GAP flap
advertisement

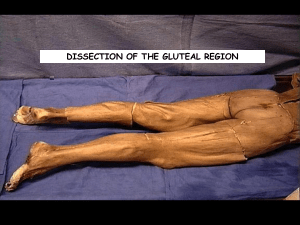
Gluteus Maximus Origin o Behind posterior gluteal line of ilium and sacrum, lumbar fascia, sacrotuberous ligament Insertion o Deep ¼ inserts into gluteal tuberosity o Superficial ¾ inserts into iliotibial tract (inserts into lateral condyle of tibia) Nerve supply from inferior gluteal nerve Skin island (SGAP breast reduction) o place the flap design much higher on the buttock than is traditionally described to allow for the ultimate scar line to rest at the junction of the aesthetic units of the lower back and upper buttock. o possible to raise skin flaps of up to 30 cm by 13 cm with a pedicle length of 6 cm to 10.5 cm, and leave behind an anatomically and functionally intact muscle Blood supply o Type III o Superior (posterior div) and inferior gluteal (ant division) o Superior Gluteal Artery As the superior gluteal artery passes the greater sciatic foramen, it divides into a superficial and a deep branch. deep branch travels in between the gluteus medius muscle and the iliac bone. superficial branch goes on to supply the gluteus muscle and the overlying skin territory. It is this superficial branch of the gluteal artery that nourishes the fat and skin in musculocutaneous flaps in this region. superficial branches further subdivide in the plane between the gluteus maximus and gluteus medius into three ramifying branches, which may be called posterior, intermediate, and anterior The posterior branch is closely attached to the undersurface of the gluteus maximus, gives off numerous branches, and pierces the muscle and reaches the overlying skin. The gluteus maximus muscle flap for breast reconstruction is harvested using these skin and muscle perforators The anterior branch runs between the gluteus maximus and gluteus medius, supplying them both. Terminal branches may emerge at the superolateral edge of the gluteus maximus to pierce the deep fascia and supply skin. These skin perforators are used in the superior gluteal perforator free flap. Once the perforating vessels are followed down through the deep layer of the muscular fascia, the caliber of the vessels, especially the vein, increases rapidly. It is not uncommon to encounter a venous confluents with a diameter of 8 to 10 mm and five or six joining vessels. The number of branches of both the vein and artery also increases once the deep fascia is opened. o Inferior Gluteal Artery Terminal branch of anterior division of internal iliac May arise as common trunk with SGA Arises below piriformis with internal pudendal vessels medially and sciatic nerve laterally lies adjacent to the posterior femoral cutaneous nerve. Major blood supply to lower 2/3rd of gluteus maximus 2 branches – medial and lateral Disadvantages 1. exposure of sciatic nerve – more prone to chronic pain syndrome 2. skin flap is over weight bearing aspect of buttock Landmarks: o location where the superior gluteal artery exits the suprapiriform foramen is marked on the skin at the proximal one third of a line that connects the posterior superior iliac spine and the lateral apex of the greater trochanter. o position of the piriform muscle is located by connecting the middle of a line between the posterior superior iliac spine and the coccyx with the superior edge of the greater trochanter of the femur o main perforators are localized by unidirectional Doppler flowmetry in an area above the piriform muscle, laterodistally to the exit point of the superior gluteal artery and parallel to the first line. o Inferior gluteal found halfway between a line drawn from the PSIS to the ischial tuberosity (A) Markings of the anatomical landmarks and localization of the perforators. The dotted lines delineate the area where main perforators of the superior gluteal artery (SGA) can be expected. PIS, posterior iliac spine; TROCH, trochanter; X, location of a major perforator. (B) Positioning of the skin paddle in case of a free SGAP breast reconstruction.