Intact mirror-tracing and - Faculty Virginia
advertisement

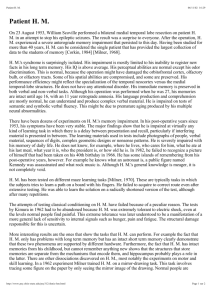
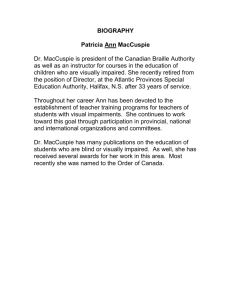
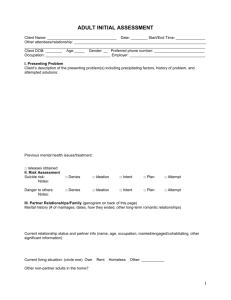
Copyright 1997 by the American Psychological Association, Inc. 0894-4105/97/$3.00 Neuropsychology 1997, Vol. II, No.2, 272-281 Intact Mirror-Tracing and Impaired Rotary-Pursuit Skill Learning in PatientsWith Huntington's Disease:Evidence for Dissociable Memory Systemsin Skill Learning John D. E. Gabrieli Glenn T. Stebbins, laswinder Singh Rush-Presbyterian-St.Luke's Medical Center Rush-Presbyterian-St.Luke's Medical Center, and StanfordUniversity Daniel B. Willingham Universityof VIrginia Christopher G. Goetz Rush-Presbyterian-St. Luke's Medical Center Skill learning in early-stageHuntington'sdisease(HD) patientswas comparedwith that of nonnal controls on 2 perceptual-motortasks,rotary pursuit and mirror tracing. HD patients demonstrateda dissociationbetweenimpaired rotary-pursuit and intact mirror-tracing skill learning. These results suggestthat different fonns of perceptual-motorskill learning are mediatedby separableneuralcircuits.A striatalmemorysystemmay be essentialfor sequence or open-loopskill learning but not for skills that involve the closed-looplearning of novel visual-responsemappings.It is hypothesizedthat working memory deficits in HD resulting from frontostriataldamagemay accountbroadly for intact and impaired long-tenn learning andmemoryin HD patients. Dissociations in patients with brain injuries between intact and inlpaired fonDSof learning provide evidencefor the existenceof memorysystems,particularneuralnetworks that mediate specific mnemonic processes.Patients with global amnesiahave bilateral lesionsin medial-temporalor diencephalic brain regions, and they exhibit a relatively circumscribeddeficit in the learning and rememberingof new events and facts, a fonD of memory that has been temled declarative(Cohen & Squire, 1980). The deficit is evident in explicit testsof recall and recognitionfor recent episodesor materialsencounteredin thoseepisodes(Oraf & Schacter, 1985). Amnesic patients, however, have shown intact memory perfonnanceon two broad classesof tasks where memory is measuredimplicitly or indirectly by a changein perfonnanceandwithout explicit referenceto any prior study or training episode: skill-learning tasks and repetition-primingtasks. In skill-learning tasks,memory is measuredas inlproveJohn D. E. Gabrieli, Department of Neurological Sciences, Rush-Presbyterian-St.Luke's Medical Center,Chicago, illinois, and Department of Psychology, Stanford University; Glenn T. Stebbins,JaswinderSingh,and ChristopherG. Goetz,Department of Neurological Sciences,Rush-Presbyterian-St.Luke's Medical Center, Chicago, illinois; Daniel B. Willingham, Departmentof Psychology,University of Virginia. JaswinderSingh is now at the Departmentof Psychiatryand BehavioralSciences,Northwestern University. This researchwas supportedby grantsfrom the Office of Naval Research(NOOOI4-92-J-184) and from the McDonnell-PewProgram in Cognitive Neuroscience. Correspondenceconcerningthis article should be addressedto John D. E. Gabrieli, Departmentof Psychology,StanfordUniversity, Stanford, California 94305. Electronic mail may be sent via Internet to gabrieli@psych.stanford.edu. 272 ment with practice in perceptual-motor, perceptual, or cognitive performance. Amnesic patients have shown intact skill learning on a number of tasks, including mirror tracing (Gabrieli, Corkin, Mickel, & Growdon, 1993; Milner, 1962), rotary pursuit (Cermak, Lewis, Butters, & Goodglass, 1973; Corkin, 1968; Heindel, Butters, & Salmon, 1988), serial reaction time (Nissen & Bullemer, 1987; Nissen, WIllingham, & Hartman, 1989), and reading mirror-reversed text (Cohen & Squire, 1980; Martone, Butters, Payne, Becker, & Sax, 1984). In repetition-priming tasks, memory is measured as a change in the speed or accuracy of processing a stimulus, usually a word or picture, due to prior exposure to that stimulus. Amnesic patients have shown intact repetition priming on a number of tasks involving words (e.g., Graf, Shimamura, & Squire, 1985; Graf, Squire, & Mandler, 1984; Warrington & Weiskrantz, 1970), representational pictures (Cave & Squire, 1992), and novel, nonrepresentational pictures (Gabrieli, Milberg, Keane, & Corkin, 1990; Musen & Squire, 1992; Schacter, Cooper, Tharan, & Rubens, 1991). The sparing of skill learning and repetition priming in amnesia indicates that those forms of memory do not depend upon the medial-temporal and diencephalic brain structures that are vital for declarative memory, but it does not indicate how many different forms of memory are involved in either skill learning or repetition priming or what neural networks subserve those forms of memory. Studies of patients with neurodegenerative diseases,especially Huntington's disease (HD) and Alzheimer's disease (AD), have provided evidence about the functional neural architecture of skill learning and repetition priming. HD patients have shown impaired skill learning on tasks of rotary pursuit (Heindel et al., 1988; Heindel, Salmon, Shults, Walicke, & Butters, 1989), reading mirror-reversed text (Martone et al., 1984), and, more variably, serial reaction time (Koopman & Nissen, 273 INTACf AND IMPAIRED SKll..L LEARNING IN HD 1991; Wlllingham & Koroshetz, 1993). HD patients, however, often show intact repetition priming (Heindel et al., 1989; Salmon, Shimamura, Butters, & Smith, 1988). AD patients have shown the reverse dissociation, exhibiting intact skill learning on tasks of rotary pursuit (Eslinger & Damasio, 1986; Heindel et al., 1988, 1989), mirror tracing (Gabrieli et al., 1993), and serial reaction time (Koopman, 1991; Koopman & Nissen, 1987) and impaired repetition priming (e.g., Gabrieli et al., 1994; Heindel et al., 1989; Keane, Gabrieli, Fennema, Growdon, & Corkin, 1991; Monti et al., 1996; Salmon et al., 1988; Shimamura, Salmon, Squire, & Butters, 1987). The double dissociation between skill learning and repetition priming in HD and AD indicates that at least some forms of skill learning and repetition priming are mediated by different memory systems. Further, knowledge of the prominent pathology in the early stages of the two diseases (in later stages of both diseases patients are untestable) provides evidence about the neural networks that mediate skill learning and repetition priming. Postmortem studies (Vonsattel et al., 1985), in vivo structural imaging (Starkstein et al., 1989), and in vivo functional imaging (Kuhl et ai, 1982; Young et al., 1986) indicate that the caudate and putamen, structures that are part of the basal ganglia or striatum, are especially affected in HD. Conversely, the striatum is relatively spared in AD (Arnold, Hyman, Flory, Damasio, & Van Hoesen, 1991; Brun & Englund, 1981). Thus, it appears that the basal ganglia are part of a memory system that mediates various forms of skill learning but not repetition priming. AD patients have marked hippocampal lesions (Arnold et al., 1991; Brun & Englund, 1981; Hyman, Van Hoesen, Damasio, & Barnes, 1984), but it is unlikely that those lesions account for their repetition-priming deficits because amnesic patients with hippocampal lesions exhibit preserved repetition priming. AD patients, unlike most amnesic patients, have marked pathology in frontal, temporal, and parietal association areas, with relative sparing of primary sensory, cerebellar, and striatal regions. Therefore, cortical areas damaged in AD, but not in HD or amnesia, may constitute memory systems that mediate repetition priming. Repetition priming, however, can be further decomposed into perceptual priming, reflecting implicit memory for stimulus fonn, and conceptual priming, reflecting implicit memory for stimulus meaning (e.g., Blaxton, 1989; Roediger, Weldon, & Challis, 1989). Both perceptual and conceptual priming are spared in amnesia, but the two forms of priming dissociate in AD patients who are often intact on perceptual priming tasks (e.g., Gabrieli et al., 1994; Keane et al., 1991) but are impaired on conceptual priming tasks (e.g., Monti et al., 19%; Salmon et al., 1988). Therefore, perceptual forms of priming may be mediated by modality-specific perceptual cortices, which are relatively spared in AD, and conceptual forms of priming may be mediated by association cortices, which are severely compromised in AD. This interpretation is supported by evidence from lesion and imaging studies indicating that visual perceptual priming is mediated by occipital cortex and that conceptual priming is mpti;"t..J1 hv left frontal and temporal-parietal cortices (Blaxton et al., 1996; Buckner et al., 1995; Demb et al., 1995; Fleischman et al., 1995; Gabrieli, Fleischman, Keane, Reminger, & Morrell, 1995; Gabrieli, Singh, Stebbins, & Goetz, 1996; Keane, Gabrieli, Mapstone, Johnson, & Corkin, 1995; Raichle et al., 1994; Squire et al., 1992; Swick & Knight, 1996). In the present study, we aimed to examine whether two forms of perceptual-motor skill learning that are spared in amnesia are further dissociable. Such a dissociation would indicate that various forms of skill learning, like various forms of repetition priming, are mediated by separable memory systems. Therefore, we examined the skill learning of one group of early-stage HD patients on both rotarypursuit and mirror-tracing tasks. We hypothesized that HD patients would show impaired learning of the rotary-pursuit skill as other HD patients have done before (Heindel et al., 1988, 1989). The performance of HD patients on mirror tracing has not been examined previously. Cerebellar lesions impair mirror-tracing skill learning (Sanes, Dimitrov, & Hallett, 1990), but it is not known whether the striatum is essential for such skill learning. One difficulty in assessingmotor skill learning in HD is the inherent confound between baseline performance ability and learning in a group of patients with a motor disease. If patients are tested under conditions identical to those for normal control participants, then any deficit could reflect initial performance difficulties, or learning difficulties, or both. This is not just a nuisance issue in measurement, because it is plausible that changes in the same neural network that mediates initial, unskilled performance constitute the basis of later, skilled performance. To minimize the confounding effects of initial performance and skill learning, some investigators have equated initial performance between HD and control groups by testing the HD patients under easier conditions (Heindel et al., 1988, 1989). We chose the same approach in our study and also explored the implications of that approach. For rotary pursuit, HD and controls were tested at speeds of rotation that resulted in equivalent initial performance. In addition, 3 other HD patients were tested under conditions that resulted in superior initial performance, so that we could examine what consequences such manipulations of initial performance have for rotary-pursuit skill learning. For mirror tracing, HD and controls were tested with one of three patterns of descending difficulty (star, diamond, square). Method Participants There were 21 participants:12 HD patients(5 male, 8 female) and 9 (3 male, 6 female)healthynormal control participants(NC; seeTable 1). The diagnosisof HD was madeby a board-certified neurologist based on a positive family history of HD and the presenceof choreatic movements.Severity of HD was assessed with the Huntington's DiseaseFunctionalCapacityScale(Shoulson & Fahn, 1979),which stagesdiseaseseverityfrom I (minimal disability) to 5 (completedisability). The HD patientswere all in the early stagesof the disease:4 patientswere ratedat Stage2, 6 274 GABRIEU, SlEBBINS, SINGH, Wll..LINGHAM, AND GOE1Z Table 1 Participant Characteristics Durationb 2 3 4 5 6 7 8 9 10 11 12 M SD 38 40 52 31 47 40 41 41 67 37 42 48 43. .7 9..2 14 12 14 12 12 16 12 14 14 12 12 14 13.2 1.3 26 26 30 28 25 29 28 26 26 27 25 26 27.0 1,.6 6 7 2 4 5 7 4 7 6 5 7 3 5.3 1.7 RP, MT RP, MT RP, MT RP, MT RP, MT RP, MT RP RP RP RP. t RP. t RP. t NC 3 2 2 . 3 - 4 - 2 3 2 2.1 1.0 HDFCS 4 4 2 3 3 2 2 3 3 3 3 2 2.8 0.7 42.8 14.6 29.9 13.8 2.1 0.3 Note. MMSE = Mini-Mental StateExamination;Ham-D = Hamilton DepressionRating Scale. RP = rotary pursuit; MT = mirror tracing; RP+ = rotary pursuit with 10-sbaseline;HDFCS = Huntington's DiseaseFunctional Disability Scale; HD = Huntington's disease;NC = nonna! control. "In years. bDurationofHD in years. M SD patientsat Stage3, and2 patientsat Stage4. Presenceor absenceof dementiawas assessedusing the Mini-Mental State Examination (MMSE; Folstein,Folstein,& McHugh, 1975).All patientsscored above 24, the standardcut-off score for dementia. Presenceor absenceof depressionwas assessed using the Hamilton Depression Rating Scale (Hamilton, 1960). All patients scored below 10, indicating that none was depressed.Nine HD participants completed the rotary-pursuittask, and 6 of those also performed the mirror-tracingtask.An additional3 HD participantsperformedthe rotary-pursuit task at a starting point superior to the NC participants. The 9 NC participants were hospital volunteers, community volunteers,and spousesof the HD participantsin good health by self-reportandnot dementedby MMSE scores(Table 1). The HD and NC groups did not differ significantly in regard to age or education.The NC group had significantly higher MMSE scores, 1(19) = 5.13,p < .001. All 9 participantsperformed the rotarypursuit task, and 8 participantsalso performedthe mirror-tracing task. Materials The rotary-pursuitapparatuspresenteda O.75-in.-diameter(1.91 cm) circular target,located3.25in. (8.26 cm) away from the center of the apparatus,that rotatedclockwise in a circular path. Participantsheld a stylus,anda photoelectricdevicetriggereda clock that measuredhow long the stylus was held directly over the targeton each trial. The mirror-tracing apparatusconsistedof an aluminum plate on which nonconductingtape was placed in one of three patterns:a six-pointedstar,a four-sideddiamond,or a square.One patternat a time was mountedon a woodenboard that was hidden from the participants' view by a near-vertical metal barrier. Participantshadto reacharoundthe metalbarrier and could seethe pattern and their handonly in a mirror, mountedon the far side of the woodenboard.For eachtrial, a counterrecordedthe numberof times participantswent off the pattern (errors), and a stopwatch recordedthe time to completetracing of the pattern. Procedure For rotary pursuit, participantsheld a stylus in their preferred hand and were told to try to maintaincontactwith a rotating spot. The apparatuscould be adjustedto move the target at various rotationsper minute for each20-s trial. An initial set of five trials wasusedto determine,individually for eachparticipant,how many rotations per minute yielded an initial performanceof about 5 s. That rotation rate was then used for the skill-learning session, which consistedof three blocks, with each block comprisedof eight 20-s trials. There was a 20-s intertrial interval. The three blocks were separatedby intervalsof about 10 min, during which participantsperformedothertests. For Inirror tracing, participantsheld the stylus in their preferred hand and were told to trace around the pattern, from a starting mark, working as quickly and accuratelyas possible.All participantswereinitially presentedwith the starpattern.If theparticipant could not initiate a movementon the star,the diamondfigure was mounted;if the participant could not initiate a movementon the diamond, the squarewas mounted.All skill-learning trials were conductedwith onepatternperparticipant.Testingconsistedof two blocks with five trials per block. Therewere no intervals between trials, andthe two blockswere separated by intervalsof 10-15 min during which participantsperformedothertests. Results Rotary Pursuit The skill-learning measurewas time-on-targetper trial (maximumof 20 s). The HD and NC groupswere testedat meanrotationsper minute,respectively,of28.3 s (SD = 9.3) and 44.4 s (SD = 9.8); this difference was significant, 1(12)= 3.10,p < .01.The two groupswerewell matchedon initial time-on-targetperformancewith the HD and NC INTACT AND IMPAIRED SKll..L LEARNING IN HD groups scoring, respectively, means of 5.6 s and 6.3 s (p > .70). Time-on-target scores were analyzedin a repeatedmeasuresanalysisof variance (ANOYA) with variablesof group (HD, NC), block (Block 1, Block 2, Block 3), and trial (eight trials per block); trials were nestedwithin blocks. Participants showed skill learning by increasing time-on-target across blocks, F(2, 32) = 54.55, MSE = 3.04,p < .001,andtrials,F(7, 112)= 4.55,MSE= 1.54, p < .01.The HD group,however,showedlessskill learning than the NC group as evidencedby a significant effect of group, F(I, 16) = 16.87,MSE = 63.46,p < .001, and a significantinteractionbetweengroup andblock, F(2, 32) = 38.31, p < .001. A separate analysis of the data from the 6 HD and 8 NC participants who also performed mirror tracing showed a reliable skill-learning deficit in the HD patients,with a significanteffect of group,F(I, 12) = 12.96, MSE = 62.45,p < .01, anda significantinteractionbetween group andblock, F(7, 84) = 3.14,MSE = 3.08,p < .01 (see Figure 1). The HD patientsdemonstratedlessskill learningthanthe NC group, but the question remained as to whether they 275 showed any skill learning at all. A repeatedmeasures ANaYA on the meantime-on-targetper block for the lID patients did not reveal a reliable change across blocks (p > .26). The lID patients who performed the task at rotation ratesthat yielded an initial time-on-targetof about 10 s (superiorto that of the NC and other lID group) also showedno rotary-pursuitskill learning(seeFigure2). Mirror Tracing In the HD group, 4 participants traced the star, 1 participant traced the diamond, and 1 participant traced the square. In the NC group, 7 participants traced the star, and 1 participant traced the square. The skill-learning measures were completion time (number of seconds taken to trace a pattern) and errors (number of contacts with the metal plate signifying departures from the pattern; see Figure 3). Mean performance on Trial 1 was not matched as closely as in the rotary-pursuit task. On Trial 1, the HD and NC groups did not differ reliably for completion time (lID: M = 93.8, SD = 69.6;NC: M = 60.6,SD = 32.1),t(12) = 1.2,p = Trial Figure 1. Rotary-pursuitresultsfor patientswith Huntington'sdisease(HD) and normal control (NC) participants.Top: Mean time on targetfor 9 HD and9 NC participantsin threeblocks of eight trials. Bottom: Mean time on target for 6 HD and 8 NC participants who also performed the mirror-tracin2task.Bracketsarestandarderrorsof the means. ~ GABRIEU, STEBBINS, SINGH, WllLINGHAM, 276 12. AND GOETZ --, I 'II ~ ~ ~ "OJ 10 C) .. 10 I- E> c G---~e- 0 GI E 8 ~ i= c 10 GI / 7 --E1 ~ .L Figure 2. Rotary-pursuitresultsfor 9 normal control (NC) participants;9 patientswith Huntington's disease(HD) whoseinitial performancewas equatedwith that of NC participantsby slowing the speedof rotation,and3 patientswith Huntington'sdisease(HD+) whoseinitial performancewas madesuperiorto that ofNC participantsby further slowing the speedof rotation.Meantime on target per block. .25, but the HD patients made more errors (lID: M = 29.8, SD = 19.5; NC: M = 12.8, SD = 8.4),1(12) = 1.2,p < .05. Completion-time scores and error scores (see Figure 3) were analyzed in separate repeated measures ANOVAs with Trial Trial Figure 3. Mirror-tracing resultsfor 6 patientswith Huntington's disease(HD) and 8 normal control (NC) participants.Top: Mean numberof errorsfor two blocksof five trials. Bottom:Meantime to tracepatternsfor the sameparticipantson the sametrials. Brackets are standarderrorsof the means. variables of group (RD, NC), block (Block 1, Block 2), and trial (five trials per block); trials were nested within blocks. Participants showed skill learning by tracing the patterns progressively faster acrossblocks, F(I, 12) = 15.44, MSE = 1125.31, P < .01, and trials, F(4, 48) = 15.70, MSE = 129.12,p < .001, and by making fewer errors across blocks, F(I, 12) = 8.86, MSE = 107.80, p < .05, and trials, F(4, 48) = 8.85, MSE = 22.30,p < .001. For both skill-learning measures, there were Block X Trial interactions, indicating that within-block improvement across trials decreasedacross blocks: for completion time, F(4, 48) = 4.57, p < .01; for errors, F(4, 48) = 3.38,p < .05. There was no main effect of group on either skill-learning measure and, most important, no interaction between group and either block or trial, indicating that the HD and NC groups improved similarly on mirror tracing. Discussion This studyexaminedwhetherHD patientswould show a skill-learning deficit on mirror tracing, as they have on skill-learning tasks of rotary pursuit, serial reaction time, and mirror reading.The HD patients in the presentstudy were impaired relative to control participants on rotarypursuit skill learning. In fact, HD patients showed no reliable rotary-pursuit skill learning whether their initial level of performancewas equal to or superior to that of control participants.From the first to the last trial, HD and NC groups improved their rotary-pursuit performanceby 16% and 48%, respectively.The HD impairment is consistent with prior findings (Heindelet al., 1988, 1989).In stark contrast,the sameHD patientsshowedmirror-tracing skill learningthat was statisticallyindistinguishablefrom that of control participants.HD mirror-tracing skill learning was robust. From the first to the last trial, HD and NC groups improved the accuraciesof their performancesby 70% and 48%, respectively,and increasedthe speedof their perfor- INTACT AND IMPAIRED SKILL LEARNING IN HD mances by 56% and 67%, respectively. Thus, there was a clear-cut dissociation in a group of HD patients between impaired rotary-pursuit skill learning and intact mirrortracing skill learning. The preservation of mirror-tracing skill learning in HD must be considered with some caution for several reasons. First, initial HD performance was not equated fully with that of the NC group. On the first trial, HD patients were not significantly slower than NC participants, but they were significantly less accurate. The finding, however, that HD patients had intact mirror-tracing skill learning on the speed measure where there was no reliable initial difference favors the interpretation that the HD group showed normal learning. Second, the interpretation of preserved mirror-tracing skill learning rests on the absenceof any statistically reliable interaction between groups and learning measures, and this absence occurred with small groups of participants. The study, however, had sufficient statistical power to detect the rotary-pursuit deficit. Further, inspection of the HD learning curves on the mirror-tracing task shows that their skill learning closely paralleled that of the NC group. Thus, there is no apparent evidence that HD patients had any deficit that would become significant in a larger sample. It will be assumed, therefore, for purposes of the remaining discussion, that HD patients had intact mirror-tracing skill learning that was complicated by their motor and cognitive disease. There are no published studies of mirror tracing in HD, but there is a study of prism adaptation in HD (paulsen, Butters, Salmon, Heindel, & Swenson, 1993). In that study, participants pointed toward a target while wearing distorting prisms that shifted objects 20° laterally. HD patients, relative to control and AD participants, failed in adapting to the prisms after visuomotor feedback. The prism and mirrortracing tasks share some apparent features: Both tasks involve visually guided motor learning in an environment with transposed visuomotor relations. Paulsen et al., however, found that there was a correlation between dementia severity and impaired prism adaptation in the HD patients (but not in the AD patients): Less demented HD patients were unimpaired. The dementia severity of HD patients in the present study resembles that of the less demented HD group in the Paulsen study. The two studies are actually in accord, therefore, in finding that mildly demented HD patients retain the ability to acquire motor skills in altered visuomotor environments. Other studies with HD patients provide further evidence that dementia severity or other patient variables can have major consequenceson HD patients' skill-learning abilities. Heindel et al. found correlations between dementia severity and both rotary pursuit learning (1988, 1989) and weight biasing (Heindel, Salmon, & Butters, 1991). More demented HD patients have shown impaired cognitive skill learning on the Tower-of-Hanoi and Tower-of- Toronto puzzles, but HD patients with less dementia have shown intact cognitive skill learning on those tasks (although this latter finding was more variable for the Tower-of- Toronto study; Butters, Wolfe, Martone, Granholm, & Cermak, 1985; Saint-Cyr, Taylor, & Lang, 1988). Dementia severity appears to be an important variable in determinin~ HD patients' skill-learning perfor- 277 mance, but that variability does not apply to the dissociation in the present study that occurred in a single group of patients. There are several ways to consider the dissociation between HD performance on two skill-learning tasks. One constraint is that it is single, not a double, dissociation. Thus, it could be that learning on both tasks involves the same memory system, but that rotary pursuit has greater demands upon that system than does mirror tracing. It was, however, more difficult to equate HD patients on the mirror-tracing than the rotary-pursuit task, and more HD patients could perform the rotary-pursuit than the mirror-tracing task. These findings do not favor the notion that mirror tracing is less demanding of a common memory system than is rotary pursuit. Alternatively, skill learning on the two tasks may be mediated by memory systems that differ only by a single component that is essential for rotary pursuit but not mirror tracing. In either case, no double dissociation would be expected. A third possibility is that the two skill-learning tasks depend upon separable brain regions. The integrity of the striatum appears essential for rotary-pursuit skill learning, because such learning is consistently impaired in HD patients and also in patients with Gilles de la Tourette's syndrome who have abnormal striatal anatomy (Stebbins, Singh, Weiner, Goetz, & Gabrieli, 1995). Conversely, the cerebellum may be essential for mirror-tracing skill learning. Patients with lesions in some, but not all, locations in the cerebellum have been reported to show impaired mirrortracing skill learning (Sanes et al., 1990). Cerebellar patients have also been reported to show impaired motor adaptation in other altered visual environments (Gauthier, Hofferer, Hoyt, & Stark, 1979; Weiner, Hallett, & Funkenstein, 1983) and impaired visually guided tracking (Beppu, Suda, & Tanaka, 1984; Beppu, Nagaoka, & Tanaka, 1987). Therefore, it is possible that a double dissociation between the two kinds of learning could occur in patients with striatal or cerebellar lesions. The performance, however, of cerebellar patients on rotary-pursuit skill learning remains to be determined. Rotary pursuit and mirror tracing differ in many ways, and it is unknown as to what critical difference between the tasks renders skill learning impaired or intact in HD. Two studies have reported single dissociations in HD on skill-learning tasks that were more matched in perceptual and motor demands. In a serial reaction time task, HD participants were impaired in learning a sequence-specific skill for pressing four keys in response to targets appearing in four locations in a recurring sequence (Willingham & Koroshetz, 1993). HD patients had an impairment in using the recurring sequence to predict where the next target would appear.The same HD patients showed intact skill learning when the task was to press a key one position to the right of the target. In this task, there was no sequence to be learned. Rather, participants learned a new mapping between visual stimuli (targets in a particular location) and motor responses (pressing the key one position to the right). In a task where participants tracked a cursor with a joystick, HD patients showed a normal pattern of skill learning when the cursor moved 278 GABRIEU. STEBBINS. SINGH. Wll..LINGHAM. AND GOETZ randomly but impaired learning when the cursor moved in a repeating pattern (Wlllingham, Koroshetz, & Peterson, 1996). Willingham proposed that the two within-task dissociations could be explained by a distinction between the learning of repetitive motor sequences,which depends upon the striatum, and the learning of new mappings between visual cues and motor responses, which does not depend upon the striatum. Thus, HD patients were impaired for learning repeated sequences of movements in both studies but were intact for learning new, constant mappings between visual cues and motor responses.The same distinction could apply to the present study. Skill learning on rotary pursuit may involve the learning of a pattern-specific series of repetitive movements. Indeed, the rotary-pursuit task in the present study and the tracking of a repeating sequence (Willingham et al., 1996) are quite similar in this regard. Rotary-pursuit skill learning does not require any new mapping between visual cues and motor responses. Conversely, skill learning on mirror tracing appears straightforwardly to reflect the learning of a new mapping between reversed visual inputs and motor outputs. Further, mirror tracing may not involve sequence-specific learning because both control and AD groups demonstrated nearly perfect transfer of training across two different patterns that involved different sequences of movements (Gabrieli et al., 1993). Thus, Willingham's distinction between two kinds of skill learning is consistent with the HD dissociation between impaired rotary-pursuit learning and intact mirror-tracing learning. A second distinction that may apply to the HD dissociation is that between closed-loop and open-loop skillieaming. Skill learning for mirror tracing may be classified as closed-loop skillieaming because participants are provided continuous external, visual feedback about errors in movement. Participants can pause at any moment to use current perceptual feedback about present position and direction of movement to correct any error in the motor programming controlling their movements. Knowledge of results is continuous and immediate. In rotary pursuit, however, the target moves too rapidly and continuously for participants to use current visual feedback as a cue for motor programming or a source for error correction. Rather, skill learning for rotary pursuit may be classified as open-loop learning where good performance requires participants to program movements on the basis of a prediction about where the target will be by the time a motor command is executed. Thus, learning a skill for rotary pursuit, like learning a skill for serial reaction time responses to a recurrent sequence, involves responding to future target locations that are sequentially predicted upon the basis of currently perceived target locations. Further, knowledge of results is delayed in rotary pursuit. Participants receive visual feedback that their hand has left the target after a faulty prediction has been followed. Thus, neither error correction nor successful motor programming can be driven by present perceptual information. Rather, participants must construct a model that uses present perceptual feedback as a predictor for motor programming and update that model after an error has occurred. Th~ idea that the striatum has a specific role in open-loop learning has both supportive and contradictory evidence. Studies with Parkinson's disease (PD) patients have indicated that the striatum may be critical for open-loop motor movements that are guided by prediction rather than by response to current sensory information (Cooke, Brown, & Brooks, 1978; Flowers, 1978; Stem, Mayeux, Rosen, & llson, 1983; but see, Hockerman & Aharon-Peretz, 1994). When performing tracking tasks, PD patients were abnormally dependent upon visual feedback and did not show the anticipatory motor planning that normal participants did. Another study, however, reported a normal advantage for PD patients when they tracked a target moving in a repeating versus a random pattern (Bloxham, Mindel, & Frith, 1984). PD patients without dementia, however, exhibit intact rotary-pursuit learning (Heindel et al., 1989), so it appears that motor and skill-learning deficits vary considerably among PD, as well as RD, patients. The sequencingmapping and open-closed loop distinctions need not be contradictory. For example, animal studies indicate that striatal cells code open-loop movements only during the performance of sequencesof movements (Kimura, Aosaki, Hu, Ishida, & Watanabe, 1992). Thus, under many circumstances, the learning of sequencesmay involve open-loop learning, whereas the learning of mappings may involve closed-loop learning. Finally, it is of interest to consider whether there are similarities between the perceptual-motor skill-learning deficits seen in RD and more nonmotoric learning and memory deficits also seen in early RD. RD patients are impaired often on Tower cognitive skill-learning tasks (Butters et al., 1985; Saint-Cyr et al., 1988). These cognitive tasks are open-loop in nature because they require the selection of movements in response to a mental model of a problem solution; there is no perceptual information that provides definitive feedback to guide performance (except for the final step of the problem). The patients in the present study also exhibited a characteristic RD pattern of verbal memory deficits comprised of relatively intact recognition performance and impaired performance on tests of free recall, self-ordering pointing, and recency judgments (Singh, Gabrieli, Stebbins, & Goetz, 1994). Gabrieli et al. (1996) proposed that this pattern of intact and impaired verbal memory performance reflects the severe impairment of working memory in RD, PD, and Tourette's syndrome. Verbal memory tasks are intact or impaired to the extent they make demands upon the reduced working memory capacities exhibited by RD, PD, and Tourette's patients (Gabrieli et al., 1996; Singh et al., 1994; Stebbins et al., 1995). Open-loop skill learning that involves the planning of sequences of movements may also have much higher demands on working memory than closed-loop skillieaming that uses visual cues to guide. Indeed, Goldman-Rakic (1987) noted that a fundamental feature of working memory is that it guides behavior on the basis of internal, symbolic models as opposed to external, perceptual feedback. Thus, it is plausible that damage to frontostriatal working memory systems in RD, PD, and Tourette's syndrome diminishes long-term learning and memory on tasks that require internally guided, open-loop thought, including INTACT AND IMPAIRED SKILL LEARNING IN HD certain perceptual-motor skills (rotary pursuit, serial response time with sequences), cognitive skills (Tower problems), and strategic verbal memory (recall, recency judgments). Other learning and memory tasks that are less dependent on working memory capacity may be relatively or fully intact in HD, PD, and Tourette's, including perceptualmotor skills (mirror tracing) and nonstrategic verbal memory tasks (recognition). It is likely that the diverse forms of long-term learning and memory impaired in striatal patients do not depend on a single frontostriatal system but rather on multiple, anatomically distinct frontostriatal loops (Alexander, DeLong, & Strick, 1986). The loops mediate working memory processesin different domains (WIlson, 0' Scalaidhe, & Goldman-Rakic, 1993), but they may mediate the same kinds of working memory contributions in each of those domains. This hypothesis, although speculative, would provide an integrated account for the various forms of learning and memory that do and do not depend upon the integrity of the basal ganglia. References Alexander, G. E., DeLong, M. R., & Strick, P. L. (1986). Parallel organization of functionally segregated circuits linking basal ganglia and cortex. Annual Review of Neuroscience, 9, 357-381. Arnold, S. E., Hyman, B. T., Flory, J., Damasio, A. R., & Van Hoesen, G. W. (1991). The topographical and neuroanatomical distribution of neurofibrillary tangles and neuritic plaques in the cerebral cortex of patients with Alzheimer's disease. Cerebral Cortex, 1, 103-116. Beppu, H., Nagaoka, M., & Tanaka, R. (1987). Analysis of cerebellar motor disorders by visually-guided elbow tracking movement. 2. Contribution of the visual cues on slow ramp pursuit. Brain, 110, 1-18. Beppu, H., Suda, M., & Tanaka, R. (1984). Analysis of cerebellar motor disorders by visually-guided elbow tracking movement. Brain, 107, 787-809. B1axton, T. A. (1989). Investigating dissociations among memory measures: Support for a transfer-appropriate processing framework. Journal of Experimental Psychology: Learning, Memory, and Cognition, 15, 657-668. Blaxton, T. A., Bookheimer, S. Y., Zeffiro, T. A., Fig10zzi, C. M., William, D. G., & Theodore, W. H. (1996). Functional mapping of human memory using PET: Comparisons of conceptual and perceptual tasks. Canadian Journal of Experimental Psychology, 50, 42-56. Bloxham, C. A., Mindel, T. A., & Frith, C. D. (1984). Initiation and execution of predictable and unpredictable movements in Parkinson's disease.Brain, 107, 371-384. Brun, A., & Englund, E. (1981). Regional pattern of degeneration in Alzheimer's disease: Neuronal loss and histopathological grading. Histopathology, 5, 549-564. Buckner, R. L., Petersen, S. E., Ojemann, J. G., Miezin, F. M., Squire, L. R., & Raichle, M. E. (1995). Functional anatomical studies of explicit and implicit memory retrieval tasks. Journal of Neuroscience, 12, 12-29. Butters, N., Wolfe, J., Martone, M., Granholm, E., & Cermak, L. S. (1985). Memory disorders associated with Huntington's disease: Verbal recall, verbal recognition, and procedural memory. Neuropsychologia, 6, 729-744. Cave, C. B., & Squire, L. R. (1992). Intact and long-lasting repetition priming in amnesia. Journal of Experimental Psychology: Learning, Memory, and Cognition, 18,509-520. 279 Cennak, L. S., Lewis, R., Butters, N., & Goodglass,H. (1973). Role of verbal mediation in perfonnanceof motor tasks by Korsakoffpatients.Perceptionand Motor Skills, 37, 259-263. Cohen, N. J., & Squire, L. R. (1980). Preservedlearning and retention of pattern-analyzingskill in amnesia:Dissociationof knowing how andknowing that.Science,210, 207-210. Cooke, J. D., Brown, J. D., & Brooks, V. B. (1978). Increased dependenceon visual infonnation for movement control in patientswith Parkinson'sdisease.CanadianJournal of Neurological Sciences,5, 413-415. Corkin, S. (1968).Acquisition of motor skill after bilateral medial temporal-lobeexcision.Neuropsychologia,6, 255-265. Demb,J. B., Desmond,J. E., Wagner,A. D., Vaidya,C. J., Glover, G. H., & Gabrieli, J. D. E. (1995). Semanticencoding and retrieval in the left inferior prefrontalcortex:A functional MRI study of task difficulty and process specificity. Journal of Neuroscience,15, 5870-5878. Eslinger,P.J., & Damasio,A. R. (1986).Preservedmotor learning in Alzheimer's disease:Implicationsfor anatomyand behavior. JournalofNeuroscience,6,3006-3009. Fleischman,D. A., Gabrieli, J. D. E., Reminger,S., Rinaldi, J., Morrell, F., & Wilson, R. (1995). Conceptual priming in perceptualidentification for patientswith Alzheimer's disease anda patientwith a right occipital lobectomy.Neuropsychology, 9, 187-197. Flowers,K. (1978). Lack of prediction in the motor behaviourof Parkinsonism.Brain, 101, 35-52. Folstein, M. F., Folstein, S. E., & McHugh, P. R. (1975). "Mini-mental state."A practical methodfor gradingthe cognitive state of patients for the clinician. Journal of Psychiatric Research,12, 189-198. Gabrieli, J. D. E., Corkin, S., Mickel, S. F., & Growdon, J. H. (1993). Intact acquisition and long-tenD retention of mirrortracing skill in Alzheimer's diseaseand in global amnesia. BehavioralNeuroscience,107, 899-910. Gabrieli, J. D. E., Fleischman,D. A., Keane, M. M., Reminger, S. L., & Morrell, F. (1995). Double dissociation between memorysystemsunderlyingexplicit andimplicit memoryin the humanbrain. PsychologicalScience,6, 76-82. Gabrieli,J. D. E., Keane,M. M., Stanger,B. Z., Kjelgaard,M. M., Corkin, S., & Growdon, J. H. (1994). Dissociations among structural-perceptual,lexical-semantic,and even-fact memory systemsin amnesic,Alzheimer's, and nonnal subjects.Cortex, 30,75-103. Gabrieli,J. D. E., Milberg, W., Keane,M. M., & Corkin, S. (1990). Intact priming of patternsdespiteimpaired memory.Neuropsychologia,28, 417-427. Gabrieli, J. D. E., Singh,J., Stebbins,G. T., & Goetz,C. G. (1996). Reducedworking memory span in Parkinson's disease:Evidence for the role of frontostriatal system in working and strategicmemory.Neuropsychology, 10, 322-332. Gauthier,G. M., Hofferer, J. M., Hoyt, W. F., & Stark,L. (1979). Visual-motoradaptation:Quantitativedemonstrationin patients with posterior fossa involvement. Archives of Neurology,36, 155-160. Goldman-Rakic,P.S. (1987).Circuitry of primateprefrontalcortex and regulation of behavior by representationalmemory.In F. Plum (Ed.), Handbookof physiology-the nervoussystemV (pp. 373-417).New York: Oxford University Press. Graf, P.,& Schacter,D. L. (1985).Implicit andexplicit memoryfor new associationsin nonnal and amnesic subjects.Journal of ExperimentalPsychology:Learning, Memory, and Cognition, 11,501-518. Graf, P.,Shimamura,A. P., & Squire,L. R. (1985).Priming across modalities and priming acrosscategory levels: Extending the 280 GABRIEU, STEBBINS, SINGH, WILLINGHAM, AND GOE1L domainof preservedfunction in amnesia.Journal of Experimental Psychology:Learning,Memory,and Cognition,11,386-396. Oraf, P., Squire,L. R., & Mandler,G. (1984).The informationthat amnesicpatientsdo not forget.Journal of ExperimentalPsychology: Learning,Memory,and Cognition,10, 164-178. Hamilton, M. (1960). A rating scale for depression.Journal of Neurology,Neurosurgery,and Psychiatry,23, 56-62. Heindel, W. C., Butters, N., & Salmon, D. P. (1988). Impaired learning of a motor skill in patientswith Huntington'sdisease. BehavioralNeuroscience,102, 141-147. Heindel,W. C., Salmon,D. P.,& Butters,N. (1991).The biasingof weight judgments in Alzheimer's and Huntington's disease:A priming or programmingphenomenon?Journal of Clinical and ExperimentalNeuropsychology,13, 189-203. Heindel, W. C., Salmon,D. P., Shults, C. W., Walicke, P. A., & Butters, N. (1989). Neuropsychologicalevidencefor multiple implicit memorysystems:A comparisonof Alzheimer's,Huntington's, andParkinson'sdiseasepatients.TheJournal of Neuroscience,9, 582-587. Hockerman, S., & Aharon-Peretz,J. (1994). Two-dimensional tracingandtrackingin patientswith Parkinson'sdisease.Neurology,44,III-116. Hyman,B. T., Van Hoesen,G. W., Damasio,A. R., & Barnes,C. L. (1984).Alzheimer's disease:Cell-specificpathologyisolatesthe hippocampalformation.Science,225, 1168-1170. Keane,M. M., Gabrieli, J. D. E., Fennema,A. C., Orowdon,J. H., & Corkin, S. (1991). Evidence for a dissociation between perceptual and conceptual priming in Alzheimer's disease. BehavioralNeuroscience,105,326-342. Keane,M. M., Gabrieli, J. D. E., Mapstone,H., Johnson,K. A., & Corkin, S. (1995). Double dissociationof memory capacities after bilateral occipital-lobe or medial temporal-lobelesions. Brain, 118,1129-1148. Kimura, M., Aosaki, T., Hu, Y., Ishida,A., & Watanabe,K. (1992). Activity of primateputamenneuronsis selectiveto the modeof voluntary movement:Visually guided,self initiated, or memoryguided.ExperimentalBrain Research,89, 473-477. Knopman,D. (1991). Long-term retention of implicitly acquired learningin patientswith Alzheimer's disease.Journal of Clinical and ExperimentalNeuropsychology, 13(6),880-894. Knopman, D. S., & Nissen, M. J. (1987). Implicit learning in patients with probable Alzheimer's disease.Neurology, 37, 784-788. Knopman, D., & Nissen, M. J. (1991). Procedural learning is impaired in Huntington's disease:Evidence from the serial reactiontime task.Neuropsychologia,29, 245-254. Kuhl, D. E., Phelps,M. E., Markham, C. H., Metter, E. J., Riege, W. H., & Winter, J. (1982). Cerebralmetabolismand atrophyin Huntington'sdiseasedeterminedby FDG and computedtomographicscan.Annalsof Neurology,12, 425-434. Martone,M., Butters,N., Payne,M., Becker,J. T., & Sax, D. S. (1984).Dissociationsbetweenskill learningandverbalrecognition in amnesiaand dementia.Archives of Neurology, 41, 965-970. Milner, B. (1962).Les troublesde la memoire accompagnantdes lesions hippocampiquesbilaterales [Memory problems with bilateral hippocampallesions].In Psychologiede l'hippocampe. Paris:CentreNationalde la RechercheScientifique. Monti, L. A., Gabrieli, J. D. E., Reminger,S. L., Rinaldi, J. A., Wilson, R. S., & Fleischman,D.A. (1996).Differential effectsof aging and Alzheimer's diseaseupon conceptualimplicit and explicit memory.Neuropsychology, 10, 101-112. Musen, G., & Squire,L. R. (1992).Nonverbalpriming in amnesia. Memory and Cognition,20, 441-448. Nissen, M. J., & Bul1emer, P. (1987). Attentional requirements of learning: Evidence from perfonnance measures. Cognitive Psychology, 19, 1-32. Nissen, M. J., Willingham, D., & Hartman, M. (1989). Explicit and implicit remembering: When is learning preserved in amnesia? Neuropsychologia, 27,341-352. Paulsen, J. S., Butters, N., Salmon, D. P., Heindel, W. C., & Swenson, M. R. (1993). Prism adaptation in Alzheimer's and Huntington's disease. Neuropsychology, 7,73-81. Raichle, M. E., Fiez, J. A., Videen, T. 0., MacLeod, A. K., Pardo, J. V., Fox, P. E., & Petersen, S. E. (1994). Practice-related changes in human brain functional anatomy during nonmotor learning. Cerebral Cortex, 4, 8-26. Roediger, H. L., Weldon, M. S., & Challis, B. H. (1989). Explaining dissociations between implicit and explicit measures of retention: A processing account. In H. L. ROediger & F. I. M. Craik (Eds.), Varieties of memory and consciousness: Essays in honour of Endel Tulving (pp. 3-14). Hillsdale, NJ: Erlbaum. Saint-Cyr, J. A., Taylor, A. E., & Lang, A. E. (1988). Procedural learning and neostriatal function in man. Brain, 111,941-959. Salmon, D. P., Shimamura, A. P., Butters, N., & Smith, S. (1988). Lexical and semantic deficits in patients with Alzheimer's disease. Journal of Clinical and Experimental Neuropsychology, 10, 477-494. Sanes, J. N., Dimitrov, B., & Hallett, M. (1990). Motor learning in patients with cerebellar dysfunction. Brain, 113, 103-120. Schacter, D. L., Cooper, L. A., Tharan, M., & Rubens, A. B. (1991). Preserved priming of novel objects in patients with memory disorders. Journal of Cognitive Neuroscience, 3, 117-130. Shimamura, A. P., Salmon, D. P., Squire, L. R., & Butters, N. (1987). Memory dysfunction and word priming in dementia and amnesia. Behavioral Neuroscience, 101, 347-351. Shoulson, I., & Fahn, S. (1979). Huntington's disease: Clinical care and evaluation. Neurology, 29, 1-3. Singh, J., Gabrieli, J. D. E., Stebbins, G. T., & Goetz, C. G. (1994). Impairment of working memory in patients with Huntington s disease. Manuscript submitted for publication. Squire, L. R., Ojemann, J. G., Miezin, F. M., Petersen, S. E., Videen, T. 0., & Raichle, M. E. (1992). Activation of the hippocampus in normal humans: A functional anatomical study of memory. Proceedings from the National Academy of Sciences, USA, 89, 1837-1841. Starkstein, S. E., Fo1stein, S. E., Brandt, J., Pearlson, G. D., McDonnell, A., & Fo1stein, M. (1989). Brain atrophy in Huntington's disease. Neuroradiology, 31, 156-159. Stebbins, G. T., Singh, J., Weiner, J., GOetz, C. G., & Gabrieli, J. D. E. (1995). Selective impairments of memory functioning in unmedicated adults with Gilles de la Tourette's syndrome. Neuropsychology, 9, 329-337. Stem, Y., Mayeux, R., Rosen, J., & llson, J. (1983). Perceptual motor dysfunction in Parkinson's disease: A deficit in sequential and predictive voluntary movement. Journal of Neurology, Neurosurgery, and Psychiatry, 46, 145-151. Swick, D., & Knight, R. T. (1996). Is prefrontal cortex involved in cued recall? A neuropsychological test of PET findings. Neuropsychologia, 34, 1019-1028. Vonsattel, J. P., Myers, R. H., Stevens, T. J., Ferrante, M. S., Bird, E. D., & Richardson, E. P. (1985). Neuropathological classification of Huntington's disease. Journal of Neuropathology and Experimental Neurology, 44, 559-577. Warrington, E. K., & Weiskrantz, L. (1970). The amnesic syndrome: Consolidation or retrieval? Nature, 228, 628-630. Weiner, M. J., Hallett, M., & Funkenstein, H. H. (1983). Adaptation to lateral displacement of vision in patients with lesions of the central nervous system. Neurology, 33, 766-772. INTACf AND IMPAIRED SKll..L LEARNING IN HD Willingham, D. B., & Koroshetz, W. J. (1993). Evidence for dissociable motor skills in Huntington's diseasepatients. Psychobiology, 21, 173-182. Willingham, D. B., Koroshetz, W. J., & Peterson, E. W. (1996). Motor skills have diverse neural bases: Spared and impaired skill acquisition in Huntington's disease. Neuropsychology, 10, 315321. Wilson, F. A. W., O'Scalaidhe, S. P., & Goldman-Rakic, P. S. (1993). Dissociation of object and spatial processing domains in primate prefrontal cortex. Science, 260, 1955-1957. 281 Young,A. B., Penney,J. B., Startosa-Rubenstein, S., Markel, D. S., Berent,S., Giordani, B., Ehrenkaufer,R., Jewett,D., & Hichwa, R. (1986). PET scan investigationsof Huntington's disease: Cerebral metabolic correlates of neurological features and functionaldecline.Annalsof Neurology,20, 296-303. ReceivedSeptember13, 1994 RevisionreceivedOctober22,1996 AcceptedOctober23,1996 .