Coblation Versus Bipolar Diathermy for Adult Tonsillectomy
advertisement

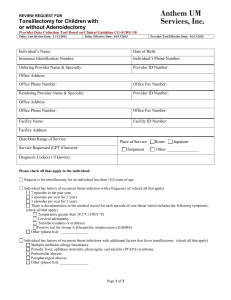
Med. J. Cairo Univ., Vol. 80, No. 1, September: 491-494, 2012 www.medicaljournalofcairouniversity.com Coblation Versus Bipolar Diathermy for Adult Tonsillectomy AHMED H. FAWZY, M.D.; AYMAN HUSSIEN, M.D.; AHMED HUSSEIN, M.D. and BAHER ASHOUR, M.D. The Department of Otorhinolaryngology, Faculty of Medicine, Cairo University Abstract leads to ischemia and protracted cycle of pain. This does not completely subside until the muscle becomes covered with mucosa 14-21 days after surgery [5] . Objective: To compare coblation and bipolar diathermy tonsillectomy in adults in terms of operative time, operative blood loss, post operative pain and post operative complications. Patients and Methods: Thirty patients (aged 18-40 years) scheduled for tonsillectomy were enrolled in this study, the patients were randomized using sealed envelopes to have one tonsil removed by coblation and the other tonsil removed with bipolar diathermy. Operative time and operative blood loss were recorded for each side separately and compared. The patients were given a pain diary to record the level of pain on each side using a visual analog score for 7 days. They were asked also to report any complications. Results: Operative time and operative blood loss were significantly less in the coblation sides ( p<0.001). The mean pain score on the coblation sides was significantly lower 2nd compared to the diathermy sides on the 1 st and post operative days. Conclusion: This study can be added to the studies recommending the use of coblation for tonsillectomy in adults based on the minimal post-operative pain and similar morbidity compared to bipolar diathermy. Key Words: Tonsillectomy – Coblation -– Bipolar diathermy – Post operative pain. The operating principle of coblation or electrodissociation is similar to bipolar diathermy or electrosurgery. In both methods, an alternating current passing between the active electrodes in the tip of the device produces destruction on the target tissue adjacent to the electrodes. In bipolar diathermy, direct contact between electrodes and tissue produces local temperatures of 400°C -600°C resulting in heating of intracellular contents and subsequent vaporization of the cell [6] . In contrast, in coblation, a sodium rich medium must fill the physical space between the electrodes. The coblator causes dissociation of the medium into free sodium ions, which are responsible for the destruction of intercellular bonds, resulting in tissue dissociation. This reaction is achieved at temperatures between 60°C and 70°C with minimal collateral thermal tissue damage [7] . This aim of this study was to compare coblation to bipolar diathermy tonsillectomy in adults in terms of operative time, operative blood loss, post operative pain and post operative complications. Introduction TONSILLECTOMY and adenoidectomy are commonly performed otolaryngological operations, accounting for up to 20% of all operations performed by otolaryngologists [1] . Material and Methods This prospective, randomised, controlled study was conducted from June 2010 to July 2011. The study was approved by the local ethical committee. Informed consent was obtained from all patients. This study was done in accordance with the ethical standards laid down in 1964 Declaration of Helsinki. Despite a range of different techniques, including blunt dissection, guillotine, [2] diathermy, [3] and laser, [4] post operative pain remains the major side effect of the operation . Pain is the result of disruption of mucosa and glossopharyngeal and/or vagal nerve fibres followed by spasm of the pharyngeal muscles that Thirty patients (aged 18-40 years) scheduled for tonsillectomy were enrolled in the study. We excluded patients with bleeding disorders and those with history of quinzy. Correspondence to: Dr. Ahmed Hesham Fawzy, The Department of Otorhinolaryngology, Faculty of Medicine, Cairo University, E-Mail: ahesham73@yahoo.com 491 492 Coblation Versus Bipolar Diathermy for Adult Tonsillectomy The patients were randomized using sealed envelopes to have one tonsil removed by coblation and the other tonsil removed with bipolar diathermy. The patients were blinded to the technique used. Operative technique: All cases were done under general anesthesia. Coblation tonsillectomy was done using the ArthroCare ENT Coblator II Surgery System with the EVac 70 plasma wands (ArthroCare Corporation, Sunnyvale, CA). Settings were standardized at 7 for ablation and 3 for coagulation. The technique of bipolar dissection tonsillectomy was described in details in our previous work [8 ] . Anesthesia and recovery protocols were standardized for all patients. Operative time and operative blood loss were significantly less in the coblation sides (p<0.001) (Table 1). Table (1): Operative data of the patients. Operative time (min) Blood loss (ml) Coblation sides Diathermy sides 7.97±5.31 29.77±22.45 11.67±6.23 44.23±21.92 The mean pain score in the coblation sides was significantly lower compared to the diathermy sides on the 1 st and 2 nd post operative days (Table 2 and Fig. 1). Table (2): Postoperative pain score. Post op days Coblation sides Diathermy sides p-value 1 st 2 nd 3 rd 4 th 5 th 6 th 7 th 4.73±1.74 4.4±1.71 4.57±2.21 4.17±1.51 3.93±1.51 3.6±1.77 3.57±2.86 5.97±1.63 5.77±1.55 5.3±2.32 4.83±2.32 4.4±2.19 4.13±1.91 3.10±1.99 0.002 < 0.001 0.128 0.169 0.215 0.103 0.323 Intraoperative measures: Operative time (from the start of tonsillectomy to the completion of haemostasis) and operative blood loss were recorded for each side separately and compared. 7 Postoperative measures: The patients were discharged on the same day with 1 week course of amoxycillin clavulanate and paracetamol. They were instructed to return to the hospital in the event of haemorrhage. The patients were given a pain diary to record the level of pain on each side using a visual analog score for 7 days, the pain charts consisted of a 10cm linear scale with 10 gradations, ranging from 1 (no pain) to 10 (severe pain). They were asked also to report any complications. Coblation sides Diathermy sides 6 5 4 3 2 1 0 Pain-1 Pain-2 Pain-3 Pain-4 Pain-5 Pain-6 Pain-7 The data was statistically described in terms of mean ± standard deviation (± SD), and range, or frequencies (number of cases) and percentages when appropriate. Comparison of pain scores between the study groups was done using Wilcoxon signed rank test for paired (matched) samples. For comparing categorical data, McNemar test was performed. p-values less than 0.05 were considered statistically significant. All statistical calculations were done using computer programs SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA) version 15 for Microsoft Windows. Results 30 patients were included in this study with a mean age of 27.03±9 years (range from 13-47 years), males constituted 70% of the patients. Fig. (1): Pain score by day in the 2 groups. The number of patients reporting pain score >5 on either side was compared (Table 3). Table (3): The number of patients reporting pain score >5. Post op days Coblation sides (number) Diathermy sides (number) p-value 1 st 2 nd 3 rd 4 th 5 th 6th 7th 9 10 8 5 3 5 7 16 12 15 13 11 7 7 0.092 0.687 0.016 0.021 0.021 0.727 1.000 None of our patients reported any bleeding episode or any other complication. Ahmed H. Fawzy, et al. Discussion A new technique for tonsillectomy should be: Comparable to or better than existing techniques; safe to use; have a short learning curve; and be cost effective. In particular, such a new technique would preferably be associated with less postoperative pain, less intra-operative blood loss, a quicker return to normal diet and activity, and a lower risk of both reactive and secondary haemorrhage [9] . This study was conducted in a prospective randomized manner to compare coblation with bipolar diathermy tonsillectomy. Only adults were enrolled to ensure the efficiency and adequacy of pain assessment, one tonsil was removed with the coblator and the other one with the bipolar diathermy, so each patient served as his or her own control to eliminate any personal variations in pain assessment. The patients were blinded to the technique used. Similar study design have been adopted by many authors, [10-13] on the other hand, Tan et al., [14] randomized the patients not the tonsils into 2 groups; coblation and electrocautery, and Parsons et al. [15] randomized the patients into 3 groups; coblation, electrocautery and harmonic scalpel. The operative time and operative blood loss were significantly less in the coblation sides. On the other hand, other authors reported either no difference [12,13] or even more time with the coblato [11,15] . This could be attributed to the fact that we started this study after mastering the technique of coblation by doing large number of tonsillectomies in children and adults to eliminate the effect of the learning curve, other authors may have started their studies after performing smaller number of cases. In our study, a statistically significant difference in the mean pain score in favour of coblation was reported on the 1 st and 2 nd post operative days. We focused on post-operative pain from another perspective by reporting on the frequency of the sides with a pain score >5, results were again in 4th favour of coblation especially on the 3 rd , and 5 th post-operative days (p<0.05). Similar results were reported by other studies, on the other hand, Tan et al. [14] reported no differences in daily visual analog score for pain attributing this to the masking of any pain benefits from coblation tonsillectomy by the severity of pain in adult tonsillectomy in general, yet they reported a faster recovery for the coblation group. [10-13,15] 493 There are certainly other factors which alter pain, aside from the surgical instrument used. A meticulous, gentle surgical technique is universally accepted as a significant factor in post-operative pain and healing. However, when surgeons use equivalent surgical technique, the instrument used may result in an additional benefit to the patients [15] . None of our patients experienced any reactionary or secondary haemorrhage, thus excluding our study from the debate of whether coblation causes higher incidence of bleeding or not. The answer for this debate could be achieved by conducting further studies on a larger number of patients. Conclusion: We recommend the use of coblation over bipolar diathermy for tonsillectomy in adults based on the lower levels of post-operative pain and similar morbidity. Conflict of interest: The authors declare that they have no conflict of interest. References 1- BLAIR R.L., MCKERROW W.S., CARTER N.W., et al.: Audit Sub-Committee of the Scottish Otolaryngological Society. The Scottish tonsillectomy audit. J. Laryngol. Otol., 110 (20): 1-25, 1996. 2- GOYCOOLEA M.V., CUBILLOD P.M. and MARTINEZ G.C.: Tonsillectomy with a suction coagulator. Laryngoscope, 92: 818-9, 1982. 3- YUAN C.C.,YU D.Y. and JUN T.S.: Guillotine tonsillectomy without anaesthesia. Auris. Nasus. Larynx., 11: 2935, 1984. 4- MARTINEZ S.A. and AKIN D.P.: Laser tonsillectomy and adenoidectomy. Otolaryngol Clin. North. Am., 20: 371-6, 1987. 5- DEMPSTER J.H.: Post tonsillectomy analgesia: The use of benzocaine lozenges. J. Laryngol. Otol., 102: 813-4, 1988. (Grade A). 6- MADDERN BR.: Electrosurgery for tonsillectomy. Laryngoscope, 112: 11-13, 2002. 7- TEMPLE R.H. and TIMMS M.S.: Paediatric coblation tonsillectomy. Int. J. Pediatr. Otorhinolaryngol., 61: 195198, 2001. 8- HESHAM A.: Bipolar diathermy versus cold dissection in paediatric tonsillectomy. Int. J. Pediatr. Otorhinolaryngol., 73: 793-5, 2009. 9- OKO M.O., GANLY I., LOUGHRAN S., CLEMENT W.A., YOUNG D. and GEDDES N.K.: A prospective randomized single-blind trial comparing ultrasonic scalpel tonsillectomy with tonsillectomy by blunt dissection in a pediatric age group. Otolaryngol. Head & Neck Surg., 133: 579-84, 2005. 494 Coblation Versus Bipolar Diathermy for Adult Tonsillectomy 10- TIMMS M.S. and TEMPLE R.H.: Coblation tonsillectomy: a double blind randomized controlled study. J. Laryngol. Otol., 116: 450-2, 2002. 11- NOORDZIJ J.P. and AFFLECK B.D.: Coblation versus unipolar electrocautery tonsillectomy: A prospective, randomized, single-blind study in adult patients. Laryngoscope, 116: 1303-9, 2006. 12- MAGDY E.A., ELWANY S., EL-DALY A.S., ABDELHADI M. and MORSHEDY M.A.: Coblation tonsillectomy: A prospective, double-blind, randomised, clinical and histopathological comparison with dissection-ligation, monopolar electrocautery and laser tonsillectomies. J. Laryngol. Otol., 122: 282-90, 2008. 13- LITTLEFIELD P.D., HALL D.J. and HOLTEL M.R.: Radiofrequency excision versus monopolar electrosurgical excision for tonsillectomy. Otolaryngol. Head & Neck Surg., 133: 51-4, 2005. 14- TAN A.K., HSU P.P., ENG S.P., NG Y.H., LU P.K., TAN S.M., SAY J.H. and CHAN Y.H.: Coblation vs electrocautery tonsillectomy: Postoperative recovery in adults. Otolaryngol Head & Neck Surg., 135: 699-703, 2006. 15- PARSONS S.P., CORDES S.R. and COMER B.: Comparison of posttonsillectomy pain using the ultrasonic scalpel, coblator, and electrocautery. Otolaryngol. Head & Neck Surg., 134: 106-13, 2006.