The Development and Evaluation of a Geriatric Emergency
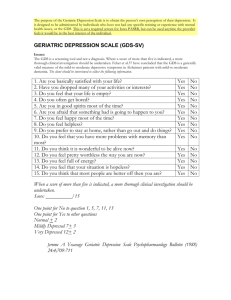
advertisement

~ 219 Geriatric EM Curriculum, Witzke, Sanders The Development and Evaluation of a Geriatric Emergency Medicine Curriculum Donald B. Witzke, PhD, Arthur B. Sanders, MD, f o r the SAEM Geriatric Emergency Medicine Task Force * I ABSTRACT . , . . _............ ... _ . . . . . . . . . . , _ . . . . ,. . . . . . . . . . . . . . . . . . . ............................. ...................................... Objective: To summarize the processes used to develop a curriculum and model of care for the emergency medical treatment of elder patients and to assess the efficacy of the teaching material in a pilot course. Methods: A survey of emergency medicine (EM) residency directors and geriatric fellowship directors was used to identify key topics for inclusion in the didactic material. An interdisciplinary consensus process was used to develop didactic as well as teaching material in geriatric EM. Pretests and posttests were administered to 46 participants in the initial course to assess knowledge gain. Subjective course evaluations were also done. Results: Test scores significantly increased from 54% correct on the pretest to 77% correct on the posttest (p c 0.001). Significant improvement in knowledge as judged by pretest and posttest results occurred in 6 of the 7 teaching modules. Subjective evaluations demonstrated good to excellent ratings for each module as well as the overall workshop. Conclusions: The process of developing a curriculum for geriatric EM is described. The initial training of instructors was effective in improving participants' knowledge of geriatric issues in EM. Participants considered the training to be effective. The effect of the training on the emergency care of elder persons remains to be determined. Key words: geriatric; emergency medicine; curriculum; education. Acad. Emerg. Med. 1997; 4:219-222. I In 1990, SAEM created an interdisciplinary Geriatric Emergency Medicine Task Force through funding by the John A. Hartford Foundation of New York to study the emergency care of elder persons in the United States. This task force concluded that principles of care for elder emergency patients have not been defined and that there was a dearth of education in geriatric emergency medicine.' In 1993, a project to develop a new model and principles of emergency care for the elder patient and a geriatric emergency medicine (EM) curriculum was implemented. This report focuses on the 3 phases in the development of the didactic and teaching material: From the University of Kentucky, College of Medicine, Lexington, KZ Department of Pathology and Laboratory Medicine and Student Testing and Evaluation, Office of Academic Affairs (DBW); and the University of Arizona, College of Medicine, Tucson, AZ, Section of Emergency Medicine, Department of Surgery (ABS). Douglas K. Miller; MD, St. Louis University? St. Louis, MO; John E. Morley, ME, BCh, St. Louis University, St. Louis, MO; Lidia Pousada, MD, New Rochelle Hospital Medical Center; New Rochelle, NY; David B. Reuben,' MD, University of California, Los Angeles, L o s Angeles, CA; Kathleen M. Richmond, RN, BS, Sisters of St. Casimir Injnnary, Chicago, IL;Sharon Sheahan, PhD, CFNP, University of Kentucky, Lexington, K E and Robert H. Woolard, M D , Brown Universiry, Providence, RI. *The following members of the Geriatric Emergency Medicine Task Force of SAEM assisred in the development of the materials in this project: Edward Bernstein. MD. Boston University. Boston, MA; Rawden Evans, PhD, MD, Universiry of Michigan, Ann Arbor; MI; Glenn Freas, MD, JD, Temple University, Philadelphia, PA; Darrin Fryer, MD, Kern Medical Center; Bakersfield, CA; David M. Habben, AS, Paramedic, Consultant. Boise, ID; Richard s. Hartoch. MD, Portland Velerans Affairs Medical Center; Portland, OR; Gordon A. Ireland, P h a d , Sr. Louis University, St. Louis, MO; Jefiey S. Jones, MD, Michigan State University, Grand Rapids, MI; Norm KalbJeisch, MD. Portland Veterans Affairs Medical Center; Portland, OR; Pamela Kidd, RN, PhD, CEN, University of Kentucky? Lexington. KY; Mark Lachs. MD, MPH, Cornell University, New York, NY; Joseph LaMantia, MD, The Albert Einstein College of Medicine, Bronx, Nu; Robert M. McNamara, MD, The Medical College of Pennsylvania, Philadelphia, PA; 1. a needs assessment of what topic areas should be included in the curriculum; Received: March 20, 1996; revision received: June 19, 1996; accepted: June 26, 1996; updated: September I , 1996. This was a project of SAEM sponsored in p a n by the John A. Hartford Foundation of New York Materials described in this article, including textbook, teaching manual, transparencies, and videotapes, are available through SAEM, 901 North Washington Avenue, Lansing, MI 48906-5137; telephone 51 7-485-5484. Address f o r correspondence and reprints: Donald B. Witzke, PhD, Department of Pathology and Laboratory Medicine, University of Kentucky College of Medicine, MN-I03 Chandler Medical Cenrer; Lexington, KY 40536-0084. Fax: 606-323-2076; e-mail: dbwitzl @pop.uky.edu 220 I ACADEMIC EMERGENCY MEDICINE TABLE 1 Geriatric Emergency Medicine Topic Organization ............................................................................. I. The Elder Person’s Special Needs in Emergency Medicine a) Demographics and Emergency Care b) Physiology of Aging c) Pharmacology and Aging d) Ethical Issues e) Attitudes and Ageism 11. Geriatric Emergency Care Model a) b) c) d) Principles of Care ED Environment Out-of-hospital Care ED Geriatric History and Physical Examination e) ED Disposition Planning f) Roles of Health Care Professionals g) Nursing Home Transfer Process 111. Instruments for ED Assessment a) Mental Status-Delirium b) Functional Assessment c) Case Finding IV. Specific Clinical Issues a) Altered Mental Status b) Functional Decline c) Trauma and Falls d) Abuse and Neglect e) Acute Myocardial Infarction f ) Acute Abdominal Pain g) Infections h) Cerebrovascular Accident i) Dizziness 2. the development of a problem-based curriculum to teach the didactic material; and 3. the evaluation of the success in teaching the curric~lum.*-~ Members of the Geriatric Emergency Medicine Education Panel participating in this developmental process included practitioners from EM, geriatrics, nursing, pharmacology, medical education, and emergency medical technicians. I ..................... METHODS Study Design: A cumculum needs assessment was performed by surveying EM educators, emergency nurses, geriatricians, and emergency medical services (EMS) personnel. A problem-based curriculum was designed by members of these health care personnel groups and evaluated among practicing emergency physicians (EPs) who registered for a continuing education course based on the curriculum. Needs Assessment: The first step employed in this initiative was establishing a set of objectives for the development of the training. This effort consisted of generating a list of topics that were relevant to the emergency health MAR 1997 VOL 4 / N O 3 care of the elder person that might form the basis of a geriatric EM A survey of 58 alphabetized topics was created by the education panel members and sent to directors of all E M residency programs in the United States, directors of geriatric fellowship training programs, and convenience samples of emergency nurses and paramedic educators. The survey queried whether each topic was included in the traininghraining materials, whether the topics were essential, and whether they were appropriate in the curriculum (the items are available from the authors). Of the 120 professionals who returned the survey, 50% were EPs, 21% geriatricians, 22% nurses, 2% EMS professionals, 3% EPIgeriatricians, 1% nurseEMS professional, and 1% other. Forty topics were rated as essential by at least 30% of the respondents. The results of the survey were discussed by members of the education panel and a final set of topics to be included was derived (Table 1). From this material the panel also developed a set of 11 principles of geriatric EM (Table 2 ) . Thirty-nine topics were used to create the curriculum and subsequently chosen to be included in the accompanying textbook, case-based instructional modules, or videotapes. These topics were rated as essential or appropriate by at least 87.1% of the respondents. Eleven topics were not included in the training materials (even though they received more than 87% of ratings in the essential and appropriate categories) because discussions of these topics by task force members indicated that they were being taught in other venues. Curriculum Development: Coals: The training goals established were: 1) to improve the emergency care for elder persons, 2 ) to educate emergency health care providers about the special needs of the elder person, and 3) to give emergency health care professionals the knowledge and tools to feel comfortable in giving optimal emergency care to the elder patients. Material Design: Each module (the introduction and 6 cases) contains a specific set of objectives consistent with the goals, around which all of the learning activities and materials are based. All modules are linked to the textbook so that the trainee can read material related to the case discussions. In designing the training, it was decided that a casebased interactive small-group (10-20 people) format would be an effective method of e d u ~ a t i o n . ’ ~ In - ’ ~the introduction to the training, an interactive discussion module presents the principles of geriatric EM and the geriatric emergency care model. We also produced and presented 2 videotapes covering attitudes toward elder persons and the recognition of delirium-2 topics considered difficult to teach by printed material. The design of the 6 cases revolves around the principles and model of geriatric EM care. Each case begins with a fall-one of the common emergency presentations Geriatric EM Cumculum, Wirzke, Sunders of the elder patient. We suggest that typically, emergency medical care professionals appropriately manage the trauma related to the fall, but that it is important to get beyond the trauma to the reasons for the fall. Each case discussion session follows a similar format, beginning with a presentation of the case history. As the case progresses, discussion points are presented to the participants. At the end of each case, the principles of geriatric emergency medical care related to the case are reviewed, along with a summary of key learning issues covered in the case. The instructor has a set of overheads with key teaching issues related to the case and uses these in the session to promote discussion and understanding. Evaluation: Pilot Test: An 8-hour training session was conducted at the annual meeting of SAEM in San Antonio in May 1995. Forty-eight EPs participated in the course. Each of the participants received a draft copy of the textbook. The training consisted of an introduction to care of the elder person, and 6 case-based interactive discussion sessions. Following the introduction, the participants were divided into 3 groups and rotated through 3 small-group casebased discussion sessions. After a break, the 3 groups rotated through the last 3 case-based discussion sessions. All the participants reconvened as a large group for a brief summary of the training, for a question-and-answer period, and to complete a training examination and evaluation. We also asked the participants to provide feedback to the training faculty about the format and content of the training. Course Feedback: Prior to the introduction, a 21-item multiple-choice examination covering the geriatric EM health care model and the conditions represented in each I TABLE 2 Pnnciples of Geriatric Emergency Medicine* ..................................................................... 1. The patient’s presentation is frequently complex. 2. Common diseases manifest atypically in this age group. 3. The confounding effects of comorbid diseases must be considered. 4. Polypharmacy is common and may be a factor in presentation, diagnosis, and management. 5. Recognition of the possibility for cognitive impairment is important. 6. Some diagnostic tests may have different normal values. 7. The likelihood of decreased functional reserve must be anticipated. 8. Social support systems may not be adequate, and patients may need to rely on caregivers. 9. A knowledge of baseline functional status is essential for evaluating new complaints. 10. Health problems must be evaluated for associated psychosocial adjustment. 11. The ED encounter is an opportunity to assess important conditions in the oatient’s Dersonal life. *Adapted with permission from: Sanders AB (ed). Emergency Care of the Elder Person. St. Louis, MO: Beverly Cracom Publications, 1996. 221 I TABLE 3 Geriatric Emergency Medicine Seminar Examination Pretest and Posttest Mean Scores (and Standard Deviations) by Topic .............................................................................. Topic Percentage Correct Significance Pretest Posttest of Re-Post Mean SD Mean SD Change Functional decline Trauma Elder abuselalcoholism Geriatric emergency medicine health care model Delirium Abdominal pain Ischemic heart disease 53 67 63 49 28 33 34 17 89 84 84 78 16 22 24 14 0.000 0.003 0.000 0.000 56 51 43 22 25 35 77 66 46 26 24 36 0.000 0.005 0.676 TOTALTESTSCORE 54 13 77 11 0.000 of the 6 cases was administered to all participants. At the end of the training, a posttest, consisting of the same multiple-choice items presented in a different order than the pretest, was administered. At the conclusion of each module, the participants were asked to complete a brief 3-item evaluation about each session. To obtain feedback prior to the final design of the training and training materials, the participants were asked t o rate the utility and the format of each training module, as well as the overall workshop. The participants also were asked to indicate whether they would recommend the session or the entire workshop to others. The participants used a 4-point rating scale to evaluate each item; 1 = less than adequate, 2 = adequate, 3 = more than adequate, and 4 = outstanding. After the brief concluding session, the participants were asked to provide their feedback about each portion of the training program. Data Analysis: Internal consistency (reliability) for the pre- and posttests was determined using Cronbach’s a. Knowledge gain was determined using the correlated measures t-test. A p-value of c0.05 was considered significant. I RESULTS ............................................................... Pretest/Posttest: Internal consistency reliabilities (Cronbach’s a)for the pretest and posttest were 0.47 and 0.46, respectively. The percentage of the 46 participants answering items correctly on the pretest ranged from 7% to 85%, with the average percentage correct being 54% (SD = 13%). On the posttest, the percentage of the 43 participants answering the items correctly ranged from 35% to loo%, with the average being 77% (SD = 11%). This change was significant at p c 0.001 (correlated-measures t-test). Correlated-measures t-tests showed significant improvement in content knowledge in the posttest compared with the pretest in the overview as well as for 5 of 6 case modules (Table 3). 222 ACADEMIC EMERGENCY MEDICINE MAR 1997 VOL 4/NO 3 Subjective Evaluation: Thirty-five of the 48 participants completed evaluations for the overall training. The average number of participants completing evaluations for each of the 7 teaching sessions was 32 and ranged from 14 to 38. The average ratings for the overall training were: 3.7 on a 4.0 scale for “overall utility of workshop”; 3.4 for “overall format of workshop”; and 3.4 for “would recommend entire workshop to others.” to which we can generalize the effectiveness of ou; training is limited. This report is designed primarily to describe the process used to develop the curriculum. This process may be useful in the development of other special areas in EM. In the future, it would be useful to track the use of this material in EM training and assess its effect on the treatment of the elder person. I DISCUSSION I CONCLUSION Previous studies have shown a need for training emergency health care professionals in the care of the elder Our solution to this problem was the development of training materials and a workshop that individuals involved with teaching emergency health care professionals could use in their institutions. In this regard, we were careful to construct a workshop that could be used by a variety of professionals in a wide variety of sessions and formats. This concern for an interdisciplinary approach to the problem of emergency health care of the elder population is highlighted by the backgrounds of the professionals represented on the education panel. The process of determining topics relevant to geriatric EM resulted in a number of important medical conditions’ being eliminated from our training materials. The limitations and restrictions imposed by the design of our training and the goals of the project made many of these decisions difficult. However, through many telephone conferences of the education panel, decisions about eliminating or including any topic were made on the basis of consensus agreement. The final list of topics we included in our training and training materials reflects issues that we believe are not adequately covered in most current training programs about the elder person. The decision to use a case-based discussion format for the presentation of a geriatric EM curriculum was not made lightly. A thorough discussion of the format was conducted among panel members. Both the personal experience of the members and the evidence from the casebased instruction literature supporting the effectiveness of such an approach for adult learners influenced the decision for the cased-based format. The process of developing a curriculum for geriatric EM is described. Consensus was used to develop principles of geriatric EM and to choose specific topics for didactics. The initial training of instructors was effective in improving the participants’ knowledge of geriatric issues in EM. The participants considered the training to be effective. The effect of the training on the emergency care of elder persons remains to be determined. I LIMITATIONS AND FUTURE OUESTIONS .. . ....... As discussed previously, our data are limited by the small numbers of trainees and questions posed. It is possible that our item sample of 21 questions was insufficient to adequately measure change or that the use of the same test items on both the pretest and the posttest may reflect only a focused learning of the content of these test items. Also, the low reliability on both the pretest and the posttest considerably limits the reliability of the change score, and may indicate that the basis for the change is a random effect. If any of these conditions is true, then the degree I REFERENCES 1. Sanders AB, Care of the elderly in emergency departments: conclusions and recommendations. Ann Emerg Med. 1992; 21:830-4. 2. Sanders AB (ed). Emergency Care of the Elder Person. St. Louis, MO: Beverly Cracom Publications, 1996. 3. Sanders AB (ed). Instructor’s Manual: Emergency Care of the Elder Person. Lansing, MI: SAEM, 1996. 4. SAEM Geriatric Emergency Medicine Task Force. Elder Persons in the Emergency Medical Care System [videotape]. Lansing, MI: SAEM, 1996. 5. Miller DK. Recognizing Delirium in the Elder Person, Perspectives for the Emergency Care Professional [videotape]. St. Louis, MO: Beverly Cracom Publications, 1996. 6 . Sanders AB. Care of the elderly in emergency departments: where do we stand? Ann Emerg Med. 1992; 21:792-5. 7. McNamara RM, Rousseau E, Sanders AB. Geriatric emergency medicine: a survey of practicing emergency physicians. Ann Emerg Med. 1992; 21 :796-801. 8. Singal BM, Hedges JR, Rousseau EW, et al. Geriatric patient emergency visits. Part I: comparison of visits by geriatric and younger patients. Ann Emerg Med. 1992; 21:802-7. 9. Hedges JR, Singal BM, Rousseau EW, et al. Geriatric patient emergency visits. Part 11: perception of visits by geriatric and younger patients. Ann Emerg Med. 1992; 21:808-13. 10. Baraff LJ, Bernstein E, Bradley K, et al. Perceptions of emergency care by the elderly: results of multicenter focus group interviews. Ann Emerg Med. 1992; 21:814-8. 11. Strange GR, Chen EH, Sanders AB. Use of emergency departments by elderly patients: projections from a multicenter data base. Ann Emerg Med. 1992; 21:819-24. 12. Jones JS, Rousseau EW, Schropp MA, Sanders AB. Geriatric training in emergency medicine residency programs. Ann Emerg Med. 1992; 21 ~ 8 2 -9. 5 13. Norman GR, Schmidt HC. The psychological basis of problembased learning: a review of the evidence. Acad Med. 1992; 6755765. 14. Dolmans DHJM, Gijselaers WH, Schmidt HG, van der Meer SB. Problem effectiveness in a course using problem-based learning. Acad Med. 1993; 681207-13. 15. Christensen CR, Hansen AJ. Teaching and the Case Method: Test, Cases, and Readings. Boston, MA: Harvard Business School, 1987.