Muscle Activation Levels of the Gluteus Maximus and

Journal of Sport Rehabilitation, 2014, 23, 1-11 http://dx.doi.org/10.1123/JSR.2012-0082
© 2014 Human Kinetics, Inc.
www.JSR-Journal.com
ORIGINAL RESEARCH REPORT
Muscle Activation Levels of the Gluteus Maximus and Medius During Standing Hip-Joint-Strengthening
Exercises Using Elastic-Tubing Resistance
James W. Youdas, Kady E. Adams, John E. Bertucci, Koel J. Brooks,
Meghan M. Nelson, and John H. Hollman
Context: No published studies have compared muscle activation levels simultaneously for the gluteus maximus and medius muscles of stance and moving limbs during standing hip-joint strengthening while using elastictubing resistance. Objective: To quantify activation levels bilaterally of the gluteus maximus and medius during resisted lower-extremity standing exercises using elastic tubing for the cross-over, reverse cross-over, front-pull, and back-pull exercise conditions. Design: Repeated measures. Setting: Laboratory. Participants:
26 active and healthy people, 13 men (25 ± 3 y) and 13 women (24 ± 1 y). Intervention: Subjects completed
3 consecutive repetitions of lower-extremity exercises in random order. Main Outcome Measures: Surface electromyographic (EMG) signals were normalized to peak activity in the maximum voluntary isometric contraction (MVIC) trial and expressed as a percentage. Magnitudes of EMG recruitment were analyzed with a
2 × 4 repeated-measures ANOVA for each muscle ( α = .05). Results: For the gluteus maximus an interaction between exercise and limb factor was significant (F
3,75
= 21.5; P < .001). The moving-limb gluteus maximus was activated more than the stance limb’s during the back-pull exercise (P < .001), and moving-limb gluteus maximus muscle recruitment was greater for the back-pull exercise than for the cross-over, reverse cross-over, and front-pull exercises (P < .001). For the gluteus medius an interaction between exercise and limb factor was significant (F
3,75
= 3.7; P < .03). Gluteus medius muscle recruitment (% MVIC) was greater in the stance limb than moving limb when performing the front-pull exercise (P < .001). Moving-limb gluteus medius muscle recruitment was greater for the reverse cross-over exercise than for the cross-over, front-pull, and back-pull exercises (P < .001). Conclusions: From a clinical standpoint there is no therapeutic benefit to selectively activate the gluteus maximus and gluteus medius muscles on the stance limb by resisting sagittal- and frontalplane hip movements on the moving limb using resistance supplied by elastic tubing.
Keywords: lower extremity, muscle performance, muscle endurance, active resisted exercise
Enhanced muscle performance or strength is frequently the primary goal of health care professionals when designing a rehabilitation program for patients.
Strengthening modes use isometric, isotonic, and isokinetic muscle activations 1–4 that challenge the muscle to function at unaccustomed levels.
5 Rehabilitation professionals use strengthening exercises for the gluteus maximus and medius in patients with a variety of musculoskeletal disorders including patellofemoral pain syndrome, 6–9 iliotibial band syndrome, 10–13 total hip arthroplasty, 14–16 total knee arthroplasty, 17 anterior cruciate ligament injury as a consequence of medial collapse of the knee, 18,19 and chronic ankle instability.
20–22
Elastic tubing has become an accepted mode of resistance training over the past 20 years among health care workers for the following reasons: low
The authors are with the Program in Physical Therapy, Mayo
Clinic, Rochester, MN.
cost, simplicity, portability, versatility, and no reliance on gravity for resistance.
2 Elastic-tubing resistance is ideal for home-based rehabilitation programs where weight machines may not be available or feasible.
23
Numerous reports exist on the usefulness of elastictubing resistance when strengthening both upper and lower extremities in a variety of patient groups.
24–29
Four popular standing weight-bearing exercises for hipmuscle strengthening use resistance provided by elastic tubing and include the front-pull (Figure 1), back-pull
(Figure 2), cross-over (Figure 3), and reverse-crossover procedures (Figure 4).
30–33 The moving non-weightbearing limb is attached to the elastic tubing by an ankle anchor cuff while the stance limb remains stationary on the support surface.
Electromyography (EMG) records motor-unit activity in a muscle or group of muscles. Researchers in health and wellness professions use EMG to observe and quantify differences in muscle activity between exercise conditions.
34,35 Investigators have discovered that higher
1
2 Youdas et al
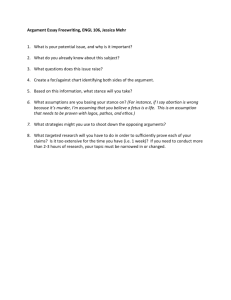
Figure 1 — Front pull. The elastic tubing is attached to the dominant left limb using an ankle anchor. With hands on hips and balancing on the right stance limb, the subject positions the moving limb posterior to the stance limb. Next, the subject flexes the hip and knee of the moving limb, pulling the tubing forward. The subject then slowly returns the moving limb to the starting position.
Figure 2 — Back pull. The elastic tubing is attached to the dominant left limb using an ankle anchor. With hands on hips and balancing on the right stance limb, the subject positions the moving limb anterior to the stance limb. Next, the subject extends the hip and knee of the moving limb, pulling the tubing posterior. The subject then slowly returns the moving limb to the starting position.
EMG signals correspond with larger strength gains.
Andersen et al 36 and Ayotte et al 37 suggest that 40% to
60% maximum voluntary isometric contraction (MVIC) is necessary to obtain strength gains. Presently there is an absence of information describing the relative activation or recruitment levels (% MVIC) of the gluteal muscles during standing weight-bearing strengthening exercises using elastic-tubing resistance.
The purpose of this study was to quantify EMG activation levels simultaneously in the gluteus maximus and medius muscles of the moving and stance limbs across the performance of 4 exercises used to strengthen hip muscles in standing using resistance provided by elastic tubing. During hip-joint-strengthening exercises in standing, using elastic-tubing resistance, the gluteus maximus and medius muscles on the stance limb must stabilize the pelvis to prevent undesirable compensatory movements of the pelvis in the transverse and frontal planes 38,39 while the primary movements are produced by the moving side. We hypothesized that the gluteus maximus and medius on the stance limb would demonstrate greater EMG activation (% MVIC) than their counterparts on the moving limb while standing using silver Theraband elastic-tubing resistance. We based this hypothesis on evidence that the weight-bearing limb bears 84% (5/6) of the body weight during single-limb stance.
39 Furthermore, in a recent study, bilateral activation and recruitment levels (% MVIC) of the gluteus medius and maximus were recorded simultaneously in stance and moving limbs during resisted lateral band walking in healthy young men and women. Both muscles demonstrated greater activation on the stance limb than the moving limb.
40 Results from the current study will provide clinicians information about bilateral muscle activation of the gluteus maximus and gluteus medius during standing exercises. Such information would be
Muscle Activation Levels During Hip-Joint Strengthening 3
Figure 3 — Cross-over. The elastic tubing is attached to the dominant left limb using an ankle anchor. While balancing on the right stance foot with hands on hips, the subject adducts the moving left foot in front of the right foot, pulling the tubing toward the stance side. The subject then slowly returns the moving limb to the starting position.
Figure 4 — Reverse cross-over. The elastic tubing is attached to the dominant left limb using an ankle anchor. While balancing on the right stance foot with hands on hips, the subject abducts the moving left foot in front of the right foot, pulling the tubing away from the stance side. The subject then slowly returns the moving limb to the starting position.
of interest to rehabilitation professionals when prescribing strengthening exercises for the gluteus maximus and medius using elastic-tubing resistance.
Methods
Design
We used a repeated-measures design to examine the gluteus maximus and medius muscle activation during cardinal-plane lower-extremity-strengthening exercises in weight bearing using elastic resistance.
Participants
Thirteen men (25.3 ± 3.1 y) and 13 women (23.7 ± 1.3 y) volunteered to participate. A priori power analysis determined that a sample size of 22 subjects was required to detect a mean difference in EMG recruitment of
10% MVIC (effect size = 0.20) between conditions with a statistical power (1 – β ) equal to .80 at α = .05.
Demographic information is presented in Table 1. At the time the study was completed, 80% (n = 21) of subjects reported engaging in a lower-extremity strength-training program. Lower-extremity resistance-training programs used free weights, and specific exercises included lunges and dumbbell or barbell squats. All subjects were participating in regular cardiovascular exercise. The average number of days engaged in a physical exercise program was 4 d/wk, with a range of 1 to 6 d/wk. Because each subject verbally reported that he or she had been engaged in a consistent physical-conditioning regimen for at least
12 months before the study, investigators did not attempt to control for subjects’ exercise frequency or type of lower-extremity muscle strengthening. All subjects were screened for normal active range of motion of the hip, knee, ankle, and foot. Subjects self-reporting a history of the following lower extremity conditions were excluded
4 Youdas et al
Table 1 Subject Demographic Information
Gender
Male (n = 13)
Female (n = 13)
Height (cm)
Mean SD
181.5
168.8
5.5
7.5
Mean
Mass (kg)
SD
80.1
64.9
11.6
8.7
Body-Mass Index (kg/m 2 )
Mean
24.2
22.7
SD
2.3
1.6
from the study: previous subluxation, dislocation, or fracture and any condition that limited physical activity for more than 2 days over the last 6 months. Furthermore, subjects were excluded if they had current complaints of neuromuscular pain, numbness, or tingling in the lower extremity and back. Study procedures were approved by the Mayo Clinic institutional review board before the start of the study. Before enrollment in the study, all subjects provided written informed consent and completed a survey that assessed their current level of physical activity.
Instrumentation
Raw EMG signals were collected with Bagnoli DE 3.1 double-differential surface EMG sensors (Delsys Inc,
Boston, MA). Sensor contacts were made from 99.9% pure silver bars 10 mm in length spaced 10 mm apart and encased in preamplifier assemblies measuring 41
× 20 × 5 mm. Preamplifiers had a gain of 10 V/V. The combined preamplifier and main amplifier permitted a gain from 100 to 10,000. Per manufacturer specifications, the common-mode rejection ratio of the system was 92 dB at 60 Hz, input impedance was greater than 10 15 Ω at 100 Hz, and estimated noise was ≤1.2 μ V. Data were collected at a sampling frequency of 1000 Hz through a
16-bit NI-DAQ PCI-6220 analog-to-digital acquisition card (National Instruments Corp, Austin, TX). Raw EMG signals were processed with EMG works Data Acquisition and Analysis software (Delsys Inc). Raw EMG data collected during the tests were band-pass filtered between
20 and 450 Hz with a fourth-order Butterworth filter and subsequently processed with a root-mean-square algorithm using moving windows with 125-millisecond time constants.
Silver Theraband elastic tubing (Hygienic Corp,
Akron, OH) with an internal diameter of 11 mm was used to provide external resistance. One end of the elastic tubing was fastened to the subject’s foot via a dog-leash snap and padded ankle anchor (Stirrup Ankle
Anchor, Therapeutic Dimensions, Inc, Spokane, WA), and the other end of the tubing was connected to a
Chatillon MSC-500 digital dynamometer with another dog-leash snap (Ametek, Largo, FL). The cut piece of tubing measured 1.21 m (4 ft) in length after the band was anchored to the dynamometer and the participant’s ankle. A fresh piece of elastic tubing was used for each subject. We recorded the relationship of the tensile force versus percentage elongation (Figure 5) for the silver
Theraband tubing before the study.
41,42 It was crucial for the investigators to know the actual variation in force of the tubing as a function of length when positioning a subject during each of the 4 exercise conditions. To calculate the relationship of force versus percentage elongation, we selected a 1.21-m piece of silver tubing and sequentially stretched it at 25% increments from
125% to 400% of its original length. The fixed end of the tubing was held in place by an investigator, and the moving end of the silver tubing was anchored to the dynamometer so we could record the tensile force required to elongate the material. The silver tubing was stretched 3 times from 125% to 400% of its resting length. The minimal external resistance provided by the silver Theraband was established at 5% of each subject’s body mass at the start of the concentric portion of each exercise.
31 This external load was selected by pilot testing before formal data collection because the external load provided appropriate resistance without evoking undesirable trunk- or hip-muscle substitution patterns. Tension in the elastic tubing was recorded using a Chatillon MSC-500 digital dynamometer (Ametek,
Largo, FL).
Procedures
Data were collected in a research laboratory by the same
4 coinvestigators, and each investigator was assigned a specific task. All subjects wore appropriate clothing to permit correct placement of EMG electrodes. They wore their own cushioned workout footwear. To allow optimal
EMG reading, each subject’s skin was abraded with an alcohol wipe until erythema was attained. Electrodes were placed superficially parallel to the direction of the muscle fibers on the subject’s left and right lower extremities. Placement of electrodes was based on guidelines of
Criswell and Cram.
43 Surface electrodes were attached to the cleansed area with adhesive interfaces (Delsys Inc,
Boston, MA) and secured with 3M Transpore medical tape (St Paul, MN). A ground electrode was placed on the medial malleolus of the stance leg. Next, subjects performed a series of manual resistance tests using 2- to
3-second hold times to set the gain on the Delsys EMG instrumentation for each muscle and provide subjects several practice trials so they were familiar with the muscle-test procedure. Verbal encouragement was provided during each formal manual muscle test. MVICs of each muscle were collected by using formal manualmuscle-testing techniques as described by Hislop and
Muscle Activation Levels During Hip-Joint Strengthening 5
Figure 5 — The relationship between tension and percent elongation of a 1.21-m (4-ft) section of silver Theraband elastic tubing.
Montgomery.
44 For the gluteus medius the subject was positioned in side-lying with the test lower extremity uppermost. Both thigh and leg were in extension and the lower extremity maintained in line with the trunk.
The untested lower extremity was flexed at the hip and knee for stability. The subject was instructed to abduct the uppermost lower extremity about 30° from midline, whereupon the examiner applied manual resistance just proximal to the malleolus. The gluteus maximus was tested with the subject prone and a pillow placed under the pelvis to provide 10° to 15° of hip flexion. With the knee maintained at 90° of flexion, the subject was instructed to extend the thigh of the tested side through the available hip-extension range of motion. The examiner applied manual resistance at the distal thigh.
Before data collection, each subject practiced performing the 4 resisted hip exercises until the movement patterns could be repeated to the investigator’s satisfaction. During these practice trials another investigator used the dynamometer to simultaneously record peak external tension in the tubing. This information was immediately reported to the subject until he or she could reproduce the external load within an interval ranging from 5% to 10% of body mass [%BM]. Each subject then completed trials of the 4 exercises in random order by performing 3 consecutive repetitions of each exercise.
We chose to use 3 repetitions of each exercise because we believed that subjects could complete 3 repetitions with proper form and without fatigue. Before data acquisition, exercise trial order was established by having a subject sequentially select 4 cards, each designating a specific exercise condition. Hip-joint range of motion was not controlled during each exercise condition. For the frontpull exercise, the moving lower extremity was advanced into femoral-on-pelvic and tibial-on-femoral flexion against resistance provided by the tubing while the subject balanced on the stance limb (Figure 1). During the back pull the moving limb relocated from a position of femoral-on-pelvic and tibial-on-femoral flexion into femoral-on-pelvic and tibial-on-femoral extension while the subject balanced on the stance-limb foot (Figure
2). The cross-over exercise involved femoral-on-pelvic adduction of the moving lower limb against resistance provided by the elastic tubing while the subject balanced on the stance-limb foot (Figure 3). In contrast, the reverse cross-over exercise involved femoral-on-pelvic abduction of the moving limb while the subject balanced on the stance limb (Figure 4). A coinvestigator demonstrated to the subject the correct overall body position for each of the exercises. Each subject correctly performed an exercise according to the approval of an investigator before EMG data were collected. A metronome set at
40 beats/min was used to standardize the duration of the 3 exercise repetitions. Subjects began each exercise in the appropriate position and performed 3 consecutive repetitions for each of the 4 randomized trial exercises.
Subjects were trained to complete each repetition—start to end range and back to the start position—within a
2-beat duration on the metronome. There was no hold time at the end range of each exercise. The subject was allowed a brief recovery period (2–3 min) between trials as the tubing was adjusted for the subsequent trial. The duration of recovery time was established during pilot testing according to feedback provided by the subjects.
Recovery-time duration was monitored by a stopwatch.
Verbal cues were used to signal to the subject to begin the 3 repetitions when he or she was ready. Repetitions were counted out loud by the examiners. We analyzed
6 Youdas et al the highest peak of the 3 repetitions during the concentric activation component, and its value was expressed as %MVIC for each muscle on both stance and moving limbs. Peak amplitudes were averaged over a 500-millisecond window of time, 250 milliseconds before peak and 250 milliseconds after the peak.
Statistical Analyses
EMG activation (%MVIC) of men and women was compared for each muscle (gluteus maximus and medius) over the 4 exercise conditions on both moving and stance limbs for a total of 16 comparisons. One comparison demonstrated a significant difference, so we chose to combine data for men and women. Descriptive statistics including means and standard deviations
(SDs) for EMG recruitment (%MVIC) in the gluteus maximus and medius were calculated for both stance and moving sides during the 4 exercises. Magnitudes of
EMG recruitment were analyzed with a 2 × 4 (2 sides
[stance limb vs moving limb] by 4 exercise conditions) repeated-measures analysis of variance (ANOVA) for each muscle included in the study ( α = .05). Post hoc simple-effects tests with Bonferroni-adjusted α were used to control α for multiple comparisons and to analyze pairwise comparisons in EMG recruitment between sides and exercise conditions when main effects of leg-position-by-exercise-condition interactions were statistically significant. Greenhouse-Geiser adjustments for degrees of freedom were applied when assumptions of sphericity were violated.
Using 1-way repeated-measures ANOVA, we also analyzed peak tension forces in %BM generated in the elastic tubing by the moving limb during each of the 4 exercise conditions. Post hoc simple-effects tests with
Bonferroni-adjusted α were used to control α for multiple comparisons and to analyze pairwise comparisons.
Data were analyzed using SPSS 17.0 software (IBM
Corp, Armonk, NY).
Results
Gluteus Maximus
Interaction between exercise and limb factor was significant (F
3,75
= 21.5; P < .001). Post hoc analyses comparing muscle activation between moving and stance limbs for a given exercise, as well as between exercises for a given limb, are found in Table 2. The moving-limb gluteus maximus was activated more highly than that of the stance limb during the back-pull exercise (P < .001). For the moving limb, gluteus maximus muscle recruitment was greater for the back-pull exercise than for the cross-over, reverse cross-over, and front-pull exercises (P < .001).
Stance-limb gluteus maximus muscle recruitment was greater in the reverse cross-over (P = .032) and front-pull
(P = .004) exercises than the cross-over exercise. No exercise exceeded the 50% MVIC threshold for strengthening.
Gluteus Medius
The interaction between exercise and limb factor was significant (F
3,75
= 3.7; P < .03). Post hoc analyses comparing muscle activation between moving and stance limbs for a given exercise, as well as between exercises for a given limb, are found in Table 3. Gluteus medius muscle recruitment (%MVIC) was greater in the stance limb than moving limb when performing the front-pull exercise (P < .001). For the moving limb, gluteus medius muscle recruitment was (1) greater for the reverse crossover exercise than for the cross-over, front-pull, and backpull exercises (P < .001) and (2) greater in the back-pull exercise than in the cross-over (P = .001) and front-pull exercises (P = .007). Stance-limb gluteus medius muscle recruitment was (1) greater for reverse cross-over than for cross-over, front-pull, and back-pull exercises (P < .001) and (2) greater for the back-pull and front-pull exercises than for the cross-over exercise (P < .001). The reverse cross-over exercise exceeded and reached 50% MVIC threshold for the moving and stance limbs, respectively.
Table 2 Comparison of Gluteus Maximus Muscle Activation Levels (%
Maximum Voluntary Isometric Contraction [MVIC]) Between the Moving and Stance Limbs During Hip-Joint-Strengthening Exercise Using Elastic-
Tubing Resistance, Mean ± SD
Exercise
Cross-over
Reverse cross-over
Front pull
Back pull
Moving-limb %MVIC
12.3 ± 13.2
16.4 ± 10.8
13.4 ± 14.2
39.6 ± 18.2†
Stance-limb %MVIC
9.5 ± 6
21.9 ± 21.7‡
17.3 ± 11.3‡
12.5 ± 8.2
P
.341
.285
.322
<.001*
*Gluteus maximus recruitment is greater in the moving limb than stance limb when performing the back-pull exercise.
†For the moving limb, gluteus maximus muscle recruitment is greater for the back-pull exercise than for the crossover, reverse cross-over, and front-pull exercise (P < .001).
‡For the stance limb, gluteus maximus muscle recruitment is greater in the reverse cross-over (P = .032) and front-pull (P = .004) exercises than the cross-over exercise.
Muscle Activation Levels During Hip-Joint Strengthening 7
Table 3 Comparison of Gluteus Medius Muscle Activation Levels (%
Maximum Voluntary Isometric Contraction [MVIC]) Between the Moving and Stance Limbs During Hip-Joint-Strengthening Exercise Using Elastic-
Tubing Resistance, Mean ± SD
Exercise
Cross-over
Reverse cross-over
Front pull
Moving-limb %MVIC
14.9 ± 17.7
52.9 ± 17.6†
16.7 ± 16.2
Stance-limb %MVIC
13.1 ± 12
50.0 ± 25.1¶
29.1 ± 19.9§
P
.653
.560
.025*
Back pull 30.7 ± 19.7‡ 31.4 ± 22.1§ .887
*Gluteus medius recruitment is greater in the stance limb than in the moving limb when performing the front-pull exercise.
†For the moving limb, gluteus medius muscle recruitment is greater for the reverse cross-over exercise than for the cross-over, front-pull, and back-pull exercises (P < .001).
‡For the moving limb, gluteus medius muscle recruitment is greater in the back-pull exercise than in the cross-over
(P = .001) and front-pull exercise (P = .007).
¶For the stance limb, gluteus medius muscle recruitment is greater for the reverse cross-over than for the crossover, front-pull, and back-pull exercises (P < .001).
§For the stance limb, gluteus medius muscle recruitment is greater for the back-pull and front-pull exercises than for the cross- over exercise (P < .001).
Elastic-Tubing Tension
Descriptive statistics for peak tension load (kg) produced in the elastic tubing as %BM are displayed in Figure 6. A difference in tension existed across the 4 exercise conditions (F
3,72
= 9.9; P < .001). Less tension was produced in the front pull than in the other 3 conditions. Elastic-band tension produced in the reverse cross-over, cross-over, and back-pull conditions was equivalent.
Discussion
We hypothesized that both gluteus maximus and medius muscles on the stance limb would demonstrate greater
EMG activation (%MVIC) than the moving-limb counterpart across the 4 exercise conditions used to strengthen hip muscles in standing using silver Theraband elastic tubing as resistance. Our hypothesis was not fully supported by our results because peak EMG recruitment varied between the moving and stance limbs depending on muscle and exercise condition.
Gluteus Maximus
During traditional sagittal-plane (front pull and back pull) and frontal-plane (cross-over and reverse cross-over) strengthening exercises using elastic-tubing resistance, the gluteus maximus is a primary femoral-on-pelvic hip extensor and external rotator during dynamic action of the moving limb, as well as a pelvic-on-femoral stabilizer in the sagittal, frontal, and transverse planes during weight bearing of the stance limb.
39 We originally hypothesized that stance-limb gluteus maximus would demonstrate greater EMG activation than that of the moving limb during resisted movements provided by the elastic tubing.
We were unable to support our hypothesis for the gluteus maximus. The only significant difference in gluteus maximus EMG recruitment between stance and moving limbs occurred during the back-pull exercise, where the moving-limb gluteus maximus demonstrated 27% more
EMG activity than the stance-limb gluteus maximus.
From a kinesiological viewpoint this is a reasonable expectation, because the elastic tubing is creating a sagittal-plane femoral-on-pelvic external-flexion moment that must be opposed by an internal-extension moment generated by the gluteus maximus during the back-pull exercise condition.
38
Moving-Limb Muscle Activation of Gluteus Maximus. When compared with the moving-limb back-pull exercise condition (39.6% MVIC), the moving-limb gluteus maximus was activated at lower levels in the frontal plane during both cross-over (12.3% MVIC) and reverse cross-over (16.4% MVIC) exercises, as well as in the sagittal plane during the front-pull exercise (13.4%).
During both frontal- and sagittal-plane femoral-on-pelvic movements, all participants were instructed to keep the foot in neutral alignment and avoid internal or external femoral rotation when pulling against tension created by the elastic tubing. To accomplish this action, the gluteus maximus, the hip’s most powerful external rotator, was recruited as a synergist to oppose the tendency of the lower limb to internally rotate.
39
Stance-Limb Muscle Activation of Gluteus Maximus. Gluteus maximus muscle recruitment ranged from 9.5% MVIC for the cross-over exercise to 21.9%
MVIC for the front-pull condition. We suggest that this low level of stance-limb gluteus maximus muscle activation may have provided frontal-plane (hip abduction) and transverse-plane (hip external rotation) stabilization to
8 Youdas et al
Figure 6 — The relationship between average silver Theraband elastic-tubing tension as a percentage of body mass versus exercise condition. Error bars represent the standard error for each of the exercise conditions. Abbreviations: RCO, reverse cross-over; CO, cross-over; FP, front pull; BP, back pull.
the weight-bearing hip joint. The gluteus maximus was possibly recruited to assist with stabilization of the pelvis and the lower limb during weight bearing while the limb attached to the elastic tubing was moving in either the sagittal or frontal planes.
38
We hypothesized that muscles of the stance-limb gluteus maximus would generate greater EMG activation (%MVIC) than those of the moving limb in standing using silver Theraband elastic-tubing resistance. This hypothesis was not supported. With the exception of the back-pull condition, EMG activation of the gluteus maximus on the stance side was equivalent to its counterpart on the moving side. For back pull, EMG activation of the stance-limb gluteus maximus (12.5% MVIC) was less than that of the moving limb (39.9%MVIC), and this difference was statistically significant (P < .001). On the basis of these data we cannot support our research hypothesis.
Implications for Gluteus Maximus Muscle Strengthening. In the current study, muscle activation (% MVIC) of the gluteus maximus failed to attain the 50% MVIC threshold recommended to produce a strengthening effect for any of the 4 exercise conditions.
36,37 The backpull exercise condition generated the greatest muscle recruitment of the gluteus maximus (39.6% MVIC) and this occurred on the moving limb. Average peak tension provided by the silver Theraband elastic tubing during the back pull was 8.8% ± 1.7% BM. Perhaps the low level of gluteus maximus muscle activation (% MVIC) resulted from the tubing resistance being too small a percentage of body mass. Therefore, it may be necessary to use higher levels of resistance—elastic-band elongation—when performing these exercises if a strengthening response from the gluteus maximus is desired. With the exception of the back-pull exercise, the majority of the exercises in this study generated gluteus maximus EMG signal amplitudes less than 20% MVIC. In well-trained men and women, exercises for the gluteus maximus using tension loads similar to those supplied in this study would be suited for endurance or motor control training.
45 Perhaps the signal amplitude of the gluteus maximus may have been increased during the back-pull condition on both moving and stance limbs by instructing participants to perform femoral-on-pelvic hip extension with greater forward trunk lean. This posture modification would increase the external trunk flexion moment and potentially generate greater muscle recruitment from the gluteus maximus.
46
Gluteus Medius
When performing resisted hip-joint-strengthening exercises in standing using elastic tubing the gluteus medius is a primary femoral-on-pelvic hip abductor of the moving limb during the reverse-cross over exercise, as well as a pelvic-on-femoral stabilizer in the frontal plane during
Muscle Activation Levels During Hip-Joint Strengthening 9 weight bearing of the stance limb.
38 We initially hypothesized the stance limb gluteus medius would demonstrate significantly greater EMG activation than the moving limb for all 4 exercise conditions. This condition was satisfied for the front-pull exercise only as the stance-limb gluteus medius demonstrated 12.4% more EMG activation than the moving-side gluteus medius. Peak signal amplitude of the stance-side gluteus medius (50%MVIC) occurred during the reverse cross-over condition.
Moving-Limb Muscle Acti vation of Gluteus
Medius The moving-limb gluteus medius generated its peak signal amplitude (52.9% MVIC) during the reverse cross-over exercise, which was anticipated because abduction is the primary femoral-on-pelvic action of the gluteus medius.
38 We assume the gluteus medius was activated in the frontal plane during the crossover exercise (14.9% MVIC) because it functioned as a stabilizing synergist to the primary femoral-on-pelvic adductor muscles. Similarly, during resisted sagittal plane movements the gluteus medius was seemingly activated during front-pull (16.7% MVIC) and back-pull (30.7%
MVIC) conditions to assist with frontal-plane stabilization in response to femoral-on-pelvic adduction generated by the adductor longus and adductor magnus muscles.
39
Statistically, there was no difference in muscle activation within the gluteus medius of the moving limb between front-pull and cross-over conditions presumably because the magnitude of external resistance provided by the elastic tubing was too low.
Stance-Limb Muscle Acti vation of Gluteus
Medius The stance-limb gluteus medius generated its peak activation (50%MVIC) during the reverse-cross over condition. This observation would be expected because the stance side gluteus medius would help fix the pelvis in response to tension developed by the moving limb gluteus medius. If not neutralized, tension within the moving limb gluteus medius would lower the pelvis in the frontal plane thus elongating the extremity and making it difficult for the subject to clear the foot from the support surface during femoral-on-pelvic abduction.
39
Stance limb gluteus medius muscle activation is critical for providing a stable platform for the weight-bearing pelvis and trunk in the frontal plane when the moving limb is resisted by elastic tubing.
38,39
We hypothesized the stance limb gluteus medius would demonstrate greater EMG activation (% MVIC) than the moving limb in standing using silver Theraband elastic tubing resistance. Nevertheless, with the exception of the front pull, activation levels of the gluteus medius from stance and moving limbs were nearly equivalent for the cross-over, reverse cross-over, and back-pull conditions. This information does not support our original hypothesis. Nevertheless, during the front-pull exercise, the stance-limb gluteus medius developed 74% more
EMG activity (%MVIC) than its counterpart on the moving limb and this difference was statistically significant (P = .025). From a pelvic-on-femoral viewpoint the gluteus medius on the stance limb can provide a useful function during resisted hip flexion of the moving limb.
Pelvic-on-femoral internal rotation about the stance hip is displayed by anterior rotation of the iliac crest on the moving limb. The gluteus medius on the stance limb can generate pelvic forward rotation to the contralateral moving limb during resisted hip flexion.
39
Implications for Gluteus Medius Muscle Strengthening In the current study muscle activation (% MVIC) of the gluteus medius reached the 50% MVIC threshold recommended for a strengthening effect in both moving
(52.9% MVIC) and stance limbs (50% MVIC) during the reverse cross-over exercise condition.
36,37 Average peak tension provided by silver Theraband elastic tubing during the reverse cross-over was 8.6% ± 1.4% BM.
Therefore, performance of the reverse cross-over using resistance supplied by elastic tubing appears to be an efficient method for generating a strengthening effect in contralateral hip abductors.
Unique Features of This Study
To our knowledge this is the only report to date that examined simultaneous activation of the gluteus maximus and gluteus medius from both moving and stance limbs during conventional strengthening exercises in standing using elastic-tubing resistance. Results from this study revealed that the gluteus maximus and medius muscles of both stance and moving limbs were recruited during resisted hip-joint-strengthening exercises in both sagittal and frontal planes when using elastic-tubing resistance.
However, we were unable to support our original hypothesis and declare that the gluteus maximus and gluteus medius on the stance limb demonstrated greater EMG activation (%MVIC) than that of the moving limb using silver Theraband elastic-tubing resistance. Hence, if weight-bearing tolerance is not a clinical concern, there is no therapeutic benefit to selectively activate the gluteus maximus and gluteus medius muscles on the stance limb by resisting sagittal- and frontal-plane hip movements on the moving limb using resistance supplied by elastic tubing.
We recognize several limitations in our study, including the use of healthy subjects, not recording subjects’ hip-joint osteokinematics during resisted sagittal- and frontal-plane movements, and the absence of elastic-band tension feedback in real time during execution of the resisted hip movements. Our participants were young, healthy, and active, limiting the generalization of our findings to individuals with reduced hip-muscle performance.
Additional research should examine greater levels of elastic-tubing resistance in populations with hip or knee pathologies, sedentary individuals, or older or younger individuals to increase the clinical applicability of our findings. Before data collection, subjects were trained to perform the 4 hip-joint exercises by the same investigator.
However, we did not record hip-joint osteokinematics of the moving lower limb during the resisted movements so we cannot claim that joint range of motion was uniform across subjects. Subsequent investigations could expand on the current findings by using digital videography to
10 Youdas et al record and measure hip-kinematic movement patterns.
Finally, we were unable to provide subjects with visual tension feedback generated by the elastic tubing [%BM] in real time for each repetition of an exercise condition.
The ability to control tension feedback [%BM] in a more precise fashion would minimize differences in muscle activity due to external loading.
Conclusions
Muscle activation levels (50% MVIC) obtained from the gluteus medius of both stance and moving limbs during the reverse cross-over revealed that strengthening could occur in young healthy subjects during elastictubing-resisted exercise in the frontal plane. Peak signal amplitude of the gluteus maximus (39.6% MVIC) was generated on the moving limb during the back-pull exercise, but this muscle recruitment failed to reach the
50% MVIC threshold recommended for strengthening.
From a clinical standpoint there is no therapeutic benefit to selectively activate the gluteus maximus and gluteus medius muscles on the stance limb by resisting sagittal- and frontal-plane hip movements on the moving limb using resistance supplied by elastic tubing.
References
1. Atha J. Strengthening muscle. Exerc Sport Sci Rev.
1981;9:1–73.
PubMed
2. Hughes CJ, Hurd K, Jones A, Sprigle S. Resistance properties of Thera-Band tubing during shoulder abduction exercise. J Orthop Sports Phys Ther. 1999;29:413–420.
PubMed doi:10.2519/jospt.1999.29.7.413
3. Morrissey MC, Harman EA, Johnson MJ. Resistance training modes: specificity and effectiveness. Med Sci Sports
Exerc . 1995;27:648–660.
PubMed
4. Kraemer WJ, Adams K, Cafarelli E, et al. American College of Sports Medicine position stand. Progression models in resistance training for healthy adults. Med Sci Sports
Exerc . 2002;34:364–380.
PubMed doi:10.1097/00005768-
200202000-00027
5. Kisner C, Colby LA. Therapeutic Exercise: Foundations and Techniques . 5th ed. Philadelphia, PA: FA Davis; 2007.
6. Bolgla LA, Malone TR, Umberger BR, Uhl TL. Hip strength and hip and knee kinematics during stair descent in females with and without patellofemoral pain syndrome.
J Orthop Sports Phys Ther . 2008;38:12–18.
PubMed doi:10.2519/jospt.2008.2462
7. Prins MR, van der Wurff P. Females with patellofemoral pain syndrome have weak hip muscles: a systematic review. Aust J Physiother. 2009;55:9–15.
PubMed doi:10.1016/S0004-9514(09)70055-8
8. Souza RB, Powers CM. Differences in hip kinematics, muscle strength, and muscle activation between subjects with and without patellofemoral pain. J Orthop
Sports Phys Ther . 2009;39:12–19.
PubMed doi:10.2519/ jospt.2009.2885
9. Khayambashi K, Mohammadkhani Z, Ghaznavi K, Lyle
MA, Powers CA. The effects of isolated hip abductor and external rotator muscle strengthening on pain, health status, and hip strength in females with patellofemoral pain: a randomized controlled trial. J Orthop
Sports Phys Ther . 2012;42:22–29.
PubMed doi:10.2519/ jospt.2012.3704
10. Fredericson M, Cookingham CL, Chaudhari AM,
Dowdell BC, Oestreicher N, Sahrmann SA. Hip abductor weakness in distance runners with iliotibial band syndrome. Clin J Sport Med. 2000;10:169–175.
PubMed doi:10.1097/00042752-200007000-00004
11. Fairclough J, Hayashi K, Toumi H, et al. The functional anatomy of the iliotibial band during flexion and extension of the knee: implications for understanding the iliotibial band syndrome. J Anat. 2006;208:316–319.
PubMed doi:10.1111/j.1469-7580.2006.00531.x
12. Fairclough J, Hayashi K, Toumi H, et al. Is iliotibial band syndrome really a friction syndrome? J Sci Med Sport.
2007;10:74–76.
PubMed doi:10.1016/j.jsams.2006.05.017
13. Noehren B, Davis I, Hamill J. Prospective study of the biomechanical factors associated with iliotibial band syndrome. Clin Biomech (Bristol, Avon). 2007;22:951–956.
PubMed doi:10.1016/j.clinbiomech.2007.07.001
14. Nilsdotter AK, Isaksson F. 2010 Patient relevant outcome
7 years after total hip replacement for OA—a prospective study. BMC Musculoskelet Disord. 2010;11:47–53.
PubMed doi:10.1186/1471-2474-11-47
15. Rasch A, Dalen N, Berg H. Muscle strength, gait, and balance in 20 patients with hip osteoarthritis followed for 2 years after THA. Acta Orthop. 2010;81:183–188.
PubMed doi:10.3109/17453671003793204
16. Jensen C, Aagaard P, Overgaard S. Recovery in mechanical muscle strength following resurfacing vs standard total hip arthroplasty—a randomized clinical trial. Osteoarthritis
Cartilage . 2011;19:1108–1116.
PubMed doi:10.1016/j.
joca.2011.06.011
17. Piva SR, Teixeira PEP, Almeida GJM, et al. Contributor of hip abductor strength to physical function in patients with total knee arthroplasty. Phys Ther. 2011;91:225–233.
PubMed doi:10.2522/ptj.20100122
18. Hewett TE, Myer GD, Ford KR, et al. Biomechanical measures of neuromuscular control and valgus loading of the knee predict anterior cruciate ligament risk in female athletes: a prospective study. Am J Sports Med. 2005;33:492–
501.
PubMed doi:10.1177/0363546504269591
19. Hollman JH, Ginos BE, Kozuchowski J, Vaughn AS,
Krause DL, Youdas JW. Relationships between knee valgus, hip-muscle strength, and hip-muscle recruitment during a single-limb step-down. J Sport Rehabil.
2009;18:104–117.
PubMed
20. Nicholas JA, Strizak AM, Veras G. A study of thigh muscle weakness in different pathological states of the lower extremity. Am J Sports Med. 1976;4:241–248.
PubMed doi:10.1177/036354657600400602
21. Nadler SF, Malanga GA, DePrince M, Stitik TP, Feinberg
JH. The relationship between lower extremity injury, low back pain, and hip muscle strength in male and female
Muscle Activation Levels During Hip-Joint Strengthening 11 collegiate athletes. Clin J Sport Med. 2000;10:89–97.
PubMed doi:10.1097/00042752-200004000-00002
22. Friel K, McLean N, Myers C, Caceres M. Ipsilateral hip abductor weakness after inversion ankle sprain. J Athl
Train . 2006;41:74–78.
PubMed
23. Andersen LL, Andersen CH, Mortensen OS, Poulsen
OM, Bjornlund IB, Zebis MK. Muscle activation and perceived loading during rehabilitation exercises: comparison of dumbbells and elastic resistance. Phys Ther.
2010;90:538–549.
PubMed doi:10.2522/ptj.20090167
24. Mikesky AE, Topp R, Wigglesworth JK, Harsha DM,
Edwards JE. Efficacy of a home-based training program for older adults using elastic tubing. Eur J Appl Physiol
Occup Physiol . 1994;69:316–320.
PubMed doi:10.1007/
BF00392037
25. Colado JC, Triplett NT. Effects of a short-term resistance program using elastic bands versus weight machines for sedentary middle-aged women. J Strength
Cond Res . 2008;22:1441–1448.
PubMed doi:10.1519/
JSC.0b013e31817ae67a
26. Lephart SM, Smoliga JM, Myers JB, Sell TC, Tsai YS.
An eight-week golf-specific exercise program improves physical characteristics, swing mechanics, and golf performance in recreational golfers. J Strength Cond Res.
2007;21:860–869.
PubMed
27. Topp R, Woolley S, Hornyak J, 3rd, Khuder S, Kahaleh B.
The effect of dynamic versus isometric resistance training on pain and functioning among adults with osteoarthritis of the knee. Arch Phys Med Rehabil. 2002;83:1187–1195.
PubMed doi:10.1053/apmr.2002.33988
28. Zion AS, De Meersman R, Diamond BE, Bloomfield DM.
A home-based resistance-training program using elastic bands for elderly patients with orthostatic hypotension.
Clin Auton Res . 2003;13:286–292.
PubMed doi:10.1007/ s10286-003-0117-3
29. Fukuda TY, Rossetto FM, Magalhaes E, Bryk FF, Lucareli
PR, de Almeida Aparecida Carvalho N. Short-term effects of hip abductors and lateral rotators strengthening in females with patellofemoral pain syndrome: a randomized controlled clinical trial. J Orthop Sports Phys Ther.
2010;40:736–742.
PubMed doi:10.2519/jospt.2010.3246
30. Han K, Ricard MD, Fellingham GW. Effects of a 4-week exercise program on balance using elastic tubing as a perturbation force for individuals with a history of ankle sprains. J Orthop Sports Phys Ther. 2009;39:246–255.
PubMed doi:10.2519/jospt.2009.2958
31. Schulthies SS, Ricard MD, Alexander KJ, Myrer JW. An electromyographic investigation of 4 elastic-tubing closed kinetic chain exercises after anterior cruciate ligament reconstruction. J Athl Train. 1998;33:328–335.
PubMed
32. Hopkins JT, Ingersoll CD, Sandrey MA, Bleggi SD. An electromyographic comparison of 4 closed chain exercises.
J Athl Train . 1999;34:353–357.
PubMed
33. Thein-Nissenbaum J, Orzehoskie J. Lower Extremity Exer- cises With Elastic Resistance. The Scientific and Clinical
Application of Elastic Resistance . Champaign, IL: Human
Kinetics; 2003:69–98.
34. Bolgla LA, Uhl TL. Electromyographic analysis of hip rehabilitation exercises in a group of healthy subjects.
J Orthop Sports Phys Ther . 2005;35:487–494.
PubMed doi:10.2519/jospt.2005.35.8.487
35. Distefano LJ, Blackburn JT, Marshall SW, Padua DA.
Gluteal muscle activation during common therapeutic exercises. J Orthop Sports Phys Ther. 2009;39:532–540.
PubMed doi:10.2519/jospt.2009.2796
36. Andersen LL, Magnusson SP, Nielsen M, Haleem J,
Poulsen K, Aagaard P. Neuromuscular activation in conventional therapeutic exercises and heavy resistance exercises: implications for rehabilitation. Phys Ther.
2006;86:683–697.
PubMed
37. Ayotte NW, Stetts DM, Keenan G, Greenway EH. Electromyographical analysis of selected lower extremity muscles during 5 unilateral weight-bearing exercises. J Orthop
Sports Phys Ther . 2007;37:48–55.
PubMed doi:10.2519/ jospt.2007.2354
38. Powers CM. The influence of abnormal hip mechanics on knee injury; a biomechanical perspective. J Orthop
Sports Phys Ther . 2010;40:42–51.
PubMed doi:10.2519/ jospt.2010.3337
39. Neumann DA. Kinesiology of the Musculoskeletal System:
Foundations for Rehabilitation . 2nd ed. St Louis, MO:
Mosby/Elsevier; 2010.
40. Youdas JW, Foley BM, Kruger BL, et al. Electromyographic analysis of trunk and hip muscles during resisted lateral band walking. Physiother Theory Pract.
2013;29:113–123.
PubMed doi:10.3109/09593985.2012
.704492
41. Hughes CJ, Page P. Scientific basis of elastic resistance.
In: Page P, Ellenbecker TS, eds. The Scientific and Clinical
Application of Elastic Resistance . Champaign, IL: Human
Kinetics; 2003:3–14.
42. Patterson RM, Jansen CWS, Hogan HA, Nassif MD.
Material properties of Thera-Band tubing. Phys Ther.
2001;81:1437–1445.
PubMed
43. Criswell E, Cram JR. Cram’s Introduction to Surface
Electromyography . 2nd ed. Sudbury, MA: Jones & Bartlett;
2011.
44. Hislop H, Montgomery J. Muscle Testing: Techniques of
Manual Examination . St Louis, MO: Saunders; 2007.
45. Ekstrom RA, Donatelli RA, Carp KC. Electromyographic analysis of core trunk, hip, and thigh muscles during
9 rehabilitation exercises. J Orthop Sports Phys Ther.
2007;37:754–762.
PubMed doi:10.2519/jospt.2007.2471
46. Pohtilla JF. Kinesiology of hip extension at selected angles of pelvi-femoral extension. Arch Phys Med Rehabil.
1969;50:241–250.
PubMed