(StAMPS) Preparation Practice Scenarios
advertisement
 Preparation Practice Scenarios")
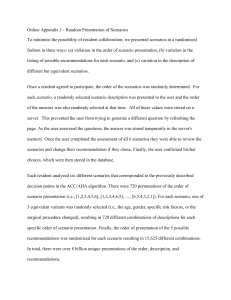
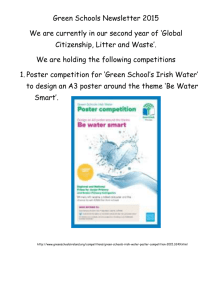
Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation including Practice Scenarios 1. Preparing for the StAMPS assessment process The information provided in this first section is a ‘generic’ discussion about the StAMPS assessment. The following sections provide some sample ‘practice’ exams and discuss in finer detail what is relevant to the specific StAMPS examination. (NB at this stage there are only examples from the Primary Curriculum and Emergency Medicine examinations available). StAMPS is an assessment modality that is designed to test higher order functions in a highly contextualised framework where candidates have the opportunity to explain what they do and demonstrate their clinical reasoning for a given scenario, as opposed to simply providing evidence of knowledge, listing facts or recalling protocols. The methodology for this assessment has been extensively researched and found to be a high level tool; StAMPS has been accepted as such by the Australian Medical Council (AMC). StAMPS is essentially a ‘hybrid’ between a viva voce and OSCE examination with the emphasis on the viva voce. Candidates are strongly advised to consider the relevant curriculum statements and prescribed reading list when preparing for the assessment, as well as familiarising themselves with the format of this assessment modality. The Primary Curriculum Assessment Blueprint provides a good guide as to which domain areas the StAMPS examination will focus on and is also of benefit for the AST StAMPs assessments. 2. What does StAMPS assess? 1. 2. 3. Is the candidate a safe clinician to work both independently and unsupervised in rural and/or remote primary care practice? Does the candidate demonstrate appropriate clinical reasoning rather than simply demonstrating recollection of facts? Has the candidate presented their answers in the context of the set geographical and logistical environment where the exam is set? How does it work? Candidates have access to a single 'Community Profile' available on the Assessment webpage. This document details the setting where the examination is deemed to be taking place and the context in which the candidate is required to answer the questions. The purpose of providing the ‘setting’ of the examination is to ensure uniformity for all candidates and to ensure that candidates are able to demonstrate how such demographic constraints may influence how they proceed with the management of the cases presented. For the Emergency Medicine exam, there is an additional supplementary profile used for some of the scenarios, that assumes the candidate works at a larger regional emergency department for a couple of weeks a year (refer to the following section on Emergency Medicine for further details). NB: All other ASTs (Adult Internal Medicine, Mental Health, Paediatrics and Surgery) will only have the single ‘Community Profile’ for their examinations. 2 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 Number of Scenarios Each examination consists of 8 scenarios. The scenarios cover a broad range of topics chosen from across the entire breadth and depth of the relevant curriculum and are contextualised to ensure the seven domains of practice are examined. Format of the StAMPS exam Candidates are provided with a 10 minute reading time prior to the start of the examination, when they can read the ‘Scenario Information’ provided for each of the 8 scenarios and make notes. Candidates are provided with paper and pencils on the day of the exam. It is recommended that the candidate uses the first 5 minutes of this time to consider the exam as a whole, then the second 5 minutes to focus on the first scenario they are allocated in the examination. Candidates are advised to ensure they are clear about the sequencing in which they will be presented with the eight scenarios. The individual scenarios involve a 10 minute period with an examiner, and consist of 2-4 core questions. The candidate is provided with a ‘time guide’ for the parts in each scenario. The examiner will provide prompts where necessary to assist the candidate. Between each scenario, the candidates have 5 minutes to read the ‘candidate material’ for the next scenario and make notes. The candidate remains in the same room for the duration of the examination, with the examiners moving from room to room between scenarios. Each scenario is examined by the same examiner for the duration of the examination. The relevant Principal examiner (or proxy) will ‘sit in’ with the regular examiners for some scenarios. The Primary Curriculum StAMPS examination is currently offered as either a ‘face-to-face’ or videolink format – refer to the Assessment calendar for details. AST-Emergency Medicine is currently only offered as a ‘face-to-face’ examination and all other AST examinations only as a ‘virtual classroom’ internet link. For both Primary Curriculum and AST-Emergency medicine examination there will be eight different examiners, each responsible for one scenario, for all other ASTs, their will usually only be two examiners, each delivering four scenarios. 3 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 Format of Scenarios Scenarios are developed from actual clinical encounters to ensure they are very firmly based upon ‘real life’ situations. Extensive work is done to ensure the different parts all have a ‘key concept’ which represents the major area to be considered in each part. The ‘key issues’ are expected to elaborate upon the ‘key concept’ and are consistent with current clinical guidelines and best practice (eg the most recent documents are guidelines from the Heart Foundation are used when referencing scenarios involving Acute Coronary Syndrome or management of Rheumatic Heart Disease). Examiners are very aware of situations where there may be differences in approach as dictated by different State Health Department regulations, and thus ensure no group of candidates are disadvantaged by this factor. Every scenario is extensively reviewed by a number of College Fellows or Fellows of other relevant Colleges (eg FACEMs in the case of the Emergency medicine examination). Every scenario is ‘road tested’ by either a candidate or Fellow who has recently sat and passed the relevant examination to ensure wording of the main questions, the prompting questions and the timing of the parts of the scenario are appropriate. Prior to the examination, extensive consideration and consultation has occurred to identify the main issues that should be covered in each part of each scenario. It should be noted that there is no one perfect answer for any given scenario and candidates do not necessarily need to exhaustively list information as there may be a number of different perfectly reasonable approaches to answering the questions posed. The examiners are looking to ensure that Candidates are able to appropriately contextualise their answers and are functioning at the standard expected for a Fellow of the College. The examiners have very carefully considered issues that suggest the candidate is not yet at the standard expected. 4. StAMPS Grades and Marking The examiners assess the candidate’s performance across five categories (below) using a global assessment scale. 1. 2. 3. 4. 5. Overall Impression Develop appropriate management plan that incorporates relevant medical & rural (community profile) contextual factors Define the problem systematically Communication Be flexible in response to new information 4 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 The Global Assessment scale has four categories: 1. Excellent: the examiner considers that the candidate demonstrated a very high level of competency. 2. Satisfactory: the examiner considers that for the curriculum and domains covered by the scenario that the candidate is considered safe to practice independently and unsupervised in the context of rural and/or remote primary care practice. 3. Borderline: the examiner considers that the candidate is not yet ready to practice independently or unsupervised – in this category it may be that some of the elements of the scenario were well covered, but not in others or that the overall performance was below that expected for a satisfactory grade. 4. Unsatisfactory: the examiner considers that from the information gathered in the scenario that the candidate is not yet safe to be practicing independently or unsupervised – this grade is also awarded in the situation where a candidate’s discussion would result in a critical – potentially life threatening or significant morbidity outcome for patient presenting with a given problem. The result of the examination is determined by looking at the grades achieved across the eight scenarios. It should be noted that the standard for the examination is ‘pre-set’ prior to the examination and that there is no statistical adjustment of results. 5. How are the results determined? The grades awarded for ‘overall impression’ are viewed in the first instance: o If a candidate has achieved a satisfactory or higher grade in all 8 scenarios, they will have passed the examination. o If they have achieved a borderline score for one scenario, but satisfactory in the other seven, they will have passed. o In the case of only five scenarios being at a satisfactory or higher grade, the overall result will be a fail. o In those cases where there is not a clear result, the other grading categories are then considered, with the category ‘Develop appropriate management plan that incorporates relevant medical & rural contextual factors’ being the next to be viewed and then if there is still no clear result the other three categories are reviewed. It should be noted that each grading category is viewed individually and that the overall impression is just that, it is not a ‘composite score’ of the other grades awarded for the scenario. The relevant principal examiner carefully reviews every examination result to ensure they are correct. 5 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 6. Examiner Training Examiners who are new to the StAMPS examination undertake specific training to ensure standardised marking/assessment. Examiners also attend update sessions on a regular basis. The following algorithm is an example of the thought process examiners are instructed to use when grading for Overall Impression (very similar algorithms are provided to them for the other categories). Examiners for the primary curriculum examination are looking at this criteria from the perspective of competent generalist primary care provider. For all the ASTs, a higher level of competency is expected, but not at the level of a specialist in the relevant area. StAMPS Algorithm Taking into consideration all the key concepts of this scenario, do you consider the Candidate to be a safe Practitioner? NO YES UNSATISFACTORY GRADE Are they performing at the level expected for FELLOW of ACRRM *Must provide reasons *Was there a significant deficiency? YE S NO BORDERLINE Must comment & provide justification Are they a 'standout' exceptional candidate NO YES SATISFACTORY EXCELLENT 6 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 7. StAMPS helpful hints Before proceeding to consider the practice scenarios, the following general comments may be useful to assist candidates to answer the examination questions in a comprehensive and professional manner. 1. Remember all scenarios are generated from an actual patient consultation/encounter, therefore during the reading time reflect back to when you last saw a patient presenting in a similar manner and think through how you managed that consultation/encounter. 2. Your examiner cannot read your mind, so it is important that you clearly outline your thought processes. For example, don’t just say ‘I’ll proceed to a primary survey’ – you must outline exactly what your approach is, don’t forget the basics such as having the patient in a monitored/resus area for major trauma/medical emergency and briefly discuss how you want them monitored, what IV lines you would insert, whether you would have them on oxygen, what staffing personnel you would want available. a. It may be helpful to think about formulating your answer as though talking a junior doctor through the process to ensure you don’t omit the basic steps. 3. Remember that this is a Fellowship exam and as such you are expected to answer in a highly contextualised manner, not just demonstrating that you remember ‘lists’ from medical school. The context is not only about the medicine, but also the circumstances of the patient and the environment in which you are working. b. Make notes during the 5 minute reading time, identify how the information dictates the context and be sure to demonstrate that you have comprehended the context. For example: a scenario that covers a potentially septic Aboriginal baby that you are assessing in a remote area clinic – identify to your examiner that you recognise the baby is seriously unwell, you may have issues with language and you know how to access the assistance of an Aboriginal Health Worker and you are very unlikely to be able to provide the definite management in your current location so that after initial management you will need to arrange for transport to an appropriate paediatric centre. 4. Pay attention to the time allocation for each part of the scenario, if for example it is one minute, then you are only expected to be providing a very brief ‘outline’ answer, if however it 5 or 6 minutes, then a more detailed and well structured answer is expected (don’t worry here, your examiner will intervene with prompting questions if required). 5. At the end of each day or week, think about one patient consult/encounter you’ve had and ‘construct’ a scenario and work through all the issues raised by that encounter. 6. Enlist help from your supervisor and/or medical educator to run you through ‘practice’ scenarios. Ideally do this under ‘exam’ conditions – have a 5 minute time to think about your response and ensure you allocate a ten minute timeframe to answer. If you are sitting for the AST examinations enlist the help of a specialist colleague in your AST discipline. If sitting for the AST-Emergency Medicine examination, ensure you have recent experience in an Emergency Department supported by FACEMs and where there is supportive supervision. 7. Ensure you are absolutely aware of the guidelines for life support, both BLS and ALS, make sure you are very familiar with legal and ethical issues, eg you must be able to clearly discuss how you proceed with reporting potential child abuse and issues related to an impaired colleague. 7 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 8. The examiners have been very clearly instructed to assist you to demonstrate your competency in managing the scenario presented. a. If your examiner interrupts you, it is with the intention of providing guidance to assist you to provide the desired discussion. b. If you don’t understand what your examiner has asked, seek clarification. 9. No one works in professional isolation, so remember to discuss with your examiner the circumstances under which you would call a specialist colleague for advice and when you will arrange for your patient to be referred to another centre for ongoing management. In the situation where transport is required, be sure to discuss the potential issues with this and how you prepare for transfer of care. 10. Make sure you are familiar with the relevant curriculum for the examination and ensure you revise those areas that you may not be so familiar or comfortable with. Look at the Assessment blueprint – it will guide you to those domain areas most likely to occur in the examination. 11. Consider undertaking the emergency courses prior to the examination if this is an area you have limited experience in. The ALSO course is highly beneficial for those candidates with limited obstetric experience. 12. Read through your local hospital guidelines for managing trauma and medical emergencies. 13. Finally, remember that this is a Fellowship exam and if you are enrolled, then you should have undertaken the necessary training and have the necessary experience, so think of it as an opportunity to demonstrate to your examiners that you are ready to be practicing independently and without supervisor, so relax and ENJOY! 8 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 8. Practice scenarios The ‘practice’ scenarios presented are examples from past examinations. The Information provided to Candidates on the following page is the information that is given to the Candidates at the commencement of the examination; the following table on the next page is the actual document from which the examiner works. On the examiner document you will see that there are 4 columns: the first is an indication of the time to spend on each part; the second is the question that the examiner will ask (this is delivered word-for-word exactly the same to every candidate); the third column lists both the ‘key concept’ which is the over-riding or headline issue to be discussed with a breakdown of ‘key issues’; the final column is a list of possible questions the examiner may ask if the candidate hasn’t spontaneously offered the requisite information. It needs to be noted that the ‘key issue’ section is heavily referenced against current guidelines/best practice, but is not necessarily totally extensive, furthermore a candidate may well pass without mentioning everything on that list. Suggested approach: 1. Read through the ‘Information to Candidate’, make notes. 2. Think about the time allocation for each part and then proceed to answer the primary questions; ideally to do this without looking at the third column which lists the points expected. 3. Read through the notes at the end of the scenario to familiarise yourself on the standard expected – this section will discuss issues that will lead to a fail grade and those that may result in a borderline grade. 9 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 ACRRM Primary Curriculum -StAMPS Examination Example ‘Practice’ Scenario: 1 Scenario Information provided to Candidate: Maria is a 59-year-old widowed cleaner who lives on her own in town. Her four children and five young grandchildren all live in the regional city 500km away. She was diagnosed with type 2 diabetes 10 years ago and hypertension five years ago. Her diabetes has been well controlled with her HbA1c usually in the range 7.0-7.5% (53-58mmol/mol) until the death of her husband thirteen months ago. Her blood pressure recordings over the past 2 years have all been <130/75 mmHg. She usually presents for regular review every three months after her routine pathology tests. Unusually, she failed to present for her most recent review and was recalled last week to have her overdue routine bloods done. Her usual medications include: Insulin glargine 30 units SC mane Metformin extended release 2g PO mane Gliclazide modified release 90mg PO mane Perindopril 5mg PO mane Aspirin 100mg PO mane Today, fingerprick random blood glucose is 22.0mmol/L, seated blood pressure is 165/90mmHg, From the pathology test taken last week her HbA1c was 10.8% (95mmol/mol) and her albumin: creatinine ratio was 28mg/mmol (normal range <3.5mg/mmol). Her weight has increased and her body mass index is now 37, up from 34 at her last visit five months ago. She tells you she stopped taking her insulin glargine a few weeks ago because it was making her feel puffy and sluggish. She avoids eye contact and appears untidy and exhausted. This scenario has 3 Parts: estimated time for each Part: Part 1 – 1 minute, Part 2 – 6 minutes, Part 3 – 3 minutes 1 1/60 2 6/60 3 3/60 Questions Key Concepts/Issue to be Demonstrated Very briefly, what are the areas of concern that need to be addressed during this consult? Key Concept: Identifies that this presentation has two key components Deteriorating diabetic control Possible underlying depression or development of hypothyroidism Key Concept: Demonstrates clear understanding of depression – diagnosis and management Prepared to explore the possible diagnosis of depression with Maria Takes a clear mental health history – must include symptoms that may indicate endogenous depression Explores patient’s safety and excludes suicidal intent Demonstrates familiarity with various diagnostic tools (eg K10, DASS, SPHERE) and can discuss the relative merits of them Considers appropriate testing to investigate differential diagnoses for depression eg FBE, EUC, LFTs, calcium, TSH, iron studies, B12, folate, CRP, ESR, sleep studies Elaborates a plan to further explore this possible diagnosis: engages with mental health team as appropriate Preliminary discussion of possible medication – able to discuss the merits of the different classes of antidepressants Identifies a clear time frame for review on this issue Demonstrates understanding of and explores issue of potential social isolation from family Discusses support services available within the community and access to them Discusses work issues, concerns re possible retirement and consequences of that for her both financially and with respect to friendships, support Key Concept: Demonstrates sound understanding of the principles of management of patients with type 2 diabetes Demonstrates appreciation of the implications of: 1. Deterioration in HbA1c 2. High random BSL 3. BP measurement 4. Increase in BMI 5. Possible renal impairment – raised ACR 6. Non-compliance with medication – explores if compliant with oral Rx recently Exploration of the patient’s expectations around management Arranges further investigations re: high HbA1c and ACR: requests EUC, lipid profile Discusses lifestyle factors of smoking/diet/exercise Demonstration of clear management plan that will prioritize issues for this patient Refers back to of the key psycho-social issues for this patients ability to manage her chronic disease: probable depression/abnormal grief reaction, isolated from family Involvement of associated practitioners: ophthalmologist / optometrist / dentist / podiatrist / dietician / diabetes educator / endocrinologist You’ve identified that depression may be a significant factor affecting Maria’s capacity for self care. How would you explore this further with her today? What are the key issues regarding her diabetic control you would want to address? Possible Prompting Questions Why do you think her results have changed so much? How will you establish the severity of Maria’s depression? What further assessments might you use? What pathology tests will you order? Who might you refer Maria to? Generally speaking, how do you decide which antidepressant to use? Would you start antidepressant medication today? If so what? What follow-up arrangements might you make? What are the key areas that must be regularly addressed with diabetic patients and why? Are there any other investigations you might like to do and why? How would you explore Maria’s expectations of her management? Why might Maria be reluctant to comply with her medication regime? 11 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 References: 1. General practice management of type 2 diabetes, 2014–2015. 176-page document co-written by RACGP and Diabetes Australia. Available online at http://www.healthinfonet.ecu.edu.au/key-resources/promotion-resources?lid=28068 2. Assessing patients with depression [revised February 2013]. In: eTG complete [Internet]. Melbourne: Therapeutic Guidelines Limited; March 2014. (Home > Psychotropic > Depression > Assessing patients with depression) 3. Principles of treatment [revised February 2013]. In: eTG complete [Internet]. Melbourne: Therapeutic Guidelines Limited; March 2014. (Home > Psychotropic > Depression > Treatment of depression > Principles of treatment) 12 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 Comments on how this scenario would be graded to result in either a borderline or fail grade: Ideally a candidate would set the scene to the examiner very briefly outlining that there are two primary issues here: o 1: Deteriorating Diabetic control and o 2: Possible depression At the start of the second question, the examiner is telling you that you’ve identified depression as a strong possibility it is therefore essential that you discuss: o An assessment of suicidal risk – failure to do this would result in an automatic fail for this station, NB there are a couple of prompting questions to more deeply probe how you assess the severity of the depression which should lead to a discussion of suicide risk. Your examiner will not however directly ask you how to assess for suicide risk as this is something that should be an automatic consideration for someone at Fellowship level. o A failure to consider the potential organic causes for depression and/or a limited approach to general management would likely lead to a borderline grade. The primary question for the third part asks about the key issues regarding diabetic control: o A failure to identify that her control has significantly deteriorated would result in a fail. o A limited approach to the cornerstones of diabetic management may result in a borderline grade. It is expected that there would be a discussion regarding HbA1c significance, BP, Weight and renal function issues. 13 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 AST Emergency Medicine NB for this examination, scenarios will either be based in the environment provided by the ‘Community Profile’ posted on the website or in a larger Regional Hospital as provided to you prior to the examination. It will be clearly stated at the start of each scenario as to which environment you are working from. 14 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 ACRRM AST-EM StAMPS Examination: Example ‘Practice’ Scenario Number: 1 Scenario Information provided to Candidate: You are called to your local hospital’s emergency department (as per the ‘Community profile’) to see David who is a 53-year-old man brought in by ambulance after falling from a ladder onto his L chest; now complaining of severe left sided pleuritic chest pain and shortness of breath. He arrives in a cervical collar. Vital signs: Pulse 106/min regular, BP: 142/88 mmHg, Respiratory rate 22/min, Oxygen saturation 96% on room air, GCS 15. Past medical history: Type 1 Diabetes (Dx age 18years), Hypertension, GORD Medication: Insulin glargine 46units SC OD, Insulin novorapid SC TDS (as per sliding scale), Ramipril 10mg PO mane No known drug allergies. NB: A major storm front has passed through and all roads are blocked and the airstrip closed for the next twelve hours. This scenario has 2 Parts: estimated time for each Part: Part 1 – 5 minute, Part 2 – 5 minutes 15 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 Step 1 5/60 Questions Please discuss your approach to assessing this patient, bearing in mind the limited facilities available to you at your local hospital Key Concepts/Issue to be Demonstrated 5/60 During your initial trauma assessment a CXR has been taken by your portable machine, This is the view that has come up on your machine please report on this and discuss your management. Key concept: Demonstrates appropriately structured and safe assessment of trauma patient. 2 Possible Prompting Questions Key Concept: Recognises significant surgical emphysema and small pneumothorax requiring insertion of Left intercostal catheter. Considers the ABCs, but recognises this patient currently has patent airway, oxygenating adequately and has an acceptable circulation. Ensures appropriate monitoring, IV access, checks BSL (essential), ECG Provides analgesia – able to discuss issues related to this and risks of developing respiratory drive/hypotension o Able to sensibly discuss possible regimes – paracetamol IV, opiates – aware of titration, supplementation with ketamine, possible paravertebral block Obtains appropriate history to assist risk stratification of mechanism of injury: o Establishes height of fall and onto what sort of surface -able to discuss mechanism of injury in general terms to assess risk for significant injury o Establishes if fall was attributable to syncopal episode – Diabetic – possible hypo/hyper episode, possible cerebral or cardiac event. Appropriate examination, addressing ABC, Cx, Tx/Lx spine, secondary survey Considers potential injuries: o Possible Head injury -No CT scan available at small hospital, will ensure neuro obs taken and repeated as indicated Able to discuss some guideline re scanning in general, eg Canadian CT rules. o Probable Chest injury – CXR, + USS if trained o Possible abdominal injury – USS eFAST o Considers Cervical spine injury - aware of Canadian or other Cx criteria – may do plain XRays if indicated o Considers other spinal injury: log roll (being very cognisant of possible L chest trauma). o Possible other injuries as yet not detected (e.g. limb fractures, soft tissue injuries) – appropriate secondary survey Discusses investigations as may be appropriate as above and bloods – including G&M depending on degree of trauma Recognises marked surgical emphysema of Left chest, should (but not essential) th pick up on small apical pneumothorax and 8 rib #. Recognises need for ICC insertion What monitoring is required? How do you assess the risk stratification for this patient? Given his past medical history what are some other key considerations? What injuries do you think are likely in this case and how will you assess them in your current setting? o Any other? What are the potential issues related to providing adequate analgesia in this patient? o What regimes might you consider? He is very irritated by the Cx collar; can you remove it for him? In a different situation where you have ready access to all imaging, how do you decide on your imaging requests? What’s the implication of those findings you’ve mentioned on the Xrays? How do you prepare a patient for the insertion of an ICC? Please discuss in detail how you will insert an ICC? 16 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 Able to discuss preparation for and technique of insertion of ICC: o Explanation of procedure to patient and any family o Consent from patient o Choice of catheter size o Appropriate monitoring o Analgesia Able to discuss the technique of insertion o Anatomical landmarks – recognises that insertion may be more difficult due to the surgical emphysema o Process of dissection to insert o Discusses how they secure the tube and dress the site o Checks functioning of underwater seal drain – ensures swinging o Orders check CXR Discusses disposition, may need for referral to surgical unit for ongoing acute care. Where does this patient need to be and why? 17 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 18 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 References: Initial evaluation and management of blunt thoracic trauma in adults: Author: Eric Legome, MD Section Editor: Maria E Moreira, MD Deputy Editor: Jonathan Grayzel, MD, FAAEM EMST workbook 19 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014 Comments on how this scenario would be graded to result in either a borderline or fail grade: The first question requires a consideration that the risk stratification for the fall needs to be considered for this patient. o A fail grade would be awarded if: There is no clearly structured approach to a primary survey with appropriate monitoring Failure to consider a medical cause for the fall – specifically mentioning possible hypoglycaemia, potential hyperglycaemia or DKA and ACS (Type 1 diabetic) Focused only on possible chest trauma, lack of consideration of the risk stratification vital to comment to your examiner how you do this – in this case need to mention height of fall. o A borderline grade may be awarded where there was limited discussion of risk stratification, limited discussion of appropriate imaging given the constraints of the health service and lack of consideration of analgesia. o NB there are extensive prompting questions to assist candidates to cover all these issues. The second part of the question requires recognition of extensive surgical emphysema and the need for intercostal catheter and transfer to a centre suited to management of this. o A Fail grade would be awarded if: CXR inadequately reported Unable to discuss approach to ICC Overall a lack of appreciation and failure to contextualise the potential complexities in this case and lack of planning for disposition of this patient would likely result in either a fail or borderline depending on how limited the discussion. 20 StAMPS Practice Scenarios Structured Assessment using Multiple Patient Scenarios (StAMPS) Preparation V1 2014