustainability, Popula>on Healthcare and the Con>nuous Learning programme (including the Pa>ent Safety Academy and Evidence Based Healthcare MSc Fellowships) Pa#ent Safety in Oxford AHSN • Best Care – Patient Safety Academy (with HETV)
• Best Care Clinical Networks
• Reducing unwarranted variation (eg improving immunisation coverage,
tackling variation in diabetes care)
• Medicines information on discharge
• Clinical Innovation Adoption – safety focus, eg
• Reducing UTIs – bladder scanner
• Electronic blood transfusion
• Patient Safety Collaborative – Charles Vincent
• 15 Collaboratives based on AHSN geographies
• Build on existing work including the Patient Safety Academy
• Locally lead engagement and prioritisation
• Capability to be built on transparency, continuous learning, prevention,
reliability, leadership, improvement and measurement, accountability, team
work and communication, negotiation (ie Berwick)
• Next steps to October 2014
• Engagement of providers and commissioners
• Identify priorities and baselining
• Develop work plan Pa>ent Safety Academy Why, What and How? Peter McCulloch Director of QRSTU Director, Pa>ent Safety Academy Why do we need the PSA? " Scien>fic evidence of frequent unintended harms in modern healthcare " Serious poli>cal and public concern " Willingness, effort but lack of exper>se, co-­‐
ordina>on and resource in NHS efforts to improve What will the PSA do? " Develop Regional programmes for improving safety and support these with training, measurement and advice " Supply specific safety and quality training needs for NHS organisa>ons in the Region and Na>onally Regional Programmes 2014-­‐6 " Improving Emergency Surgery: management of suspected appendici>s " Senior Leaders programme: improving Acute Trust safety management infrastructure " Improving the safety of Primary Care: iden>fying key dangers in general prac>ce " Improving safety in Mental Health services Bespoke training and advice: examples " Training course on Human Factors for CORESS Board members " Assistance to OUH Trust on new Handover process development " External expert review of SIRI at a London Teaching Hospital How do we work? " Exper>se & experience " QRSTU – Research group in NDS since 2006 " OxStaR – training and simula>on centre in NDA " Mul>disciplinary faculty and links " Underpinning research base " Studies of CRM-­‐based teamwork training " Studies of “lean” based systems improvement " Demonstra>on of synergy using a combined approach (S3 research programme) How do we work? Implementa>on " Training local team of Champions and suppor>ng them via: " “ Playbook” to help guide development of local programme " E-­‐mail and telephone advice " Facilita>on and liaison with Trust management " Advice and assistance with measurement Thank you QIPP team update
What does QI mean at RBFT?
July 2014
“A trust wide alignment of effort to continually improve quality in all that we do”
“A trust wide alignment of effort to continually improve quality in all that we do”
By year end 2012/13, the Trust achieved £49m in cost & income efficiencies over the last 3 years
Of this, £33m has been savings in cost (29% in pay & 71% in non pay)
Year
Target
FY 10/11
FY11/12
FY12/13
FYs 10-­‐13
20,400
21,300
12,200
53,900
Actual
CIP £000's
13,855
18,287
16,935
49,077
10,186
12,997
9,927
33,110
CIP %
73.52%
71.07%
58.62%
67.47%
Income £000's
Income %
2,838
1,247
7,003
11,088
20.48%
6.82%
41.35%
22.59%
Reduction in corporate spend
Reduction in agency / nursing spend = £5m
= £4m
Cost Cost Avoidance / Avoidance / Other £000's Other %
831
4,043
0
4,874
6.00%
22.11%
0.00%
9.93%
Reduction in
procurement
spend =
£9.4m
Reduction in clinical admin = £1m
Efficiencies in estates &
facilities = £1.9m
Reduction in
drug spend
= £1.5m
Achievement of
stretch CQUIN
targets = £5.7m
Quality Improvement Programme (QIPPs)
By year end 2012/13, the Trust will have achieved £49m in cost & income efficiencies over the last 3 years
Of this, £33m has been savings in cost (29% in pay & 71% in non pay)
Year
Target
Actual
CIP £000's
CIP %
Income £000's
Income %
But…..only 1-2% identified
FY 10/11
FY11/12
FY12/13
FYs 10-­‐13
20,400
21,300
12,200
53,900
Cost Cost Avoidance / Avoidance / Other £000's Other %
13,855
10,186
73.52%
2,838
20.48%
hanging71.07%
fruit’ already
18,287• ‘Low12,997
1,247 delivered
6.82%
16,935 • Capacity
9,927
58.62%
7,003
41.35%
within day job to deliver
49,077
33,110
67.47%
11,088
22.59%
• Affordability of CCGs
• More of the same won’t do it
Reduction in corporate spend = £4m
Reduction in agency / nursing spend = £5m
831
4,043
0
4,874
6.00%
22.11%
0.00%
9.93%
Reduction in
procurement
spend =
£9.4m
Reduction in clinical admin = £1m
Efficiencies in estates &
facilities = £1.9m
Reduction in
drug spend
= £1.5m
Achievement of
stretch CQUIN
targets = £5.7m
- ‘Insanity:
Doing the same thing over and over
again and expecting different results’
Albert Einstein/Benjamin Franklin/Anon
- Work harder!
- Waste!
Think differently! Do differently!
- Asking the Why?
- Fresh eyes
- Everyone’s responsibility
Quality Improvement
Doing the right thing for the right patient in
the right way every time
Reliability, get rid of waste, test out change
in a safe way
Drive up quality; drive down cost
Service Improvement
Winner 2011
The Approach
- Bring together all elements needed to make an
(improvement) change work
- Structure
- Explicit what need to consider and be mindful of
- From the Big to the small
Making Every Moment Count
• Quality improvement
as usual practice
• High quality training
• Supporting resources
“My whole outlook has
changed…I now look for
situations to improve…”
Trainee
“The magic is in seeing a trainee iden7fy a problem they encounter and feel empowered to make a change” Hospital Board member 45 trainees
completed 27
projects
Examples of projects
- Improved experience of children with cystic
fibrosis
- Use of longterm peritioneal drains changed
the lives of 12 patients
- Patient guided DVD to reduce anxiety prior
to anaesthesia
An approach to delivering Quality Improvement
Quality Improvement Framework: Our journey towards excellence
Shared Vision
SMART Aims
The Quality Improvement Approach
Improve it!
The vision should answer the question ‘where d o we want to get to?’ and should be the inspiration and framework for planning
The aims set should be:
Specific Enable – provide information and skills / deliberate practice
Measure
Stakeholders – crucial conversations – team and beyond
Plan
Achievable
RoI
Timeframe
Desirable – what’s in it for them?
Improvement opportunities
Measurable
Realistic
Vital Behaviours
Outcomes
Vital behaviours
Evaluate
Influencers – senior engagement and support; opinion leaders
Rewards – what are the incentives?
Environment –providing t he physical means to achieve the outcome
RBFT
QIPP
Programme
Governance Outcomes
Sustainability
Project Management Office (PMO) involvement:
To sustain the improvement requires:
-­‐Projects grouped by value (P1-­‐P3)
-­‐Tracking & monitoring
-­‐Project documents
-­‐Risk assessments
-­‐QIPP Reports -­‐
Programme Board
What are t he Process measures?
What are t he Outcome Measures?
-­‐Patient & staff engagement
-­‐Alignment with goals & structures
-­‐Infrastructure
-­‐Credible evidence
-­‐Adaptability
-­‐Continual monitoring of progress
Assurance
CQIU involvement:
-­‐
Involvement in completion & challenge of Quality Impact Assessments
-­‐ Monitoring of balancing measures
-­‐ Research capability
Shared Learning, show casing of examples such as MEMC, clinical leadership programme etc
RBFT Quality Improvement Training Programme (training, master classes, visits to centres of excellence)
Communication Strategy –sharing p lans, outcomes & celebrating success A template to delivering QI Projects
RBFT
QIPP
Programme
The Quality Improvement Approach: IMPROVE
Improvement Measure
Methodology
How…
opportunity
… do we want to improve?
…. do we generate ideas?
… good are we and how do we know?
Plan
… do we make the changes?
… do we prioritise?
RoI
… do we demonstrate it’s worth it
Outcomes
…are things different from before?
Vital Evaluate
… will our behaviours support the change
… will we know we have made a difference, and how do we keep improving?
Behaviours
…timescale?
Brainstorm
RAG S tudy
Pareto
P&L
Benchmark
Process Map
Audit
Model for Improvement
Historical analysis
Staff +Patient Engagement
Spaghetti Diagram
Baselines
PDSA
Lean
PMO Docs
5 D’s
Project Plan
Human / Financial c ost and saving
SPC
Business Cases
Owners
Timescales
Rapid Improvemen
t Events
Six Sigma
Open to change
See the benefit or bigger picture
Engagement
Review performance
Communicate change
Ensure sustainability
Celebrate Success
The Quality Improvement Approach: IMPROVE
Improvement Measure
Methodology
How…
opportunity
… do we want to improve?
…. do we generate ideas?
… good are we and how do we know?
Plan
… do we make the changes?
… do we prioritise?
RoI
… do we demonstrate it’s worth it
Outcomes
…are things different from before?
Vital Evaluate
… will our behaviours support the change
… will we know we have made a difference, and how do we keep improving?
Behaviours
…timescale?
Brainstorm
RAG S tudy
Pareto
P&L
Benchmark
Process Map
Audit
Model for Improvement
Historical analysis
Staff +Patient Engagement
Spaghetti Diagram
Baselines
PDSA
Lean
PMO Docs
5 D’s
Project Plan
Human / Financial c ost and saving
SPC
Business Cases
Owners
Timescales
Rapid Improvemen
t Events
Six Sigma
Open to change
See the benefit or bigger picture
Engagement
Review performance
Communicate change
Ensure sustainability
Celebrate Success
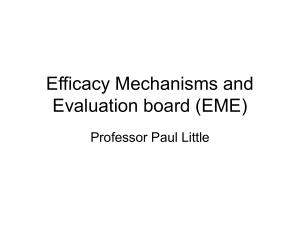
Mortality
Data quality, outliers & review group
-
Dr Foster, CHKS, SHMI
-
Use data to inform areas of concern and priorities to improve
-
Prioritised areas: HSMR weekend, pneumonia, palliative care codes
Mortality reviews & actions
Care bundles
Junior doctor alerts
All deaths reviewed with coding
Action plan to address R codes
R codes (including uncoded) by Month
450
400
400
350
No of spells
Spread of
learning
300
250
238
200
150
100
50
93
83
71
84
83
90
79
111
85
116
0
Feb-­‐ Mar-­‐ Apr-­‐ May-­‐ Jun-­‐ Jul-­‐13 Aug-­‐
13
13
13
13
13
13
Sep-­‐
13
Oct-­‐
13
Nov-­‐ Dec-­‐
13
13
Jan-­‐
14
Prevention of hospital acquired pneumonia
• Successful QIP 2010-11:
reduction in 9 HAP cases per
week to median 3 cases per
week
• Sustainability issues saw rise
in number of cases of HAP to
median 4- 6 cases per week
2012 Prevalence audits on 4 wards
5
4
3
2
1
0
1
2
3
4
2013 HAP prevalence 8 wards
10
9
8
7
6
5
4
3
2
1
0
1
2
3
4
5
6
Week
• Successful relaunch on 8
pilot wards – reduction to
median 2 per week
Drug chart changed
Concentration on
mouthcare
Next steps: Spread to all other wards beyond the 8 pilot wards
Prevention of aspiration pneumonia
Stroke unit
MDT working
Next steps: sustainability of approach on ASU
Spread to other wards where enteral feeding taking place
• % feeds being done at the correct position
improving from 63% to 89%
• Rates of pneumonia reducing from 60% to 0%
Stroke Unit – Shared Ways of Working
Stroke Unit – Shared Ways of Working
Project Ref: QI-2013-08-02
Care Group / Area: Urgent Care
Executive Sponsor: Mandy Claridge
Workshop Dates:
Ward / Dept: ASU / CASU
Team Leader: Ian Waddell
QIPP Lead: Julie Huish
Improvement:
Vision & Vital Behaviours:
Stroke patents go through 3 separate phases – Hyper-Acute Phase (0-72hrs), Acute
Phase (72hrs-14 days), and Rehabilitation Phase (14+days).
To establish one team across ASU and CASU creating a consistent quality of care for
the patient though efficient and effective working.
The ASU and CASU wards are split over two floors within the RBH with the HyperAcute and Acute Units located on Level 2 whilst Acute and Rehabilitation Units are
located on Level 1. Patients perceive this as being treated by different units and
different teams of staff.
The key output for this Structured Improvement Activity will be to develop an
Operational Framework for ASU & CASU which includes operational plans, policies
and procedures.
Opportunity:
Plan (Resource):
This improvement activity will be delivered over a series of 5 workshops:
All staff from all groupings listed working with the ASU and CASU Units.
Workshop 1 – All staff groupings, Outputs to include Requirements, Risks & Issues,
Opportunities & Benefits, and Ways of Working
Workshops 2–4 Outputs to include capturing current ways of working for each staff
grouping.
Workshop 5 – All staff groupings, Proposed Shared Ways of Working, agreed
Operational Framework
•
Measure:
Goal
1
Metric
Current
Target
Operational Framework for ASU & CASU
2
Nurses & All Ward Staff (Matrons, Specialist Stroke Nurses, HCA’s, Ward Clerks,
etc)
Doctors (Stroke, Rehabilitation, Neurologists, etc)
Therapies (OT, Physiotherapy, Speech & Therapy, Dieticians, etc)
Patient Representative – Gary Jopling, Stroke Association
•
•
•
Evaluate
RoI:
Achieved
Goal
Financial
Cashable
Financial
Non Cashable
More efficient ways of
working
2
Quality of service to
patients
Document Ref: QI/TEM/13/07/101
STROKE UNIT - Shared Ways of Working
Force Field Analysis
FOR
MDT
Stroke
Notes
8am Board
Round
MDT
Access to
Stroke Rehab
Specialist Staf f
Continuity
of Care
Patients
Discharge
Planning
Continuation of
Stroke Pathway
Access to Early
Supported
Discharge Team
Direct Access
HASU <4hrs
In-Pts Cont
Need SU and
Prov Time
Long Term
Goal Setting &
Continuity
S
H
A
R
E
D of
Selection
Communication
of Transition to
CASU
W
A
Y
S
O
F
W
O
R
K
I
N
G
AG AINS T
Stroke /
Medical
Mix
Spare Beds
Dumping
Ground
2 x Dif f erent
Care
Groups
Junior
Medical
Cover CSU
x 1 Assisted
Shower
Single Sex
Fluctuating
Demand Accomm Flex
Pts
Awaitint
NE & Care
Location of
ASU &
CASU
Bed
Management
Issues
EASY
Patient
Engagement
Better Comms
Shared
Training
Consistent
Decision
Making
MDT Meeting
Inter Working
Joint ASU
Development
Meeting
Board Round
Stroke Coordinator Beds High Up
Patient Care
Pathway
California Best
Practice
Staff Model
Big Impact
Small Impact
SMALL
BENEFITS
BIG
Work stream
Outcome
Patient Engagement
Consistent Decision Making/MDT meeting
Ongoing
Complete for ASU
Shared Training (Stars)
Complete
Joint ASU Development Meeting
Not applicable now
Patient Care Pathway
Complete
Board Round
Complete
Staff Model
Complete for both wards
Care Group Changes
Location
Complete
Complete
Complete but now not
applicable
Unit Communication
Care Group
Location
Non Cashable
1
© 2013, Royal Berkshire NHS Foundation Trust
All Rights Reserved
“The project is now closed as the 12
Stroke beds that were on
Caversham are now not designated
Stroke Beds. However the work we
completed was very positive and did
help strengthen ASU” Ian Waddell
Shared
Paperwork
IMPLEMENTATION
QIPP Improve Template for:
STROKE UNIT- PICK CHART
HARD
The objective for this event was to establish one team across ASU and
CASU creating a consistent quality of care for the patient through efficient
and effective working.
Renal AVF Process Improvement
Set - National Target Rates 80 - 85%
The objective for this event was to review & develop standardised processes for Arterio-Venous
Fistulae prevalence in HD stock population, in order to improve quality and to achieve best practice
target rates as set by the Specialist Commissioners
QIPP Improvement Charter for:
Renal AVF
Project Ref: QI-2013-07-01
Care Group / Area: Networked Care
Executive Sponsor: Dr Emma Vaux – Consultant Nephrologist
Workshop Dates:
Ward / Dept: Renal
Team Leader:
QIPP Lead: Julie Huish
QI Project Action Plan for:
No.
Improvement:
Vision & Vital Behaviours:
The Specialist Commissioners have set best practice targets for Arterio-Venous Fistulae
prevalence in HD stock population. Targets for 2013-2014 are set at 80%, whilst targets for
2015 are set at 85%.
Within RBFT the current rate of achievement is between 70-75%. Factors contributory to this
include radiology waiting times, patient compatibility, availability of theatres, failed treatment,
and refusal of treatment.
Key areas for improvement are Senior Decision Making, Failing PD and Radiology Waitlists.
Areas for review include:
•
Senior decision making in ‘Acutes’ patients
•
Senior decision making in PD patients transferring to HD (inadequate peritonitis takes)
•
Acute PD service
•
Fast track service for AVF in acute patients (instant needling grafts)
•
Surgery – operating lists at RBH
•
Radiology waitlists
•
Transplant patients (inadequate, acute rejection, PD)
•
Transfer-ins – (Hammersmith, previous access history, previous PD decisions)
To review & develop standardised processes in order to improve quality and achieve best
practice target rate of 80% for 2013-2014, and subsequent BPT rate of 85% for 2015.
Opportunity:
Plan: (Resource)
This event focuses on developing a single way of working by increasing process flow and
reducing variation.
Key outputs include –
•
SIPOC to define project boundaries
•
Documented As-Is Process Map
•
Documented To-Be Process Map with key decision points identified
•
Develop a single access Data Plan / Handover Process
•
RACI including patient accountability
Emma Vaux
Oliver Flossmann
Leo Bailey
Gill Downs
Joy Stringer
Mary Wyman
Katy Priddis
Measure:
Goal
1
2
Metric
Increase target rate in line with Best
Practice Target rates
Develop a single access Data Plan &
Handover Process
Current
Target
70-75%
80-85%
The two main areas for improvement opportunities are:
1.
2.
Improve
Patients
a.
b.
c.
d.
e.
f.
g.
h.
i.
Evaluate
RoI:
Achieved
Goal
1
the process for patients diagnosed with CKD/5 waiting to have AVF
who have had an AVF and are waiting to mature (Time of op to time of use)
Patient choice
Needling – self needling / Windsor needling practice
Radiology – new ultra sound machine
Nurse influences
Time of use
Line removal
Signed form for refusals
CV5 options
Vascular access ¼ meetings
Claire Orme
Bassam Alchi
Jane Moore
Julia Smith
Barbara Dollery
Moses Amao
Alison Galer
Financial
Cashable
Cian Chan
Lloyd Swee
Theresa Matthews
Madeleine Wallis
Angela Clarke
Alison Swain
Financial
Non Cashable
CQUINS
2
© 2013, Royal Berkshire NHS Foundation Trust
All Rights Reserved
Baseline Rate - Achieving 70%
Non Cashable
To meet national BPT
standards
Collaborative working,
efficient use of resource
Renal AVF
Action
1
Design an A0 size poster to detail the Pros and Cons of
Fistulae
2
Develop a staff booklet – A Guide to Fistulae Access
3
Develop a flow chart for the referral process
4
Develop a Trigger List for each area
5
Setting up Acute PD Service
6
Develop an education process of an acute
7
LCC has to happen within 4 weeks of referral
8
Standard Operating Procedure for Fastrack
9
*Vascular Access Service 8am till 8pm Mon to Fri
Project Ref: QI-2013-07-01 RAG
status
Owner
Target
Date
Jane
Jan 2014
End of January
Jane / Angela
Jan 2014
Date in diary by end January, complete 14/02/14
Jan 2014 Remind Cian
Cian
PD – Barbara/Ollie, LCC –
Ollie/Julia, TX – TX Nurse
+, HD – Bassam/Swee
Progress Update
(Red / Amber
/ Green)
Jan 2014 Leo / Barbara
Jan 2014 Diary date
Cian / Jill
Jan 2014 Madelaine
Jan 2014 Complete
Jane
Jan 2014 In progress
Leo/Jane/Emma
Jan 2014 By March
Angela
Jan 2014 10
Educational Link Nurse for each unit
11
Agenda for holistic meetings for all units inc vascular
Jane/Emma
Jan 2014 By end of February
12
Wednesday MDT – rag rate patients regarding access
Jane/Emma
Jan 2014 By end of February
Jan 2014 13
Weekly Theatre List
Leo/Jane/Emma
14
Weekly Clinic List
Leo/Jane/Emma
Jan 2014 15
2 x Monthly Arm Block List
Jane
Jan 2014 16
*Day Surgery Unit
Leo
Jan 2014 Jane/Emma
Jan 2014 17
Identify why patients sit with lines for a long time
Vascular meeting being set up to combine
weekly theatre and clinic lists – dates to be
confirmed
As above
Jane to follow up
*Feed into VA nurse and consultants
Document Ref: QI/TEM/13/07/101
Current Target Rate
Achieved 80%
Length of Stay
* = QI Team involvement
*
*
QI Team also
support weekly
LOS meetings
*
*
*
Respiratory and Sleep Clinics
The objective for this event was to develop and improve the departments
effectiveness and identify optimum ways of working.
QIPP Improve Template for: Respiratory & Sleep Clinics
Care Group / Area: Urgent Care
Sponsor: Mandy Claridge
Ward / Dept: Respiratory & Sleep Clinics
Team Leader: Ian Waddell
Project Ref: QI-2013-09-01
Workshop Dates: 26/09/13
Vision & Vital Behaviours:
Over the past few years the Respiratory and Sleep Clinics have grown in an
unstructured way. There are inefficiencies within the admin processes that provide
support to clinicians.
•
Plan:
•
•
rganise:
Team members from the following areas will support this improvement opportunity:
Key outputs from this workshop to include-
SIPOC-high level process map to define project boundaries and identify critical
elements within the processes
Documented As-Is Process Map with issues and concerns identified.
Documented To-Be Process Map including Responsibilities, Accountabilities, who
to Consult and Inform, including patient accountability
Measure:
valuate:
Goal
1
Admin staff
Nurses and HCA’s
Consultants
Medical Secretaries
AHP’s
Metric
Current
Target
Produce an Operational Framework
Document
2
3
Achieved
oI:
Financial
Cashable
Goal
Financial
Non Cashable
Non Cashable
1
Efficient and effective
ways of working
2
Quality of service to
patients
3
© 2013, Royal Berkshire NHS Foundation Trust
All Rights Reserved
Document Ref: QI/TEM/13/07/101
“From my perspective it was
very worthwhile to have most
of the department together and
discussing the way we work” -Dr Andy Zurek (Consultant)
Respiratory Clinic - As-IS Process Map
*Walk-Ins
Patient
Cancels
Wrong
Clinics
2 Week Waits
Choose &
Book
Conf &
Privacy
Clinic
Appointment
Contact
Centre
Appt
Changes
Confirmation
Letter
New Appt
Changes
Notes &
referral
Letter
Notes Don't
Arrive or
Taken
Maybe
Cancelled or
Changed
Clinic
Cancelled
Check-In
Front Desk
Height &
Weight
Respiratory Clinic - Ideal Process Map
Capacity for
CT etc
*DNA's
Inadaquate
Equipment
Follow Up
Clinic
Capacity &
delays
TRACKING
Other
Investigations
Tests Not
Booked
Tests Maybe
Multiple
Wait Times
Work streams:
Direct Access Oximeter Diagnostics, new on Choose & Book - In progress
Job Plans for all staff - Complete
Streamlined booking and Admin - In progress
IT Review - Complete
Review of Sleep Service Oxford Model - In progress
Explore Resmed consumables outsourcing service - In progress
Rationalisation of Suppliers - Complete
Stock List - Complete
Dr
Consultant
Phone Calls
Clinic Enviro
Direct
Referral
Sec's
Access to
Data
1
Rooms Lack
Of
X-Ray
Nurse
Consultant
Staff Levels
& capacity
Check Out
Discharge
Transport
A+ C
Letter(s)
Maybe
Multiple
Scribe
Results
Safety Net
Clinician
On Ward
Referrals
inc Physio /
Other Spec
ERR Training
Car Park
Admit to
Ward
< 6/52
<4/52
Capacity
5
Out of
Control
Park
Transport
on Time
Trust
Scas
Volunteers
Tests
No delay
Book-In
- Private
- Confidential
- Efficient
- Vent'd Area
9
Estates
A+ C
Clinicians
M.R.
Out of
Control
Seen with
notes
10
Doctor
Nurse
Physio
Check Out
Clinicians
A+ C
D/C
FU
13
Timely
Made Same Day
Other Depts
Referral
21
Tests
Out of
Control
Tests
16
Admission
Delays
Treatment
Treatment
22
25
Out of
Control
Pharmacy
18
17
19
Cinicians
Discharge
26
Tests
Referral
27
Letter
30
28
“Thanks and thanks for all your
hard work in the event” -- Dr
Grace Robinson (Consultant)
FU
24
Physiology
Radiology
Path
Cardiology
Letter GP
Results with
Notes
Letter
Monitoring
23
Out of
Control
Site
Management
& Ward
Pharmacy
GP
A+ C
IT
External
Out of
Control
14
Out of
Admission Control
No Delay /
Right Ward
15
TRACKING
Discharge
Letter
20
12
11
A+ C
Clinician
Transport
6
Clinicians
Physiology
Radiology
Clinic
Capacity
+ Space
? Generic
7
A+ C
Pre-Order
Tests
A+ C
OVERALL PICTURE
Reminder
Appt
(Improved)
8
4
Pt's Not
Getting
Letter
Delays
IT Issues
Appt
Booking +
Clarity - Who,
Where etc 3
GRADING
Treatment
Tele Calls
S/B Clinician
/ Nurse etc
2
Patient Instruction
•
•
Not by Capacity
•
To develop and improve the departments effectiveness and identify optimum ways
of working.
To ensure roles & responsibilities are fit for purpose, and increase better utilization
of resource
To ensure the patient is at the heart of the service and processes are lean behind
the patient journey.
“Thank you for organising
yesterdays event, it
wasO helpful and it will be
interesting to see what comes
from it. I look forward to
E
R
working
towards a
new improved service” -Karena Cranstone,
Respiratory Physiologist
In order to provide structure and develop more efficient ways of working, processes
and procedures within these departments need to be revisited.
“In my time with the NHS I have
been involved with a few of these
events and I can say this was one of
the best I have attended in terms of
engagement from staff meaning we
have a good chance to do
something good” – Ian Waddell,
Directorate Manager, Acute
Medicine
“Yes agree, thanks Ian for
organising this. It reminded me
that once a year team building
which we used to organise and
pay for should happen again”
-- Dr Chris Davis
(Consultant)
QIPP Lead: Julie Huish
Improvement:
29
Quality Improvement Training – 5 levels
1.
Core Induction - 30 minutes every month (for new staff)
-
Introducing Trust approach to Quality Improvement , overview of trust QI projects, how staff can get
involved, and how the QI team can offer support, QI training programme.
2. Introduction to Quality Improvement – 30 mins
3. Basic Awareness – 2 hour sessions
- Introduction to QI methodology
An interactive session, introducing:
- IMPROVE framework & templates
- An awareness of QI tools & techniques
- The journey from ‘idea’ to ‘testing’
- Includes soft ‘leadership’ change management
skills
- QI Support available
- Brings to life how the tools can be used day to
day
4. Intermediate training – 2 x half days
5. QI Ambassadors
Includes:
Recruiting QI Ambassadors across the Trust:
- Detailed understanding of QI approach
- Good understanding of QI approach & use of
tools & techniques
- Exploration of concepts & tools
- Aimed at staff wishing to make a change / lead a
project in their area of work
- Able to lead projects and facilitate others
- Ongoing follow up and development by QI team
34
RBFT Academy
Leadership, management and quality improvement skills for Doctors in training
Launched November 2013
‘Inspirational speakers’
What is it? RBFT Academy is an intensive annual
programme designed for doctors in training.
5 full day workshops and final summit over one year
The skills and knowledge learnt would equip
participants to lead, manage and contribute to quality
improvement within the NHS.
‘I have learnt so so much’
‘Excellent speakers- pitched relevant content at the right level. Thank you for
organising such an inspiring course!’
‘Brilliant, wish this was available at other Trusts’
Next steps: 2014/15 academy recruitment from August intake of trainees. Spread to other staff (band 7+) in
development
The challenges
- Senior leadership
- External consultants
- CQC & Monitor scrutiny
- Reviewing priorities to match resource
- Focus on understanding Return on Investment for QI projects
- Drive forward QI training trust wide
- Maximising opportunities to win external funding through bids
- More collaboration – PSF/Unipart / Salford / NHS Scotland/PSA/AHSN etc
- We know this works!
- Hold our nerve!
- In for the long run!
Pa>ent Safety Academy Network Event Oxford Health NHS Founda>on Trust Experience of Implemen>ng Harm Reduc>on Approaches Jill Bailey: Consultant Nurse Pa>ent Safety Caring, safe and excellent
The importance of pa#ent safety at Oxford Health NHS Founda#on Trust • Two year membership of South of England Mental Health and Integrated Trusts Safety Collabora>ve • Pilot site for MH ST • Pilot site for new ways of repor>ng restraint to NRLS as a ‘harm’ • Re-­‐modelling services to create integrated pathways – Importance of safety in transi>on – Recogni>on that we need to translate / develop harm reduc>on approaches for people at home • Organisa>onal >me and resources dedicated to recovery from failure (SIRI inves>ga>on costs) Caring, safe and excellent
The South of England Mental Health and Integrated Trust Safety Collabora#ve ! 2 Faculty members (Director of Nursing and Consultant Nurse), IHI Fellows, 24 staff par>cipants ! Quarterly Steering Board ! 2 F/T Pa>ent Safety leads (CN and Programme Manager) – 29 harm reduc#on projects across 3 coun#es " Suicide preven>on, self-­‐harm, AWOL, violence and aggression " Restraint reduc>on (prone) " CAUTIS, VTE, Pressure Ulcers, Falls, " Medica>on errors and medica>on reconcilia>on Caring, safe and excellent
Early successes: harm reduc#on in pilot sites • Safe and >mely return (AWOL and missing pa>ents) increased from baseline of 30% to 74% -­‐ sustained and re-­‐tes>ng interven>ons • Medica>on errors (prescribing and omissions) reduced by 75% in acute adult ward • Death by probable suicide in Oxon and Bucks crisis teams increased from 62 days between to 483 between using ‘Always Events’ Caring, safe and excellent
Harm reduc#on work: our learning • Good Board engagement has been cri>cal to success • Engagement with clinical staff has been rela>vely easy • Ignore middle >ers (opera>onal and professional at your peril) • Tempta>on to resort to problem solving • Focus on measurement for improvement –
–
–
–
–
–
•
Learning about measurement can be challenging Staff who feel alienated from ‘maths’ following early experiences Measurement for improvement is really measurement for judgement Moving away from tradi#onal RAG ra#ngs Determining own measures is unfamiliar Frequent and systema#c review of progress is a new way of working (audit) Spread –
–
Tempta#on to spread too quickly. Avoid spray and pray Consider carefully the condi#ons and culture of areas for re-­‐tes#ng before spread
Caring, safe and excellent
Challenges for the PSA • Be realis>c about the >me it takes to bring about cultural change • Coaching approach has been more successful – Resource intensive • Invest in specific Measurement for Improvement training • Clinical staff • Performance staff • Trust Board • Ensure clarity of Programme Manager’s role in determining spread – Test, re-­‐test, test again in different wards and teams – Avoid staff tempta>on to celebrate too early and ‘spray and pray’ • Encourage work across organisa>onal boundaries – Learning from falls work, AWOL work • Middle layer engagement is cri>cal – needs to be embraced at all levels (ownership, permission and unblocking) Caring, safe and excellent
User-Led Quality Improvement
in Neurosurgery
Nick de Pennington
SpR, Department of Neurosurgery
John Radcliffe Hospital, Oxford
My experience…
Mul>-­‐
disciplinary Outcomes Training & Support User-­‐Led nicholas.depennington@ouh.nhs.uk Working Together Dr Helen Higham
Director, OxSTaR
Director, Patient Safety Academy Building Collaboration
" L
inking with other AHSN Networks
" Linking with existing expertise
" Identifying and interacting with key players
" Patient Safety Federation
" Mental Health Safety Collaborative
" Simulation Centres
" Others?
" Developing coherent inclusive strategy
" Identifying stakeholders in priority areas
" Acute Trusts: Senior Management
" Acute Trusts: Surgery
" Mental Health: which organisations?
" Primary Care: how to relate to frontline GPs? Involving Everyone
" Iden>fying areas of need " Engaging organisa>ons in Regional projects " Sharing knowledge and best prac>ce The PSA Faculty includes…
"
"
"
"
"
"
"
"
"
"
"
"
"
"
"
"
Peter McCulloch
Helen Higham
Lauren Morgan
Lorna Flynn
Lance Holman
Christopher Pennell
Steve New
Ken Catchpole
Charles Vincent
Emma Vaux
Jill Bailey
Claire Merriman
David Griffiths
Matt Inada-Kim
Rosamund Snow
Marcus Durand
Surgeon, Safety Researcher
Anaesthestist, Safety Trainer, Simulation Expert
Postdoctoral Human Factors Researcher in Healthcare
Human Factors Researcher in Healthcare
Clinical Research Fellow
Clinical Research Fellow
Operations Management Expert, Said Business School
Patient Safety Expert, California
Professor of Psychology, Patient Safety Expert
Health Foundation Leader for Patient Safety
Mental Health Nurse, Safer Care Lead, Oxford
Head, Professional Practice Skills, Brookes University
General Practitioner
AGM Consultant, Infection Control Specialist
Patient & Public Involvement Expert
Human Factors Practitioner, Clinical Engineering Lead Future Plans
" Develop a comprehensive set of improvement projects across the AHSN region " Ensure sustainability by developing a mixed funding model " Iden>fy and mee>ng key staff training needs in the AHSN " Develop training for extra-­‐regional and Na>onal healthcare organisa>ons? " Link with other AHSNs? " Develop a strong collabora>ve research programme linked to training ?
Thank you for coming!