Case Study
Accidental Diagnosis of Multiple Myeloma
in a 44-Year-Old White Woman due to
Erroneous Results via Chemical Analyzers
Ola Bashiti, MLS(ASCP)CM
Laboratory Medicine 47:1:5-11
DOI: 10.1093/labmed/lmv011
Principle Laboratory Findings: Tables 1–7, Figures 1–4.
Patient: 44-year-old white woman.
Keywords: pseudohyponatremia, ion-selective electrode, electrolyte exclusion effect, direct potentiometry, indirect potentiometry, monoclonal
gammopathy, multiple myeloma
Chief Complaints: Cramping, nausea, shortness of breath, visual
disturbances (“seeing yellow dots”).
Medical History: Status asthmticus, tobacco use, hypertension, migraines.
returned home. After the maintenance had been completed,
I ordered the same specimen to be assayed on the AU680.
Case Description
The patient, a 44-year-old white woman, arrived at the
emergency department of St. Vincent’s Medical Center with
an array of symptoms, including cramping and visual
disturbances (she reported “seeing yellow dots”). Her
medical history included hypertension and migraines.
Because maintenance was being performed on the main
analyzer in our laboratory, the AU680 (Beckman Coulter), the
chemistry laboratory assayed the serum specimen from the
patient on the Abbott i-STAT (Abbott Laboratories Inc.).
When the test results showed the analyte levels of the
patient to be within normal limits, she was released and
Due to the low sodium levels and conflicting results
recorded by the 2 analyzers, the physician called the patient
back to the emergency department. Another specimen was
ordered and tested on the AU680 and the i-STAT. The results
on the AU680 showed once again to be critically low, and
those yielded by the i-STAT were normal. The serum specimen
was retested to determined protein and albumin values.
I observed that the protein level in the specimen was high
and the albumin level was low. I questioned these results and
was advised by the clinical chemist that the patient might be
harboring a plasma cell neoplasm. A serum protein
electrophoresis was ordered for the patient, to confirm or
contradict her condition. Immunofixation electrophoresis and
immunoglobulin quantification was carried out due to the
outcome of serum protein electrophoresis.
Abbreviations
Ig, immunoglobulin; ISE, ion-selective electrode; MM, multiple myeloma;
CBC, complete blood count; RBC, red blood cell; MCV, mean corpuscular
volume; MCHC, mean corpuscular hemoglobin concentration; FLCs, free
lights chains; WBC, white blood cell; HGB, hemoglobin; HCT, hematocrit;
MCH, mean cell hemoglobin; RDW, red-blood-cell distribution width; PLT,
platelet; MPV, mean platelet volume; SP, serum protein; G.,
Immunoglobulin G; A, Immunoglobulin A; M, Immunoglobulin M.
St. Vincent’s Medical Center, University of North Florida, Jacksonville, FL
*To whom correspondence should be addressed.
olabashiti@yahoo.com
Bone marrow studies confirmed 95% cellular bone marrow
that appeared to be composed of approximately 30%
plasma cells. Follow-up hematology studies were completed
to assist with bone marrow studies.
Questions
1. Based on the data in the chemical analysis tables, what is/
are the patient’s most significant results?
C American Society for Clinical Pathology 2015. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com
V
e5
Downloaded from http://labmed.oxfordjournals.org/ by guest on January 15, 2016
CLINICAL HISTORY
Case Study
2. Given the patient’s medical history, how can her test
results be explained? What is the reason for the difference in
sodium levels using each method of analysis?
3. Why is the discrepancy between the sodium results
important?
4. What do the additional test results indicate? What
disorders are associated with the findings?
5. What is the patient’s final diagnosis?
7. Why is the patient’s case clinically significant?
Answers
1. There is a wide difference in the sodium values reported
by each instrument. The iSTAT/Gem shows a normal sodium
value, and the AU680 presents a decreased sodium value.
The potassium level is slightly low, according to both
instruments, and the anion gap and total calcium are very
low. Further tests reveal a profoundly high protein level and
low albumin level.
2. The sodium value reported using the AU680 is described
as hyponatremia, or low sodium levels in the blood. It has
been reported that hyponatremia can be observed in plasma
with extremely high protein values1; however, it is usually
classified as pseudohyponatremia. Pseudohyponatremia is
defined as spuriously low plasma sodium concentration.2
The measured sodium concentration is low, but the actual
sodium concentration in the plasma is normal. This
measurement artifact is evident in cases of extremely high
levels of lipids (hyperlipidemia) or proteins (hyperproteinemia)
in the blood. However, hyperlipidemia is a much more
common cause for pseudohyponatremia because it
represents an increase in triglyceride and cholesterol levels,
which is found in prevalent medical conditions like diabetes
mellitus, kidney disease, and hypothyroidism.
Approximately 93% of plasma is composed of water and 7%
of solids.3 Free electrolytes are part of the water portion, and
proteins and lipids make up the solid portion. In cases of
hyperproteinemia or hyperlipidemia, the solid component
takes up most of the total plasma, causing the water
e6
Lab Medicine 2016;47:1;5–11
6
DOI: 10.1093/labmed/lmv011
Analyte
Patient Result
Normal Values
Sodium
Potassium
Chloride
Bicarbonate
Anion gap
Glucose
Blood urea nitrogen
Creatinine
Ca
Albumin-corrected Ca
122 mmol/L
3.4 mmol/L
98 mmol/L
25 mmol/L
2 mmol/L
4.66 mmol/L
3.93 mmol/L
80 mmol/L
1.98 mmol/L
2.50 mmol/L
135-145 mmol/L
3.50-5.40 mmol/L
98-110 mmol/L
22-32 mmol/L
9-22 mmol/L
3.60-5.50 mmol/L
2.50-8.20 mmol/L
53-106 mmol/L
2.10-2.60 mmol/L
2.10-2.60 mmol/L
Table 2. Chemical Analysis Using Indirect
Potentiometry
Procedure
Patient Result, mmol/L Normal Values, mmol/L
Sodium
Potassium
Chloride
Bicarbonate
Anion gap
Glucose
Blood urea nitrogen
Creatinine
Ca
Albumin-corrected Ca
122
3.40
98
25
2
4.66
3.93
80
1.98
2.50
135-145
3.50-5.40
98-110
22-32
9-22
3.60-5.50
2.50-8.20
53-106
2.10-2.60
2.10-2.60
Table 3. Protein and Albumin Results.
Procedure
Patient Result, g/dL
Normal Values, g/dl
Protein
Albumin
15.8
<1.5
6.0-8.5
3.4-5.1
Table 4. Protein Quantification for Patient Serum
Electrophoresis
Fraction
Patient Result, %
Normal Values, %
Albumin
Alpha 1
Alpha 2
Beta
Gamma
22.0
2.5
7.0
5.6
62.9
45.0-70.0
1.0-4.0
5.0-10.0
9.0-13.0
6.0-20.0
component to be greatly reduced. Pseudohyponatremia is
caused by the electrolyte exclusion effect that is found using
indirect methodology because the sodium electrolytes
become limited to a smaller volume of water.4
www.labmedicine.com
Downloaded from http://labmed.oxfordjournals.org/ by guest on January 15, 2016
6. What is the clinical significance of the suppressed
immunoglobulin (Ig)M and IgA in this patient?
Table 1. Chemical Analysis Using Direct
Potentiometry
Case Study
Table 5. Complete Blood Count for Patient’s
Blood
Cell
WBC
RBC
HGB
HCT
MCV
MCH
MCHC
RDW
PLT
MPV
Patient Result
9
5.6 10 /L
2.89 1012/L
7.9 g/dL
24.4%
84.4 fL
27.2 pg
32.2 g/dL
24.1%
39 109/L
8.7 fL
Normal Values
4.5-11 109/L
3.5-5.5 1012/L
12.0-16.0 g/dL
36.0%-46.0%
80.0-100.0 fL
25.0-35.0 pg
30.0-37.0 g/dL
11.5%-14.5%
150-450 109/L
8.0-12.0 fL
Table 6. Immunoglobulin Quantification
Results
Immunoglobulin Type
Patient Result,
mg/dL
Normal Values,
mg/dL
M
A
G
<20
<10
10,478
40-250
70-375
550-1560
My patient presents with a very high level of protein that was
nonexistent in her medical history, which implicates
pseudohyponatremia. Potassium and chloride are influenced
by the electrolyte exclusion effect in the same manner as
sodium because they are electrolytes contained in the water
portion of plasma and are measured using the same
methodology. The patient’s potassium and chloride levels
were borderline low, which was most likely caused by the
hyperproteinemia.
The anion gap evaluates the difference between measured
and unmeasured anions in the plasma and is usually used to
assess acid-base disorders or to provide quality control for
measuring all electrolytes. The calculation for anion gap is
Na - [Cl þ Bicarbonate].
The patient’s anion gap is significantly decreased. Low
values are an infrequent finding and most commonly indicate
laboratory error or hypoalbuminemia (low albumin in the
blood). Laboratory errors occur when there is an
underestimated sodium concentration due to elevated
proteins in the plasma. Hypoalbuminemia is the second most
common cause of a low anion gap. The negative charges of
www.labmedicine.com
Albumin has a direct effect on calcium. Half of the calcium in
the blood is free and metabolically active. The remaining half
is bound to albumin, with a smaller amount complexed to
anions, and is metabolically inactive. The total calcium
measurement represents the free and bound forms, whereas
the ionized calcium measurement represents the
metabolically active form. Because half the calcium in the
blood is bound to albumin, total calcium test results are
influenced by any fluctuation in albumin levels. In fact, each
1 g/dL decrease in plasma albumin level will lower the total
calcium level by approximately 0.25 mmol/L. Ionized calcium
will not be affected, making it a more ideal test for measuring
calcium levels.5 The hypoalbuminemia experienced by the
patient explains the low calcium (hypocalcemia) result
obtained using the AU680. The i-STAT provided a normal
ionized calcium level, indicating that the patient does not
have any calcium disorder and is showing
pseudohypocalcemia.
The disparity in sodium values between the 2 analyzers is
due to a difference in the methodology of potentiometry.
Potentiometry is the measurement of potential difference
between 2 electrodes. The ion-selective electrode (ISE) is a
potentiometric electrode that is most commonly used in
laboratories to estimate the concentration of specific
electrolytes in blood specimens. ISEs use high-impedance
voltmeters to measure the electrical potential generated
between a measuring electrode and a reference electrode
when the activity of a specific ion is dissolved in a solution.4
There are 2 types of ISEs: direct and indirect. The direct
method analyzes whole blood and does not involve a
predilution, and the indirect method involves automatic
dilution of the plasma specimen.1 The iSTAT uses the direct
method and the AU680 uses the indirect method.
Essentially, electrolyte concentrations are represented by the
total plasma level, which includes dissolved solids and
water. However, the clinically significant sodium value is the
plasma water concentration.6 The values in total plasma
usually correlate with that in plasma water, except in cases
of high levels of proteins or lipids in the plasma specimen
Lab Medicine 2016;47:1;5–11
DOI: 10.1093/labmed/lmv011
e7
Downloaded from http://labmed.oxfordjournals.org/ by guest on January 15, 2016
WBC, white blood cell; RBC, red blood cell; HGB, hemoglobin; HCT, hematocrit; MCV,
mean corpuscular volume; MCH, mean cell hemoglobin; MCHC, mean cell hemoglobin concentration; RDW, red blood cell distribution width; PLT, platelet; MPV, mean
platelet volume.
albumin make up most of the unmeasured anions, so
changes in the plasma albumin would be expected to alter
the plasma anion gap. Studies have found that for every
1 g/dL decrease in albumin, there is a 2.3- to 2.5-mmol/L
decrease in the anion gap.4 In this case, both causes can be
applicable to the patient’s status because the patient
demonstrated pseudohyponatremia and hypoalbuminemia.
Case Study
water per unit volume and fewer electrolytes per unit volume.
Excess dilution occurs because the same amount of diluent
is added but to a lower water component. Therefore, less
sodium is drawn from the plasma, resulting in an
underestimated electrolyte concentration. 7,8 The decrease in
the amount of water per volume of plasma due to
hyperproteinemia can be explained using the following
equation:
Serum Water ð%Þ
¼ 99:1 ð0:73 protein concentration in g=dLÞ
¼ 99:1 11:53
¼ 87:6 ðor e88%Þ
The decrease in plasma water content is 100% - 87.6% ¼
12.4%. Therefore, a 12.4% volume displacement affects the
actual sodium concentration.2
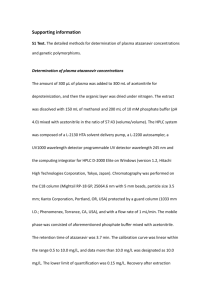
Figure 1
Serum protein electrophoresis pattern for normal control, abnormal
control, and specimen from the patient, a 44-year-old white woman.
Albumin
Alpha 2
Alpha 1
Beta
Gamma
Figure 2
Normal densitometric tracing.
when using indirect methods; the values will be falsely
decreased. The indirect method of ion-selective electrode
potentiometry is affected by the electrolyte exclusion effect
because it assumes that all plasma specimens contain 93%
water and that the volume of specimen material added to the
diluent is corrected for dilution based on this volume. The
measured concentration is modified by a factor of 0.93 to
achieve the true sodium ion concentration in plasma. In a
specimen with hyperproteinemia, the extra proteins take up
volume and displace water so that plasma contains less
e8
Lab Medicine 2016;47:1;5–11
8
DOI: 10.1093/labmed/lmv011
The direct ion-selective electrode compensates for false
hyponatremias that are encountered in the indirect method
because it is not susceptible to the electrolyte exclusion
effect. Direct potentiometry does not involve a dilution step
so it measures the activity of sodium in the water phase
rather than the total sodium concentration. The final
electrolyte value is independent of the protein (solid) content
in the plasma.8
3. Hyponatremia is the most common disturbance in blood
chemistry. Usually, it is mild, self-limiting, and not associated
with symptoms. However, severe hyponatremia can occur in
serious conditions associated with neurological symptoms.9
The symptoms reported by the patient were possible
indications for true hyponatremia. The decreased sodium
value produced by the reference analyzer could have led to
misdiagnosis and, consequently, improper treatment. The
patient was initially called back to the emergency department
to be treated for hyponatremia, which was, in fact,
pseudohyponatremia, which should not be treated.
Managing false hyponatremia can lead to clinical errors, with
potentially serious consequences, including death.
4. The serum protein electrophoresis pattern demonstrates a
defined gamma band for the patient’s serum that resembles
the abnormal control, which is known as a monoclonal
protein spike. Protein quantification shows a decreased
albumin fraction, hypoalbuminemia, and an increased
gamma fraction (hypergammaglobulinemia). These results
are also illustrated in the densometric tracings. The most
www.labmedicine.com
Downloaded from http://labmed.oxfordjournals.org/ by guest on January 15, 2016
¼ 99:1 ð0:73 15:8Þ
Case Study
Gamma
Albumin
Alpha 2 Beta
Alpha 1
Densitometric tracing in the patient, a 44-year-old white woman.
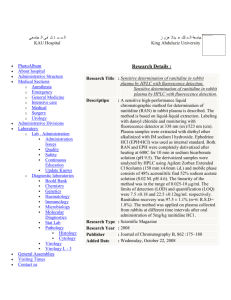
Figure 4
Immunofixation electrophoresis results in the patient, a 44-year-old
white woman. SP indicates serum protein; G, Immunoglobulin G; A,
Immunoglobulin A; M, Immunogobulin M.
prominent finding is the homogenous spike-like peak in the
gammaglobulin zone, which is expressed in manifestations
of monoclonal gammopathies.
Monoclonal gammopathies are part of a group of plasma cell
disorders in which an immunoglobulin from a single plasma
cell clone is produced in excess, generating a homogenous
M protein spike. An M spike is characterized by the presence
of a well-defined band with a single heavy chain and a band
with a light chain. Monoclonal gammopathic diseases can
range from a relatively benign condition to malignant
conditions such as multiple myeloma (MM). Therefore, MM
must be differentiated from other monoclonal gammopathic
conditions, such as lymphoplasmacytic lymphoma, plasmacell leukemia, and monoclonal gammopathy of undetermined
significance, to evaluate the severity of disease.10
www.labmedicine.com
5. The final diagnosis for the patient is multiple myeloma
(MM). Distinct features required for the diagnosis of MM
include an M-protein spike with a level greater than 3 g/dL,
greater than 10% to 15% plasma-cell involvement in the
bone marrow, and anemia with pancytopenia.10
Immunofixation was used to identify the specific type of
malignant heavy chain and light chain present (M protein),
namely, an immunoglobulin (Ig)G heavy chain and lambda
light chain. Immunoglobulin quantification provides a
preliminary diagnosis for multiple myeloma (MM) because
IgG values were greater than 3 g/dL. The results of bonemarrow studies exhibit 30% plasma-cell involvement, which
is a definite diagnosis for MM. The complete blood count
(CBC) points out a low red blood cell (RBC) count and a
normal mean corpuscular volume (MCV) and mean
corpuscular hemoglobin concentration (MCHC), which is
considered a normocytic, normochromic type of anemia in
which the platelets are decreased, indicating
thrombocytopenia.
Urine protein studies could have further aided in the
diagnosis of MM, but they were not performed. The
expected findings would be proteinuria (>1 g of protein) and
the presence of Bence-Jones proteins (lambda light chains)
in a 24-hour urine collection.13 Bence-Jones proteinuria is
confirmed by urine immunofixation electrophoresis. BenceJones proteins are monoclonal kappa or lambda
Lab Medicine 2016;47:1;5–11
DOI: 10.1093/labmed/lmv011
e9
Downloaded from http://labmed.oxfordjournals.org/ by guest on January 15, 2016
Figure 3
MM occurs when malignant plasma cells form in the bone
marrow, producing an abnormal amount of dysfunctional
immunoglobulin.11 Normal plasma cells help the immune
system by producing immunoglobulins that are composed of
proteins. Antibodies consist of 2 heavy chains and 2 light
chains. There are 5 types of heavy chains, known as
immunoglobulin (Ig)G, IgA, IgM, IgD, and IgE, as well as 2
types of light chains, termed kappa and lambda. All the
abnormal cells in MM are made up of the same antibody. So,
MM can be categorized by the type of light and heavy chains
produced. The most common type of heavy chain produced
in MM is IgG, followed by IgA and IgD. IgM myelomas are
rare, but when IgM is increased in the blood, it is usually
associated with Waldenström macroglobulinemia. MM can
be differentiated from other monoclonal gammopathies
based on features distinctive to each disease, as can be
seen in Table 7.10 Normocytic, normochromic anemia and
pancytopenia are common findings in patients with MM
because the plasma cells in the bone marrow proliferate
extensively and produce tumors that interfere with
hematopoiesis.12
Case Study
Table 7. Types of Monocolonal Gammopathy, Including Multiple Myeloma
Disease
Distinctive Features
Monoclonal gammopathy of undermined significance
<10% plasma cell involvement on bone-marrow biopsy
No anemia
Lymphoplasmacytic lymphoma
Hyperviscosity and hypercellular bone marrow
Plasma cell leukemia
M protein levels are low
Multiple myeloma
M protein level >3000 mg/dL
10%-15% plasma cell involvement on bone-marrow biopsy
Anemia, pancytopenia
M protein level <3000 mg/dL
6. The suppression of immunoglobulin (Ig)M and IgA is
clinically significant because the patient is more prone to
acquiring infections. IgM, which encompasses approximately
10% of the Ig pool, is the first antibody produced in an
immune response and is responsible for agglutination and
cytolytic reactions. IgA accounts for 15% to 20% of the Ig
pool and is the primarily found in secretions such as tears,
saliva, milk, and intestinal fluids. IgA also plays a primary role
in defense against foreign substances. For an infectious
disease to develop in the host, the organism must bypass,
overcome, or inhibit normal bodily defense mechanisms. A
decrease in IgM and IgA puts the patient at a higher risk of
recurrent infections because the immune response has a
shortcoming in its first lines of defense that recognize and
fight off infectious agents. Increased susceptibility in patients
with multiple myeloma (MM) mainly results from defective
antibody synthesis (M protein) in the bone marrow that
crowds out normal plasma cell precursors. In such patients,
there is an excess of one particular immunoglobulin that
does not fight off infection and a decrease in the normally
functional white blood cells; infections are dominantly
derived from pneumococci or gram negative bacteria.
Pneumonia, pyelonephritis, meningitis, and arthritis are the
leading causes for sepsis, which can ultimately lead to death
if bacteremia ensues.14
7. The patient entered the hospital with no relevant history of
a serious medical condition. The findings of routine
e10
Lab Medicine 2016;47:1;5–11
10
DOI: 10.1093/labmed/lmv011
Peripheral blood contains >20% plasma cells
M protein appears as a narrow spike in gamma, beta, or alpha 2 regions
chemistry tests using 2 different methods showed a
discrepancy between sodium values, with the result from
one assay instrument indicating pseudohyponatremia. The
patient should not be treated for false hyponatremia because
mistreatment could lead to potentially dangerous
consequences. Hence, direct potentiometry should be used
to test plasma that has an elevated protein. The laboratory’s
actions to solve the discrepancy in sodium values ultimately
led to the discovery of the patient’s underlying multiple
myeloma (MM).
MM represents 10% of all hematological malignant
neoplasms. The patient’s demographics (she is a 44-year-old
white woman) are unconventional for the diagnosis of MM.
The typical age at diagnosis is 66 years, with a higher
incidence in African Americans and males. It is difficult to
diagnose MM at a time when disease progression can
still be controlled because MM usually causes no symptoms
until it reaches an advanced stage. Advancing
manifestations of the disease induce numerous
complications in the body, including anemia, pancytopenia,
bone destruction, hypercalcemia, renal failure, and
neuropathic occurrences.12 The patient had already begun
displaying signs of early disease advancement with anemia
and thrombocytopenia. Therefore, diagnosing MM at the
present stage will help stop her disease progression and aid
her prognosis.
References
1. Levy GB. Determination of sodium with ion-selective electrodes. Clin
Chem. 1981;27(8):1435–1438.
2. Higgins C. Pseudohyponatremia. Acutecare testing Web site. http://acutecar
etesting.org/en/articles/pseudohyponatremia. Accessed October 16, 2015.
www.labmedicine.com
Downloaded from http://labmed.oxfordjournals.org/ by guest on January 15, 2016
immunoglobulin free lights chains (FLCs) that are not
attached to the heavy-chain portion of the immunoglobulin
molecule. Approximately 46% of cases of MM in which the
patient produces intact immunoglobulin monoclonal proteins
have excess monoclonal FLCs in the urine by
immunofixation.14
Immunogloblin M protein is present
Case Study
3. Dhatt G, Talor Z, Kazory A. Letters to the editor: direct ion-selective electrode method is useful in diagnosis of pseudohyponatremia. J Emerg
Med. 2012;43(2):348–349.
4. Kraut JA, Madias NE. Serum anion gap: its uses and limitations in clinical
medicine. Clin J Am Soc Nephrol. 2007;2:162–174.
5. Calcium. American Association for Clinical Chemistry Web site. http://lab
testsonline.org/understanding/analytes/calcium/tab/glance/. Accessed
October 16, 2015.
6. Spitalnik SL, Arinsburg SA, Jhang JS. Clinical Pathology Board Review.
Philadelphia, PA: Elsevier Saunders; 2014. p. 223.
7. Garibaldi BT, Cameron SJ, Choi M. Pseudohyponatremia in a patient with
HIV and hepatitis C coinfection. J Gen Intern Med. 2008;23(2):202–205.
8. Ladenson JH, Apple FS, Aguanno JJ, Koch DD. Sodium measurements
in multiple myeloma: two techniques compared. Clin Chem.
1982;28(12):2383–2386.
9. Fortgens P, Pillay TS. Pseudohyponatremia revisted: a modern-day pitfall.
Arch Pathol Lab Med. 2011;135:516–519.
10. O’Connell TX, Horita TJ, Kasravi B. Understanding and interpreting serum
protein electrophoresis. Am Fam Physician. 2005;71(1): 105–112.
11. Barrick MC, Mitchell SA. Multiple myeloma: recent advances for this common plasma cell disorder. Am J Nurs. 2001;101(4):6–12.
12. About Multiple Myeloma. University of California San Francisco Web site.
http://cancer.ucsf.edu/research/multiple-myeloma/. Accessed October
16, 2015.
13. Shah D, Multiple Myeloma Workup. Medscape Web site. http://emedi
cine.medscape.com/article/204369-workup. Accessed October 16,
2015.
14. Turgeon ML. Immunology & Serology in Laboratory Medicine. 5th ed.
St.Louis, MI: Elsevier Inc; 2014. p. 371–373.
Downloaded from http://labmed.oxfordjournals.org/ by guest on January 15, 2016
www.labmedicine.com
Lab Medicine 2016;47:1;5–11
DOI: 10.1093/labmed/lmv011
e11